
THE EFFECTIVENESS OF AUDIO HYPNOTHERAPY IN REDUCING POSTPARTUM DEPRESSION DURING NEW NORMAL
Rosyati Pastuty1*, Elita Vasra1, Gustiana2
1Department of Midwifery, Health Polytechnic of Palembang, Indonesia
2Department of Midwifery, Health Polytechnic of Aceh, Indonesia
* Corresponding author:
Rosyati Pastuty, Jl. Inspektur Yazid, Sekip Jaya, Kec. Kemuning, Kota Palembang, Sumatera Selatan 30114, Indonesia, Orcid: https://orcid.org/0000-0003-0804-2291
Email: rrosyatipastuty@gmail.com

Cite this article
ABSTRACT
Background: Postpartum depression is a life-threatening mental health disorder and occurs in 10-15% of women. “Globally, the incidence of postpartum depression reaches 10-15%. There are few reports in countries such as Malta, Malaysia, Austria, Denmark and Singapore. While in other countries such as Brazil, South Africa, Taiwan, Korea, Italy, and Costa Rica, symptoms of postpartum depression are reported to be quite high”. “Based the criteria of the Diagnostic and Statistical Manual of Mental Disorders, fourth edition (DSM-IV) and the Edinburgh Postnatal Depression Scale (EPDS). Audio hypnotherapy, which is the provision of positive suggestions delivered through MP3, is a method to reduce the level of postpartum depression. This study aims to determine the effectiveness of audio hypnotherapy in reducing postpartum depression during the new normal.
Materials and Methods: This quasi-experimental study used a pretest-posttest design involving 60 postpartum mothers with a history of normal delivery at 2 Midwife's clinics in Palembang City and 1 Midwife's clinic in Aceh. Postpartum depression levels were assessed using the Edinburgh Postnatal Depression Scale (EPDS). Data analysis used Paired Samples Test to determine differences in postpartum depression levels before and after listening to Hypnotherapy audio.
Results: There was a decrease in postpartum mothers' depression level after listening to hypnotherapy audio for ± 2 weeks. Depression incidence before giving audio hypnotherapy has a mean value = 11.15, while after giving audio hypnotherapy, it increases to 8.90, with P-value <0.05.
Conclusion: Audio hypnotherapy therapy has proven to be effective in reducing the incidence of depression in postpartum mothers.
Keywords: Audio Hypnotherapy, depression, Post-partum mother
INTRODUCTION
Antepartum Depression (APD) and Postpartum Depression (PPD), are disorders characterized by mood swings during pregnancy and after childbirth, which have a negative impact on the physical and mental health of mothers and children [1,2]. Melville et al [3] in their study reported that prevalence rates ranged from 4.8% to 18.4% for mild depression, and from 5.1% to 12.7% for severe depression.
Globally, the incidence of postpartum depression reaches 10-15%. There are few reports in countries such as Malta, Malaysia, Austria, Denmark and Singapore. While in other countries such as Brazil, South Africa, Taiwan, Korea, Italy, and Costa Rica, symptoms of postpartum depression are reported to be quite high. A study in India, involving 359 primiparous mothers, reported an 11% incidence of postpartum depression [4,5].
Approximately 70% of new mothers have mild depressive symptoms which generally peak in the 2 to 5 days after delivery. These symptoms usually begin to subside spontaneously within 2 weeks, but if not detected immediately and treatment is delayed, it can develop into postpartum depression [6].
Most pregnant women who face the birth process experience feelings of anxiety, even depression. Factors causing postpartum depression consist of biological factors, characteristics and background of the mother. Levels of the hormones estrogen (estradiol and estriol), progesterone, prolactin, cortisol which increase and decrease too quickly or too slowly are biological factors that cause postpartum depression [7]. The greater the decrease in estrogen and progesterone levels after childbirth, the greater the tendency for a woman to experience depression in the first 10 days after giving birth [8]. The estrogen and progesterone exert a suppressive effect on the activity of the monoamine oxidase enzyme. This enzyme can inactivate both noradrenaline and serotonin, which play a role in mood and depression. Estradiol and estriol are the active forms of estrogen formed by the placenta. Estradiol functions to strengthen the function of neurotransmitters by increasing the synthesis and reducing the breakdown of serotonin. Therefore, theoretically the decrease in estradiol levels due to childbirth plays a role in causing postpartum depression [2,6,9,10]. Biological causative factors are difficult and rarely measured in terms of maternal depressive symptoms [11]. Other factors that influence maternal depressive symptoms described in several studies include interpersonal variables (neural disorders, poor life experiences), social variables (marital dissatisfaction, lack of social support), and clinical variables related to pregnancy (risk in current pregnancy, problems with previous pregnancy) [12].
Antepartum Depression (APD) and Postpartum Depression (PPD) together are called perinatal depression. Various diagnostic criteria with major depression occur during pregnancy or within 4 weeks after delivery [13]. Based on previous research, women with a history of high levels of stress may be at increased risk for perinatal depression [14,15].
Based on the criteria of the Diagnostic and Statistical Manual of Mental Disorders, fourth edition (DSM-IV) [16] and the Edinburgh Postnatal Depression Scale (EPDS) [17], mothers with symptoms of postpartum depression are defined by several major symptoms, including a depressed mood or decreased pleasure. These symptoms include impaired appetite, physical agitation or psychomotor slowing, weakness, decreased concentration, and suicidal ideation. Mothers also often feel insomnia even though the baby has fallen asleep. These symptoms must be present throughout the day and last for at least two weeks [3,9].
Women who experienced depression during pregnancy had seven times the risk of developing postpartum depression than women who did not have symptoms of antenatal depression. An observational study of 78 depressed women in the first trimester of pregnancy found that postpartum depression did not occur in all women who received treatment, both psychotherapy and pharmacotherapy, compared with 92% of women who were depressed and did not receive treatment. Supportive and psychological interventions are more effective when performed after delivery than when they are initiated during pregnancy [18].
Mothers with postpartum depression need extensive treatment with both pharmacological and non-pharmacological therapies. Through non-pharmacological therapy, such as psychological therapy, mothers can find the right way to deal with the symptoms of depression, deal with disorders that arise, or think positively when the situation is stressful [19,20].
There are several non-pharmacological techniques to relieve anxiety such as pregnancy exercise, distraction, biofed back, yoga, acupressure, aroma therapy, steam therapy and hypnosis. Hypnosis is a natural method used to relieve fear, panic, tension, and other pressures. Hypnosis is done by making direct contact with the subconscious, by giving suggestions in order to build various positive emotional conditions [21,22].
Khoirunnisa et al., [21] used a narrative review method to explore types of interventions for postpartum depression and found that several interventions such as music therapy [22], postpartum exercise [23], aerobic exercise [24], laughter therapy [25], cognitive behavior Therapy [26], Effleurage Massage Therapy [27], Acupressure Therapy [28], are effective in reducing postpartum depression.
Based on some of these studies provides an illustration that not many hypnotherapy interventions have been thoroughly scrutinized considering the impact of depression on postpartum mothers; we are therefore interested in analyzing the effectiveness of Audio Hypnotherapy in reducing postpartum depression, especially in the new normal period in 2021.
MATERIALS AND METHODS
Study design
This type of research is a quasi-experimental design using a pretest - posttest design.
Study Population
This research was conducted in January–December 2021 at the Teti Herawati Midwife clinic, Meli Rosita Palembang City and the Mariana Aceh Besar Indonesia, midwife clinic involving 60 participants who were randomly selected and had met the sample inclusion requirements such as being healthy after giving birth, having never received hypnotherapy audio, mentally healthy, and has a cell phone. Demographic characteristics of postpartum women collected in this study were age, education, occupation and parity.
Sample size
The number of samples involved was 60 participants who were randomly selected from the population. Calculating the number of samples is determined using the Slovin formula [29], where from 71 people in the population, d = 0.05, the number of samples is 60.
Instruments
The incidence of postpartum depression will be measured using a standardized questionnaire developed by Cox et al., the Edinburgh Postnatal Depression Scale (EPDS). This questionnaire consists of 10 questions; each has four responses with a Likert scale from 0 – 3. The maximum value is 30, and the lowest is 0. It is called experiencing depression if the score is ≥ 10. EPDS has a sensitivity of 80% and a specificity of 84.4 % [23]. Meanwhile, EPDS in Indonesian has a sensitivity of 86% and a specificity of 78% [24].
The scale shows how the mother felt during the previous week. In doubtful cases it may be useful to repeat the tool after 2 weeks. This scale is not used to detect mothers with anxiety neuroses, phobias or personality disorders [25].
Interventions
Audio hypnotherapy is giving positive suggestions or orders to the subconscious mind to change thoughts, feelings, and behaviors for the better through MP3 voice recordings sent via WhatsApp groups. In this study, hypnotherapy was carried out by selfhypnosis using standardized hypnotherapy audio recording media. The selfhypnosis method with standard hypnotherapy audio recording media for 30 minutes in stages; pre-induction (introduction, explaining goals, and building trust), filling in the informed consent sheet, explaining the use of tools, induction (the relaxation process brings the patient to the subconscious mind with Hanung techniques), deepening (trance), suggestion (giving messages with the aim of certain), and termination (slowly awakening the patient).
Before the intervention, all respondents filled out the EPDS questionnaire to determine the risk of postpartum depression. Then, respondents listened to Hypnotherapy audio for ± 30 minutes every night before going to bed for 2 weeks. After undergoing an audio Hypnotherapy intervention for 2 weeks, all respondents filled out the EPDS questionnaire to determine the risk of postpartum depression.
Ethical Consideration
Before the respondents filled out the questionnaire, the researchers first explained their informed consent about the scope of the research. Then after the prospective respondent agreed, the respondent signed an agreement to become a respondent. All data about respondents will be kept confidential and only used for research purposes.No economic incentives were offered or provided for participation in this study. The study protocol matched the Declaration of Helsinki ethical guidelines for clinical studies. This research has been approved by the Health Research Ethics Commission of the Health Polytechnic of the Palembang Ministry of Health with the number 1250/KEPK/Adm2/VIII/2021.
Statistical analysis
The statistical analysis was performed by SPSS software version 16. 0. Data are presented as number and percentage for categorical variables, and continuous data expressed as the mean ± standard deviation (SD) unless otherwise specified. The first statistical test, the McNemar test, aims to analyze differences in depression status before and after the intervention using categorical data. Before conducting the different tests, first, we tested the normality of the data using the Kolmogorov Smirnov and found the data was not normally distributed. The research data were analyzed using the Wilcoxon test. This test was performed on same data sample in two different periods where the data were not normally distributed. It is considered significant if the research variable has a P-value <0.05.
RESULTS
The characteristics of respondents in this study include age, education, employment status and parity. The following is the frequency distribution of the respondents' characteristics in this study:
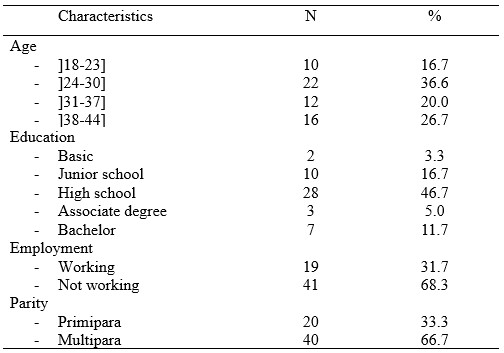
Table 1. Frequency Distribution of Respondents Characteristics
Table 1 shows that most of the mothers aged 24-30 years were 22 mothers (36.6%). The respondents' education is mostly High school as many as 28 respondents (46.7%). Most respondents did not work as many as 41 (68.3%), and multipara as many as 40 respondents (66.7%).
The results of statistical tests and the distribution of depression status before and after the intervention are presented in table 2.

Table 2. Distribution of depression incidence before and after interventions
Table 2 shows that before the intervention there were 26 depressed respondents then after the intervention there were 12 respondents. Based on the McNemar test, a p-value <0.05 was obtained, meaning that there were differences in depression status before and after the intervention.

Table 3. Normality Test Results of depression incidence pretest and posttest audio hypnotherapy
Table 3 shows that the results of the Kolmogorov Smirnov statistical test obtained a P-value <0.05, so the normality is rejected. The depression incidence data at the pre-post test audio hypnotherapy not normally distributed. Therefore, the statistical difference test was tested using Wilcoxon.
The results of the audio hypnotherapy pre-post test statistics and the mean depression incidence values are presented in table 4.
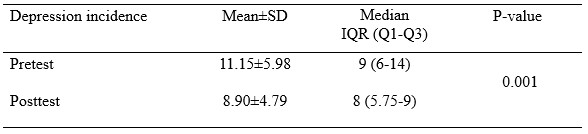
Table 4. Average Depression Incidence Pretest and Posttest Audio Hipnoterapy
Table 4 shows that depression incidence before giving audio hypnotherapy has a mean value = 11.15, while after giving audio hypnotherapy, it decreases to 8.90, with P-value <0.05.
DISCUSSION
Most pregnant women who face the birth process experience feelings of anxiety, even depression. Factors causing postpartum depression consist of biological factors, characteristics and background of the mother. Levels of the hormones estrogen (estradiol and estriol), progesterone, prolactin, cortisol which increase and decrease too quickly or too slowly are biological factors that cause postpartum depression [7]. The greater the decrease in estrogen and progesterone levels after childbirth, the greater the tendency for a woman to experience depression in the first 10 days after giving birth [8].
The estrogen and progesterone exert a suppressive effect on the activity of the monoamine oxidase enzyme. This enzyme can inactivate both noradrenaline and serotonin, which play a role in mood and depression. Estradiol and estriol are the active forms of estrogen formed by the placenta. Estradiol functions to strengthen the function of neurotransmitters by increasing the synthesis and reducing the breakdown of serotonin. Therefore, theoretically the decrease in estradiol levels due to childbirth plays a role in causing postpartum depression [9,10]. Biological causative factors are difficult and rarely measured in terms of maternal depressive symptoms [11]. Other factors that influence maternal depressive symptoms described in several studies include interpersonal variables (neural disorders, poor life experiences), social variables (marital dissatisfaction, lack of social support), and clinical variables related to pregnancy (risk in current pregnancy, problems with previous pregnancy) [12].
The results of the current study showed a decrease in the level of postpartum depression before and after listening to audio hypnotherapy. This means that listening to audio hypnotherapy can reduce the level of postpartum depression, where postpartum mothers feel comfortable, calm and relaxed after listening to audio hypnotherapy, although not every night or every day. Audio hypnotherapy is a hypnosis therapy, where respondents get positive suggestions through MP3 audio sent via cellphone. Hypnotherapy or clinical hypnosis is an integrative mind-body technique using hypnotic suggestions for specific therapeutic purposes that are identified jointly by the hypnotherapist and client [26].
The results of the Paired Samples Test analysis showed a difference in the average level of depression before and after listening to audio hypnotherapy with a significance value of P-value 0.001. For this reason, it can be concluded that audio hypnotherapy can reduce the level of depression in pregnant women, especially during the Covid-19 pandemic. The average decrease in anxiety levels of pregnant women before and after listening to audio hypnotherapy is 2.6.
Hypnotherapy has long been believed to reduce postnatal pain by giving suggestions in the form of positive commands [27]. Through the process of hypnosis, the patient is brought into a relaxed state in order to calm the autonomic nervous system and induce positive emotions that affect the patient's coping mechanisms for pain perception [28]. It stimulates positive emotions for more norepinephrine production, reduces ROS production, increases tryptophan levels, and stimulates the ventricular nucleus which functions to secrete oxytocin in the dopamine system, and subsequently plays a role in pain modulation [6,29]. A deeper hypnotic state (trance) can help activate the endorphins and encephalin system that can inhibit the production of substance P, a pain sensitizing agent in the dorsal horn of the spinal cord [30].
Some respondents experienced persistent depression despite the intervention. This condition was caused by the respondent's disobedience in carrying out audio hypnotherapy. Most of the respondents underwent audio hypnotherapy at night before going to bed. Some respondents listen when they feel uncomfortable or when they have free time. Some respondents do not run audio hypnotherapy every night.
In the future, audio hypnotherapy in order to reduce the level of depression in postpartum mothers can be an important alternative therapy besides the provision of medical drugs.
CONCLUSION
Before the intervention, there were 26 depressed respondents. Then after the intervention, there were 12 respondents. Audio hypnotherapy has been proven effective in reducing depression in postpartum mothers.
LIMITATIONS
The assessment of the level of depression in the current study is still subjective. Future research can use more real/objective measurements or combine subjective and objective scales. Furthermore, the research location only involves 3 places, therefore it cannot compare the results of similar studies in different populations.
The future research must be carried out involving several regions. This study also showed the possibility that socio-demographic factors' influence could not be controlled because the respondent's character was not matched.
FUNDING STATEMENT
This research did not receive any specific grant from funding agencies in the public, commercial, or not for profit sectors.
COMPETING INTERESTS STATEMENT
There are no competing interests for this study.
AUTHORS’ CONTRIBUTION
All authors equally contributed to preparing this article.
REFERENCES
- Field T. Prenatal depression effects on early development: a review. Infant behavior and development. 2011;34(1):1–14.
- Woods SM, Melville JL, Guo Y, Fan M-Y, Gavin A. Psychosocial stress during pregnancy. American journal of obstetrics and gynecology. 2010;202(1):61-e1.
- Melville JL, Gavin A, Guo Y, Fan M-Y, Katon WJ. Depressive disorders during pregnancy: prevalence and risk factors in a large urban sample. Obstetrics and gynecology. 2010;116(5):1064.
- Shorey S, Chee CYI, Ng ED, Chan YH, San Tam WW, Chong YS. Prevalence and incidence of postpartum depression among healthy mothers: a systematic review and meta-analysis. Journal of psychiatric research. 2018;104:235–48.
- Wang Z, Liu J, Shuai H, Cai Z, Fu X, Liu Y, et al. Mapping global prevalence of depression among postpartum women. Translational psychiatry. 2021;11(1):1–13.
- Varga K, Kekecs Z. Oxitocina y cortisol en interacción hipnótica. International Journal of Clinical and Experimental Hypnosis. 2014;62(1):111–28.
- Rizkiani I, Respati SH, Sulistyowati S, Budihastuti UR, Prasetya H. The Effect of Hypnotherapy on Serum Cortisol Levels in Post-Cesarean Patients. Journal of Maternal and Child Health. 2021;1(2549–0257):258–66.
- Yuniasti RD, Upoyo AS, Taufik A. The Effect of Hypnotherapy on Pain Intensity in Postoperative Patients: A Systematic Review. IJNP (Indonesian Journal of Nursing Practices). 2021;5(2):112–22.
- Lara MA, Navarrete L, Nieto L. Prenatal predictors of postpartum depression and postpartum depressive symptoms in Mexican mothers: a longitudinal study. Archives of women’s mental health. 2016;19(5):825–34.
- Campbell SB, Cohn JF. Prevalence and correlates of postpartum depression in first-time mothers. Journal of abnormal psychology. 1991;100(4):594.
- Mahandaru AH, Respati SH, Sulistyowati S, Laqif A, Prasetya H. The Effect of Hypnotherapy on Postpartum Pain and Depression in Women with Post Caesarean Delivery. Indonesian Journal of Medicine. 2021;6(2):194–205.
- Millizia A, Syafridah A. The Effect of Murottal Al-Quran Therapy on Pain in Post Cesarean Surgery Patients at Abby Mother and Child Hospital, Lhokseumawe City. Arkus. 2022;8(1):198–202.
- Dørheim SK, Bondevik GT, Eberhard-Gran M, Bjorvatn B. Sleep and depression in postpartum women: a population-based study. Sleep. 2009;32(7):847–55.
- Gjerdingen DK, Yawn BP. Postpartum depression screening: importance, methods, barriers, and recommendations for practice. The Journal of the American Board of Family Medicine. 2007;20(3):280–8.
- Eberhard-Gran M, Tambs K, Opjordsmoen S, Skrondal A, Eskild A. A comparison of anxiety and depressive symptomatology in postpartum and non-postpartum mothers. Social psychiatry and psychiatric epidemiology. 2003;38(10):551–6.
- Carter MJ. Diagnostic and statistical manual of mental disorders. Therapeutic recreation journal. 2014;48(3):275.
- Cox JL, Chapman G, Murray D, Jones P. Validation of the Edinburgh Postnatal Depression Scale (EPDS) in non-postnatal women. Journal of affective disorders. 1996;39(3):185–9.
- Stewart DE, Vigod S. Postpartum depression. New England Journal of Medicine. 2016;375(22):2177–86.
- Seymour-Smith M, Cruwys T, Haslam SA, Brodribb W. Loss of group memberships predicts depression in postpartum mothers. Social psychiatry and psychiatric epidemiology. 2017;52(2):201–10.
- Patel M, Bailey RK, Jabeen S, Ali S, Barker NC, Osiezagha K. Postpartum depression: a review. Journal of health care for the poor and underserved. 2012;23(2):534–42.
- Leger J, Letourneau N. New mothers and postpartum depression: a narrative review of peer support intervention studies. Health & social care in the community. 2015;23(4):337–48.
- Howell EA, Bodnar-Deren S, Balbierz A, Loudon H, Mora PA, Zlotnick C, et al. An intervention to reduce postpartum depressive symptoms: a randomized controlled trial. Archives of women’s mental health. 2014;17(1):57–63.
- Santos IS, Matijasevich A, Tavares BF, Barros AJD, Botelho IP, Lapolli C, et al. Validation of the Edinburgh Postnatal Depression Scale (EPDS) in a sample of mothers from the 2004 Pelotas Birth Cohort Study. Cadernos de saude publica. 2007;23:2577–88.
- Nasri Z, Wibowo A, Biostatistika D, Ghozali EW, Jiwa K. Faktor determinan depresi postpartum di kabupaten Lombok Timur. Pusat Penelitian dan Pengembangan Humaniora dan Manajemen Kesehatan; 2018.
- Levis B, Negeri Z, Sun Y, Benedetti A, Thombs BD. Accuracy of the Edinburgh Postnatal Depression Scale (EPDS) for screening to detect major depression among pregnant and postpartum women: systematic review and meta-analysis of individual participant data. bmj. 2020;371.
- Mubarokah RI, Prasetya H, Respati SH. The Effectiveness of Hypnotherapy to Reduce Anxiety in Pre-Caesarean Section Women. Journal of Maternal and Child Health. 2020;5(1):12–8.
- Kendrick C, Sliwinski J, Yu Y, Johnson A, Fisher W, Kekecs Z, et al. Hypnosis for acute procedural pain: a critical review. International Journal of Clinical and Experimental Hypnosis. 2016;64(1):75–115.
- Alarcon R. Synopsis of psychiatry: Behavioral sciences and clinical psychiatry. American Journal of Psychiatry. 1992;149(7):972–4.
- Sanders VM. The beta2-adrenergic receptor on T and B lymphocytes: do we understand it yet? Brain, behavior, and immunity. 2012;26(2):195–200.
- Price, Wilson A. Patofisiologi: Konsep Klinis Proses-proses Penyakit (Pathophysiology Clinical Concepts of Disease Processes), Buku I. Penerbit Buku Kedokteran EGC; 1995.
![]() This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
THE EFFECT OF PARENTAL HOLDING ON PAIN LEVELS INFANT DURING MEASLES IMMUNIZATION: QUASI-EXPERIMENTAL STUDY
Nesi Novita1*, Ratnaningsih Dewi Astuti2, Yeni Elviani3, Emi Latifah Sukasna4
1,4Department of Midwifery, Health Polytechnic of Palembang, Indonesia
2Department of Pharmacy, Health Polytechnic of Palembang, Indonesia
3Department of Nursing, Health Polytechnic of Palembang, Indonesia
* Corresponding author: Nesi Novita: Jl. InspekturYazid, Sekip Jaya, Kec. Kemuning, Kota Palembang, Sumatera Selatan 30114, Department of Midwifery, Health Polytechnic of Palembang, Indonesia, Orcid : https://orcid.org/0000-0002-1572-5448, Email: nesinovita51@gmail.com
Cite this article
ABSTRACT
Background: Immunization is the most effective and efficient public health effort in preventing various dangerous diseases, one of which is measles immunization. In practice, it is very closely related to needles that can cause anxiety, pain, avoidance, and even suffering in children when visiting health services to get vaccines. Parental care is a form of non-pharmacological intervention to treat pain. The purpose of this study was to determine the effect of parental maintenance on infant pain levels during measles immunization.
Methods: Quasi-experimental research method with pretest posttest control group design. The number of samples was 42 respondents who were divided into an intervention group and a control group in the working area of the Taman Bacaan Health Center Jambi city, Indonesia. This research was carried out in May-July 2021. The instrument used is the Face, Legs, Activity, Cry and Consolability (FLACC) scale and parental holding Standard Operating Procedures (SOP). Research statistical test with paired t test and independen t test.
Results: The results obtained p-value < 0.0001 with the level of pain in infants during measles immunization in the intervention group with an average of 5.52 and a standard deviation of 0.928, while the level of pain in infants during measles immunization in the control group with an average of 8.24 and standard deviation 1.044.
Conclusion: The parental grip in the position of holding the baby facing the chest with the parents affects the baby's level of pain during measles immunization. It is hoped that parental holding can be used as an alternative during immunization so that babies are more comfortable and can reduce pain.
Keywords: Parental Holding, Pain Management, Complementary Therapy, Measles Immunization
INTRODUCTION
Immunization is a public health effort that is most effective and efficient in preventing various dangerous diseases [1,2]. The magnitude of the role of immunization has been recorded in history to save the world community from illness and even death from diseases such as smallpox, polio, tuberculosis, hepatitis B, diphtheria, including measles [3–5]. Immunization is an effort to actively generate or increase a person's immunity to disease and if exposed to the disease, he or she will not get sick or experience mild illness [6].
Immunization is a critical agenda in children’s health. The World Health Organization (WHO) has set a goal that all countries should reach 90% coverage of all vaccines by 2020. The coverage rate considerably varies among countries. Today there are still 19.4 million unvaccinated children globally. Among those children, 60% come from 10 countries, and Indonesia is on that list [7,8].
In the Indonesian Health profile, the number of diseases that can be prevented by immunization for tetanus neonatorum increased in 2019, accompanied by suspected measles which also increased from 8,429 cases in the previous year, to 8,819 suspected cases of measles. Complete basic immunization coverage for infants from the 2019 target is expected to be 95% where in 2017 it reached 80% but in 2018 it decreased to 68.75% in districts/cities [7].
Immunization, which is mostly given in the form of injections, will create new problems. Pain and trauma due to immunization injections are effects that need attention in addition to other unexpected side effects. These side effects can be one of the causes of the lack of immunization coverage [8,9]. Parents assume that repeated immunizations can make children feel pain, which in turn contributes greatly to refusal, non-adherence to schedules, and delays in immunization [10]. Anxiety and pain due to injection are complaints that are often conveyed by both parents and children due to immunization. This condition makes parents reluctant to come to health services afterwards [8,11]. More than 90% of children experience severe stress during immunization which results in parents not complying with the existing schedule. The results of studies in America show that 24% of parents and 63% of children are afraid of needles when immunizations affect 7-8% of children with incomplete immunization status [8]. Needle phobia is estimated to reach 10-20% of the population [11].
One type of non-pharmacological intervention that has been developed to treat this pain is parental holding with hug therapy. Parental holding involves close contact between parent and baby, with the baby in the parent's arms, facing each other and parallel, and there is eye contact between the two. Parental grip may reduce the response to procedures that are painful for the baby, such as exercise [9]. Parents can get the attention and attention of their babies, this is in line with the recommendations from WHO to give special attention to babies during technique. According to Sari [9] hugs from parents to their children will help the pituitary gland secrete endorphins which function to improve the immune system, improve the ability to reduce pain, besides that the baby will avoid fear, anxiety and stress. In addition, the comfortable feeling that arises due to the mother's embrace is able to make the baby's body to secrete endorphins. Endorphins can improve mood, reduce anxiety, causing muscles to relax, and calm. So that the level of pain experienced by the baby will decrease [10,11].
According to Modanloo et al. [12] vaccination for early childhood is one of the most important public health interventions therefore clinical practice guidelines recommend the use of pain management strategies for infants during vaccination. Immunization is closely related to needles that can cause anxiety, avoidance, and even distress in children during visits to health services to get vaccines [13]. Medical procedures performed using needles such as immunizations are a source of pain for children. In addition, children will also feel anxiety and fear that become trauma which will continue into adulthood [14].
Pain is a protective mechanism that alerts the body that there will be tissue damage in the body that can affect survival [15]. This procedure is a painful procedure for children especially when immunized without adopting pain management [16]. Young children have difficulty understanding pain and procedures performed by health workers. Toddlers have difficulty interpreting the pain experienced, usually the toddler responds to pain with crying or facial expressions and simple words for toddlers who are able to speak [17].
Wahyuni & Suryani [18] resulted in an average pain scale before being given parental holding was 7.8 with a standard deviation of 1.4 and a minimum - maximum value range 5.0-10.0, and the average pain scale after parental holding was given was 3.6 with a standard deviation of 1.6 and a minimum-maximum value range of 1.0-7.0. With the result that 12 respondents who received parental holding intervention experienced a decrease in pain scale by a difference of 4, and the results of the sample t test were obtained p <0.05, meaning that there is a difference in pain scale before and before being given parental holding.
Research Sri Rahyanti et al [19] in Jakarta using a randomized clinical trial method and involving 34 respondents aged 1 to 4 years who were included in the intervention group and the control group, it was found that parental holding and upright position results in significant differences in pain scores in children were compared with the group that was not given parental holding and upright position with a p-value < 0.0001.
The results of the preliminary study at the time of giving technique midwives will perform a distraction technique (guided imagery) on the baby by saying there is something interesting on the other side, hidden the syringe used and giving breast milk after the exercise.
The problem in this study was pain management in infants during immunization is still not optimal and has an impact on ongoing trauma into adulthood. Is there any effect of parental holding on the baby's pain level during measles immunization?
The purpose of the study was to carry out parental holding it would affect the level of infant assistance during measles in the work area of the Taman Bacaan Health Center Palembang. The benefits are in order to provide comfort for babies during immunization and to make standard operating procedures (SOPs) with parental holding techniques that can be applied by health workers.
METHODS
Study design
This study used quantitative research methods with a quasi-experimental design and a pre-test post-test control group design.
Study Population
The population and sample are all infants under the age of 1 year given measles immunization in the working area of Taman Bacaan Health Center conducted on May-July 2021.
Inclusion criteria consisted of infants aged 9-12 months, The baby's parents agree that their child is a respondent, and the baby's parents agree to provide parental holding. And the exclusion criteria include babies who are not directly accompanied by their parents, babies who are not directly accompanied by their parents crying and not being soothed before the injection, sick or contraindication of immunization, and parents who refuse to be respondents.
Sample size
The numbers of samples involved were 42 participants who were chosen randomly or randomly from the population. The sample was divided into an intervention group of 21 respondents in (given parental holding by hugging) and 21 respondents in the control group (held and on the lap by his mother). Calculation of the number of samples was determined using the Slovin formula [20], where from a population of 47 people, d = 0.05, the total sample was 42 people. The research population, also known as the target population in this study, was the number of toddlers aged <1 year who visited the Taman Bacaan Health Center in Jambi City, Indonesia, conducted on May-July 2021, totaling 47 people.
Instruments
The independent variable is parental holding, and the dependent variable is the level of pain in infants during measles immunization. Pain variables were measured using the FLACC Pain Assessment Tools instrument. The FLACC Behavioral Pain Scale is a pain assessment tool for children less than three years of age or with cognitive impairment. FLACC is an acronym for Face, Legs, Activity, Cray, and Consolability (face, legs, activity, crying, and controllability). The five components are totaled, and the severity of pain is determined from a score of 0-10.
The assessment consisted of facial expressions (0-2), leg movements (0-2), activity (0-2), crying (0-2), ability to be entertained (0-2). The results of the behavioral scores are: 0: No Pain, 1-3: mild pain/mild discomfort, 4-6: moderate pain and 7-10: severe pain/severe discomfort. Measurement of the pain level variable was carried out before the intervention (pre-test) and 15 minutes after the intervention (post-test).
The type of intervention in this study was parental holding by hugging (Intervention group), and held and on the lap by the mother (control group). Both of these interventions were only carried out once when the child was given measles immunization.
Ethical Consideration
Prior to the implementation of measles immunization, the researcher first asked the mother's willingness to provide informed consent. After the consent became the research sample, the baby's mother signed the informed consent. No economic incentives were offered or provided for participation in this study. The study protocol matched the Declaration of Helsinki ethical guidelines for clinical studies. This research has been approved by the Health Research Ethics Commission of the Health Polytechnic of the Jambi Ministry of Health with the number LB.02.06/2/51/2021.
Statistical analysis
Data are presented as numbers and percentages for categorical variables. Continuous data were expressed as mean ± standard deviation (SD) or median with Interquartile Range (IQR). To see the distribution of research data, the Kolmogorov Smirnov test was used. The research data is normally distributed. Then proceed with bivariate analysis using the Paired t test. The Paired t test was used to determine the effect of Parental holding on infant pain level during measles immunization. Then to analyze the differences between the intervention and control groups, using the Independent t test. All tests with p-value <0.05 were considered significant. Statistical analysis was performed using the SPSS version 16.0 application.
RESULTS
The research respondents were 42 respondents, which were divided into 21 respondents in the intervention group and 21 respondents in the control group. The general description of the frequency distribution by gender and age can be seen in the following table:
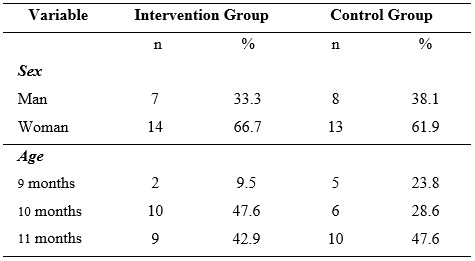
Table 1. Frequency distribution of general characteristics of the sample
Based on table 1, it is known that in the intervention group most of them were female, namely 66.7%, and in the control group most were female, namely 61.9%. While the age variable in the intervention group was mostly 10 months old, namely 47.6%, and in the control group most were 11 months old, namely 47.6%.
To find out the distribution of research data, a normality test of the data was carried out, presented in table 2.

Table 2. Data normality test
Based on table 2, the research data obtained were normally distributed with p-value > 0.05.
Bivariate analysis aims to explain or describe the dependent variable, namely the level of infant pain during measles immunization in the intervention group and the control group.
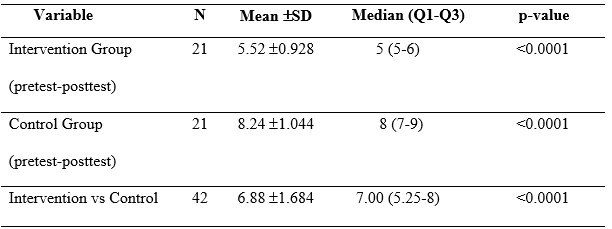
Table 3. Analysis of the effect of parental holding on infant pain levels
Based on table 3, it is known that the results of paired t test have the effect of parental holding on the baby's pain level during measles immunization with a p-value < 0.0001 . The mean value of the two groups (intervention and control) is 6.88. The result of independent t test is a p-value <0.05, it means that there is a difference in the effect of the two interventions on the pain level of infant during measles immunization.
DISCUSSION
The purpose of the study was to carry out parental holding it would affect the level of infant assistance during measles in the work area of the Taman Bacaan Health Center Palembang. In this study, the age of the respondents was between 9-11 months; based on Minister of Health regulations no. 42 of 2013 the first measles immunization was given to infants aged 9 months. Measles immunization is given in 2 doses, namely when the baby is 9 months old (as basic immunization), and when the baby is 9 months old (as basic immunization). when the child is 2 years old (as a follow-up immunization) [21]. According to Perry et al. [17] young children have difficulty understanding pain and procedures performed by health workers. Toddlers have difficulty interpreting the pain experienced, usually the toddler responds to pain with crying or facial expressions and simple words for toddlers who are able to speak. Babies have not been able to express pain with words; therefore the level of pain in infants is measured using the FLACC scale which is seen through the baby's responses in the form of behaviour, facial expressions, crying, and movements.
In this study, the observed of level pain was in infants aged 9-12 months, babies could not show the pain response, it was necessary to have skills of health workers to assess the baby’s pain level based on the FLACC scale, besides that most mothers said they were afraid to accompany the baby directly during immunization. In this study, it was stated that there was a significant decrease in the infant's pain level during measles immunization with a p-value < 0.0001 and the minimum and maximum pain values obtained from the control group (who were not given parental holding) of 7.00 and 10.00. to the minimum - maximum values in the intervention group (given parental holding) of 4.00 and 7.00.
This study is in line with research Modanloo et al. [12] which states that pain management strategies during vaccination can be carried out by holding. While in this study, parental holding is done by hugging or hugging. According to Sari [9] hugs from parents to their children will help the pituitary gland secrete endorphins which function to increase the immune system, increase the ability to reduce feelings of anxiety. In addition, the baby will avoid fear, anxiety and stress. Increased endorphins can affect mood, reduce anxiety, cause muscles to relax, and calm down, therefore, the level of pain experienced by the baby will decrease. Endorphins are natural substances produced by the body whose job is to inhibit the passage of pain sensations from the traumatized body part to the brain. Everyone's endorphin levels are different, this causes different responses to the same type of pain [22]. Besides being useful for inhibiting pain, endorphins also have other benefits, namely to regulate hormone production, reduce persistent aches and pains, and control stress [23,24]. In line with research Qiu et al. [25] which states that endorphins are endogenous opioids that are released in response to pain and increase pain inhibition when an organism is exposed to stress or painful stimuli (acute pain). In this study, painful stimuli in the form of measles immunization injections can affect the release of endorphins.
This study is in line with research Dewi et al. [26] which states that babies who given parental holding will feel a sense of love and comfort from their parents, so that the fear and anxiety they experience will be reduced because of their parents holding them. Parental hugs provide a sense of comfort and reduce pain levels in children.
In this study, the difference in the level of infant pain in the intervention group and the control group can be seen from the pain response felt by the baby, as evidenced by changes in facial expressions, grimacing, body squirming, crying, body rigidity, restlessness, to an increase in stress hormones. Parental holding involves close contact between parents and babies, with the baby in the parent's arms, facing each other and parallel, and there is eye contact between the two. Parental holding may reduce the response to procedures that are painful for the baby, such as immunizations. Parents can distract and calm their babies, this is in line with the recommendations from WHO to pay special attention to babies during immunization. When babies are immunized using injections, parental holding by hugging other forms of touch that can minimize pain, make babies feel more comfortable and good, so that it has an impact on the baby's quality of life by getting a direct touch of love from the parents [18].
Parental holding comfort to the baby and mother at the time of immunization with the injection technique, so that immunization does not have an impact on causing trauma to babies until they are adults for fear of being injected. In addition, it can be used as an alternative effort for health workers when giving immunizations to minimize level pain in infants.
Researchers would like to convey that these two interventions have been proven to reduce immunization pain in children. although in the independent t test the two interventions had differences in reducing the pain scale in immunized children. This means that the way the mother holds or hugs the child during immunization has a calming effect on the child.
The strength of this study compared to previous studies lies in the comparison of the effects of 2 different interventions on the pain scale during measles immunization in children which was not carried out in the previous study, which only used 1 intervention in the form of parental holding.
CONCLUSION
Parental holding has an effect on reducing pain in infants when given measles immunization by providing a sense of comfort, and reducing distress in infants. So that health workers can use this method as an alternative in reducing pain levels in infants when immunized. Parental holding can be used as a basis in formulating policies or standard operating procedures (SOPs) for the management of measles immunization, namely the provision of parental holding as one of the procedures in reducing pain levels in infants during immunization. With this policy, it is hoped that health workers will apply techniques to reduce pain in infants when immunized against measles.
LIMITATION OF STUDY
One of the limitations of this study is the very small sample size (a pilot study). The research location only involves one region, therefore it cannot compare the results of similar studies in different populations. In addition to these two things, the environmental conditions where the vaccination is carried out must be designed not to have little effect on the research results. Likewise, the clothing of health workers must be adapted because usually, children are treated at hospitals or trauma clinics in white clothes.
FUNDING STATEMENT
This research did not receive any specific grant from funding agencies in the public, commercial, or not for profit sectors.
CONFLICT OF INTEREST
The authors report no conflict of interest.
ACKNOWLEDGEMENT
We would like to thank the director of the Department of Midwifery and Pharmacy, Palembang Health Polytechnic for supporting this research
AUTHORS’ CONTRIBUTION
All authors equally contributed to preparing this article.
REFERENCES
1. Whitney CG, Zhou F, Singleton J, Schuchat A. Benefits from immunization during the vaccines for children program era—United States, 1994–2013. Morbidity and Mortality Weekly Report. 2014;63(16):352.
2. Doherty M, Buchy P, Standaert B, Giaquinto C, Prado-Cohrs D. Vaccine impact: Benefits for human health. Vaccine. 2016;34(52):6707–14.
3. Greenwood B. The contribution of vaccination to global health: past, present and future. Philosophical Transactions of the Royal Society B: Biological Sciences. 2014;369(1645):20130433.
4. Miller MA, Sentz JT. Vaccine-preventable diseases. 2011;
5. Ehreth J. The value of vaccination: a global perspective. Vaccine. 2003;21(27–30):4105–17.
6. Kemenkes R. Buku Ajar Imunisasi. Pusat Pendidikan dan Pelatihan Tenaga Kesehatan. 2014.
7. UNICEF WHO. Progress and challenges with achieving universal immunization coverage: 2019 estimates of National immunization coverage [Internet]. Februari 10, 2020. Geneva, Switzerland: WHO; 2019. Available from: https://www.who.int/%0Aimmunization/monitoring_surveillance/who-immuniz.pdf.
8. Hardhantyo M, Chuang Y-C. Urban-rural differences in factors associated with incomplete basic immunization among children in Indonesia: A nationwide multilevel study. Pediatrics & Neonatology. 2021;62(1):80–9.
9. Indah. Pengaruh parental holding terhadap distress anak selama prosedur insertion intravena (IV) di ruang rawat inap anak RSUD Adnan WD Payakumbuh tahun 2019. stikes perintis padang; 2019.
10. Nurlaila N, Baniyah N, Iswati N. Terapi Dekapan dapat Menurunkan Kecemasan Anak saat Pemberian Terapi Intravena. Jurnal Berita Ilmu Keperawatan. 2022;15(1):27–33.
11. Utario Y, Rustina Y, Efendi D. Family Centered Care Intervention Effectively Reduces Parental Anxiety in Perinatology Ward. Dunia Keperawatan: Jurnal Keperawatan dan Kesehatan. 2021;9(1):143–51.
12. Modanloo S, Stacey D, Dunn S, Choueiry J, Harrison D. Parent resources for early childhood vaccination: An online environmental scan. Vaccine. 2019;37(51).
13. Harrington JW, Logan S, Harwell C, Gardner J, Swingle J, McGuire E, et al. Effective analgesia using physical interventions for infant immunizations. Pediatrics. 2012;129(5).
14. Canbulat Şahiner N, Inal S, Sevim Akbay A. The Effect of Combined Stimulation of External Cold and Vibration During Immunization on Pain and Anxiety Levels in Children. Journal of Perianesthesia Nursing. 2015;30(3).
15. Sherwood. Fisiologi Manusia: Dari Sel Ke Sistem. 8th ed. Jakarta: Jakarta. EGC; 2012.
16. Özdemir FK, Tüfekci FG. The effect of using musical mobiles on reducing pain in infants during vaccination. Journal of Research in Medical Sciences. 2012;17(7).
17. Perry AG, Potter PA, Ostendorf WR. Clinical Nursing Skills & Techniques. Elsevier. 2014.
18. Wahyuni F, Suryani U. Efektifitas Terapi Mendekap Dan Terapi Musik Dalam Menurunkan Skala Nyeri Pada Bayi Saat Dilakukan Imunisasi Campak. Jurnal Ilmiah Keperawatan Sai Betik. 2021;16(1):13–23.
19. Sri Rahyanti NM, Nurhaeni N, Wanda D. Could a Certain Sitting Position Reduce the Pain Experienced by a Child? The Benefits of Parental Holding and an Upright Position. Comprehensive Child and Adolescent Nursing. 2017;40.
20. Sugiyono D. Metode penelitian pendidikan pendekatan kuantitatif, kualitatif dan R&D. Alfabeta; 2013.
21. Kemenkes R. Peraturan Menteri Kesehatan Republik Indonesia No. 42 Tahun 2013. 2013.
22. Mawaddah E, Rusmini R, Ningsih MU, Mardiatun M. Penerapan Konsep Atraumatic Care Saat Pemasangan Infus dan Venipunktur pada Anak. Jurnal Keperawatan Terpadu (Integrated Nursing Journal). 2021;3(1):17–27.
23. Khasanah NN, Astuti IT. Teknik Distraksi Guided Imagery sebagai Alternatif Manajemen Nyeri pada Anak saat Pemasangan Infus. Jurnal Kesehatan. 2017;8(3):326–30.
24. Hafizzanovian H, Oktariana D, Apriansyah MA, Yuniza Y. peluang terjadinya immunization stress-related response (isrr) selama program vaksinasi covid-19. Jurnal Kedokteran dan Kesehatan: Publikasi Ilmiah Fakultas Kedokteran Universitas Sriwijaya. 2021;8(3):211–22.
25. Qiu J, Jiang Y fei, Li F, Tong Q hong, Rong H, Cheng R. Effect of combined music and touch intervention on pain response and β-endorphin and cortisol concentrations in late preterm infants. BMC Pediatrics. 2017;17(1).
26. Dewi TS, Mardiah W, Rukmasari EA. Respon dan Pengelolaan Nyeri Pada Bayi Saat Imunisasi Pentabio di Wilayah Kerja Puskesmas Haurpanggung. In: Proceeding Seminar Nasional Keperawatan. 2020. p. 116–21.
![]() This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
THE EFFECT OF VIRTUAL EDUCATION ON THE KNOWLEDGE OF POSTPARTUM MOTHERS ABOUT BREASTFEEDING DURING THE COVID-19 PANDEMIC: QUASI-EXPERIMENTAL DESIGN
Imelda, Atika Fadhilah Danaz Nasution*, Ika Murtiarini, Rosmaria, Diniaty
Department of Midwifery, Health Polytechnic of Jambi, Indonesia
Corresponding author: Atika Fadhilah Danaz Nasution, Jl. Prof DR GA Siwabessy No.42, Buluran Kenali, Kec. Telanaipura, Kota Jambi, Jambi 36122, Indonesia.
Orcid: https://orcid.org/0000-0002-4181-8621; Email: atikapoltekkes@gmail.com

Cite this article
Abstract
Introduction: Postpartum mothers and newborns are a group that is vulnerable to COVID-19. Due to the COVID-19 pandemic, access to essential services such as breastfeeding counseling in hospitals, health clinics, and home visits has been disrupted. Postpartum mothers will immediately breastfeed. Therefore there is a need for knowledge, appropriate information, and support to provide breast milk, especially during the COVID-19 pandemic. This study aims to analyze the effect of virtual counseling on the knowledge of postpartum mothers during the COVID-19 pandemic at the Delima Midwife Clinic in Jambi City.
Materials and Methods: The current study utilized a quasi-experimental design with one group design pretest-posttest approach. This research was conducted in January-October 2021 and involved 75 postpartum mothers. This study using the zoom app. and questionnaire. Data analysis using Wilcoxon statistical test.
Results: The results showed an increase in knowledge where before being given virtual education, most of the respondents' knowledge was in the Poor category, as much as 80% (mean 6.18). After the intervention, the knowledge of most respondents in the Good category was 46.7% (mean 12.15) with P-value <0.05.
Conclusion: The study concludes that virtual counseling significantly affects the knowledge of postpartum mothers about breastfeeding during the COVID-19 pandemic.
Keywords: Postpartum Mothers, Breastfeeding, COVID-19 pandemic, Counseling, Virtual.
INTRODUCTION
Coronavirus Disease 2019 (COVID-19) is an infectious disease caused by Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2). SARS-CoV-2 is a new type of coronavirus that has never been previously identified in humans [1,2]. There are at least two types of coronaviruses known to cause diseases that can cause severe symptoms, such as Middle East Respiratory Syndrome (MERS) and Severe Acute Respiratory Syndrome (SARS) [3]. The average incubation period is 5-6 days, with the most prolonged incubation period being 14 days. In severe cases of COVID-19, it can cause pneumonia, acute respiratory syndrome, kidney failure, and even death [4,5].
The spread of COVID-19 has reached almost all provinces in Indonesia, with the number of cases and deaths increasing. This condition impacts the political, economic, social, cultural, defense and security aspects, as well as the welfare of the people in Indonesia [6]. Indonesia reported its first case of COVID-19 on March 2, 2020, and the number continues to grow until now. The data on confirmed cases of COVID-19 in Indonesia as of October 21, 2021, were 4.237.834 people, 143.120 people died, and patients who had recovered were 4.079.120 people [7]. Meanwhile, in Jambi Province, COVID-19 cases increased sharply. As of October 3, 2021, the Jambi Provincial Government recorded 29.616 positive confirmed cases of COVID-19, 768 people died, and 28.476 people recovered [8].
Postpartum mothers and newborns are a group that is vulnerable to the COVID-19 virus [9,10]. During the COVID-19 pandemic, access to essential services such as breastfeeding counseling in hospitals, health clinics, and home visits has been disrupted [11,12]. The amount of inaccurate information and news circulating about the safety of breastfeeding has reduced the number of breastfeeding mothers because mothers are afraid of transmitting diseases to their babies even though this is the most appropriate moment to provide the best intake for babies through breastfeeding. After all, breast milk contains immune substances which protect children from infections and chronic diseases and reduces the chances of suffering from health problems later in life. The Covid-19 virus has never been found in breast milk [13,14].
Social restrictions during the COVID-19 pandemic require staying at home so that continuous care cannot be carried out, both health workers to make visits and mothers and babies to check their health status at the nearest health service. The impact of this situation can cause stress and worry for postpartum mothers who are still adapting to breastfeeding activities. Breastfeeding mothers need to continue to get support in the form of assistance to overcome problems during the breastfeeding process [2,15].
The current state of the COVID-19 pandemic has made it difficult for postpartum mothers to get information and consult face-to-face due to the strict rules of physical distancing. This condition resulted in a decrease in the number of visits by postpartum mothers to health workers. The limitations of accessing information on exclusive breastfeeding from health workers can be overcome by providing health promotions delivered via Telemedia, where postpartum mothers can communicate virtually and see some presentation materials and videos of good and correct breastfeeding techniques [16,17].
Health promotion through Telemedia/online is expected to increase the knowledge of postpartum mothers about exclusive breastfeeding and sound and correct breastfeeding techniques. This online learning for postpartum mothers is expected to help postpartum mothers to obtain information and consult during the COVID-19 pandemic.
This study aims to examine the effect of Virtual Counseling on Postpartum Mother's Knowledge of Breastfeeding during the Covid-19 Pandemic at the Delima Midwife Clinic in Jambi City.
Method
Trial design
The current study utilized quasi-experimental design with one group design pretest-posttest approach.
Participants
This research was conducted in January-October 2021 and involved 75 postpartum mothers who were randomly selected and met the sample inclusion requirements, such as breastfeeding mothers, mothers who have never participated in counseling activities about breastfeeding, and who have the Zoom app.
Intervention
The research variable is the knowledge of postpartum mothers. Before the intervention was given, the researcher first measured the level of knowledge of postpartum mothers (pre-test). After being given the intervention, the researcher again measured the level of knowledge of postpartum mothers (post-test). In this study, the intervention model provided was virtual education about breastfeeding, which was carried out once for 1 hour, i.e., 45 minutes of material delivery and 15 minutes of discussion). In this study, researchers explain the principles of breastfeeding, including the correct way of breastfeeding. The researcher presented the material with a poster or picture of the correct breastfeeding technique.
The knowledge questionnaire consists of 33 questions with correct and incorrect answer choices. If the postpartum mother answered correctly, she was given a score of 1; if the answer was wrong, she was given a score of 0. The range of scores obtained was between 0-33. The questionnaire used the Guttman scale. The contents of the postpartum mother's knowledge questionnaire included the benefits of breastfeeding, breastfeeding techniques, breastfeeding positions, correct breastfeeding steps, duration and frequency of breastfeeding, milk release, milk storage, breast care, nutrition during breastfeeding, and problems in breastfeeding.
The Guttman scale has an important feature where it is a cumulative scale and only measures one dimension of a multidimensional variable; therefore, this scale is dimensionless. The data obtained are interval data or dichotomous ratios (two alternatives) [18].
Researchers did not try out the knowledge questionnaire because this questionnaire was adopted from Nalsalisa's study [19]. The results of the validity test obtained a p-value <0.05 on 33 questions. For the reliability test, this questionnaire is reliable because the value of r count> r table is reliable.
The researcher has worked as a lecturer and researcher for 10-15 years and has Master and Doctoral degrees. The researcher has done much research in the health sector and has compiled many questionnaires, so the researcher prepared a questionnaire for this study. Before the research was conducted, the questionnaire was tested on ten postpartum mothers, and the results indicated that two questions had to be replaced because they were invalid.
Outcomes
This study has produced a description of the knowledge of postpartum mothers before and after virtual educational interventions and the effect of virtual education interventions on postpartum mothers' knowledge.
Sample size
75 postpartum mothers who have been calculated using the Slovin formula at a precision (d) = 0.1, the total population is 307 people. The study population, also known as the target population in this study, is the number of postpartum mothers who visited the Delima Midwife Clinic, Jambi City, Indonesia, in 2020, totaling 307 people.
Ethical Consideration
No economic incentives were offered or provided for participation in this study. In this study, because the subject was still a minor so the researcher had asked for and obtained parental consent so that their child could participate in the study. The study was performed in accordance with the ethical considerations of the Helsinki Declaration. This study obtained ethical feasibility under the Health Research Ethics Commission of the Ministry of Health, Jambi, and registration number: LB.02.06/2/161/2021.
Statistical analysis
Data are presented as numbers and percentages for categorical variables. Continuous data were expressed as mean ± standard deviation (SD) or median with Interquartile Range (IQR). To see the distribution of research data, the Kolmogorov Smirnov test was used. Then proceed with bivariate analysis using the Wilcoxon test. All tests with p-value (p)<0.05 were considered significant. Statistical analysis was performed using the SPSS version 16.0 application.
RESULTS
The characteristics of respondents in this study include age, education, employment status and parity. The following is the frequency distribution of the respondents' characteristics in this study:

Table 1. Frequency Distribution of Respondents Characteristics
The majority of respondents are in the age range of 32-38, have high school education, do not work and have multiparous status.

Table 2. Distribution of knowledge before and after interventions
Most of the respondents' knowledge before the intervention was in the Poor category, as much as 80%. After the intervention, the knowledge of postpartum mothers was mainly in the Good category, as much as 46.7%.
Table 3 shows that the Kolmogorov Smirnov statistical test results obtained a significant value of knowledge at the pretest and posttest virtual education, each less than 0.05.

Table 3. Normality Test Results of Knowledge pretest and posttest virtual education
The knowledge data at the pretest and posttest virtual education not normally distributed. Therefore, the statistical difference test was tested using Wilcoxon (Table 4)

Table 4. Average Knowledge Pretest and Posttest Virtual Education
Table 4 shows that knowledge before giving virtual education has a mean value = 6.18, while after giving virtual education, it increases to 12.15, with P-value <0.05.
DISCUSSION
Postpartum conditions cause a partial decrease in immunity due to physiological changes during pregnancy, making postpartum women more susceptible to viral infections. Therefore, the COVID-19 pandemic will likely cause severe consequences for postpartum mothers. Social distancing measures are effective in reducing disease transmission. It also applies to postpartum mothers to limit themselves to not being exposed to the outside environment, let alone traveling to pandemic areas [20,21]. The risk of postpartum mothers being infected with COVID-19 is one of them when visiting a postnatal check-up at a midwifery clinic or hospital, so mothers must increase their vigilance by continuing to be disciplined in the use of PPE [21,22]. Postpartum mothers can limit visits to obstetric clinics or hospitals by conducting online consultations, actively self-checking for signs and dangers during pregnancy, and only making visits when things are worrying. This study aims to analyze the effect of virtual education on postpartum mothers' knowledge about breastfeeding [13,23]. Based on the univariate analysis, it is known that most of the respondents have less knowledge (80%), and a small portion (5.7%) have good knowledge. Health promotion cannot be separated from activities or efforts to convey health messages to communities, groups, or individuals.
There are still many mothers who say that mothers who are confirmed positive for COVID-19 cannot breastfeed their babies directly. The world Health organization still recommends that mothers continue breastfeeding their babies but must follow hygiene procedures. SARS-CoV-2 has not been detected in mothers with suspected or confirmed COVID-19, and there is no evidence that the virus is transmitted through breast milk [22,24].
Postpartum mothers who have good knowledge increased to 42% after counseling. The mean value of knowledge before counseling was done was 6.18, then after virtual counseling, there was an increase in the mean value of postpartum mothers' knowledge about breastfeeding to 12.15.
There is an increase in knowledge of breastfeeding mothers about breastfeeding during the COVID-19 pandemic. It is hoped that changes in behavior will occur, such as giving exclusive breastfeeding to their babies because concerns about transmission of COVID-19 through breast milk have been answered, namely that it is not proven to transmit COVID-19, and breastfeeding mothers can also provide breast milk exclusively with due observance of health protocols. Thus, even though the baby is in a pandemic, the baby's needs are still met with the mother giving exclusive breastfeeding even though the mother is still working and can still provide exclusive breastfeeding [25].
The statistical test results obtained a P value < 0.05, so it can be concluded that virtual counseling affects postpartum mothers' knowledge about breastfeeding during the COVID-19 pandemic. Silalahi's research (2012) reported differences in the level of knowledge of postpartum mothers after being given counseling. There was an effect of counseling on exclusive breastfeeding on mothers' knowledge about exclusive breastfeeding.
This finding strengthens the previous finding that reported that knowledge for the intervention group obtained a mean value of 58.89. In contrast, the control group obtained a mean value of 45.47, with P-value = 0.012, meaning that counseling affects the knowledge of postpartum mothers in the Timbusseng Village Work Area, Pattallassang District, Kab. Gowa [26].
Extension activities can be carried out with two-way communication where the communicator (extension) provides the communicant opportunity to provide feedback on the material. This interactive discussion on two-way communication is expected to trigger the desired behavior change. This health education's success is determined by the material presented and the interpersonal relationships between communicators and communicants [16,27]. An indicator of the success of extension that can be measured quickly is the similarity of meaning or understanding of what is conveyed by the communicator and accepted by the communicant [24,28].
Virtual counseling media is an alternative for health workers to consult postpartum mothers during the COVID-19 pandemic to reduce the risk of spreading COVID-19 disease, which can endanger pregnant women and neonates. The Good knowledge of the mother determines the correct breastfeeding technique. Good knowledge about the importance of breastfeeding and ways to breastfeed will form a positive attitude, and then correct breastfeeding behavior will occur [24,29].
CONCLUSION
Virtual counseling has a significant effect on the knowledge of postpartum mothers about breastfeeding during the COVID-19 pandemic.
STUDY LIMITATIONS
There are limitations to the number of research samples, and samples only come from one location; therefore, the results of this study cannot be differentiated from samples or participants with different characters in other locations. Future research must involve many samples, and research locations must also be heterogeneous.
FUNDING STATEMENT
This research did not receive any specific grant from funding agencies in the public, commercial, or not for profit sectors.
CONFLICT OF INTEREST
The authors report no conflict of interest.
AUTHORS’ CONTRIBUTION
All authors equally contributed to preparing this article.
ACKNOWLEDGEMENT
We would like to thank the director of the Department of Midwifery, Health Polytechnic of Jambi, Indonesia for supporting this research.
REFERENCES
1. Palmquist AEL, Parry KC, Wouk K, Lawless GC, Smith JL, Smetana AR, et al. Ready, Set, BABY live virtual prenatal breastfeeding education for COVID-19. Journal of Human Lactation. 2020;36(4):614–8.
2. Nguyen PH, Kim SS, Nguyen TT, Hajeebhoy N, Tran LM, Alayon S, et al. Exposure to mass media and interpersonal counseling has additive effects on exclusive breastfeeding and its psychosocial determinants among Vietnamese mothers. Maternal & child nutrition. 2016;12(4):713–25.
3. Shu Y, He H, Shi X, Lei Y, Li J. Coronavirus disease‑2019. World Academy of Sciences Journal. 2021;3(2):1.
4. World Health Organization. The Corona Virus Disease 2019 (COVID-19). 2020;
5. Kumar D, Malviya R, Sharma PK. Corona virus: a review of COVID-19. EJMO. 2020;4(1):8–25.
6. Yamali FR, Putri RN. Dampak covid-19 terhadap ekonomi indonesia. Ekonomis: Journal of Economics and Business. 2020;4(2):384–8.
7. Kompas.com. UPDATE 21 Oktober: 143.120 Orang di Indonesia Meninggal akibat Covid-19 [Internet]. 21 Oktober 2021. 2021. Available from: https://nasional.kompas.com/read/2021/10/21/18281271/update-21-oktober-143120-orang-di-indonesia-meninggal-akibat-covid-19
8. Analisis TP&, PENANGANAN S, Provinsi C-19, Jambi. Pemetaan Risiko Covid-19 Kabupaten/Kota di Provinsi Jambi [Internet]. 3 Oktober 2021. 2021. Available from: https://corona.jambiprov.go.id/v2/files/zonasi/Pemetaan Risiko_3 Oktober 2021.pdf
9. Liu H, Wang L-L, Zhao S-J, Kwak-Kim J, Mor G, Liao A-H. Why are pregnant women susceptible to COVID-19? An immunological viewpoint. Journal of reproductive immunology. 2020;139:103122.
10. Barrero-Castillero A, Beam KS, Bernardini LB, Ramos EGC, Davenport PE, Duncan AR, et al. COVID-19: neonatal–perinatal perspectives. Journal of Perinatology. 2021;41(5):940–51.
11. Schindler-Ruwisch J, Phillips KE. Breastfeeding during a pandemic: The influence of COVID-19 on lactation services in the Northeastern United States. Journal of Human Lactation. 2021;37(2):260–8.
12. Sikorski J, Renfrew MJ, Pindoria S, Wade A. Support for breastfeeding mothers: a systematic review. Paediatric and perinatal epidemiology. 2003;17(4):407–17.
13. Singh AP, Kumar VHS, Panda S. Supporting Breastfeeding in 2021 and Beyond—Lessons from the Pandemic. Pediatric Reports. 2021;13(2):289–301.
14. Theurich MA, McCool-Myers M, Koletzko B. Supporting breastfeeding of small, sick and preterm neonates. In: Seminars in Perinatology. Elsevier; 2021. p. 151387.
15. Lima ACMACC, Chaves AFL, Oliveira MG de, Lima SAFCC, Machado MMT, Oriá MOB. Breastfeeding consultancy during the COVID-19 pandemic: experience report. Escola Anna Nery. 2020;24.
16. Haider R, Ashworth A, Kabir I, Huttly SRA. Effect of community-based peer counsellors on exclusive breastfeeding practices in Dhaka, Bangladesh: a randomised controlled trial. The lancet. 2000;356(9242):1643–7.
17. Haider R, Kabir I, Huttly SRA, Ashworth A. Training peer counselors to promote and support exclusive breastfeeding in Bangladesh. Journal of Human Lactation. 2002;18(1):7–12.
18. Sugiyono D. Metode penelitian pendidikan pendekatan kuantitatif, kualitatif dan R&D. 2013;
19. Nalsalisa J. Pengaruh Konseling Laktasi terhadap Breasfeeding Self-Efficacy pada Ibu Menyusui di Wilayah Kerja Puskesmas Sungai Mandau Tahun 2020. Universitas Pahlawan Tuanku Tambusai; 2020.
20. Giacalone A, Rocco G, Ruberti E. Physical health and psychosocial considerations during the COVID-19 outbreak. Psychosomatics. 2020;61(6):851–2.
21. Dubey S, Biswas P, Ghosh R, Chatterjee S, Dubey MJ, Chatterjee S, et al. Psychosocial impact of COVID-19. Diabetes & Metabolic Syndrome: clinical research & reviews. 2020;14(5):779–88.
22. Ceulemans M, Verbakel JY, Van Calsteren K, Eerdekens A, Allegaert K, Foulon V. SARS-CoV-2 infections and impact of the COVID-19 pandemic in pregnancy and breastfeeding: Results from an observational study in primary care in Belgium. International journal of environmental research and public health. 2020;17(18):6766.
23. Wilson JC. Using social media for breastfeeding support. Nursing for Women’s Health. 2020;24(5):332–43.
24. Anderson AK, Damio G, Young S, Chapman DJ, Pérez-Escamilla R. A randomized trial assessing the efficacy of peer counseling on exclusive breastfeeding in a predominantly Latina low-income community. Archives of Pediatrics & Adolescent Medicine. 2005;159(9):836–41.
25. Rochmawati R, Kusmintarti A, Fary V, Elfaristo L, Pembayun EL, Hayuningsih S, et al. Meningkatkan Kapasitas Ibu Menyusui Melalui Penyuluhan Kesehatan Mengenai Pemberian ASI Eksklusif Selama Masa Pandemi COVID-19. Sasambo: Jurnal Abdimas (Journal of Community Service). 2021;3(2):76–82.
26. Syahrir S, Alam S. Faktor-Faktor yang Berhubungan dengan Teknik Menyusui pada Ibu di Puskesmas Pattallassang Kabupaten Takalar. Al-Sihah: The Public Health Science Journal. 2016;8(2):130–8.
27. Graffy J, Taylor J. What information, advice, and support do women want with breastfeeding? Birth. 2005;32(3):179–86.
28. Anandita MYR. Penyuluhan Kesehatan Melalui Telemedia Pada Ibu Hamil tentang Mempersiapkan Pemberian ASI Eksklusif. Jurnal Pengabdian Masyarakat Bakti Parahita (p-ISSN-2747-2094). 2020;1(01).
29. Aidam BA, Perez-Escamilla R, Lartey A. Lactation counseling increases exclusive breast-feeding rates in Ghana. The Journal of nutrition. 2005;135(7):1691–5.
![]() This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
The Effectiveness of Electric Toothbrushes and Conventional Toothbrushes in Reducing Plaque Scores on School-Aged Children with Mental Impairment: Pilot Study
Rusmiati*, Rosmawati, Sri Febrianti, Andriani
Department of Dental Health, Health Polytechnic Ministry of Health Jambi, Indonesia
Corresponding author: dr. Rusmiati, Tazar Street, BuluranKenali, Kec. Telanaipura, Kota Jambi, Jambi 36361, Indonesia, Orcid :https://orcid.org/0000-0003-0913-4219, Phone: +62 823-0615-7373, Email: rusmiati.dentalpoltekkes@gmail.com

Cite this article
ABSTRACT
Introduction: Improving the quality of life of children is one of the goals of the health development program. The growth of children's health is not discriminated against in this scenario. All children with special needs or impairments are covered by child health services, whether at Special Schools (SS), other institutions, or in the community. This study aimed to evaluated the effectiveness of using an electric toothbrushes, compared to conventional toothbrushes, in the reduction of dental plaque score.
Methods: This study was designed as a quasi-experimental study with a pretest-posttest design. All school-aged children with mental impairment in SS Jambi City, Indonesia were included in this study. Overall, 20 children were assigned to the intervention group (n=10) and to the control group (n=10). The Personal Hygiene Performance-Modified (PHP-M) was used to examine plaque index for the assessment of dental and oral hygiene.
Results: In the pretest-posttest, mean difference values in plaque scores were statistically significant in both the intervention (19.50±3.89, p<0.009) and control (17.90±1.61, p<0.001) groups. A statistically significant reductions was showed in mean post-test plaque index (p<0.001) in the intervention group compared to the control group (14.50 ±7.83; 32.80± 13.14, respectively).
Conclusion: When compared to conventional toothbrushes, electric toothbrushes are more effective in reducing plaque scores in mentally retarded children at SS Jambi City.
Keywords: Conventional toothbrush, Electric toothbrush, Plaque score, Children, Mental impairment
INTRODUCTION
Overall health, well-being, and quality of life are all influenced by dental and oral health[1,2]. Oral health is a state of a person who is free of chronic oral diseases, facial pain, mouth and throat cancer, infections and sores, gum disease, tooth decay, tooth loss, and other diseases that impair the ability to bite, chew, smile, and talk[3].
Dental and oral health care are crucial components of comprehensive health care[4–6]. Dental and oral health indicators represent the Global Goals for Oral Health 2020. One of the technical activities of the WHO Global Oral Health Program (GOHP) is to offer advice to nations on how to build policies for preventing and promoting dental and oral illnesses[7].
Improving the quality of life of children is one of the goals of the health development program. In this situation, the development of children's health is not discriminatory, and child health services are available to all children with special needs or disabilities, regardless of whether they are in special schools (SS), other institutions, or the community[8–10].
According to the 2012 Susenas (National socio-economic survey for Indonesia), 2.45 per cent of Indonesia's population has impairments [11]. Mental retardation is one group of people with disabilities. Individuals with mental impairment are referred to as having mental retardation (mental retardation). Mental retardation, according to the American Association of Mental Deficiency (AAMD), is defined as a significant divergence from general intellectual functioning that coexists with adaptive behaviour impairments and manifests during the formative period [12].
Indahwati, et al [13] compared the dental and oral hygiene of mentally disabled and deaf students in SS-B and SS-C Tomohon City. According to the findings, mentally disabled kids had lower oral and dental hygiene than deaf students. According to Martens L et al. [14], mentally impaired children's motor abilities at the age of 12 are lower than that of normal children, and mentally disabled children have difficulties holding and using a toothbrush. Rosmawati's [15] study demonstrates that children with special needs have poor dental and oral health with an average Decay Missing Filled-Teeth (DMF-T) score of three.
Because mentally retarded children endure physical and mental development delays, such as disruptions in sensorimotor coordination, children with special needs require particular health services, one of which is children with special needs for mental retardation [16–19]. According to an interview with the principal of the State Extraordinary School 2 in Jambi City, the students at the school have a joint tooth brushing program after recess directed by the teacher and use a conventional toothbrush. However, the prevalence of dental caries remains high [20].
Brushing the teeth prevents dental caries, and the toothbrush most usually used to remove plaque is a standard toothbrush. Traditional toothbrushes need motor coordination from users, but sensorimotor skills are limited in mentally disabled youngsters.
According to some authors, manual toothbrushing entails the application of much higher pressure than the use of power brushes. Powered toothbrushes appear to be helpful in improving the oral health of physically or mentally handicapped individuals because these devices require minimal hand motion and coordination skills. Some models are designed with each bristle rotating individually and are effective plaque removers [21,22].
Considering the benefits of an electric toothbrush, it can make it easier for mentally handicapped children to clean their teeth and mentally disabled children in SS Jambi City have never used an electric toothbrush, it is vital to investigate the usefulness of conventional and electric toothbrushes in them. This study aims to evaluate the effectiveness of using an electric toothbrushes, compared to conventional toothbrushes, in the reduction of dental plaque score.
METHODS
Study design
A monocentric pilot study, with pretest-posttest design, was carried out from February to July 2022 at State Special School 2 in Jambi City, Indonesia.
Sample size
The minimum sample size required for this study was calculated using the G*Power program, considering effect size of 0.82, α-value of 0.05, power of 0.80, and sample group ratio of 1 [23]. In public health research, the value of sample size strength is at least 80%, therefore, we choose an effect size of 82% (lowest).
Participants
Eligible subject were selected according to the following inclusion criteria: all children in SS Jambi, diagnosed with mild mental retardation [24], aged 10-16 years, Dental caries index ≥ 6.6, unkempt teeth, Dental plaque score 1, bracesless. Children with moderate and severe mental retardation who were unwilling and under ten years old, Dental caries index < 6.6, Dental plaque score > 1, kempt teeth, braces and were excluded. Overall, 20 children participated in the study and were split into Intervention (n=10) and Control groups (n=10) which were randomly defined.
Intervention
After enrollment, participants were randomly assigned into a control group (n=10), in which they used a conventional toothbrush, and in the intervention group (n=10), in which they used an electric toothbrush. In both groups, the dental plaque score was evaluated at baseline (T0) and after seven days (T1). On the day 7th (T1), all participants were advised to brush their teeth and not eat food for 30 minutes before the oral health examination was conducted. All participants were instructed to brush their teeth in the morning after getting up, lunch, and dinner using the same toothpaste for both study groups. The DMF-T index is an index to assess dental and oral health status in terms of permanent dental caries [25,26]. The DMF-T index is an assessment of the total number of teeth or surfaces that are Decayed/Carious (D), Missing (M), and Filling (F) for everyone. The severity of dental caries at the age of 12 years or older is categorized into five categories, including very low severity with a DMF-T value of 0.0 – 1.0. Then the low severity level with a DMF-T value of 1.2 -2.6. Moderate severity with a DMF-T value of 2.7 – 4.4. And a high severity level with a DMF-T value of 4.5 – 6.5, and a very high severity level with a DMF-T value of ≥ 6.6
Outcomes
Disclosing solution was used to carry out the procedure for measuring plaque scores. It works by putting a disclosing solution on the subject’s tooth surface and recording the findings. Dental and oral hygiene was assessed using PHP-M (Personal Hygiene Performance-Modified). The assessment begins by making imaginary lines on the teeth to form 5 imaginary lines. The lingual and labial surfaces of the teeth were examined. If a plaque was observed in one area, it was given a score of 1. Otherwise, a score of 0 or a sign was provided (-). Plaque assessment findings were calculated by summing each plaque on each tooth surface, resulting in a plaque score for each tooth ranging from 0-to 10. Plaque scores for all teeth can range from 0 to 60, with 0-20 indicating good criteria, 21-40 indicating moderate criteria, and 41-60 indicating poor criteria.
Ethical Consideration
In this study, parents of the children had given their consent to the study. Before carrying out data collection, the researcher first took care of ethical permission. The authors state that this study followed all ethical clearance processes and was approved by the health research ethics committee of Jambi University Faculty of Medicine and Health Sciences, with number: LB.02.06/2/04/2022.
Statistical methods
For categorical variables, data were presented as numbers or percentages. The mean, standard deviation (SD), or median with Interquartile Range are used to express continuous data (IQR). Before the statistical test was carried out, the data normality test was first carried out using Shapiro Wilk test.
The non-parametric test used was Wilxocon to assess pre vs post conventional groups, while the Mann Whitney test was used to assess pre vs pre both study groups. The non-parametric tests were used for non normal data. The Paired T-Test was employed in data analysis to see if there was a difference in mean plaque scores before and after using a traditional toothbrush versus an electric toothbrush. The difference in plaque scores before and after treatment between the conventional toothbrush group and the electric toothbrush group was investigated using the independent T-Test. All tests with a p-value (p) of less than 0.05 were deemed significant. The SPSS version 16.0 application was used for statistical analysis.
RESULTS
Participants characteristics
The general characteristics of children, as shown in Table 1:
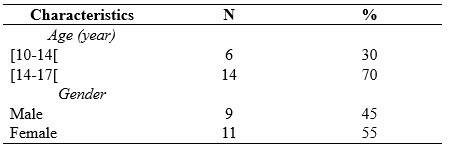
Table 1. Characteristics of childrens
The results of research on childrens with mental retardation SS Jambi City, as shown in Table 2:
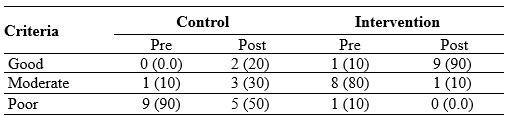
Table 2. Frequency Distribution of Plaque Score Criteria Based on PHP-M Index
Table 2 shows that before brushing their teeth, the criteria for plaque scores of children were one child (10%) with moderate criteria and nine children (90%) with poor criteria. After brushing their teeth, the criteria for plaque scores of children were two children (20%) with good criteria, three children (30%) with moderate criteria, and five children (50%) with poor criteria.
Before brushing their teeth with an electric toothbrush, the plaque score of children was eight children (80%) with moderate criteria, one child (10%) with good criteria, and one child (10%) with poor criteria. After brushing their teeth, the plaque score of nine children (90%) with good criteria and one child (10%) with moderate criteria.

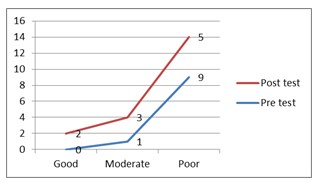
Figure 1. Plaque score criteria for control Figure 2. Plaque score criteria for intervention
group children group children
Because the sample size was less than 50 children, the Shapiro Wilk test was employed to determine the normality of the data. The sample size in this study was 20 children, as shown in Table 3:
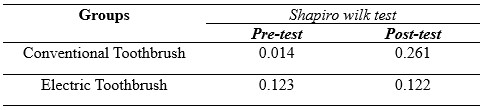
Table 3. Normality Test Results of Plaque Score Data for Children with Mental Requirements in SS Jambi City
The non-parametric test will be continued since the pre-test results in the conventional toothbrush group had an aberrant distribution of 0.014<0.05, and the post-test data were typically distributed at 0.261 > 0.05, as shown in table 3. In the meantime, the results in the electric toothbrush group were normally distributed, with a pre-test of 0.123 > 0.05 and a post-test of 0.122 > 0.05, respectively, followed by a parametric test.

Table 4. Test of the Effectiveness of Using Conventional Toothbrushes and Electric Toothbrush on Decreasing Plaque Scores in SS Jambi City
Table 4 shows that the mean score of plaque before brushing teeth is 52.30, whereas the mean score of children's plaque drops to 32.80 after brushing, indicating a 19.50 decrease in the mean value. The p-value for the paired data effectiveness test is < 0.009, indicating that using a conventional toothbrush to reduce plaque scores in mentally disabled children at SLBN 2 Jambi City is thriving. The mean score of plaque before cleaning teeth is 32.40, that the mean score of children's plaque falls to 14.50 after brushing, and that the mean value decreases by 17.90. The findings of the paired data effectiveness test show that the p-value is < 0.001, indicating that using an electric toothbrush to reduce plaque scores in mentally disabled children in SS Jambi City is beneficial.
The mean post-test value for the conventional toothbrush group is 32.80, while the electric toothbrush group is 14.50, with a P-Value of < 0.001. It indicates the difference in plaque score reduction effectiveness between conventional and electric toothbrushes in mentally disabled children.
The use of electric toothbrushes is more effective in reducing plaque scores in mentally retarded children at SS Jambi City, based on this description.
DISCUSSION
The current study is based on the theoretical basis of the physical condition of children with mental retardation. It has been known that children with mental disorders have mobility limitations, specifically in their extremities. This situation raises question marks about their ability to brush their teeth. Some studies have proven that mentally impaired children's motor abilities are lower than normal children, and mentally disabled children have difficulties holding and using a toothbrush. Children with special needs have poor dental and oral health with an average Decay Missing Filled-Teeth (DMF-T). So in this study, we evaluated the effectiveness of using an electric toothbrushes, compared to conventional toothbrushes, in the reduction of dental plaque score.
We reported that the use of conventional toothbrushes helped lower plaque scores in children with mental retardation in SS Jambi. These findings are in line with research conducted by Sitepu et al. [27] that using soft toothbrushes reduces plaque scores in mentally disabled children and a study conducted by Basith et al. [28] on 40 kids with Down syndrome in India. They observed manual or conventional toothbrushes to eliminate plaque and reduce gingivitis in children with Down syndrome for two months in each group.
In this study, it was also found that electric toothbrushes reduced the number of plaque scores in mentally disabled children in SS Jambi. Electric toothbrushes are effective in reducing OHI-S rates in children with Down syndrome, according to research conducted by Az Zahra et al. [29] and research conducted by Vandana et al. [30] on 30 people with mental problems who were observed for 45 days showed that brushing teeth with an electric toothbrush can reduce the number of mycobacteria in the oral cavity of mentally disabled children.
Plaque removal is the most critical activity for maintaining good teeth and oral health. The most popular tool for eliminating supra-gingival plaque is a toothbrush. However, most people do not clean their teeth correctly, and there is still a lot of plaque on the surface of their teeth [31].
Although electric toothbrushes are more expensive, because of the numerous designs and colors, they are thought to be more effective in raising the interest of mentally challenged youngsters in brushing their teeth. Electric toothbrushes are also good teeth cleaning equipment for preventing biofilm or plaque from forming on the surface of the teeth [32].
After brushing their teeth with an electronic toothbrush, the growing criteria for plaque scores in youngsters improve. This is due to the fact that the movement utilized in electric toothbrushes is better and more successful in reaching all parts of the mouth, as it is a systematic movement [33].
Mentally retarded children usually have difficulty in imitating the way of brushing their teeth that has been shown because their fine motor development is worse than normal children in general. Furthermore, mentally retarded children's eye and hand coordination is severely impaired. As a result, the child will have difficulties with fine motor movements, which will prevent the youngster from executing actions that demand concentration and complex hand movements [34]. Electric toothbrushes are more effective for intellectually impaired youngsters because of this. Because electric toothbrushes move automatically and children can feel the proper vibration to massage the gum and gingival area, they are a good choice for youngsters. As a result, using an electric toothbrush is more efficient and effective [29].
Although the results of this study have reported that electric toothbrushes are very suitable for use by children with mental retardation, the role of parents is highly expected. Parents or companions are required to take a more active role in encouraging mentally challenged youngsters to clean their teeth twice a day, in the morning after breakfast and at night before bed. We really hope that in the future the production of electric toothbrushes will be further improved at a price that can be affordable by all circles of society.
Based on the results of this study, we strongly recommend the use of an electric toothbrush, especially for students with mental retardation.
CONCLUSION
When compared to electric toothbrushes, electric toothbrushes are more effective in reducing plaque scores in mentally retarded children at SS Jambi City.
Study Limitations
One of the limitations of this study is the very small sample size (a pilot study), we collected data at only one center in Indonesia, which may limit the generalizability of our results to the larger population, so that in the future it is necessary to conduct similar studies in a larger population. Another limitation of the study was that the genders were not matched in the second group, which may have influenced the study results.
Authors’ contribution
All authors equally contributed to preparing this article.
Acknowledgement
We express our gratitude to the director Director of Health Polytechnic, Ministry of Health Jambi, Indonesia for its support for the implementation of this research
Funding
This research received funding from the Development and Empowerment of Human Resources in Public Health (BPPSDMK) Indonesia
Conflict Of Interest
The authors declare that there was no conflict of interest in this research.
REFERENCES
1. Van der Weijden GA, Timmerman MF, Nijboer A, Lie MA, Van der Velden U. A comparative study of electric toothbrushes for the effectiveness of plaque removal in relation to toothbrushing duration: Timerstudy. Journal of clinical periodontology. 1993;20(7):476–81.
2. Zahra AAA, Audrey NW, Ichyana DS, Saskianti T, Pradopo S, Nelwan SC, et al. Effectiveness of the Use of Manual and Electric Toothbrushes and the Effect of Educational Brushing Teeth with Video Animation on OHI-S Children with Down syndrome. Indonesian Journal of Dental Medicine. 2021;4(1):6–10.
3. WHO. Oral Health [Internet]. World Health Organization. 2018. Available from: https://www.who.int/news-room/fact-sheets/detail/oral-health
4. Govindaraju L, Gurunathan D. Effectiveness of Chewable Tooth Brush in Children-A Prospective Clinical Study. Journal of clinical and diagnostic research: JCDR. 2017;11(3):ZC31.
5. Deery C, Heanue M, Deacon S, Robinson PG, Walmsley AD, Worthington H, et al. The effectiveness of manual versus powered toothbrushes for dental health: a systematic review. Journal of Dentistry. 2004;32(3):197–211.
6. Davidovich E, Shafir S, Shay B, Zini A. Plaque removal by a powered toothbrush versus a manual toothbrush in children: A systematic review and meta-analysis. Pediatric Dentistry. 2020;42(4):280–7.
7. Kementerian Kesehatan Republik Indonesia. Pedoman Paket Dasar Pelayanan Kesehatan Gigi dan Mulut di Puskesmas. Jakarta; 2012.
8. Kementerian Kesehatan RI. Pedoman Pelayanan Kesehatan Anak di Sekolah Luar Biasa (SLB) Bagi Petugas Kesehatan. Jakarta; 2010.
9. Ganesh M, Shah S, Parikh D, Choudhary P, Bhaskar V. The effectiveness of a musical toothbrush for dental plaque removal: A comparative study. Journal of Indian Society of Pedodontics and Preventive Dentistry. 2012;30(2):139.
10. Aass AM, Gjermo P. Comparison of oral hygiene efficacy of one manual and two electric toothbrushes. Acta Odontologica Scandinavica. 2000;58(4):166–70.
11. Badan Pusat Statistik. SURVEI SOSIAL EKONOMI NASIONAL 2012 [Internet]. 2012. Available from: https://sirusa.bps.go.id/sirusa/index.php/kuesioner/202
12. Grossman HJ, Begab MJ. Classification in mental retardation. Washington, DC: Amer Assn on Intellectual & Devel; 1983.
13. Indahwati V, Mantik MFJ, Gunawan PN. Perbandingan Status Kebersihan Gigi dan Mulutpada Anak Berkebutuhan Khusus SLB-B dan SLB-C Kota Tomohon. e-GIGI. 2015;3(2).
14. Martens L, Marks L, Goffin G, Gizani S, Vinckier F, Declerck D. Oral hygiene in 12‐year‐old disabled children in Flanders, Belgium, related to manual dexterity. Community dentistry and oral epidemiology. 2000;28(1):73–80.
15. Rosmawati R, Surayah S. Status Kesehatan Gigi Dan Mulut Pada Anak Berkebutuhan Khusus Penyandang Cacat Fisik Di SLB Prof. Dr. Sri Soedewi Sofwan, SH JAMBI. JURNAL BAHANA KESEHATAN MASYARAKAT (BAHANA OF JOURNAL PUBLIC HEALTH). 2018;2(1).
16. Carina C, Panjaitan M, Anastasia I, Adhana A. Perbedaan efektivitas sikat gigi elektrik dengan sikat gigi manual dalam penurunan indeks plak pada anak-anak tunanetra. Prima Journal of Oral and Dental Sciences. 2020;3(2):33–8.
17. Pasyah F. Gambaran Kekerasan Bulu Sikat Gigi Terhadap Penurunan Debris Indeks Pada Siswa/i Kelas VIII-1 SMPN 3 Perbaungan Kec. Perbaungan kab. Serdang Bedagai. Poltekkes Kemenkes Medan; 2019.
18. Ichyana D. Efektifitas Sikat Gigi Manual Dan Sikat Gigi Elektrik Terhadap Skor Ohi-S Anak Down Syndrome [Internet]. Universitas Airlangga; 2019. Available from: https://repository.unair.ac.id/93229/
19. Hasanuddin SH. Efektivitas Pendidikan Kesehatan Menggunakan Media Video Dengan Media Cerita Bergambar Terhadap Keterampilan Menggosok Gigi Anak Usia Prasekolah. Universitas Islam Negeri Alauddin Makassar; 2018.
20. Department of Health Jambi Province. Profile Health Department of Health Jambi Province [Internet]. Jambi, Indonesia; 2020. Available from: http://dinkes.jambiprov.go.id/file/informasi_publik/MTYxNTE2NDQyOA_Wkt1615164428_XtLnBkZg.pdf
21. Vorwerk L, Ghassemi A, Hooper W, Patel V, Milleman J, Milleman K. Comparative plaque removal efficacy of a new powered toothbrush and a manual toothbrush. J clin dent. 2016;27(3):76–9.
22. García‐Carrillo A, Jover A, Plá R, Martorell A, Sota C, Gómez‐Moreno G, et al. Manual versus sonic powered toothbrushing in patients with intellectual disability: a cluster‐randomized clinical trial. Journal of Clinical Periodontology. 2016;43(8):684–93.
23. Faul F, Erdfelder E, Lang A-G, Buchner A. G* Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behavior research methods. 2007;39(2):175–91.
24. Association AP. American Psychiatric Association: Diagnosti c and Statistical Manual of Mental Disorders, Arlington. 2013.
25. Jaime RA, Carvalho TS, Bonini GC, Imparato JCP, Mendes FM. Oral health education program on dental caries incidence for school children. Journal of clinical pediatric dentistry. 2015;39(3):277–83.
26. Hariyani N, Soebekti RH, Setyowati D, Bramantoro T, Palupi LS, Putriana E. Factors influencing the severity of dental caries among Indonesian children with autism spectrum disorder–a pilot study. Clinical, cosmetic and investigational dentistry. 2019;11:227.
27. Sitepu DT, Edi IS, Hidayati S. Penurunan Indeks Plak Gigi Ditinjau Dari Penggunaan Sikat Gigi Hard, Medium, Dan Soft. Jurnal Ilmiah Keperawatan Gigi. 2021;2(2):1–6.
28. Basith A, Monica, Biir. Comparative Evaluation of Effectiveness of Manual and Electric Tooth Brush (Oral - B) in Elimination of Dental Plaque and Gingivitis. 2019;4(March):45–50.
29. Az Zahra AA, Audrey NW, Ichyana DS, Saskianti T, Pradopo S, Nelwan SC, et al. Effectiveness of the Use of Manual and Electric Toothbrushes and the Effect of Educational Brushing Teeth with Video Animation on OHI-S Children with Down syndrome. Indonesian Journal of Dental Medicine. 2021;4(1):6.
30. Vandana KL, Tatuskar PV, Valavalka NN. A Comparative Evaluation Of Manual And Powereed Brushing On Oral Health And Microbial Of Mentallu Challenged Induvidual. 2020;(May):113–8.
31. Bahammam S, Chen CY, Ishida Y, Hayashi A, Ikeda Y, Ishii H, et al. Electric and manual oral hygiene routines affect plaque index score differently. International Journal of Environmental Research and Public Health. 2021;18(24).
32. Silva AM, Miranda LFB, Araújo ASM, Prado Júnior RR, Mendes RF. Electric toothbrush for biofilm control in individuals with Down syndrome: A crossover randomized clinical trial. Brazilian Oral Research. 2020;34(June).
33. Rahman eddy, Ilmi MB. Perbedaan Sikat Gigi Biasa Dengan Sikat Gigi Elektrik Terhadap Penurunan Debris Indeks Pada Murid Kelas V Madrasah Diniyah islamiyah Kindaung Banjarmasin. Jurnal Kesehatan Indonesia. 2019;9(3):122–8.
34. Hakim AR. Pengaruh Motorik Kasar Anak Tunagrahita Terhadap Motorik Halus. Jurnal Ilmiah PENJAS. 2016;2(2):33–49.
![]() This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
EFFECTIVENESS OF E-BOOK APPLICATION MODEL UTERINE ATONY MANAGEMENT GUIDE AND POCKETBOOK IN IMPROVING MIDWIFE KNOWLEDGE AND SKILLS IN BASIC CARE: PRE-POST STUDY
Titik Hindriati1*, Nuraidah1, Rosmaria1, Diniyati1
1. Department of Midwifery, Health Polytechnic of Jambi, Indonesia
* Corresponding author: Titik Hindriati, Jl. Prof DR GA Siwabessy No.42, BuluranKenali, Kec. Telanaipura, Kota Jambi, Jambi 36122 Department of Midwifery, Health Polytechnic of Jambi, Indonesia. Orcid :https://orcid.org/0000-0001-7604-8068. Email: titikpoltekkes@gmail.com
Cite this article
Abstract
Background: Midwives are one of the main health workers at the frontline of health development to accelerate the decline in Maternal Mortality Rate (MMR) and Infant Mortality Rate (IMR). Therefore, competent and skilled midwives are needed in carrying out clinical procedures, especially in handling emergency cases of postpartum hemorrhage, with critical analysis skills. This study aims to determine the effectiveness of e-book application model uterine hypotonia management guide and pocket book in improving midwife knowledge and skills in basic care.
Method: The research design used was pre-post study, which was carried out in February-April 2021. The population and sample in this study were all midwives who provided delivery assistance at the Jambi City Health Center, totaling 64 respondents. Data analysis used the Wilcoxon and Mann-Whitney tests.
Results: In each intervention group, all variables, including knowledge and skills, are increased in both groups defined. The results showed that the educational media application of guidelines and pocketbooks on postnatal emergency management increased knowledge and skills.
Conclusion: The two study groups had a significant effect on increasing the knowledge and skills of midwives in handling postnatal emergencies due to uterine atony.
Keywords: Midwive, Emergency handling, learning media, pocket books, applications
Introduction
The role of health workers will determine the success of development programs in the health sector [1–3]. Midwives are one of the main health workers spearheading health development to accelerate the decline in Maternal Mortality Rate (MMR) and Infant Mortality Rate (IMR) [4]. For this reason, it is necessary to have midwives who have the ability and skills in clinical procedures, especially in proper management in handling emergency cases of postpartum mothers due to uterine atony with critical analytical skills [5,6].
According to the World Health Organization (WHO), the maternal mortality rate in the world in 2015 was 216 per 100,000 live births, with the highest number in developing countries, namely 239 per 100,000 live births, or 20 times higher than the maternal mortality rate in developed countries, which were only 12 per 100,000 live births [7]. Nearly 75% of all maternal deaths are caused by postpartum hemorrhage, infection (usually after delivery), high blood pressure during pregnancy (pre-eclampsia and eclampsia), and unsafe abortion [8].
Based on the 2012 Indonesian Demographic and Health Survey (IDHS), the maternal mortality rate in Indonesia is 359 per 100,000 live births. It shows a downward trend to 117 per 100,000 live births in 2017, while the Maternal Mortality Rate (MMR) target is according to the Sustainable Development Goals (SDGs) of 70 per 100,000 live births in 2030 [9]. The Maternal Mortality Rate (MMR) in Jambi city in 2018 was 18.86/100 live births, and in 2019 it increased to 46.15/100 live births, although this data is still below the national Maternal Mortality Rate (MMR). Medical factors that are direct causes of maternal death are bleeding by 42%, pregnancy poisoning (eclampsia) 13%, miscarriage (abortion) 11%, infection 10%, delayed labor / prolonged labor 9% and other causes 15% [10].
Obstetric emergencies are life-threatening health conditions that occur during pregnancy or during and after labor and birth [11,12]. The government's effort to reduce Maternal Mortality Rate (MMR) and Infant Mortality Rate (IMR) is to provide quality basic maternal and neonatal health services, namely Basic Emergency Obstetrics and Neonatal Services (PONED) at the Puskesmas. However, the maternal and neonatal emergency case services at the PONED Health Center have not been running according to the targeted expectations [13].
The high maternal and infant mortality rate can be caused by the lack of skilled midwives as health service providers, starting from pregnancy to delivery. To improve the knowledge and skills of midwives as service providers, maximum innovation is needed, including the provision of a pocketbook for handling emergency midwifery. This guideline is compiled in the form of a pocketbook equipped with an algorithm to facilitate health workers in handling emergency obstetric cases quickly. The second option can be using an android application that contains an e-book of obstetric emergency case materials, especially in the treatment of uterine atony [14,15].
In Interactive Multimedia, the stimulus appears by presenting exercises related to the material so that the midwife can respond by typing or pressing a button and then facilitated by feedback [16–19]. The existence of an attractive program display can lead to motivation so that aspects of learning readiness will also appear [20–23]. Multimedia applications can assess midwifery/psychomotor skills in basic services to detect emergency cases. Midwives as spearheads for maternal and infant health are good in theory and practice, especially for handling emergency cases. A midwife must provide quality midwifery services to prevent complications and maternal death due to complications [15,24].
The current study aims to evaluate the effectiveness of e-book application model uterine atony management guide and pocket book in improving midwife knowledge and skills in basic care.
Methods
Design
The design used is development, where this method is used to produce certain products and test the effectiveness of these products. Product testing is done by using pre-post Study.
Participants
The research respondents were 64 midwives (divided into 32 people in group 1 and 32 people in group 2) at PutriAyu Health Center and PakuanBaru Health Center who were randomly selected with the inclusion criteria of midwives who provide delivery services and have a working period of more than one year.
Intervention
The variables of this study are the knowledge and skills of the midwife who will be measured before and after the educational intervention using the application of postpartum emergency guidance due to uterine atony and pocketbooks.
The knowledge questionnaire has objective criteria of good or low, uses a Guttman scale, and consists of 15 questions with a rating range of 0-15. The variable of midwifery skill in this study was defined as the ability of the midwife to practice the procedures for handling emergency obstetrics, in this case uterine atony.
The skill questionnaire has good or poor objective criteria, uses a Guttman scale, and consists of 15 question items with an assessment range of 0-15.
The Guttman scale was used in this study because the variables used were nominal scales. The Guttman scale has an important characteristic, which is that it is a cumulative scale and measures only one dimension of a multi-dimensional variable, so that this scale has an undimensional nature. The data obtained are in the form of interval data or dichotomy ratios (two alternatives) [25].
The group 1 received an intervention providing education on using an emergency postpartum guide application due to uterine atony for seven days. The group 2 will receive an education pocketbook on handling emergency postpartum due to uterine atony for seven days. On the first day before giving the intervention, researchers measured the level of knowledge using a questionnaire in both study groups, as well as the skills of midwives were measured using a questionnaire consisting of the midwife's ability to prepare tools, prepare patients, perform actions according to procedures, evaluate patient responses to actions that have been taken. midwife, and the ability of the midwife to document the actions that have been taken.
The first stage is the research starting from determining the team, determining the development schedule, selecting and determining the scope, structure, and order of the material, determining multimedia specifications, and making storyboards. The second stage is the development stage consisting of expert validation, practitioner validation, and the implementation and evaluation stages. The third stage is the Effectiveness Test.
Blinding
In this study, 2 enumerators were used to collect research data. The previous enumerators did not know the participants because they were students who had been trained by the researcher before collecting data. The enumerators involved in this study were final year students who were about to complete their midwifery diploma, and were tasked with helping researchers collect data in the field by distributing questionnaires, however, the assessment of participants' skills was assessed by the researcher.
Statistical methods
Data were presented as numbers or percentages for categorical variables. Continuous data are expressed as the mean ± standard deviation (SD), or median with Interquartile Range (IQR). The data obtained were analyzed by univariate and bivariate, from the normality test (Kolmogorov Smirnov) obtained abnormal data so that the analysis used the Wilcoxon and Mann Whitney test. All tests with p-value (p)<0.05 were considered significant. Statistical analysis was performed using the SPSS version 16.0 application.
Ethical Consideration
Registered prospective respondents have signed an informed consent and there is no incentive to participate in the study and the anonymity of participants is guaranteed. Before carrying out data collection, the researcher first took care of ethical permission.
The authors state that this study followed all ethical clearance processes and was approved by the health research ethics committee of Ministry of Health Polytechnic of Jambi, Indonesia, and registration number: LB.02.06/2/167/2021.
Results
The results of the univariate analysis, which aims to determine the frequency of each variable studied, can be seen in the following table:
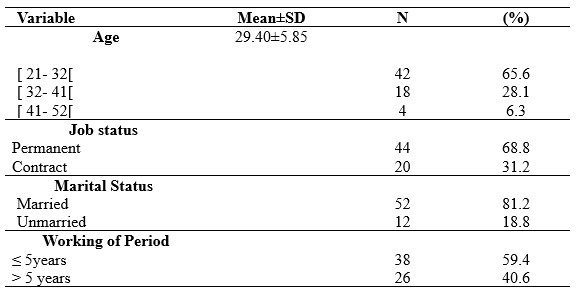
Table 1. Demographic data of participants
Table 1 shows that the dominant respondents aged 21-32 year are 41 people (65.6%), have employment status as permanent employees as many as 44 people (68.8%), 52 people are married (81.2%), and have a working period of ≤5 years as many as 38 people (59.4%).
Based on the normality test, the statistical test used in this study is non-parametric, with the results as shown in the following table:
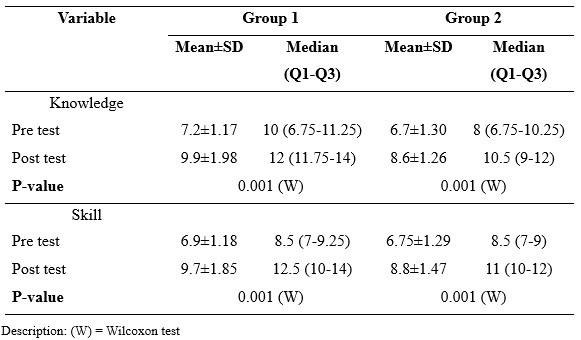
Table 2. Differences in mean values and Wilcoxon test results
Table 2 shows that in each intervention group, group 1 vs group 2, all variables, both knowledge and skills, have increased. In group 1 (e-book emergency guidance application) the median value of knowledge before intervention was 10 with a mean value of 7.2 while in group 2 (pocket book) it had a median value of 8 with a mean value of 6.7. After the intervention, group 1 (e-book emergency guidance application) had a median value of knowledge of 12 with a mean value of 9.9, while group 2 (pocket book) had a median value of 10.5 with a mean value of 8.6.
On the skill variable, in group 1 (e-book emergency guidance application) the median value before intervention was 8.5 with a mean value of 6.9 while in group 2 (pocket book) it had a median value of 8.5 with a mean value of 6.75. After the intervention, group 1 (emergency guide application e-book) had a median skill score of 12.5 with a mean value of 9.7, while group 2 (pocket book) had a median value of 11 with a mean value of 8.8.
The differences in knowledge and skills between the two study groups are presented in table 3.
Table 3. Result of Mann Whitney test
Table 3 shows that the results of the Mann Whitney test prove that there is no difference between the two study groups in improving the knowledge and skills of midwives, in the sense that both groups (group 1 and group 2) are equally effective in improving the knowledge and skills of midwives in handling emergency obstetric cases.
Discussion
The information obtained by previous respondents strongly influences a person's level of knowledge. When the pre-test was carried out, the results obtained showed that the midwife had less knowledge before being given an android application for handling postnatal emergencies and a pocketbook. After the intervention, the respondent's knowledge increased by 71% in the group that received Android educational media. In contrast, the group that received pocketbooks in the group 2 also increased even though it was only 57%.
The Mobile Application, Education for handling postnatal emergencies, provides menus of information on handling postnatal emergencies, especially animated videos so that participants pay more attention to and master the techniques of handling postnatal emergencies.
Educational media serves to mobilize as many senses as possible to an object to facilitate the perception of the recipient of information [26]. The media will help clarify the information conveyed because it can be more interesting and interactive and overcome the limitations of space, time, and human senses. So that the information conveyed can be clearer and easier to understand according to the purpose for which it will be used [27]. Educational materials can be packaged according to the characteristics of each media used [28]. Today's cellphones not only function as a means of telecommunications but have switched functions to become androids that can do many things [29]. Mobile phones with functions like this can be known as smartphones. Smartphones can assist in medical activities, such as establishing diagnosis and therapy. From various forms of information technology and telecommunications, mobile phones are considered a suitable medium for increasing knowledge in the current developing era. The use of this smartphone is more effective than the module without the application [30,31].
Wahyuni's research [32] on the effect of smartphone applications on a person's knowledge and skills in stimulating the growth and development of toddlers shows an increase in knowledge and skills. Therefore, providing education through interesting media based on Android will make it easier for someone to stimulate independently. In addition to these researchers, other researchers state an effect of using printed media in the form of pocketbooks on increasing the knowledge of postpartum mothers. The study states that print media is the most frequently used and easy-to-reach media, for example, pocketbooks [33]. Pocket books occupy an important position in providing education because they provide clear and practical messages that allow readers to read at any time without the need for the internet to access them and are equipped with images that match the material, making it easier to understand the material [34].
Studies among various healthcare professionals reported mixed results regarding the usefulness of the e-learning, mobile learning and technology-enhanced learning. A Cochrane systematic review conducted by Vaona et al in [35] compared traditional learning with e-learning and reported that e-learning may make little or no difference in health professionals’ behaviours, skills or knowledge. A study conducted by Subhash et al, [36] among medical students reported that smartphones can be effectively used for learning. A study conducted by Snashall et al, [15] among medical students reported that medical apps can be used as an adjunct in medical education, though the evidence remains limited. Furthermore, data analysis showed that the respondent's skills increased after being given an intervention using an application for handling postnatal emergencies 43%. After being given education through a pocketbook in the group 2, the increase was lower than 21.4%. The results of the Mann-Whitney test in this study showed that there was no difference in knowledge and skills between the two study groups regarding postnatal emergency management who received the android application and the group who received a pocketbook. It shows that any media used can improve knowledge and skills because the function of the media is to help facilitate learning for students, provide a more real experience, attract greater attention from respondents because it is not boring, and all senses of respondents can be activated, attract more attention and interest of respondents in learning [37]. The most plausible reason is that the skill of midwives is higher in the group that received application media education compared to pocketbooks because the application media can be studied anytime and anywhere and displays interesting features and videos of emergency obstetric emergencies, especially uterine atony, so that midwives able to understand and remember strongly the material seen and heard [38].
Conclusion
The application model of pocket books and e-books for the management of uterine atony has been proven to be effective in improving the knowledge and skills of midwives in primary care.
Study Limitations
The limitation of this study is that this research involves a small number of samples so that this type of research is a preliminary study, and only involves a certain location, namely 1 area, so it cannot compare the results of this study to the character of the community in different locations. In the future it is necessary to conduct research on a large regional scale and the number of samples in a very large size.
Acknowledgement
We would like to express our gratitude to the director of the Midwifery Department of Jambi health polytechnic who has supported this research.
Funding statement
This research did not receive any specific grant from funding agencies in the public, commercial, or not for profit sectors.
Competing interests statement
There are no competing interests for this study.
Authors’ contribution
TH and NU were responsible for the study conception and design; RO performed the data collection; TH and DN performed the data analysis; NU, and RO were responsible for the drafting of the manuscript; TH and NU made critical revisions to the paper for important intellectual content.
References
1. Ani M, Azizah N, Rahmawati VE, Mardiah A, Febriyeni F, Astuti ED, et al. Pengantar Kebidanan. Yayasan Kita Menulis; 2021.
2. Liu A, Sullivan S, Khan M, Sachs S, Singh P. Community health workers in global health: scale and scalability. Mount Sinai Journal of Medicine: A Journal of Translational and Personalized Medicine. 2011;78(3):419–35.
3. Franco LM, Bennett S, Kanfer R. Health sector reform and public sector health worker motivation: a conceptual framework. Social science & medicine. 2002;54(8):1255–66.
4. Erawati AD, Rinayati R, Wahyuning S. Midwife roles to decline maternal mortality rate. International Journal of Public Health Science. 2020;9(1):29–33.
5. Scholes J, Endacott R, Biro M, Bulle B, Cooper S, Miles M, et al. Clinical decision-making: midwifery students’ recognition of, and response to, post partum haemorrhage in the simulation environment. BMC Pregnancy and Childbirth. 2012;12(1):1–12.
6. Maslovitz S, Barkai G, Lessing JB, Ziv A, Many A. Recurrent obstetric management mistakes identified by simulation. Obstetrics & Gynecology. 2007;109(6):1295–300.
7. Organization WH. Trends in maternal mortality: 1990-2015: estimates from WHO, UNICEF, UNFPA, World Bank Group and the United Nations Population Division. World Health Organization; 2015.
8. Organization WH. Trends in maternal mortality 2000 to 2017: estimates by WHO, UNICEF, UNFPA, World Bank Group and the United Nations Population Division. World Health Organization; 2019.
9. Kementerian Kesehatan RI. Laporan Riskesdas 2018. Laporan Nasional Riskesdas 2018. 2018.
10. BPS Provinsi Jambi. Jambi dalam angka [Internet]. 2019. Available from: https://jambi.bps.go.id/
11. Teela KC, Mullany LC, Lee CI, Poh E, Paw P, Masenior N, et al. Community-based delivery of maternal care in conflict-affected areas of eastern Burma: perspectives from lay maternal health workers. Social Science & Medicine. 2009;68(7):1332–40.
12. Susilawati E, Johari A, Marzal J, Anggereini E. Effects of Multimedia E-Books and Augmented Reality on Knowledge and Skills of Health Sciences Students: A Systematic Review. Journal of Client-Centered Nursing Care. 2022;8(2):99–110.
13. Rayfitra MR, Achmad F, Yuniarti Y. Perbandingan Tingkat Pengetahuan Bidan sebelum dan setelah Pemberian Edukasi mengenai Manajemen Kegawatdaruratan Obstetri di Puskesmas Mampu Poned Kota Bandung. 2020;
14. Sadagheyani HE, Tatari F, Raoufian H, Salimi P, Gazerani A. The effect of multimedia-based education on students’ anger management skill. Educacion Medica. 2021;22(3):149–55.
15. Snashall E, Hindocha S. The use of smartphone applications in medical education. Open Medicine Journal. 2016;3(1).
16. Tirtaningrum DA, Sriatmi A, Suryoputro A. Analisis Response Time Penatalaksanaan Rujukan Kegawatdaruratan Obstetri Ibu Hamil. Media Kesehatan Masyarakat Indonesia Universitas Hasanuddin. 2018;14(2):139–46.
17. Mustafa AR, Ramadany S, Sanusi Y, Made S, Stang S, Syarif S. Learning Media Applications for Toddler Midwifery Care about Android-Based Fine Motor Development in Improving Midwifery Students Skills. International Journal of Health and Medical Sciences. 2020;3(1):130–5.
18. Kardina I, Ramadany S, Sanusi Y, Made S, Stang S, Syarif S. Children’s Midwifery Learning Media Application About Android-based Rough Motor Development in Improving Midwifery Student Skills. International Journal of Health and Medical Sciences. 3(1):146–52.
19. Gebze DA, Perwati S. Improving problem-solving ability in physics through android-based mobile learning application. In: Journal of Physics: Conference Series. IOP Publishing; 2020. p. 12022.
20. Alwy Al-beity F, Pembe AB, Kwezi HA, Massawe SN, Hanson C, Baker U. “We do what we can do to save a woman” health workers’ perceptions of health facility readiness for management of postpartum haemorrhage. Global Health Action. 2020;13(1):1707403.
21. Ventola CL. Mobile devices and apps for health care professionals: uses and benefits. Pharmacy and Therapeutics. 2014;39(5):356.
22. Prasetyo H, Kristiyanto A, Doewes M. The Development of Android-Based Mobile Learning Media in Healthy Lifestyle Teaching Materials for Senior High School Students. International Journal of Multicultural and Multireligious Understanding. 2019;6(2):188.
23. Jesse GR. Smartphone and app usage among college students: Using smartphones effectively for social and educational needs. In: Proceedings of the EDSIG Conference. 2015.
24. Hasnah H, Triratnawati A. Penelusuran Kasus-Kasus Kegawatdaruratan Obstetri yang Berakibat Kematian Maternal: Studi kasus di RSUD Purworejo, Jawa Tengah. Makara J Heal Res. 2010;7(2):38–48.
25. Sugiyono. Metode Penelitian Kuantitatif, Kualitatif dan R&D. Bandung: PT Alfabet; 2016.
26. Gamar MM, Tati ADR. Utilization of ICT-Based Learning Media in Local History Learning. In: Journal of Physics: Conference Series. IOP Publishing; 2021. p. 12079.
27. Rohaeti EE, Bernard M, Primandhika RB. Developing interactive learning media for school level mathematics through open-ended approach aided by visual basic application for excel. Journal on Mathematics Education. 2019;10(1):59–68.
28. Puspitarini YD, Hanif M. Using Learning Media to Increase Learning Motivation in Elementary School. Anatolian Journal of Education. 2019;4(2):53–60.
29. Safitri I, Pasaribu R, Simamora SS, Lubis K. The effectiveness of android application as a student aid tool in understanding physics project assignments. Jurnal Pendidikan IPA Indonesia. 2019;8(4):512–20.
30. Hafis M, Meliasari R. Analisis Penggunaan Aplikasi pada Smartphone sebagai Media Pembelajaran. JIIP-Jurnal Ilmiah Ilmu Pendidikan. 2021;4(8):740–7.
31. Barnett J, Harricharan M, Fletcher D, Gilchrist B, Coughlan J. myPace: an integrative health platform for supporting weight loss and maintenance behaviors. IEEE journal of biomedical and health informatics. 2014;19(1):109–16.
32. Wahyuni T, Syswianti D, Hidayat DR. Uji Diagnostik Aplikasi Mother Cares (Moca) Untuk Deteksi Dini Risiko Penyimpangan Perkembangan Balita. 2019;
33. Ahmady A, Ashari AE. Efektifitas buku saku dalam meningkatkan pengetahuan pendamping ibu nifas di Kabupaten Mamuju. Jurnal Kesehatan Manarang. 2018;4(2):122–7.
34. Azadirachta FL, Sumarmi S. Pendidikan Gizi menggunakan media buku saku meningkatkan pengetahuan dan praktik konsumsi sayur dan buah pada siswa sekolah dasar. Media Gizi Indonesia. 2017;12(2):107–15.
35. Vaona A, Banzi R, Kwag KH, Rigon G, Cereda D, Pecoraro V, et al. E‐learning for health professionals. Cochrane Database of Systematic Reviews. 2018;(1).
36. Subhash TS, Bapurao TS. Perception of medical students for utility of mobile technology use in medical education. International Journal of Medicine and Public Health. 2015;5(4).
37. Stegeman CA, Zydney J. Effectiveness of multimedia instruction in health professions education compared to traditional instruction. American Dental Hygienists’ Association. 2010;84(3):130–6.
38. Ahmar H, Budi P, Ahmad M, Mustary M, Hutagaol IO. The Influence of Problem Based Learning Model Based on Midwifery First Stage of Childbirth Care Module in Improving Learning Quality. International Journal of Psychosocial Rehabilitation. 2020;24(2).
![]() This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
Assessment of quality of life for hypertensive patients: Integrative review for Potential of Novel Assessment Tools of quality of life
La Ode Alifariki1*, Sri Susanty2, Heriviyatno Julika Siagian3, Daryono Daryono4
1Department of Epidemiology, Medical School, Halu Oleo University, Kendari, Indonesia
2Department of Nursing, Medical School, Halu Oleo University, Kendari, Indonesia
3Department of Medical Surgical Nursing, College of Science and Technology, Sembilanbelas November University, Kolaka, Indonesia
4Nursing Department, Health Polytechnic Ministry of Health Jambi, Indonesia
Corresponding author: La Ode Alifariki, Kampus Hijau Bumi Tridharma, Anduonohu, Kec. Kambu, Kota Kendari, Sulawesi Tenggara 93232, Indonesia. Orcid: https://orcid.org/0000-0003-4120-7465. Email: ners_riki@yahoo.co.id

Cite this article
ABSTRACT
Background & Aim: The body of literature on QoL has steadily grown over recent years, spurred by the promotion of research and the cross-cultural adaptation and validation of assessment instruments in different languages. However, limited information exists on the most commonly used instruments against the backdrop of current demographic and epidemiological trends. The aim this study to evaluate QoL assessment instruments used in hypertensive patients.
Methods & Materials: This review was conducted using the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement. Databases used including Sciencedirect, Cochrane library, Pubmed, Proquest, and the Wiley Online Library, utilizing keywords that are tailored to the Mesh Terms. Systolic Blood Pressure (SBP) value at least 140 mmHg and/or Diastolic Blood Pressure (DBP) value at least 90 mmHg, or the patient had a history of hypertension and was administered with antihypertensive drugs, English version, observational studies that presented Health-Related Quality of Life (HRQoL) scores in hypertensive individuals using varied assessment tools (WHOQoL BREF, SF-36, MINICHAL, etc) where these tools assess the situation of the patient's quality of life based on the domain of life (physiological, psychological, social interaction, etc.) in the form of numbers, and published between January 2000 to December 2021 were inclusion criteria of the study. Relevant studies were read critically, analyzed, and described in detail. Survey data were processed in the form of comparative tables.
Results: A total of 2,287,348 references were found through databases, and for the final screening, twenty-two articles were finally designated as articles to be reviewed. The SF-36 (SF-8, SF-12), WHOQoL BREF, MINICHAL, and PECVEC are assessment tools used in the studies included in this review. The SF-36 was the most widely used tool in the studies included in this review. One of the critical domains to assess is spiritual, where none of the studies included this domain.
Conclusion: The SF-36 is the most frequently used assessment tool. However, this form is a general form that is not explicitly intended to assess the quality of life in hypertension only. The spiritual domain is one of the important items that need to be included in the QoL assessment tool.
Keyword: Quality of life, assessment tool, hypertension
INTRODUCTION
Hypertension is one of the most common chronic diseases that threaten the health of human beings. Poor adherence to treatment and low control rate of hypertension are the risk factors for coronary heart disease, stroke, and renal insufficiency, causing a great disease burden worldwide [1–3]. For a long time, the evaluation for the health condition of hypertension patients is usually based on the control of patients’ blood pressure (BP) or the degree of damage to the target organ [4–6]. As the medical model has changed from the biological medical model to the biological–psychosocial medical model, it is difficult to comprehensively and accurately assess chronic diseases (such as hypertension) in terms of incidence, death rate, cure rate, and life expectancy. Thus, the health-related quality of life (HRQoL) has gradually arisen with great attention in the world [7–9].
Quality of Life (QoL) is a broad ranging concept affected in a complex way by the person’s physical health, psychological state, level of independence, social relationships, personal beliefs and their relationship to salient features of their environment[10]. Health related QoL (HRQoL) is emerging as an important outcome in hypertension and can be adversely affected by hypertension itself and side-effects of antihypertensive drugs. However reports of HRQoL among hypertensive individuals have been conflicting, with some studies finding worse HRQoL among hypertensive compared to the general population, while Moum T et al reported no impact of hypertension on HRQoL in some / all domains. There is a paucity of studies reporting QoL in Indian hypertensive patients [8,11,12]. Assessing QoL is of essence, as this concept serves as an indicator in clinical trials for specific diseases, assesses the physical and psychosocial impact that the disorders may have on affected individuals, allowing a better knowledge about the patient and their adaptation to their unhealthy condition. Roca-Cusachs et al reported that hypertensive patients had a significant reduction in QoL compared to normotensive patient [13,14].
Scales measuring HRQoL of hypertensive patients include EuroQOL five-dimension questionnaire, WHO QoL-100 (the well-being questionnaire), SF-36 (the Medical Outcomes 36 Item Short-form Health Survey), and so on. SF-36 is the most widely used scale for assessing HRQoL, which has high reliability. In addition, SF-12, the shorter form of SF-36, is an effective alternative to the SF-36 in hypertension. Although many articles showed a significantly lower HRQoL of hypertension patients, some still present no difference in many domains [7,15,16].
Another quality of life assessment form that is starting to be widely used is MINICHAL. MINICHAL, an assessment tool focusing on people with hypertension, was formed in 2002 by a group from Spain [13], and it was shown to be effective in the measurement of HRQoL of elderly people with hypertension linked to the supplementary health sector and evidenced a lower impairment in HRQoL among the elderly practicing physical activity [17].
The body of literature on QoL has steadily grown over recent years, spurred by the promotion of research and the cross-cultural adaptation and validation of assessment instruments in different languages. However, limited information exists on the most commonly used instruments against the backdrop of current demographic and epidemiological trends. In light of the above, the aim of this study was to evaluate QoL assessment instruments used in hypertensive patients.
METHODS
Review Protocol
This integrative review was conducted using the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) statement [18]. The current study tries to evaluate QoL assessment instruments used in hypertensive patients from articles that have been published in the period January 2000 to December 2021.
Searching strategy
Relevant articles were searched and collected using Sciencedirect, Cochrane library, Pubmed, Proquest, and the Wiley Online Library, with a publication time between 2000 and 2021. The search keywords were adjusted according to the Mesh terms for health research. The keywords used vary, depending on the search engine used. In general, the keywords focus on Quality of life OR HRQoL AND Hypertension AND Measurement AND Assessment tool OR WHOQoL OR SF-36 OR MINICHAL. Summary of keywords used in each databases are reported in table 1.
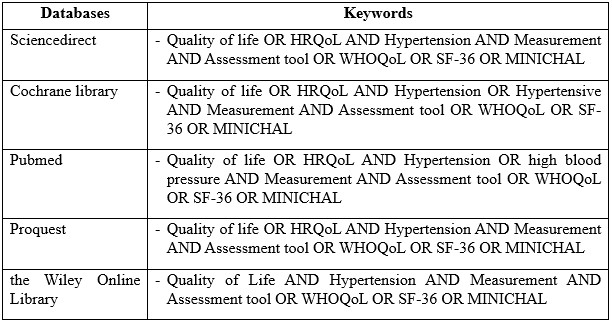
Table 1. Search string in databases
Study eligibility
Inclusion criteria: Hypertension is defined as Systolic Blood Pressure value at least 140 mmHg and/or Diastolic Blood Pressure value at least 90 mmHg, or the patient had a history of hypertension and was administered with antihypertensive drugs. Language was restricted to English. All observational studies that presented Health Related Quality of Life (HRQoL) scores in hypertensive individuals using varied assessment tools (WHOQoL BREF, SF-36, MINICHAL, etc) where these tools assess the situation of the patient's quality of life based on the domain of life (physiological, psychological, social interaction, etc.) in the form of numbers, published between January 2000 to December 2021. In addition, we manually searched the cited reference of potentially eligible articles and published reviews.
Studies were excluded if they were carried out in special groups (armies, a pasturing area, etc.) and cannot represent the general population; they compared HRQoL of individuals randomized to different antihypertensive agents or placebo or other interventions.
Study selection and data analyses
After a further authentication of the articles, cross sectional, and case-control study design were chosen for final analysis. Relevant studies were read critically, analyzed, and described in detail. The methodological quality of studies was evaluated using National Institute of Health (NIH) for observational cohort and cross sectional studies. The checklist has 14 questions including Q1: Was the research question or objective in this paper clearly stated?; Q2: Was the study population clearly specified and defined?; Q3: Was the participation rate of eligible persons at least 50%?; Q4: Were all the subjects selected or recruited from the same or similar populations (including the same time period)? Were inclusion and exclusion criteria for being in the study prespecified and applied uniformly to all participants?; Q5: Was a sample size justification, power description, or variance and effect estimates provided?; Q6: For the analyses in this paper, were the exposure(s) of interest measured prior to the outcome(s) being measured?; Q7: Was the timeframe sufficient so that one could reasonably expect to see an association between exposure and outcome if it existed?; Q8: For exposures that can vary in amount or level, did the study examine different levels of the exposure as related to the outcome?; Q9: Were the exposure measures (independent variables) clearly defined, valid, reliable, and implemented consistently across all study participants?; Q10: Was the exposure(s) assessed more than once over time?; Q11: Were the outcome measures (dependent variables) clearly defined, valid, reliable, and implemented consistently across all study participants?; Q12: Were the outcome assessors blinded to the exposure status of participants?; Q13: Was loss to follow-up after baseline 20% or less?; Q14: Were key potential confounding variables measured and adjusted statistically for their impact on the relationship between exposure(s) and outcome(s)? relating to the research question, selection of study subjects, statistical analysis and measurement and selection of timeframe between exposure and outcome to see an effect. The quality grading of studies was done as Good (G) if the overall rating was at least 70%, Fair (F) if rating was at least 50% and poor (P) if the rating was less than 50% . The table assists in identifying the key characteristics of each study included in this review, with quality of life in patients with hypertension theme.
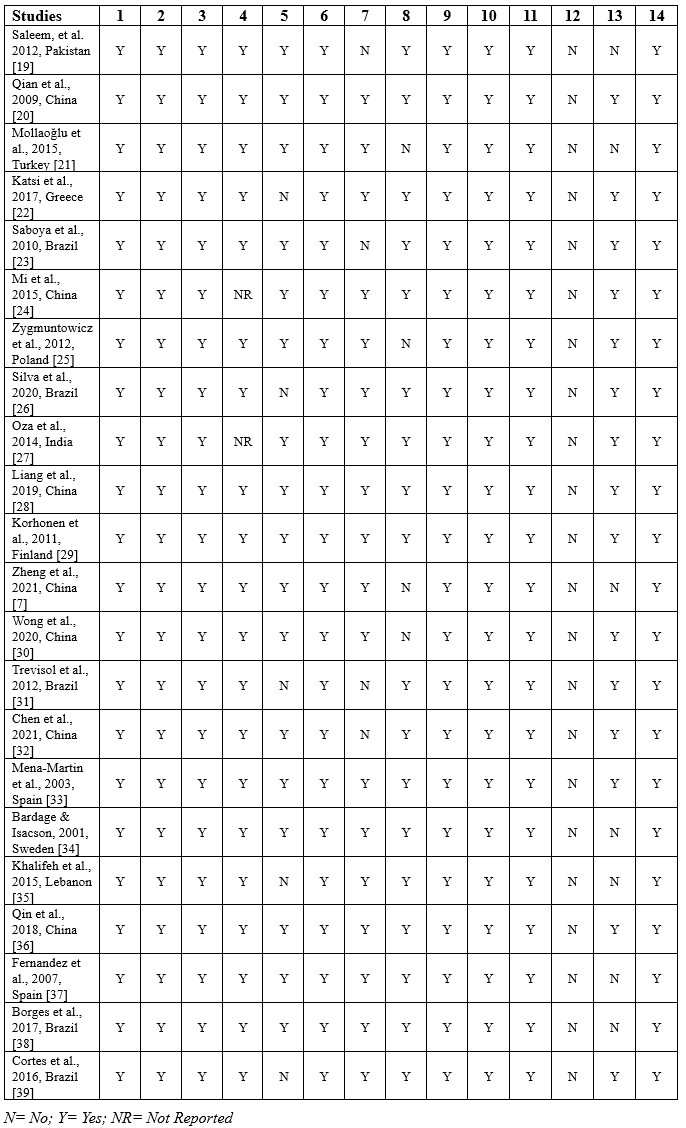
Table 2. Summary of quality assessment
RESULTS
Search Results
Combining the output of the searches in the various databases, a total of 2,287,348 references were found. After duplicates were removed, 1,918,891 potentially relevant references remained from the database searches. 1,918,854 articles removed by reasons of irrelevant, review/report, not full text, book chapter. 22 articles were finally designated as articles to be reviewed. The main focus of this integrative review is the evaluation of quality of life assessment tools used in hypertensive patients.
The authors developed tables for data analysis with the study design, participants characteristics including the number, assessment tools used, domain of measurements, measurement method, and the main results of Quality of Life assessment tools. PRISMA flow chart for study selection, can be seen in figure 1.

Figure 1. PRISMA flowchart for Study selection
Characteristics of the studies
The studies included in this review are from several countries globally, including China (n=7), Brazil (n=5), and one study each in Pakitan, Turkey, Greece, Lebanon, Sweden, Spain, Finland, and India. The study design used mainly was cross-sectional, which focused on the relationship between hypertension and the quality of life. The assessment tools used vary, including WHOQoL-BREF, SF-36, SF-12, SF-8, MINICHAL, and PECVEC. Several studies used a control group to compare the quality of life of people with hypertension with people who did not suffer from hypertension. Self-reported and face-to-face interviews measure the quality of life through a questionnaire format. Several studies included in this review also did not determine the degree of hypertension which was the inclusion criteria in the study conducted. Overall, 140 mmHg for systolic blood pressure is the standard for patients with hypertension.
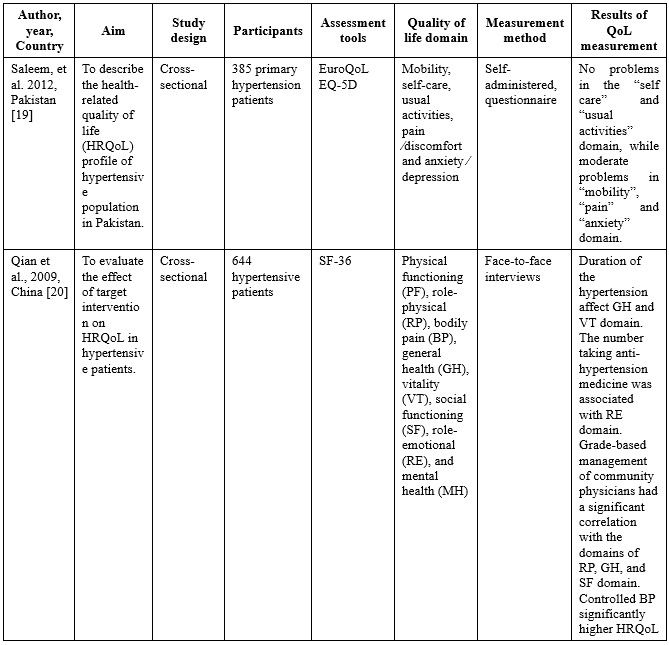
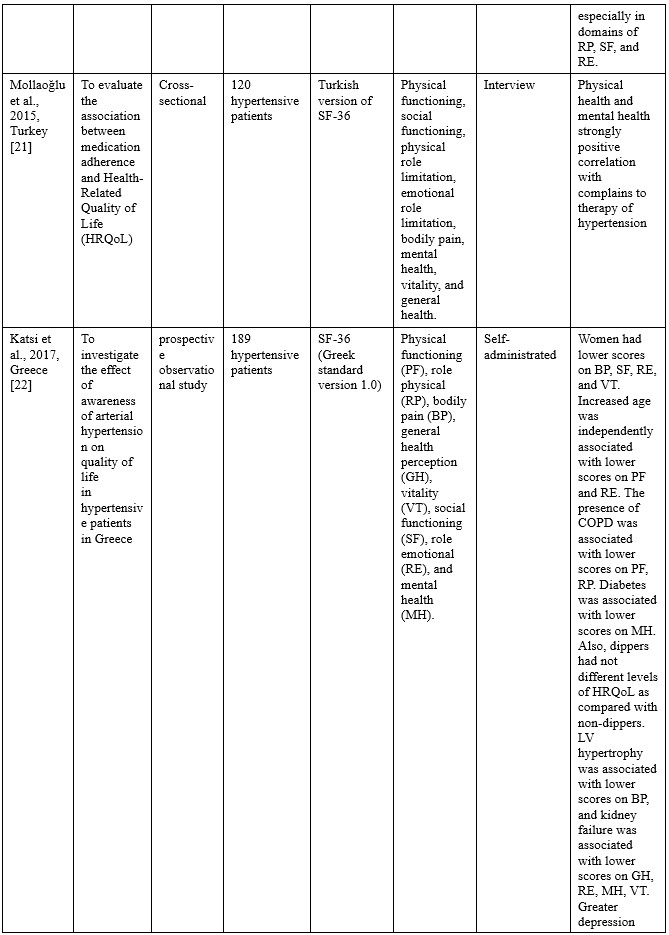
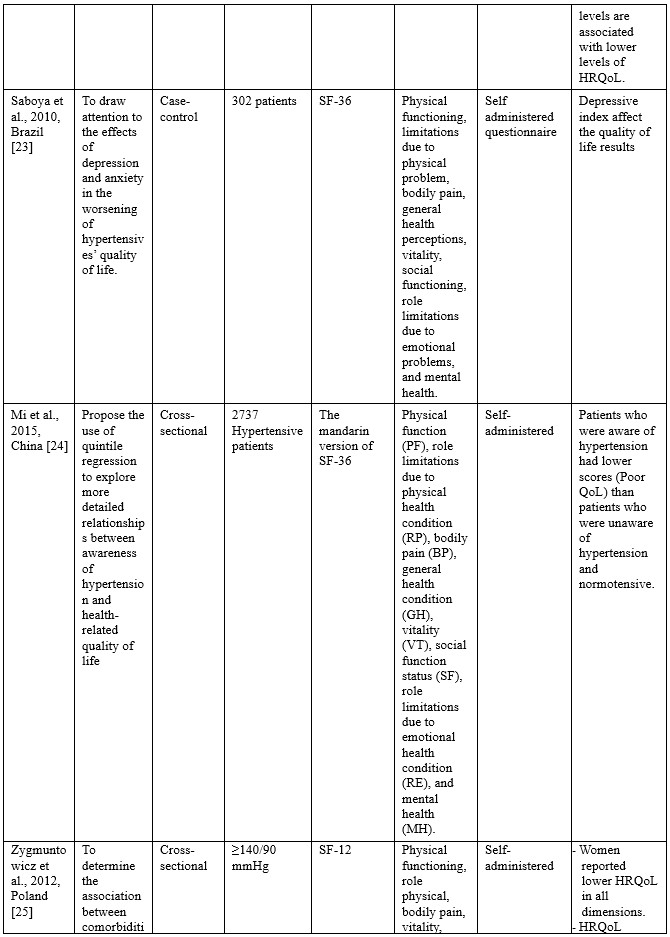
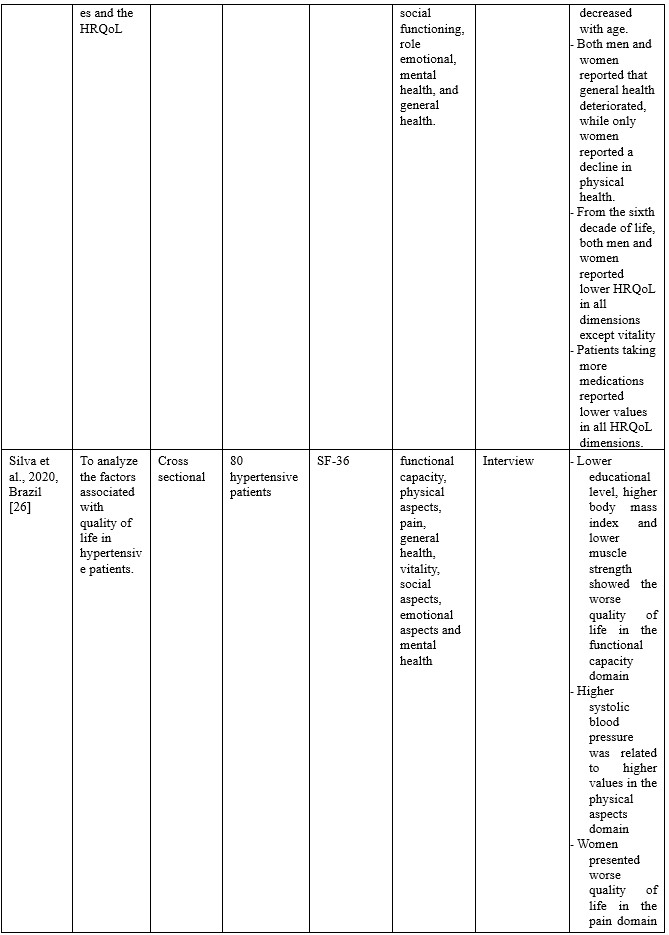
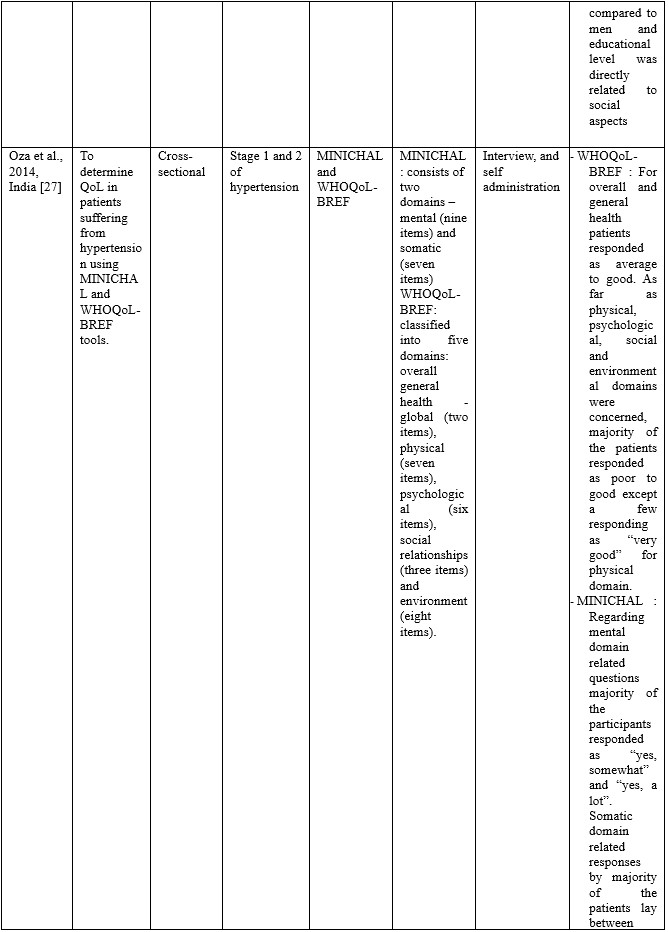
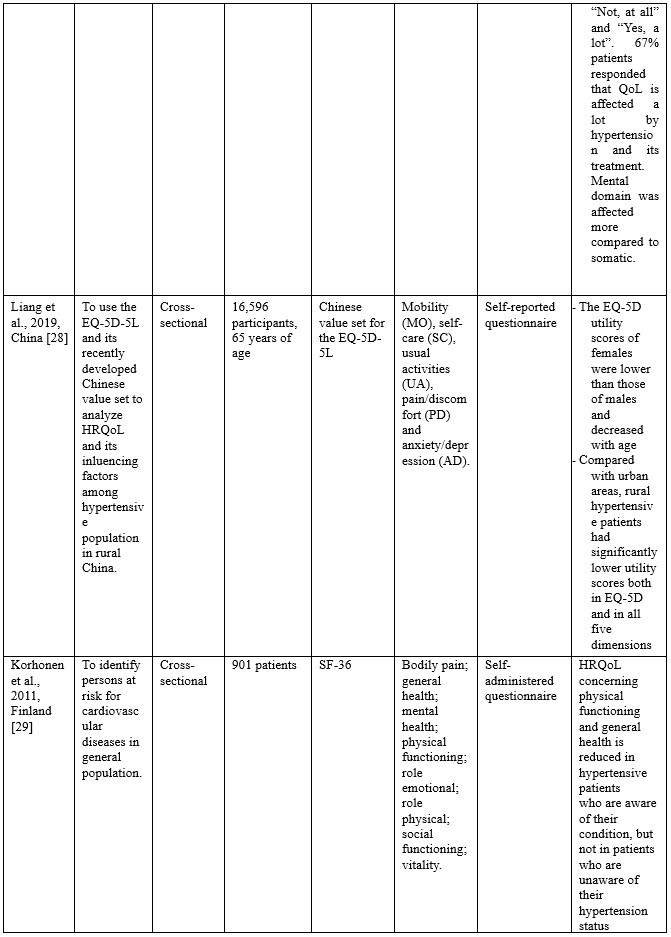

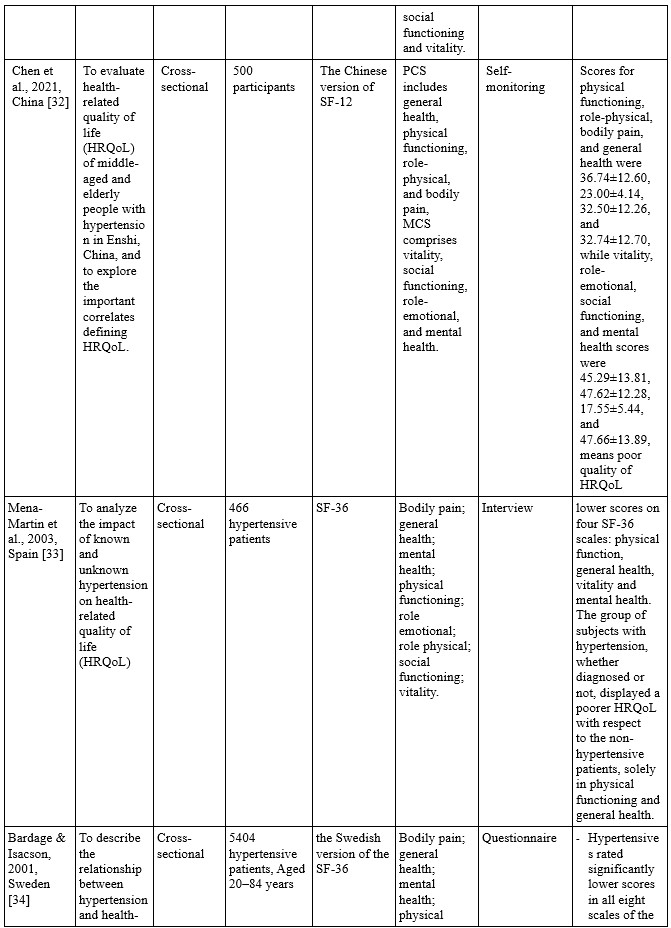
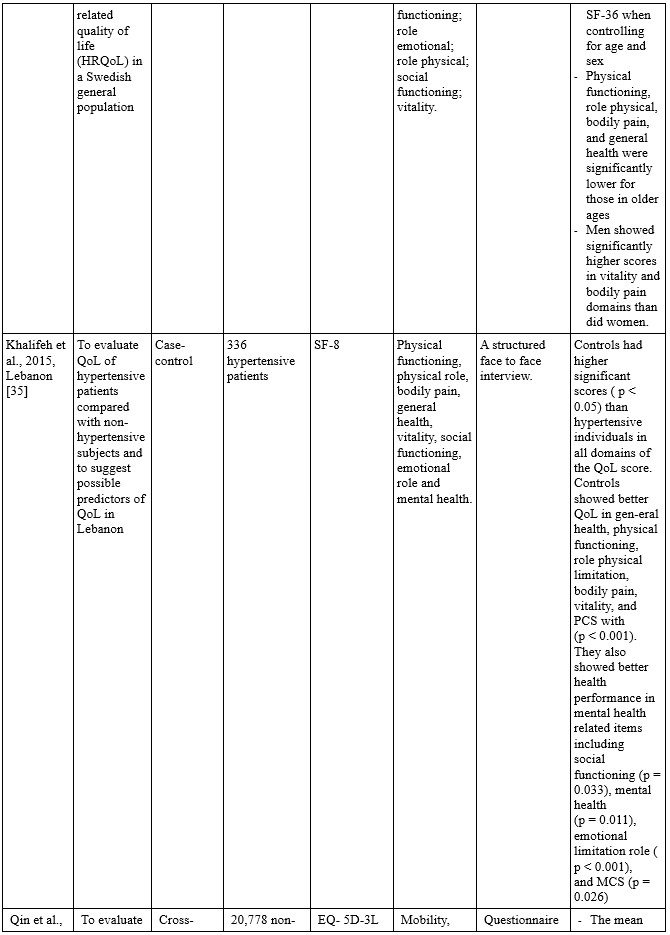
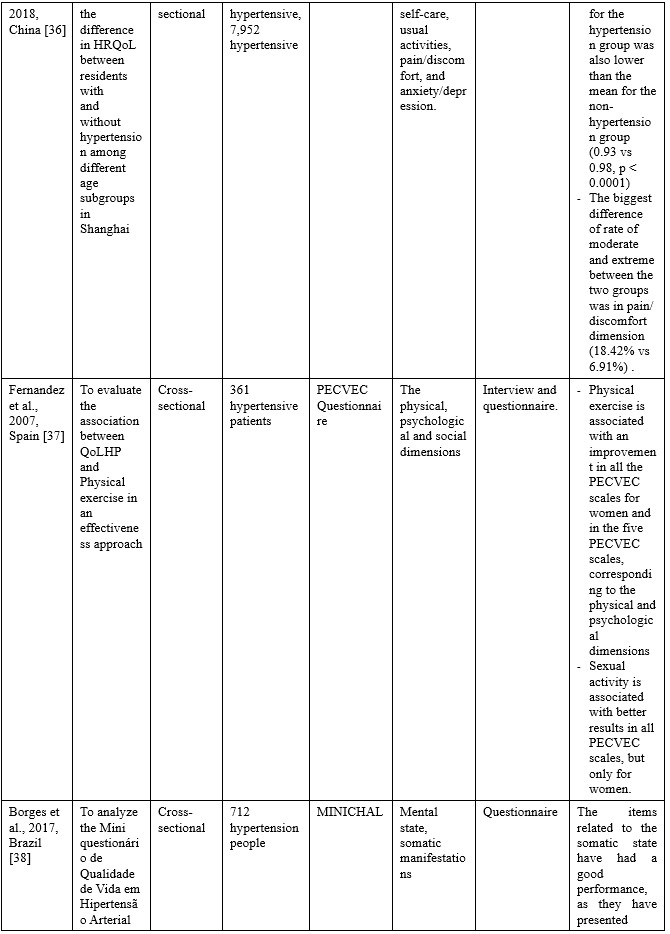

Table 3. Characteristics of the studies included
Quality of Life Domains
Based on the assessment tool used, the assessment domains for hypertension sufferers include general health, physical, psychological, social relationship, and environment (WHOQoL-BREF), mobility, self-care, usual activities, pain/discomfort, and anxiety/depression (EuroQoL EQ 5D), Physical functioning, role physical, bodily pain, general health, vitality, social functioning, role emotional, and mental health (SF-36, SF-12, SF-8), mental, and somatic (MINICHAL), the physical, psychological, and social dimensions (PECVEC). Most studies conducted in non-English countries translate the assessment items into the language of each country to make it easier for participants to answer the question items in each assessment tool.
QoL measurement results
In general, the assessment results of the quality of life in patients with hypertension on all the assessment tools used show a low score, which means the quality of life is low. The results of the quality of life assessment based on each assessment tool can be described as follows:
In studies using the 5D EQ, the problems found in the quality of life domain include mobility, pain, anxiety [19], while other studies indicate a decrease in scores in all domains in the 5D EQ [7,28,30]. Meanwhile, for the study conducted by Qin et al. [36], which compared the quality of life between patients with hypertension and those without hypertension, it was found that only the pain/discomfort dimension showed a very significant difference in scores.
In the studies using SF-36, -12, and -8, it was found that the duration of suffering from hypertension affected general health and vitality dimensions. The amount of consumption of antihypertensive drugs is related to the role emotional dimension, and controlled blood pressure has a significantly better effect on the quality of life, especially in the domains of role-physical, social functioning, and role emotional [20]. One study revealed that physical health and mental health domains had a strong positive influence on adherence to hypertension therapy [21]. Studies in Greece revealed that women had lower BP, SF, RE, and VT scores. Increased age was independently associated with lower scores on PF and RE [22,25]. Saboya et al. [23] found that the depression index affects the quality of life outcomes. One study in China revealed that patients who were aware of hypertension had lower scores (Poor QoL) than patients who were unaware of hypertension and normotensive [24]. Lower educational level, higher body mass index, and lower muscle strength showed the worse quality of life in the functional capacity domain. Higher systolic blood pressure was related to higher values in the physical aspects domain. Women presented worse quality of life in the pain domain than men, and educational level was directly related to social aspects [26]. Decreases in physical functioning and general health scores occurred in hypertensive patients aware of their condition [29]. A study in Brazil found that patients with hypertension had a lower quality of life than normotensive participants in all measurement domains [31,32,34,35]. Another study in Spain noted that people with hypertension had a low quality of life, especially in physical function, general health, vitality, and mental health.
Another measurement used MINICHAL, which consists of two domains, namely mental state and somatic manifestations. Oza et al. [27] found that the mental domain had more impact than the somatic domain. Meanwhile, in a study in Brazil, it was found that women have a better quality of life compared to men in the mental state domain.
DISCUSSION
This integrative review was carried out as our first step in conducting future projects to measure the quality of life of people with hypertension. Differences in culture, race, economic situation, geographical location, and so on in the world underlie our thinking to explore the possibility of imbalances in the assessment tool used internationally and has been tested for validity. However, some of the literature in this study has modified the item assessment tool used primarily for language. We realize that it is not enough to generalize its reliability and feasibility, especially in Indonesia and other countries in the Asian continent, which has extreme contrasts in culture with countries on the continent of Europe, America, and others.
The WHOQoL-BREF is one of the most commonly used generic Quality of Life (QoL) questionnaire which was developed simultaneously across a broad range of member countries, assuring that it could be used more multi-culturally and multi-lingually than any other existing QoL tool. It emphasises subjective response rather than objective life condition, with assessment made over the preceding two weeks [25]. WHOQoL-BREF consists of four main domains including physical health, psychological, social relationship, and environment. The aspects included in these domains include the physical health domain consisting of Activities of daily living, Dependence on medicinal substances and medical aids, Energy and fatigue, Mobility, Pain and discomfort, Sleep and rest, and Work Capacity [40]. The psychological domain consists of Body image and appearance, Negative feelings, Positive feelings, Self-esteem, Spirituality / Religion / Personal beliefs, thinking, learning, memory, and concentration. The social relationship domain consists of Personal relationships, Social support, and Sexual activity. Domain environment consists of financial resources, Freedom, physical safety and security, health and social care: accessibility and quality, Home environment, Opportunities for acquiring new information and skills, Participation in and opportunities for recreation/leisure activities, Physical environment (pollution/noise/traffic/climate), and Transport [41,42].
The 3-level version of EQ-5D (EQ-5D-3L) was introduced in 1990 by the EuroQol Group. The EQ-5D-3L essentially consists of 2 pages: the EQ-5D descriptive system. The EQ-5D-3L descriptive system comprises the following five dimensions: mobility, self-care, usual activities, pain/discomfort and anxiety/depression. Each dimension has 3 levels: no problems, some problems, and extreme problems. The patient is asked to indicate his/her health state by ticking the box next to the most appropriate statement in each of the five dimensions. This decision results into a 1-digit number that expresses the level selected for that dimension. The digits for the five dimensions can be combined into a 5-digit number that describes the patient’s health state. The 5-level EQ-5D version (EQ-5D-5L) was introduced by the EuroQol Group in 2009 to improve the instrument’s sensitivity and to reduce ceiling effects, as compared to the EQ-5D-3L. The EQ-5D-5L essentially consists of 2 pages: the EQ-5D descriptive system. The descriptive system comprises five dimensions: mobility, self-care, usual activities, pain/discomfort and anxiety/depression. Each dimension has 5 levels: no problems, slight problems, moderate problems, severe problems and extreme problems. The patient is asked to indicate his/her health state by ticking the box next to the most appropriate statement in each of the five dimensions. This decision results in a 1-digit number that expresses the level selected for that dimension. The digits for the five dimensions can be combined into a 5-digit number that describes the patient’s health state [28,43,44].
The Short Form (SF) -36, -12, -8 is a health status profile originally designed to measure health status of patients and outcomes of patients. Health status could be compared between groups of patients by type of intervention, disease, or type of health insurance. The original target population was individuals living in the community. The SF-36 is used today in outpatient settings and with community-dwelling older adults. The 36 questions on the SF-36 are meant to reflect 8 domains of health, including physical functioning, physical role, pain, general health, vitality, social function, emotional role, and mental health. The categories of physical role and emotional role reflect performance at the activity and participation levels [45,46].
MINICHAL consists of the short version of Calidad de Vida em la Hipertensión Arterial (CHAL), developed and validated in Spain. This is a self-administered instrument comprised of 16 items divided into the Mental Status (1 to 10) and Somatic Manifestations (11 to 16) dimensions. The mental domain includes questions one to nine and score ranges from 0 to 27 points. The somatic domain includes questions 10 to 16 and score ranges from 0 to 21 points. Last question is related to the overall impact of hypertension on the QoL. The score scale is Likert scale with four possible answers (0 = No, not at all; 1 = yes, somewhat; 2 = yes, a lot; 3 = yes, very much). Total points range from 0 (best level of health) to 51 (worst level of health) [47,48].
PECVEC considers the physical, psychological and social dimensions of QoL. Patients performance and well-being are assessed in each dimension. The physical dimension is measured according to two scales: lists of symptoms (17 items) and physical functions (eight items). The psychological dimension is measured according to three scales: psychological function (eight items), positive state of mind (five items) and negative state of mind (eight items). The social dimension is measured according to two scales: social function (six items) and social well-being (five items). The items are Likert-scaled from 0 (worst) to 4 (best) [37,49].
Quality of life is a reflection of holistic aspects of human well-being. Holistic health care includes biological, psychological, sociological, and spiritual aspects, so to assess the quality of life of a person with hypertension, it is obligatory to fully represent the items from the holistic aspect of the assessment. Differences in culture, economic status, race, geographical situation make it difficult to generalize an assessment tool.
In the results of the QoL measurement, there are several differences in the problems that most bother hypertensive patients. Studies that measured QoL using the 5DEQ showed that the most disturbing domains were mobility, pain, and anxiety. However, in another study, the pain was the main difference between hypertensive and non-hypertensive patients. There are possible factors that play a role in influencing the 5DEQ score in patients with hypertension, as shown in a study in China in the community during the COVID 19 pandemic, where the most frequently reported problems were pain/discomfort, followed by anxiety/depression, and self-care were the least frequently reported problem. The study also revealed that Men were more likely to report problems in mobility than women. Meanwhile, the above 60 years group reported the most problems in mobility, usual activities, pain/discomfort, and anxiety/depression [50].
In the results of the QoL measurement, there are several differences in the problems that most bother hypertensive patients. Studies that measured QoL using the 5DEQ showed that the most disturbing domains were mobility, pain, and anxiety. However, in another study, the pain was the main difference between hypertensive and non-hypertensive patients. There are possible factors that play a role in influencing the 5DEQ score in patients with hypertension, as shown in a study in China in the community during the COVID 19 pandemic, where the most frequently reported problems were pain/discomfort, followed by anxiety/depression, and self-care were the least frequently reported problem. The study also revealed that Men were more likely to report problems in mobility than women. Meanwhile, the above 60 years group reported the most problems in mobility, usual activities, pain/discomfort, and anxiety/depression [50].
CONCLUSION
Overall, the existing assessment tools have been recognized for their validity and reliability. The SF-36 is the most frequently used assessment tool, because it is considered the easiest to use and in accordance with conditions in several regions of the world. However, this form is a general form that is not explicitly intended to assess the quality of life in hypertension only. Holistically, the existing assessment tools have not touched the spiritual domain, where this domain in some countries is an essential factor in daily life.
Limitations
Our main limitation is access to reputable databases, as this is our main barrier in all articles assessing hypertensive patients' quality of life using various tools. The results of this review is probably suitable only in Indonesia and some Asian countries which have similar cultural issue.
Acknowledgement
We would like to express our gratitude to all parties, particularly the dean of the medical college of Haluoleo University and the dean of Science and Technology College of Sembilanbelas November University.
Conflict of interest
There is no conflict of interest.
Authors’ contribution
All authors equally contributed to preparing this article.
REFERENCES
1. Sudayasa IP, Alifariki LO, Rahmawati, Hafizah I, Jamaludin, Milasari N, et al. Determinant juvenile blood pressure factors in coastal areas of Sampara district in Southeast Sulawesi. Enfermeria Clinica. 2020;30(Supplement 2):585-588. doi: 10.1016/j.enfcli.2019.07.167.
2. Susanty S, Sukurni S, Siagian HJ. Analisis Bibliometrik Penelitian Pengobatan Herbal Penderita Hipertensi di Indonesia Menggunakan VOS-Viewer. Jurnal Keperawatan Silampari. 2022;5(2):764–71.
3. Sari AP, Lubis R. Determinant of Hypertension, Obesity and Smoking on Stroke Events in Hospital Patients at Regional General Hospital of Rokan Hulu Riau District, 2018 (Epidemiology and Public Health). Britain International of Exact Sciences (BIoEx) Journal. 2020;2(1):384–9.
4. Bangu, Siagian,H.J,Alifariki,L.O T. Differences of sodium consumption pattern hypertension sufferer in coastal and highland communities in Wakatobi islands. revista bionatura. 2021;6(2).
5. Suzanne Oparil, Maria Czarina Acelajado, George L. Bakris, Dan R. Berlowitz R, Cífková, Anna F. Dominiczak, Guido Grassi, Jens Jordan, Neil R. Poulter A, Rodgers and PKW. Hypertension. Physiology & behavior. 2016;176(1):100–106.
6. Kurnianto A, Kurniadi Sunjaya D, Ruluwedrata Rinawan F, Hilmanto D. Prevalence of Hypertension and Its Associated Factors among Indonesian Adolescents. International Journal of Hypertension. 2020;2020.
7. Zheng E, Xu J, Xu J, Zeng X, Tan WJ, Li J, et al. Health-related quality of life and its influencing factors for elderly patients with hypertension: evidence from Heilongjiang Province, China. Frontiers in public health. 2021;9:176.
8. Xiao M, Zhang F, Xiao N, Bu X, Tang X, Long Q. Health-related quality of life of hypertension patients: a population-based cross-sectional study in Chongqing, China. International Journal of Environmental Research and Public Health. 2019;16(13):2348.
9. Susanti N, Siregar PA, Falefi R. Determinan kejadian hipertensi masyarakat pesisir berdasarkan kondisi sosio demografi dan konsumsi makan. Jurnal Ilmiah Kesehatan (JIKA). 2020;2(1):43–52.
10. Atan G. Relationship between demographic features, adherence to treatment and quality of life of hypertension patients in Turkey. International Journal of Caring Sciences. 2017;10(3):1624–32.
11. Eom A-Y. Influencing factors on health related to quality of life in hypertension patients. Journal of Korean Biological Nursing Science. 2009;11(2):136–42.
12. Xie Z, Liu K, Or C, Chen J, Yan M, Wang H. An examination of the socio-demographic correlates of patient adherence to self-management behaviors and the mediating roles of health attitudes and self-efficacy among patients with coexisting type 2 diabetes and hypertension. BMC Public Health. 2020;20(1):1–13.
13. Badia X, Roca-Cusachs À, Dalfó A, Gascón G, Abellán J, Lahoz R, et al. Validation of the short form of the Spanish Hypertension Quality of Life Questionnaire (MINICHAL). Clinical therapeutics. 2002;24(12):2137–54.
14. Bahari G, Scafide K, Krall J, Mallinson RK, Weinstein AA. Mediating role of self‐efficacy in the relationship between family social support and hypertension self‐care behaviours: A cross‐sectional study of Saudi men with hypertension. International journal of nursing practice. 2019;25(6):e12785.
15. Ye R, Liu K, Zhang Z, Gong S, Chen X. Health-related quality of life of hypertension in China: a systematic review and meta-analysis. Journal of Cardiovascular Medicine. 2018;19(8):430–8.
16. Zhang Y, Zhou Z, Gao J, Wang D, Zhang Q, Zhou Z, et al. Health-related quality of life and its influencing factors for patients with hypertension: evidence from the urban and rural areas of Shaanxi Province, China. BMC health services research. 2016;16(1):1–9.
17. Pequeno NPF, de Araújo Cabral NL, Marchioni DM, Lima SCVC, de Oliveira Lyra C. Quality of life assessment instruments for adults: a systematic review of population-based studies. Health and quality of life outcomes. 2020;18(1):1–13.
18. Moher D, Liberati A, Tetzlaff J, Altman DG, Altman D, Antes G, et al. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement (Chinese edition). Journal of Chinese Integrative Medicine. 2009;7(9):889–96.
19. Saleem F, Hassali MA, Shafie AA, Awad GA, Atif M, ul Haq N, et al. Does treatment adherence correlates with health related quality of life? Findings from a cross sectional study. BMC public health. 2012;12(1):1–7.
20. Qian Y, Zhang J, Lin Y, Dong M, Xu M, Qian Y, et al. A tailored target intervention on influence factors of quality of life in Chinese patients with hypertension. Clinical and Experimental Hypertension. 2009;31(1):71–82.
21. Mollaoğlu M, Solmaz G, Mollaoğlu M. Adherence to therapy and quality of life in hypertensive patients. Acta Clinica Croatica. 2015;54(4).
22. Katsi V, Kallistratos MS, Kontoangelos K, Sakkas P, Souliotis K, Tsioufis C, et al. Arterial hypertension and health-related quality of life. Frontiers in Psychiatry. 2017;8:270.
23. Saboya PP, Bodanese LC, Zimmermann PR, Gustavo A da S, Macagnan FE, Feoli AP, et al. Lifestyle intervention on metabolic syndrome and its impact on quality of life: a randomized controlled trial. Arquivos brasileiros de cardiologia. 2016;108:60–9.
24. Mi B, Dang S, Li Q, Zhao Y, Yang R, Wang D, et al. Association between awareness of hypertension and health-related quality of life in a cross-sectional population-based study in rural area of Northwest China. Medicine. 2015;94(29).
25. Zygmuntowicz M, Owczarek A, Elibol A, Olszanecka-Glinianowicz M, Chudek J. Blood pressure for optimal health-related quality of life in hypertensive patients. Journal of hypertension. 2013;31(4):830–9.
26. Silva GO, Andrade-Lima A, Germano-Soares AH, Lima-Junior D de, Rodrigues SLC, Ritti-Dias RM, et al. Factors Associated with Quality of Life in Patients with Systemic Arterial Hypertension. International Journal of Cardiovascular Sciences. 2020;33:133–42.
27. Oza BB, Patel BM, Malhotra SD, Patel VJ. Health related quality of life in hypertensive patients in a tertiary care teaching hospital. J Assoc Physicians India. 2014;62(10):22–9.
28. Liang Z, Zhang T, Lin T, Liu L, Wang B, Fu AZ, et al. Health-related quality of life among rural men and women with hypertension: assessment by the EQ-5D-5L in Jiangsu, China. Quality of Life Research. 2019;28(8):2069–80.
29. Korhonen PE, Kivelä S-L, Kautiainen H, Järvenpää S, Kantola I. Health-related quality of life and awareness of hypertension. Journal of hypertension. 2011;29(11):2070–4.
30. Wong ELY, Xu RH, Cheung AWL. Health-related quality of life in elderly people with hypertension and the estimation of minimally important difference using EQ-5D-5L in Hong Kong SAR, China. The European Journal of Health Economics. 2020;21(6):869–79.
31. Trevisol DJ, Moreira LB, Fuchs FD, Fuchs SC. Health-related quality of life is worse in individuals with hypertension under drug treatment: results of population-based study. Journal of human hypertension. 2012;26(6):374–80.
32. Chen Q, Ran L, Li M, Tan X. Health-related quality of life of middle-aged and elderly people with hypertension: A cross-sectional survey from a rural area in China. Plos one. 2021;16(2):e0246409.
33. Mena-Martin FJ, Martin-Escudero JC, Simal-Blanco F, Carretero-Ares JL, Arzua-Mouronte D, Herreros-Fernandez V. Health-related quality of life of subjects with known and unknown hypertension: results from the population-based Hortega study. Journal of hypertension. 2003;21(7):1283–9.
34. Bardage C, Isacson DGL. Hypertension and health-related quality of life: an epidemiological study in Sweden. Journal of clinical epidemiology. 2001;54(2):172–81.
35. Khalifeh M, Salameh P, Al Hajje A, Awada S, Rachidi S, Bawab W. Hypertension in the Lebanese adults: Impact on health related quality of life. Journal of epidemiology and global health. 2015;5(4):327–36.
36. Qin Y, Guo Y, Tang Y, Wu C, Zhang X, He Q, et al. Impact of hypertension on health-related quality of life among different age subgroups in Shanghai: the subpopulation treatment effect pattern plot analysis. Journal of human hypertension. 2019;33(1):78–86.
37. Cuevas Fernandez FJ, Marco Garcia MT, Rodriguez Alvarez C, Iglesias Giron MJ, Aguirre‐Jaime A. Is there an association between physical exercise and the quality of life of hypertensive patients? Scandinavian Journal of Medicine & Science in Sports. 2007;17(4):348–55.
38. Borges JWP, Moreira TMM, Schmitt J, Andrade DF de, Barbetta PA, Souza ACC de, et al. Measuring the quality of life in hypertension according to Item Response Theory. Revista de Saúde Pública. 2017;51.
39. de Souza Côrtes DC, Arantes AA, Mendonça APP, dos Santos Silva J. Quality of life and hypertension. International Journal of Cardiovascular Sciences. 2016;29(6):512–6.
40. Ganesh Kumar S, Majumdar A, Pavithra G. Quality of life (QOL) and its associated factors using WHOQOL-BREF among elderly in urban Puducherry, India. Journal of clinical and diagnostic research: JCDR. 2014;8(1):54.
41. Ha NT, Duy HT, Le NH, Khanal V, Moorin R. Quality of life among people living with hypertension in a rural Vietnam community. BMC public health. 2014;14(1):1–9.
42. Melchiors AC, Correr CJ, Pontarolo R, Santos F de O de S, Souza RA de P. Quality of life in hypertensive patients and concurrent validity of Minichal-Brazil. Arquivos Brasileiros de cardiologia. 2010;94(3):357–64.
43. Zhang L, Guo X, Zhang J, Chen X, Zhou C, Ge D, et al. Health-related quality of life among adults with and without hypertension: A population-based survey using EQ-5D in Shandong, China. Scientific reports. 2017;7(1):1–7.
44. Wong ELY, Xu RH, Cheung AWL. Health-related quality of life among patients with hypertension: population-based survey using EQ-5D-5L in Hong Kong SAR, China. BMJ open. 2019;9(9):e032544.
45. Côté I, Grégoire J-P, Moisan J, Chabot I. Quality of life in hypertension: the SF-12 compared to the SF-36. Journal of Population Therapeutics and Clinical Pharmacology. 2004;11(2).
46. Chua R, Keogh AM, Byth K, O’Loughlin A. Comparison and validation of three measures of quality of life in patients with pulmonary hypertension. Internal medicine journal. 2006;36(11):705–10.
47. Schulz RB, Rossignoli P, Correr CJ, Fernández-Llimós F, Toni PM de. Validation of the short form of the Spanish hypertension quality of life questionnaire (MINICHAL) for Portuguese (Brazil). Arquivos brasileiros de cardiologia. 2008;90:139–44.
48. Soutello ALS, Rodrigues RCM, Jannuzzi FF, São-João TM, Martinix GG, Nadruz Jr W, et al. Quality of life on arterial hypertension: Validity of known groups of MINICHAL. Arquivos Brasileiros de Cardiologia. 2015;104:299–307. doi: 10.5935/abc.20150009. Epub 2015 Feb 27. PMID: 25993593; PMCID: PMC4415866.
49. Fernández-López JA, Fernandez-Fidalgo M, Martin-Payo R, Rödel A. Job stress and quality of life of primary care health-workers: evidence of validity of the PECVEC questionnaire. Atencion Primaria. 2007;39(8):425–31.
50. Ping W, Zheng J, Niu X, Guo C, Zhang J, Yang H, Shi Y. Evaluation of health-related quality of life using EQ-5D in China during the COVID-19 pandemic. PLoS One. 2020 Jun 18;15(6):e0234850. doi: 10.1371/journal.pone.0234850. PMID: 32555642; PMCID: PMC7302485.
![]() This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
Music-based intervention in Covid-19 hospitalization: a perspective through Consolidated Framework for Implementation Research (CFIR)
Alessio Pesce1
1Department of internal Medicine, ASL2, Savona, Italy
Corresponding Author: Alessio Pesce, MSN, Local Health Authority (ASL2), Piazza Sandro Pertini n. 10, 17100 Savona, Italy, Email: al.pesce@asl2.liguria.it
https://orcid.org/0000-0003-2702-4101

Cita questo articolo
Abstract
COVID-19 patients survive in isolation with stringent measures of infection containment, leading to anxiety, fear, stress, loneliness, and depression. Music is recognized as useful to promote multiple health outcomes, including anxiolytic effects, pain-relieving, and relaxing effects that favour well-being and social interaction in healthcare settings. The Consolidated Framework for Implementation Research (CFIR) allows to implement music in hospital, restricting methodological weaknesses. The importance of exploring the in-patients’ preferences, usages, and feelings for COVID-19 before initiating a music-based intervention is crucial.
Keywords: Music-Therapy, Covid-19, Patient preference, Nursing
Introduction
Music represents an interdisciplinary topic, transversal to medicine and human sciences. It constitutes a non-pharmacological intervention aimed at multiple health outcomes, including anxiolytic effects, pain-relieving, and relaxing effects that promote well-being and social interaction in healthcare settings [1,2,3]. Music-based interventions, therefore, can also be used to relieve psycho-social need in COVID-19 patients [1]. Clinical observation has revealed that patients with COVID-19 may experience diarrhea, nausea, decreased appetite, rash, and other adverse reactions during antiviral treatments [1]. Similarly, hospitalized patients survive in isolation with stringent measures of infection containment, leading to anxiety, fear, stress, loneliness, and depression, even to the point of evoking obsessive thoughts; in severe cases these effects compromise prognoses impacting on mortality and adverse events. There is ample evidence of the need for interventions, with greater relevance on health determinants in the community and hospital context, such as loneliness and social isolation that are fundamental for anxiety and depression development. Furthermore, in percentage terms, loneliness is associated with a 50% increase in the risk of developing dementia and a 30% increase in the risk of heart disease and stroke [4]. Since the early 1900s, music has been used as a mean to improve the psychological well-being of people experiencing situations of isolation or detention; this area of interest is currently at the forefront of scientific research.
Discussion
Music is recognized as useful to promote social interactions and emotional regulation, strongly improving people well-being in a pandemic context [5]. To date, research protocols are available in the hypothesis that music can reduce anxiety, depression or improve quality of life in COVID-19 patients [6]. However, to provide scientific evidence, studies are needed to explore patients' perspectives and determine the effects of music-based intervention during hospitalization. Some authors [7] remark how essential is the compatibility between proposed music pieces and people's preferences, and how these may vary depending on expectations at a specific time, health conditions, or healthcare environment. A crucial aspect in music-based interventions is the proper selection of music pieces. Listening to specific types / genres of favorite music or sounds is likely to have an emotional impact based on patients' clinical condition. Systematic reviews show that patients' music background and listening habits were drastically underestimated, reported in only 7.7% of studies conducted [8]. In only about 25% of the studies, patient feedbacks on music interventions were explored [8]. In UK [9], a scientific framework was used to integrate music in hospital. Through the Consolidated Framework for Implementation Research (CFIR), a protocol has been developed to integrate the patient's preferred music into the care pathway by providing in-ear music players. The CFIR presents five domains that must be satisfied in order to support the implementation of the intervention. Domains include: Characteristics of intervention, Individuals involved, Outer and Inner setting and Implementation process [9].
The CFIR constructs starts from the evidence of efficacy in music-based intervention available in literature, proceeding through its feasibility analysis, considering socio-political, organizational and applicability domains in healthcare setting, through systematic surveys among patients and healthcare professionals. Carter et Al [9], applying CIFR, defined pre-recorded music-based intervention as easy to be implemented in the treatment protocol and sustainable in economic and training terms, through programming with a qualified music expert. Personality variables, cognitive-affective components [10] and the patient's clinical condition, especially respiratory system efficiency and symptom burden, show a close correlation with music preferences [7], stated even before COVID-19 disease. Therefore, the importance of exploring the in-patients’ preferences, usages, and feelings for COVID-19 before initiating a music-based intervention is crucial. This knowledge, would allow health and music professionals to personalize the intervention and to explore important correlations between habitual music preferences and attitudes than those experienced by the patient as result of proposed music listening. Studies uniquely states methodological weaknesses in music-based interventions [8,11]. There is a lack of scientific rigor in music selection, involvement of music experts, and objective reporting and description of the music pieces used [11]. Music, also, was rarely selected to achieve specific effects according to reference frameworks [8,11]. Patients often selected pieces without a scientific rationale, resulting a little directional effect. The opportunity to identify music mechanisms for action would allow researchers to advance beyond basic questions about efficacy and begin to answer questions about how, why, and for whom an intervention works [11].
The implementation of CFIR would also provide a new methodological approach in clinical practice, promoting a personalised music-based intervention, according to the needs of the institutional settings and the patient's preferences. Music promotes early weaning to invasive mechanical ventilation [12], social interaction [13], quality of life and sleep [14,15], mood and well-being in healing environment [16]; reducing procedural stress and the need for anxiolytic and sedative drugs [17,18]. Significant psycho-physical benefits, in condition of clinical stability or instability, represent important outcomes in COVID-19 hospitalization. Relaxation, distraction, entertainment and emotional support of listening to music, according to the patient's preferences through the CFIR framework, can also contribute, with scientific rationale, to cope loneliness, isolation, fear and psychopathological states resulting from COVID-19 disease.
Conflict of interest
The Author declare that there is no conflict of interest.
Funding
The author states that he has not obtained any funding or financial sponsors.
References
1. Hen X, Li H, Zheng X, Huang J. Effects of music therapy on COVID-19 patients' anxiety, depression, and life quality: A protocol for systematic review and meta-analysis. Medicine (Baltimore). 2021 ;100(26):e26419.
2. Bradt J, Dileo C, Myers-Coffman K, Biondo J. Music interventions for improving psychological and physical outcomes in people with cancer. Cochrane Database Syst Rev. 2021;10(10):CD006911.
3. Kakar E, Billar RJ, van Rosmalen J, Klimek M, Takkenberg JJM, Jeekel J. Music intervention to relieve anxiety and pain in adults undergoing cardiac surgery: a systematic review and meta-analysis. Open Heart. 2021;8(1):e001474.
4. Rico L., Caballero F., Martìn M., Cabello M., Ayuso-Mateos, Miret M. Association of loneliness with all-cause Mortality. A meta-analysis. PLoS One. 2018; 13(1):e0190033.
5. Cabedo-Mas A, Arriaga-Sanz C, Moliner-Miravet L. Uses and Perceptions of Music in Times of COVID-19: A Spanish Population Survey. Front Psychol. 2021; 11:606180.
6. Chen X, Li H, Zheng X, Huang J. Effects of music therapy on COVID-19 patients' anxiety, depression, and life quality: A protocol for systematic review and meta-analysis. Medicine (Baltimore). 2021 Jul 2;100(26):e26419.
7. Liwka A, Pilinski R, Przybyszowski M, Pieniazek M, Marciniak K, Wloch T, et al. The influence of asthma severity on patients' music preferences: Hints for music therapists. Complement Ther Clin Pract. 2018; 33:177-183.
8. Williams C, Hine T. An investigation into the use of recorded music as a surgical intervention: A systematic, critical review of methodologies used in recent adult controlled trials. Complement Ther Med. 2018; 37:110-126.
9. Carter JE, Pyati S, Kanach FA, Maxwell AMW, Belden CM, Shea CM, et al. Implementation of Perioperative Music Using the Consolidated Framework for Implementation Research. Anesth Analg. 2018; 127(3):623-631.
10. Greenberg DM, Baron-Cohen S, Stillwell DJ, Kosinski M, Rentfrow PJ. Musical Preferences are Linked to Cognitive Styles. PLoS One. 2015; 10(7):e0131151.
11. Robb SL, Hanson-Abromeit D, May L, Hernandez-Ruiz E, Allison M, Beloat A, et al. Reporting quality of music intervention research in healthcare: A systematic review. Complement Ther Med. 2018; 38:24-41.
12. Bradt J, Dileo C. Music interventions for mechanically ventilated patients. Cochrane Database Syst Rev. 2014;2014(12):CD006902.
13. Boster JB, Spitzley AM, Castle TW, Jewell AR, Corso CL, McCarthy JW. Music Improves Social and Participation Outcomes for Individuals With Communication Disorders: A Systematic Review. J Music Ther. 2021 Mar 16;58(1):12-42.
14. Bradt J, Dileo C, Myers-Coffman K, Biondo J. Music interventions for improving psychological and physical outcomes in people with cancer. Cochrane Database Syst Rev. 2021 Oct 12;10(10):CD006911.
15. Kakar E, Venema E, Jeekel J, Klimek M, van der Jagt M. Music intervention for sleep quality in critically ill and surgical patients: a meta-analysis. BMJ Open. 2021 May 10;11(5):e042510.
16. McCaffrey R. Music listening: its effects in creating a healing environment. J Psychosoc Nurs Ment Health Serv. 2008 Oct;46(10):39-44.
17. Walter S, Gruss S, Neidlinger J, Stross I, Hann A, Wagner M, et al. Evaluation of an Objective Measurement Tool for Stress Level Reduction by Individually Chosen Music During Colonoscopy-Results From the Study "ColoRelaxTone". Front Med (Lausanne). 2020 Sep 15;7:525.
18. Fu VX, Oomens P, Klimek M, Verhofstad MHJ, Jeekel J. The Effect of Perioperative Music on Medication Requirement and Hospital Length of Stay: A Meta-analysis. Ann Surg. 2020 Dec;272(6):961-972.
![]() This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
LEARNING MODEL METHODS EMOTIONAL DEMONSTRATION (EMO DEMO) IN PREVENTION OF NON-COMMUNICABLE DISEASES: QUASI-EXPERIMENTAL STUDY
Winda Triana*, Pahrur Razi, Ervon Veriza, Solihin Sayuti
Department of Health Promotion, Health Polytechnic of Ministry of Health Jambi, Indonesia
* Corresponding author: Winda Triana, Jl. Prof DR GA Siwabessy No.42, Buluran Kenali, Kec. Telanaipura, Kota Jambi, Jambi 36122Department of Midwifery, Health Polytechnic of Jambi, Indonesia.Orcid :https://orcid.org/0000-0003-0574-7915. Email: trianawinda146@gmail.com
Cita questo articolo
ABSTRACT
Background. The development of science and technology in the field of medicine encourages experts to always conduct research on various diseases, including one of them is the incidence of infectious diseases in order to overcome suffering and death due to these diseases.This study aimed to analyze the effectiveness of the emo demo method in increasing knowledge and skills about the prevention of non-communicable diseases.
Methods. This quasi-experimental study using two groups of pretest-posttest design involved 100 participants, whose data were collected using a questionnaire and tested using the Wilcoxon test.
Results. Both knowledge and skills variables show differences before and after the intervention of providing education, namely there is an increase in knowledge and skills to prevent non-communicable diseases. There are different mean values between pre-test and post-test knowledge and skills, meaning that mathematically indicates there are differences in knowledge and skills before and after Emo Demo.
Conclusion. The Demonstration Emotional Method learning model is effective in increasing students' knowledge and skills about preventing non-communicable diseases.
Keyword: Counseling, Learning, Student, Knowledge, Skill
INTRODUCTION
Addressing Non Communicable Disease (NCDs) is integral to the 2030 Agenda for Sustainable Development [1]. Sustainable Development Goal (SDG) target 3.4 calls for a one-third reduction in premature mortality from NCDs by 2030. Many other SDG 3 targets are important for NCDs. Achieving the NCD-related SDG 3 targets can deliver shared gains across the development agenda, given the multidirectional relationship between NCDs, poverty, inequalities, economic growth, climate action and other SDG goals and targets [2].
Globally, non-communicable diseases, including cardiovascular disease, accounted for greater than 70% of all deaths in 2017 [3]. Non-Communicable Disease (NCD) is a catastrophic disease with the highest cause of death in Indonesia [4,5]. The National Health Research and Development Agency shows an increase in the development of NCDs in Indonesia due to the NCD trend followed by a shift in disease patterns [6].
An unhealthy lifestyle causes the high prevalence of NCD in Indonesia. The shift in the condition of NCD disease is expected to have a significant impact on Indonesia's human resources and economy in 2030-2040. Indonesia will face a demographic bonus where the productive age is much higher than the non-productive age group [7].
A 2018 National Basic Health Research (Riskesdas) results show that 95.5% of Indonesians consume fewer vegetables and fruit. 33.5% of people lack physical activity, 29.3% of people of productive age smoke every day, 31% have central obesity, and 21.8% are obese adults [6]. Lifestyle changes should be made as early as possible as an investment in future health. Controlling risk factors must also be done as early as possible. People must have health awareness to know their body condition to make it easier to treat before too late[8].
Emotional Demonstration (Emo Demo) is a behaviour change communication strategy that uses the incorporation of Behavior Communication Change (BCC) and Behavior Communication Definition (BCD). BCC is an interactive process between individuals, groups, or communities to develop communication strategies to achieve positive behaviour change. BCD is a communication process which makes direct use of individual psychological constructs involving feelings, needs and thoughts. It is one of the methods that is being widespread and gaining attention[9–12].
The Global Alliance for Improved Nutrition (GAIN) is a Swiss-based foundation first launched at the United Nations Headquarters in 2002 to address nutrition issues. Indonesia encourages changes in feeding behaviour to prevent stunting in children through the Emo-Demo Program. The Emo-Demo targets one essential behaviour that we change: exclusive breastfeeding and a steady and balanced diet, healthy snacks and balanced, complementary foods, and washing hands with soap[13–15].
Developing an NCD prevention control model in the younger generation is very important so that they become productive, academically intelligent, and healthy. Avoiding healthy adolescents with NCD can be combined with efforts that have been carried out in the community. Through Integrated Development Post-NCD (IDP-NCD), prevention of NCD risk factors can be done as soon as possible so that the incidence of NCD in the community can be suppressed[7].
IDP-NCD risk factor surveillance has been carried out in every health centre in Jambi City (20 health centres). NCD risk factors found through the implementation of IDP in Jambi City have increased in the period 2016 to 2019. The NCD risk factors are smoking, lack of physical activity, fewer vegetables and fruit, and being overweight[16]. Based on the 2019 annual report, the five most prominent diseases at the Jambi City Health Center were hypertension at 47.42%, the most aged >59 years (19,223) cases. Diabetes Mellitus by 20%, Myalgia by 20%, Coronary Heart disease by 2.8%, and an increase in the age of 45-59 years with 1,528 cases[16].
The Simpang IV Sipin Health Center is one of the Telanaipura District Health Centers, Jambi City, with the results of risk factor screening at the NCDIDP in 2019 of 15.34%. This value is far from the MSS target of 100%. NCDIDP is a part of Community Based Health Efforts (UKBM). The target population aged 15-59 in 2019 in 21,935 people in the Telanaipura District Health Center Work Area. SMAN 5 is located in the work area of the Simpang IV Sipin Health Center, with 1200 students, where the senior high school age is in the range of 15 years and over. This high school age is very vulnerable to early disease if there is no early detection and regular monitoring is in the risk factor category. NCD includes smoking, consumption of alcoholic beverages, unhealthy eating patterns, and lack of physical activity, obesity, stress, hypertension, hyperglycemia, and hypercholesterolemia.
Considering the impact of the emergence of NCD, it is necessary to establish an NCD IDP and Utilize IDP with the emo demo method. It is hoped that with the formation of IDP-NCD volunteers in SMAN 5, all students will be interested in using IDP-NCD through the Emotional Demonstration Method Learning Model in Prevention of Non-Communicable Diseases at IDP NCD SMAN 5 Jambi City.
METHODS
Trial design
This research is a quasi-experimental study using two groups of pretest-posttest design
Participants
This study involved 100 participants, who were carried out in September-October 2020 at SMAN 5 (High school) Jambi City, involving high school students who were randomly selected with the inclusion criteria of students who had never received health education about non-communicable disease emodemos; grade Fourth, Fifth, and Lower Sixth, while students who were sick during the study were not included in the study.
Intervention
The research variables are students' knowledge and skills. Before the intervention was given, the researcher first measured the level of knowledge and skills of the students/participants (pre-test). After being given the intervention, the researcher again measured the level of knowledge and skills of the students/participants (post-test). In this study, the intervention model given is the emotional demonstration learning model (emo demo) which is carried out once with a duration of 1 hour, which is 45 minutes of material delivery and 15 minutes of discussion). In this study, the researchers provided an explanation of non-communicable diseases to participants, accompanied by games about pictures and stickers of people with non-communicable diseases. the next step is for participants to try to explain about the pictures and stickers they get.
The knowledge and skills questionnaire consists of 22 questions with right and wrong answer choices. If the student answers correctly, he is given a score of 1, and if the answer is wrong, he is given a score of 0. The range of scores obtained is between 0-22. Both questionnaires use the Guttman scale. Meanwhile, students' skills were measured using a questionnaire consisting of 8 questions with right and wrong answer choices. If the mother answered correctly, she was given a score of 1, and if the answer was wrong, she was given a score of 0. The range of scores obtained was between 0-8. Both questionnaires use the Guttman scale.
The Guttman scale has an important characteristic, which is that it is a cumulative scale and measures only one dimension of a multi-dimensional variable, so that this scale has an undimensional nature. The data obtained are in the form of interval data or dichotomy ratios (two alternatives) [17].
Researchers have worked as lecturers and researchers between 10-15 years and have academic degrees Masteral Degree and Doctorate. Researchers have done much research in the health sector and have compiled many questionnaires, so the researchers have prepared the questionnaires in this study. Before the research was conducted, the questionnaire was piloted on ten students, and the results showed that two questions had to be replaced because they were invalid. The knowledge questionnaire contains the respondent's understanding of non-communicable diseases ranging from understanding, to overcoming them, while the skills questionnaire contains activities carried out in detecting and preventing non-communicable diseases.
Outcomes
This study compares the knowledge and skills of students in preventing the incidence of non-communicable diseases after being given an intervention in the form of an emo demo.
Sample size
This study involved 100 participants who were taken randomly using simple random sampling technique and sourced from three high school classes, namely grades Fourth, Fifth, and Lower Sixth.
Ethical Consideration
No economic incentives were offered or provided for participation in this study. In this study, because the subject was still a minor so the researcher had asked for and obtained parental consent so that their child could participate in the study. The study was performed in accordance with the ethical considerations of the Helsinki Declaration. This study obtained ethical feasibility under the Health Research Ethics Commission of the Ministry of Health, Jambi, and registration number: LB.02.06/2/153/2020.
Statistical analysis
Data are presented as numbers and percentages for categorical variables. Continuous data were expressed as mean ± standard deviation (SD) or median with Interquartile Range (IQR). Then proceed with bivariate analysis using the Wilcoxon test. The Wilcoxon test was used to determine the effect of the emo demo intervention on knowledge and skills. All tests with p-value (p)<0.05 were considered significant. Statistical analysis was performed using the SPSS version 16.0 application.
RESULTS
The characteristics of respondents in this study include age, gender and class level. The following is the frequency distribution of the respondents' characteristics in this study:
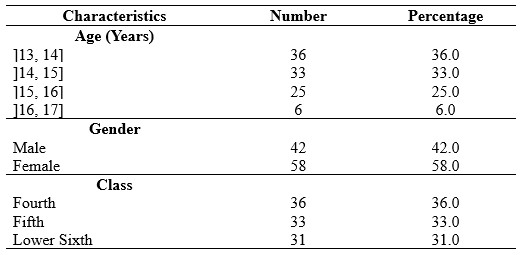
Table 1. Frequency Distribution of Respondents Characteristics
In Table 1 it is known that respondents in this study were female dominant as much as 58%, the most age was ]13, 14] years as much as 36% and the students came from class Fourth dominant.
Students' knowledge before being given the Emotional Demonstration Method learning model in the prevention of non-communicable diseases, is presented in table 2.
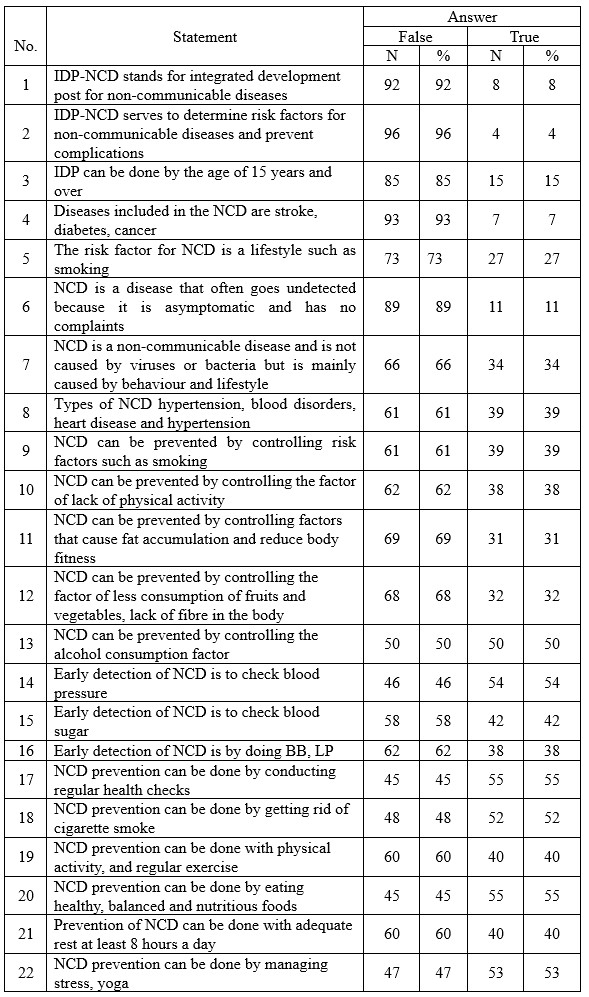
Table 2. Distribution of Respondents based on students' knowledge before being given the Emotional Demonstration Method learning model in the prevention of NCD
Table 2 shows that 92% did not know the abbreviation of IDP, 93% did not know what diseases were included in NCD 96%, students did not know the function of IDP, 89% of students did not know the symptoms of NCD.
Knowledge after being given the Demonstration Emotional Method learning model about prevention of non-communicable diseases at IDP-NCD SMAN 5 Jambi City, can be seen in table 3.
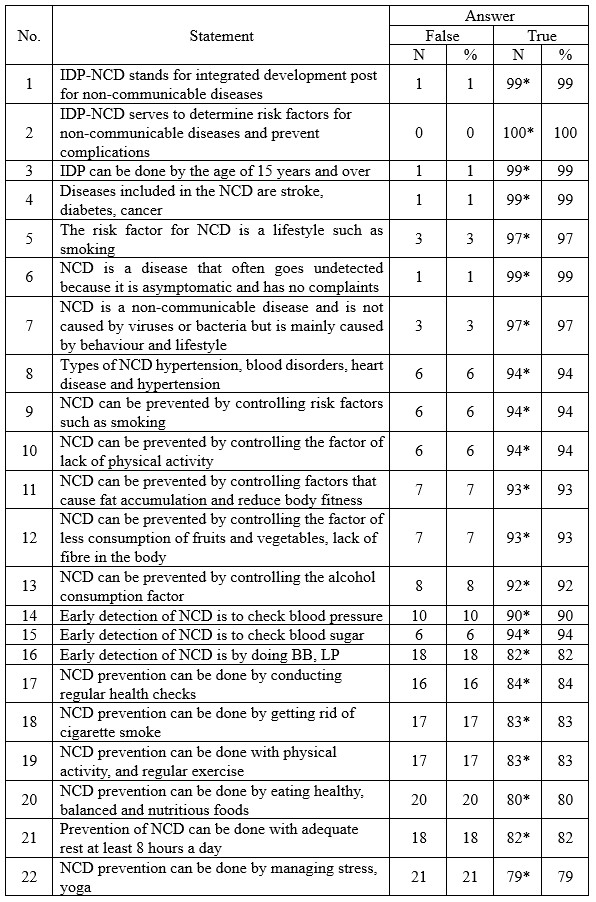
Description: an asterisk (*) is the correct answer
Table 3. Distribution of respondents based on knowledge after being given the Emotional Demonstration Method learning model in the prevention of non-communicable diseases
Table 3 shows that there are 100% of respondents who answered correctly about the function of the NCD IDP, 99% answered TRUE that IDP can be done aged 15 years and over, and 99% answered TRUE that the types of diseases included in the NCD are stroke, diabetes, cancer, 97% answered It is true that NCD is a non-communicable disease and is not caused by viruses or bacteria, but is caused more by behaviour and lifestyle.
Skills before being given the Emotional Demonstration Method learning model in preventing non-communicable diseases at IDP NCD SMAN 5 Jambi City in 2021 can be seen in table 4.
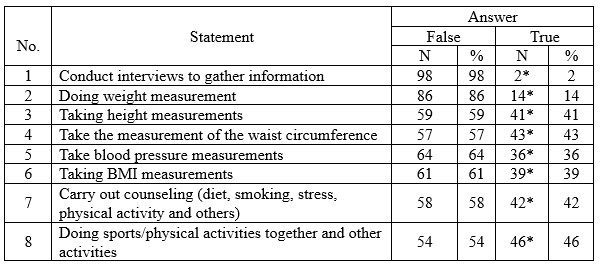
Description: an asterisk (*) is the correct answer
Table 4. Distribution of Respondents based on student skills before being given the Emotional Demonstration Method learning model in the prevention of non-communicable diseases
Table 4 shows that 98% did not conduct interviews to gather information, 86% did not weigh weight, 64%, and 61% did not measure BMI.
Skills after being given the Emotional Demonstration Method learning model in preventing non-communicable diseases at IDP NCD SMAN 5 Jambi City in 2021, can be seen in table 5,
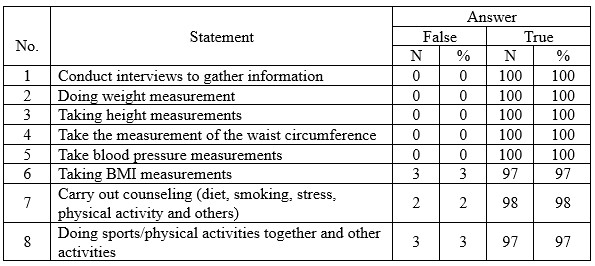
Table 5. Distribution of Respondents based on student skills after being given the Emotional Demonstration Method learning model in the prevention of non-communicable diseases
Table 5 shows that 100% of them were able to conduct interviews to dig up information, weigh weight, measure height, measure abdominal circumference, and measure blood pressure.
Table 6 shows that the Kolmogorov Smirnov statistical test results obtained a significant value of knowledge and skills both at the pre-test and post-test Emo Demo, each less than 0.05.
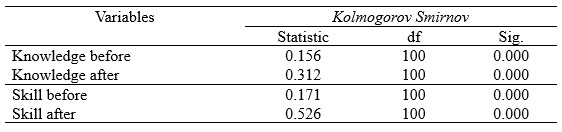
Table 6. Normality Test Results of Knowledge and Skills pre test and post test Emo Demo
The knowledge and skills data at the pre-test and post-test Emo Demo are not normally distributed. Therefore, the statistical difference test was tested using Wilcoxon (table 7).
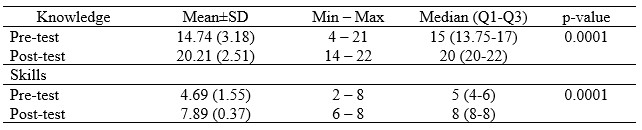
Table 7. Average Knowledge and Skills Pre and Post-test Emo Demo
Table 7 shows that there are different mean values between pre-test and post-test knowledge and skills, meaning that mathematically indicates there are differences in knowledge and skills before and after Emo Demo.
DISCUSSION
Based on the study results, it was known that the participant's level of knowledge and skills regarding the prevention of non-communicable diseases was deficient prior to the intervention. It may be influenced by the low level of education and material on non-communicable diseases that are not included in the high school education curriculum.
The success of health education for school-age children is determined by the selection of educational methods following the characteristics of school-age children and the factors that will be influenced as a result of the education carried out [10,12,13].
Change can only happen in response to something new, exciting and fun. Health education methods usually used tend to instil knowledge before forming new behaviours. The emo demo method was carried out as an intervention using the behavioural-centred design (BCD) approach. This approach seeks to include psychological elements as innovations to change individual behaviour. The combination of science and creativity in the preparation of messages makes this method able to transfer behaviour change messages that are more readily accepted by the target [14,15,18].
In line with previous research by Padila [19] at Aisyiyah 1 Kindergarten, Bengkulu City, it was found that before the intervention was given, most of them received a one-star category as many as 27 people (90%), while the number of respondents after the intervention mostly experienced an increase in ability and received a four-star category, totaled 23 people (76.7%). Similarly, Aisyah's research [20] at Al Kautsar Integrated Kindergarten, Mojokerto, Indonesia, found a change in knowledge after receiving material through demonstration media (emo demo) on washing hands in 7 steps.
The results of this study reject the null hypothesis regarding the effect of the emotional demonstration method on how to prevent non-communicable diseases by school students. The results of this study are in line with Aisyah's research [20] which states that the emo demo method improves children's knowledge, behaviour, and habits to wash their hands properly and correctly. Fermi Avissa [21] also found that the demonstration method improved the knowledge and skills of handwashing in preschool children at TK Flamboyan Platuk Surabaya.
Another study aims to apply the Emo Demo education method in reinforcing the mother's intentions and actions in providing vegetable and fruit menus for the family. The results showed an increase in the intention of homemakers in the intervention group by 6.8 points with a p-value = 0.003, while in the control group, the opposite occurred in the form of a decrease in score by 6.8 (p = 0.229)[12].
Emo Demo is a highly participatory activity guide that aims to convey a simple message in a fun and emotional way, thus making it memorable and impactful compared to other conventional behaviour change strategies [4,11,22].
Emo Demo connects three crucial components in learning: allowing people to learn firsthand through experimentation, providing information, involving other parts of the brain, and touching emotions. In addition, the delivery of the Emo Demo is carried out using teaching aids to make the Emo Demo easy to remember and the message conveyed is accurate so that the message is more easily absorbed and the target is willing to try new behaviours [4,14,15,23].
Giving lessons to students through the emotional demonstration method is considered effective in increasing students' knowledge and skills. Through this method, students are given education by delivering material accompanied by animated videos. After that, students can do direct practice on ways to control non-communicable diseases. Such as measuring blood pressure, weighing weight and height, carrying out counselling, exercising together and others so that the lesson material is memorable in students' memories and hard to forget. It is proven that the dominant skills of students after being given skills lessons, it is seen that almost 100 students get a score of 100.
In general, the study results found that the knowledge and skills of respondents increased after the intervention. However, some respondents did not change after receiving education through emo demos and video media. It might be due to their poor memory.
CONCLUSION
The Demonstration Emotional Method learning model is effective in increasing students' knowledge and skills about preventing non-communicable diseases.
LIMITATION
The limitations of this study include the minimal number of samples, and this study only involved one country, namely Indonesia, so the results may be different when comparing the effects of emo demos and intervention videos on students in other countries or even in the European countries.
FUNDING STATEMENT
This research did not receive any specific grant from funding agencies in the public, commercial, or not for profit sectors.
CONFLICT OF INTEREST
The authors report no conflict of interest.
ACKNOWLEDGEMENT
We would like to thank the director of the Department of Health Promotion, Jambi Health Polytechnic for supporting this research.
AUTHOR CONTRIBUTIONS
WT and PR were responsible for the study conception and design; EV performed the data collection; PR and SS performed the data analysis; WT, PR, and SS were responsible for the drafting of the manuscript; WT and PR made critical revisions to the paper for important intellectual content.
REFERENCES
1. United Nation. Last accessed: 19 July 2022. [Internet]. 2015. Available from: https://www.un.org/ga/search/view_doc.asp?symbol=A/RES/70/1&Lang=E. Last accessed: 29 August 2022.
2. World Health Organization (WHO). Non-communicable disease prevention and control: a guidance note for Investment cases [Internet]. 2019. Available from: https://apps.who.int/iris/bitstream/handle/10665/311180/WHO-NMH-NMA-19.95-eng.pdf. Last accessed: 29 August 2022.
3. Martinez R, Lloyd-Sherlock P, Soliz P, Ebrahim S, Vega E, Ordunez P, et al. Trends in premature avertable mortality from non-communicable diseases for 195 countries and territories, 1990–2017: a population-based study. The Lancet Global Health. 2020;8(4):e511–23.
4. Maryani H, Kristiana L, Paramita A, Andarwati P, Izza N. Pengelompokan Provinsi berdasarkan Penyakit Menular dan Penyakit Tidak Menular untuk Upaya Pengendalian Penyakit dengan Pendekatan Multidimensional Scaling (MDS). Buletin Penelitian Sistem Kesehatan. 2021;24(3):213–25.
5. Yarmaliza Y, Zakiyuddin Z. Pencegahan Dini terhadap Penyakit Tidak Menular (PTM) melalui GERMAS. Jurnal Pengabdian Masyarakat Multidisiplin. 2019;2(3):168–75.
6. Kemenkes RI. Hasil utama RISKESDAS 2018 [Internet]. Kementerian Kesehatan Badan Penelitian dan Pengembangan Kesehatan. Jakarta; 2018. Available from: https://kesmas.kemkes.go.id/assets/upload/dir_519d41d8cd98f00/files/Hasil-riskesdas-2018_1274.pdf. Last accessed: 20 June 2022.
7. Kementerian Kesehatan. Profil Kesehatan Indonesia [Internet]. Jakarta: Depkes RI; 2021. Available from: https://pusdatin.kemkes.go.id/resources/download/pusdatin/profil-kesehatan-indonesia/Profil-Kesehatan-indonesia-2019.pdf. Last accessed: 19 July 2022.
8. Kemenkes Republik Indonesia. Profil Kesehatan Indonesia tahun 2020 [Internet]. Pusdatin. Jakarta; 2020. Available from: https://www.kemkes.go.id/downloads/resources/download/pusdatin/profil-kesehatan-indonesia/Profil-Kesehatan-Indonesia-Tahun-2020.pdf. Last accessed: 19 July 2022.
9. Amareta DI, Ardianto ET. Peningkatan praktik cuci tangan pakai sabun pada anak usia sekolah dengan metoda emo demo. Sanitasi: Jurnal Kesehatan Lingkungan. 2017;9(2):88–93.
10. Rosita A, Dahrizal D, Lestari W. Metode Emo Demo Meningkatkan Pengetahuan dan Sikap Cuci Tangan Pakai Sabun (CTPS) pada Anak Usia Sekolah. Jurnal Keperawatan Raflesia. 2021;3(2):11–22.
11. Amareta DI, Ardianto ET. Penyuluhan Kesehatan dengan Metode Emo Demo Efektif Meningkatkan Praktik CTPS di MI Al-Badri Kalisat Kabupaten Jember. Prosiding. 2017;
12. Suriah IF, Rachmat M, Arundhana AI. Strengthening the Intentions and Actions of the Mother in Preparing Vegetables and Fruit Menus through the Emotional Demonstration Method. Journal of Management Practices, Humanities and Social Sciences. 2018;2(2):42–8.
13. Triana W, Verza E, Razi P. The Effect of Emotional Demonstration Methods and Video Learning on Hand Washing on Knowledge and Skills of Housewives. NSC Nursing. 2022;1(2):13–27.
14. Nurmaningsih N, Nisa SH. The Effect of Nutrition Education With The Emotional Demonstration Method on Mother’s Awareness In Feeding Underweight Toddlers. Jambura Journal of Health Sciences and Research. 2021;3(2):241–9.
15. Olief Syafrudin R, Apriyatmoko R. Perbedaan Praktik Cuci Tangan Pakai Sabun Untuk Pencegahan Penyebaran Virus Corona Sebelum dan Sesudah Diberikan Pendidikan Kesehatan Dengan Metode Emotional Demonstration Pada Remaja di Kelurahan Ngempon Kecamatan Bergas. Universitas Ngudi Waluyo; 2021.
16. Dinkes Kota Jambi. Profil Kesehatan Kota Jambi [Internet]. Jambi; 2020. Available from: http://dinkes.jambiprov.go.id/all_profil_kesehatan. Last accessed: 19 July 2022.
17. Sugiyono. Metode Penelitian Kuantitatif, Kualitatif dan R&D. Bandung: PT Alfabet; 2016.
18. Rahmawati R. Pengembangan Intervensi Emotional Demostration Terhadap Perubahan Perilaku Pola Makan Remaja Di Kabupaten Gorontalo= Development Of Emotional Demonstration Interventions On Changes In Adolescent’s Eating Patterns At Gorontalo District. Universitas Hasanuddin; 2022.
19. Padila P, Andri J, Harsismanto J, Andrianto MB, Admaja RD. Pembelajaran Cuci Tangan Tujuh Langkah melalui Metode Demonstrasi pada Anak Usia Dini. Journal of Telenursing (JOTING). 2020;2(2):112–8.
20. Aisah N, Reza M, Psi S. Meningkatkan Kemampuan Mencuci Tangan Melalui Metode Demonstrasi pada Kelompok B di TK Unggulan Terpadu Al Kautsar Mojokerto. Online), 3(3): 1-8, diakses pada tanggal 2 Januari 2018. 2014;3(3):1–8.
21. Avissa F, Nursalam N, Ulfiana E. Efektivitas Pendidikan Kesehatan Metode Demonstrasi Dan Metode Ceramah Dengan Media Booklet Terhadap Perubahan Pengetahuan Dan Tindakan Mencuci Tangan Pada Anak Prasekolah. Fundamental and Management Nursing Journal. 2012;1(1):59–66.
22. Ermawati I, Yuliana W, Hakim B. Pengaruh Metode Emotional Demonstration Terhadap Peningkatan Cakupan Penimbangan Balita Di Posyandu. Journal of Health Sciences. 2020;13(2):165–71.
23. Muyassaroh Y, Fatmayanti A. Pengaruh Permainan Emo-Demo ATIKA (Ati, Telur, Ikan) Terhadap Pengetahuan, Sikap dan Tingkah laku Pencegahan Anemia Pada Ibu Hamil. Jurnal Ilmu Keperawatan dan Kebidanan. 2021;12(2):222–8.
![]() This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
RELATIONSHIP OF KNOWLEDGE, DEFECATION BEHAVIOR AND FLY DENSITY WITH INCIDENCE OF DIARRHEA ON CHILDREN: A CASE CONTROL STUDY
Suparmi Suparmi *, Rina Fauziah
Department of Sanitation, Health Polytechnic of Jambi, Indonesia
* Corresponding author: Suparmi, Jl. Dr. Tazar, Buluran Kenali, Kec. Telanaipura, Kota Jambi, Jambi 36361, Department of Sanitation, Health Polytechnic of Jambi, Indonesia. Orcid : https://orcid.org/ 0000-0002-0695-9496. Email: suparmi.poltekkes@gmail.com

Cita questo articolo
Abstract
Introduction: Diarrhea is a significant public health problem because it is the third major contributor to child morbidity and mortality in various countries, including Indonesia. This study aimed to determine the relationship between the density of flies in the geographic area, the knowledge of the mothers, their defecation behavior, and the presence of diarrhea in children in Jambi City, Indonesia
Materials and Methods: This type of research is a quantitative study with a case-control approach involving 76 children under five, namely 38 cases and 38 control groups. The research data were analyzed using the Odds Ratio test.
Results: Mothers who have less knowledge are 12 times more likely to have a toddler suffering from diarrhea than mothers who have good knowledge. Mothers with poor behavior in dealing with toddlers' defecation habits will have a 5 times greater risk of having a toddler with diarrhea problems; on the other hand, if mothers behave well in dealing with children's defecation problems, then the toddler will not be at risk of having diarrhea. The density of flies does not provide a significant risk for the incidence of diarrhea in infants.
Conclusion: the incidence of diarrhea in children under five in the Putri Ayu Public Health Center in Jambi City is influenced by low parental knowledge and bad defecation behavior
Keyword: Availability of latrines, Behavior, Knowledge, Diarrhea, Children
Introduction
Diarrhea is the expulsion of feces with increasing frequency (three times a day) and changes in the consistency to become soft or watery, with or without blood/mucus [1–5]. Diarrhea is also a public health problem in developing countries like Indonesia because of its high morbidity and mortality. Diarrhea is an endemic disease and a potentially extraordinary disease often associated with death [6–8]. Of all deaths of children under five due to diarrheal diseases, 78% occur in Africa and Southeast Asia [9,10]. In 2019 cases in Indonesia were 4,485,513 people with diarrhea services for toddlers 40%. In 2016, people with diarrhea of all ages served at health facilities amounted to 3,176,079 people, and in 2017 it increased to 4,274,790 people. In that year, there have been 21 outbreaks spread across 12 provinces and 17 districts/cities. In 2017, the coverage of services for children with diarrhea in Indonesia was 40.07%, with the highest being West Nusa Tenggara (96.94%) [11].
Diarrhea is a symptom of infection in the intestinal tract, which can be caused by various bacterial, viral and parasitic infections. Infection is spread through contaminated food and drink, or from person to person as a result of poor sanitation. Diarrhea is usually transmitted through food and drink contaminated with feces and vomit from people with diarrhea. Transmission of diarrhea can also be caused by the behavior of defecating in any place, not washing hands after defecating, not washing hands before and after eating [12–14].
The formation of behavior starts from the knowledge or information that has just been obtained. The individual must first know the benefits and advantages of the knowledge or information they get before adopting it in behavior. The more information obtained, the stronger a person's attitude will change. A person becomes healthy if his daily behavior is healthy and sound. Otherwise, if someone is sick, his daily behavior is wrong or unhealthy [15–17].
The relationship between fly density and the incidence of diarrhea is that the higher the density of flies, the higher the incidence of diarrhea. Transmission routes of the diarrheal disease include water and food, and mechanical arthropods [18].
Toddlers are an age group that is vulnerable to nutrition and prone to disease, especially infectious diseases, one of which is diarrhea. Diarrhea attacks many toddlers because their immune systems are weak, so they are very susceptible to viruses that cause diarrhea. Toddlers who suffer from diarrhea tend to be more at risk of becoming dehydrated quickly. This condition is hazardous and has a negative impact because it can inhibit child growth and development, which can reduce the quality of life [17,19,20].
The prevalence of diarrhea in children in Jambi Province in 2018 was around 7.7%. In 2016 from 11 districts/cities, the incidence of diarrhea in Jambi city has increased. The highest number of sufferers from 2014, as many as 10,491 cases. In 2015, as many as 15,429 cases compared to other districts/cities in Jambi Province, while the incidence of diarrhea was 1,005 cases in 2019 in the Putri Ayu Health Center Work Area, Jambi City [21].
Based on this phenomenon, conducted this study to determine the relationship between knowledge, public defecation behavior, and fly density with diarrhea incidence.
Methods
Design
This research is a quantitative research with a Case-Control study approach
Participants
This research was conducted in Legok Village, Jambi City, Indonesia. The research was carried out in January-April 2020, involving 76 mothers with a ratio of the number of cases and controls being 1:1; in this study, the number of case groups was 38 respondents, and the control group was 38 respondents with matching mothers education. The case group is mothers who have children suffering from diarrhea while in the control group are mothers who have children who do not suffer from diarrhea.
The minimum sample size required for this study was calculated using the G*Power program, considering effect size of 0.3, α-value of 0.05, power of 0.85, and sample group ratio of 1 [22].
The selection of research samples was carried out randomly with inclusion criteria such as mothers who have toddlers and mothers who have never been respondents in previous studies with the theme of diarrhea.
Intervention
In this study, there are three independent variables: mother's knowledge, fly density, and defecation behavior, with diarrhea incidence as the dependent variable. All questions in the study used a dichotomous scale so that the scale used was the Guttman scale [23].
The density of flies has the objective criteria of dense and less dense and was measured using a Guttman scale questionnaire with 10-item questions and a rating range of 0-10, if the respondent answered yes was given a score of 1 and the answer was not given a score of 0.
Defecation behavior variables have good objective criteria and are not measured using a Guttman scale questionnaire with 10-item questions and a rating range of 0-10, if the respondent answered yes was given a score of 1 and the answer was not given a score of 0.
Mother's knowledge has the objective criteria of dense and less dense and was measured using a Guttman scale questionnaire with 10-item questions and a rating range, if the respondent answered correctly was given a score of 1 and the wrong answer was given a score of 0. The incidence of diarrhea varies, but there are objective criteria for cases and controls, which are measured using a Guttman scale questionnaire.
The variable incidence of diarrhea has objective criteria for cases and controls measured using a Guttman scale questionnaire with 10 item questions with a rating range of 0-10, if the respondent answered yes was given a score of 1 and the answer was not given a score of 0.
Blinding
In this study, 2 enumerators were used to collect research data. The previous enumerators did not know the participants because they were students who had been trained by the researcher before collecting data.
Ethical Consideration
No economic incentives were offered or provided for participation in this study. Before carrying out data collection, the researcher first took care of ethical permission.
The authors state that this study followed all ethical clearance processes and was approved by the health research ethics committee of Jambi University, Faculty of Medicine and Health Sciences, and registration number: LB.03.02./3.5/121/2019.
Statistical analysis
Data were presented as numbers or percentages for categorical variables. Continuous data are expressed as the mean ± standard deviation (SD), or median with Interquartile Range (IQR). The Odds Ratio was used to evaluate significant differences of proportions or percentages between two groups. If the OR value is more than 1.0 then it is considered significant or the variable is considered a risk factor. Statistical analysis was performed using the SPSS version 16.0 application. All tests with p-value (p) < 0.05 were considered significant.
Results
The characteristics of the respondents in this study can be seen in table 1 below.

Table 1. Distribution of respondent characteristics
Table 1 shows that the age group of 26-30 years dominated the respondents as much as 76.3% in the case group. The elementary education level was 39.5%, the dominant working mother was 57.9%, and primiparas were 60.5%. While in the control group, the age group of 26-30 years dominated the respondents as much as 76.3%, the elementary education level was 39.5%, the dominant working mothers were 52.6%, and multiparas were 68.4%. In the case group, the median age of children was 59.5 while in the control group it was 52, and the frequency was almost the same.
Table 2 shows that mothers who have less knowledge are 12 times more likely to have a toddler suffering from diarrhea than mothers who have good knowledge.
Mothers with poor behavior in dealing with toddlers' defecation habits will have a 5 times greater risk of having a toddler with diarrhea problems; on the other hand, if mothers behave well in dealing with children's defecation problems, then the toddler will not be at risk of having diarrhea.
The density of flies does not provide a significant risk for the incidence of diarrhea in toddler.

Table 2. Frequency Distribution of Respondents Based on Research Variables
Discussion
This study aimed to determine the relationship between the density of flies in the geographic area, the knowledge of the mothers, their defecation behavior, and the presence of diarrhea in children in Jambi City, Indonesia. Knowledge results from 'knowing,' which occurs after people have sensed a particular object. Sensing occurs through the five human senses, namely the senses of sight, hearing, smell, taste, and touch. Most human knowledge is obtained through the eyes and ears [24]. Knowledge of cognition is an essential domain for forming one's actions (overt behavior). Based on experience and research, behavior based on knowledge will be more lasting than behavior that is not based on knowledge [25]. The results of statistical tests show that mothers who have less knowledge are 12 times more likely to have a toddler suffering from diarrhea than mothers who have good knowledge. The results of this study are in line with the results of research conducted by Hartati [26], namely there is a significant relationship between respondents' knowledge and the incidence of diarrhea with a p-value of 0.001. also in line with research conducted by Palancoi [18], namely there is a significant relationship between respondents' knowledge and the incidence of diarrhea with a p-value of 0.010.
Based on the data obtained, some respondents have a low level of knowledge about diarrhea. A mother tends to find it challenging to protect and prevent her toddler from transmitting diarrhea. This low knowledge of mothers is due to the lack of information or counseling provided by health workers, making it difficult to prevent and take action when a child has diarrhea. The author suggests that health workers at the Putri Ayu Health Center increase the socialization of maternal and child health books and counseling about diarrhea so that public knowledge about diarrhea increases. Defecation-prone mothers are five times less likely to have a toddler who has diarrhea than mothers who have normal bowel habits. The findings of this study are consistent with those of Ambar and Suci [27], who found a significant association between defecation behavior and the occurrence of diarrhea with a p-value of 0.002. From the data at the research location, it is known that there are respondents who have poor defecation behavior. The behavior of open defecation reflects a culture of public ignorance, which can be interpreted as an attitude of not caring about anything. In this case, the community does not care about the detrimental effects of open defecation on themselves and others. Clean and healthy living behavior has a close relationship with diarrhea incidence. The behavior of washing hands before eating, feeding the baby, and defecating is a factor in breaking the chain of transmission of diarrheal diseases.
Based on the author's observations, it is known that most of the sewerage facilities (latrines) in the research location do not meet the requirements, such as not having a septic tank. Family restrooms that do not meet the requirements cause environmental pollution, including soil pollution, water pollution, food contamination, and the breeding of flies. The author suggests changing the habit of open defecation (BAB) into clean and healthy living behavior (PHBS) and seeking latrines that meet sanitary requirements, among others, by having a septic tank and maintaining the cleanliness of the feces disposal site to avoid diarrhea. Flies are one type of nuisance insect and can be disease-transmitting insects to human health that can spread disease. The presence of flies in an area can be used to indicate that the area is not clean or hygienic [28]. One of the causes of diarrhea is the contamination of food and drink by bacteria carried by house flies. This fly is considered a nuisance because it perches in damp and dirty places, such as garbage. If microorganisms contaminate the food infested by house flies, bacteria, protozoa, eggs/larvae of worms, or even viruses that are carried and removed from the mouths of flies and, when eaten by humans, can cause diarrheal disease [17,29]. The eradication of flies affects the entire community. Garbage is linked to the emergence and reproduction of flies. Insecticides can also eradicate flies, albeit this is less effective. Keeping the house clean, not littering, utilizing sanitary latrines (water-sealed latrines), and leading a clean and healthy lifestyle are all actions that must be taken to remove flies [14]. The number of flies does not appear to be a substantial risk factor for diarrhea in toddlers. The findings of this study agree with those of Firmansyah [1], who found that there is no significant link between fly density and diarrhea incidence, with a P-value of 0.080. The findings of the field investigation revealed that some respondents had a high degree of fly density. The researchers saw a lot of waste surrounding the house, which was tossed haphazardly, resulting in the appearance of flies. The presence of a large number of flies might be caused by poor or unclean housing cleanliness. If the house is in the high category, flies will land wherever, including food and drinks that are not covered in the house, and there will be bacterial contamination from flies to food and drinks for toddlers, causing digestive system disorders and diarrhea in many toddlers. Because of their good understanding of food processing, such as covering food after cooking or washing hands before cooking, many of the respondents were aware of the dangers of flies as a cause of diarrhea.
Conclusion
The incidence of diarrhea in children under five in the Putri Ayu Public Health Center in Jambi City is influenced by low parental knowledge and bad defecation behavior. The author recommends that individuals pay attention to the cleanliness of their homes, particularly their rubbish, because flies are intimately associated to garbage because garbage serves as a breeding place for them. It is expected that the community will further improve clean and healthy living behavior, especially by taking steps to prevent diarrhea, such as washing hands after defecating and before eating with soap and seeking latrines that meet sanitation requirements. Sanitation requirements include having a septic tank and maintaining the cleanliness of the waste disposal site, and not getting used to defecating in the river.
Limitations
The limitation of this research is the number of samples is very limited and does not compare the variables studied in the community between countries, in the future research must be carried out involving a larger community with coverage between countries.
Acknowledgement
We would like to thank the director of the Department of Health Sanitasion, Jambi Health Polytechnic for supporting this research.
Funding statement
This research did not receive any specific grant from funding agencies in the public, commercial, or not for profit sectors.
Competing interests statement
There are no competing interests for this study.
Author’s Contributions
SP and RF were responsible for the study conception and design; performed the data collection; and performed the data analysis; were responsible for the drafting of the manuscript; SP made critical revisions to the paper for important intellectual content.
References
1. Aryandari KRP. Faktor-Faktor Risiko Kejadian Diare Akut Pada Anak Usia Dibawah Tiga Tahun: Studi Observasional Analitik di Rumah Sakit Islam Sultan Agung Semarang. Universitas Islam Sultan Agung; 2021.
2. Nurbaiti N, Priyadi P, Maksuk M. Faktor Risiko Kejadian Diare Pada Balita di Puskesmas Kabupaten Muara Enim. Jurnal Sanitasi Lingkungan. 2021;1(1):13–8.
3. Ningsi SW. Pola Spasiotemporal Dan Faktor Risiko Kejadian Diare Pada Balita di Indonesia. Universitas Hasanuddin; 2021.
4. Ethelberg S, Olesen B, Neimann J, Schiellerup P, Helms M, Jensen C, et al. Risk factors for diarrhea among children in an industrialized country. Epidemiology. 2006;24–30.
5. Arivia N, Ratnadi IGAA, Kartinawati KT. Faktor Risiko Tingginya Angka Kejadian Diare Pada Balita Di Puskesmas Kabupaten Gianyar, Bali. AMJ (Aesculapius Medical Journal). 2021;1(1):55–62.
6. Hanif DI, Martini S. The relationship between the density of flies and the management of livestock waste with the incidence of diarrhea in the community of dairy farmers in Pudak Kulon Village, Ponorogo, Indonesia. Journal of Public Health in Africa. 2019;10(s1).
7. Iryanto AA, Joko T, Raharjo M. Literature Review: Faktor Risiko Kejadian Diare Pada Balita Di Indonesia. Jurnal Kesehatan Lingkungan. 2021;11(1):1–7.
8. Farag TH, Faruque AS, Wu Y, Das SK, Hossain A, Ahmed S, et al. Housefly population density correlates with shigellosis among children in Mirzapur, Bangladesh: a time series analysis. PLoS neglected tropical diseases. 2013;7(6):e2280.
9. Cruvinel LB, Ayres H, Zapa DMB, Nicaretta JE, Couto LFM, Heller LM, et al. Prevalence and risk factors for agents causing diarrhea (Coronavirus, Rotavirus, Cryptosporidium spp., Eimeria spp., and nematodes helminthes) according to age in dairy calves from Brazil. Tropical Animal Health and Production. 2020;52(2):777–91.
10. Van Roon AM, Mercat M, van Schaik G, Nielen M, Graham DA, More SJ, et al. Quantification of risk factors for bovine viral diarrhea virus in cattle herds: a systematic search and meta-analysis of observational studies. Journal of dairy science. 2020;103(10):9446–63.
11. Kemenkes RI. Hasil utama RISKESDAS 2018 [Internet]. Kementerian Kesehatan Badan Penelitian dan Pengembangan Kesehatan. Jakarta; 2018. Available from: https://kesmas.kemkes.go.id/assets/upload/dir_519d41d8cd98f00/files/Hasil-riskesdas-2018_1274.pdf
12. Trisiyani G, Syukri M, Halim R, Islam F. Faktor Risiko Kejadian Diare pada Anak Usia 6-24 bulan di Kota Jambi. Jurnal Sehat Mandiri. 2021;16(2):158–69.
13. Heryanto E, Sarwoko S, Meliyanti F. Faktor Risiko Kejadian Diare Pada Balita Di Uptd Puskesmas Sukaraya Kabupaten Oku Tahun 2021. Indonesian Journal of Health and Medical. 2022;2(1):10–21.
14. Ganguly E, Sharma PK, Bunker CH. Prevalence and risk factors of diarrhea morbidity among under-five children in India: A systematic review and meta-analysis. Indian journal of child health. 2015;2(4):152.
15. Arvelo W, Kim A, Creek T, Legwaila K, Puhr N, Johnston S, et al. Case–control study to determine risk factors for diarrhea among children during a large outbreak in a country with a high prevalence of HIV infection. International Journal of Infectious Diseases. 2010;14(11):e1002–7.
16. Bai Y, Dai Y-C, Li J-D, Nie J, Chen Q, Wang H, et al. Acute diarrhea during army field exercise in southern China. World Journal of Gastroenterology. 2004;10(1):127.
17. Mehal JM, Esposito DH, Holman RC, Tate JE, Callinan LS, Parashar UD. Risk factors for diarrhea-associated infant mortality in the United States, 2005–2007. The Pediatric infectious disease journal. 2012;31(7):717–21.
18. Palancoi NA. Hubungan antara pengetahuan dan lingkungan dengan kejadian diare akut pada anak di Kelurahan Pabbundukang Kecamatan Pangkajene Kabupaten Pangkep. Jurnal Kesehatan. 2014;7(2).
19. Gulliksen SM, Jor E, Lie KI, Hamnes IS, Løken T, Åkerstedt J, et al. Enteropathogens and risk factors for diarrhea in Norwegian dairy calves. Journal of Dairy Science. 2009;92(10):5057–66.
20. Bahartha AS, AlEzzi JI. Risk factors of diarrhea in children under 5 years in Al-Mukalla, Yemen. Saudi medical journal. 2015;36(6):720.
21. Dinkes Kota Jambi. Profil Kesehatan Kota Jambi [Internet]. Jambi; 2020. Available from: http://dinkes.jambiprov.go.id/all_profil_kesehatan
22. Faul F, Erdfelder E, Lang A-G, Buchner A. G* Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behavior research methods. 2007;39(2):175–91.
23. Notoatmodjo. Metodologi Penelitian Kesehatan. Jakarta: Jakarta. CV.Rineka Cipta. Hal 145-149; 2012.
24. Altindag D, Cannonier C, Mocan N. The impact of education on health knowledge. Economics of Education Review. 2011;30(5):792–812.
25. Zagzebski L. What is knowledge? The Blackwell guide to epistemology. 2017;92–116.
26. Hartati S, Nurazila N. Faktor Yang Mempengaruhi Kejadian Diare Pada Balita Di Wilayah Kerja Puskesmas Rejosari Pekanbaru. Jurnal Endurance: Kajian Ilmiah Problema Kesehatan. 2018;3(2):400–7.
27. Winarti A, Nurmalasari S. Hubungan Perilaku Buang Air Besar (BAB) dengan Kejadian Diare di Desa Krajan Kecamatan Jatinom Kabupaten Klaten. INVOLUSI Jurnal Ilmu Kebidanan. 2016;7(12).
28. Firmansyah YW, Ramadhansyah MF, Fuadi MF, Nurjazuli N. Faktor-Faktor Yang Mempengaruhi Kejadian Diare Pada Balita: Sebuah Review. Bul Keslingmas. 2021;40(1):1–6.
29. George CM, Perin J, De Calani KJN, Norman WR, Perry H, Davis Jr TP, et al. Risk factors for diarrhea in children under five years of age residing in peri-urban communities in Cochabamba, Bolivia. The American journal of tropical medicine and hygiene. 2014;91(6):1190.
![]() This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
Nurses’ knowledge of Diagnostic-Therapeutic Care Pathways (DTCP): A cross-sectional study
Ubaldino Ubaldi1*, Valentina Accinno2, Margherita Ascione3, Concetta Pane4
- Department of Ageing, Neurological, Orthopaedic and Head and Neck Sciences C.E.M.I, IRCCS - Fondazione Policlinico Gemelli - Rome (Italy)
- Department of Women's and Children's Health Sciences and Public Health DH Clinical Pharmacology, IRCCS - Fondazione Policlinico Gemelli - Rome (Italy)
- Integrated Operative Unit Maternal and Childhood Coordination - ASL Napoli 3 SUD, Naples (Italy)
- Integrated Operative Unit Maternal and Childhood Coordination - ASL Napoli 3 SUD, Naples (Italy)
*Corresponding Author: Ubaldino Ubaldi, Clinical Nurse, IRCCS - Fondazione Policlinico Gemelli - Rome. Nurses Department of Ageing, Neurological, Orthopaedic and Head and Neck Sciences C.E.M.I

Cita questo articolo
ABSTRACT
Introduction: Management by processes and clinical care pathways are now fundamental and indispensable requirements for quality improvement in healthcare organisations. The basic idea is to design a system that allows for continuous improvement in the way in which the key player in healthcare, i.e. the patient, is managed. If this were to happen, the best experiences to date tell us, it would definitively improve outcomes, efficiency and appropriateness. Moreover, patients perceive and appreciate this difference, allowing health professionals to operate at their best.
Objective: To assess the knowledge and application of the DTCPs by the nursing staff.
Materials and methods: The cross-sectional study took place in the period between June and September 2019 at the Operative Units of digestive surgery, hepatobiliary surgery, breast surgery and gynaecological surgery of the “Fondazione Policlinico Gemelli IRCCS in Rome”. A questionnaire was administered only to permanent nurses.
Results: A total of 64 questionnaires were administered of which 27 were correctly completed (response rate 42.1%) and considered valid for analysis. The sample of respondents was predominantly female (74.07%), 81.48% held a Bachelor's degree and 40.74% held a Master's degree. 55.56% knew what DTCPs were, but there was no in-depth knowledge of them in the sample. In fact, 55.56% knew whether there were active DTCPs in their region; 7.41% that nurses cannot participate in DTCPs and only 11.11% that nurses cannot participate in the review of individual DTCPs, while 59.26% were aware of the professional figures involved in the drafting and review of DTCPs. 25.93% knew what the diagnostic phase was based on and 14.81% that there were no active memoranda of understanding with public or private facilities in the diagnostic phase. Finally, only 25.93% were aware that the user could not be used in the evaluation of the outcome.
Conclusions: Although the interviewees were familiar with clinical care pathways, for most of them there had never been active involvement, they agreed on user involvement instead.
Keywords: nursing care, clinical care pathways, patient safety, diagnostic-therapeutic care pathways
INTRODUCTION
The reorganisation of the hospital network (Ministerial Decree 70/2015) and the reorganisation of Primary Care (Law 189/2012 - Balduzzi Decree) have brought about a profound and structural change in patient care and treatment in the Italian National Health Service [1-2]. The reorganisation of Primary Care, with the establishment of the AFTs (Regional Functional Aggregations) and the UCCPs (Complex Units of Primary Care), has meant tackling the problem of chronicity, with patient care, according to the Chronic Care Model and the model of integrated and structured Clinical Networks. It is a process of structural change and as such entails the need for a new culture in the definition, management and verification of the process of taking care of chronic patients: all this represents the real 'Reform'. The operational tool for treating chronic patients and co-morbidities is the Diagnostic-Therapeutic Care Pathways (DTCPs), which therefore represent the lintel of the new system [3-4].
Clinical/healthcare pathways predefine an optimal scheme of the sequence of behaviours in relation to the diagnostic, therapeutic and care pathway to be activated in the face of a typical clinical situation, in order to maximise the effectiveness and efficiency of activities [5]. DTCPs represent multidisciplinary care management technologies that map activities in a healthcare pathway, which are now considered fundamental and indispensable requirements for improving the quality of healthcare organisations in accordance with the logic of clinical governance [6]. The aim is to increase the quality of care across the continuum, improving risk-adjusted patient outcomes, promoting patient safety, increasing user satisfaction and optimising the use of resources [7].
In the entirety of its definition, construction, implementation and monitoring phases, it makes it possible to structure and integrate activities and interventions involved in the active and global care of citizens presenting health problems through a process approach, in a multidisciplinary context and on different areas of intervention (hospital, region, etc.), making it possible to assess the appropriateness of the activities carried out with regard to the objectives, the reference recommendations (Guidelines, good practices) and available resources [8]. It also allows for a measurement of activities and a comparison of results with specific indicators, leading to an improvement in each intervention in terms of effectiveness and efficiency. The need to find a shared theoretical and operational reference on what is meant by 'diagnostic therapeutic care pathway' is common among those who, at different levels and with different roles, deal with the planning of healthcare and social-health services and for those who work in them [9-10] .
The organisation of care by DTCPs is indirectly referred to by the 'Gelli' Legislative Decree (No 24/2017), the aim of which is to improve the quality of the National Health System, seeking to do so also by acting on the pillar of appropriateness of healthcare intervention, in particular, Article 5 of the aforementioned law regulates the way in which the healthcare profession is exercised, obliging healthcare professionals (doctors, nurses, physiotherapists, etc.) to adhere to the use of official guidelines and good clinical care practices [11]. Hence the need to investigate nurses' knowledge of DTCPs.
Objective
Assessing nurses' knowledge and perceptions of DTCPs
MATERIALS AND METHODS
The cross-sectional study was conducted during June-September 2019 at the Operative Units of digestive surgery, hepatobiliary surgery, breast surgery and gynaecological surgery at the “Fondazione Policlinico Gemelli Istituto di Ricovero e Cura a Carattere Scientifico in Rome (IT)”. Authorisation was requested and obtained from SITRA (Servizio Infermieristico Tecnico Riabilitazione Aziendale - Company Rehabilitation Technical Nursing Service) to proceed with the administration of a questionnaire, filled out anonymously, to the nurses on duty in the above-mentioned operational units.
The distribution took place after an interview with the nursing coordinators, providing verbal information on the questionnaire and confirmation of the processing of the data in aggregate form, not resulting in any distribution by name. After the distribution of the questionnaires to the nurses in the operating units by the coordinators, the latter collected them and placed them in a single container, which was then returned to the authors of the study.
All nurses who took part in the study well understood and signed the consent form, in which the purpose of the study and the methodology of conducting it were explained, and the personal data processing form.
The questionnaire, created ad hoc, was structured after a thorough literature search and listed in Appendix A, after the references section. The questionnaire was validated on a sub-sample of 10 nurses from the investigated sample, i.e. the questionnaire was submitted to them twice, at a minimum time interval of three days, and the statistical correlation between the two sets of answers was assessed, using the two-proportion test, with the two answers being statistically correlated if p-value >0.05 (i.e. the answers given, particularly with regard to the DTCP, were consistent at two different time points).
The questionnaire consists of 21 multiple-choice items structured as follows:
- 5 items on biographical characteristics: years of service, assigned operational unit, gender, educational qualification, post basic training;
- 16 items on DTCPs: what is a DTCP; participation of nurses in DTCP training courses; existence of DTCPs in their region and which types; whether clinical audits are planned and how often and others.
Informed consent was signed by all patients included in this study and anonymity was guaranteed. No economic incentives were offered or provided for participation in this study. The study was performed following the ethical considerations of the Helsinki Declaration[12].
Inclusion and exclusion criteria
All nurses of both sexes with a permanent contract type, who speak and understand Italian well, were included in this study, while all nurses temporarily assigned by the cooperatives (fixed-term and/or temporary assignment) were excluded from the study. However, this is a sample study with probabilistic sample selection (the only common element of inclusion is the existence of an open-ended contract).
Statistical analysis
Data was presented as numbers or percentages for categorical variables. Continuous data is expressed as the mean ± standard deviation (SD), or median with Interquartile Range (IQR).
A binomial test was performed to compare two mutually exclusive proportions or percentages in groups. The chi square test and Fisher's exact test were performed to evaluate significant differences in proportions or percentages between two groups. Particularly Fisher’s exact test was used where the chi-square test was not appropriate. The multiple comparison chi-square tests were used to define significant differences between percentages. In this case, if the chi-square test was significant (α level: 0.05), the residual analysis with the Z-test was performed. All tests with p-value(p) <0.05 were considered significant. The statistical analysis was performed by Matlab statistical toolbox version 2008 (MathWorks, Natick, MA, USA).
RESULTS
A total of 64 questionnaires were administered, 13 in digestive surgery, 14 in hepatobiliary surgery, 21 in breast surgery and 16 in cancer surgery. Only 27 questionnaires (42.8%) were returned and completed. Specifically:
- digestive surgery, 13 questionnaires delivered, 5 returned completed (38.4%).
- general surgery - hepatobiliary, 14 questionnaires delivered, 9 returned completed (64.2%);
- retroperitoneal cancer surgery, 21 questionnaires delivered, 6 returned completed (28.5%);
- gynaecological oncology, 16 questionnaires delivered, 7 returned and completed (43.7%);
In Table 1 below, we have reported the characteristics of our sample of nurses

Table 1. Characteristics of the 27 subjects participating in this study Items 1-5 of the questionnaire
Table 1 shows that the sample has a length of service ranging from 11 to 20 years (44%), is predominantly female (74%) and holds a bachelor’s degree (81%), while 40.7% of the respondents hold a Master's degree.
Table 2 shows the interviewees' knowledge of the Diagnostic-Therapeutic Care Pathway (DTCP).


Table 2. Knowledge of the interviewees about the DTCP. Items 6-15 of the questionnaire. The correct answer is indicated in bold and with an asterisk.
Table 3 shows the interviewees’ knowledge of the DTCP Protocols.

Table 3. Knowledge of the interviewees about the DTCP Protocols. Items 16-18 of the questionnaire The correct answer is indicated in bold and with an asterisk.
Table 4 shows the monitoring associated with the DTCP
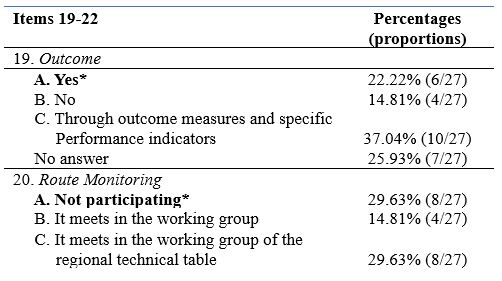

Table 4. Knowledge of the interviewees about the monitoring associated with the DTCP. Items 19-22 of the questionnaire The correct answer is indicated in bold and with an asterisk.
Finally, Table 5 shows all the statistical tests performed in this study


Table 5. Statistical tests performed in this study. Unanswered questions were not considered in the statistical analysis for each item. The correct answer in the questionnaire is indicated in bold
From Table 5, it can be seen that in our sample, there was no significant difference by seniority of service (p=0.368) and by medical area (p=0.730), while there was a significant presence of female gender (74.07%, p<0.0001) and of subjects with a Bachelor's degree (81.48%, p<0.0001). On the other hand, with regard to postgraduate education, subjects with a Master's degree were significantly more present (40.74%, p<0.0001), together with the option 'Other' (25.93%, p=0.0013).
With regard to knowledge of DTCP courses, the most frequent answer was Answer A: 'DTCP describes the pathway that a person with health problems takes between one or more health organisations and defines the best sequence of actions necessary to achieve the health objectives identified a priori' (55.56%, p<0.0001), whereas when asked about participation in DTCP courses, the answer 'No' was the significantly most frequent (74.08%, p<0.0001). Regarding knowledge of active DTCP courses in one's region, the most frequent answer was 'YES' (55.56%, p<0.0001).
When asked about knowledge of which DTCPs were active (Item 9) and of DTCPs for neurodegenerative diseases (Item 10), there was no significant difference between the answers.
In Item 11, concerning 'nurse participation', Answer C: 'partly' was the most frequent (55.56%, p<0.0001), similarly for Item 12 (Answer C: 70.37%, p<0.0001).
With regard to the clinical audit (Item 13), there was no significant difference between the various answers. In contrast, for audit cadence (Item 14), Answer D: '1/year' was the most frequent (55.56%, p<0.0001).
With regard to knowledge of published audits (Item 15), there was no significant difference between the various answers.
With regard to Item 16 (Other professional figures), the significantly more frequent answer was Answer C: 'all professional, rehabilitation medical figures provided in the multidisciplinary teams specific to that clinical condition' (59.26%, p<0.0001).
For Item 17 (DTCP phases), the most frequent answer was 'YES' (48.15%,p=0.0084). Similarly for Item 18 (SI: 51.85%, p<0.0001).
There was no significant difference between the responses associated with Items 19, 20 and 21, whereas for Item 22 (user involvement), the 'YES' response was the significantly more present (48.15%, p=0.0084),
DISCUSSION
The cross-sectional study was conducted with the aim of exploring and assessing the knowledge of DTCPs by nurses in service at the Fondazione Policlinico Gemelli (IRCCS) assigned to the Operative Units of digestive surgery, hepatobiliary surgery, breast surgery and gynaecological surgery through the administration of a questionnaire.
Almost half of the nurses interviewed to date, despite having completed a Bachelor's and a Master's degree, are not aware of the importance of DTCPs in terms of quality of care and the achievement of health outcomes: all organisations, including health care organisations, are composed of a series of processes or sets of actions, oriented towards creating value for those who know and use them [13]. It is likely that the study of Guidelines, Protocols, Procedures and DTCPs undertaken in the 1st year programme should also be taken up in the following years in the degree course, combining theory with practice.
Almost all of the nurses (74.08%), who participated in the study, were never involved in participating in the drafting of such pathways, without considering the importance of a broadly participatory approach of all components (management and technical-professional) of the organisation and the use of decision-support techniques (use of scientific evidence, audits between professionals) [14].
Healthcare institutions can use DTCPs and promote evidence-based practice to benefit quality and reduce costs [15]; however, research suggests that compliance with the use of DTCPs is low [16].
Another barrier could be resistance to the practice of change in working environments
[17], however with a proper implementation and evaluation process, change in healthcare is achievable [18].
The nurses' thoughts on user involvement are significant: in the light of these results, it can be stated that the attempt to introduce a multidisciplinary logic in healthcare organisations is hindered by the very peculiarity of the context, which is of a professional nature, in which management cannot impose itself on professionals, but must instead involve them. The task of management today is to succeed in creating those conditions that actively involve health professionals in spontaneously innovating clinical practice [19].
CONCLUSION
The implementation of DTCPs can offer the patient timely and real continuity of care, through the identification of qualified care and the integration of all professional figures. The study conducted included the assessment of nurses' knowledge on DTCPs. The results obtained show a gap in nurses' knowledge of DTCPs and this preliminary study provides several insights to improve the knowledge of DTCPs among nurses in order to ensure better continuity of patient care.
Strengths and Limitations of the study
The study has some limitations. In particular, the sample examined is a monocentric and small sample; a larger sample could have provided additional insights, reducing the possibility of statistical bias.
The study could be a preliminary step to a larger one including other operating units, not previously taken into account, so as to offer new insights given the importance of the topic for nurses.
Funding
This research did not receive any form of funding.
Conflict of interest
The authors declare that they have no conflicts of interest associated with this study.
REFERENCES
- Decreto Ministeriale 2 aprile 2015 n. 70 Regolamento recante definizione degli standard qualitativi, strutturali, tecnologici e quantitativi relativi all'assistenza ospedaliera. (G.U. 4 giugno 2015, n. 127)
- LEGGE 8 novembre 2012, n. 189Conversione in legge, con modificazioni, del decreto-legge 13 settembre 2012, n. 158, recante disposizioni urgenti per promuovere lo sviluppo del Paese mediante un piu' alto livello di tutela della salute. (12G0212) (GU n. 263 del 10-11-2012 - Suppl. Ordinario n. 201)
- Casati G., Panella M., Di Stanislao F., Gestione per processi professionali e percorsi assistenziali, terza edizione, Roma Ancona, Marzo 2005.
- Casati G., Vichi M.C., Il percorso assistenziale del paziente in ospedale, McGraw-Hill Companies SRL, Milano, 2002.
- Specchia M.L., Poscia A., Volpe M., Parente P., Capizzi S., Cambieri A., De Belvis A.G., Does Clinical Governance Influence the appropriateness of hospital stay? Bio Med Central Health Services Research, Aprile 2015.
- Broda et Al., Clinical Pathway: un metodo per il miglioramento della qualità in ambito ospedaliero, Scuola di Specializzazione di Igiene e Medicina Preventiva, Università di Torino.
- Janicek M., Casi clinici ed evidence – based medicine, Roma 2001.
- Atwal A., Caldwell K., Do multidisciplinary integrated care pathways improve interprofessional collaboration, Scandinavian Journal of Caring Sciences, 16(4):360-7,2002.
- Croce D., Sebastiano A., Castiglioni Rusconi M., Carenzi A., I PDT/PDTA nelle organizzazioni sanitarie: una meta-analisi della letteratura internazionale, economia e management “s.d” pp38-39 [online]Casati G., La gestione per processi in sanità, QA Vol 13. 1, (2002).
- Casati G., Vichi C. Il percorso assistenziale del paziente: partener di Sanità & Management Consulting Srl. Giornale di tecniche nefrologiche & dialitiche, anno XV n 2., S. Donato Milanese, Milano 2002.
- LEGGE 8 marzo 2017, n. 24 “Disposizioni in materia di sicurezza delle cure e della persona assistita, nonché in materia di responsabilità professionale degli esercenti le professioni sanitarie.” (17G00041) (GU Serie Generale n.64 del 17-03-2017)
- World Medical Association; “Dichiarazione di Helsinki della World MedicalAssociation: principi etici per la ricerca biomedica che coinvolge gli esseri umani”; 2013; Volume 5:Issue 10; e1000059
- ARESS (Agenzia Regionale per i Servizi Sanitari della Regione) Piemonte, Raccomandazioni per la costruzione dei PDTA e PIC nelle aziende sanitarie della Regione Piemonte, 2007
- Noto G, Raschetti R, Maggini M,. Gestione integrata e percorsi assistenziali. Roma: Il Pensiero Scientifico Editore. 2011
- Every N., Hochman J., Becker R., Kopecky S., & Cannon C. Critical pathways: A review. Circulation, 10, 461. 2000
- Kinsman, L. Clinical pathway compliance and quality improvement. Nursing Standard, 18, 33–35. 2004
- Seckel M., & Miller, K. Potential barriers to implementing practice alerts. AACN Reseach Work Group. 2005–2006
- Goudreau K. Notes from the board. Clinical Nurse Specialist, 20, 215–216. 2006.
- Kingston, M., Krumberger, J., & Peruzzi, W., Enhancing outcomes: Guidelines, standards, and protocols AACN Clinical Issues: Advanced Practice in Acute and Critical Care, 11, 363–374. 2000.
Appendix A
COGNITIVE QUESTIONNAIRE ON NURSES' PERCEPTIONS OF DTCPs.
Dear colleague,
We are two nurses who work at the Fondazione Policlinico Gemelli and we are conducting a cognitive survey, with the aim of surveying the knowledge of health workers on the subject of Diagnostic-Therapeutic Care Pathways.
We ask you to take a few minutes of your time to answer the questions in the questionnaire, assuring you that the results will be treated absolutely anonymously and used for statistical purposes only.
Thank you for your participation.
1. Years of service:
A. less than 10
B. 11-20
C. More than 20
2. In which area are you assigned?
A. critical area
B. medicine
C. surgery
D. Other......
3. Gender:
A. M
B. F
4. Basic qualification:
A. Qualifying title
B. University diploma
C. Bachelor's degree
5. Post-basic training (multiple answers possible)
A. Advanced training courses.....................................................
B. Master's degree (one or more) .............................................
C. Master's/Specialist Degree
D. Level II Master's degree (one or more).............................................
E. Other...........................
6. What is a Diagnostic-Therapeutic Care Pathway (DTCP)?
A. The DTCP describes the 'journey' that a person with health problems takes between one or morehealth organisations and defines the best sequence of actions necessary to achieve thehealth objectives identified a priori.
B. The DTCP is a set of guidelines, protocols and procedures
C. The DTCP is a structured pathway of healthcare acts
7. Have you ever participated in DTCP training courses?
A. Yes
B. No
C. I have never been contacted
8. Are there active DTCPs in your region?
A. Yes
B. No
C. In the planning stage for implementation
9. If you answered 'Yes' to the previous question, which one?
A. Single integrated rehabilitation pathway for the stroke patient
B. Pathway for the care and rehabilitation of patients with disorders of consciousness due to severe acquired brain injury
C. Diagnostic and therapeutic care pathway for chronic obstructive pulmonary disease
D. Definition of the pathway for early detection of suspected cases of DSA and indication for diagnosis and certification
E. Operational guidelines for the implementation in the regional network of social and health services and integrated pathways for adults with SLA
F. Operational guidelines for the prevention, diagnosis, treatment and care of people with dementia
G. Other DTCPs …………………………………………………………………………………………………………………………………………………………………
10. In your Regional Health Agency, have DTCPs been activated that may affect Neurodegenerative and Neurodevelopmental diseases?
A. Yes
B. No
C. They are in the planning stage
11. Does the professional figure of the nurse participate, and to what extent, in the drafting of the specific DTCP?
A. Yes
B. No
C. Partially
D. Participates in specific regional technical tables as a representative of the professional association
12. Does the nurse participate, and to what extent, in the review of individual DTCPs?
A. Yes
B. No
C. Only partially
13. Are clinical audits of individual DTCPs planned?
A. YES
B. NO
C. Partially
14. How often are specific audits planned for each DTCP?
A. One/month
B. One/every two months
C. One/semester
D. One/year
E. Other...
15. Are the DTCPs published on the company website or in the appropriate sections and therefore consultable by the various professionals?
A. YES
B. No
C. Only partially
16. What other professional figures are envisaged in the drafting/revision of individual DTCPs?
A. Only doctors
B. Only physiotherapists
C. All the professional, medical and rehabilitation figures foreseen in the multidisciplinary teams specific to that clinical condition
17. The DTCP envisages a Diagnostic phase and a Therapeutic-Assistance phase: are PACC, PIC and Day Service envisaged in the diagnostic phase?
A. Yes
B. No
18. Are memoranda of understanding currently in place with accredited public and/or private healthcare facilities in the Diagnostic phase?
A. Yes
B. No
C. Partially (please specify)………………………………………………….
19. In DTCPs, is the outcome used, and in what way, as a check on the effectiveness, efficiency, cost-effectiveness and appropriateness of the Pathway?
A. Yes
B. No
C. Through outcome measures and specific performance indicators set out in individual documents
20. To what extent does the nurse participate in pathway monitoring activities?
A. Not participating
B. Meetings in the working group
C. Meeting in the working group of the regional technical table
21. Are teleconsultation, telemonitoring and teleassistance activities provided for within the individual DTCPs?
A. Yes
B. No
C. In part (specify)………………………………………………….
22. Is user involvement in outcome assessment foreseen in the DTCPs?
A. Yes
B. No
Authorisation for data processing for statistical purposes consent
□ ………………………………………………………….
□ ………………………………………………………….
![]() This work is licensed under a Creative Commons
This work is licensed under a Creative Commons
Attribution-NonCommercial-NoDerivatives 4.0 International License.
THE IMPACT OF HEALTH EDUCATION ON KNOWLEDGE, ATTITUDE, PRACTICE, AND PREVENTION OF IRON DEFICIENCY ANEMIA AMONG ADOLESCENT FEMALES: A SYSTEMATIC REVIEW
Sarinah Siregar*1, Asni Johari2, Muhammad Rusdi2, Syahrial2
1Health Polytechnic, Jambi Ministry of Health, Jambi, Indonesia
2 Jambi University, Indonesia
Corresponding author: Sarinah Siregar, Prof DR GA Siwabessystreet, No.42, Buluran Kenali, Kec. Telanaipura, Kota Jambi, Jambi 36122, Phone :+62 813-6685-5307
Email: sarinah.siregar.poltekkes@gmail.com
Cita questo articolo
ABSTRACT
Introduction: Women in reproductive age are at high risk of iron deficiency anemia during the menstrual cycle. Adequate knowledge, attitudes, practices, and prevention towards anemia are necessary. There is a dearth of information on the evaluation of study characteristics and the overall quality of evidence of intervention studies in improving knowledge, attitudes and practices of anemia among adolescents.
Aim: The purpose of this study is to examine the impact of health education interventions on the knowledge, attitudes, practices, and prevention towards anemia in adolescent girls. Therefore, the review question are “What health education methods are best used to improve knowledge, attitudes, practices, and prevention of adolescent?”, “What is the effect of health education interventions on anemia in adolescent girls?”
Methods: This systematic review was conducted using the Preferred Reporting Items for Systematic Reviews and Meta-Analyses Protocols) Checklist whichinvolved studies published between 2000 to 2021 through the databases of PubMed, ScienceDirect, Willey online Library, Cochrane, in English version. Study quality assessed using the National Institutes of Health (NIH) on controlled intervention studies. The risk of bias of the studies included assessed using The Cochrane Risk of Bias Assessment Tool.Data of the studies included were synthesized thematically in order to understand the effectiveness of mobile application. At identification stage, there are 1,414 publications were discovered through backward searching of relevant papers. The full-text screening was conducted on 34 articles and the finding 22 articles failed to meet eligibility criteria at the full-text screening stage, and only 12 articles were finally eligible for further analysis. There are twelve studies included in this study, strengthening the components of health education and increasing Iron-Folic Acid (IFA) knowledge among adolescent girls is beneficial in reducing iron deficiency anemia in adolescent girls
Results: The results of the review article showed that health education interventions, giving iron supplements and multivitamins were effective in overcoming iron deficiency anemia in adolescent girls. Educational interventions also increase the knowledge of young women about iron deficiency anemia
Conclusions: Health Education intervention for the treatment of iron deficiency anemia among adolescent female improved their knowledge, attitude, practice,and prevention
Keywords: adolescent girl, health education, iron deficiency anemia, anemia
INTRODUCTION
Anemia is a medical complication in which the number and size of red blood cells, or the hemoglobin concentration, falls below the reference range. It has the potential consequence of impairing or reducing the capacity of the blood to transport oxygen throughout the body [1–3]. Anemia is resulting from both poor nutritional status and/or poor health condition. Globally the most significant cause of anaemia is iron-deficiency (ID). The onset of anemia secondary to iron deficiency is generally assumed to account 50% of anemia occurred in the world [4].
Women of reproductive age (adolescent girls) are at a high-risk group so that 25% of students suffer iron deficiency anemia during the menstrual cycle [5,6]. Because in a period of growth and development, they need iron every day is more than 3 times that of young men [7]. The results study by Gunatmaningsih [8] showed that respondents in a period of menstruating have 1.842 times greater risk of anemia, the duration of menstruation is a predictor of anemia [9]. Blood loss during menstruation can lead the iron deficiency anemia. The amount of blood lost during one menstrual period ranges from 20-25 cc, iron loss 12.5-15 mg/month, or 0.4-0.5 mg/day. If this is added to the basal loss of 1.25 mg/day, then the total amount of iron lost is 1.25 mg/day. The volume of blood that comes out more than 80 ml occurs in adolescents who have long menstrual periods [10]. Menstrual problems can interfere the school activities and daily activities too [11].
Another factor that can exacerbate anemia in adolescent girls is the lack of iron intake, where iron in adolescent girls is needed to accelerate growth and development. The results of Shalini's research in India found that the intake of iron-rich foods low was 72% [12]. Tangerang indicated that the total iron intake in girls aged 10–12 years who suffered from anemia was only 5.4 mg/day or 25%, which is lower than the daily requirement of 20 mg/day according to the 2013 Nutritional Adequacy Ratio (RDA) [13].
Anemia causes fatigue, decreased learning concentration that impact learning achievement, can reduce work productivity [14] and quality of life in adults [15]. Anemia can reduce the body's resistance so which can increase the risk of infection. The high prevalence of anemia among adolescents if not handled properly will continue into adulthood and contributed greatly to the increase in maternal mortality (MMR), the risk of giving birth to babies with low birth weight (LBW), and stunting [14,16].
WHO (2014), has a target in 2025 to reduce the prevalence of anemia in women of childbearing age by 50% [5]. In WHO (2011) recommendations for the prevention of anemia for adolescent girls and women of childbearing age by focusing on promotive and preventive activities, through efforts to increase consumption of nutrients that contain lots of Fe, provide blood-added tablets, and increase fortification of foodstuffs with iron and acid folate. Blood supplement tablets are iron folate tablets where each tablet contained 200 mg of ferrous sulfate as well as 60 mg of elemental iron and 0.025 mg of folic acid [17].
A few studies have shown that supplementation of tablets containing 200 mg of ferrous sulfate and 0.25 mg of folic acid that increases in average Hb in adolescent girls after being given treatment [18,19]. The results of the Singh RS research (2018), effective nutritional counseling and supplements play an important role in preventing nutritional deficiencies, such as anemia [20]. Education/counseling to parents increases the cure rate for anemia in preschool-aged children, through increasing adherence to IFA consumption [21]. Adolescence also is an unique point of intervention as people of this age group are more receptive to changes in lifestyle that may determine their life course later [22]. Previous studies showed that adolescents have poor knowledge, attitudes and practices about malnutrition and dietary intake [23],[24],[25],[26]. Providing them with knowledge about iron deficiency could prevent them from anemia and the impact later in life. Enhancing health education interventions on knowledge, attitudes and practices, especially among adolescents, is potentially important in reducing anemia and mitigating short and long term consequences associated with health outcomes and those of their future offspring. There is a dearth of information on the evaluation of study characteristics and the overall quality of evidence of intervention studies in improving knowledge, attitudes and practices among adolescents especially in Asia region. Since the mid-1800s, when nursing was first acknowledged as a unique discipline, the responsibility for teaching has been recognized as an important role of nurses as caregivers. The focus of nurses’ teaching efforts is on the care of the sick and promotion of the health of the well public. In accordance to this review topic, a nurse has a great responsibility to teach people regarding nutritional anaemia. This systematic review aimed to examine the impact of health education interventions on the knowledge, attitude, practice, and prevention of iron deficiency anemia among Asian adolescent girls. This review provides an overview of the importance of educational interventions, and nurses may play an important role in educating families about anaemia and empowering them to achieve the best possible outcomes for adolescent.
MATERIAL AND METHODS
Review Protocol
We used the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) statement 2020 in conducting this study [27]. The study analyzed the effectiveness of health education in preventing anemia among adolescent females based on peer-reviewed studies published from 2000 to 2021. The participants, intervention, comparator, outcome, and study design (PICOS) criteria outlined in Table 1 were used to select studies for inclusion in this review.
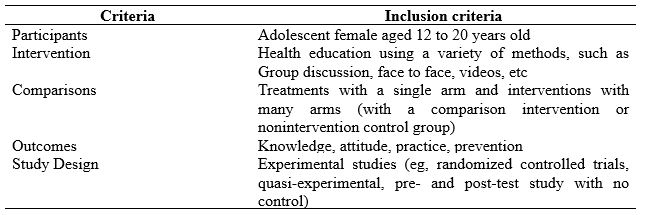
Table 1. Studies Criteria based on PICOS
Searching strategy
Databases used in collecting relevant literature include Sciencedirect, Cochrane library (Central), Pubmed, and the Wiley Online Library. We could not use other databases due to limited access or are not free access. The defined keywords adhere to the Mesh term for health research. The keywords being used are varied because they are tailored to the search engine. The keywords focus on nutritional education, empowering, Educational intervention, peer education, health promotion OR Health information AND iron deficiency anemia OR anemia AND adolescent girls OR female students. A summary of keywords combination used in each database used is reported in Table 2.
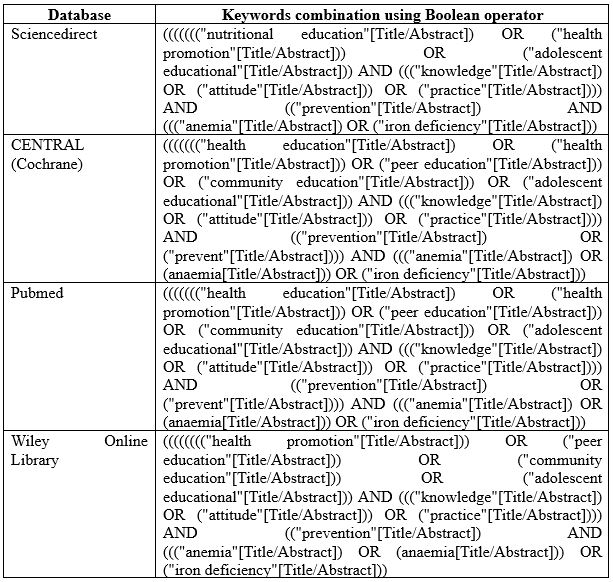
Table 2. Search strings in databases
Eligibility Criteria
We included all studies with evidence reporting the effectiveness of educational interventions in reducing and preventing iron deficiency anaemia, published from January 2000 to December 2021, written in English, and published in peer-reviewed journals. All studies using adolescent female or female students in either school or community-based settings are included in this review. Health education in any methods, intervention duration of three days at minimum, and followed up on a week, month, or year are also included in this study. Studies that reported incomplete information were excluded from duplicate publications, systematic reviews, commentaries, and letters to editors that did not provide primary data.
Information Source
After compiling keywords that match the Mesh terms, the next step is to start searching the database with free access status. The time span determined by the authors has been mutually agreed upon and is considered sufficient to describe the theme raised. Literature searches on Sciencedirect were conducted in June 2021, Cochrane library in November and December 2021, Pubmed in May 2021, and the Wiley Online Library in December 2021. We also carried out a hand search of articles, comments, letters to editors, and proceedings. The articles obtained are then collected into separate folders, for further screening. We also got several articles from the results of a bibliography search in the article.
Selection Process
Two authors independently screened each record (title/abstract), disagreement between the authors resolved by first author. Screening is done by adjusting the title, objectives, and conclusions. Other required information is obtained from the main body of the study. The screening focus was based on the inclusion criteria of this systematic review.
Study Quality
Methodologically, article quality assessment used tools from the National Institutes of Health (NIH) on controlled intervention studies. There is an assessment sheet for assessing the methodology and compliance with the inclusion criteria of this study. Scores <30% of the criteria were classified as "poor", scores between 30 and 70% were classified as "moderate", and scores >70% were classified as "good" study quality. We agreed to include articles that fall into the "fair" and "good" categories.
Risk of bias
The Cochrane Risk of Bias Assessment Tool was used to evaluate the types of bias in each of the studies. The Cochrane Collaboration Risk of Bias Tool scale contains 12 items, which assess the internal and external validity of studies. The review evaluated and rated the 12 items. Items rated ‘yes’ were scored as ‘1′, while no or unable to determine or unclear or non-applicable were all scored as ‘0′. Higher scores and percentages indicate a lower risk of bias. The level of bias within each category for each study was rated as ‘high risk’ or ‘low risk’. Each criterion had equal weight, or the same value; the total score was calculated as the percentage of the maximum value obtained. Studies with scores above the mean score were considered to have a low risk of bias, while studies below the mean value are considered to have a high risk of bias.
Data Extraction and synthesis
An independent author (SS, AJ) conducted the extraction. Discrepancies among those two authors are resolved by consensus after consulting with other investigators (MR) when failed to meet an agreement.
The extraction items consist of First author/year, country, study design (Quasi-experimental, Randomized Controlled Trial), sample size, age, type of intervention, outcomes.
RESULTS
Study Selection
A systematic electronic search identified that 1,414 publications were discovered through backward searching of relevant papers. The full-text screening was conducted on 34 articles. A total of 22 articles failed to meet eligibility criteria at the full-text screening stage, and only 12 articles were finally eligible for further analysis. The search results follow the PRISMA 2020 flow diagram (Fig. 1).
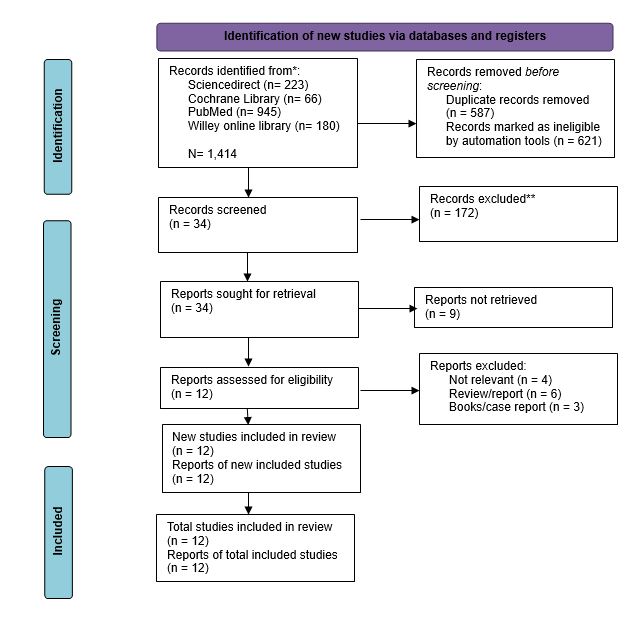
Figure 1. PRISMA flow diagram for literature search
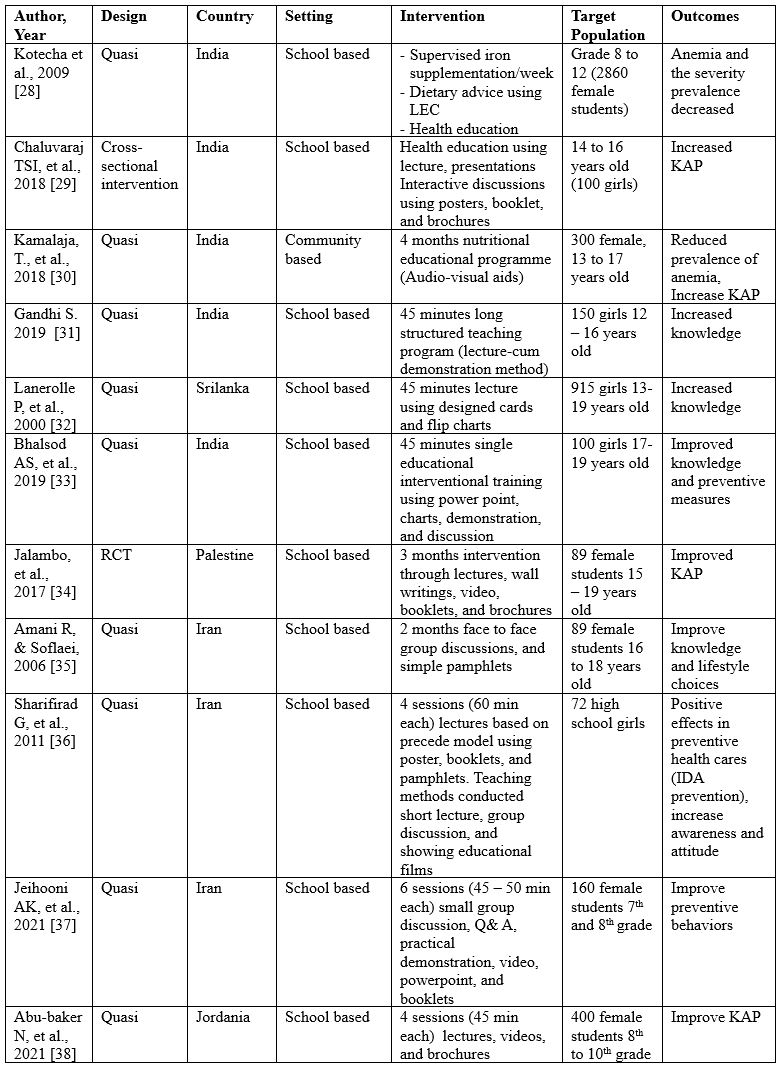
Table 3. Characteristics of the studies included
Study characteristics
Of the 12 studies that met the criteria for this review, 5 were studies conducted in India, 4 were studies in Iran, and one was conducted in Sri Lanka, Jordan, and Palestine. The study designs used were also quite varied, but most of the studies used a quasi-experimental design with a case-control approach (n= 10), and each study used an RCT and cross-sectional intervention design.
Quality Assessment
Assessment of the methodological quality of studies resulted in 6 studies with a good quality score [38] and 6 studies with a fair quality score [28].
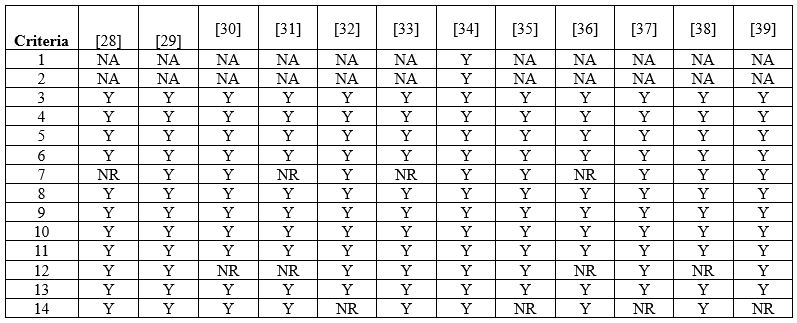
Table 4. Summary of studies quality assessment based on NIH
*Y: yes; NA: not applicable; NR: not reported
Risk of Bias
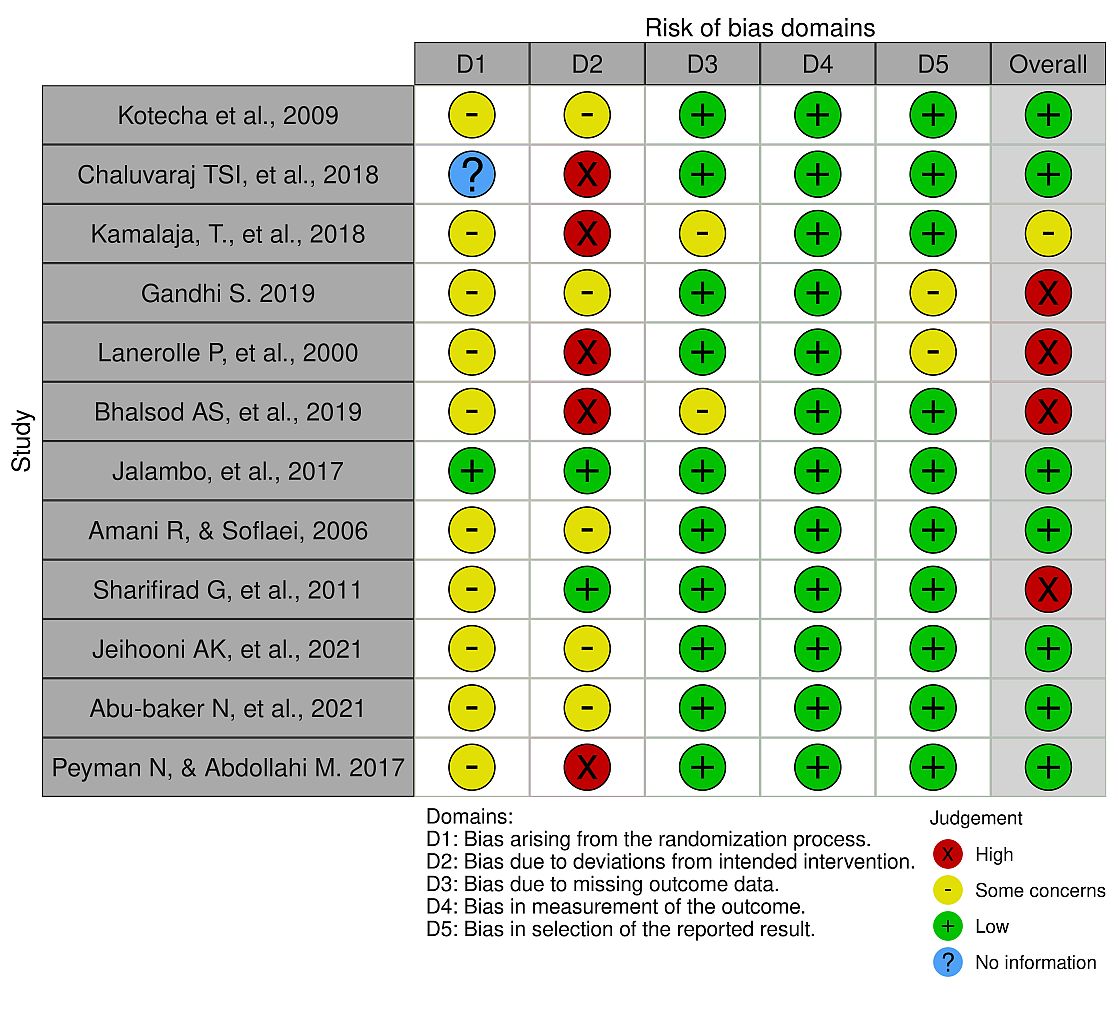
Figure 2. The Risk of Bias summary
Study setting and participants
Only 1 out of 12 studies met the inclusion criteria using a community-based setting [30]. Participants involved in the whole study were in the age range between 12-19 years old (First grade to twelfth grade), which was categorized into adolescence. Furthermore, for the gender of the participants, many of the studies we excluded were using male and female participants.
Types of intervention
The following interventions alone or in any combination were reviewed, such as Health education [28–31,33,36], Nutrition education [32,34,35,37,38], health information [39], and micronutrient supplementation (Iron) and dietary advice [28,32,34]. The shortest intervention duration was 45 minutes [29,31–33] while the longest duration was three months [34].
Types of Outcomes
We included all studies that met the inclusion criteria and limited access to relevant studies in other databases meant that we could not continue this review in the meta-analysis. For primary outcomes determined are Knowledge [31–33,35], Attitude, practice [29,30,34,38]. Meanwhile, secondary outcomes include decreased anaemia prevalence [28,30], improved prevention behaviour [33,36,37,39].
Knowledge, Attitude, Practice
In their study, Chaluvaraj et al. explained that despite numerous health education sessions in school, most female adolescents lack knowledge about anemia, its causes, prevention, and management. The study's overall findings indicated that female adolescents' knowledge, attitudes, and practices were moving in a desirable direction after the intervention. Adolescent healthcare services and facilities must be improved. Comprehensive nutritional education about anemia and its consequences for adolescents can pay considerable dividends in women's future lives [29].
According to the Kamalaja et al. study, rural adolescent girls lack essential health, food, and nutrition information. It could be due to a lack of purchasing power, access to nutritious food, false beliefs and taboos, and a lack of mass media such as TV, radio, and newspapers. Those methods provide information on good nutrition and a lack of government and non-government programs available for the health and well-being of adolescents. The health and nutrition education intervention significantly impacted subjects' nutrition knowledge [30].
Adolescent girls in the Gandhi study had moderately sufficient knowledge, attitude, practice of anemia prior to the teaching program. The majority (76.6 percent) of the adolescent children's knowledge became adequate after the structured video teaching program. Furthermore, there was no correlation between knowledge level and selected demographic variables such as age, gender, education, family type, father's job, mother's job, and monthly income [31].
Balshod et al. discovered that a single educational session significantly improves adolescent girls' knowledge of anemia. Such education interventions are to be carried out regularly in order to improve their knowledge. It encourages them to live healthy lifestyles, preventing anemia and other micronutrient deficiencies [33].
Iron deficient female adolescents in Gaza were discovered to have insufficient nutrition knowledge, attitude, and practice which could contribute to their haemoglobin and ferritin levels. Normal ferritin and hemoglobin levels, on the other hand, necessitate good knowledge, a positive attitude, and good practice. A nutrition education intervention was found to significantly improve knowledge, attitude, and practice [34].
Amani and Soflaei study aimed to improve knowledge of adolescent through the nutrition campaign. The intervention resulted in a significant change in nutritional knowledge and food-group scores consumption of adolescent girls taking part in the public education campaign [35].
Abu-Baker et al. found that more than half of the participants had adequate overall knowledge, attitude, and practice of IDA, many had insufficient knowledge of related issues, such as prior knowledge of anemia, its consequences, or foods that increase iron absorption. Implementing a nutrition education program would effectively improve female adolescents' knowledge, attitude, and practice regarding IDA. The intervention group significantly improved in these aspects after the intervention compared to the control group. Prior research has shown that implementing a structured and comprehensive educational program, even if it is a short-term program, is an effective strategy for improving knowledge, attitude, and practice among adolescents [38].
Prevention, Behavioral changes
Kotecha et al. In their study conducted IFA supplementation intervention once a week. It has proved its potential of not only improving haemoglobin but also improvement of iron stores. The serum ferritin data of over 800 girls confirmed the validity and consistency of the finding. Thus, this strategy of once a week IFA supplementation when given under supervision was effective [28].
The PRECEDE educational model was used in the Sharifirad et al. study. The PRECEDE educational model emphasizes self-care, incentives, and self-reliance through training. This method was the most effective in increasing participant knowledge and changing their attitudes toward behavior change. The PRECEDE framework is a systematic health education process that has been used in numerous studies to help organize a procedure for systematically developing programs. The main advantage of using this framework is that it delineates the factors associated with healthy behavior. It was discovered that educational programs based on the PRECEDE model were effective in controlling IDA and achieving success in other fields of study [36].
DISCUSSION
This review summarizes findings from a total of 12 studies and including 5,355 participants. Most of the studies included in this review were Quasi experimental and assessed the impact of educational intervention on the knowledge and health status among adolescents regarding iron deficiency anemia (IDA). The interventions included Nutrition education, health information, dietary advice, and supplementary micronutrient (Iron).
Given the WHO building block framework, the service delivery platform in all included studies was schools. The nutrition intervention was delivered through school teachers, student classroom monitors, and the research team. None of the included studies detailed details relating to health information systems. In all included studies, researchers provided nutritional supplements, and various non-profit organizations provided some funding. In all included studies, the investigator directly led the intervention. High school girls are one of the most important high-risk groups regarding IDA. That is why this age group was considered as a study subject.
Among the main results, we can confirm that educational intervention can positively impact knowledge, attitudes, practices, behaviour, awareness, and improvement of anaemia conditions in participants with anaemia. Giving daily or weekly iron supplements reduced the severity of anaemia experienced by participants. Only a small number of studies have provided participants with iron supplementation in addition to providing education or health information, so we cannot fully believe in the effectiveness of micronutrient supplementation. These findings require caution in interpretation since there have been very few studies, and because the quality of the results is low or very low, so they can only be seen as preliminary findings.
Booklets are the most widely used media in the studies included in this review [29,34,36,37,39]. These media used by combining several other media such as videos, power points, pamphlets, in channelling or transferring knowledge about anaemia, the results obtained show a positive effect where KAP has increased [29,34].
The overall quality of evidence-based was moderate. It indicates the reliability of the overall intervention approach and determination. The results propose the need to (i) improve the standards and procedures in intervention strategy and outcome apprising in randomized controlled trials to pinpoint actual outcomes relevant to the study population. (ii) Identify the outcomes that tend to improve the significance of health/nutrition education interventions. (iii) To enable the comparison of the methodology of the study in order to determine the factors that promote the effectiveness of health/nutrition education interventions among adolescents. Improving the methodological quality, such as random sequence generators, allocation concealment, blinding of participants, managing the dropout, including matter-of-fact reporting, and follow-up after the intervention will increase the study's quality and the overall quality outcome. More detailed and appropriate studies should focus on middle and low-income countries as they bear more global malnutrition and early marriage burden, especially adolescent females. In low- and middle-income countries, most adolescent girls have become mothers with inadequate knowledge concerning malnutrition and its consequences. Focusing on young women is crucial for themselves and their children in a short time in preventing the intergenerational cycle of IDA transmission.
The limitations of the review include limited access to the several databases which make we were unable to gain possible relevant studies. We are unable to continue with meta analysis because we only collect very few studies with moderate quality. Randomized controlled trials should be followed up to ensure continuity of the intervention. Future studies are expected to include follow-up in their research protocol. Furthermore, future studies should focus on underprivileged low- and middle-income populations through either school-based or community-based interventions.
CONCLUSIONS
Based on the studies in the review, it showed that Educational intervention for the treatment of iron deficiency anemia among adolescent female give positive impact on knowledge, attitude, practice, behavior, and awareness
Acknowledgments
We would like to thank the director of the Jambi Health Polytechnic for supporting this research.
Funding Source
This research did not receive any outside funding or support.
Authors contribution
All authors equally contributed to preparing this article
Conflict of interests
The authors declared no conflict of interest.
REFERENCES
- World Health organization. Regional office for South. East Asia. 2011;65.
- World Health Organization. Global targets 2025 to improve maternal, infant and young children nutrition. World Health Organization; 2017.
- Benedict RK, Schmale A, Namaste S. Adolescent nutrition 2000-2017: DHS data on adolescents age 15-19. In ICF; 2018.
- De Benoist B, Cogswell M, Egli I, McLean E. Worldwide prevalence of anaemia 1993-2005; WHO global database of anaemia. 2008;
- WHO. Anaemia Policy Brief. 2012;(6):1–7.
- McDaniel Jenny K. and Caryn E. Sorge. 2019. Diagnostic Approach to Anemia in Childhood and Adolescents. Springer link. DOI: 10.1007/978-3-319-96487-4_2
- Martini. Faktor - Faktor yang Berhubungan dengan Kejadian Anemia pada Remaja Putri di Man 1 Metro. Jurnal Kesehatan Metro Sai Wawai. 2015;VIII(1):1–7.
- Gunatmaningsih D. Faktor-faktor yang berhubungan dengan kejadian anemia pada remaja putri di SMA Negeri 1 Kecamatan Jatibarang Kabupaten Brebes tahun 2007. Universitas Negeri Semarang; 2007.
- Mengistu G, Azage M, Gutema H. Iron Deficiency Anemia among In-School Adolescent Girls in Rural Area of Bahir Dar City Administration, North West Ethiopia. Anemia. 2019;2019:1–9.
- Wijiastuti H. Faktor-faktor yang Berhubungan dengan Anemia pada Remaja Putri di Tsanawiyah Negeri Cipondok Tangerangtle. 2006;
- Chan, Symphorosa S C Pm Yuen, Ka Wah Yiu DSS. Menstrual Problems and health -seeking behavior in Hong Kong Chinese girls. Hong Kong Med J. 2009;15:18–23.
- Gunaratna Nilupa S, Honorati Masanja SM at all. No Title. PLoS ONE. 2015;
- Kurniawan YAI, Muslimatun S. Iron-Zinc Supplementation Among Adolescent Girls At Elementary School. 2005;(1):1–9.
- Kemenkes RI. Pedoman Penaggulangan Anemia pada Remaja Putri dan Wanita Usia Subur (WUS). Jakarta; 2016.
- Cappellini MD, Musallam KM, Taher AT. Iron deficiency anaemia revisited. Journal of Internal Medicine. 2020;287(2):153–70.
- Awisaba RE. Hubungan Antara Status Gizi dengan Tingkat Kebugaran Jasmani Tim Futsal Putra O2SN SMK Daerah Istimewa Yogyakarta. 2014.
- WHO. Guideline: Intermittent iron and folic acid supplementation in menstruating women. World Health Organization. 2011;1–30.
- Sayogo S, Sudardjat SS, Sudarsono S, Wirawan R, Margono S, Cobiac L. A study on the intervention scheme to reduce anemia in female adolescences, in Curug, Tangerang. Medical Journal of Indonesia. 2000;9(3):175–80.
- Joshi M, Gumashta R. Weekly iron folate supplementation in adolescent girls--an effective nutritional measure for the management of iron deficiency anaemia. Global journal of health science. 2013;5(3):188–94.
- Singh M, Honnakamble RA, Rajoura OP. Knowledge, Attitude and Practice Change about Anemia after Intensive Health Education among Adolescent School Girls of Delhi: An Intervention Study. International Journal of Medicine and Public Health. 2019;9(3):71–3.
- Shet Arun S; Merrick Zwarenstein; Abha Rao; Paul Jebaraj; Karthika Arumugam; Salla Atkins; Maya Mascarenhas; Neil Klar; Maria Rosaria Galanti.Shet Arun S; Merrick Zwarenstein; Abha Rao; Paul Jebaraj; Karthika Arumugam; Salla Atkins; Maya Mascarenhas; Neil. No Title. 2019;
- Bakrania S, Ghimire A, Balvin N. Bridging the gap to understand effective interventions for adolescent well-being: An evidence gap map on protection, participation, and financial and material well-being in low-and middle-income countries. UNICEF Office of Research-Innocenti New York, NY, USA; 2018.
- Rah JH, Melse-Boonstra A, Agustina R, van Zutphen KG, Kraemer K. The Triple Burden of Malnutrition Among Adolescents in Indonesia. Vol. 42, Food and Nutrition Bulletin. SAGE Publications Sage CA: Los Angeles, CA; 2021. p. S4–8.
- Singh M, Rajoura OP, Honnakamble RA. Anemia-related knowledge, attitude, and practices in adolescent schoolgirls of Delhi: A cross-sectional study. International Journal of Health & Allied Sciences. 2019;8(2):144–8.
- Shahzad S, Islam K, Azhar S, Fiza S, Ahmed W, Murtaza Z. Impact of knowledge, attitude and practice on iron deficiency anaemia status among females of reproductive age group (20-21-year-old) studying in Government Home Economics College Lahore, Pakistan. International Archives of BioMedical and Clinical Research. 2017;3(4):31–6.
- Sharmila P, Kumar MA, Rajagopala S. Knowledge, attitude and practices (KAP) related to Pandu Roga (Iron deficiency Anaemia) among adolescent girls attending Ayurveda tertiary care hospital and nearby schools-a survey. Journal of Ayurveda and Integrated Medical Sciences. 2019;4(04):154–9.
- Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. International Journal of Surgery. 2021;88:105906.
- Kotecha P V, Nirupam S, Karkar PD. Adolescent girls’ anaemia control programme, Gujarat, India. Indian J Med Res. 2009;130(5):584–9.
- Chaluvaraj TS, Satyanarayana PT. Change in knowledge, attitude and practice regarding anaemia among high school girls in rural Bangalore: An health educational interventional study. Natl J Community Med. 2018;9:358–62.
- Kamalaja T, Prashanthi M, Rajeswari K. Effectiveness of health and nutritional education intervention to Combat anemia problem among adolescent girls. Int J Curr Microbiol Appl Sci. 2018;7(9):3152–62.
- Gandhi S. Effectiveness of Video Teaching Programme on Knowledge about Anaemia among Countryside Children with Anaemia. International Journal of Nursing Education. 2019;11(4).
- Lanerolle P, Atukorala S, De Silva G, Samarasinghe S, Dharmawardena L. Evaluation of nutrition education for improving iron status in combination with daily iron supplementation. Food and Nutrition Bulletin. 2000;21(3):259–69.
- Bhalsod AS, Dave NN, Thakor N. Impact of educational intervention regarding anaemia and its preventive measures among adolescent girls of Government Arts College of Vadodara, Gujarat, India. 2019;
- Jalambo MO, Naser IA, Sharif R, Karim NA. Knowledge, attitude and practice of iron deficient and iron deficient anemic adolescents in the Gaza Strip, Palestine. Asian Journal of Clinical Nutrition. 2017;9(1):51–6.
- Amani R, Soflaei M. Nutrition education alone improves dietary practices but not hematologic indices of adolescent girls in Iran. Food and nutrition bulletin. 2006;27(3):260–4.
- Sharifirad G, Golshiri P, Shahnazi H, Shakouri S, Hassanzadeh A. PRECEDE educational model for controlling iron-deficiency anaemia in Talesh, Iran. JPMA-Journal of the Pakistan Medical Association. 2011;61(9):862.
- Khani Jeihooni A, Hoshyar S, Afzali Harsini P, Rakhshani T. The effect of nutrition education based on PRECEDE model on iron deficiency anemia among female students. BMC Women’s Health. 2021;21(1):1–9.
- Abu-Baker NN, Eyadat AM, Khamaiseh AM. The impact of nutrition education on knowledge, attitude, and practice regarding iron deficiency anemia among female adolescent students in Jordan. Heliyon. 2021;7(2):e06348.
- Peyman N, Abdollahi M. Using of information–motivation–behavioral skills model on nutritional behaviors in controlling anemia among girl students. Journal of Research and Health. 2017;7(2):736–44.
![]() This work is licensed under a Creative Commons
This work is licensed under a Creative Commons
Attribution-NonCommercial-NoDerivatives 4.0 International License.
The Influence of Consuming Sauropus Androgynus L. Merr, Moringa Oleifera Lam, and Vigna Cylindrica (L) Skeels on Breastfeeding Mothers: Randomized Controlled Trial
Ajeng Galuh Wuryandari1*, Indarmien Netty Ariasih1, Julaecha2
1Department of Midwifery, Health Polytechnic Jambi, Jambi, Indonesia
2Baiturrahim of College of Health Sciences, Jambi, Indonesia
Corresponding author: Ajeng Galuh Wuryandari, dr. Tazar Street, Buluran Kenali, Kec. Telanaipura, Kota Jambi, Jambi 36361, Indonesia, Orcid :https://orcid.org/ 0000-0002-7513-4666, Phone: +62 812-7978-0909, Email: wuryandariajenggaluh@gmail.com

Cita questo articolo
Background: Much scientific evidence shows the benefits of L. Merr, Moringa Oleifera Lam, and Vigna Cylindrica (L) Skeels. The leaves of these plants can be easily found in almost all of Indonesia and are a local food ingredient for Indonesian people. This study analyses the effect of the consumption of Sauropus Androgynus L. Merr, Moringa Oleifera Lam, and Vigna Cylindrica (L) Skeels on increasing the production of breastmilk while breastfeeding.
Methods: The research design used in this study was one group pretest-posttest design. The sample was taken by purposive sampling with 37 breastfeeding mothers with children aged <40 days who met the inclusion criteria. The intervention was to provide products processed as daily dishes, namely " sayur bening "with a composition of 150 grams of each plants (L. Merr, Moringa Oleifera Lam, and Vigna Cylindrica (L) Skeels), then measure the milk production by looking at how much the amount of breast milk increases after consuming the product for five days in a row, with the same seasonings. Data analysis using Wilcoxon test.
Results: The number of respondents in the study was 37 people with an age range between 19-39 years, with a child age range of 4-40 days, and the number of children owned by the respondents between 1-5 people. Analysis using the Wilcoxon test, it was found that all respondents (100%) experienced an increase in breastfeeding with p-value < 0.05, the same result was also shown in the comparison of birth weight with children's body weight after being given the intervention.
Conclusion: Consumption of Sauropus Androgynus L. Merr, Moringa Oleifera Lam, and Vigna Cylindrica (L) Skeels was statistically proven to differ in the amount of breast milk expenditure significantly. Kathree processing is adapted to everyday cooking so that postpartum nursing mothers can easily accept the taste and appearance.
Keywords: Sauropus Androgynus L. Merr, Moringa Oleifera Lam, Vigna Cylindrica (L) Skeels, Breastfeeding, Mothers
Introduction
Breast milk makes the world healthier, smarter, and more equal [1–3]. The benefits of breastfeeding can reduce the incidence of infection, increase intelligence, possibly protect against overweight and diabetes, and prevent cancer for mothers [4,5]. The Lancet report on maternal and child nutrition states that 800,000 child deaths can be prevented through breastfeeding and calls for breastfeeding support, but says that almost worldwide report a decrease in the rate of exclusive breastfeeding, including Indonesia. The reasons why women avoid or stop breastfeeding range from medical, cultural, and psychological reasons to physical discomfort and discomfort [6,7]. These things are not trivial, and many mothers without support turn to bottle feeding of formula. Multiplying across populations and involving multinational commercial interests, this situation has catastrophic consequences at the level of breastfeeding and the next generation's health [8–10].
The mother's nutritional status during breastfeeding is an effect of the nutritional status of the mother before pregnancy and during pregnancy (weight gain during pregnancy). Maternal weight gain during pregnancy depends on the nutritional status of the mother before pregnancy [11,12]. One of the most common factors associated with the failure of exclusive breastfeeding is the factor of breastfeeding that has not come out in the first week after delivery and the mother's view that her milk production is not enough. Exclusive breastfeeding for six months is one of the global strategies to improve infants' growth, development, health, and survival. Although there are many benefits of exclusive breastfeeding for babies, mothers, families and communities, its coverage is still low in various countries, including Indonesia [13,14]. The Basic of Health Research 2010 data shows that the coverage of exclusive breastfeeding for infants up to six months is only 15.3% [10].
Hereditary habits that have become local cultural wisdom in the Danau Sipin District area are various vegetables that are believed to increase breast milk, including banana hearts, long bean leaves, katu leaves, moringa leaves and many more. While in 2019, Lake Sipin was chosen to be the winner of the National Clean and Healthy Behavior Competition, the vegetables above have become regional local wisdom, with a variety of dishes derived from moringa, katu, long beans, kates. Danau Sipin District consists of 5 Kelurahan. There is 1 community health centre, namely the Putri Ayu Community Health Center. For January - September 2019, the target number of exclusive breastfeeding was 458 mothers, who gave exclusive breastfeeding 256 mothers, who did not give exclusive breastfeeding 49 for various reasons, while those who did not visit 153.
Various studies have been conducted to increase breast milk, including by giving oxytocin massage and the results are also significant. The culture of eating various vegetables such as katu leaves, Lembayung leaves (long beans) and banana flower, moringa and green beans related to their function as lactagogues is still focused on extracting and scientifically proving the function of long bean leaves and katu, moringa and kates leaves as lactagogue Traditionally processed form, namely as clear or boiled vegetables, stir-fry [5,15].
Danau Sipin sub-district in the work area of Putri Ayu Community Health Center which has a work area of 5 sub-districts. There is one coordinating midwife who is ready to participate in this research. Likewise, the head of the Driving the Empowerment of Family Welfare and his team and cadres. The leaves of long beans, katuk, and moringa are very potential to be developed both in terms of their benefits as lactagogues and the nature of these plants, which are very easy to grow with a short harvest life. Its use is still limited among Javanese and Malay tribesmen, with the processed form only as clear vegetables or boiled alone or mixed. However, not all villages have Moringa leaves, or Long bean leaves, all the time.
So far, breastfeeding mothers only consume L.Merr leaves which are used as laktagogums, whereas L.Merr leaves or also known as lavender leaves have greater benefits. Likewise, Moringa Oleifera Lam, and Vigna Cylindrica (L) Skeels leaves both contain laktagogums and saponins as well as polyphenols that can increase prolactin levels. Prolactin is a hormone that plays a major role in breast milk production [16-20]. Therefore, the development of functional supplementary food products for nursing mothers containing kathree leaves, namely Lembayung, katu, and moringa in the form of ready-to-eat products.
This study aims to analyze the effect of consumption of Kathree (Sauropus Androgynus L. Merr, Moringa Oleifera Lam, and Vigna Cylindrica (L) Skeels) on increasing the production of breast milk in postpartum mothers.
Materials and Methods
Trial design
The Randomized Controlled Trial with design of this study was one group's pretest-posttest design, namely a research design that contained a pretest before being given treatment and a posttest after being given treatment.
Participants
The sample is mothers who have babies aged < 40 days in the working area of Putri Ayu Health Center. Sampling was done by purposive sampling with 37 mothers who breastfed children aged <40 days who met the inclusion criteria. The inclusion criteria for the sample were healthy mothers and babies, primigravida mothers, while the exclusion criteria were mothers suffering from depression. The sample of this study was randomly selected from 105 postpartum mothers who visited the community health center polyclinic.
The data used in this study is secondary data from the documentation of quarterly reports at the Putri Ayu Health Center and the Jambi City Health Service which was carried out in December 2019-September 2020. The dependent variable of the study was the production of breast milk, measured by criteria 1) Frequency of urination, newborns who get enough Breast milk then urinate for 24 hours at least 6-8 time. 2) Characteristics of urination, clear yellow urine color. 3) Frequency of bowel movements, bowel patterns 2-5 times per day. 4) Color and characteristics of bowel movements, in the first 24 hours the baby excretes bowel movements which is dark green, thick and sticky, which is called meconium and beyond is golden yellow, not too runny and not too thick 5) The number of hours of sleep for babies who have enough breast milk for 2-4 hours. 6) Baby's weight. Signs of adequacy of breast milk in infants are: weight gain of more than 10% in the first week. As explained earlier that the questionnaire on breast milk production uses 6 question items, if the respondent answers yes, he will be given a score of 1 and if he answers no, he will be given a score of zero. Breast milk production questionnaire using the Guttman scale with a score range of 0-1. Breast milk production is said to be smooth if at least 4 of the 6 indicators observed in infants. If the value is less than 4 it is said no smoothly.
Intervention
Participants were given an intervention in the form of food consisting of 150 grams of each plant (L. Merr, Moringa Oleifera Lam, and Vigna Cylindrica (L) Skeels (Herbarium Medanense (Meda). The dose of food (vegetables) was determined based on the daily requirement of vitamins and minerals for postpartum mothers, namely 150 grams of vegetables consumed. 3 times a day for 7 days, if toxic effects occur during consumption of vegetables, the mother and baby will be referred to the clinic. Input (Q1) is the production of breast milk, then the mother is given Kathree vegetables (X) as an intervention, after that comes the output (Q2) in this case changes in breast milk production.
Randomisation
Sample selection using a simple random method
Blinding
In this study, 3 enumerators were used to collect research data. The previous enumerators did not know the participants because they were students who had been trained by the researcher before collecting data.
Statistical methods
Data were presented as numbers or percentages for categorical variables. Continuous data are expressed as the mean ± standard deviation (SD), or median with Interquartile Range (IQR). The data obtained were analyzed by univariate and bivariate, from the normality test (Kolmogorov Smirnov) obtained abnormal data so that the analysis used the Wilcoxon test.
All tests with p-value (p)<0.05 were considered significant. Statistical analysis was performed using the SPSS version 16.0 application.
Ethical Consideration
Registered prospective respondents have signed an informed consent and there is no incentive to participate in the study and the anonymity of participants is guaranteed. Before carrying out data collection, the researcher first took care of ethical permission. The authors state that this study followed all ethical clearance processes and was approved by the health research ethics committee of Ministry of Health Polytechnic of Jambi, Indonesia, and registration number: LB.02.06/2/18/2019.
Results
The results of the univariate analysis, which aims to determine the frequency of each variable studied, can be seen in the table 1.
Table 1 shows that most respondents in group aged 20-30 years amounted to 14 people (37.8%).
Majority of respondents’education level is low education as much as 70.3%, the dominant occupation of respondents is housewives as much as 51.4%.

Table 1. Frequency Distribution of Respondents' Characteristics
The normality test results showed that the data on the measurement of the amount of breast milk expenditure before and after the intervention was abnormal data. The results showed that all respondents (100%) experienced an increase in breastfeeding with p-value < 0.05. Statistically, there is a significant difference between before giving Kathree and after. The results can be clearer as in the table below.

Table 2. Wilcoxon Test Analysis Results about Breast Milk Production
According to the Wilcoxon test, 37 respondents experienced an increase in the amount of milk expulsion. The results of this study prove that dietary factors such as L. Merr, Moringa Oleifera Lam, and Vigna Cylindrica (L) Skeels, with a p-value < 0.05. Based on the results of this study, out of the five respondents, the baby's body weight increased by around 300 - 400 grams for 7 days of administration of purple leaf. Thus it can be stated that the provision of processed mauve leaves affects the increase in breast milk production for postpartum mothers.

Figure 1. Description of milk production
Figure 1 shows the fluctuation of post partum breast milk production before giving Kathree and an increase in milk production after the intervention.
Discussion
This study proves that food factors have a significant effect on breast milk production in addition to psychological factors and baby's suction power. Kathree gift which consists of Moringa leaves, katuk leaves, and long bean leaves, also known as mauve leaves.
Moringa oleifera Lam (synonym: Moringa pterygosperma Gaertner), commonly known as Moringa, is the most popular Moringacae clan species. Moringa oleifera grows in the form of three and is long-lived (perennial) with a height of 7-12 meters. It also has sympodial branches that point upward or oblique and tend to grow in line and lengthwise. Can grow both in the lowlands and highlands to an altitude of ± 1000 m above sea level, often planted as a barrier or fence in the yard or field.
Moringa oleifera is a local food ingredient that can be developed in the culinary of breastfeeding mothers because it contains phytosterol compounds that function to increase and accelerate milk production (lactagogum effect). Increased breast milk production, increased nutritional intake of infants, which is expected to impact the nutritional status of infants [21-22].
Moringa leaves contain high amounts of vitamin A, vitamin C, B vitamins, calcium, potassium, iron and protein which are easily consumed and assimilated by the human body. In addition, Moringa is also known to contain more than 40 anti-oxidants [23]. This content is needed by postpartum mothers who breastfeed. Breastfeeding mothers need more nutrients than during pregnancy. During breastfeeding, she needs extra energy to restore her health condition after giving birth, daily activities such as breast milk formation. In the first month after giving birth, milk production is generally abundant so that it comes out a lot and is sucked by the baby, so the mother is hungry and thirsty faster. In order for the number of calories to be balanced with the needs, adequate nutrition is needed because the energy will be reprocessed to form breast milk. During breastfeeding, the mother produces about 800-1000cc of breast milk [9,24,25].
Breast milk also contains protective compounds that can prevent babies from infectious diseases. Breastfeeding also has a tremendous emotional effect that can affect the inner relationship between mother and baby and affect the psychological development of the baby. Exclusive breastfeeding can optimize the baby's growth. Factors that influence breastfeeding are mothers who are well supported by their families and lactation education which can increase their knowledge, attitudes and behavior to provide exclusive breastfeeding for up to 6 months [24,26-28].
Previous research conducted by Zakaria [21] in Maros District on 70 breastfeeding mothers 6 weeks after giving birth showed that giving Moringa leaf extract and powder could increase breast milk volume, but the increase in the group that received the extract was higher than the group, get powder, but does not affect the quality of breast milk (iron, vitamin C and vitamin E).
Moringa oleifera is one of the alternative plants that are believed to have the potential to reduce malnutrition, hunger, prevent low birth weight, increase maternal hb levels, prevent DNA damage due to stress and prevent anemia in pregnant women [25].
Research by Situmorang [29] by giving katuk leaf stew to nursing mothers as much as 3x1 with 150 cc of katuk leaf stew. Katuk leaves are useful for increasing breast milk, for fever, and many other things. Based on research, katuk leaf infusion can increase milk production in mice. Katuk leaf root infusion has a diuretic effect at a dose of 72 mg / 100 g BW. Katuk vegetable consumption for nursing mothers can prolong the time to breastfeed the baby. The process of boiling katuk leaves can eliminate anti-protozoa properties. Katuk leaf infusion levels of 20%, 40%, and 80% in mice did not cause congenital defects and did not cause reabsorption. Raw katuk leaf juice is used for natural body slimming in Taiwan. The protein content in katuk leaves is nutritious to stimulate the release of breast milk. While the steroid and polyphenol content in it can function to increase prolactin levels. Thus the production of breast milk can increase. The steroids together with vitamin A also promote the proliferation of new alveolar-alveolar epithelium. Thus, there will be an increase in the number of elveoli in the gland which will automatically increase milk production. One of the reasons women do not give breast milk to their babies is that there is not enough milk to not be satisfied with breastfeeding. This is one of the factors that exclusive breastfeeding fails so that the mother gives formula milk to her child [12].
From the research results of Rahmawati [24] conducted a study on giving katuk leaves on increasing the production of sheep's milk. From the results of these studies, it turns out that the 20% katuk leaf extract solution given in vitro can increase milk production> 20%. The milk composition did not change, there was an increase in glucose metabolism activity by> 50%.
Suyanti & Anggraeni, [30] also states that giving katuk leaf decoction which is drunk 3 times a day (150cc in 1x drink) for 7 days can increase milk production by 50-120 ml. The Man Whitney statistical test p value <0.05 showed a significant effect of katuk leaf decoction on breast milk production based on the baby's weight gain. Mothers with sufficient breast milk can be seen from the frequency of weight gain for babies on day 10 [27].
Long bean plant (Vigna cylindrica (L) Skeels) is one plant that people believe can enlarge breasts and increase milk production. This plant has a proliferative effect on breast cells because it contains phytoestrogens, which are natural estrogens found in plants. This compound can stimulate proliferation if it binds to estrogen receptors. Long bean leaves contain 34 kilocalories of energy, 4.1 grams of protein, 5.8 grams of carbohydrates, 0.4 grams of fat, 134 milligrams of calcium, 145 milligrams of phosphorus, and 6 milligrams of iron. In addition, the Long Bean Leaves also contain as much vitamin A as 5240 IU, vitamin B1 0.28 milligrams and vitamin C 29 milligrams [5,31].
In the future, the plants from this research can be used as an alternative therapy for pregnant women who lack milk production. In addition to the effects or side effects that have not been widely reported, these three plants are very easy to find and inexpensive.
Conclusion
Moringa leaves, katuk leaves and long bean leaves were statistically proven to have significant differences in the amount of breastfeeding. Kathree processing is adapted to the form of everyday cooking so that postpartum nursing mothers can easily accept the taste and appearance. Kathree can easily be found in almost all over Indonesia, and is the local wisdom of the Indonesian people.
Study limitations
In our research, it has limitations such as the number of participants being fewer, and in this study there were 3 types of plants used for the intervention and no data analysis was carried out on each type of plant so that the efficacy of each plant could not be known, so in the future it is necessary further research
Author contributions
AGW and J contributed on concepting and designing the research. AGW and INA searched literature, analyze and interpret the data. AGW and J contributed to the paper's conceptualization, critical revision, and edited the overall improvement. All authors drafting manuscript, read and approved the final submitted paper.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Conflict of interest
There is no conflict of interest to declare.
References
- Piro SS, Ahmed HM. Impacts of antenatal nursing interventions on mothers’ breastfeeding self-efficacy: an experimental study. BMC pregnancy and childbirth. 2020;20(1):1–12.
- Dewey KG. Nutrition, growth, and complementary feeding of the brestfed infant. Pediatric Clinics of North America. 2001;48(1):87–104.
- Butte NF, Lopez-Alarcon MG, Garza C. Nutrient adequacy of exclusive breastfeeding for the term infant during the first six months of life. World Health Organization; 2002.
- Burns E, Triandafilidis Z. Taking the path of least resistance: a qualitative analysis of return to work or study while breastfeeding. International breastfeeding journal. 2019;14(1):1–13.
- Ignjatović S, Buturović Ž. Breastfeeding divisions in ethics and politics of feminism. Sociologija. 2018;60(1):84–95.
- Brown A. Breastfeeding as a public health responsibility: A review of the evidence. Journal of Human Nutrition and Dietetics. 2017;30(6):759–70.
- Hadju Veni. Infant Nutritional Status Of 0-6 Months Of Exclusive Breastfeed Due To The Application Of Moringa Leaf Extract In Breastfeeding Mothers. Health Notions. 2018;2(6):669–74.
- Lancet T. Breastfeeding: achieving the new normal. The Lancet. 2016 Jan;387(10017):404.
- Infodatin Kemenkes RI. Situasi Dan Analisis ASI Eksklusif 2014. Pusat Data dan Informasi Kementerian Kesehatan RI; 2014.
- Kemenkes RI. Hasil utama RISKESDAS 2018 [Internet]. Kementerian Kesehatan Badan Penelitian dan Pengembangan Kesehatan. Jakarta; 2018. Available from: https://kesmas.kemkes.go.id/assets/upload/dir_519d41d8cd98f00/files/Hasil-riskesdas-2018_1274.pdf
- Langer-Gould A, Smith JB, Albers KB, Xiang AH, Wu J, Kerezsi EH, et al. Pregnancy-related relapses and breastfeeding in a contemporary multiple sclerosis cohort. Neurology. 2020;94(18):e1939–49.
- Sandhi A, Lee GT, Chipojola R, Huda MH, Kuo S-Y. The relationship between perceived milk supply and exclusive breastfeeding during the first six months postpartum: a cross-sectional study. International Breastfeeding Journal. 2020;15(1):1–11.
- Rezal F. Hubungan Pengetahuan, Sikap dan Status Ekonomi dengan Pemberian ASI Esklusif Pada Bayi Usia 0-6 Bulan di Wilayah Kerja Puskesmas Lampeapi Kabupaten Konawe Kepulauan. Nursing Care and Health Technology Journal (NCHAT). 2021;1(2):94–101.
- La Adili DRS, Salma WO, Tosepu R. Factors related to the exclusive breastfeeding in the working area of PHC Poasia, Kendari City. Iberoamerican Journal of Medicine. 2021;3(4):300–6.
- Mensah KA, Acheampong E, Anokye FO, Okyere P, Appiah-Brempong E, Adjei RO. Factors influencing the practice of exclusive breastfeeding among nursing mothers in a peri-urban district of Ghana. BMC research notes. 2017;10(1):1–7.
- Purnanto NT, Himawati L, Ajizah N. Pengaruh Konsumsi Teh Daun Kelor Terhadap Peningkatan Produksi ASI di Grobogan. Jurnal Keperawatan dan Kesehatan Masyarakat Cendekia Utama. 2020;9(3):268–71.
- Johan H, Anggraini RD, Noorbaya S. Potensi Minuman Daun Kelor Terhadap Peningkatan Produksi Air Susu Ibu (ASI) PAda Ibu Postpartum. Sebatik. 2019;23(1):192–4.
- Firdausi A, Qomar UL. Penerapan Pemberian Olahan Daun Lembayung dalam Produksi ASI. Proceeding of The URECOL. 2019;33–9.
- Widyawaty ED, Fajrin DH. Pengaruh Daun Lembayung (Vigna sinensis L.) Terhadap Peningkatan Produksi Asi Pada Ibu Menyusui Bayi 0-6 Bulan. NERSMID: Jurnal Keperawatan dan Kebidanan. 2020;3(2):93–100.
- Suwanti E, Kuswati K. Pengaruh Konsumsi Ekstrak Daun Katuk Terhadap Kecukupan Asi Pada Ibu Menyusui Di Klaten. Interest: Jurnal Ilmu Kesehatan. 2016;5(2):132–5.
- Zakaria Z, Hadju V, As’ ad S, Bahar B. Pengaruh Pemberian Ekstrak Daun Kelor Terhadap Kuantitas Dan Kualitas Air Susu Ibu (Asi) Padaibu Menyusui Bayi 0-6 Bulan. Media Kesehatan Masyarakat Indonesia. 2016;12(3):161–9.
- Heryati, Paath EF, Rumdasih Y. Nutrition in Reproductive Health. Jakarta: EGC; 2005.
- Mutiara T, Titi ES, Estiasih W. Effect lactagogue moringa leaves (Moringa oleifera Lam) powder in rats. Journal of basic and applied scientific Research. 2013;3(4):430–4.
- Gunanegara RF, Suryawan A, Sastrawinata US, Surachman T. Efektivitas Ekstrak Daun Katuk dalam Produksi Air Susu Ibu untuk Keberhasilan Menyusui. Maranatha Journal of Medicine and Health. 2010;9(2):151203.
- Hackman, N. M., Schaefer, E. W., Beiler, J. S., Rose, C. M., & Paul IM. Breastfeeding Outcome Comparison By Parity. Breastfeeding Medicine. 2015;10(3):156–62.
- Djama N. Effect of Long Bean Leaves Consumption on Increased Breast Milk Production in Breastfeeding Mothers. Jurnal Riset Kesehatan. 2018;7(1):5.
- Emmanuel A. A Literature Review Of The Factors That Influence Breastfeeding. International Of Nursing And Health Science. 2015;2(3):28–36.
- Estiyani A, Suwondo A, Rahayu S, Suharyo Hadisaputro MNW, Susiloretni KA. The Effect Of Moringa Oleifera Leaves On Change In Blood Profile In Postpartum Mothers. Belitung Nursing Journal. 2017;3(3):191–7.
- Situmorang TS. The Effect of Consumption of Water Decoction of Katuk Leaves on the Expenditure of Breast Milk Production in Postpartum Mothers in the Independent Practice Midwife Manurung Medan in 2018. Stikes Murni Teguh. 2019;1(2).
- Suyanti S, Anggraeni K. Efektivitas Daun Katuk Terhadap Kecukupan Air Susu Ibu (Asi) Pada Ibu Menyusui Di Bidan Praktek Mandiri (Bpm) Bd. Hj. Iin Solihah, S. St., Kabupaten Majalengka. Journal of Midwifery Care. 2020;1(1):1–10.
- Fachruddin F, Suprayogi A, Hanif N. Addition of Katuk Leaf Hexane Fraction of Zanzibar Varieties in Feed Increased Milk Production, Display of Mother and Young Rats. Jurnal Veteriner. 2017;18(2289–296).
![]() This work is licensed under a Creative Commons
This work is licensed under a Creative Commons
Attribution-NonCommercial-NoDerivatives 4.0 International License.