Winda Triana*, Pahrur Razi, Ervon Veriza, Solihin Sayuti
Department of Health Promotion, Health Polytechnic of Ministry of Health Jambi, Indonesia
* Corresponding author: Winda Triana, Jl. Prof DR GA Siwabessy No.42, Buluran Kenali, Kec. Telanaipura, Kota Jambi, Jambi 36122Department of Midwifery, Health Polytechnic of Jambi, Indonesia.Orcid :https://orcid.org/0000-0003-0574-7915. Email: trianawinda146@gmail.com
Cita questo articolo
ABSTRACT
Background. The development of science and technology in the field of medicine encourages experts to always conduct research on various diseases, including one of them is the incidence of infectious diseases in order to overcome suffering and death due to these diseases.This study aimed to analyze the effectiveness of the emo demo method in increasing knowledge and skills about the prevention of non-communicable diseases.
Methods. This quasi-experimental study using two groups of pretest-posttest design involved 100 participants, whose data were collected using a questionnaire and tested using the Wilcoxon test.
Results. Both knowledge and skills variables show differences before and after the intervention of providing education, namely there is an increase in knowledge and skills to prevent non-communicable diseases. There are different mean values between pre-test and post-test knowledge and skills, meaning that mathematically indicates there are differences in knowledge and skills before and after Emo Demo.
Conclusion. The Demonstration Emotional Method learning model is effective in increasing students’ knowledge and skills about preventing non-communicable diseases.
Keyword: Counseling, Learning, Student, Knowledge, Skill
INTRODUCTION
Addressing Non Communicable Disease (NCDs) is integral to the 2030 Agenda for Sustainable Development [1]. Sustainable Development Goal (SDG) target 3.4 calls for a one-third reduction in premature mortality from NCDs by 2030. Many other SDG 3 targets are important for NCDs. Achieving the NCD-related SDG 3 targets can deliver shared gains across the development agenda, given the multidirectional relationship between NCDs, poverty, inequalities, economic growth, climate action and other SDG goals and targets [2].
Globally, non-communicable diseases, including cardiovascular disease, accounted for greater than 70% of all deaths in 2017 [3]. Non-Communicable Disease (NCD) is a catastrophic disease with the highest cause of death in Indonesia [4,5]. The National Health Research and Development Agency shows an increase in the development of NCDs in Indonesia due to the NCD trend followed by a shift in disease patterns [6].
An unhealthy lifestyle causes the high prevalence of NCD in Indonesia. The shift in the condition of NCD disease is expected to have a significant impact on Indonesia’s human resources and economy in 2030-2040. Indonesia will face a demographic bonus where the productive age is much higher than the non-productive age group [7].
A 2018 National Basic Health Research (Riskesdas) results show that 95.5% of Indonesians consume fewer vegetables and fruit. 33.5% of people lack physical activity, 29.3% of people of productive age smoke every day, 31% have central obesity, and 21.8% are obese adults [6]. Lifestyle changes should be made as early as possible as an investment in future health. Controlling risk factors must also be done as early as possible. People must have health awareness to know their body condition to make it easier to treat before too late[8].
Emotional Demonstration (Emo Demo) is a behaviour change communication strategy that uses the incorporation of Behavior Communication Change (BCC) and Behavior Communication Definition (BCD). BCC is an interactive process between individuals, groups, or communities to develop communication strategies to achieve positive behaviour change. BCD is a communication process which makes direct use of individual psychological constructs involving feelings, needs and thoughts. It is one of the methods that is being widespread and gaining attention[9–12].
The Global Alliance for Improved Nutrition (GAIN) is a Swiss-based foundation first launched at the United Nations Headquarters in 2002 to address nutrition issues. Indonesia encourages changes in feeding behaviour to prevent stunting in children through the Emo-Demo Program. The Emo-Demo targets one essential behaviour that we change: exclusive breastfeeding and a steady and balanced diet, healthy snacks and balanced, complementary foods, and washing hands with soap[13–15].
Developing an NCD prevention control model in the younger generation is very important so that they become productive, academically intelligent, and healthy. Avoiding healthy adolescents with NCD can be combined with efforts that have been carried out in the community. Through Integrated Development Post-NCD (IDP-NCD), prevention of NCD risk factors can be done as soon as possible so that the incidence of NCD in the community can be suppressed[7].
IDP-NCD risk factor surveillance has been carried out in every health centre in Jambi City (20 health centres). NCD risk factors found through the implementation of IDP in Jambi City have increased in the period 2016 to 2019. The NCD risk factors are smoking, lack of physical activity, fewer vegetables and fruit, and being overweight[16]. Based on the 2019 annual report, the five most prominent diseases at the Jambi City Health Center were hypertension at 47.42%, the most aged >59 years (19,223) cases. Diabetes Mellitus by 20%, Myalgia by 20%, Coronary Heart disease by 2.8%, and an increase in the age of 45-59 years with 1,528 cases[16].
The Simpang IV Sipin Health Center is one of the Telanaipura District Health Centers, Jambi City, with the results of risk factor screening at the NCDIDP in 2019 of 15.34%. This value is far from the MSS target of 100%. NCDIDP is a part of Community Based Health Efforts (UKBM). The target population aged 15-59 in 2019 in 21,935 people in the Telanaipura District Health Center Work Area. SMAN 5 is located in the work area of the Simpang IV Sipin Health Center, with 1200 students, where the senior high school age is in the range of 15 years and over. This high school age is very vulnerable to early disease if there is no early detection and regular monitoring is in the risk factor category. NCD includes smoking, consumption of alcoholic beverages, unhealthy eating patterns, and lack of physical activity, obesity, stress, hypertension, hyperglycemia, and hypercholesterolemia.
Considering the impact of the emergence of NCD, it is necessary to establish an NCD IDP and Utilize IDP with the emo demo method. It is hoped that with the formation of IDP-NCD volunteers in SMAN 5, all students will be interested in using IDP-NCD through the Emotional Demonstration Method Learning Model in Prevention of Non-Communicable Diseases at IDP NCD SMAN 5 Jambi City.
METHODS
Trial design
This research is a quasi-experimental study using two groups of pretest-posttest design
Participants
This study involved 100 participants, who were carried out in September-October 2020 at SMAN 5 (High school) Jambi City, involving high school students who were randomly selected with the inclusion criteria of students who had never received health education about non-communicable disease emodemos; grade Fourth, Fifth, and Lower Sixth, while students who were sick during the study were not included in the study.
Intervention
The research variables are students’ knowledge and skills. Before the intervention was given, the researcher first measured the level of knowledge and skills of the students/participants (pre-test). After being given the intervention, the researcher again measured the level of knowledge and skills of the students/participants (post-test). In this study, the intervention model given is the emotional demonstration learning model (emo demo) which is carried out once with a duration of 1 hour, which is 45 minutes of material delivery and 15 minutes of discussion). In this study, the researchers provided an explanation of non-communicable diseases to participants, accompanied by games about pictures and stickers of people with non-communicable diseases. the next step is for participants to try to explain about the pictures and stickers they get.
The knowledge and skills questionnaire consists of 22 questions with right and wrong answer choices. If the student answers correctly, he is given a score of 1, and if the answer is wrong, he is given a score of 0. The range of scores obtained is between 0-22. Both questionnaires use the Guttman scale. Meanwhile, students’ skills were measured using a questionnaire consisting of 8 questions with right and wrong answer choices. If the mother answered correctly, she was given a score of 1, and if the answer was wrong, she was given a score of 0. The range of scores obtained was between 0-8. Both questionnaires use the Guttman scale.
The Guttman scale has an important characteristic, which is that it is a cumulative scale and measures only one dimension of a multi-dimensional variable, so that this scale has an undimensional nature. The data obtained are in the form of interval data or dichotomy ratios (two alternatives) [17].
Researchers have worked as lecturers and researchers between 10-15 years and have academic degrees Masteral Degree and Doctorate. Researchers have done much research in the health sector and have compiled many questionnaires, so the researchers have prepared the questionnaires in this study. Before the research was conducted, the questionnaire was piloted on ten students, and the results showed that two questions had to be replaced because they were invalid. The knowledge questionnaire contains the respondent’s understanding of non-communicable diseases ranging from understanding, to overcoming them, while the skills questionnaire contains activities carried out in detecting and preventing non-communicable diseases.
Outcomes
This study compares the knowledge and skills of students in preventing the incidence of non-communicable diseases after being given an intervention in the form of an emo demo.
Sample size
This study involved 100 participants who were taken randomly using simple random sampling technique and sourced from three high school classes, namely grades Fourth, Fifth, and Lower Sixth.
Ethical Consideration
No economic incentives were offered or provided for participation in this study. In this study, because the subject was still a minor so the researcher had asked for and obtained parental consent so that their child could participate in the study. The study was performed in accordance with the ethical considerations of the Helsinki Declaration. This study obtained ethical feasibility under the Health Research Ethics Commission of the Ministry of Health, Jambi, and registration number: LB.02.06/2/153/2020.
Statistical analysis
Data are presented as numbers and percentages for categorical variables. Continuous data were expressed as mean ± standard deviation (SD) or median with Interquartile Range (IQR). Then proceed with bivariate analysis using the Wilcoxon test. The Wilcoxon test was used to determine the effect of the emo demo intervention on knowledge and skills. All tests with p-value (p)<0.05 were considered significant. Statistical analysis was performed using the SPSS version 16.0 application.
RESULTS
The characteristics of respondents in this study include age, gender and class level. The following is the frequency distribution of the respondents’ characteristics in this study:
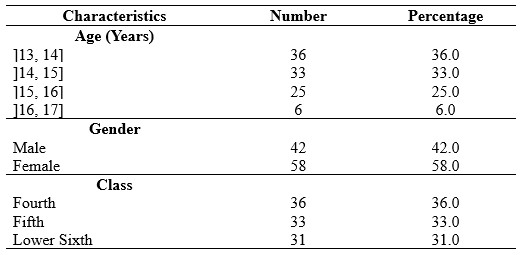
Table 1. Frequency Distribution of Respondents Characteristics
In Table 1 it is known that respondents in this study were female dominant as much as 58%, the most age was ]13, 14] years as much as 36% and the students came from class Fourth dominant.
Students’ knowledge before being given the Emotional Demonstration Method learning model in the prevention of non-communicable diseases, is presented in table 2.
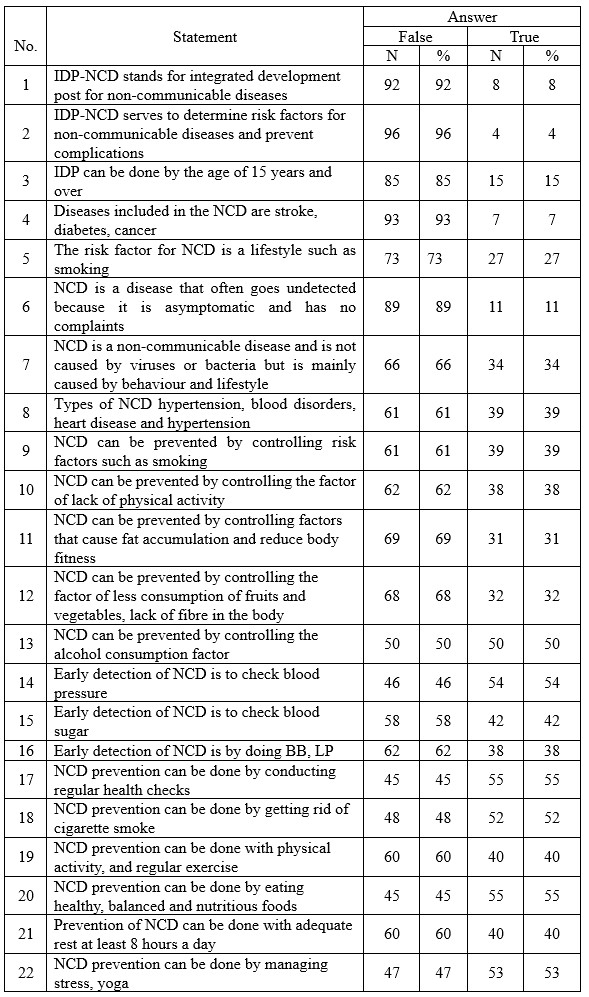
Table 2. Distribution of Respondents based on students’ knowledge before being given the Emotional Demonstration Method learning model in the prevention of NCD
Table 2 shows that 92% did not know the abbreviation of IDP, 93% did not know what diseases were included in NCD 96%, students did not know the function of IDP, 89% of students did not know the symptoms of NCD.
Knowledge after being given the Demonstration Emotional Method learning model about prevention of non-communicable diseases at IDP-NCD SMAN 5 Jambi City, can be seen in table 3.
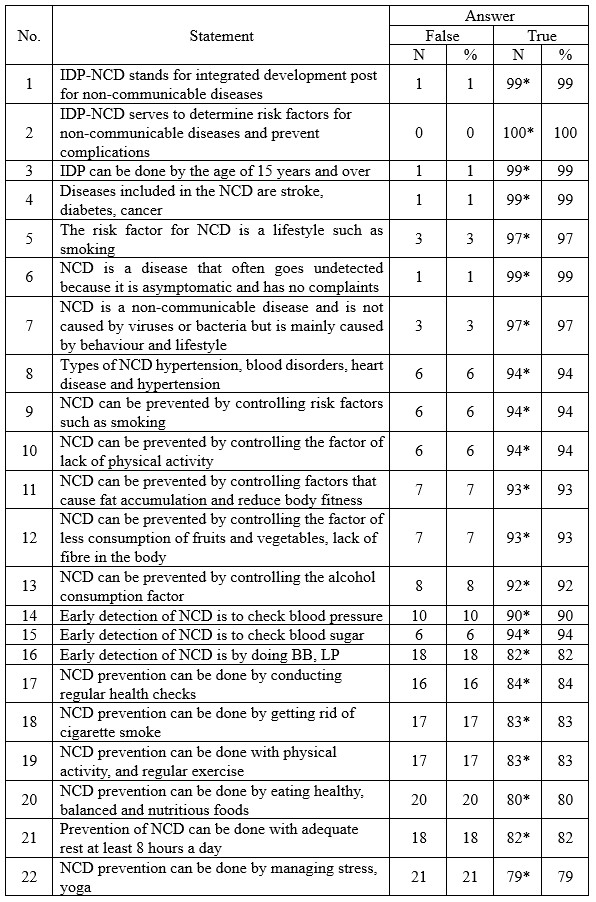
Description: an asterisk (*) is the correct answer
Table 3. Distribution of respondents based on knowledge after being given the Emotional Demonstration Method learning model in the prevention of non-communicable diseases
Table 3 shows that there are 100% of respondents who answered correctly about the function of the NCD IDP, 99% answered TRUE that IDP can be done aged 15 years and over, and 99% answered TRUE that the types of diseases included in the NCD are stroke, diabetes, cancer, 97% answered It is true that NCD is a non-communicable disease and is not caused by viruses or bacteria, but is caused more by behaviour and lifestyle.
Skills before being given the Emotional Demonstration Method learning model in preventing non-communicable diseases at IDP NCD SMAN 5 Jambi City in 2021 can be seen in table 4.
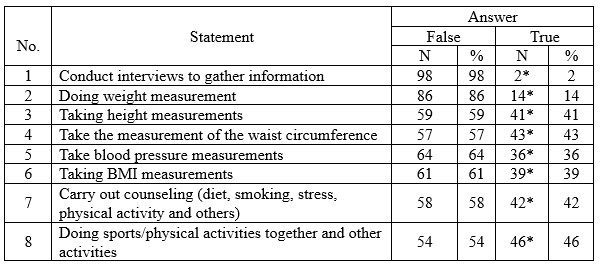
Description: an asterisk (*) is the correct answer
Table 4. Distribution of Respondents based on student skills before being given the Emotional Demonstration Method learning model in the prevention of non-communicable diseases
Table 4 shows that 98% did not conduct interviews to gather information, 86% did not weigh weight, 64%, and 61% did not measure BMI.
Skills after being given the Emotional Demonstration Method learning model in preventing non-communicable diseases at IDP NCD SMAN 5 Jambi City in 2021, can be seen in table 5,
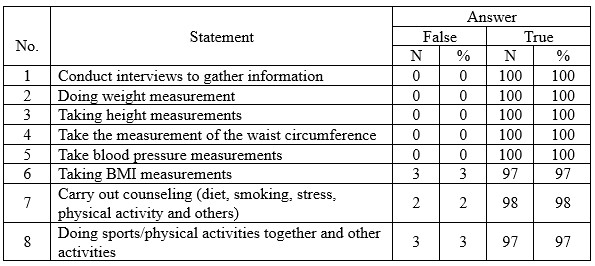
Table 5. Distribution of Respondents based on student skills after being given the Emotional Demonstration Method learning model in the prevention of non-communicable diseases
Table 5 shows that 100% of them were able to conduct interviews to dig up information, weigh weight, measure height, measure abdominal circumference, and measure blood pressure.
Table 6 shows that the Kolmogorov Smirnov statistical test results obtained a significant value of knowledge and skills both at the pre-test and post-test Emo Demo, each less than 0.05.
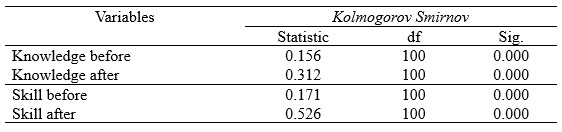
Table 6. Normality Test Results of Knowledge and Skills pre test and post test Emo Demo
The knowledge and skills data at the pre-test and post-test Emo Demo are not normally distributed. Therefore, the statistical difference test was tested using Wilcoxon (table 7).
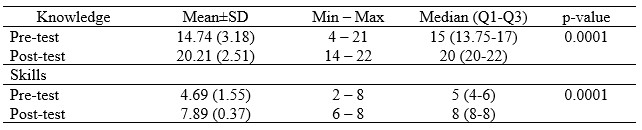
Table 7. Average Knowledge and Skills Pre and Post-test Emo Demo
Table 7 shows that there are different mean values between pre-test and post-test knowledge and skills, meaning that mathematically indicates there are differences in knowledge and skills before and after Emo Demo.
DISCUSSION
Based on the study results, it was known that the participant’s level of knowledge and skills regarding the prevention of non-communicable diseases was deficient prior to the intervention. It may be influenced by the low level of education and material on non-communicable diseases that are not included in the high school education curriculum.
The success of health education for school-age children is determined by the selection of educational methods following the characteristics of school-age children and the factors that will be influenced as a result of the education carried out [10,12,13].
Change can only happen in response to something new, exciting and fun. Health education methods usually used tend to instil knowledge before forming new behaviours. The emo demo method was carried out as an intervention using the behavioural-centred design (BCD) approach. This approach seeks to include psychological elements as innovations to change individual behaviour. The combination of science and creativity in the preparation of messages makes this method able to transfer behaviour change messages that are more readily accepted by the target [14,15,18].
In line with previous research by Padila [19] at Aisyiyah 1 Kindergarten, Bengkulu City, it was found that before the intervention was given, most of them received a one-star category as many as 27 people (90%), while the number of respondents after the intervention mostly experienced an increase in ability and received a four-star category, totaled 23 people (76.7%). Similarly, Aisyah’s research [20] at Al Kautsar Integrated Kindergarten, Mojokerto, Indonesia, found a change in knowledge after receiving material through demonstration media (emo demo) on washing hands in 7 steps.
The results of this study reject the null hypothesis regarding the effect of the emotional demonstration method on how to prevent non-communicable diseases by school students. The results of this study are in line with Aisyah’s research [20] which states that the emo demo method improves children’s knowledge, behaviour, and habits to wash their hands properly and correctly. Fermi Avissa [21] also found that the demonstration method improved the knowledge and skills of handwashing in preschool children at TK Flamboyan Platuk Surabaya.
Another study aims to apply the Emo Demo education method in reinforcing the mother’s intentions and actions in providing vegetable and fruit menus for the family. The results showed an increase in the intention of homemakers in the intervention group by 6.8 points with a p-value = 0.003, while in the control group, the opposite occurred in the form of a decrease in score by 6.8 (p = 0.229)[12].
Emo Demo is a highly participatory activity guide that aims to convey a simple message in a fun and emotional way, thus making it memorable and impactful compared to other conventional behaviour change strategies [4,11,22].
Emo Demo connects three crucial components in learning: allowing people to learn firsthand through experimentation, providing information, involving other parts of the brain, and touching emotions. In addition, the delivery of the Emo Demo is carried out using teaching aids to make the Emo Demo easy to remember and the message conveyed is accurate so that the message is more easily absorbed and the target is willing to try new behaviours [4,14,15,23].
Giving lessons to students through the emotional demonstration method is considered effective in increasing students’ knowledge and skills. Through this method, students are given education by delivering material accompanied by animated videos. After that, students can do direct practice on ways to control non-communicable diseases. Such as measuring blood pressure, weighing weight and height, carrying out counselling, exercising together and others so that the lesson material is memorable in students’ memories and hard to forget. It is proven that the dominant skills of students after being given skills lessons, it is seen that almost 100 students get a score of 100.
In general, the study results found that the knowledge and skills of respondents increased after the intervention. However, some respondents did not change after receiving education through emo demos and video media. It might be due to their poor memory.
CONCLUSION
The Demonstration Emotional Method learning model is effective in increasing students’ knowledge and skills about preventing non-communicable diseases.
LIMITATION
The limitations of this study include the minimal number of samples, and this study only involved one country, namely Indonesia, so the results may be different when comparing the effects of emo demos and intervention videos on students in other countries or even in the European countries.
FUNDING STATEMENT
This research did not receive any specific grant from funding agencies in the public, commercial, or not for profit sectors.
CONFLICT OF INTEREST
The authors report no conflict of interest.
ACKNOWLEDGEMENT
We would like to thank the director of the Department of Health Promotion, Jambi Health Polytechnic for supporting this research.
AUTHOR CONTRIBUTIONS
WT and PR were responsible for the study conception and design; EV performed the data collection; PR and SS performed the data analysis; WT, PR, and SS were responsible for the drafting of the manuscript; WT and PR made critical revisions to the paper for important intellectual content.
REFERENCES
1. United Nation. Last accessed: 19 July 2022. [Internet]. 2015. Available from: https://www.un.org/ga/search/view_doc.asp?symbol=A/RES/70/1&Lang=E. Last accessed: 29 August 2022.
2. World Health Organization (WHO). Non-communicable disease prevention and control: a guidance note for Investment cases [Internet]. 2019. Available from: https://apps.who.int/iris/bitstream/handle/10665/311180/WHO-NMH-NMA-19.95-eng.pdf. Last accessed: 29 August 2022.
3. Martinez R, Lloyd-Sherlock P, Soliz P, Ebrahim S, Vega E, Ordunez P, et al. Trends in premature avertable mortality from non-communicable diseases for 195 countries and territories, 1990–2017: a population-based study. The Lancet Global Health. 2020;8(4):e511–23.
4. Maryani H, Kristiana L, Paramita A, Andarwati P, Izza N. Pengelompokan Provinsi berdasarkan Penyakit Menular dan Penyakit Tidak Menular untuk Upaya Pengendalian Penyakit dengan Pendekatan Multidimensional Scaling (MDS). Buletin Penelitian Sistem Kesehatan. 2021;24(3):213–25.
5. Yarmaliza Y, Zakiyuddin Z. Pencegahan Dini terhadap Penyakit Tidak Menular (PTM) melalui GERMAS. Jurnal Pengabdian Masyarakat Multidisiplin. 2019;2(3):168–75.
6. Kemenkes RI. Hasil utama RISKESDAS 2018 [Internet]. Kementerian Kesehatan Badan Penelitian dan Pengembangan Kesehatan. Jakarta; 2018. Available from: https://kesmas.kemkes.go.id/assets/upload/dir_519d41d8cd98f00/files/Hasil-riskesdas-2018_1274.pdf. Last accessed: 20 June 2022.
7. Kementerian Kesehatan. Profil Kesehatan Indonesia [Internet]. Jakarta: Depkes RI; 2021. Available from: https://pusdatin.kemkes.go.id/resources/download/pusdatin/profil-kesehatan-indonesia/Profil-Kesehatan-indonesia-2019.pdf. Last accessed: 19 July 2022.
8. Kemenkes Republik Indonesia. Profil Kesehatan Indonesia tahun 2020 [Internet]. Pusdatin. Jakarta; 2020. Available from: https://www.kemkes.go.id/downloads/resources/download/pusdatin/profil-kesehatan-indonesia/Profil-Kesehatan-Indonesia-Tahun-2020.pdf. Last accessed: 19 July 2022.
9. Amareta DI, Ardianto ET. Peningkatan praktik cuci tangan pakai sabun pada anak usia sekolah dengan metoda emo demo. Sanitasi: Jurnal Kesehatan Lingkungan. 2017;9(2):88–93.
10. Rosita A, Dahrizal D, Lestari W. Metode Emo Demo Meningkatkan Pengetahuan dan Sikap Cuci Tangan Pakai Sabun (CTPS) pada Anak Usia Sekolah. Jurnal Keperawatan Raflesia. 2021;3(2):11–22.
11. Amareta DI, Ardianto ET. Penyuluhan Kesehatan dengan Metode Emo Demo Efektif Meningkatkan Praktik CTPS di MI Al-Badri Kalisat Kabupaten Jember. Prosiding. 2017;
12. Suriah IF, Rachmat M, Arundhana AI. Strengthening the Intentions and Actions of the Mother in Preparing Vegetables and Fruit Menus through the Emotional Demonstration Method. Journal of Management Practices, Humanities and Social Sciences. 2018;2(2):42–8.
13. Triana W, Verza E, Razi P. The Effect of Emotional Demonstration Methods and Video Learning on Hand Washing on Knowledge and Skills of Housewives. NSC Nursing. 2022;1(2):13–27.
14. Nurmaningsih N, Nisa SH. The Effect of Nutrition Education With The Emotional Demonstration Method on Mother’s Awareness In Feeding Underweight Toddlers. Jambura Journal of Health Sciences and Research. 2021;3(2):241–9.
15. Olief Syafrudin R, Apriyatmoko R. Perbedaan Praktik Cuci Tangan Pakai Sabun Untuk Pencegahan Penyebaran Virus Corona Sebelum dan Sesudah Diberikan Pendidikan Kesehatan Dengan Metode Emotional Demonstration Pada Remaja di Kelurahan Ngempon Kecamatan Bergas. Universitas Ngudi Waluyo; 2021.
16. Dinkes Kota Jambi. Profil Kesehatan Kota Jambi [Internet]. Jambi; 2020. Available from: http://dinkes.jambiprov.go.id/all_profil_kesehatan. Last accessed: 19 July 2022.
17. Sugiyono. Metode Penelitian Kuantitatif, Kualitatif dan R&D. Bandung: PT Alfabet; 2016.
18. Rahmawati R. Pengembangan Intervensi Emotional Demostration Terhadap Perubahan Perilaku Pola Makan Remaja Di Kabupaten Gorontalo= Development Of Emotional Demonstration Interventions On Changes In Adolescent’s Eating Patterns At Gorontalo District. Universitas Hasanuddin; 2022.
19. Padila P, Andri J, Harsismanto J, Andrianto MB, Admaja RD. Pembelajaran Cuci Tangan Tujuh Langkah melalui Metode Demonstrasi pada Anak Usia Dini. Journal of Telenursing (JOTING). 2020;2(2):112–8.
20. Aisah N, Reza M, Psi S. Meningkatkan Kemampuan Mencuci Tangan Melalui Metode Demonstrasi pada Kelompok B di TK Unggulan Terpadu Al Kautsar Mojokerto. Online), 3(3): 1-8, diakses pada tanggal 2 Januari 2018. 2014;3(3):1–8.
21. Avissa F, Nursalam N, Ulfiana E. Efektivitas Pendidikan Kesehatan Metode Demonstrasi Dan Metode Ceramah Dengan Media Booklet Terhadap Perubahan Pengetahuan Dan Tindakan Mencuci Tangan Pada Anak Prasekolah. Fundamental and Management Nursing Journal. 2012;1(1):59–66.
22. Ermawati I, Yuliana W, Hakim B. Pengaruh Metode Emotional Demonstration Terhadap Peningkatan Cakupan Penimbangan Balita Di Posyandu. Journal of Health Sciences. 2020;13(2):165–71.
23. Muyassaroh Y, Fatmayanti A. Pengaruh Permainan Emo-Demo ATIKA (Ati, Telur, Ikan) Terhadap Pengetahuan, Sikap dan Tingkah laku Pencegahan Anemia Pada Ibu Hamil. Jurnal Ilmu Keperawatan dan Kebidanan. 2021;12(2):222–8.
![]() This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.