Rusmiati*, Rosmawati, Sri Febrianti, Andriani
Department of Dental Health, Health Polytechnic Ministry of Health Jambi, Indonesia
Corresponding author: dr. Rusmiati, Tazar Street, BuluranKenali, Kec. Telanaipura, Kota Jambi, Jambi 36361, Indonesia, Orcid :https://orcid.org/0000-0003-0913-4219, Phone: +62 823-0615-7373, Email: rusmiati.dentalpoltekkes@gmail.com

Cite this article
ABSTRACT
Introduction: Improving the quality of life of children is one of the goals of the health development program. The growth of children’s health is not discriminated against in this scenario. All children with special needs or impairments are covered by child health services, whether at Special Schools (SS), other institutions, or in the community. This study aimed to evaluated the effectiveness of using an electric toothbrushes, compared to conventional toothbrushes, in the reduction of dental plaque score.
Methods: This study was designed as a quasi-experimental study with a pretest-posttest design. All school-aged children with mental impairment in SS Jambi City, Indonesia were included in this study. Overall, 20 children were assigned to the intervention group (n=10) and to the control group (n=10). The Personal Hygiene Performance-Modified (PHP-M) was used to examine plaque index for the assessment of dental and oral hygiene.
Results: In the pretest-posttest, mean difference values in plaque scores were statistically significant in both the intervention (19.50±3.89, p<0.009) and control (17.90±1.61, p<0.001) groups. A statistically significant reductions was showed in mean post-test plaque index (p<0.001) in the intervention group compared to the control group (14.50 ±7.83; 32.80± 13.14, respectively).
Conclusion: When compared to conventional toothbrushes, electric toothbrushes are more effective in reducing plaque scores in mentally retarded children at SS Jambi City.
Keywords: Conventional toothbrush, Electric toothbrush, Plaque score, Children, Mental impairment
INTRODUCTION
Overall health, well-being, and quality of life are all influenced by dental and oral health[1,2]. Oral health is a state of a person who is free of chronic oral diseases, facial pain, mouth and throat cancer, infections and sores, gum disease, tooth decay, tooth loss, and other diseases that impair the ability to bite, chew, smile, and talk[3].
Dental and oral health care are crucial components of comprehensive health care[4–6]. Dental and oral health indicators represent the Global Goals for Oral Health 2020. One of the technical activities of the WHO Global Oral Health Program (GOHP) is to offer advice to nations on how to build policies for preventing and promoting dental and oral illnesses[7].
Improving the quality of life of children is one of the goals of the health development program. In this situation, the development of children’s health is not discriminatory, and child health services are available to all children with special needs or disabilities, regardless of whether they are in special schools (SS), other institutions, or the community[8–10].
According to the 2012 Susenas (National socio-economic survey for Indonesia), 2.45 per cent of Indonesia’s population has impairments [11]. Mental retardation is one group of people with disabilities. Individuals with mental impairment are referred to as having mental retardation (mental retardation). Mental retardation, according to the American Association of Mental Deficiency (AAMD), is defined as a significant divergence from general intellectual functioning that coexists with adaptive behaviour impairments and manifests during the formative period [12].
Indahwati, et al [13] compared the dental and oral hygiene of mentally disabled and deaf students in SS-B and SS-C Tomohon City. According to the findings, mentally disabled kids had lower oral and dental hygiene than deaf students. According to Martens L et al. [14], mentally impaired children’s motor abilities at the age of 12 are lower than that of normal children, and mentally disabled children have difficulties holding and using a toothbrush. Rosmawati’s [15] study demonstrates that children with special needs have poor dental and oral health with an average Decay Missing Filled-Teeth (DMF-T) score of three.
Because mentally retarded children endure physical and mental development delays, such as disruptions in sensorimotor coordination, children with special needs require particular health services, one of which is children with special needs for mental retardation [16–19]. According to an interview with the principal of the State Extraordinary School 2 in Jambi City, the students at the school have a joint tooth brushing program after recess directed by the teacher and use a conventional toothbrush. However, the prevalence of dental caries remains high [20].
Brushing the teeth prevents dental caries, and the toothbrush most usually used to remove plaque is a standard toothbrush. Traditional toothbrushes need motor coordination from users, but sensorimotor skills are limited in mentally disabled youngsters.
According to some authors, manual toothbrushing entails the application of much higher pressure than the use of power brushes. Powered toothbrushes appear to be helpful in improving the oral health of physically or mentally handicapped individuals because these devices require minimal hand motion and coordination skills. Some models are designed with each bristle rotating individually and are effective plaque removers [21,22].
Considering the benefits of an electric toothbrush, it can make it easier for mentally handicapped children to clean their teeth and mentally disabled children in SS Jambi City have never used an electric toothbrush, it is vital to investigate the usefulness of conventional and electric toothbrushes in them. This study aims to evaluate the effectiveness of using an electric toothbrushes, compared to conventional toothbrushes, in the reduction of dental plaque score.
METHODS
Study design
A monocentric pilot study, with pretest-posttest design, was carried out from February to July 2022 at State Special School 2 in Jambi City, Indonesia.
Sample size
The minimum sample size required for this study was calculated using the G*Power program, considering effect size of 0.82, α-value of 0.05, power of 0.80, and sample group ratio of 1 [23]. In public health research, the value of sample size strength is at least 80%, therefore, we choose an effect size of 82% (lowest).
Participants
Eligible subject were selected according to the following inclusion criteria: all children in SS Jambi, diagnosed with mild mental retardation [24], aged 10-16 years, Dental caries index ≥ 6.6, unkempt teeth, Dental plaque score 1, bracesless. Children with moderate and severe mental retardation who were unwilling and under ten years old, Dental caries index < 6.6, Dental plaque score > 1, kempt teeth, braces and were excluded. Overall, 20 children participated in the study and were split into Intervention (n=10) and Control groups (n=10) which were randomly defined.
Intervention
After enrollment, participants were randomly assigned into a control group (n=10), in which they used a conventional toothbrush, and in the intervention group (n=10), in which they used an electric toothbrush. In both groups, the dental plaque score was evaluated at baseline (T0) and after seven days (T1). On the day 7th (T1), all participants were advised to brush their teeth and not eat food for 30 minutes before the oral health examination was conducted. All participants were instructed to brush their teeth in the morning after getting up, lunch, and dinner using the same toothpaste for both study groups. The DMF-T index is an index to assess dental and oral health status in terms of permanent dental caries [25,26]. The DMF-T index is an assessment of the total number of teeth or surfaces that are Decayed/Carious (D), Missing (M), and Filling (F) for everyone. The severity of dental caries at the age of 12 years or older is categorized into five categories, including very low severity with a DMF-T value of 0.0 – 1.0. Then the low severity level with a DMF-T value of 1.2 -2.6. Moderate severity with a DMF-T value of 2.7 – 4.4. And a high severity level with a DMF-T value of 4.5 – 6.5, and a very high severity level with a DMF-T value of ≥ 6.6
Outcomes
Disclosing solution was used to carry out the procedure for measuring plaque scores. It works by putting a disclosing solution on the subject’s tooth surface and recording the findings. Dental and oral hygiene was assessed using PHP-M (Personal Hygiene Performance-Modified). The assessment begins by making imaginary lines on the teeth to form 5 imaginary lines. The lingual and labial surfaces of the teeth were examined. If a plaque was observed in one area, it was given a score of 1. Otherwise, a score of 0 or a sign was provided (-). Plaque assessment findings were calculated by summing each plaque on each tooth surface, resulting in a plaque score for each tooth ranging from 0-to 10. Plaque scores for all teeth can range from 0 to 60, with 0-20 indicating good criteria, 21-40 indicating moderate criteria, and 41-60 indicating poor criteria.
Ethical Consideration
In this study, parents of the children had given their consent to the study. Before carrying out data collection, the researcher first took care of ethical permission. The authors state that this study followed all ethical clearance processes and was approved by the health research ethics committee of Jambi University Faculty of Medicine and Health Sciences, with number: LB.02.06/2/04/2022.
Statistical methods
For categorical variables, data were presented as numbers or percentages. The mean, standard deviation (SD), or median with Interquartile Range are used to express continuous data (IQR). Before the statistical test was carried out, the data normality test was first carried out using Shapiro Wilk test.
The non-parametric test used was Wilxocon to assess pre vs post conventional groups, while the Mann Whitney test was used to assess pre vs pre both study groups. The non-parametric tests were used for non normal data. The Paired T-Test was employed in data analysis to see if there was a difference in mean plaque scores before and after using a traditional toothbrush versus an electric toothbrush. The difference in plaque scores before and after treatment between the conventional toothbrush group and the electric toothbrush group was investigated using the independent T-Test. All tests with a p-value (p) of less than 0.05 were deemed significant. The SPSS version 16.0 application was used for statistical analysis.
RESULTS
Participants characteristics
The general characteristics of children, as shown in Table 1:
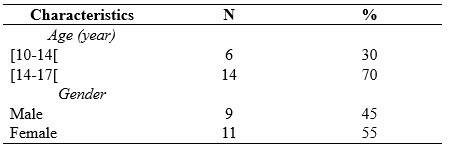
Table 1. Characteristics of childrens
The results of research on childrens with mental retardation SS Jambi City, as shown in Table 2:
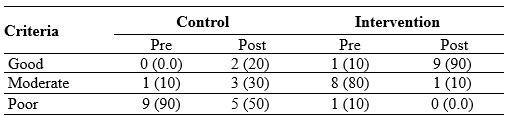
Table 2. Frequency Distribution of Plaque Score Criteria Based on PHP-M Index
Table 2 shows that before brushing their teeth, the criteria for plaque scores of children were one child (10%) with moderate criteria and nine children (90%) with poor criteria. After brushing their teeth, the criteria for plaque scores of children were two children (20%) with good criteria, three children (30%) with moderate criteria, and five children (50%) with poor criteria.
Before brushing their teeth with an electric toothbrush, the plaque score of children was eight children (80%) with moderate criteria, one child (10%) with good criteria, and one child (10%) with poor criteria. After brushing their teeth, the plaque score of nine children (90%) with good criteria and one child (10%) with moderate criteria.

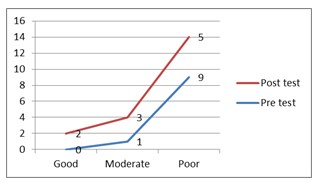
Figure 1. Plaque score criteria for control Figure 2. Plaque score criteria for intervention
group children group children
Because the sample size was less than 50 children, the Shapiro Wilk test was employed to determine the normality of the data. The sample size in this study was 20 children, as shown in Table 3:
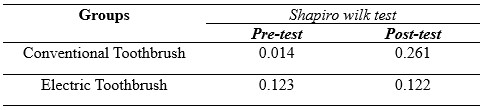
Table 3. Normality Test Results of Plaque Score Data for Children with Mental Requirements in SS Jambi City
The non-parametric test will be continued since the pre-test results in the conventional toothbrush group had an aberrant distribution of 0.014<0.05, and the post-test data were typically distributed at 0.261 > 0.05, as shown in table 3. In the meantime, the results in the electric toothbrush group were normally distributed, with a pre-test of 0.123 > 0.05 and a post-test of 0.122 > 0.05, respectively, followed by a parametric test.

Table 4. Test of the Effectiveness of Using Conventional Toothbrushes and Electric Toothbrush on Decreasing Plaque Scores in SS Jambi City
Table 4 shows that the mean score of plaque before brushing teeth is 52.30, whereas the mean score of children’s plaque drops to 32.80 after brushing, indicating a 19.50 decrease in the mean value. The p-value for the paired data effectiveness test is < 0.009, indicating that using a conventional toothbrush to reduce plaque scores in mentally disabled children at SLBN 2 Jambi City is thriving. The mean score of plaque before cleaning teeth is 32.40, that the mean score of children’s plaque falls to 14.50 after brushing, and that the mean value decreases by 17.90. The findings of the paired data effectiveness test show that the p-value is < 0.001, indicating that using an electric toothbrush to reduce plaque scores in mentally disabled children in SS Jambi City is beneficial.
The mean post-test value for the conventional toothbrush group is 32.80, while the electric toothbrush group is 14.50, with a P-Value of < 0.001. It indicates the difference in plaque score reduction effectiveness between conventional and electric toothbrushes in mentally disabled children.
The use of electric toothbrushes is more effective in reducing plaque scores in mentally retarded children at SS Jambi City, based on this description.
DISCUSSION
The current study is based on the theoretical basis of the physical condition of children with mental retardation. It has been known that children with mental disorders have mobility limitations, specifically in their extremities. This situation raises question marks about their ability to brush their teeth. Some studies have proven that mentally impaired children’s motor abilities are lower than normal children, and mentally disabled children have difficulties holding and using a toothbrush. Children with special needs have poor dental and oral health with an average Decay Missing Filled-Teeth (DMF-T). So in this study, we evaluated the effectiveness of using an electric toothbrushes, compared to conventional toothbrushes, in the reduction of dental plaque score.
We reported that the use of conventional toothbrushes helped lower plaque scores in children with mental retardation in SS Jambi. These findings are in line with research conducted by Sitepu et al. [27] that using soft toothbrushes reduces plaque scores in mentally disabled children and a study conducted by Basith et al. [28] on 40 kids with Down syndrome in India. They observed manual or conventional toothbrushes to eliminate plaque and reduce gingivitis in children with Down syndrome for two months in each group.
In this study, it was also found that electric toothbrushes reduced the number of plaque scores in mentally disabled children in SS Jambi. Electric toothbrushes are effective in reducing OHI-S rates in children with Down syndrome, according to research conducted by Az Zahra et al. [29] and research conducted by Vandana et al. [30] on 30 people with mental problems who were observed for 45 days showed that brushing teeth with an electric toothbrush can reduce the number of mycobacteria in the oral cavity of mentally disabled children.
Plaque removal is the most critical activity for maintaining good teeth and oral health. The most popular tool for eliminating supra-gingival plaque is a toothbrush. However, most people do not clean their teeth correctly, and there is still a lot of plaque on the surface of their teeth [31].
Although electric toothbrushes are more expensive, because of the numerous designs and colors, they are thought to be more effective in raising the interest of mentally challenged youngsters in brushing their teeth. Electric toothbrushes are also good teeth cleaning equipment for preventing biofilm or plaque from forming on the surface of the teeth [32].
After brushing their teeth with an electronic toothbrush, the growing criteria for plaque scores in youngsters improve. This is due to the fact that the movement utilized in electric toothbrushes is better and more successful in reaching all parts of the mouth, as it is a systematic movement [33].
Mentally retarded children usually have difficulty in imitating the way of brushing their teeth that has been shown because their fine motor development is worse than normal children in general. Furthermore, mentally retarded children’s eye and hand coordination is severely impaired. As a result, the child will have difficulties with fine motor movements, which will prevent the youngster from executing actions that demand concentration and complex hand movements [34]. Electric toothbrushes are more effective for intellectually impaired youngsters because of this. Because electric toothbrushes move automatically and children can feel the proper vibration to massage the gum and gingival area, they are a good choice for youngsters. As a result, using an electric toothbrush is more efficient and effective [29].
Although the results of this study have reported that electric toothbrushes are very suitable for use by children with mental retardation, the role of parents is highly expected. Parents or companions are required to take a more active role in encouraging mentally challenged youngsters to clean their teeth twice a day, in the morning after breakfast and at night before bed. We really hope that in the future the production of electric toothbrushes will be further improved at a price that can be affordable by all circles of society.
Based on the results of this study, we strongly recommend the use of an electric toothbrush, especially for students with mental retardation.
CONCLUSION
When compared to electric toothbrushes, electric toothbrushes are more effective in reducing plaque scores in mentally retarded children at SS Jambi City.
Study Limitations
One of the limitations of this study is the very small sample size (a pilot study), we collected data at only one center in Indonesia, which may limit the generalizability of our results to the larger population, so that in the future it is necessary to conduct similar studies in a larger population. Another limitation of the study was that the genders were not matched in the second group, which may have influenced the study results.
Authors’ contribution
All authors equally contributed to preparing this article.
Acknowledgement
We express our gratitude to the director Director of Health Polytechnic, Ministry of Health Jambi, Indonesia for its support for the implementation of this research
Funding
This research received funding from the Development and Empowerment of Human Resources in Public Health (BPPSDMK) Indonesia
Conflict Of Interest
The authors declare that there was no conflict of interest in this research.
REFERENCES
1. Van der Weijden GA, Timmerman MF, Nijboer A, Lie MA, Van der Velden U. A comparative study of electric toothbrushes for the effectiveness of plaque removal in relation to toothbrushing duration: Timerstudy. Journal of clinical periodontology. 1993;20(7):476–81.
2. Zahra AAA, Audrey NW, Ichyana DS, Saskianti T, Pradopo S, Nelwan SC, et al. Effectiveness of the Use of Manual and Electric Toothbrushes and the Effect of Educational Brushing Teeth with Video Animation on OHI-S Children with Down syndrome. Indonesian Journal of Dental Medicine. 2021;4(1):6–10.
3. WHO. Oral Health [Internet]. World Health Organization. 2018. Available from: https://www.who.int/news-room/fact-sheets/detail/oral-health
4. Govindaraju L, Gurunathan D. Effectiveness of Chewable Tooth Brush in Children-A Prospective Clinical Study. Journal of clinical and diagnostic research: JCDR. 2017;11(3):ZC31.
5. Deery C, Heanue M, Deacon S, Robinson PG, Walmsley AD, Worthington H, et al. The effectiveness of manual versus powered toothbrushes for dental health: a systematic review. Journal of Dentistry. 2004;32(3):197–211.
6. Davidovich E, Shafir S, Shay B, Zini A. Plaque removal by a powered toothbrush versus a manual toothbrush in children: A systematic review and meta-analysis. Pediatric Dentistry. 2020;42(4):280–7.
7. Kementerian Kesehatan Republik Indonesia. Pedoman Paket Dasar Pelayanan Kesehatan Gigi dan Mulut di Puskesmas. Jakarta; 2012.
8. Kementerian Kesehatan RI. Pedoman Pelayanan Kesehatan Anak di Sekolah Luar Biasa (SLB) Bagi Petugas Kesehatan. Jakarta; 2010.
9. Ganesh M, Shah S, Parikh D, Choudhary P, Bhaskar V. The effectiveness of a musical toothbrush for dental plaque removal: A comparative study. Journal of Indian Society of Pedodontics and Preventive Dentistry. 2012;30(2):139.
10. Aass AM, Gjermo P. Comparison of oral hygiene efficacy of one manual and two electric toothbrushes. Acta Odontologica Scandinavica. 2000;58(4):166–70.
11. Badan Pusat Statistik. SURVEI SOSIAL EKONOMI NASIONAL 2012 [Internet]. 2012. Available from: https://sirusa.bps.go.id/sirusa/index.php/kuesioner/202
12. Grossman HJ, Begab MJ. Classification in mental retardation. Washington, DC: Amer Assn on Intellectual & Devel; 1983.
13. Indahwati V, Mantik MFJ, Gunawan PN. Perbandingan Status Kebersihan Gigi dan Mulutpada Anak Berkebutuhan Khusus SLB-B dan SLB-C Kota Tomohon. e-GIGI. 2015;3(2).
14. Martens L, Marks L, Goffin G, Gizani S, Vinckier F, Declerck D. Oral hygiene in 12‐year‐old disabled children in Flanders, Belgium, related to manual dexterity. Community dentistry and oral epidemiology. 2000;28(1):73–80.
15. Rosmawati R, Surayah S. Status Kesehatan Gigi Dan Mulut Pada Anak Berkebutuhan Khusus Penyandang Cacat Fisik Di SLB Prof. Dr. Sri Soedewi Sofwan, SH JAMBI. JURNAL BAHANA KESEHATAN MASYARAKAT (BAHANA OF JOURNAL PUBLIC HEALTH). 2018;2(1).
16. Carina C, Panjaitan M, Anastasia I, Adhana A. Perbedaan efektivitas sikat gigi elektrik dengan sikat gigi manual dalam penurunan indeks plak pada anak-anak tunanetra. Prima Journal of Oral and Dental Sciences. 2020;3(2):33–8.
17. Pasyah F. Gambaran Kekerasan Bulu Sikat Gigi Terhadap Penurunan Debris Indeks Pada Siswa/i Kelas VIII-1 SMPN 3 Perbaungan Kec. Perbaungan kab. Serdang Bedagai. Poltekkes Kemenkes Medan; 2019.
18. Ichyana D. Efektifitas Sikat Gigi Manual Dan Sikat Gigi Elektrik Terhadap Skor Ohi-S Anak Down Syndrome [Internet]. Universitas Airlangga; 2019. Available from: https://repository.unair.ac.id/93229/
19. Hasanuddin SH. Efektivitas Pendidikan Kesehatan Menggunakan Media Video Dengan Media Cerita Bergambar Terhadap Keterampilan Menggosok Gigi Anak Usia Prasekolah. Universitas Islam Negeri Alauddin Makassar; 2018.
20. Department of Health Jambi Province. Profile Health Department of Health Jambi Province [Internet]. Jambi, Indonesia; 2020. Available from: http://dinkes.jambiprov.go.id/file/informasi_publik/MTYxNTE2NDQyOA_Wkt1615164428_XtLnBkZg.pdf
21. Vorwerk L, Ghassemi A, Hooper W, Patel V, Milleman J, Milleman K. Comparative plaque removal efficacy of a new powered toothbrush and a manual toothbrush. J clin dent. 2016;27(3):76–9.
22. García‐Carrillo A, Jover A, Plá R, Martorell A, Sota C, Gómez‐Moreno G, et al. Manual versus sonic powered toothbrushing in patients with intellectual disability: a cluster‐randomized clinical trial. Journal of Clinical Periodontology. 2016;43(8):684–93.
23. Faul F, Erdfelder E, Lang A-G, Buchner A. G* Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behavior research methods. 2007;39(2):175–91.
24. Association AP. American Psychiatric Association: Diagnosti c and Statistical Manual of Mental Disorders, Arlington. 2013.
25. Jaime RA, Carvalho TS, Bonini GC, Imparato JCP, Mendes FM. Oral health education program on dental caries incidence for school children. Journal of clinical pediatric dentistry. 2015;39(3):277–83.
26. Hariyani N, Soebekti RH, Setyowati D, Bramantoro T, Palupi LS, Putriana E. Factors influencing the severity of dental caries among Indonesian children with autism spectrum disorder–a pilot study. Clinical, cosmetic and investigational dentistry. 2019;11:227.
27. Sitepu DT, Edi IS, Hidayati S. Penurunan Indeks Plak Gigi Ditinjau Dari Penggunaan Sikat Gigi Hard, Medium, Dan Soft. Jurnal Ilmiah Keperawatan Gigi. 2021;2(2):1–6.
28. Basith A, Monica, Biir. Comparative Evaluation of Effectiveness of Manual and Electric Tooth Brush (Oral – B) in Elimination of Dental Plaque and Gingivitis. 2019;4(March):45–50.
29. Az Zahra AA, Audrey NW, Ichyana DS, Saskianti T, Pradopo S, Nelwan SC, et al. Effectiveness of the Use of Manual and Electric Toothbrushes and the Effect of Educational Brushing Teeth with Video Animation on OHI-S Children with Down syndrome. Indonesian Journal of Dental Medicine. 2021;4(1):6.
30. Vandana KL, Tatuskar PV, Valavalka NN. A Comparative Evaluation Of Manual And Powereed Brushing On Oral Health And Microbial Of Mentallu Challenged Induvidual. 2020;(May):113–8.
31. Bahammam S, Chen CY, Ishida Y, Hayashi A, Ikeda Y, Ishii H, et al. Electric and manual oral hygiene routines affect plaque index score differently. International Journal of Environmental Research and Public Health. 2021;18(24).
32. Silva AM, Miranda LFB, Araújo ASM, Prado Júnior RR, Mendes RF. Electric toothbrush for biofilm control in individuals with Down syndrome: A crossover randomized clinical trial. Brazilian Oral Research. 2020;34(June).
33. Rahman eddy, Ilmi MB. Perbedaan Sikat Gigi Biasa Dengan Sikat Gigi Elektrik Terhadap Penurunan Debris Indeks Pada Murid Kelas V Madrasah Diniyah islamiyah Kindaung Banjarmasin. Jurnal Kesehatan Indonesia. 2019;9(3):122–8.
34. Hakim AR. Pengaruh Motorik Kasar Anak Tunagrahita Terhadap Motorik Halus. Jurnal Ilmiah PENJAS. 2016;2(2):33–49.
![]() This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.