ANALYSIS OF HOSPITAL ANTIBIOTIC PRESCRIPTIONS AFTER THE IMPLEMENTATION OF STEWARDSHIP: A RETROSPECTIVE OBSERVATIONAL STUDY IN TWO HOSPITALS IN NORTH-EASTERN SICILY
Salvatore Coppolino1*, Veronica Crucitti1, Febronia Federico1,
Emanuele Leotta1, Nadia Caporlingua2
- Unità Operativa Semplice (U.O.S.) Farmacia, Presidio Ospedaliero Barone Ignazio Romeo, Messina (Italy).
- Unità Operativa Semplice (U.O.S.) Farmacia, Presidio Ospedaliero Mistretta, Messina (Italy).
* Corresponding author: Salvatore Coppolino, Dirigente Farmacista, Presidio Ospedaliero Barone Ignazio Romeo, Via Giuseppe Mazzini, 14 Patti (Me) sacoppolin@yahoo.it

Cite this article
ABSTRACT
Introduction: Antimicrobial resistance is a global problem caused by the inappropriate use of antibiotics. To combat this phenomenon, multidisciplinary antimicrobial stewardship programmes have been initiated, the primary objectives of which include improving both the level of appropriateness of prescription and clinicians’ awareness of the correct use of antibiotics.
Objective/Purpose: The objective of the work was to conduct an analysis of antibiotic consumption at hospital level to assess the appropriateness of antibiotic prescription in a number of Operational Units.
Method: From 01/01/2021 to 31/12/2022, data were extracted from the Pharmacy Operational Unit’s management software on the dispensing of antibiotics (injectable and oral use), the Defined Daily Doses, and the number of dosage units dispensed to the General Medicine, Intensive Care, General Surgery and Neurorehabilitation Operational Units of two hospitals.
Results: Total antibiotic consumption was 7,845 dosage units in 2021 and 10,182 in 2022. The comparison of the defined daily dose values (4,565,485 in 2021 and 5,079,671 in 2022) is indicative of the use of antibiotics with different dosages, with a percentage increase of 11.3%. A comparison was also made between the Defined Daily Doses/100 bed-days delivered in 2021 and the regional and national figures, yielding a significantly lower figure than these latter figures.
Conclusions: The loss of antibiotic efficacy threatens to throw healthcare systems into crisis, leading to in an increase in morbidity and mortality from infections. The implementation of antimicrobial stewardship programmes remains, at present, the best tool to harness in order to curb the phenomenon of antimicrobial resistance. There is therefore a need for increasingly specialised professionals in the field of infectious diseases. Nurses and pharmacists play a crucial role in antimicrobial stewardship programmes, as they collaborate not only in the implementation of antimicrobial guidelines, but also in the review of individual patient regimens in order to optimise treatment and in the training of healthcare personnel on the appropriate use of antimicrobials.
Keywords: antimicrobial resistance, antimicrobial stewardship, antibiotics, appropriateness of prescription
INTRODUCTION
Antimicrobial resistance is a growing global public health problem that could lead, unless action is taken, to 10 million deaths a year by 2050 [1,2].
It is a complex phenomenon with a multifactorial genesis: the increased use of antibiotics (including inappropriate use), the spread of hospital infections with antibiotic-resistant micro-organisms (and the limited control of these infections), and the increase in international travel with the consequent increased spread of strains. Many pathogens are also simultaneously resistant to several classes of antibiotics (multidrug resistance) [3].
The resistance of bacteria to antibiotics can be divided into two types: natural (or innate) resistance and acquired resistance.
Acquired resistance is the result of clonal selection due to the selective pressure exerted by the drug and can be broken down into chromosomal resistance, which accounts for about 10-15% of all resistance, and extra-chromosomal resistance, which accounts for about 90% of all resistance and is mediated by gene sequences in plasmids or transposons (mobile genetic elements) [4,5].
The mechanisms whereby microorganisms become resistant to antibiotics include the production of antibiotic-inactivating enzymes (the production of ꞵ-lactamases, for example, is one of the most widespread resistance mechanisms. The enzyme hydrolyses the ꞵ-lactam ring, a pharmacophore, resulting in the loss of activity of the molecule); altered envelope permeability; altered targeting (altering the DNA gyrase by substituting a single amino acid makes the enzyme resistant to quinolone antibiotics); active transport systems (protein-coding genes that act as efflux pumps for antibiotics) and alternative metabolic pathways.
The Italian periodic national surveillance report (AR-ISS), published in 2021 by the Istituto Superiore di Sanità, highlighted the main pathogens (Staphylococcus aureus, Streptococcus pneumoniae, Enterococcus faecalis, Enterococcus faecium, Escherichia coli, Klebsiella pneumoniae, Pseudomonas aeruginosa and Acinetobacter species) responsible for the phenomenon of antimicrobial resistance, the use of which should be closely monitored.
In 2021, 33.1% of Klebsiella pneumoniae isolates and 8.8% of Escherichia coli isolates were multi-resistant to third-generation cephalosporins, aminoglycosides and fluoroquinolones; for Pseudomonas aeruginosa, the percentage of resistance to three or more antibiotics (piperacillin/tazobactam, ceftazidime, carbapenems, aminoglycosides and fluoroquinolones) was 11.4%; a high percentage of multi-resistance (fluoroquinolones, aminoglycosides and carbapenems) (85.4%) was observed for Acinetobacter species. The national figures on carbapenem-resistant Enterobacteriaceae (CRE) infections reported as many as 2,192 cases in 2021, confirming the widespread occurrence of carbapenem-resistant Enterobacteriaceae bacteraemia in Italy, especially in hospitalised patients [6].
Inappropriate use of antibiotics is associated with unfavourable outcomes, such as death, treatment failure and adverse reactions, resulting in an increased burden of care on the healthcare system, duration of antibiotic therapy and duration of hospitalisation [7,8]. It
also promotes the selection of resistant strains and the spread of antimicrobial resistance [9,10].
In Italy, the high levels of antibiotic resistance and antibiotic consumption require urgent prevention and monitoring action. Despite the downward trend, consumption continues to be higher than the European average, both in the human and veterinary sectors, with considerable interregional variability. Furthermore, in European maps of the distribution of resistant bacteria in Europe, Italy holds, together with Greece, the record for the spread of resistant germs. One of the main causes behind the increase in resistance in Italy and worldwide is the excessive use of antibiotics, especially after the emergency linked to the COVID-19 pandemic. To combat antimicrobial resistance, so-called “Antimicrobial Stewardship” (AS) [11] programmes have been initiated. These represent a series of interventions aimed at promoting and monitoring the correct choice of antibiotic, dosage and duration of treatment to preserve the future effectiveness of these molecules in real-life everyday clinical practice [12,13].
The Antimicrobial Stewardship Team (AST) is a multidisciplinary corporate body that must include an infectious disease specialist, a hospital pharmacist, a hygiene specialist, a nurse and a clinical microbiologist [13,14].
The primary objectives are to improve the level of appropriateness of prescription and clinical and microbiological indicators, to increase awareness among healthcare professionals on the correct use of antibiotics and the prevention of care-related infections, and to reduce costs due to short- and long-term clinical complications. Each member of the AST Team must cooperate with the corporate Hospital Infection Committee (HIC) for the activities within their competence. The resolution establishing the AST must define the responsibilities and methods of cooperation with the corporate HIC. It is of paramount importance that there is no ambiguity of roles between the AST and the HIC at corporate level, and that both maintain well-defined and closely interconnected areas of activity established by each individual health authority.
At local level, the Sicily Region, with Local Government Decree no. 703 of 04/08/2020, has drawn up a regional guideline document for the organisation of corporate AS programmes, setting out the lines of action to be followed by all companies. These include the implementation of the antimicrobial stewardship corporate function and the appointment of departmental representatives for each individual Operational Unit, represented by a doctor and a nurse, increased audits and feedback on the appropriateness of prescription, the establishment of lists of high-concern antibiotics, the implementation of a structured and informed system for infectious disease consultancy, the preparation of semi-annual reports, the drafting of corporate protocols for antibiotic therapy and prophylaxis and empirical therapy in hospitalised patients, company training and impact assessments [15].
With the CRE Regional Directive (DASOE/8/21932), in implementation of the circular of the Ministry of Health no. 1479 of 17/01/2020, the Sicily Region has initiated a surveillance programme for bacteraemias caused by carbapenem-resistant Enterobacteriaceae (CRE). The Directive provides for the collection of case reports on the regional territory, data analysis, monitoring, dissemination and evolution of infections, with periodic transmission of the data to the Italian National Health Institute (Istituto Superiore di Sanità) [16].
All the actions undertaken by the Sicily Region form part of the 2020-2025 Regional Prevention Plan, which represents the main planning, prevention and health promotion tool, as it places the citizen at the centre of the interventions, accompanying them throughout all phases of life, with the aim of achieving the highest level of health. The Regional Plan envisages, by 2025, the establishment of AST in all Regional Health Authorities [17].
Objective/Purpose
The objective of the work was to conduct an analysis of the consumption of antibiotics in certain Operational Units at the “Barone Ignazio Romeo” Hospital in Patti and the “San Salvatore” Hospital in Mistretta, part of the Provincial Health Authority of Messina, to assess the appropriateness of their use per Operational Unit.
MATERIALS AND METHODS
Sampling and eligibility
A retrospective observational analysis was conducted between 01/01/2021 and 31/12/2022.
The data were obtained from the consumption of antibiotics provided by the hospital pharmacies at the hospitals concerned in the five Operational Units considered.
Tools
For the implementation of this study, paper prescription forms for injectable antibiotics and the consumption of both antibiotics administered both intravenously (i.v.) and orally (p.o.), provided by the Pharmacy Operational Units of the two hospitals in Patti and Mistretta, were considered.
The injectable antibiotic prescription form used for administration bears the patient’s initials, the required active substance, the number of vials, the dosage, the duration of treatment, and whether it is targeted treatment or empirical treatment. The data on the dispensing of antibiotics by the two Pharmacy Operational Units, both for injection and oral use, to the General Medicine, Intensive Care, General Surgery and Neurorehabilitation Operational Units of the Patti and Mistretta Hospitals, facilities belonging to the Messina Provincial Health Authority (ASP), were extracted from the corporate management software. The number of beds per single Operational Unit and per year are shown in Table 1.

Table 1. Numbers of beds in different Operational Units at Patti and Mistretta hospitals
The data were collected by the researchers and processed in aggregate form for research purposes only. All the authors who took part in the observational study are hospital pharmacists, some with twenty years of service and a PhD in Pharmaceutical Sciences. All the authors have obtained the Specialisation in Hospital Pharmacy or in Pharmacology and Clinical Toxicology. To ensure confidentiality, each patient was assigned a number. For all the antibiotics dispensed, the Defined Daily Doses (DDDs) were considered, i.e. the average doses taken daily by an adult patient, with reference to the main therapeutic indication of the drug [18] and the number of dosage units dispensed to the individual Operational Units. Consumption was calculated as DDD/100 bed-days according to the scheme used by the Italian National Observatory on the Use of Medicines (OsMed) in the national report on the use of antibiotics in Italy for the year 2021[19].
Statistical Analyses
The data have been presented as numbers and percentages for categorical variables and in terms of the arithmetic mean in the case of continuous variables. For the management of our data, the calculation of DDDs, Delta (2022-2021) and Pareto diagrams were carried out using an Excel spreadsheet. In particular, the Pareto diagram was used to understand which factors could most influence our results.
RESULTS
Total antibiotic consumption was 7,845 dosage units in 2021 and 10,182 in 2022. The comparison of the DDD values (4,565,485 in 2021 and 5,079,671 in 2022) is indicative of the use of antibiotics at different dosage strengths, as an increase in DDD corresponds to an increase in the doses administered at different dosage strengths, allowing a comparison of consumption as it is a technical tool for measuring drug prescriptions. In 2022, there was a percentage increase of 11.3%. The analysis of DDDs was carried out on 100 bed-days provided per individual Operational Unit.
For Patti Hospital (Table 2), for the General Surgery department, 485,762 DDDs were provided in 2021 and 784.869 in 2022; for General Medicine, 1,817,933 DDDs in 2021 and 2,354,803 DDDs; for Intensive Care, 598,954 DDDs in 2021 and 736.244 DDDs in 2022; while for the Operational Unit of Mistretta Hospital (Table 3), 1,249,067 were provided for the General Medicine department in 2021 and 433.301 for 2022 and for the Neurorehabilitation department, 414.488 DDDs in 2021 and 770.457 DDDs in 2022.



Table 2. Comparison of antibiotic consumption in 2021 and 2022 at Patti Hospital.

Table 3. Comparison of antibiotic consumption in 2021 and 2022 at Mistretta Hospital.
For the year 2021, the consumption of DDD/100 bed-days in the Operational Units at the two hospitals examined was compared with the regional data and with the national data based on the findings of the 2021 National Report “The use of antibiotics in Italy” produced by OsMed [20]. The DDD/100 bed-days provided in 2021 was 70.6 at national level; in the Sicily Region it was 81.6, while in the Operational Units we examined it was 44.3.
The analysis of the data shows for Patti Hospital an increase in the consumption of amoxicillin/clavulanic acid, both p.o. and i.v. (Δ%=0.47), piperacillin/tazobactam (Δ%=1.23) and levofloxacin (Δ%=0.5) in General Surgery. An increase in the use of third-generation cephalosporins (Δ%=1.68), ciprofloxacin, both p.o. and i.v. (Δ%=1.21%), gentamicin (Δ%=0.73), linezolid and (Δ%=0.2) piperacillin/tazobactam (Δ%=1.54) was observed in General Medicine. Finally, an increase in the use of third-generation cephalosporins (Δ%=0.81), ciprofloxacin (Δ%=0.2), gentamicin (Δ%=0.06) and piperacillin/tazobactam (Δ%=1.35) was also observed in Intensive Care.
For Mistretta Hospital, there was no significant difference in Δ% between 2021 and 2022, only a clear reduction in the consumption of ceftriaxone (Δ% = -6) in General Medicine and an increase in amoxicillin/clavulanic acid, both p.o. and i.v. (Δ%=0.98%), and an increase in ertapenem (Δ%=0.61%) in Neurorehabilitation. From the prescription forms viewed, it was found that empirical prescriptions correspond to 92.8%, while those based on antibiogram evaluation only account for 7.2% of total prescriptions. Parenteral Amoxicillin/Clavulanic acid is used for otitis, sinusitis and COPD (chronic obstructive pulmonary disease), Cefazoline for respiratory tract infections and peritonitis, ceftazidime for gram-negative bacteria and Pseudomonas infections and for surgical interventions; ciprofloxacin for COPD, respiratory and urinary tract infections; gentamicin as a broad-spectrum antibiotic; meropenem for staphylococcal and streptococcal infections; piperacillin/tazobactam for pneumonia; teicoplanin for resistant Staphylococcus aureus infections. Further analysis was carried out on antibiotics for injectable use that required the use of prescription forms to monitor their appropriate use. The following antibiotics were considered: ciprofloxacin, colistin, fosfomycin, imipenem/cilastatin, levofloxacin, linezolid, meropenem, teicoplanin, tigecycline and vancomycin.
A comparison between 2021 and 2022 was performed using the Pareto diagram (Figure 1 and 2).

Figure 1. Pareto diagram of injectable antibiotics under monitoring for the years 2021 and 2022.
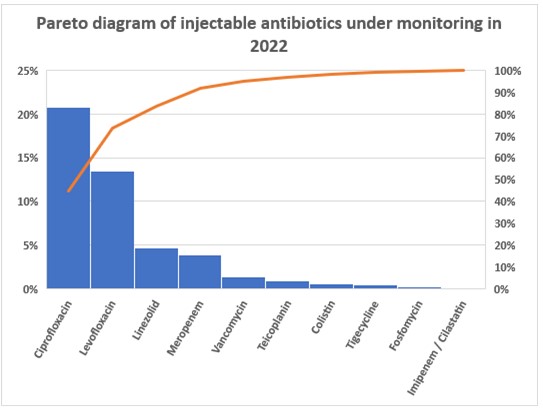
Figure 2. Pareto diagram of injectable antibiotics under monitoring for the years 2021 and 2022.
The Pareto diagrams showed that in 2022, there was a reduction in prescriptions for ciprofloxacin, levofloxacin and tigecycline. Increases were found for linezolid and meropenem. For the other antibiotics, prescriptions have remained constant or have undergone slight increases.
DISCUSSION
The analysis of paper prescription forms shows a consumption based more on empirical treatment (92.8%) than on antibiogram evaluations (7.2%), a situation that has prompted further corrective action by the AST and HIC, such as compulsory antibiograms for the antibiotics vancomycin, tigecycline, teicoplanin, meropenem, linezolid and the combination imipenem/cilastine.
Furthermore, for high-cost injectable antibiotics, such as fosfomycin or the meropenem/vaborbactam combination, a specific prescription form has been drawn up, in which certain requirements must be fulfilled by the patient to be eligible for that treatment, so that these antibiotics are reserved for cases where there are no valid treatment alternatives. Analysis of the Pareto diagrams showed that the use of the prescription form proved to be a valuable tool for improving appropriateness of prescription.
Although COVID-19 put the appropriate use of antibiotics at risk, especially in the early stages of the pandemic – for instance the improper use of azithromycin – hospital pharmacists and nursing coordinators worked hard to draw up and implement internal protocols on the use of antibiotics in Operational Units to ensure their rational use.
Hospital pharmacists and nursing coordinators play a crucial role in antimicrobial stewardship (AS) programmes, as they are involved in the development and management of antimicrobial guidelines, the review of individual patient regimens to optimise treatment, and the training of healthcare personnel on the appropriate use of antimicrobials.
The results from the cohort examined show that to ensure appropriate use and targeted treatment, thus avoiding the phenomenon of antibiotic resistance, it is necessary to isolate the bacterium responsible for the infection and carry out an antibiogram before administering certain antibiotics to hospitalised patients. Specifically, this procedure concerns vancomycin, tigecycline, teicoplanin, meropenem, linezolid, levofloxacin, the imipenem/cilastatin combination, fosfomycin, colistimethate and ciprofloxacin.
The AS strategy, which has been followed in our hospitals to date, involves a careful and thorough patient assessment, the choice of the most suitable antimicrobial to be prescribed, its administration and the monitoring of the patient once treatment has begun. This last phase includes the possibility of reducing the duration of antimicrobial treatment, converting the route of administration from intravenous to oral, modifying the dose based on any clinical conditions that might affect the patient’s pharmacokinetics, such as excretory system deficiencies, monitoring the use of the prescribed antibiotic, monitoring adherence to treatment, and informing the patient on the appropriate use of antimicrobials [21,22]. The hospital pharmacist plays a crucial role in the fight against antibiotic resistance by acting as a link between the clinician and the microbiology laboratory. This surveillance activity results in a positive effect on how antibiotics are prescribed by healthcare professionals, leading to a reduction in hospital infections.
The use of antibiotics must also be monitored in real-life everyday clinical practice. The nursing coordinator collects and reports to the hospital pharmacist any adverse reactions to antibiotics to confirm or otherwise the initial risk/benefit ratio with which the drug was marketed.
CONCLUSIONS
The effects of resistance, i.e., the inability of antibiotics, administered at therapeutic doses, to reduce survival or inhibit the replication of pathogenic bacteria, can be observed worldwide. Recently, the phenomenon has been further aggravated by their often inappropriate use.
The implementation of AS programmes in all health authorities remains, at present, the best tool to harness in order to curb the phenomenon of antimicrobial resistance.
The discovery of new molecules with antimicrobial activity capable of treating infections by multiresistant microorganisms is not an immediate tool; years of preclinical and clinical studies are required for a new molecule to be marketed. The phenomenon of antimicrobial resistance is urgent and requires an immediate solution to combat it. Increasingly more specialised figures are needed in the field of infectious diseases than just clinicians, and therefore hospital pharmacists and nursing staff must also be adequately trained to be able to give their best possible support in the battle against antimicrobial resistance.
LIMITATIONS
The work conducted is based on prescription forms and consumption data of antibiotics used by injection or orally. The work considers a limited geographical area. Lastly, a further limitation of the study is the lack of inferential analysis of our data.
Ethical considerations
No formal approval by the Local Ethics Committee was necessary for this type of study, since it is a publication concerning consumption data and aggregated data.
No economic incentives were provided for this analysis. Authorisation for the use of prescription forms was issued by the Hospital’s Medical Director, the consumption data derive from reports certified by the Corporate Management Control. The participants’ anonymity was ensured. The study was conducted in accordance with the ethical considerations of the Declaration of Helsinki.
Funding statement
This research did not receive any specific contributions from public, commercial or non-profit funding bodies.
Conflicts of interest
The authors do not report any conflicts of interest.
Contributions of the authors
All authors contributed equally to the production of this study.
REFERENCES
- Akpan, M.R., Ahmad, R., Shebl, N.A., et al. A review of quality measures for assessing the impact of antimicro- bial stewardship programs in hospitals. Antibiotics (Basel). 2016;5(1):5.
- O’Neill, J. Tackling drug-resistant infections globally: final report and recommendations. The review on antimicrobial resistance. 2016. https://amr-review.org/sites/default/files/160525_Final%20paper_with%20cover.pdf. Last accessed on July 23, 2023.
- Garau, J., Nicolau, D.P., Wullt, B., et al. Antibiotic stewardship challenges in the management of community-acquired infections for prevention of escalating antibiotic resistance. J Glob Antimicrob Resist. 2014;2(4):245–53.
- Antimicrobial resistance (AMR) Disponibile su: http://www.ecdc.europa.eu/en/activities/surveillance/EARS-Net/. Last accessed on August 19, 2023
- World Health Organization. Antimicrobial resistance Global Report on surveillance 2014. http://www.who.int. Last accessed on August 08, 2023.
- Aspetti epidemiologici in Italia Sorveglianza nazionale dell’Antibiotico-Resistenza (AR-ISS) https://www.epicentro.iss.it/antibiotico-resistenza/epidemiologia-italia. Last accessed on August 19, 2023.
- Spoorenberg, V., Hulscher, M.E, Akkermans, R.P., Geer- lings SE. Appropriate antibiotic use for patients with urinary tract infections reduces length of hospital stay. Clin Infect Dis. 2014;58(2):164–9.
- Ortega, M., Marco, F., Soriano, A., Almela M., Martinez J.A., Munoz A. et al. Epidemiology and prognostic determinants of bacteraemic catheter-acquired urinary tract infection in a single institution from 1991 to 2010. J Infect. 2013;67(4):282–7.
- Dalfino, L., Bruno, F., Colizza, S., Concia E., Novelli A., Rebecchi F.S. et al. Cost of care and antibiotic prescribing attitudes for community acquired complicated intra-abdominal infections in Italy: a retrospective study. World J Emerg Surg. 2014; 9:39.
- Magill, S.S., O’Leary, E., Janelle, S.J., Thompson D.L., Dumyati G., Nadle J. et al. Changes in Prevalence of Health Care-Associated Infections in U.S. Hospitals. N Engl J Med. 2018; 379(18):1732-1744
- Karki, T., Plachouras, D., Cassini, A., Suetens C. Burden of healthcare-associated infections in European acute care hospitals. Wiener Medizinische Wochenschrift. 2019; 169: 3–5.
- Goff, D.A., Rybak, M.J. Global antimicrobial stewardship: challenges and successes from frontlinestewards. Infect Dis Ther. 2015;4(Suppl 1):1–3.
- Society for Healthcare Epidemiology of America. Infectious dis- eases society of America, pediatric infectious diseases society. policy statement on antimicrobial stewardship by the Society for Healthcare Epidemiology of America (SHEA), the Infectious Diseases Society of America (IDSA), and the Pediatric Infectious Diseases Society (PIDS). Infect Control Hosp Epidemiol. 2012;33(4):322–7.
- Dellit, T.H., Owens, R.C., McGowan, J.E., Gerding D.N., Weinstein R.A., Burke J.P. et al. Infectious diseases society of America and the society for healthcare epidemiology of America guidelines for developing an institutional program to enhance antimicrobial stewardship. Clin Infect Dis.2007;44(2):159–77.
- European Centre for Disease Prevention and Control. Proposals for EU guidelines on the prudent use of antimicrobials in humans, 2017. https://www.ecdc.europa.eu/en/publications-data/proposals-eu-guidelines-prudent-use-antimicrobials-humans. Last accessed on July 23, 2023.
- Decreto Assessoriale n. 703 del 04/08/2020 della Regione Sicilia http://pti.regione.sicilia.it/portal/page/portal/PIR_PORTALE/PIR_LaStrutturaRegionale/PIR_AssessoratoSalute/PIR_Infoedocumenti/PIR_DecretiAssessratoSalute/PIR_DecretiAssessoriali/PIR_DecretiAssessorialianno2020/DA%20N.%20703.pdf. Last accessed on July 23, 2023.
- Direttiva Regionale CRE (DASOE/8/21932) https://www.qualitasiciliassr.it/sites/doc/cre/direttiva_cre_dasoe21392_29042021.pdf. Last accessed on July 23, 2023.
- Piano Regionale della prevenzione 2020-2025. http://www.quadernidellasalute.it/portale/prevenzione/DELIBERE_PRP_2020-2025/Sicilia/Allegato_1-PRP_23_12_2020-2025_integrato.pdf. Last accessed on July 23, 2023.
- Gli strumenti: il metodo di classificazione secondo il sistema ATC/DDD Bollettino d’informazione sui farmaci. Anno IX N. 6. http://www.agenziafarmaco.gov.it/wscs_render_attachment_by_id/111.61850.1150390484813676c.pdf?id=111.61855.1150390485109. Last accessed on August 08, 2023.
- L’uso degli antibiotici in Italia Rapporto Nazionale Anno 2021. https://www.aifa.gov.it/documents/20142/1853258/Rapporto_Antibiotici_2021.pdf Last accessed on August 08, 2023.
- Gilchrist, M., Wade, P., Ashiru-Oredope, D., Howard P., Sneddon J, Whitney L. et al. antimicrobial stewardship from policy to ptice: experiences from UK antimicrobial pharmacists. Infect Dis Ther. 2015;4(Suppl 1):51–64.
- Barlam, T.F., Cosgrove, S.E., Abbo, L.M., MacDougall C., Schuet A.N., SeptimusEJ., et al. Implementing an antibiotic stewardship pro- gram: guidelines by the infectious diseases Society of America and the society for healthcare epidemiology of America. Clin Infect Dis. 2016;62(10): e51–77.
![]() This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
Increasing Diversity at the Highest Levels of Nursing: Perspectives of a Doctor of Nursing Practice Graduate
Monica Jaramillo1*
- Independent Author, Florida, US.
*Corresponding Author: Monica Jaramillo DNP, MSN/Ed., RN-NLC, CNE®n, CCRN.
Instructor, mentor, and tutor of various healthcare programs. I am not affiliated with any institution when writing and submitting this manuscript to the NSC journal for open-access publication.
Florida, US. Email: MonicaJaramilloDNP@Gmail.com
Open Researcher and Contributor ID: https://orcid.org/0009-0005-0572-4061

Cite this article
Abstract
Introduction: There is a need to increase diversity at the highest levels of education in nursing to ensure competent transcultural services for the growing multicultural population worldwide. The Doctor of Nursing Practice (DNP) is a terminal degree that significantly impacts change advocacy. This commentary includes the perspectives of an immigrant nurse in her journey to completing a doctoral degree while contributing to diversity.
Discussion: Diversity, Equity, Inclusion, and Accessibility (DEIA) positively impacts nursing and healthcare systems at many levels. It is imperative to advocate for equal services for all individuals while inspiring nurses and other healthcare professionals to further their careers by achieving advanced education degrees conducive to propelling health services forward. The author seeks to inspire nurses worldwide to continue their educational journey and encourage immigrants to believe they can do it despite their fears and hesitation.
Keywords: Diversity; Equity; Inclusion; Accessibility; DEIA; Doctor of Nursing Practice.
Introduction
Immigrant nurses can face many challenges when trying to succeed in a place away from home, and this can negatively affect their desire to return to school and achieve higher degrees of education, especially terminal degrees such as the Doctor of Nursing Practice (DNP). Individuals moving to different countries must perform under the same standards as those with inherent language and culture.[1,2] Recent literature suggests that many challenges employees, employers, students, and organizations face regularly relate to the lack of adequate cross-culturalism competencies.[3] Furthermore, professionals from different geographic areas, such as Taiwan and Mexico, report experiencing multiple challenges in succeeding in scholarly endeavors with English as an additional language.[5] Accordingly, increasing diversity at all levels of health care and the nursing profession is imperative to ensure competent transcultural services for the growing multicultural population.[4] This article aims to inspire other nurses to pursue their call for further education while adding to diversity in nursing at the doctoral level worldwide. This author is a Latin-American intensive care nurse and nurse educator who completed the DNP program in the United States despite multiple fears resulting from being an immigrant nurse and a busy young mother in another country with English as an additional language. The author shares her journey through international open access, hoping it will inspire others experiencing any dilemmas related to Diversity, Equity, Inclusion, and Accessibility (DEIA) while considering achieving advanced education degrees. This commentary article includes a discussion and a conflict of interest statement while exploring the importance of taking the first step, believing in self, and abiding by solid values.
Discussion
Taking the First Step
Coming from a country where English is not the primary language can pose a significant barrier to diverse nurses from various geographic areas since advancing their careers in a different country by increasing their education without having the full command of the new language can slow down the learning process by adding fear and intimidation. In addition, English remains the dominant language for academic projects and scientific publications worldwide.[5] At first, the author experienced hesitation in enrolling in the DNP program due to language and other barriers that could arise due to disparities. But the persistent call to serve others and the burning passion for adding to diversity while advancing her career inspired her to take the first step. That initial decision was to continue advanced education programs like the master’s degree and related certificates until reaching the highest degree in nursing without forgetting to embrace her differences as an immigrant and follow her passion for the profession and service. Since then, the author has enjoyed inspiring nurses and allied health students to put their fears aside. After overcoming all fears and limiting beliefs, the author became a role model for other nurses. As a role model for the profession, the author has ensured excellence and professionalism in clinical and academic practices while engaging in life-long learning conducive to expanding knowledge, skills, and attitudes personally and professionally. In this author’s experience, taking the first step, per their individual goals and aspirations, can initiate a cascade of events that eventually will lead to empowerment and successful decisions.
Believing in Self
Another crucial element of success in higher education degrees is to believe in and honor the self. Self-confidence is vital to ensure not only the completion of projects but also positive outcomes.[6] In this author’s experience, this means being confident in individual abilities and embracing all skills and differences. Early in her educational journey, while living in a country away from home, the author learned that having a solid and positive relationship with herself was vital to her growth and expansion. Self-reflection while exploring innovative ways to cultivate self-love and self-motivation was crucial to her drive to complete all advanced nursing education. This author has always seen herself as a person with big dreams. Still, it was not until she started trusting in her competencies and believing she could accomplish anything that she started impacting herself and others around her. All nurses, immigrants or not, worldwide must believe in their abilities and capabilities while ensuring a positive self-image and respect for their differences.
Abiding by Solid Values
Values and beliefs are also vital components of successful educational pathways. Values in the nursing profession are essential foundations to ensure safe, effective, and meaningful practices.[7,8] This author knew she needed to be true to herself while expanding her nursing knowledge and skillsets, mainly since she lives far from most of her family and support systems. Since the author’s values represent the framework influencing her decisions as a nurse and student, she needed to align all core values with her selected terminal degree. For example, her values have always helped her carry out the nursing practice with integrity while doing what is best for everyone involved. Also, one of this author’s passions is translating research evidence into all professional practices with active participation in change advocacy conducive to diversity and equal opportunities for all human beings. Therefore, she sought advanced educational programs that would lead her to give back to the nursing profession through leadership, scientific publications, and professional endeavors while engaging in cutting-edge research, evidence-based practice, and professional literacy. The author is now using all those experiences and her background as an immigrant to contribute at a grander scale to diversity in nursing while advocating for others to join similar efforts.
Inspiration
In conclusion, these personal and professional stories seek to inspire many to believe in themselves and advocate for DEIA. Overcoming the fear of being an immigrant nurse in another country wanting to achieve a terminal degree of education entitles taking the first step, believing in self, and abiding by solid core values. The author sincerely hopes nobody lets their diverse and unique talents die without exploring and sharing them with the world. People can accomplish anything they desire with hard work and determination. The world needs diversity today more than ever, considering the growth of multicultural groups, and each nurse’s unique background can signify a tremendous contribution to inclusion at all levels of the nursing profession.
Funding Statement
This research received no external funding.
Conflict of Interest Statement
The author declares no conflict of interest.
References
- Larsen R, Mangrio E, Persson K. Interpersonal communication in transcultural nursing care in India: A descriptive qualitative study. Journal of Transcultural Nursing. 2020;32(4).
- Oducado RMF, Sotelo M, Ramirez LM, Habaña M, Belo-Delariarte RG. English Language proficiency and its relationship with academic performance and the nurse licensure examination. Nurse Media Journal of Nursing. 2020;10(1).
- Comeaux E, Grummert SE, Mireles DC. A critical review of the literature on cultural competency in student affairs: Toward transformative cultural responsiveness. Journal of Diversity in Higher Education. 2021.
- McFarland MR, Wehbe-Alamah HB. Leininger’s Theory of Culture Care Diversity and Universality: An overview with a historical retrospective and a view toward the future. Journal of Transcultural Nursing. 2019;30(6).
- Hanauer DI, Sheridan CL, Englander K. Linguistic injustice in the writing of research articles in English as a second language: Data from Taiwanese and Mexican researchers. Written Communication. 2018;36(1).
- Costa RR de O, Medeiros SM de, Coutinho VRD, Mazzo A, Araújo MS de. Satisfaction and self-confidence in the learning of nursing students: Randomized clinical trial. Escola Anna Nery. 2020;24(1).
- Poorchangizi B, Borhani F, Abbaszadeh A, Mirzaee M, Farokhzadian J. The importance of professional values from nursing students’ perspective. BMC Nursing. 2019;18(1).
- Turale S, Meechamnan C, Kunaviktikul W. Challenging times: Ethics, nursing and the COVID‐19 pandemic. International Nursing Review. 2020;67(2).
![]() This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
Workplace Violence Experienced by Nurses in Northern Region Hospitals of Morocco: A Cross-Sectional Study
Safae Ouma1,2, Maria Leyre Lavilla Lerma 3, Nabil Benomar3 and Nabila Rouahi4,*
1 Higher Institute of Nursing Professions and Technical Sciences, ISPITS, Boulevard Abdelkhalaq Torres, Route de Martil, 93100, Tetouan, Morocco. safaeouma21@gmail.com
2 PhD student, Faculty of Health Sciences, University of Jaen, Campus Las Lagunillas s/n, 23071 Jaén, Spain.
3 Faculty of Health Sciences, University of Jaen, Campus Las Lagunillas s/n, 23071 Jaén, Spain; llavilla@ujaen.es; nben@ujaen.es
4 Higher Institute of Nursing Professions and Technical Sciences ( ISPITS Annexe Kenitra), Route de Casablanca, 10120, Rabat, Morocco. rouahinbl@gmail.com
* Correspondence : Rouahi Nabila (Rouahi N), Professor at Higher Institute of Nursing Professions and Technical Sciences ( ISPITS Annexe Kenitra), Route de Casablanca, 10120, Rabat, Morocco.
e-mail : rouahinbl@gmail.com

Cite this article
Abstract
Background: Workplace violence (WPV) perpetrated against health professionals is a major problem in health sector. It affects health and performance of workers. The aims of this study were: 1) to assess WPV facing nurses in the northern region of Morocco and 2) to identify the related factors.
Methods: We conducted a cross-sectional study in the northern region of Morocco from October to December 2021. In total, 391 volunteer nurses working in 13 hospitals were enrolled. A self-reported questionnaire, ‘Violent Incident Form’ (VIF), was distributed to the participants. It assesses verbal and physical violence.
Results: We obtained 98% response rate and 97% of the respondent nurses faced at least one WPV episode the last year. Verbal violence is the most common type of violence. Significant factors as age of the victims (c2 = 15.34; p = 0.038) and the assaulters (c2 = 27.66; p <0.001), and mental condition of the assaulter (c2 = 28.27; p = 0.003) were obtained. According to post hoc residual z test, nurses aged between 40 and 49 and over 60 y.o were more exposed to physical violence than other groups, while the aggressors were younger aggressors (19-30 y.o.) and over 60 ; wherears significant less frequent were cases of aggressors aged between 31 and 50 y.o.
Conclusion: A high exposure of nurses to WPV in northern Moroccan hospitals is noted. The significant factors of violence obtained must be considered for the control and prevention of WPV among nurses in Moroccan hospitals.
Keywords: Morocco; nurses; hospital; verbal violence; physical violence; workplace violence; questionnaire
Introduction
The Workplace violence (WPV) is a worldwide problem within the healthcare sector. The effect of this phenomenon on the performance of an organization makes it a serious issue that we should study in all dimensions. The World Health Organization classifies workplace violence into physical and non-physical violence [1]. This publication specifies that these categories of WPV include physical assault, homicide, verbal abuse, bullying/mobbing, sexual/racial harassment, and threatening behavior. The National Institute for Occupational Safety and Health also defines it as a violent act, including physical assaults and threats of assault directed toward persons at work or on duty [2]. Other classifications, based on the relationship between the two parties involved in the incident, are also known [3, 4].
The notified incidence of violence in the health sector constitutes almost a quarter of all the incidents of WPV perpetrated in all the other sectors [5]. Consequently, WPV affects the work demand [6], the quality of healthcare, and the psychological state of the health workers [7].
In health facilities, 52.2% to 87.3% of health workers reported an experience of physical violence during their careers. Many more are threatened or exposed to verbal abuse. Patients and visitors are responsible for a great number of incidents [8]. Pich and Roche [8] confirmed that all the categories of health workers are concerned with WPV, but the highest rate of reported cases is observed among nurses and midwives in both public and private sectors and different geographic areas.
According to Cebrino et al, a worldwide bibliometric analysis reveals that the number of studies on WPV perpetrated against healthcare personnel grew between 1992 and 2019 [9]. Most reported WPV factors include psychological setting, illness of the perpetrators, miscommunication, younger nurse age, and alcohol use [10]. Chapman et al. [11] identified the predicting behaviors that must alert nurses on the occurrence of a WPV incident and then help them manage it. It was found that nurses suffer from WPV approximately two times more than physicians [12]. Despite the growing interest and the high number of studies published on WPV perpetrated against healthcare workers, this phenomenon is still underestimated. According to Kvas and Seljak, this is due to unreported cases and a large tolerance of WPV among health professionals [13].
In Morocco, non-medical health professionals represent 56% of health human resources; physicians represent 22% and administrates 22% [14]. The first category of health personnel includes Nurses (69%), Midwives (16%), Health technicians such as medical analysis laboratory and imagery personnel (11%), rehabilitation personnel (4%), and social worker (1%). According to the same document, 60% are female gender and 40% are male gender.
The first study conducted in Morocco on WPV in the healthcare sector was published in 2010 [15]. Moroccan healthcare workers are at high risk of exposure to WPV [16]. A report on the Moroccan working environment showed a higher workload and higher stress levels in the workplace [17]. Additionally, the same authors observed the absence of an ergonomic workplace, the non-availability of resources, and the ignorance of consequences of exposure to violence in the Moroccan healthcare sector. The reality is that few data are available and published on WPV in the Moroccan health sector.
For a better control and prevention of this phenomenon, it is important to know the occurrence and the factors associated with WPV perpetrated against nurses in Moroccan hospitals. To intervene and manage these incidents as quickly as possible, nurses need to be able to know and identify factors that can alert them to the possibility that a violent incident may occur [11]. This interest is in line with policies issued by Moroccan Health authorities. Additionally, Moroccan high governmental authorities and health authorities adopted laws and procedures to be applied in the case of any kind of aggression facing health professionals in their workplace. The authorities adopted this strategy during the year 2021.
The study questions are 1) What is the occurrence of the WPV in northern region hospitals of Morocco and 2) What are the factors related to WPV among nurses exposed to WPV in the hospitals of this area. Only 1 study has investigated this phenomenon in Morocco, specifically in the emergency unit of the national hospital located in Rabat city.
Objectives
The aims of this study were 1) to assess the WPV perpetrated against nurses in hospitals of the northern area of Morocco and 2) to identify the related factors.
Materials and Methods
Study area, study design and tool
We performed a cross-sectional field study. The study was conducted in a geographic area located in the north-west of Morocco (35.2630° N, 5.5617° W). Mediterranean Sea borders this area from the north and the Atlantic Ocean from the west. Rabat-Salé- Kénitra region and Fès-Meknès region border the area from the southeast and the east. A total of 12.5 million of inhabitants live in this area. The estimated number of non-medical health professionals working in the hospitals of this area was 1749.
To achieve the aims of our study, we adopted a self-reported questionnaire, Violent Incident Form (VIF). This questionnaire was initially developed by Arnetz [18], and used after that in several WPV survey studies [7, 19, 20]. The VIF assesses verbal violence and physical violence (spitting, biting, kicking, scratching/pinching, slapping/hitting punching, pushing, restraining, use of object or weapon, others). It reports also the circumstances, perpetrator, reactions and consequences of the violence. The questionnaire consists of 18 questions with binary (Yes/No) or multiple-choice responses. One section describes the characteristics of the victim and the aggressor. The other section describes the related factors of WPV experienced by nurses over the preceding 12 months.
Authorizations and ethical consideration
In accordance with the Declaration of Helsinki, we first obtained the authorization of the Regional Health Authorities and the approval of the Ethics Committee (protocol code 28/2021). Anonymous identification, data protection, and voluntary participation were ensured. Additionally, all the participants in the study gave their written agreement to participate in the survey by filling out a consent form.
Subjects, sampling, recruitment and data collection procedure
Participants were enrolled according to these inclusion criteria: being nurse and working for at least 2 years in the hospital as full-time worker. We excluded nursing students and nursing trainees. We unexpectedly visited the hospitals of the study area. The procedure to recruit the eligible subjects is the following. We went to each nurse’s supervisor in each hospital and asked him to distribute, among the eligible nurses, the pack of supports and tools of this survey. The individual pack contained the VIF questionnaire, along with a cover letter and a consent form. The sample size was estimated by Bernoulli sampling [21], according to the following formula.

We considered the central value of the prevalence interval as the representative value of the interval, i.e. 70%, IC=95%, Z-score 1.96 and a Δ=5%. In this way the minimum size was estimated equal to 323 nurses. We expanded the estimated sample up to 379 to reduce any statistical bias, due to any questionnaires not completed or with missing data. In this regard, we distributed 391 questionnaires. We recruited 387 volunteers and consenting nurses. The nurses were asked to describe the most significant WPV incident that they experienced during the 12 months preceding the study, as indicated in the VIF. Among the volunteers, 379 nurses experienced a WPV incident. They completed the questionnaire independently and anonymously. Afterwards, they deposited the completed questionnaires in a sealed box that we previously distributed in each hospital. Then, we collected the boxes 15 days after. The period of data collection lasted from October to December 2021.
Statistical analysis
We analyzed the data using the package IBM SPSS Statistics for Windows, version 21.0. Armonk, NY: IBM Corporation. Multiple responses were possible on the section of the checklist dealing with type of violence and other variables. The type of violence as dependent variable was categorized into verbal violence, physical violence (spitting, biting, kicking, scratching/pinching, slapping/hitting, punching, pushing, restraining, use of object or weapon) and Both, based on the approach of these authors [22]. Descriptive statistics were conducted to determine the characteristics of the study sample. Data were presented as frequencies and percentages. The multicomparison chi-square test was used to define significant differences among groups. Fisher’s exact test was used where the chi-square test was not appropriate. If the statistical test considering all options of responses for an item was positive (p-value <0.05), then the highest percentage value for an option was compared statistically to the sum of the percentages of all the other options, in order to point out probable triggers of WPV. Additionally, we performed a post hoc multiple chi-square test or multiple Fisher’s exact test (if the chi-square test or Fisher’s exact test were significant) to identify significantly more or less frequent categories. We applied the 2 tailed residual z test for significant variables. A value higher than +1.96 standard deviations is considered significant. The critical value is the same for each tail. All tests with p< 0.05 were considered significant.
Results
Demographic characteristics of the victims and the assaulters
We distributed the questionnaires to 391 nurses working in hospitals located in the study area. In total, 387 nurses informed the questionnaire with 98% response rate. Among the respondents, 97% of the nurses experienced at least one WPV episode during the preceding year. The demographic characteristics of the assaulted nurses and the assaulters are illustrated in Table 1.

Table 1. Demographic data of victims and WPV perpetrators in hospitals, northern region of Morocco, 2021.
Our data showed that the majority of the nurses (78%) aged less than 39 years old. The sex ratio (Male-to-Female) was 0.7. Most of the victims were females (60%), whereas most of the assaulters were male (70%). The majority of assaulters aged between 31 and 50 years old.
Violence pattern among nurses
The data on the type of violence facing nurses are presented in Table 2. The most common type of violence was verbal violence (70 %). The main forms of physical violence were Slapping/Hitting (29 %) and Kicking (26 %).

Table 2. Type of WPV facing nurses (n=379) in northern region hospitals of Morocco, 2021.
Profile of the victims and the aggressors
The data on the profile of the victims, aggressors and factors related to WPV are illustrated in Table 3.
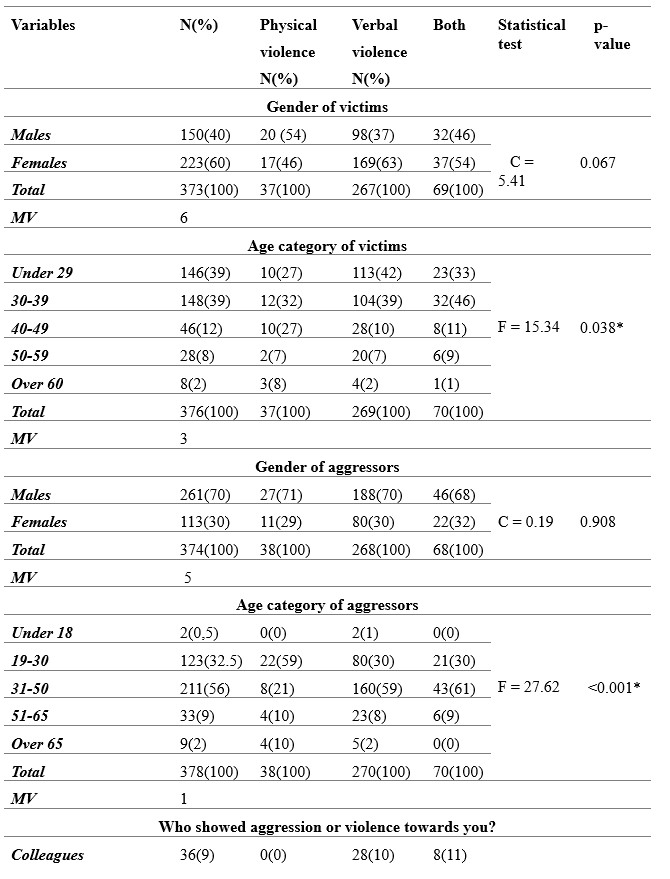

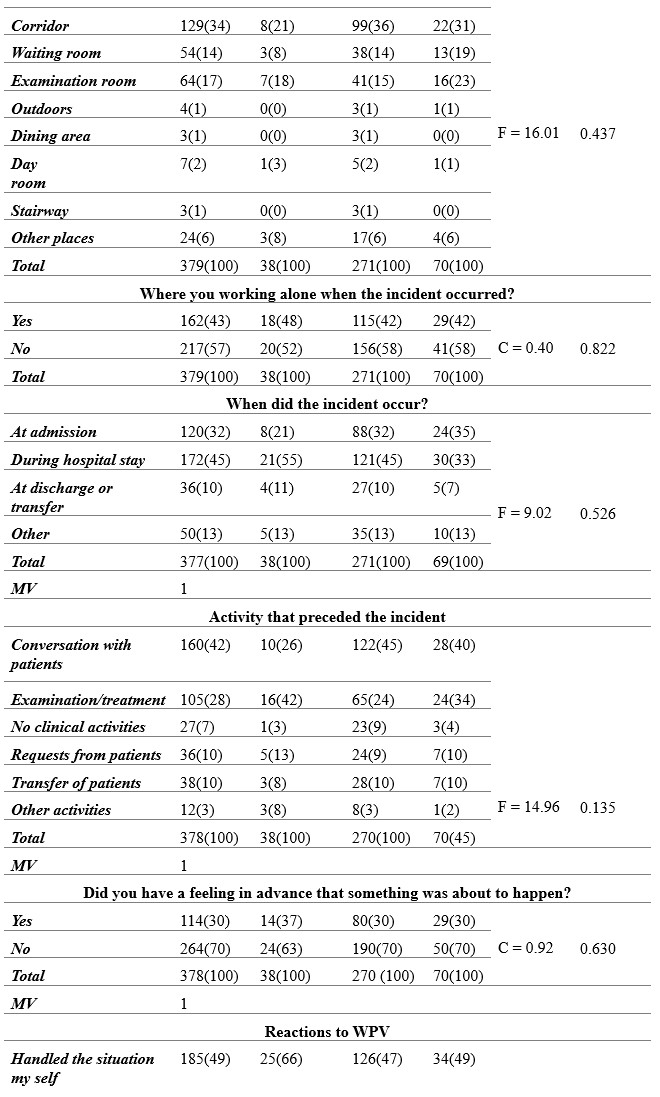
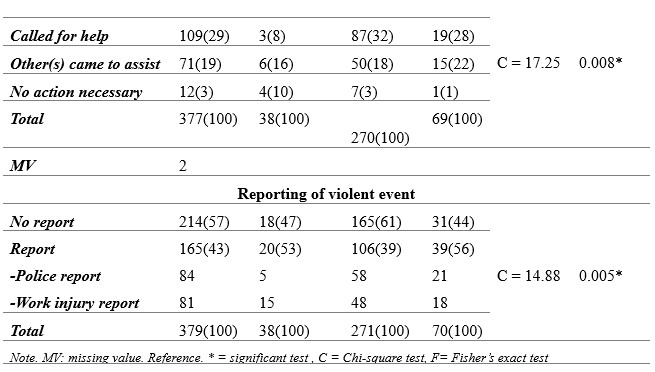
Table 3. Circumstances and factors associated with violence using VIF questionnaire among nurses, Morocco, 2021.
The data on the post hoc statistics, based on 2 tailes residual z test for significant variables previously obtained using Chi-square or Fisher tests, are reported in Table 4.
Considering the profile of the victims, our results indicated that nurses having less than 39 years old were significantly more exposed to WPV than the elders (c2 = 15.34; p = 0.038). Focusing on 40-49 and 60 or older age groups of the victims, the standardized residuals are significant for physical violence. This finding suggests a significant positive association between 40-49 (z = 2.6) and 60-older age groups (z = 2.5) and the physical violence.
Regarding the aggressors, we found that males perpetrate more violence than females. Neverthless, this result was not statistically significant. We observed that the age category of the aggressor was significantly associated with violence (c2 = 27.66; p < 0.001). The aggressors belonging to 31-50 years old age category perpetrated more WPV than other age categories. Comparing this age category to the others, we found that this interval can be considered as a trigger of WPV (p < 0.001).
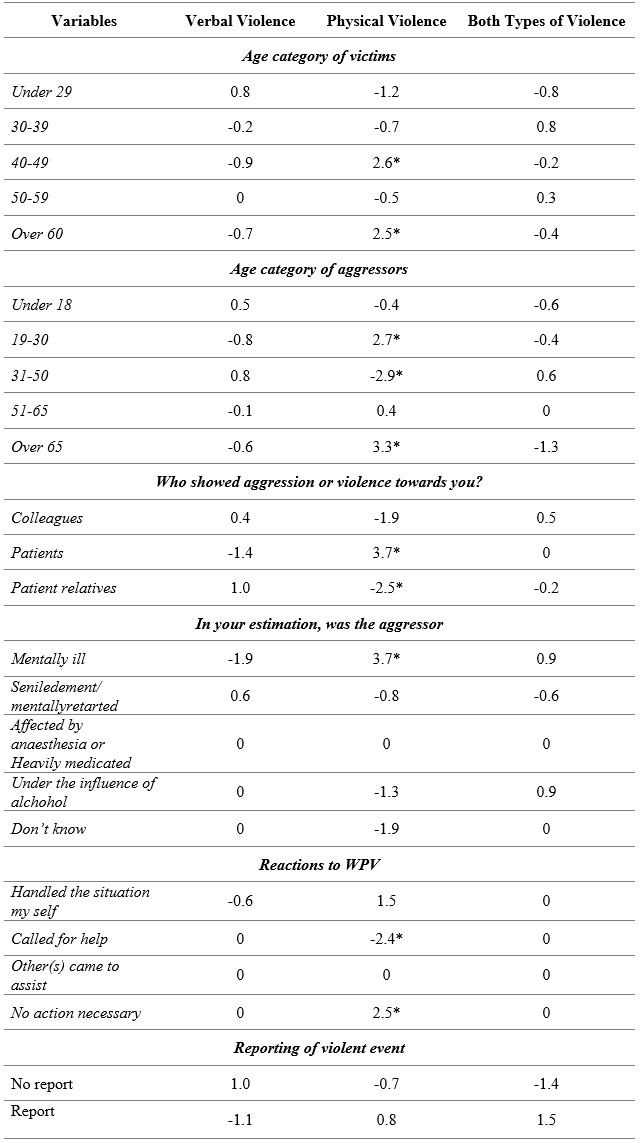
Table 4. Post hoc statistics, based on 2 tailes residual z test applied to significant risk factors of WPV experienced by nurses, Morocco 2021. Significant z values were marked with an asterisk.
Additionally, post hoc statistics based on residual standardized z test, were significant for 19-30 and over 65 age groups of the aggressors (z = 2.7 and z = 3.3 respectively) for physical violence. This result indicates a significant positive association between these age grousp and physical violence. At the opposite, we obtained a significant negative association between 31-50 age group and physical violence (z = – 2.9).
With regards to the nature of the relationship between the parties involved in the incident, the data showed that this factor was strongly and significantly associated with violence (c2 = 28.17; p < 0.001). The most frequently notified profile of the aggressor was the patient’s relatives (50%). Comparing this profile of the perpetrator to the others, we found that patient’s relatives is probably a trigger of WPV (p = 0.001). Moreover, according to post hoc statistics based on residual standardized z test, we obtained that the profile ‘Patients’ was positively associated with physical violence (z = 3.7) and ‘Patients relatives’ profile was negatively associated with physical violence (z = – 2.5).
Considering the emotional and psychological state of the aggressor, it was significantly associated with violence (c2 = 28.28; p = 0.003). Comparing the state of the aggressor ‘Mentally ill’ to the other states, we found that the mentally ill aggressor can be considered as a significant alerting factor of violence (p = 0.006). On the other hand, the standardized residual z test indicated that ‘Mentally ill’ aggressor’s state is positively associated with physical violence (z = 3.7). This finding suggest that mentally ill aggressors are more likely authors of physical violence than the aggressors with other mental and psychological disorders.
Circumstances and factors associated with WPV
Considering the circumstances of the violence, the time of violent incidents was not significantly associated with WPV. Nevertheless, we observed that aggressive episodes occurred with a high frequency throughout daily shift (68%). About the place of WPV occurrence, the corridors were the most frequently signalized place (34%) than other places. However, the result was not statistically significant. Regarding the situation if the victim was working alone or not, the frequency of violence was slightly high (57%) when the victim was not working alone.
Looking for which step during the patient journey the incidents occur mainly, we observed that most of the events occurred during the hospital stay (45%) and at admission (32 %). Nevertheless, the results were not statistically significant.
Considering the activities preceding the incident, we found that ‘Conversation with the patient’ was the most frequent (42%), followed by ‘Examination/treatment’ (28%).
Prediction, reactions and management of workplace violence
Considering the feeling in advance that something was about to happen, most of the victims (70%) responded by No. This result indicates that the great majority of the nurses were not able to identify suspicious behaviors.
Regarding the reactions to WPV, half of the victims opted for handling the situation themselves and this result was statistically significant (c2 = 17.96; p = 0.008). Comparing the option ‘Handled the situation my self’ to all the other options, we found that this option is a probable trigger of WPV (p = 0.088). Post hoc residual statistics showed a negative association of the option ‘Call for help with physical violence (z = -2.4). About the option ‘No action necessary’, residual statistics showed a positive association with physical violence. in general, the results on the reactivity of the nurses express a non-responsiveness.
Our data showed a low reporting level of the violence occurring in Moroccan hospitals. We observed that 57% of the nurses did not formally report the violence in a police report or a work injury report. This result was statistically significant (c2 = 14.9; p = 0.005). Finally, Data indicates that the most frequent negative effect of WPV on the nurses was the psychological problem (74%).
Discussion
In this study, we have explored the occurrence of workplace violence among nurses and the associated factors in northern region hospitals of Morocco. It presents the first data on occupational violence facing nurses in Morocco to our knowledge. We obtained a high exposure to WPV among nurses working in this area. This finding was similar to the data reported in these studies [6, 11, 23-28]. Moreover, comparing the WPV frequency between different studies is difficult [6, 20, 23]. This difficulty may be due to the different case definition of different categories of violence adopted by the authors, the use of different tools, and the application of different study designs. In addition, individual differences in perception of violence forms can lead to different results. Overall, verbal violence was more frequent than physical violence. In addition, Arnetz et al report that the violence pattern facing healthcare professionals is different between different health units providing different kind of healthcare [18].
Profile of the victims and the aggressors
Focusing on the age of the victims, we observed that younger nurses, i.e., under 39 years old, faced more workplace violence than elderly nurses. This finding is consistent with the literature [10, 29, 30]. We suggest the insertion of a training module on the management and prevention of WPV in the nursing academic course and the first years after employment in Moroccan health facilities.
Considering the gender of the aggressors, despite the fact that this factor was not statistically significant, but the proportion of male aggressors was very high (70%) compared to females (30%). This item was reported as a factor of violence in these studies [19, 31, 32]. Regarding the assaulter’s age, we found that it was a statistically significant factor of violence. This finding is consistent with the last cited studies.
The significantly most incriminated assaulters were the patients’ relatives. This result is supported by these studies [24, 26, 28, 32-35]. This finding may be linked to the fact that patients and their relatives have high expectations of healthcare professionals, and when they perceive that their needs are not satisfied, they may adopt aggressive attitudes [3, 36]. According to post hoc residual z test, significant statistics showed that nurses aged between 40 and 49 and over 60 y.o were more exposed to physical violence than other age categories, while the aggressors aged between (19-30 y.o.) and over 60. In addition, significant less frequent were cases of aggressors aged between 31 and 50 y.o.
These victims and aggressors age categories must be considered by the healthcare professionals in the management and the control of WPV.
Circumstances and factors associated with WPV
Despite the fact that our findings were not statistically significant, most of the incidents occurred during daily shifts. This finding is in accordance with these studies [37, 38]. Other authors obtained contradictory data [28, 32].
About WPV place, the most frequently signalized place was the corridors (35%). These data are consistent with these studies [29, 10]. The fact that the results on the circumstances were not statistically significant may be linked to the great number of the response options, the reduced number of the participants in each response option, and the limited sample size.
Prediction, reactions and management of workplace violence
Considering the feeling in advance that an incident will occur, the majority of the incidents were not expected by the nurses. This result is in accordance with the data found in the literature on the predictive factors of WPV [39]. This finding expresses a need to sensitize and inform the nurses about workplace violence. Regarding the consequences of WPV, the most negative effect was psychological problems. This result is in line with the findings of the previously cited study.
Beside this result, we obtained a low reporting of the violent incidents. This finding is in accordance with the results obtained by these authors [40, 41]. It is probably due to the lack of a notification system of WPV, the lack of information on how to report the incident, the ignorance of labor laws and rights, and the victims may believe that the reporting is useless or the act of violence is not considered a crime.
Conclusions
A high exposure of nurses to WPV in northern Moroccan hospitals is noted. Verbal violence is more predominant than physical violence. Considering the profile of the assaulters, the majority are male and the most incriminated are the patients’ families. Significant risk factors such as age of the victims and the assaulters were obtained. The mental condition of the assaulter is significantly associated to violence perpetrated against nurses. These results should alert policymakers about the violent workplace incidents committed in Moroccan hospitals. We recommend the conduction of large-scale studies to inform policymakers about the exact magnitude and factors of WPV in other hospitals and non-hospital settings in all regions of the kingdom. Then the implementation of a program on the prevention and management of WPV for nurses and other categories of healthcare professionals. Another preventive aspect is the setting of a WPV notification system in hospitals to help operative managers on time to address the factors that lead to workplace violence.
Limitations
Despite the fact that most of our findings are supported by the data published on workplace violence, our study has some limitations. The main limitation is that VIF asks about violence experienced the past year only. Another limitation about the severity of the violence is related to the fact that the VIF reports if the participant experienced a violent event or not, but the participant is not asked about how often he faced incidents during the year. Finally, since our study was conducted in the northern area only, our findings are not generalized to the whole population of nurses working in Moroccan hospitals or other healthcare facilities. In order to have representative results on the violence through all the country, further studies must be extended to a larger period of time and cover all the regions of Morocco.
Funding: This research received no external funding.
Institutional Review Board Statement: The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board (or Ethics Committee) of “Comithé d’Ethique pour la Recherche Biomédicale CERBO (protocol code 28/2021 and date of 11/10/2021).
Informed Consent Statement: Informed consent was obtained from all subjects involved in the study. Written informed consent has been obtained from the patient(s) to publish this paper.
Data Availability Statement: Data is unavailable due to privacy and national restrictions.
Conflicts of Interest: The authors declare no conflict of interest.
Author Contributions: Conceptualization, S.O (Safae Ouma); N.B (Nabil Benomar) and N.R (Nabila Rouahi); Methods, S.O; N.B and N.R; Software, S.O and N.R; Validation, S.O; N.B; M.L.LL (Maria LeyreLavilla Lerma) and N.R; Formal analysis: MLLL; Investigation, S.O; Resources, S.O; N.B and N.R; Data curation, S.O; N.R and N.R; Writing—Original draft preparation, S.O and N.R; Writing—review and editing, S.O; N.B; MLLL and N.R; Visualization, S.O; N.B; MLLL and N.R; Supervision, N.B and N.R; Project administration, N.B and N.R; Funding acquisition, None. All authors have read and agreed to the published version of the manuscript.
Acknowledgments: We would like to thank the nurses who participated in this research and staff of the hospitals who facilitated the fluent conduction of the study for their efforts in the data collection.
References
- Krug, E. G., Dahlberg, L. L., Mercy, J. A., Zwi, A. B., Lozano, R. (2002). World report on violence and health. World Health organization. https://apps.who.int/iris/handle/10665/42495.
- National Institute for Occupational Safety and Health. (2002). Violence : Occupational hazards in hospitals. http://doi.org/10.26616/NIOSHPUB2002101.
- Phillips, J. P. (2016). Workplace Violence against Health Care Workers in the United States. New England Journal of Medicine, 374(17), 1661‑1669. https://doi.org/10.1056/NEJMra1501998.
- Wassell, J. T. (2009). Workplace violence intervention effectiveness : A systematic literature review. Safety Science, 47(8), 1049‑1055. https://doi.org/10.1016/j.ssci.2008.12.001.
- Tuncel, E. K., Dundar, C., Sunter, A. T., Canbaz, S., &Peksen, Y. (2009). Violence towards primary healthcare workers in Samsun, Turkey. 18.Conference: 12th World Congress on Public Health World Health Organization
- Park, M., Cho, S.-H., & Hong, H.-J. (2015). Prevalence and Perpetrators of Workplace Violence by Nursing Unit and the Relationship Between Violence and the Perceived Work Environment : Workplace violence against nurses. Journal of Nursing Scholarship, 47(1), 87‑95. https://doi.org/10.1111/jnu.12112.
- Khalil, M., &Alameddine, M. (2020). Recruitment and retention strategies, policies, and their barriers : A narrative review in the Eastern Mediterranean Region. Health Science Reports, 3(4). https://doi.org/10.1002/hsr2.192.
- Pich, J., & Roche, M. (2020). Violence on the Job: The Experiences of Nurses and Midwives with Violence from Patients and Their Friends and Relatives. Healthcare, 8(4). 522. http://doi.org/10.3390/healthcare8040522.
- Cebrino, J., &Portero de la Cruz, S. (2020). A worldwide bibliometric analysis of published literature on workplace violence in healthcare personnel. PLOS ONE, 15(11), e0242781. https://doi.org/10.1371/journal.pone.0242781.
- Kamchuchat, C., Chongsuvivatwong, V., Oncheunjit, S., Yip, T. W., &Sangthong, R. (2008). Workplace Violence Directed at Nursing Staff at a General Hospital in Southern Thailand. Journal of Occupational Health, 50(2), 201‑207. https://doi.org/10.1539/joh.O7001.
- Chapman R, Perry L, Styles I, Combs S. Predicting patient aggression against nurses in all hospital areas. British Journal o Nursing. 2009. 18(8) : 476 – 483.
- Partridge, B.; Affleck, J. Verbal abuse and physical assault in the emergency department: Rates of violence, perceptions of safety, and attitudes towards security. Australas. Emerg. Nurs. J. 2017, 20, 139–145. [CrossRef]
- Kvas, A., & Seljak, J. (2014). Unreported workplace violence in nursing : Unreported workplace violence in nursing. International NursingReview, 61(3), 344‑351. https://doi.org/10.1111/inr.12106.
- Human Resources report of the Ministry of Health, 2016.
- Belayachi, J., Berrechid, K., Amlaiky, F., Zekraoui, A., &Abouqal, R. (2010). Violence toward physicians in emergency departments of Morocco : Prevalence, predictive factors, and psychological impact. Journal of Occupational Medicine and Toxicology, 5(1), 27. https://doi.org/10.1186/1745-6673-5-27.
- Giurgiu DL., Jeoffrion C., Roland-Lévy C, Grasset B., Brigitte Dessomme BK., Moret L., Roquelaure Y., Caubet A., Verger C., El Houssine Laraqui C., Lombrai Pl., Geraut C, and Tripodi D. 2016. Wellbeing and occupational risk perception among health care workers: a multicenter study in Morocco and France. J.Occup Med Toxicol. 2016; 11: 20. http://doi.org/10.1186/s12995-016-0110-0.
- Semlali H. (2010). The Morocco Country Case Study: Positive Practice Environments. Morocco Case Study: Health Care Environments in Morocco. Global Health Workforce Alliance, WHO, Geneva. http://www.who.int/workforcealliance/knowlege/resources/ppemorocco/en/index.html
- Arnetz JE, Arnetz BB, Söderman E. Violence toward health care workers. Prevalence and incidence at a large, regional hospital in Sweden. AAOHN J. 1998 Mar;46(3):107-14. PMID: 9582726.
- Ferri, P., Silvestri, M., Artoni, C., & Di Lorenzo, R. (2016). Workplace violence in different settings and among various health professionals in an Italian general hospital : A cross-sectional study. Psychology Research and Behavior Management, 9, 263‑275. https://doi.org/10.2147/PRBM.S114870.
- Magnavita, N., &Heponiemi, T. (2012). Violence towards health care workers in a Public Health Care Facility in Italy: A repeated cross-sectional study. BMC Health Services Research, 12(1), 108. https://doi.org/10.1186/1472-6963-12-108.
- Strand, M. M., Estimation of a population total under a “Bernoulli sampling” procedure. The American Statistician, 1979. 33(2), 81-84.
- Khalid GM, Idris UI, Jatau AI, Wada YH, Adamu Y, Ungogo MA. Assessment of occupational violence towards pharmacists at practice settings in Nigeria. Pharmacy Practice. 2020 Oct-Dec;18(4):2080. https://doi.org/10.18549/PharmPract.2020.4.20.
- Ayranci, U., Yenilmez, C., Balci, Y., &Kaptanoglu, C. (2006). Identification of Violence in Turkish Health Care Settings. Journal of Interpersonal Violence, 21(2), 276‑296. https://doi.org/10.1177/0886260505282565.
- Kitaneh, M., &Hamdan, M. (2012). Workplace violence against physicians and nurses in Palestinian public hospitals : A cross-sectional study. BMC Health Services Research, 12(1), 469. https://doi.org/10.1186/1472-6963-12-469.
- Alsaleem, S., Alsabaani, A., Alamri, R., Hadi, R., Alkhayri, M., Badawi, K., Badawi, A., Alshehri, A., & Al-Bishi, A. (2018). Violence towards healthcare workers : A study conducted in Abha City, Saudi Arabia. Journal of Family & Community Medicine, 25, 188‑193. https://doi.org/10.4103/jfcm.JFCM_170_17.
- Hamdan, M., & Abu Hamra, A. (2015). Workplace violence towards workers in the emergency departments of Palestinian hospitals : A cross-sectional study. Human Resources for Health, 13(1), 28. https://doi.org/10.1186/s12960-015-0018-2.
- Rafeea, F., AlAnsari, A., Musbah Abbas, E., Elmusharaf, K & Abu Zeid, M. (2017). Violence toward health workers in Bahrain Defense Force Royal Medical Services´ emergency department. Open Access Emergency Medicine, 9, 113‑121. https://doi.org/10.2147/OAEM.S147982.
- Zafar, W., Siddiqui, E., Ejaz, K., Shehzad, M. U., Khan, U. R., Jamali, S., &Razzak, J. A. (2013). Health Care Personnel and Workplace Violence in the Emergency Departments of a Volatile Metropolis : Results from Karachi, Pakistan. The Journal of Emergency Medicine, 45(5), 761‑772. https://doi.org/10.1016/j.jemermed.2013.04.049.
- Adib, S. M., Al-Shatti, A. K., Kamal, S., El-Gerges, N., & Al-Raqem, M. (2002). Violence against nurses in healthcare facilities in Kuwait. International Journal of Nursing Studies, 39(4), 469‑478. https://doi.org/10.1016/S0020-7489(01)00050-5.
- Alameddine, M., Mourad, Y., &Dimassi, H. (2015). A National Study on Nurses’ Exposure to Occupational Violence in Lebanon : Prevalence, Consequences and Associated Factors. PLOS ONE, 10(9), e0137105. https://doi.org/10.1371/journal.pone.0137105.
- Gerberich, S. G. (2004). An epidemiological study of the magnitude and consequences of work related violence : The Minnesota Nurses’ Study. Occupational and Environmental Medicine, 61(6), 495‑503. https://doi.org/10.1136/oem.2003.007294.
- Lei, Z., Yan, S., Jiang, H., Feng, J., Han, S., Herath, C., Shen, X., Min, R., Lv, C., & Gan, Y. (2022). Prevalence and Risk Factors of Workplace Violence Against Emergency Department Nurses in China. International Journal of Public Health, 67, 1604912. https://doi.org/10.3389/ijph.2022.1604912.
- Algwaiz, W. M. (2012). Violence exposure among health care professionals in Saudi public hospitals. Saudi Med J. 2012. 7.
- Muñoz del Carpio-Toia, A., Begazo Muñoz del Carpio, L., Mayta-Tristan, P., Alarcón-Yaquetto, D. E., & Málaga, G. (2021). Workplace Violence Against Physicians Treating COVID-19 Patients in Peru : A Cross-Sectional Study. The Joint Commission Journal on Quality and Patient Safety, 47(10), 637‑645. https://doi.org/10.1016/j.jcjq.2021.06.002.
- Sachdeva, S., Jamshed, N., Aggarwal, P., & Kashyap, S. (2019). Perception of workplace violence in the emergency department. Journal of Emergencies, Trauma, and Shock, 12(3), 179. https://doi.org/10.4103/JETS.JETS_81_18.
- Usman, N., Dominic, B., Nwankwo, B., Nmadu, A., Omole, N., & Usman, O. (2022). Violence towards health workers in the workplace : Exploratory findings in secondary healthcare facilities in Kaduna metropolis, Northern Nigeria. Babcock University Medical Journal, 5(1). https://doi.org/10.38029/babcockunivmedj.v5i1.118.
- Albashtawy, M., Al-Azzam, M., Rawashda, A., Batiha, A.-M., Bashaireh, I., &Sulaiman, M. (2015). Workplace Violence Toward Emergency Department Staff in Jordanian Hospitals : A Cross-Sectional Study. Journal of Nursing Research, 23(1), 75‑81. https://doi.org/10.1097/jnr.0000000000000075.
- Fernandes, C. M. B., Raboud, J. M., Christenson, J. M., Bouthillette, F., Bullock, L., Ouellet, L., & Moore, C. F. (2002). The effect of an education program on violence in the emergency department. Annals of Emergency Medicine, 39(1), 47‑55. https://doi.org/10.1067/mem.2002.121202.
- Alshahrani, M., Alfaisal, R., Alshahrani, K., Alotaibi, L., Alghoraibi, H., Alghamdi, E., Almusallam, L., Saffarini, Z., Alessa, S., Alwayel, F., Saffarini, L., Alrawdhan, A., Mapusao, C., Asonto, L. P., Alsulaibikh, A., &Aljumaan, M. (2021). Incidence and prevalence of violence toward health care workers in emergency departments : A multicenter cross-sectional survey. International Journal of Emergency Medicine, 14(1), 71. https://doi.org/10.1186/s12245-021-00394-1.
- Garg, R., Garg, N., Sharma, D.K., Gupta, S. (2019). Low reporting of violence against health-care workers in India in spite of high prevalence. Medical Journal Armed Forces India. 75. 211-215. doi: 10.1016/j.mjafi.2018.11.011.
- Alfuqaha O., Albawati N., Alhiary S., Alhalaiqa F., Haha M., Musa S., Shunnar O and AL Thaher Y 5. (2022). Workplace Violence among Healthcare Providers during the COVID-19 Health Emergency: A Cross-Sectional Study. Behav. Sci. 2022, 12, 106. https://doi.org/10.3390/bs12040106.
![]() This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
Systems compared: Capillary glucose self-monitoring and Flash glucose monitoring system. Cross-sectional study
Francesco Saverio Auricchio¹*, Maria Russo²,
Maddalena Lettieri¹, Nicolas Craparotta¹
¹Department of Translation Medical Sciences, University Federico II, Naples.
²San Giovanni di Dio Civil Hospital of Frattamaggiore, Asl Naples 2 North, Naples.
*Corresponding author: Francesco Saverio Auricchio, Department of Translation Medical Sciences, University Federico II, Naples.
Email: francescosaverio.auricchio@unina.it

Cite this article
ABSTRACT
Introduction: In recent years, with the rapid advancement of technology, tools capable of minimising discomfort for the diabetic patient are becoming increasingly popular, thereby increasing adherence to treatment. The use of technology improves glycometabolic compensation and quality of life.
Objective: The aim of the present study is to verify, in the group using the Flash Glucose Monitoring system, improved diabetes management and satisfaction in insulin-treated patients.
Materials and Methods: A retrospective cross-sectional study was performed through the administration of the “Diabetes Treatment Satisfaction Questionnaire”. The study was performed from January to July 2019. 82 validated questionnaires were administered in the Italian version. Participants were 47 women (39 Type 1 Diabetes Mellitus and 8 Type 2 Diabetes Mellitus) and 35 men (19 Type 1 Diabetes Mellitus and 16 Type 2 Diabetes Mellitus).
Results: Results show that subjects with the Flash Glucose Monitoring system have greater satisfaction than those using the Self-Monitoring of Blood Glucose system. Patients using Flash Glucose Monitoring showed 83.9% satisfaction, while patients using Self-Monitoring of Blood Glucose showed 33.3% complete satisfaction. The average glycosylated haemoglobin of the group of subjects using Flash Glucose Monitoring was 53.2 mmol/mol, while that of subjects with self-monitoring of capillary blood glucose was 60.3 mmol/mol.
Conclusions: The adoption of new technologies has benefits for the patient that positively affect quality of life. The study showed better glycometabolic compensation in the group of patients using Flash Glucose Monitoring. Diabetes carries significant costs to public health, and prevention and improvement of care could be a primary goal for the community and health systems.
Keywords: Diabetes mellitus; Telemedicine; Technology; Flash glucose monitoring; Self-monitoring of blood glucose
INTRODUCTION
Diabetes mellitus is a chronic disease characterised by increased concentration of glucose in the blood. The vast majority of diabetes cases fall into two broad aetiopathogenic categories. In one category, Type 1 Diabetes Mellitus (DMT1), the cause is an absolute lack of insulin secretion due to an autoimmune pathological process that occurs in the pancreatic islets and/or genetic alterations. In the other category, Type 2 Diabetes Mellitus (DMT2), the cause is a combination of resistance to insulin activity and an inadequate compensatory insulin secretory response. In the latter category, a degree of hyperglycemia sufficient to cause pathological and functional alterations in various target tissues, but without clinical symptoms, may be present for a long time before diabetes is detected [1].
DMT2 is considerably the most frequent form of diabetes (it affects 90% of cases) and is typical of middle age. It emerges as a multifactorial disease that involves both genetic predisposition and multiple environmental factors [2]. In 2021, the International Diabetes Federation (IDF) estimated that 537 million were diagnosed with diabetes mellitus and predicted that this figure will reach 643 million by 2030 and 783 million by 2045. In addition, the IDF estimated that, in 2021, 541 million people had reduced glucose tolerance. The number of children and adolescents living with diabetes is constantly increasing. In 2021, more than 1.2 million children and adolescents were diagnosed with Type 1 Diabetes Mellitus.
Direct health expenditures due to diabetes are already close to $1 trillion and will exceed this figure by 2030. The 10th edition of the IDF Diabetes Atlas also shows that hyperglycaemia in pregnancy affects about one in six pregnancies. Another cause for alarm is the consistently high percentage (45%) of people with undiagnosed diabetes, which is predominantly type 2. This highlights the urgent need to improve the ability to diagnose people with diabetes, many of whom do not know they have the condition, and to provide appropriate and timely care to all people with diabetes as soon as possible [3]. One-fifth of people with type 1 diabetes are in low- and lower-middle-income countries. The residual life expectancy of a 10-year-old child diagnosed with Type 1 Diabetes Mellitus in 2021 ranged from an average of 13 years in low-income countries, to 65 years in high-income countries [4].
Diabetes therapy is often substitutive and is based on partly frequent or continuous insulin administrations. The objective of replacement therapy is to maintain blood glucose concentrations in a physiological range, trying to avoid or in any case limit both episodes of hypoglycaemia and hyperglycaemia. It is therefore necessary to continuously harmonise insulin therapy, nutrition and exercise, also taking into account the hyperglycaemic effect of stress, intercurrent diseases and, in the case of the child, even in changes in a growing body [5]. To be able to live with your diabetes, without being overwhelmed by it, you need good blood sugar control. To judge the effectiveness of the control, it is necessary to measure the reactions of the body to the treatment, even if you are not on drug therapy, but proper care is based on lifestyle changes and physical activity [6]. Through monitoring, it is possible to intervene in the most appropriate way, bringing or maintaining blood glucose levels as close as possible to the reference values [7]. The American Diabetes Association (ADA) recommends that all diabetics try by any and all means to maintain blood sugar control so as to reduce the risk of complications [8].
Diabetes, a systemic disease not to be overlooked, has chronic complications that can also be disabling and fatal. Diabetes presents macrovascular complications, including coronary heart disease, stroke, and peripheral vascular disease, and microvascular complications, such as end-stage renal disease, retinopathy, and neuropathy, along with lower limb amputations. Complications are responsible for much of the health spending associated with diabetes. There is also a growing recognition of a diverse set of causal conditions, including cancers, ageing-related outcomes (e.g. dementia), infections, and liver disease [9]. Daily monitoring of diabetes, due to frequent capillary sampling obtained by finger prick, is painful and this can make it difficult to adhere to a diabetes management plan. In recent years, thanks to the increasing number of technologies available for glycaemic monitoring and insulin administration, there has been a real revolution in the care of people with diabetes mellitus [10].
The Flash Glucose Monitoring (FGM) system avoids inconvenience to patients due to repeated capillary punctures, providing continuous measurement of blood glucose [11] through a system consisting of a small circular sensor applied to the back of the arm that, at intervals of one minute, measures glucose in the interstitial fluid, by means of a small filament inserted under the skin and held in place by a small adhesive pad. Using this circuit, the patient is able to detect blood glucose in real time, and wirelessly transmit all the information necessary to evaluate the glycaemic trend.
The purpose of this study is to look at the impact of the FGM system on glycaemic control in insulin-treated diabetic patients, verifying whether those who use the FGM system have better diabetes management, as well as a better degree of satisfaction than those who use Self-monitoring of Blood Glucose (SMBG).
MATERIALS AND METHODS
The following cross-sectional study was carried out by administering a questionnaire validated in its Italian version, found in the international literature. The Italian adaptation of the “Diabetes Treatment Satisfaction Questionnaire” (DTSQ) was used [12]. This questionnaire has been specifically designed to measure satisfaction with diabetes treatments and can be used in both patients with type 1 diabetes and those with type 2 diabetes. The level of treatment satisfaction in the two patient groups (FGM and SMBG) and the frequency of perception of episodes of hypoglycaemia and hyperglycaemia were analysed and compared. The study began in January 2019 and was completed in July of the same year. 82 questionnaires of the validated Italian version of the DTSQ were administered. The questionnaire includes 8 questions, 6 of which are added together in a single score that varies between 8 (very unsatisfied) and 36 (very satisfied). The remaining two questions, used individually, explore the perceived frequency of episodes of hypo- and hyperglycaemia [13], through an incremental score of 1 (never) to 6 (very often). We also investigated the personal characteristics of the sample (gender and age), the type of diabetes (DMT1 and DMT2), the methods of glycaemic control (SMBG and FGM) and the value of glycosylated haemoglobin (HbA1c).
The questionnaires were administered online, on Facebook™ social media and through the Google Forms™ platform, within special groups dedicated to the diabetic patient, namely Diabetica: il gruppo sul diabete tipo 1, Diabete.com, Diabetici Insieme. The survey was conducted through the use of convenience sampling. Adherence to the questionnaire was voluntary and the questionnaire was made anonymous at source. The consent to the participation and use of the data was considered acquired at the time of sending the questionnaire. The data were analysed in aggregate form. Approval by the Local Ethics Committee was not required for this type of study.
The following inclusion criteria were defined: subjects of both sexes, patients with DMT1, patients with DMT2, patients on pharmacological treatment, patients aged > 6 years. The following exclusion criteria were defined: patients aged < 6 years, patients not pharmacologically treated or patients who follow only a diet and/or physical activity.
Statistical analyses
The data collected were processed through the use of the “LibreOffice6.2™” package for descriptive statistical analysis. The same data were analysed with the statistical software “RStudio™” for the analysis of the variables under analysis. Data are presented as number and percentage for categorical variables and continuous data are expressed as mean ± standard deviation (SD), median and interquartile range (IQR). The confidence interval (CI) was calculated for mean age and HbA1c. The different variables were analysed and correlated to assess whether there were differences in diabetes management and satisfaction in the two patient groups (SMBG and FGM). The chi-squared test was performed for the two levels of satisfaction obtained in relation to the two types of treatment. The Shapiro-Wilk test was used to determine whether the variables were distributed normally and, subsequently, the non-parametric Wilcoxon-Mann-Whitney test was carried out for unpaired data, since the variables were not distributed normally. All tests with a p-value <0.05 were considered significant.
RESULTS
The sample consisted of 82 diabetic subjects, of whom 58 (70.7%) had a diagnosis of DMT1, while 24 (29.3%) had a diagnosis of DMT2.
The subjects included in the study had a variable age. The mean age was 37.5 years (95% CI: 34.1-40.9; SD=15.4). The study included the distribution of patients according to sex.
The analysis of the data showed greater participation in the completion of the questionnaire by females (47 subjects, equal to 57.3% of the sample) compared to males (35 subjects, equal to 42.7% of the sample). For the purposes of the study, patients were divided according to the type of glycaemic monitoring: SMBG and FGM. On analysing the data, it was observed, as is known, that the glycemic self-monitoring system using capillary puncture is the most widespread system.
Of the 82 subjects who participated in the study, 51 subjects used the SMBG system (62.2%) and 31 subjects (37.8%) used the FGM system. The different levels of satisfaction for the related types of monitoring were also analysed.
For the evaluation of the different levels of satisfaction, of a maximum score of 36 (sum of the maximum scores of each score), a score < 12 was considered as totally unsatisfactory, a score between 12 and 24 as partially satisfactory and finally a score between 24 and 36 as satisfactory. The scores obtained were categorised and analysed.
The results, extrapolated from the questions investigating objective data, were stratified according to gender and are reported in Table 1.

Table 1. Characteristics of 82 diabetic patients stratified by gender.
The effectiveness of diabetes treatment should not be assessed solely on the basis of HbA1c levels as it should also focus on patient-reported outcomes such as patient satisfaction, well-being and quality of life. The DTSQ was developed to assess patient satisfaction in the treatment of diabetes.
Table 2 shows the results obtained from the questionnaire.

Table 2. Summary of the percentages of responses obtained from the DTSQ questionnaire administered to 82 diabetic patients (the score for each field ranges from 1 to 6, where 1 means “very dissatisfied” and 6 means “very satisfied”).
Table 3 shows the results obtained from the DTSQ, stratified into three categories: “Satisfaction yes”, “Partial satisfaction”, “Satisfaction no”,
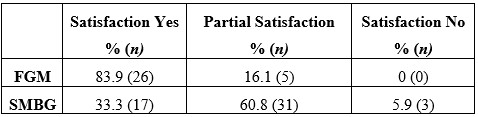
Table 3. Results obtained according to the evaluation criteria of the scale used (score < 12 = totally unsatisfactory, score between 12 and 24 = partially satisfactory, score between 24 and 36 = satisfactory).
Subjects with the FGM system show greater satisfaction than those using the SMBG system. Patients using Flash Glucose Monitoring showed 83.9% satisfaction, 16.1% partial satisfaction and 0% total dissatisfaction. Patients using capillary glucose self-monitoring, on the other hand, showed complete satisfaction for 33.3% of the sample (1 out of 3), partial satisfaction for the treatment equal to 60.8% and total dissatisfaction equal to 5.9% (Table 3).
The results obtained show that the FGM group had a dissatisfaction (satisfaction no) value of 0. The purpose of the study was to demonstrate a significant difference in satisfaction in the two different monitoring groups. The results obtained by the partially satisfied (partial satisfaction), considered as negative and not sufficient, were merged with those of the not satisfied (satisfaction no). Table 4 shows the new classification.

Table 4. Comparison between the results obtained for “satisfaction yes” and the combined results of “satisfaction no” and “partial satisfaction”
In Table 4 the results obtained for “partial satisfaction” were considered as negative values and therefore added to the values obtained for “satisfaction no”.
Table 4 shows a significant relationship between the groups and the satisfaction variable. In particular, the chi-squared test showed a significantly higher presence of satisfaction in the FGM group compared to the SMBG group (19.74, 83.9% vs 33.3%, chi-squared=19.74, p<0.0001). In other words, there is significantly greater treatment satisfaction in diabetic patients using the FGM monitoring system compared to the traditional method (SMBG). Differences in glycosylated haemoglobin were also analysed in the two patient groups. The mean glycosylated haemoglobin of the FGM group was 53.2 mmol/mol (95% CI: 49.0-57.4), while that of subjects with self-monitoring of capillary blood glucose was 60.3 mmol/mol (95% CI: 55.9-64.6).
For inferential analysis, the Wilcoxon-Mann-Whitney nonparametric test was used for two independent samples, as the data distributions were not normal. The different variables covered by the research were compared in relation to the monitoring system used by the patient (Table 5). Statistical analysis of both samples (SMBG and FGM) was performed. The samples were first analysed independently and then compared.

Table 5. Comparison between SMBG and FGM samples, regarding the different variables considered in our study, such as Satisfaction yes, HbA1c, Hyperglycaemia, Hypoglycaemia, tot DTSQ Satisfaction.
In the study sample, as seen in the descriptive statistical analysis, there was some difference between the glycosylated haemoglobins of the two groups. This comparison parameter was analysed using the Wilcoxon-Mann-Whitney test. The test showed that the difference is statistically significant, p-value= 0.029.
Another variable under study was the analysis of the frequency of perception of episodes of both
hypoglycaemia and hyperglycaemia. The frequencies of these perceptions were compared for the two classes of patients by performing an inferential analysis. With regard to the comparison of the perception of hypoglycaemic episodes, the test did not show a statistically significant difference, p-value = 0.22. The test also showed no statistically significant significance when comparing the perception of hyperglycaemic episodes, p-value = 0.30.
Finally, the degree of patient satisfaction in relation to the type of monitoring was investigated.
As seen above during the descriptive statistical analysis, there was a significant difference in satisfaction in the two groups. Statistical inference was performed to test whether the relationship between monitoring systems and satisfaction was statistically significant. The non-parametric Wilcoxon-Mann-Whitney test was chosen for two independent samples (p-value Shapiro-Wilk test = 0.024, so the distribution is not normal).
The test showed a statistically significant difference between the two groups (p-value < 0.0001).
DISCUSSION
Based on the material found in the international scientific literature, the results obtained from the study show a good match in measuring the satisfaction of diabetic patients with blood glucose monitoring. Flash glucose monitoring allows frequent glucose checks with increased time in range and reduced time in hyper- and hypoglycaemia [14]. The use of innovative tools, capable of providing greater patient comfort, is helpful in achieving better outcomes and better management of a chronic condition such as diabetes. The Impact study showed that FGM was able, in comparison to conventional systems, to increase the frequency of monitoring (up to 15 scans per day), reduce the time spent in hypoglycaemia and result in no increase in glycosylated haemoglobin at six months. FGM decreases hypoglycaemia in patients with DMT1 by an average of 74 minutes per day, with a 38% reduction compared to the control group in the 6 a.m. to 11 p.m. time slot and a 40% reduction in the time spent in hypoglycaemia in the 11 p.m. to 6 a.m. period [15].
A retrospective study, conducted in the US, and a meta-analysis, conducted in the US and Canada, showed that, with the use of the FGM system, glycosylated haemoglobin was significantly reduced in DMT2 [16].
The FGM system tends to improve treatment satisfaction, can lead to improved glycaemic control in patients with DMT2 undergoing multi-injection therapy, without increasing the frequency of hypoglycaemia [17], improving daily glycaemic control and self-care behaviour [18].
The research included the administration of the DTSQ in order to be able to analyse possible differences between the two monitoring groups and confirmed what has been stated by the various studies in the literature. The analysed sample is not representative of the entire population of diabetics as it comes from the online patient groups only, however, the patients belong to different settings as well as to different regions. In agreement with the findings in the literature, this research has shown that the use of the FGM system improves the quality of life and satisfaction of patients and promotes their well-being. The FGM system not only benefits the patient, who has greater awareness of glucose trends throughout the day, but also benefits the physician himself, who can better monitor diabetes compensation, hypoglycaemic and hyperglycaemic load in order to make the necessary changes to drug treatment [19]. Research has shown the benefits of using innovative monitoring systems.
This system is easy to wear and, with a painless scan, allows the measurement of glucose levels in the interstitial fluids of people with diabetes mellitus, even through clothing. Each scan shows both the current glucose value and the glucose data for the last 8 hours. A trend arrow helps the patient to assess the trend of blood sugar: whether it is increasing or decreasing and at what rate. These graphs allow adult patients and parents of children with diabetes to take all the necessary steps to avoid serious glycaemic imbalances. Indeed, the FGM system avoids repetitive fingertip pricks for blood glucose measurement, which cause pain, embarrassment and discomfort to the patient, and consequently allows more frequent glucose monitoring. This allows optimal management of the disease and its complications, helping to prevent, and thus reduce, episodes of hypoglycaemia and hyperglycaemia. In this regard, an additional variable was considered in the study, which involved analysing the frequency of perception of episodes of both hypoglycaemia and hyperglycaemia for the two classes of patients by performing an inferential analysis. However, the difference was not statistically significant. In addition to the limited sample size, this is due to the problems of perception of the problem and the type of data collected (self-reported).
The burden of caring for people with diabetes is considerable and the cost grows exponentially as co-morbidities increase, with hospitalisation being the main cost factor. The FGM system promotes the self-care of patients with diabetes mellitus and can help prevent acute disease-related events such as ketoacidosis and severe hypoglycaemia, thus reducing hospitalisations. Investing resources in new technologies, and thus in treatments and devices that reduce diabetes-related events, is a cost-effective strategy and thus amounts to reducing costs for the SSN (National Health Service).
The FGM system also fits well with the recent development of new digital technologies. Thanks to these advances, while on the one hand we have witnessed the increasing development of telecommunication, enabling the user to take advantage of health services through remote communication [20], on the other hand there have been significant advances in medical and technological studies, from the combination of which Telemedicine was born. It guarantees greater continuity of care, better quality of life and savings in terms of health expenditure. This enables simple and immediate doctor-patient communication, reducing outpatient visits as well as offering personalised and effective care management. Women treated with telemedicine feel better cared for through the continuous exchange of information between doctor and patient [21]. With the use of these new tools and technologies, the aim is to achieve a more sustainable management of diabetes and a more rational and modern approach to remotely managed care. Moreover, it should not be overlooked that the use of such systems allows the concept of patient empowerment to take hold, which is fundamental in the management of chronic diseases, as it enables the patient’s active participation in the treatment decision-making process.
CONCLUSIONS
The adoption of new technologies to detect blood glucose has benefits for the patient that positively influence quality of life. The improved control of the disease, linked to increased frequency of glucose monitoring, allows the reduction of glycosylated haemoglobin levels, thus achieving improved glycometabolic control. The study showed that there was a statistically significant difference in glycosylated haemoglobins between the two groups (FGM and SMGB). Glycosylated haemoglobin provides a good indication of the amount of glucose present in the blood over the past few months and is therefore a valid test for diagnosing and monitoring diabetes and, above all, diabetes management. The use of the FGM system, as confirmed by the study, allows the improvement of the quality of life of people with diabetes mellitus as well as better management of the disease. Reducing morbidity and mortality and improving the quality of life of people with diabetes mellitus is one of the current challenges for healthcare professionals.
LIMITATIONS OF THE STUDY
Although the study conducted confirmed what is already widely found in the literature, it is not without its limitations. The limitations of the study are related to the way the questionnaire was administered and the choice of sampling, which was carried out according to a non-probabilistic method that does not give all units of the population the same probability of being part of the sample. Indeed, convenience sampling was chosen for data collection. With convenience sampling, patients are not recruited randomly, so the resulting sample is subject to bias. Further limitations are represented by the sample size, which is especially useful to allow generalisation of the results, and the administration of the questionnaire to paediatric patients and young adults up to 18 years of age. For this class of patients, 8 were aged < 18 years (9.8 % of the sample), 3 were aged < 10 years (3.7 % of the sample). It is likely that the answer to the questionnaire was provided by the parent, who therefore has a system of perception of the problem that is not the patient’s own. A further study with a larger sample size would be needed to demonstrate the statistically significant reduction between perceptions of hypoglycaemic and hyperglycaemic episodes in subjects using the FGM system compared to those using the SMGB.
FUNDING
The authors did not receive any external funding to support this research.
AUTHORS’ CONTRIBUTION
All the authors contributed to the same extent to the realisation of the research.
CONFLICT OF INTEREST
The authors declare that they have no conflicts of interest.
LEGEND ACRONYMS AND ABBREVIATIONS
ADA = American Diabetes Association; DMT1 = Type 1 Diabetes Mellitus; DMT2 = Type 2 Diabetes Mellitus; DTSQ = Diabetes Treatment Satisfaction Questionnaire; FGM = Flash Glucose Monitoring; HbA1c = Glycosylated Hemoglobin; CI = Confidence Interval; IDF = International Diabetes Federation; IQR= Interquartile Scrap; SMBG = Self-monitoring of Blood Glucose; SSN = National Health Service
REFERENCES
- American Diabetes Association. Diagnosis and classification of diabetes mellitus. Diabetes Care 2014; 37(Suppl. 1): (S81–S90)2, 1993.
- Leslie RDG. Causes of diabetes. Genetic and environmental factors. Wiley & Sons, Chicester, 1993.
- Dianna J. Magliano, Edward J. Boyko. IDF Diabetes Atlas 10th edition scientific committee. Brussels: International Diabetes Federation; 2021.
- Gabriel A Gregory, Thomas I G Robinson, Sarah E Linklater, Fei Wang, Stephen Colagiuri, Carine de Beaufort et al. Global incidence, prevalence, and mortality of type 1 diabetes in 2021 with projection to 2040: a modelling study. Lancet Diabetes Endocrinol. 2022 Oct; 10(10):741-760.
- Lo Scalzo A, Abraha I, Bonomo MA, Chiarolla E, Migliore A, Paone S et al. Flash Continuous Glucose Monitoring Systems – Rapid HTA report for diabetes subjects in insulin therapy. Agenas: Rome, 2018.
- Fox C, Kilvert A. Il diabete di tipo 2. Tutte le risposte a portata di mano. Versione italiana a cura di Edoardo Mannucci e Caterina Lamanna. Ercules Comunicazioni, 2012.
- American Diabetes Association (ADA). Standards of Medical Care in Diabetes. Diabetes Care 2018; 41, Suppl. 1, 2018.
- Implication of Diabetes Control and Complication Trial. Diabetes Care, 2004.
- Wenqi Fan, Haipeng Pang, Zhiguo Xie, Gan Huang, and Zhiguang Zhou. Circular RNAs in diabetes mellitus and its complications. Front Endocrinol (Lausanne). 2022; 13: 885650.
- Mariarosaria De Luca, Michele Modestino, Olimpia Iacono, Anna De Simone, Vincenzo Guardasole, Angelo Foglia. Advanced hybrid closed-loop: review of the current systems available in Italy for the treatment of type 1 diabetes mellitus. JAMD 2022| VOL. 25 | N° 2: 121.
- Yaron M, Roitman E, Aharon-Hananel G, Landau Z, Ganz T, Yanuv I et al. Effect of Flash Glucose Monitoring Technology on Glycemic Control and Treatment Satisfaction in Patients With Type 2 Diabetes. Diabetes Care. 2019 Apr 29.
- Nicolucci A, R Giorgino, D Cucinotta, G Zoppini, M Muggeo, S Squatrito et al. Validation of the Italian version of the WHO-Well-Being Questionnaire (WHO-WBQ) and the WHO-Diabetes Treatment Satisfaction Questionnaire (WHO-DTSQ). Diabetes Nutr Metab. 2004 Aug;17 (4):235-43.
- Nicolucci A. L’uso dei questionari sulla qualità della vita. G It Diabetol Metab ,2006.
- Timothy C Dunn, Yongjin Xu , Gary Hayter , Ramzi A Ajjan. Real-world flash glucose monitoring patterns and associations between self-monitoring frequency and glycaemic measures: A European analysis of over 60 million glucose tests. Diabetes Res Clin Pract. 2018 Mar;137:37-46.
- Bolinder J, Antuna R, Geelhoed-Duijvestijn P, Kroger J, Weitgasser R. Novel glucose-sensing technology and hypoglycaemia in type 1 diabetes: a multicentre, non-masked, randomised controlled trial. Lancet, 2016.
- Anders L Carlson, Timothy Dilon Daniel, Andrea DeSantis, Serge Jabbour, Esra Karslioglu French , Davida Kruger et al. Flash glucose monitoring in type 2 diabetes managed with basal insulin in the USA: a retrospective real-world chart review study and meta-analysis. BMJ Open diabetes Res Care. 2022 Jan; 10(1):e002590.
- Marianna Yaron, Eytan Roitman, Genya Aharon-Hananel, Zohar Landau, Tali Ganz, Ilan Yanuv et al. Effect of Flash Glucose Monitoring Technology on Glycemic Control and Treatment Satisfaction in Patients With Type 2 Diabetes. ADA Volume 42,Issue 7, 2019 July.
- Reng-Na Yan, Ting-Ting Cai1, Lan-Lan Jiang 1, Ting Jing 1, Ling Cai , Xiao-Jing Xie et al. Real-Time Flash Glucose Monitoring Had Better Effects on Daily Glycemic Control Compared With Retrospective Flash Glucose Monitoring in Patients With Type 2 Diabetes on Premix Insulin Therapy. Front Endocrinol (Lausanne).2022 Feb 10;13:832102.
- Concetta Irace, Sergio Di Molfetta. Il monitoraggio in continuo della glicemia: stato dell’arte. Aggiornamento in tema di tecnologie. Dicembre 2022| Vol 34.| N° 4.
- Michael J. Ackerman, Rosemarie Filart, Lawrence P. Burgess, Insup Lee, and Ronald K. Poropatich.Developing Next-Generation Telehealth Tools and Technologies: Patients, Systems, and Data Perspectives.Telemedicine and e-Health.Feb 2010.93 95.
- Ming W, Lucy H Mackillop, Andrew J Farmer, Lise Loerup, Katy Bartlett, Jonathan C Levy et al. Telemedicine Technologies for Diabetes in Pregnancy: A Systematic Review and Meta-Analysis J Med Internet Res 2016; 18 (11):e290.
![]() This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
Healthy Nurses: Tips for Enhancing Mental, Emotional, and Spiritual Well-being
Monica Jaramillo1*
1. Independent Author, Florida, US
*Corresponding Author: Monica Jaramillo DNP, MSN/Ed., RN-NLC, CNE®n, CCRN.
Instructor, mentor, and tutor of various healthcare programs and currently not affiliated with any institution when I submitted this manuscript to the Journal. Florida, US. Email: MonicaJaramilloDNP@Gmail.com
Open Researcher and Contributor ID: https://orcid.org/0009-0005-0572-4061
Cite this article
Abstract
Introduction: Recent literature suggests a detrimental burden affecting nurses of all settings and backgrounds. Mental and emotional problems such as moral distress, burnout, compassion fatigue, depression, and severe stress are a few of the many issues nurses are experiencing worldwide. Nurses need enhanced guidance and support regarding caring for their health and well-being.
Discussion: It is imperative to advocate for healthier nurses worldwide. Nurses are experiencing several mental issues and burnout due to a lack of resilience and self-care management. All key stakeholders internationally need to aid nurses with feasible tools that promote mindfulness and improvement of self-care while ensuring stability. The key to enhancing nurses’ mental, emotional, and spiritual well-being could be to offer holistic support conducive to mind-body-spirit and physical health.
Keywords: Healthy Nurses; Holistic; Wholistic; Mental; Emotional; Spiritual; Well-being.
Introduction
Nursing is a caring and compassionate profession full of holistic practices that advocate for the health and well-being of entire communities. Unfortunately, nurses worldwide continue failing in the call to care for themselves in the same empathetic manner as they care for others.[1-3] Nurses nowadays face burnout, fatigue, depression, and severe mental problems such as moral distress and compassion fatigue, to name some of the many stressors, at an exponential rate.[1,2] Healthy nurses are associated with better care outcomes since they represent strong role models for the community and positive health and wellness advocates.[1-3] It is time to advocate more actively for our nurses’ health and well-being while providing support conducive to enhancing their mental, emotional, and spiritual well-being. This work aims to inspire change in nursing through practical advice for all stakeholders while empowering nurses to build resilience and positive self-care practices.
Healthy nurses care for their physical, emotional, spiritual, and mental health while living life to its maximum capacity. Healthy nursing professionals prioritize their well-being as much as they prioritize those they care for. These nurses represent significant advocacy to all communities as they role-model positive and empathetic self-care practices conducive to healthy and meaningful living.[3] Indeed, the health and well-being of nurses are valuable and essential concepts to cultivate to ensure positive outcomes. The importance of healthy nurses is entitled to the impact of these professionals on their communities.[1-3] Nurses are the caregivers and the image many have to look after. Many individuals from all communities around the globe follow nurses’ advice regarding healthy living, and these individuals see nurses are their exemplars of living meaningful lives.[1,2] It is time for nurses of all practice settings and levels of expertise to take a more active role in their health while using the available resources to live their lives to the fullest. Seek help in your institutions or from national and international associations. Many resources are at hand to support you in all ways that ensure the professional development and advancement of the nursing profession and the health and well-being of all nurses. One example of the multiple national resources available for nurses in the United States is the American Nurses Association (ANA). This organization represents and supports 4.3M nurses nationwide while empowering them to thrive in all aspects of their personal and professional lives.[4] The multiple initiatives ANA has established to ensure healthy nurses while ensuring a healthy country are worth exploring. In the end, it all entitles building resilience and incorporating self-care. Nurses’ resilience represents coping with unforeseen or stressful situations and returning to healthy and balanced wellness after a crisis, while self-care promotes mind and body wholeness.[5,6] This composition explores the definition and importance of healthy nurses, tips for building resilience, feasible techniques for wholistic self-care, and recommendations. This commentary includes a discussion and a conflict of interest statement.
Discussion
Resilience is the ability to withstand adversity.[5] Undoubtedly, all nurses, despite their area of expertise, face some level of difficulty and stress. Nurses must be mindful of the need to adapt to challenging situations successfully.[5,6] This author’s most remarkable experiences with resilience and mindfulness arise from clinical experiences in intensive care and the pressure of completing advanced-practice nursing degrees of education toward the terminal degree in nursing. The chaos of multiple professional and personal demands and the responsibility of caring for patients in a life-death environment is highly challenging. Still, from tough situations like this emerge great realizations. Accordingly, the scientific evidence around the globe is conclusive in suggesting that nurses worldwide need mental and emotional support to mitigate their stress and burnout.[1-3] It is imperative for nurses to improve their resilience and for all key stakeholders to support the health and well-being of nurses with tools that will enhance wholeness.[5,6] Some of the most helpful tips for building resilience in this author’s experience include using all the available resources, starting soon in the career, practicing gratitude, sparking the passion for nursing often, and taking enough time for self-care daily. In this regard, seeking help when first needed while exploring resources such as counseling, mentoring, connections, or community programs is ideal. Similarly, gratitude and purpose or passion for nursing can increase resilience. Lastly, self-care is another valuable component of resilience worth exploring separately.
Self-care is also vital for every person’s health and well-being, not just for nurses. This concept means taking care of self while ensuring both physical and mental, spiritual, and mental health in a comprehensive or wholistic manner. Now, wholistic can mean different things to different people, and the term may be unknown to many others.[7] For this author, this term means ensuring holistic practices that entitle the whole aspects of the person and caring for self comprehensively and holistically while embracing mind-body-spirit. Seeing self-care from this wholistic approach can be the key to improve not only resilience but nurses’ mental, physical, emotional, and spiritual well-being.
In this author’s experiences, feasible techniques to ensure wholistic self-care in nurses and all individuals despite their culture and background are as follows. First, be true to yourself by following your mind and heart’s desires. Advocating for your well-being first is vital, as hard as this may sound for many nurses considering our call to serve others. Follow your preferences, call to help, and continue that path with your health in mind. Second, perform regular physical activities that are attractive to you personally. This step can be as simple as taking the stairs at work instead of the elevator to have peace of mind that you are incorporating self-care into your daily practices. Third, engage in excellence groups or advocacy associations of your interest as much as possible to promote self-pride. Fourth, be an active advocate for self-care practices in your organization. For this, you may explore the available resources and recommend a practice change policy that promotes more initiatives to ensure the health and well-being of nursing staff. Lastly, do not forget to be kind to yourself and reward yourself often for your achievements.
It is imperative to ensure the health and well-being of nurses around the globe. Healthy nurses are professionals who live their lives to the fullest while inspiring the community to live healthy and meaningful lives. Ensuring nurses’ physical, mental, emotional, and spiritual well-being requires strong resilience and conscious self-care. These wholistic practices can positively impact all nurses directly while indirectly improving entire communities’ health. It is time to increase advocacy regarding nurses’ health while reminding these professionals to utilize available resources, seek help when needed, practice activities they enjoy, ensure self-care as part of their daily routines, and be kind to themselves. The author hopes to inspire all stakeholders to advocate for healthier nurses and invites further research and studies concerning this vital topic for global public health.
Funding Statement
This research received no external funding.
Conflict of Interest Statement
The author declares no conflict of interest
References
- Wand T, Glover S, Paul D. What should be the future focus of mental health nursing? Exploring the perspectives of mental health nurses, consumers, and allied health staff. International Journal of Mental Health Nursing. 2021;31(1).
- Khatatbeh H, Pakai A, Al‐Dwaikat T, et al. Nurses’ burnout and quality of life: A systematic review and critical analysis of measures used. Nursing Open. 2021;9(3).
- Rykkje L, Søvik MB, Ross L, McSherry W, Cone P, Giske T. Educational interventions and strategies for spiritual care in nursing and healthcare students and staff: A scoping review. Journal of Clinical Nursing. 2021.
- American Nurses Association. Healthy Nurse, Healthy Nation [Internet]. American Nurses Association; [cited 2023 April 18]. Available from: https://www.nursingworld.org/practice-policy/hnhn/
- Janzarik G, Wollschläger D, Wessa M, Lieb K. A group intervention to promote resilience in nursing professionals: A randomised controlled trial. International Journal of Environmental Research and Public Health. 2022;19(2):649.
- Zeb H, Arif I, Younas A. Mindful self-care practice of nurses in acute care: A multisite cross-sectional survey. Western Journal of Nursing Research. 2021;44(6):019394592110045.
- Chizhande I. No health without wholistic health: An empirical approach to mental health cultivation. Asian Journal of Research in Social Sciences and Humanities. 2022;12(4):416-424.
![]() This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
MUSIC THERAPY FOR PAIN AND ANXIETY IN HOSPITALIZED CHILDREN: A SYSTEMATIC REVIEW OF RANDOMIZED CONTROLLED TRIAL
Arvida Bar1, Monalisa2*, Netha Damayantie3, Halimah4
1,2,3,4Department of Nursing, Health Polytecnic of Jambi, Indonesia
* Corresponding author: Monalisa, Jl. Dr. Tazar, Buluran Kenali, Kec. Telanaipura, Kota Jambi, Jambi 36361, Indonesia, Orcid: https://orcid.org/0000-0002-4879-3893
Email: monalisa.poltekkes@gmail.com
Phone: +62 821-8656-3003

Cite this article
ABSTRACT
Introduction. Music has been widely recognized for its effectiveness in controlling anxiety and pain. However, in particular groups such as children, the implementation may be challenging, especially regarding the type of music selection. The aim of the study is to evaluate the music therapy efficacy on pain and anxiety management in pediatric care to improve the management of pain and anxiety in the pediatric population.
Methods. This review was written according to the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) statement. In assessing the impact of music therapy as a method of pain and anxiety management in pediatric care, a database tracking was conducted for articles publicized between 2000 and 2022. The databases used including Sciencedirect, Cochrane library, PubMed, and Wiley online library. Articles were deemed if the study subjects ranged in age from 0 to 21 years old, the intervention was live or recorded music, and the study took place in an inpatient background.
Results. 1,129 publications were discovered. In final search of literature, there are 12 articles included in this review. There is consistent and consequential evidence that music may relieve pain and anxiety in hospitalized children before and during procedures. The type of music that is widely used is classical and traditional instrumental music. In addition, there were only two studies using nursery rhymes.
Conclusion. The patient’s preference in choosing music for children enables them to determine the appropriateness of therapy. Classical music can be the main choice in applying music therapy in reducing anxiety and pain in children.
Keywords: Pediatric; music; pain; anxiety; inpatient; nurse
INTRODUCTION
Extreme anxiety may harm a child’s physical and psychological health, cause adverse postoperative outcomes that hinder recuperation, rehabilitation and reduce a child’s alliance in self-care [1–3]. Hospitalized children may experience anxiety due to daily activities, recurring convulsions, loss of control, or loneliness [4–6]. According to the current study, compelling pain and anxiety management are critical to healing [7,8]. Untreated pain and anxiety may cause diverted recovery, extended hospitalization, impaired physical growth and development, faked personality, and a lifelong nervousness of medical providers and treatments to be inducted [6,9–12].
There are multiple hindrances to implementing sufficient management of child care. Many parents and healthcare providers fear the side effects of pain and anxiety remedies [13–16]. Since 1999, the U.S. pediatric mortality rate, ages 0 to 19, has nearly tripled due to illicit prescription opioids [18]. Due to the risks and harmful effects of sole reliance on pharmacological treatments, Governments and healthcare providers are striving for alternative non-pharmacological modalities for manipulating pain and anxiety, particularly in children [19].
Music, touch, and nurse-led distraction techniques are non-pharmacological therapies currently widely used in pediatric care [20]. This therapy is effective in helping reduce the dose and duration of pain and anxiety medications and improve pain and anxiety scores; thus, nurses can continue to maintain their autonomy [21,22]. Focusing on music therapy turns out that this therapy has the potential to reduce or even eliminate the need for pharmacological therapy (18). Music also impacts human emotional and physiological responses by diverting attention from the symptoms of pain and anxiety that arise (19). The theory best known as the mechanism of pain, Gate Control, posits that pain receptors collaborate to transmit pain signals to the brain [23]; thus, distractions such as music can block specific pain pathways and reduce the amount of pain felt. Music therapy sessions allow individuals to express their pain and anxiety in healthy ways, such as through improvised songs and playing instruments [24,25]. Music has been used in clinical settings such as general practice (medical and dental) and more specialized settings such as surgery and related medical professions (such as physiotherapy and speech therapy). It is essential to recognize differences between the clinical practice of music therapists, who are certified, and the use of music by lay practitioners, who are not explicitly trained or have some background in music psychology or clinical psychology [26,27].
Previous systematic reviews of randomized controlled trial studies concluded the excellent efficacy of music therapy for children in controlling pain and anxiety when facing medical procedures. However, these studies could have clearly shown the type of music and therapy delivery method, which is still a big question [28]. Another review study found that the evidence for the effectiveness of using music to reduce dental anxiety in children is inconclusive and of limited quality [27]. The present review study aims to assess the effect of music therapy on pain and anxiety management in pediatric care to improve pain and anxiety management in the pediatric population from existing literature published from 2000 to 2022. The time-lapse choosen to updating studies in previous review. Review question including what types of music most used? What method used to deliver the music?
METHODS
Review Protocol
Following the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) 2020 guidelines, we conducted a systematic review of the literature consisting of Randomized Controlled Trials (RCTs) that apprised the effectiveness of music therapy in alleviating pain and anxiety in pediatric care [29].
Eligibility Criteria
We removed duplicates and uploaded articles to the web-based bibliography and database manager. It was then distributed to the team members, and a single reviewer initially reviewed the title and abstract. The following step was a full-text review by two reviewers. Additional reviewers were organized to deal with contentions to reach a consensus. The inclusion criteria include subjects ranged in age from 0 to 21, using live or recorded music in a hospital setting, effective or ineffective in alleviating pain and anxiety, and the full text was available in English. Articles are excluded if located in an outpatient setting, such as an emergency department or venipuncture clinic; music therapy by a music therapist; in labour or involving pregnant adolescents; during surgery or under general anaesthesia, or occurs in the neonatal intensive care unit (NICU) or pediatric intensive care unit (PICU). Babies treated in the NICU must be excluded because premature babies’ nervous systems are immature, so they respond to pain differently from full-term babies. Although not all babies treated in the NICU are premature, several articles do not always distinguish between premature and full-term babies born in the NICU. Theses or dissertations, conference articles, comments, editorial reports, and poster presentations are exempt.

Table 1. PICOS statement
Information source
A medical librarian searched a database for articles published in the previous ten years, from 2000 to 2022, in May 2022. Sciencedirect, Cochrane library, PubMed, and Wiley online library were all searched.
Search Strategy
PubMed, Sciencedirect, Wiley Online Library, and the Cochrane Library were among the databases searched. Furthermore, we also search on the list of references in the article that meet the criteria to broaden the search results further. In creating a comprehensive search strategy for each database, the following search terms were used: (1) pediatric, child, adolescent, infant, infant, toddler, adolescent, adolescent, male, female, (2) pain, tone, voice (3) anxiety (4) hospitalization, hospitalization, procedure, postoperative, surgery. A review of all included study references was also conducted. We also add filters to each database, including publication type and research design.

Table 2. Search String
Data Collection
Two authors independently screened the title and abstract to suit the inclusion criteria, if it was not clear, then they continued by reading the main text. No automation tools were used in selection literatures.
Data Extraction
To extract the required data, we followed the McMaster Critical Review Form-Quantitative Studies v. 2.0 and added some information that we think is important. The data we extracted included authors, countries, outcomes, study designs, participants, interventions, evaluation methods, and main findings. Two authors performed data extraction independently. The finalization of the extraction process was read and endorsed by the first author.
Quality of the Study
Study quality was assessed by two authors independently using the Critical Appraisal Skills Program (CASP) for the Randomized Controlled Trial [30]. This tool consists of 11 questions which are divided into four sections with the choices of Yes, No, and Can’t Tell checklist columns. We categorize the quality of studies into High, Medium, and Low. High quality studies if you have answers YES 10 – 11/11, medium quality if you have answers YES 7 – 9/11, and Low quality if answers YES ≤6/11.
Study Risk of Bias Assessment
The risk of bias or validity in the process and results of a systematic review is reflected in its methodological quality. The Cochrane Handbook 5.2.0 was used to reckon methodological quality. Two authors independently assessed the risk of bias in the included studies. In the circumstance of a disagreement, refer it to the corresponding author for arbitration. The Cochrane bias risk assessment tool was used to evaluate the risk of RCTs, which possessed random sequence generation, allocation concealment, blinding of subjects and researchers, blinding of outcome assessment, insufficient outcome data, and selective reporting.
RESULTS
Study Selection
A systematic electronic search identified that 1,129 publications were discovered through backward searching of relevant papers. The full-text screening was conducted on 783 articles. A total of 692 articles failed to meet eligibility criteria at the full-text screening stage, and only 12 articles were finally eligible for further analysis. The search results follow the PRISMA 2020 flow diagram (Fig. 1).
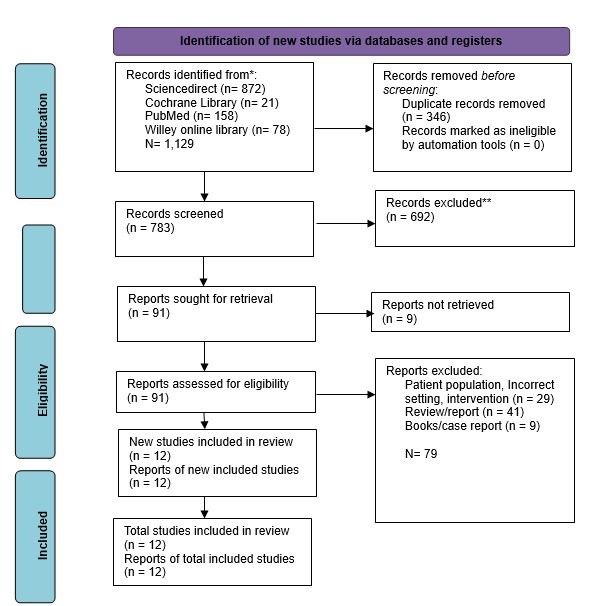
Figure 1. PRISMA flow diagram for literature search


Table 3. Characteristics of studies included.
Study Characteristics
Eleven randomized controlled trials (RCTs) and one quasi-experimental study met the inclusion criteria and was analyzed. The studies included 543 participants ranging in age from seven days to 18 years. The research was conducted in eight countries: India (8.33%, n=1) [31], Brazil (8.33%, n=1) [32], Iran (16.67%, n=2) [33,34], South Korea (8.33%, n=1) [35], the United Kingdom (UK) (8.33%, n=1) [36], Vietnam (8.33%, n=1) [37], the United States (US) (16.67%, n=2) [38,39], Turkey (8.33%, n=1) [25], and China (16.67%, n=2) [40,41].
Studies reported the implementation of music therapy before a procedure (n =5, 41.67%), during a procedure (n =4, 33.33%), after a procedure (n =6, 50%), or at any time during a hospitalization (n =2 16.67%), music-based interventions were used. The time spent listening to music ranged from 1 minute to at least 30 minutes. Most of the studies (n=7, 58.3%) used recorded music with headphones (n=7, 58.3%); one used speakers and ambient music.
The studies in the analysis scrutinized the effects of music-based interventions on pain (n=5, 41.67%) and anxiety (n=5, 41.67%). Some studies found a consequential lowering in pain scores in the music group (n=3), while others found no significant reduction (n=2). Before and during procedures, all studies conveyed a significant reduction in anxiety scores in the music group (n=5). Only one study discovered no significant lessening in anxiety scores in the music group following surgery.
Study quality
Based on the results of the study quality assessment which consisted of thirteen questions, only four studies were in the High Quality category, and eight other studies were in the Medium Quality category.

Table 4. Summary of quality assessment
Risk of Bias in Studies
Based on the bias assessment, all studies are in the low category in the Bias in measurement of the outcome domain. For overall bias, there are four studies that are in the Some Concerns category, and eight studies that are in the Low risk of bias category.

Figure 2. Traffic-light plot for RoB in individual study
Effect on Anxiety
There are eight studies [25,32,34,35,37,38,40] who analyzed the effect of music on pediatric anxiety in dealing with hospital care situations. The measurements of participants’ anxiety levels used a variety of instruments, including The Observational Scale of Behavioral Distress (OSBD), the modified Yale Preoperative Anxiety Scale (mYPAS), and The Spielberger State-Trait Anxiety Inventory (STAIC). Overall there was a significant decrease in anxiety in the studies that analyzed the effects of this music intervention.
Effect on Pain
There are nine studies [25,31,33,36–41] who analyzed the effect of music on the level of pain experienced by pediatricians. However, two studies showed insignificant results in reducing experienced pain [31,41]. The instruments used to measure pain include Wong-Baker Faces (WB-FACES), Visual Analog Scale (VAS), Numeric rating scale (NRS), and The Children’s Hospital of Eastern Ontario Pain Scale (CHEOPS).
DISCUSSION
Non-pharmacologic methods are widely used as forms of pain, fear, and vomiting control for children in the hospital setting. There are several medical procedures in the hospital that can provide an unpleasant experience, especially in Pediatric care. This review evaluated the impact of music therapy as a corroborative strategy for pain and anxiety control in hospitalized children. The publications’ central theme was statistically meaningful evidence that music can decline anxiety before and during procedures [32,34,35,37,38,40,41]. However, results concerning pain, often viewed as physiologic analogs to pain, were mixed [31,32,36–39,41]. Music-based interventions are also secure for hospitalized children, according to the evidence. Only one RCT reported any negative effects, deemed minor and mostly related to headphone affliction or no refinement in pain or anxiety scores [37].
It is crucial to explore patient factors that contributed to music interventions’ success in employing this review’s findings. Several studies have emphasized the importance of patient discretion in deciding on music for children [32,37,39,41]. Researchers have allowed two-year-olds to choose the type of music they want to listen to in several research studies [37,39,41]. According to one study, this sovereignty contributed to lower pain and anxiety levels in music groups [37]. In another study, subjects were reluctant to listen to researcher-selected music, resulting in significant sample loss [32]. It reflects a broader healthcare shift towards patient-centered care over the past decades, recognizing the importance of patient preferences in achieving positive health outcomes[24]. Music-based interventions deliver tangible ways for children to partake directly in care giving and manage challenging situations.
It is also important to regard the kit for implementing musical interventions. There is a high reliance on pre-recorded audio delivered through headphones. It exemplifies the viability and cost-effectiveness of music interventions in the hospital. The costs associated with the equipment needed to play music are relatively affordable, and several previous studies suggest that nurses may execute interventions without formal internship [32,35,37,39,41].
Music treatment is unassailable, affordable, and uncomplicated to learn, and hospital nurses can use it efficiently [42]. Music in nursing practice can be used unattended or in concurrence with other methods, such as jaw relaxation [43] and therapist guidance [44]; it can be used in a variety of sets, circumstances, and people for a miscellany of pursuits [43–47]. According to studies, 20-90 minutes of music therapy is an adequate remedy time. The following types of music were played: Sedative music [48], researcher-supplied music and subject-preferred music, smoothing music, and easy-listening music are all examples of sedative [46].
Music therapy may activate the natural analgesia in the human body that leads to alleviating pain, known as Endorphine [49]. Endorphine is a neuro hormone provoking pleasant sensations. The pain will be relieved along with parasympathetic system activation, which leads to the relaxation of the body. Aside from feel-good chemicals, nor-adrenaline and serotonin contribute enormously to pain relief via attenuated transmission of the brain’s descending impulse. The descending control system is a sensory neuron fiber that runs from the midbrain (precisely the peri-aqueductal gray matter) to the inter-neuronal inhibitory system [50–52]. The system will remain active in response to the stimulus of soft music, which inhibits the transmission of the pain stimulus. Music therapy has been shown to stimulate the axons or nerve fibers on the ascending tracts of RAS neurons (Reticular Activating System). The stimulus is transmitted to the cerebral cortex, limbic system, and corpus callosum through the autonomous nervous and neuro-endocrine systems. When one is immersed in soft music, the limbic system is aroused, causing it to secrete phenylethylamine (neuroamin), which controls impulse and mood emotion. Music stimulates the parasympathetic nervous system to work on the sympathetic nerves, causing the switch to alpha-type brain waves to yield soothing outcomes on the autonomic nervous system [53–55].
The physiological justification backs up the study’s finding that music therapy has a positive effect on reducing or relieving anxiety and pain in children. Nurses ought to employ a combination of pharmacologic and non-pharmacologic interventions to relieve pain and avoid the medication’s unwanted side effects [56]. It lays the hypothetical underpinnings for skillful or qualified nurses to gain new knowledge of other methods effective in relieving pain and anxiety, such as the use of music therapy, in health-care facilities. It echoes the assertion made by Huang, Good, and Zauszniewski [48] that music therapy is one of the interventional techniques that has concrete proof nursing theories to proficiently alleviate anxiety and pain.
Indeed although all considerations included in this integrator writing survey are of tall or great quality, it is conceivable that the comes about might have been impacted by pondering confinements. For case, a few ponder utilized a little test measure or did not incorporate a test estimate calculation. Test estimate was famous when evaluating the quality of each article. In expansion, most things did not dazzle the analysts, spectators, or members. Even though blinding in the investigation is critical to play down any conceivable inclination, it is troublesome to do so with music-based mediations, especially live music.
Two studies used an invalidated pain or anxiety scale in the study population, which was highlighted when appraising the precision of each article [37,41]. Because pain and anxiety are subjective, they are challenging to assess. Standardized pain and anxiety scales are used by providers to assess pain and anxiety, especially in nonverbal or nonresponsive patients. CHEOPS, FACES, FPS-R, NRS, and VAS pain scales were used in the studies. The m-YPAS and STAIC anxiety scales were used in the studies. While there are numerous pain and anxiety scales available, a validated and user-friendly pain or anxiety scale may not always be obtainable or ubiquitously used for the workforce being ascertained.
A wide age range of participants was used in multiple studies. From infancy to adolescence, children’s emotions, personalities, behavior, and speech will grow and develop. The way children react to stimuli like pain and anxiety will vary based on their developmental stage and age. Despite the fact that the studies only looked at children aged 0 to 18, the use of such a wide age range of individuals makes the reliability analysis of the findings questionable.
LIMITATION
In our search for full-text articles, we only collected 12 articles due to the limited access we faced, which prevented us from further exploring the magnitude of the effect of music therapy on pain and anxiety in children in the form of a meta-analysis. Some of the studies we include are also in the Some Concern category, so using the results of this study requires caution. However, we believe that nurses can apply music therapy autonomously in managing pain and anxiety in children as a form of nursing implementation and improving the quality of care.
CONCLUSION
For children in the hospital, pain, and anxiety often come to them in various incredibly invasive medical procedures. Music therapy can be the first choice for nurses to offer children with minimal side effects and is friendly to children’s conditions. Physiologically, music therapy can trigger natural analgesics in the body through neurohormones that have a calming effect. Based on studies that apply music therapy, the type of music generally used in classical music is delivered through headphones. Future studies can further examine how music therapy influences chronic pain conditions in children.
Conflict of Interests
There is no conflict of interest.
Ethical Approval
Ethics approval Ethical approval will not be required because this study will retrieve and synthesize data from already published studies.
Acknowledgments
We would like to express our gratitude to all parties, particularly the director of Health Polytechnic of Jambi.
Author’s Contribution
All authors equally contributed to preparing this article.
Funding/Support
This research did not receive any specific grant from funding agencies in the public, commercial, or not for profit sectors.
REFERENCES
- van der Heijden MJE, Jeekel J, Rode H, Cox S, van Rosmalen J, Hunink MGM, et al. Can live music therapy reduce distress and pain in children with burns after wound care procedures? A randomized controlled trial. Burns. 2018;44(4):823–33.
- Anggerainy SW, Wanda D, Nurhaeni N. Music therapy and story telling: Nursing interventions to improve sleep in hospitalized children. Comprehensive child and adolescent nursing. 2019;42(sup1):82–9.
- Zhu X, Haegele JA, Healy S. Movement and mental health: Behavioral correlates of anxiety and depression among children of 6–17 years old in the US. Mental Health and Physical Activity. 2019;16:60–5.
- Gomes GLL, Fernandes M das GM, Nóbrega MML da. Hospitalization anxiety in children: conceptual analysis. Revista brasileira de enfermagem. 2016;69:940–5.
- Li WHC, Chung JOK, Ho KY, Kwok BMC. Play interventions to reduce anxiety and negative emotions in hospitalized children. BMC pediatrics. 2016;16(1):1–9.
- Delvecchio E, Salcuni S, Lis A, Germani A, Di Riso D. Hospitalized children: anxiety, coping strategies, and pretend play. Frontiers in public health. 2019;7:250.
- Gogoularadja A, Bakshi SS. A Randomized study on the efficacy of music therapy on pain and anxiety in nasal septal surgery. International Archives of Otorhinolaryngology. 2020;24:232–6.
- Cırık V, Efe E. THE EFFECT OF MUSIC THERAPY IN CHILDREN’S HEALTH. Journal of Educational & Instructional Studies in the World. 2018;8(2).
- Chow CHT, Van Lieshout RJ, Schmidt LA, Dobson KG, Buckley N. Systematic review: audiovisual interventions for reducing preoperative anxiety in children undergoing elective surgery. Journal of pediatric psychology. 2016;41(2):182–203.
- Lerwick JL. Minimizing pediatric healthcare-induced anxiety and trauma. World journal of clinical pediatrics. 2016;5(2):143.
- Fronk E, Billick SB. Pre-operative anxiety in pediatric surgery patients: Multiple case study analysis with literature review. Psychiatric Quarterly. 2020;91(4):1439–51.
- Johnson AA, Berry A, Bradley M, Daniell JA, Lugo C, Schaum-Comegys K, et al. Examining the effects of music-based interventions on pain and anxiety in hospitalized children: An integrative review. Journal of Pediatric Nursing. 2021;60:71–6.
- Bawa M, Mahajan JK, Aggerwal N, Sundaram J, Rao KLN. Barriers to pediatric pain management in children undergoing surgery: A survey of health care providers. Journal of Pain & Palliative Care Pharmacotherapy. 2015;29(4):353–8.
- Katende G, Mugabi B. Comforting strategies and perceived barriers to pediatric pain management during IV line insertion procedure in Uganda’s national referral hospital: A descriptive study. BMC pediatrics. 2015;15(1):1–8.
- Greenfield K, Carter B, Harrop E, Jassal S, Bayliss MJ, Renton K, et al. Healthcare professionals’ experiences of the barriers and facilitators to pediatric pain management in the community at end-of-life: a qualitative interview study. Journal of Pain and Symptom Management. 2022;63(1):98–105.
- Sabeti F, Mohammadpour M, Pouraboli B, Tahmasebi M, Hasanpour M. Health Care Providers’ experiences of the non-pharmacological pain and anxiety management and its barriers in the Pediatric Intensive Care Units. Journal of Pediatric Nursing. 2021;60:e110–6.
- Rudd RA, Aleshire N, Zibbell JE, Gladden RM. Increases in drug and opioid overdose deaths—United States, 2000–2014. Morbidity and mortality weekly report. 2016;64(50 & 51):1378–82.
- Gaither JR, Shabanova V, Leventhal JM. US national trends in pediatric deaths from prescription and illicit opioids, 1999-2016. JAMA network open. 2018;1(8):e186558–e186558.
- Bizzio R, Cianelli R, Villegas N, Hooshmand M, Robinson M, Hires KA, et al. Exploring non-pharmacological management among anesthesia providers to reduce preoperative distress in children. Journal of pediatric nursing. 2020;50:105–12.
- Giordano F, Zanchi B, De Leonardis F, Rutigliano C, Esposito F, Brienza N, et al. The influence of music therapy on preoperative anxiety in pediatric oncology patients undergoing invasive procedures. The Arts in Psychotherapy. 2020;68:101649.
- Uggla L, Bonde L, Hammar U, Wrangsjö B, Gustafsson B. Music therapy supported the health‐related quality of life for children undergoing haematopoietic stem cell transplants. Acta paediatrica. 2018;107(11):1986–94.
- Mondanaro JF, Sara GA, Thachil R, Pranjić M, Rossetti A, Sim GE, et al. The effects of clinical music therapy on resiliency in adults undergoing infusion: a randomized, controlled trial. Journal of Pain and Symptom Management. 2021;61(6):1099–108.
- Melzack R, Wall PD. Pain Mechanisms: A New Theory: A gate control system modulates sensory input from the skin before it evokes pain perception and response. Science. 1965;150(3699):971–9.
- Finnerty R. Music therapy as an intervention for pain perception. Anglia Ruskin University, Cambridge, England. 2006;
- Bulut M, Alemdar DK, Bulut A, Şalcı G. The effect of music therapy, hand massage, and kaleidoscope usage on postoperative nausea and vomiting, pain, fear, and stress in children: A randomized controlled trial. Journal of Perianesthesia Nursing. 2020;35(6):649–57.
- Stegemann M. therapy and other music-based interventions in pediatric health care: An overview. Medicines;
- Ainscough SL, Windsor L, Tahmassebi JF. A review of the effect of music on dental anxiety in children. European Archives of Paediatric Dentistry. 2019;20(1):23–6.
- Klassen JA, Liang Y, Tjosvold L, Klassen TP, Hartling L. Music for pain and anxiety in children undergoing medical procedures: a systematic review of randomized controlled trials. Ambulatory pediatrics. 2008;8(2):117–28.
- Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. International Journal of Surgery. 2021;88:105906.
- Programme CAS. CASP randomised controlled trial checklist. 2018.
- Balan R, Bavdekar SB, Jadhav S. Can Indian classical instrumental music reduce pain felt during venepuncture? The Indian Journal of Pediatrics. 2009;76(5):469–73.
- Franzoi MAH, Goulart CB, Lara EO, Martins G. Music listening for anxiety relief in children in the preoperative period: a randomized clinical trial. Revista latino-americana de enfermagem. 2016;24.
- Sabzevari A, Kianifar H, Jafari SA, Saeidi M, Ahanchian H, Kiani MA, et al. The effect of music on pain and vital signs of children before and after endoscopy. Electronic physician. 2017;9(7):4801.
- Kazemi S, Ghazimoghaddam K, Besharat S, Kashani L. Music and anxiety in hospitalized children. Journal of Clinical and Diagnostic Research. 2012;6(1):94–6.
- Kim SJ, Oh YJ, Kim KJ, Kwak Y-L, Na S. The effect of recorded maternal voice on perioperative anxiety and emergence in children. Anaesthesia and intensive care. 2010;38(6):1064–9.
- Longhi E, Pickett N, Hargreaves DJ. Wellbeing and hospitalized children: can music help? Psychology of music. 2015;43(2):188–96.
- Nguyen TN, Nilsson S, Hellström A-L, Bengtson A. Music therapy to reduce pain and anxiety in children with cancer undergoing lumbar puncture: a randomized clinical trial. Journal of Pediatric Oncology Nursing. 2010;27(3):146–55.
- Noguchi LK. The effect of music versus nonmusic on behavioral signs of distress and self-report of pain in pediatric injection patients. Journal of Music Therapy. 2006;43(1):16–38.
- Suresh S, De Oliveira GS, Suresh S. The effect of audio therapy to treat postoperative pain in children undergoing major surgery: a randomized controlled trial. Pediatric Surgery International. 2015;31(2):197–201.
- Liu Y, Petrini MA. Effects of music therapy on pain, anxiety, and vital signs in patients after thoracic surgery. Complementary therapies in medicine. 2015;23(5):714–8.
- Yu H, Liu Y, Li S, Ma X. Effects of music on anxiety and pain in children with cerebral palsy receiving acupuncture: A randomized controlled trial. International Journal of Nursing Studies. 2009;46(11):1423–30.
- Wang C-F, Sun Y-L, Zang H-X. Music therapy improves sleep quality in acute and chronic sleep disorders: A meta-analysis of 10 randomized studies. International journal of nursing studies. 2014;51(1):51–62.
- Good M, Anderson GC, Ahn S, Cong X, Stanton‐Hicks M. Relaxation and music reduce pain following intestinal surgery. Research in nursing & health. 2005;28(3):240–51.
- Gutgsell KJ, Schluchter M, Margevicius S, DeGolia PA, McLaughlin B, Harris M, et al. Music therapy reduces pain in palliative care patients: a randomized controlled trial. Journal of pain and symptom management. 2013;45(5):822–31.
- Chaput-McGovern J, Silverman MJ. Effects of music therapy with patients on a post-surgical oncology unit: A pilot study determining maintenance of immediate gains. The Arts in Psychotherapy. 2012;39(5):417–22.
- Allred KD, Byers JF, Sole M Lou. The effect of music on postoperative pain and anxiety. Pain Management Nursing. 2010;11(1):15–25.
- Wurjatmiko AT. The effects of music therapy intervention on the pain and anxiety levels of cancer patient: A systematic review. International Journal of Nursing Education. 2019;11(4):14–8.
- Huang S-T, Good M, Zauszniewski JA. The effectiveness of music in relieving pain in cancer patients: a randomized controlled trial. International journal of nursing studies. 2010;47(11):1354–62.
- Aktaş YY, Karabulut N. The use of cold therapy, music therapy and lidocaine spray for reducing pain and anxiety following chest tube removal. Complementary therapies in clinical practice. 2019;34:179–84.
- Cowen R, Stasiowska MK, Laycock H, Bantel C. Assessing pain objectively: the use of physiological markers. Anaesthesia. 2015;70(7):828–47.
- McInnis PM, Braund TA, Chua ZK, Kozlowska K. Stress-system activation in children with chronic pain: a focus for clinical intervention. Clinical Child Psychology and Psychiatry. 2020;25(1):78–97.
- Wei Y, Liang Y, Lin H, Dai Y, Yao S. Autonomic nervous system and inflammation interaction in endometriosis-associated pain. Journal of Neuroinflammation. 2020;17(1):1–24.
- Riganello F, Cortese MD, Arcuri F, Quintieri M, Dolce G. How can music influence the autonomic nervous system response in patients with severe disorder of consciousness? Frontiers in neuroscience. 2015;9:461.
- Akimoto K, Hu A, Yamaguchi T, Kobayashi H. Effect of 528 Hz music on the endocrine system and autonomic nervous system. Health. 2018;10(09):1159.
- Yamashita K, Kibe T, Ohno S, Kohjitani A, Sugimura M. The effects of music listening during extraction of the impacted mandibular third molar on the autonomic nervous system and psychological state. Journal of Oral and Maxillofacial Surgery. 2019;77(6):1153-e1.
- Yaban ZS. Usage of non-pharmacologic methods on postoperative pain management by nurses: Sample of turkey. International Journal of Caring Sciences. 2019;12(1):529–41.
![]() This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
Evaluation of M-Health On Medication Adherence In Tuberculosis Patients: A Systematic Review
Rd. Mustopa1*, Damris2, Syamsurizal2, M. Dwi Wiwik Emawati2
1Department of Medical Laboratory Technology, Health Polytechnic of Jambi, Jambi, Indonesia
2Doctoral Study Program, Faculty of Mathematics and Natural Sciences, Jambi University, Jambi, Indonesia
Corresponding author. Rd. Mustopa, JL. Haji Agus Salim Nomor 09 Kota Baru – Jambi 36361, Indonesia.
Orcid : https://orcid.org/0000-0002-6407-1452.
Phone: +62 821-9668-7959
Email: rdmustopa979@gmail.com
Cite this article
ABSTRACT
Background & Aim: The success of the TB control program is closely related to patient adherence to treatment. Previous studies have provided many views regarding the use of variants of mHealth on TB patient adherence, but the results still need to be clarified. This review aims to evaluate and provide an overview of mHealth RCTs on medication adherence in the patient with tuberculosis.
Methods & Materials: The PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guideline was followed to report study findings. A literature search for studies in the period of 2018-2022 in PubMed, Cochrane, CINAHL and Sciencedirect databases was conducted. Randomized controlled trials (RCTs) that analyzed the effect of mHealth on medication adherence outcomes (treatment completion, treatment adherence, missed doses, and non-completed rate) were included. Adult patients with either active or latent TB infection were included. The Cochrane ’Risk of bias’ assessment tool was used to assess the risk of bias of eligible studies.
Result: Overall, searches on databases generated 2,607 articles, and only 18 articles met the criteria. Two authors independently screened and extracted data from eligible studies. There are two devices used in mHealth in the last five years: software (SMS, We chat, and Whatsapp) and hardware (MERM, eDOT, WOT). Based on descriptive analysis, the hardware mHealth is superior to the software mHealth. Close monitoring and measurement of the use of DOT hardware demonstrates the accuracy of treatment success.
Conclusion: It was found that mHealth interventions can be an advantageous approach. However, the interventions showed variable effects regarding the direction of effect and the rate of improvement of TB treatment adherence and clinical outcomes.
Keywords: Tuberculosis; eHealth; digital health; Adherence; digital adherence.
INTRODUCTION
Tuberculosis is a disease that requires the sufferer’s adherence to a standardized treatment program to completely get rid of Mycobacterium, which is the main cause of this disease, from the sufferer’s body [1–3]. A total of 1.6 million people died from TB in 2021 (including 187,000 people living with HIV). Worldwide, TB is the 13th leading cause of death and the second infectious killer after COVID-19 (above HIV/AIDS). TB is a treatable and curable disease. Drug-susceptible TB disease is treated with a standard 4-month or 6-month course of 4 antimicrobial drugs (isoniazid and rifampicin) that are provided with support to the patient by a health worker or trained treatment supporter [4]. The high number of TB cases worldwide is part of patient non-adherence with treatment programs, which allows for an increase in new TB cases [5]. Non-adherence of TB patients to treatment can be seen from the large number of TB patients who are resistant to standard therapy or what is known as Drug Resistant-Tuberculosis (DR-TB). There are 157,903 Drug Resistant-Tuberculosis (DR-TB) cases in 2020 [6]. To overcome this situation, since 1995 WHO has introduced the DOTs (Directly Observed Treatment, Short-course) strategy. The study states that knowledge is the biggest variable in this aspect of non-adherence, without neglecting other variables such as attitudes and behaviour of TB patients [7]. For this reason, the focus of TB control should be on increasing compliance and changing patient behaviour [8].
The World Health Organization (WHO) has provided a good strategy for managing TB, primarily targeting patient compliance, which has long been known as Directly Observed Treatment (DOT). The strategy consisted of standard treatment using Rifampicin for six months for new cases and eight months for repeat cases [9]. These repeat cases were patients who had dropped out of treatment or failed to undergo previous treatment [10,11]. So, the DOT strategy and program are fine. This strategy requires a better approach and is adapted to the conditions of society. The limitations of the officers who will run this program should be a consideration for the birth of innovations to find which approach is better to do to significantly improve and change the compliance and behaviour of TB patients [12,13]. The birth of a very progressive digital technology that began in the 20th century can be the main choice in solving the problem of treating tuberculosis in the community through innovations in delivering pre-existing programs [14]. In several decades, studies on the use of digital technology to improve TB patient adherence and behaviour have increased sharply in various parts of the world.
The term commonly known today for using mobile devices to support public health care and practice is ‘mHealth, as introduced by WHO. mHealth also includes all mobile devices that use wireless or Bluetooth technology [9]. mHealth is particularly suitable for adherence interventions, as it involves using devices such as smartphones, Personal Digital Assistants (PDAs), tablets and many others [15–18]. These devices support several media, such as Short Messaging Services (SMS) or text messaging, voice or video calls, and specialized software applications (Apps) [15]. Previous studies involving mHealth included Liu and his team, who used a telephone reminder system to increase TB patient compliance [11]. In addition, there are studies using media SMS to serve as reminders for TB patients with good results [19–21].
Based on our initial search of the available studies, the results still need to be clarified. There are no results that show the certainty of the effectiveness of mHealth used. In addition, most of the studies over the five years showed that mHealth variations were similar. Likewise, previous review studies evaluate a lot from just one mHealth variant. To that end, the current review aims to evaluate and provide an overview of mHealth RCTs on medication adherence in the patient with tuberculosis.
METHODS
Design
This review was compiled based on the 2020 Preferred Reporting Items for Systematic-review and Meta-Analysis (PRISMA) guidelines [22].
Eligibility Criteria
This review was restricted to studies published in English, and included studies published through 2018 to 2023. Study types were limited to RCTs. In this review, an intervention for adherence and behaviour were defined as any strategy (e.g., self-management for diseases, and medication reminder) to change or maintain patient’s adherence and behaviour to improve health. We included studies on interventions that used mobile devices (wireless and portable electronics including cellular phones, wearable devices, laptop, personal assistance devices, and tablet PC) or mobile technologies (any technologies that enable communication with remote areas, such as phone call, video call, short messaging service [SMS], multimedia messaging service, online-chat, and email) to promote medication adherence. Observational study, non-intervention study, case report, study protocol, and commentary were excluded in this review.
Information Source
A literature search was performed on several reputable databases, such as PubMed, Sciencedirect, CINAHL, and Cochrane. The search was carried out in the period November 2022 to January 2023.
Search Strategy
The keyword structure was compiled based on study population, intervention, comparison, outcome, and design were developed for the specific databases used. The search strategies for each database provided in the search string table (Table 1).
Selection Process
Two authors independently screened all titles and abstracts from the collected literature. Then read the entire text of each article to assess its eligibility based on predetermined inclusion criteria. Discrepancies that arise are resolved through discussion, even if it is possible to ask for the consideration of the first author. The selection process is described in detail in the PRISMA diagram.
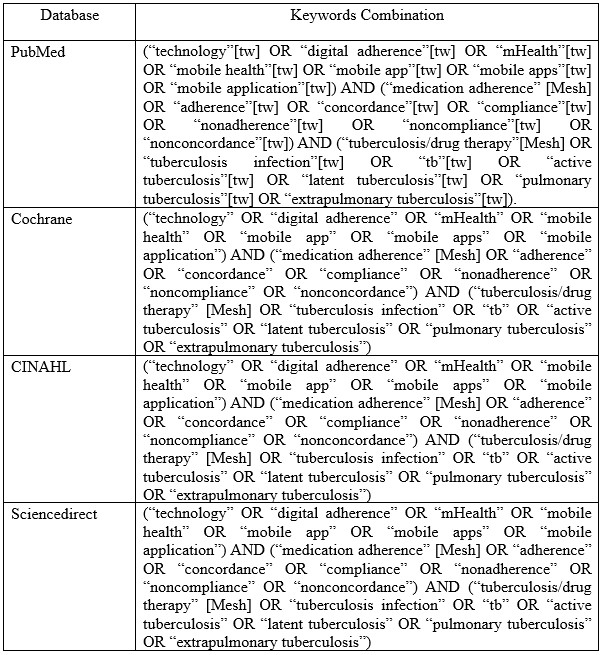
Table 1. Search string in databases
Data Extraction
DM and SR conducted eligibility evaluation based on the title and abstract. The full texts of potentially eligible articles were retrieved and assessed by DM, SR and MD conducted further independent verification of the abstract and full-text screening. Any disagreements among the reviewers were resolved by discussion. Data from the selected articles were extracted by DM, SR, MD and then verified by RM for relevant information, such as publication year, type of mHealth intervention, setting, population, main findings, and control groups.
Assessment of risk of bias in included studies
Two review authors independently assess the risk of bias of each included trial using the Cochrane ’Risk of bias’ assessment tool, and discuss any differences of opinion (Higgins et al., 2011). In the case of missing or unclear information, we will contact the trial authors for clarification. The Cochrane approach assesses risk of bias across six domains: sequence generation and allocation concealment (selection bias), blinding of participants and personnel (performance bias), blinding of outcome assessors (detection bias), incomplete outcome data (attrition bias), selective outcome reporting (reporting bias), and other potential biases. For each domain we will record the methods used by the trial authors to reduce the risk of bias and assign a judgment of either ’low’, ’high’, or ’unclear’ risk of bias.
RESULTS
Overall search on databases resulted in a total of 2,607 articles. After removing 2070 articles for duplication, ineligibility and other reasons, 537 articles were left ready for screening. In the end, 18 articles were declared eligible to be included in this review study after removing 16 articles for reasons including not being an RCT study, not being focused on TB, and being a protocol study.
In full regarding the process of searching for articles can be seen in figure 1, while, in table 2 we reported the characteristics of the articles included in our study
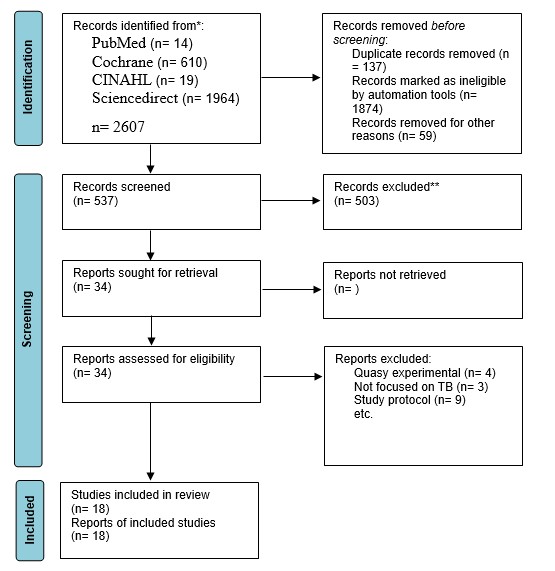
Figure 1. Flow diagram of the studies selection
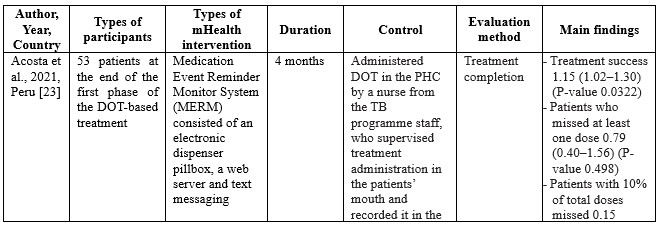

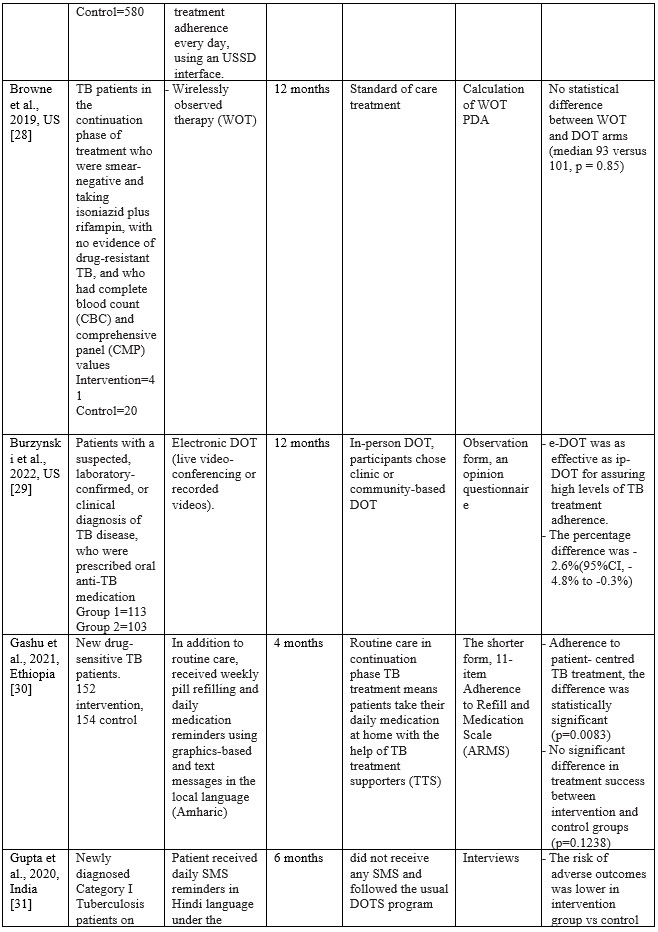
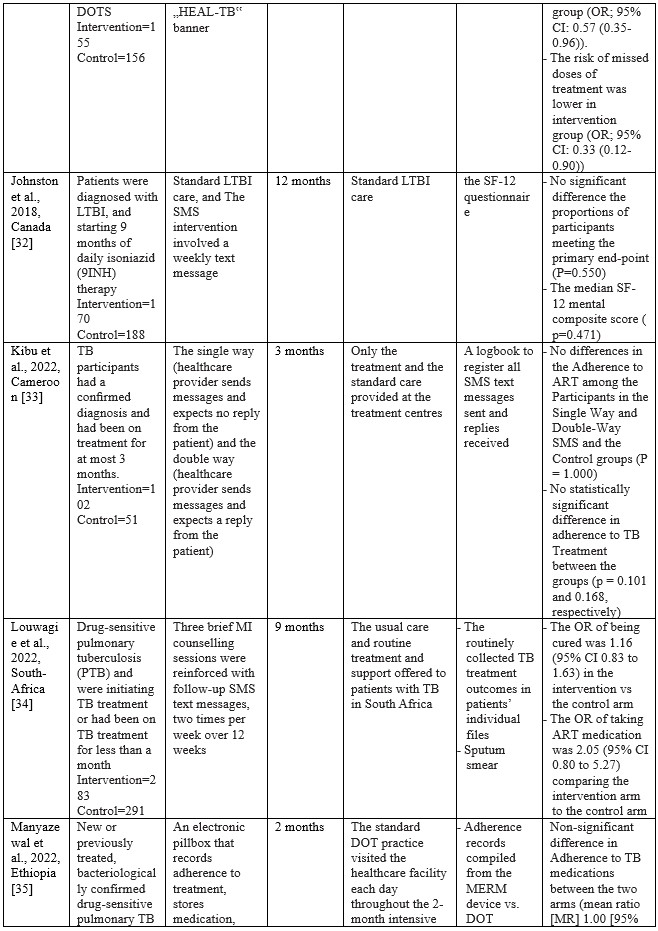
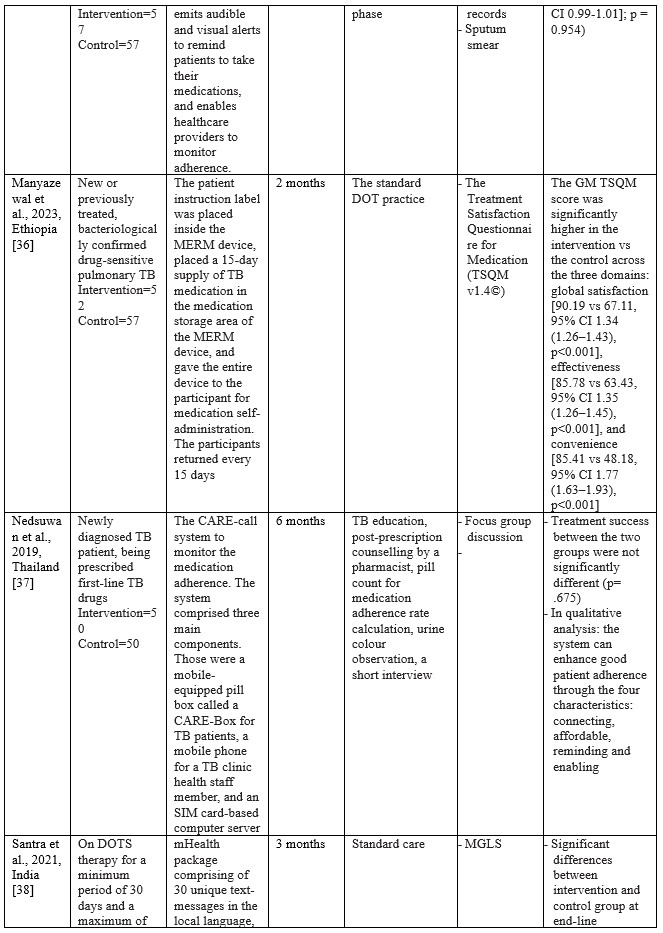

Table 2. Characteristics of Studies Included
Summary of Risk of Bias assessment
The risk of bias in eligible studies using The Cochrane Collaboration’s tool resulted in the conclusion that there were four studies with a high risk of bias and one unclear.
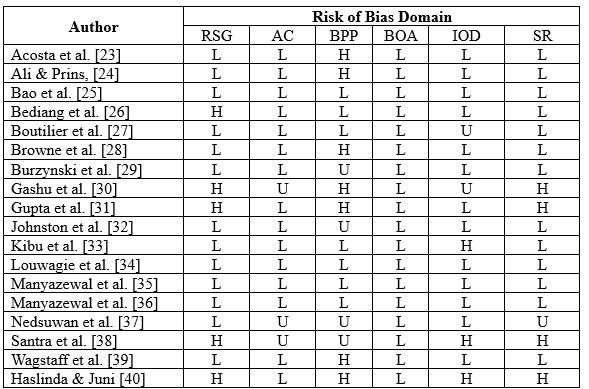
*RSG= Random sequence generation, AC= Allocation Concealment, BPP= Blinding Of Participants and Personnel, BOA= Blinding of Outcome assessment, IOD= Incomplete Outcome Data, SR= Selective Reporting; H= High risk of bias; U= Unclear risk of bias; L= Low risk of bias.
Characteristics of eligible studies
Studies on using m-health applications as innovations to improve adherence, change behaviour, and the success of TB treatment in the last decade have shown a significant increase. We have collected 18 RCT studies from several countries, including Ethiopia (n=3), South Africa (n=2), India (n=2), Cameroon (n=2), US (n=2), and one study each in Thailand, Peru, Sudan, China, Kenya, Canada, and Malaysia. The number of TB patients included in the study ranged from 61 to 1,189, ranging from 18 to 60 years. Most of the studies involved participants newly diagnosed with TB based on positive bacteriology, On DOTS therapy, smears, negative pulmonary tuberculosis (PTB), being prescribed first-line TB drugs, and drug-sensitive pulmonary tuberculosis (PTB). The shortest duration of intervention given was two months, and the longest was 12 months.
m-Health intervention used
Based on the collected studies, the applications used include Short Messages Service (SMS), Medication Event Reminder Monitor System (MERM), WeChat groups, USSD interface, Wirelessly observed therapy (WOT), Digital Adherence Technologies (DATs), Electronic DOT (live video-conferencing or recorded videos), The CARE-call system, and TB@Clicks (Whatsapp).
Several m-Health collected from eligible studies can be broadly grouped into software and hardware applications. In general, m-health applications that use software provide information as reminders and TB education in writing or pictures. Through the SMS route, various interventions are carried out, starting every day, every two days, twice a week, and every week [24,26,27,31–34,38,39]. Through the We-Chat application, there is no time limit for interactions between patients and supervisors taking medication; at any time, patients can discuss all obstacles and questions with supervisors and fellow patients [25]. As for the Whatsapp application, studies report that in the intensive phase, reminders are given to patients every day and 1 to 3 months after the intervention package is carried out [40]. Through telephone calls, patients are also reminded and controlled by supervisors. The duration of each phone call is 10 minutes [24,38].
The hardware used in the intervention includes the Medication Event Reminder Monitor System (MERM), which is a pillbox dispenser that will sound an alarm at the set time to take medicine [23,35,36]. This model is similar to another system called CARE box; it is just that, in this system, when the lid of the box is opened, it will automatically make a missed call to the server [37]. Another device is Wirelessly Observed Therapy (WOT), a sensory device that enters the body to record what the patient consumes, including TB drugs. The data stored on the sensor is linked to a mobile device as information material for supervisors [28]. For E-DOT, a camera device records real-time video of the patient’s medication-taking activities; this system is also used to conduct video conferencing between supervisors and patients [29].
Effects of m-Health on TB patient adherence
In summary, m-Health, with its various variants, has a positive effect in that patients experience increased adherence and changes in behaviour, even though this is not stated explicitly. Several studies have found a positive effect on treatment success related to patient adherence, with P values of 0.0322 [23,24], 0.88 [26], 0.001 [27], 0.85 [28], 0.1238 [30], 0.782 [31], 0.550 [32], 0.101 [33], 0.443 [34], 0.954 [35], 0.001 [36], 0.675 [37], 0.005 [38], 0.03 [40]. Meanwhile, changes in patient behaviour can be seen in findings such as increased self-management behaviour with a P value <0.001 [25], lower risk of missed doses [31], taking ART medication with an OR value 2.05 [34], return to the clinic with a P value of 0.001 [39].
Comparisons between the intervention and control groups in all studies showed no significant differences. However, the intervention using the m-Health variant showed superiority compared to the control group, most of which were in the main form of standard care, Directly Observation Treatment (DOT).
Using MERM, TB patient adherence to treatment is higher than the DOT standard, where TB patients are 1.15 times more compliant when intervened with MERM than the DOT standard [23]. The patients in the SMS intervention group had a lower failure rate (6.8%; 5 of 74 patients) compared to the control group (10.8%; 8 of 74 patients) [24]. In a study conducted by Bediang and colleagues using m-Health in the form of SMS, treatment success was higher in the intervention group compared to the control group (111 patients: 106 patients) [26]. Using SMS messages daily and an unstructured supplementary services data (USSD) interface shows that the probability of unsuccessful treatment outcomes for individuals in the intervention group is approximately 0.08 less than for individuals in the control group [41]. Browne and colleagues found that WOT was superior to DOT in supporting confirmed daily adherence to TB medications, where (3,738 out of 4,022) prescribed doses were confirmed in the WOT treatment, significantly different (p < 0.001) from the 63.1% (1,202 out) of 1,904) of prescribed doses observed in the DOT arm [28]. One hundred seventy-three patients completed the treatment program through the DOT electronic intervention [29]. One hundred ten patients out of a total of 139 TB patients adhered to treatment after intervention using a Mobile phone-based weekly refilling with a daily medication reminder system [30]. Gupta and colleagues found that the treatment success rates in the intervention group using SMS reminders were 86.4%, and the control group was 76.2% [42]. Louwagie and colleagues found that after six months of text SMS intervention, 120 of 133 patients adhered to the TB treatment given [34]. Manyazewal and colleagues using MERM found seven patients completed treatment compared to the control group of 5 [35]. Nedsuwan and colleagues found that using the mobile-based CARE-call system, the number of non-adherence patients in the intervention group was significantly lower than that of the control group (7.5% vs. 27.5%) [37]. Santra and colleagues found that the proportion of participants adherent to DOTS in the intervention group using phone calls and text messages increased from 85.5% at baseline to 96.4% at endline, postintervention [38]. Wagstaff and colleagues found that using SMS messages, as many as 62.0% of patients returned to the clinic in two days compared to 51.5% in the control group [39]. Using the Whatsapp message intervention, Haslinda and Juni found that the number of respondents who adhered to medication was higher in the group that received the intervention (81.8%) compared to the control group (69.1%) [40].
DISCUSSION
This systematic review study aims to evaluate and provide an overview of mHealth RCTs on medication adherence in the patient with tuberculosis which we have successfully conducted by collecting eighteen eligible studies from 2018 to 2022. One of the reasons we limited our literature search to the last five years was to see application innovations that were used along with the development of the digital world in this period. The expectancy is that the latest technological advances in this digitalization era will make it more straightforward to develop information innovations, especially concerning the health sector, to educate patients and the public.
Since the emergence of digital devices, health practitioners are increasingly competing to take advantage of this progress as a good opportunity to help improve public health in preventive and curative ways. M-Health has been attracting attention since it emerged as an innovation that effectively streamlines interactions between healthcare workers and patients, especially in supervising patients such as TB with strict rules for taking drugs for a certain duration. With a relatively lower cost, m-Health can be the first choice in addition to existing programs for monitoring TB patients. For this reason, this study provides an overview of the effectiveness of the m-Health variant from RCT studies in the 2018 to 2022 period regarding adherence and behaviour changes in TB sufferers during the treatment period. The m-Health variants used in the study are software and hardware. This review study analyzed m-Health variants that were not discussed in several previous systematic reviews [43–46].
The m-Health used in the last Five years
Until the last five years, SMS is still an option to remind TB patients to take their medicine. In contrast to previous review studies [45,46], the effectiveness of SMS in monitoring the treatment of TB patients in this review showed no significant difference between the SMS intervention group and the control group with standard care using DOT. Even using the Whatsapp application, TB patient compliance did not show any significance, even though adherence to treatment in the intervention group was higher than the control group [40]. However, with the widespread use of cellphones with the Android system or iPhone Operating System (iOS) among the public, choosing intervention using SMS or chat remains the best choice considering the low cost and efficient application. In contrast to the findings of Bao and colleagues in China, the We-Chat application used as an intervention showed a significant increase in adherence and repeat visits to the clinic during a TB treatment program [25]. Besides the effectiveness of existing smartphone-based applications, various obstacles can be faced, especially for populations in remote areas, where cellular networks and even the internet may be inadequate, especially if the quality of the patient’s cell phone does not support the use of these applications [47].
Behaviours expected of TB sufferers include not spitting, covering the nose and mouth when coughing or sneezing, and wearing a mask [48]. Of course, TB sufferers expect this behaviour to be carried out as one of the steps to prevent the spread of the disease in the surrounding environment [49]. However, the family should be involved in education on the prevention and care of TB patients. The family has an important role in the patient’s treatment process, including preventing the spread of the disease so that it does not affect the people who live in the same house and the people around the house. Families can provide arrangements at home according to good health standards, especially for TB patients. For this reason, further studies need to analyze this educational intervention for families with TB sufferers.
Some of the studies included in this review also provide interventions using a variety of hardware such as the Medication Event Reminder Monitor System (MERM), CARE box, Wirelessly Observed Therapy (WOT), and Electronic-Directly Observation Treatment (E-DOT). These devices are under recommendations from the World Health Organization (WHO) to increase the adherence of TB patients undergoing six months of treatment [14]. Of the six studies that implemented these hardware devices, overall, they showed better success than using software on TB patient adherence to taking medication. The MERM system allows TB patients to take medication daily because the device cover will open at a predetermined time [23]. Manyazewal and the team also used a MERM system with a tool called evriMED500, in the form of a pillbox consisting of a medicine container and an electronic module connected to an indicator light and an alarm [35,36]. The MERM system in the study did not show superiority over the standard care of the control group. However, it should be recognized that the adherence dimension has many independent variables that may play a large role in influencing interventions. Unfortunately, the study of the use of the MERM system that we found did not carry out an analysis of the potential factors. So that bias in the study is likely to occur.
Another device used is Wirelessly Observed Therapy (WOT), a sensory device that enters the body through the mouth. A patch detector in the torso area will read all sensor activity. The data recorded from the patch detector is transmitted wirelessly via Bluetooth technology to mobile phones, computers, or other gadgets [50]. Browne stated that WOT is very safe to apply without significant side effects, only in the form of minimal irritation due to the direct use of patches on the skin [28]. Statistically, WOT is superior to DOT; in other words, WOT is effective in increasing TB patient adherence to treatment. However, the application of WOT is likely to be constrained, especially in countries with lower middle incomes, because this technology is still relatively expensive, and there are suggestions to replace the patch every five days to avoid irritation [28]. Previous studies have also confirmed that using WOT can increase adherence to antiviral HCV therapy in populations at high risk of non-adherence [51].
Another hardware option we found in one study was the use of e-DOT in real-time or recorded video, depending on patient preference [29]. Real-time video allows patients to interact directly with TB program officers with the help of Skype software. Burzynski and colleagues found that e-DOT is similar to in-person-DOT but has equal effectiveness. For this reason, e-DOT can be applied according to the patient’s choice. Especially during a pandemic such as COVID-19, electronic DOT is the best choice to reduce the spread and worsen TB patients’ conditions, as found by Lippincott and colleagues in implementing the Vdot COVID-19 pandemic where this method has high effectiveness and is the first choice. In contrast, in-person DOT is recommended to be carried out later [52]. Haberer and Subbaraman added that implementing eDOT might encounter technical challenges, inaccuracies, costs, and an unsupportive health system [47].
The potential of mHealth on TB patient adherence
Compliance of TB patients with the treatment program can be seen from the success of the treatment. Of the various types of mHealth that we collected, almost all showed an increase in adherence of TB sufferers to the treatment given. Although, comparison with the control group mostly showed insignificant differences.
The use of SMS text generally shows more potential than the DOT standard. Two studies show that compliance with TB patients using SMS text interventions is similar to DOT standards [32,33]. The study states that there may be several factors that influence the failure of TB patient compliance even though they have been reminded via SMS messages, including the lack of more personalized engagement, the didactic nature of the messages, and the SMS message is received when the patient was not near his/her medication all contributed to the failure to reduce poor adherence [53]. For this reason, in the future, this can be a consideration in implementing interventions using text SMS, where controlling these situations is essential to consider. However, based on the success of increasing adherence from studies using text SMS, it was stated that patient compliance was one time greater than the DOT standard. The same thing was also found in the use of Whatsapp, where significant treatment success occurred in TB patients who were given education through messages via Whatsapp [40].
The medication event reminder monitor (MERM) system in studies using it also shows positive potential to improve TB patient adherence to treatment. In addition, using MERM can also reduce the workload of health workers [54]. One problem identified using MERM is the possibility of removal of the medication from the pillbox, for example, for work-related reasons, which prevents the recording of pill dispensing. Although the potential of MERM is not superior to in-person DOT, MERM can be used as an alternative to improve TB patient compliance. The identical thing is also found in using electronic DOT and WOT. This hardware allows stricter supervision and accurate recording of each drug-taking activity so that health workers can more easily measure treatment success.
LIMITATION
The limitations encountered in this review include limited access to several reputable databases, which does not allow us to explore further relevant articles. In addition, this review includes studies of low to high quality due to the small number of articles we have collected. For this reason, writers who want to use the results of this review must be careful and analyze them more carefully.
CONCLUSION
This review shows that using m-Health can be the first choice in handling TB cases with the DOT strategy. Hardware as part of mHealth has more potential to increase TB patient adherence and behaviour change. TB patient compliance with medication programs and stopping the spread of TB through good behaviour will be very significant in reducing TB cases, recurrent cases and new cases. mHealth is the best choice as a companion to the ongoing DOT program, primarily as a medium for disseminating information needed by patients during their treatment period. In the era of digitalization today and in the future, mHealth is undoubtedly the main route in health services, as illustrated during the pandemic of certain diseases that did not allow face-to-face meetings. However, further efficacy studies at the clinical level are needed, while always protecting privacy.
REFERENCES
- Acharya B, Acharya A, Gautam S, Ghimire SP, Mishra G, Parajuli N, et al. Advances in diagnosis of Tuberculosis: an update into molecular diagnosis of Mycobacterium tuberculosis. Molecular biology reports. 2020;47:4065–75.
- Asriati A, Kusnan, Adius, Alifariki L. Faktor Risiko Efek Samping Obat dan Merasa Sehat Terhadap Ketidakpatuhan Pengobatan Penderita Tuberkulosis Paru. JURNAL KESEHATAN PERINTIS (Perintis’s Health Journal). 2019;6(2):134–9.
- Putri S, Alifariki LO, Fitriani F, Mubarak M. The Role of Medication Observer And Compliance In Medication Of Pulmonary Tuberculosis Patient. Jurnal Kesehatan Prima [Internet]. 2020 Feb 29;14(1). Available from: http://jkp.poltekkes-mataram.ac.id/index.php/home/article/view/248
- World Health Organization (WHO). Tuberculosis [Internet]. 27 October 2022. 2022. Available from: https://www.who.int/news-room/fact-sheets/detail/tuberculosis
- Harding E. WHO global progress report on tuberculosis elimination. The Lancet Respiratory Medicine. 2020;8(1):19.
- Dean AS, Auguet OT, Glaziou P, Zignol M, Ismail N, Kasaeva T, et al. 25 years of surveillance of drug-resistant tuberculosis: achievements, challenges, and way forward. The Lancet Infectious Diseases. 2022;
- Ghozali MT, Murani CT. Relationship between knowledge and medication adherence among patients with tuberculosis: a cross-sectional survey. Bali Medical Journal. 2023;12(1):158–63.
- Asriati A. Faktor Risiko Ketidakpatuhan Pengobatan Penderita Tuberkulosis Paru di Kota Kendari. Jurnal Keperawatan Terapan (e-Journal). 2019;5(2):103–10.
- World Health Organization. Digital health for the End TB Strategy: an agenda for action. World Health Organization; 2015.
- El Emeiry F, Shalaby S, El-Magd GHA, Madi M. Treatment outcomes of tuberculosis among new smear-positive and retreatment cases: a retrospective study in two Egyptian governorates. The Egyptian Journal of Chest Diseases and Tuberculosis. 2019;68(3):274.
- Ying R, Huang X, Gao Y, Wang J, Liu Y, Sha W, et al. In vitro Synergism of Six Antituberculosis Agents Against Drug-Resistant Mycobacterium tuberculosis Isolated from Retreatment Tuberculosis Patients. Infection and Drug Resistance. 2021;3729–36.
- Margineanu I, Louka C, Vincenti-Gonzalez M, Saktiawati AMI, Schierle J, Abass KM, et al. Patients and medical staff attitudes toward the future inclusion of ehealth in tuberculosis management: perspectives from six countries evaluated using a qualitative framework. JMIR mHealth and uHealth. 2020;8(11):e18156.
- Zhang J, Yang Y, Qiao X, Wang L, Bai J, Yangchen T, et al. Factors influencing medication nonadherence to pulmonary tuberculosis treatment in tibet, china: a qualitative study from the patient perspective. Patient preference and adherence. 2020;1149–58.
- World Health Organization. Handbook for the use of digital technologies to support tuberculosis medication adherence. World Health Organization; 2017.
- Hamine S, Gerth-Guyette E, Faulx D, Green BB, Ginsburg AS. Impact of mHealth chronic disease management on treatment adherence and patient outcomes: a systematic review. Journal of medical Internet research. 2015;17(2):e52.
- Bartels SL, Van Knippenberg RJM, Dassen FCM, Asaba E, Patomella A-H, Malinowsky C, et al. A narrative synthesis systematic review of digital self-monitoring interventions for middle-aged and older adults. Internet interventions. 2019;18:100283.
- He Q, Zhao X, Wang Y, Xie Q, Cheng L. Effectiveness of smartphone application–based self‐management interventions in patients with type 2 diabetes: A systematic review and meta‐analysis of randomized controlled trials. Journal of advanced nursing. 2022;78(2):348–62.
- Zhu MM, Choy BNK, Lam WWT, Shum J. Randomized control trial of the impact of Patient Decision Aid (PDA) developed for Chinese primary open-angle glaucoma patients. Ophthalmic Research. 2023;
- Hirsch-Moverman Y, Daftary A, Yuengling KA, Saito S, Ntoane M, Frederix K, et al. Using mHealth for HIV/TB treatment support in Lesotho: enhancing patient–provider communication in the START study. Journal of acquired immune deficiency syndromes (1999). 2017;74(Suppl 1):S37.
- Mohammed S, Glennerster R, Khan AJ. Impact of a daily SMS medication reminder system on tuberculosis treatment outcomes: a randomized controlled trial. PloS one. 2016;11(11):e0162944.
- Farooqi RJ, Ahmed H, Ashraf S, Zaman M, Farooq S, Farooqi JI. Feasibility and acceptability of Mobile SMS reminders as a Strategy to improve drugs adherence in TB Patietns. Pakistan Journal of Chest Medicine. 2017;23(3):93–100.
- Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. International Journal of Surgery. 2021;88:105906.
- Acosta J, Flores P, Alarcon M, Grande-Ortiz M, Moreno-Exebio L, Puyen ZM. A randomised controlled trial to evaluate a medication monitoring system for TB treatment. The International Journal of Tuberculosis and Lung Disease. 2022;26(1):44–9.
- Ali AOA, Prins MH. Mobile health to improve adherence to tuberculosis treatment in Khartoum state, Sudan. Journal of Public Health in Africa. 2019;10(2).
- Bao Y, Wang C, Xu H, Lai Y, Yan Y, Ma Y, et al. Effects of an mHealth intervention for pulmonary tuberculosis self-management based on the integrated theory of health behavior change: randomized controlled trial. JMIR public health and surveillance. 2022;8(7):e34277.
- Bediang G, Stoll B, Elia N, Abena J-L, Geissbuhler A. SMS reminders to improve adherence and cure of tuberculosis patients in Cameroon (TB-SMS Cameroon): a randomised controlled trial. BMC public health. 2018;18:1–14.
- Boutilier JJ, Yoeli E, Rathauser J, Owiti P, Subbaraman R, Jónasson JO. Can digital adherence technologies reduce inequity in tuberculosis treatment success? Evidence from a randomised controlled trial. BMJ Global Health. 2022;7(12):e010512.
- Browne SH, Umlauf A, Tucker AJ, Low J, Moser K, Gonzalez Garcia J, et al. Wirelessly observed therapy compared to directly observed therapy to confirm and support tuberculosis treatment adherence: a randomized controlled trial. PLoS medicine. 2019;16(10):e1002891.
- Burzynski J, Mangan JM, Lam CK, Macaraig M, Salerno MM, deCastro BR, et al. In-person vs electronic directly observed therapy for tuberculosis treatment adherence: A randomized noninferiority trial. JAMA Network Open. 2022;5(1):e2144210–e2144210.
- Gashu KD, Gelaye KA, Lester R, Tilahun B. Effect of a phone reminder system on patient-centered tuberculosis treatment adherence among adults in Northwest Ethiopia: a randomised controlled trial. BMJ Health & Care Informatics. 2021;28(1).
- Gupta A, Bhardwaj AK, Singh H, Kumar S, Gupta R. Effect of ‘mHealth’Interventions on adherence to treatment and outcomes in Tuberculosis patients of district Shimla, Himachal Pradesh, India: A Randomised Control Trial. Indian Journal of Preventive & Social Medicine. 2020;51(3):125–36.
- Johnston JC, van der Kop ML, Smillie K, Ogilvie G, Marra F, Sadatsafavi M, et al. The effect of text messaging on latent tuberculosis treatment adherence: a randomised controlled trial. European Respiratory Journal. 2018;51(2).
- Kibu OD, Siysi VV, Albert Legrand SE, Asangbeng Tanue E, Nsagha DS. Treatment Adherence among HIV and TB Patients Using Single and Double Way Mobile Phone Text Messages: A Randomized Controlled Trial. Journal of Tropical Medicine. 2022;2022.
- Louwagie G, Kanaan M, Morojele NK, Van Zyl A, Moriarty AS, Li J, et al. Effect of a brief motivational interview and text message intervention targeting tobacco smoking, alcohol use and medication adherence to improve tuberculosis treatment outcomes in adult patients with tuberculosis: a multicentre, randomised controlled tri. BMJ open. 2022;12(2):e056496.
- Manyazewal T, Woldeamanuel Y, Holland DP, Fekadu A, Marconi VC. Effectiveness of a digital medication event reminder and monitor device for patients with tuberculosis (SELFTB): a multicenter randomized controlled trial. BMC medicine. 2022;20(1):310.
- Manyazewal T, Woldeamanuel Y, Getinet T, Hoover A, Bobosha K, Fuad O, et al. Patient-reported usability and satisfaction with electronic medication event reminder and monitor device for tuberculosis: a multicentre, randomised controlled trial. eClinicalMedicine. 2023;56:101820.
- Ratchakit-Nedsuwan R, Nedsuwan S, Sawadna V, Chaiyasirinroje B, Bupachat S, Ngamwithayapong-Yanai J, et al. Ensuring tuberculosis treatment adherence with a mobile-based CARE-call system in Thailand: a pilot study. Infectious Diseases. 2020;52(2):121–9.
- Santra S, Garg S, Basu S, Sharma N, Singh MM, Khanna A. The effect of a mhealth intervention on anti-tuberculosis medication adherence in Delhi, India: A quasi-experimental study. Indian Journal of Public Health. 2021;65(1):34.
- Wagstaff A, Van Doorslaer E, Burger R. SMS nudges as a tool to reduce tuberculosis treatment delay and pretreatment loss to follow-up. A randomized controlled trial. PLoS One. 2019;14(6):e0218527.
- Haslinda N, Juni MH. Effectiveness of health education module delivered through Whatsapp to enhance treatment adherence and successful outcome of tuberculosis in Seremban district, Negeri Sembilan, Malaysia. International Journal of Public Health and Clinical Sciences. 2019;6(4):145–59.
- Boutilier JJ, Jónasson JO, Yoeli E. Improving tuberculosis treatment adherence support: the case for targeted behavioral interventions. Manufacturing & Service Operations Management. 2022;24(6):2925–43.
- Das Gupta D, Patel A, Saxena D, Koizumi N, Trivedi P, Patel K, et al. Choice‐Based Reminder Cues: Findings From an mHealth Study to Improve Tuberculosis (TB) Treatment Adherence Among the Urban Poor in India. World Medical & Health Policy. 2020;12(2):163–81.
- Laksono EB, Johan A, Erawati M. The Utilization of Mobile-Health Intervention In Improving Treatment Compliance Behavior In Tuberculosis Patients. Nurse and Health: Jurnal Keperawatan. 2022;11(2):275–86.
- Shariful IM. Theories applied to m-health interventions for behavior change in low-and middle-income countries: a systematic review. Telemedicine and e-Health. 2018;
- Nglazi MD, Bekker L-G, Wood R, Hussey GD, Wiysonge CS. Mobile phone text messaging for promoting adherence to anti-tuberculosis treatment: a systematic review. BMC infectious diseases. 2013;13(1):1–16.
- Sarabi RE, Sadoughi F, Orak RJ, Bahaadinbeigy K. The effectiveness of mobile phone text messaging in improving medication adherence for patients with chronic diseases: a systematic review. Iranian Red Crescent Medical Journal. 2016;18(5).
- Haberer JE, Subbaraman R. Digital technology for tuberculosis medication adherence: promise and peril. Vol. 17, Annals of the American Thoracic Society. American Thoracic Society; 2020. p. 421–3.
- Lucya V. Prevention of Tuberculosis: Literature Review. KnE Life Sciences. 2021;630–4.
- Lönnroth K, Roglic G, Harries AD. Improving tuberculosis prevention and care through addressing the global diabetes epidemic: from evidence to policy and practice. The lancet Diabetes & endocrinology. 2014;2(9):730–9.
- Hafezi H, Robertson TL, Moon GD, Au-Yeung K-Y, Zdeblick MJ, Savage GM. An ingestible sensor for measuring medication adherence. IEEE Transactions on Biomedical Engineering. 2014;62(1):99–109.
- Bonacini M, Kim Y, Pitney C, McKoin L, Tran M, Landis C. Wirelessly observed therapy to optimize adherence and target interventions for oral hepatitis C treatment: observational pilot study. Journal of Medical Internet Research. 2020;22(4):e15532.
- Lippincott CK, Perry A, Munk E, Maltas G, Shah M. Tuberculosis treatment adherence in the era of COVID-19. BMC infectious diseases. 2022;22(1):800.
- Liu X, Lewis JJ, Zhang H, Lu W, Zhang S, Zheng G, et al. Effectiveness of electronic reminders to improve medication adherence in tuberculosis patients: a cluster-randomised trial. PLoS medicine. 2015;12(9):e1001876.
- Wang N, Zhang H, Zhou Y, Jiang H, Dai B, Sun M, et al. Using electronic medication monitoring to guide differential management of tuberculosis patients at the community level in China. BMC infectious diseases. 2019;19(1):1–9.
![]() This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
EFFECT OF GUIDED EDUCATION ON PERCEPTION AND ATTITUDE OF CHILDBEARING WOMEN TOWARDS CAESAREAN SECTION IN NIGERIA
Mary Idowu Edward1*, Oluwaseun Segun Bolarinwa2,
Omowumi Suuru Ajibade3, Temilola Mabel Aregbesola4
1,2,3, Department of Adult and Mental Health Nursing, Faculty of Nursing Science, University of Medical Sciences, Akure Campus, Akure, Ondo State,
4Basic Health Center Iloro, Akure, South, Ondo State, Nigeria
Corresponding Author: Mary Idowu Edward RN, RM, RNE, PhD. Nursing. Department of Adult and Mental Health Nursing, Faculty of Nursing Science, University of Medical Sciences, Akure Campus, Akure, Ondo State. Email: edwardmary@unimed.edu.ng

Cite this article
ABSTRACT
Background: Nigerian women are unwilling to have a Caesarean section because of the general belief that abdominal delivery is a reproductive failure on their part regardless of the feasibility of vaginal birth after Caesarean section and the decreasing mortality from Caesarean sections.
Aim: The primary objective of this study was to investigate the existence of a significant relationship between pregnant women’s knowledge and attitudes toward cesarean delivery before and after training.
Materials and Methods: The study employed a pre/post-test study design, using questionnaires to obtain data from 152 childbearing women attending antenatal in Iloro Basic Health Centre, Akure, Ondo State. Descriptive statistics were used to summarize and present data. Associations between variables were tested using Spearman correlation at a p-value 0.05 level of significance.
Results: The researcher found a significant relationship between the knowledge and attitude of pregnant women towards Caesarean section delivery before and after the training. The findings revealed an increase in the knowledge of mothers after the educational intervention, mothers would opt for a Caesarean section if it is necessary to protect them and the baby and they believe that it is a woman’s right to choose a Caesarean section for herself. Significant relationship exists between knowledge and attitudes toward the Caesarean section.
Conclusion: It was concluded that childbearing mothers still believe that vagina delivery is a natural delivery and there is joy attached to it, however, most women would still prefer vagina delivery to Caesarean section. The study recommends a need for awareness programs to enhance women’s and the community positive perception towards the Caesarean section in Nigeria.
Keywords: Guided Education, Perception, Attitude, Childbearing women, Caesarean Section
Introduction
Worldwide, Caesarean section accounts for about 15% of births. Caesarean section is one of the oldest procedures in obstetric practice and may be a necessary end in the termination of pregnancy to abort or minimize complications to the mother, foetus, or both [1]. At the onset, the operation was associated with high morbidity and mortality rates, largely because of the low level of medical science available at the time [2]. This type of surgery has been in existence throughout medical history and has steadily progressed from being one that is totally fatal to one that is safe for both the mother and the foetus [1]. In developed countries, the operation of Caesarean section has become well established with ease and safety, hence there is a lure for the procedure with women opting for it, increasingly for non-medical reasons [3]. It is the most commonly performed major obstetric operation in the world and there is no doubt that it has contributed to improved obstetric care throughout the world [4]. In Africa, the cesarean section is usually performed when a vaginal birth is deemed hazardous either to the foetus or the mother [5].
Available evidence pertaining to the population-based prevalence of Caesarean section in Nigeria reveals a threshold that is, far below the 10% recommended by the WHO [5]. Moreover, there has been no significant increase in the population-based Caesarean section rates for several years in Nigeria [7]. For instance, in 2008, merely 2% of births were delivered through a Caesarean section in Nigeria, and the rate remained unchanged in 2013. This is considerably low and suggests unmet needs which may contribute to poor maternal and neonatal outcomes in the country [5].
Interestingly, pregnant women’s perception of Caesarean section has been an essential consideration for providers of healthcare in the USA [7]. One of the major reasons is that a positive perception can lead to an effective adaptation to the maternal role whiles a negative perception can leave women with a sense of failure, loss of control, personal disappointment, and a cause to distrust their personal abilities as childbearing women, hence the need to promote positive perceptions in Caesarean section related issues [8]. For a healthy women population, the choice of delivery option is an important decision [9]. In developing countries, the negative perception of Caesarean section has led to the under utilization of the procedure[9]. Although there are many who consider the Caesarean section to be either safe or unsafe, more costly than the normal vaginal delivery, and more prone to complications than the SVD, there are some African women who perceive a Caesarean section to be a sign of female infidelity, a “curse,” or a “failure of womanhood”.
In a study carried out to assess the attitude of women toward a Caesarean section in Nigeria, it was found that vaginal delivery was the preferred mode of delivery by 93% of the respondents while 7% preferred a Caesarean section as the mode of delivery [11]. Expectant parents make many choices which usually include the site for delivery and the choice between spontaneous vaginal delivery and Caesarean section [10]. The reasons for this choice are being a natural process, being good for the mother’s health, and safety, and being an easy process [12]. Most of the women thought that Caesarean delivery can lead to long-term ill effects on the mother’s health. All the women who preferred elective Caesarean delivery initially said that they would rather opt for painless labour and vaginal delivery if offered over Caesarean section [11].
Nonetheless, the world health body emphasizes the need for Caesarean section service provision to every woman in need of it regardless of the prevailing population-based rates [13]. When medically indicated, Caesarean section has the potential for reducing maternal/neonatal mortalities and morbidities including delivery complications such as obstetric fistula [14]. However, a non-medically indicated Caesarean section has no associated additional benefits for mothers and newborns, rather like any surgery, it carries both short-term and/or long-term health risks [14]. Some studies have been conducted on Caesarean section utilization in Nigeria including a survey that examined the perception of pregnant women and found that a high proportion of the study participants were averse to Caesarean section delivery [5]. Significant associations between Caesarean section and parity, maternal weight, child’s birth weight, and previous Caesarean section were reported in another study [13]. However, it is not strange to hear many pregnant women ventilating the wrong attitude toward Caesarean section as an alternative method of birth [15]. In Nigeria, a number of women believe a Caesarean section is a last resort used to deliver pregnant women of their babies, many will even say, being told that they are going to deliver their babies through a Caesarean section is like giving a death warrant [13].
Traditionally, Nigerian women are unwilling to have a Caesarean section because of the general belief that abdominal delivery is a reproductive failure on their part regardless of the feasibility of vaginal birth after Caesarean section and the decreasing mortality from Caesarean sections. Inaccurate cultural perception about Caesarean section delivery accounts for the poor attitude of women towards Caesarean section [5]. Only one-third of women demonstrate a positive attitude towards Caesarean delivery as against 95.5% for vaginal delivery in the same group of respondents. The study concluded no significant differences in attitude and knowledge scores according to women’s levels of education [16]. It is necessary to note that the issue of vaginal birth is not only peculiar to developing countries but also to some developed countries. Women still choose vaginal birth after having a Caesarean section even in the case of postdates slated for elective Caesarean section. Hence, it is imperative to educate the average pregnant woman irrespective of her level of education and parity on Caesarean section. Therefore, this study assessed the effect of guided education on the perception and attitude of childbearing women toward Caesarean section.
Objectives of the study
- The primary objective of this study was to investigate the existence of a significant relationship between pregnant women’s knowledge and attitudes toward cesarean delivery before and after training.
- The secondary objective of the study was to describe the levels of knowledge and attitude of childbearing mothers about cesarean section before and after the educational intervention and the factors for not accepting cesarean section as a mode of delivery among women.
Hypothesis
HO1: There is no significant relationship between the knowledge and attitude of pregnant women towards Caesarean section delivery before and after the intervention.
Materials and Methods
Study Design, Population, and Area
The study utilized a quasi-experimental pre/post-test design. This design was adopted by the researcher because it will help to ascertain the effect of guided education on the perception and attitude of childbearing women towards Caesarean section in Basic Health Center Iloro, Akure South Local Government Area. The research setting for this study is Basic Health Center Iloro, Akure South Local Government Area. The head-quarter of Akure South Local government area is Akure town. Akure is a city in southwestern Nigeria and the capital of Ondo State. The metro area population of Akure in 2022 was 717,000 a 3.76% increase from 2021 which was 691,000[17]. Basic Health Center Iloro is a step above your ordinary health center, they make the provision of primary health care a full package. Health professionals and caregivers are available to give postnatal care.
The population of this study was composed of childbearing women attending the antenatal clinic in Basic Health Center Iloro, Akure South Local Government Area. The study population was randomly selected.
Sample Size Estimation, Sampling Technique, Data, collection, and Analysis
To estimate the minimum number n of childbearing women to investigate the effect of guided education on the perception and attitude toward Caesarean section, we considered the Gaussian theory [18]:
where N is the population size from which the sample size was defined. It resulted that the minimum estimated sample size of childbearing women required for a survey of a population of 255 mothers is equal to 143. It is evaluated, considering a z-score at 95%, an error e = 10% and hypothesizing a prevalence p equal to 70% about the impact of guided education. In addition to reduce statistical biases connected to information/data loss the sample size is enlarged to 152 mothers.

Instruments
The research instrument used was developed ad hoc, considering an extensive search of empirical studies on caesarian sections and was administered before and after the nurse-led education [9,19,21,22,23]. The instrument has the following sections: Demographic characteristics of the respondents (7 items), knowledge of childbearing mothers on caesarean section (8 items), perception of the childbearing mother towards the caesarean section (7 items) and the attitude of a childbearing mother towards the caesarean section (10 items), and factors for not accepting caesarean section as the mode of delivery among the women (8 items). The reliability test of the instruments was Cronbach’s alpha value of 0.83. The demographic, knowledge and factor data were scored using frequency and percentage while perception and attitude data were scored using 3 point likert scale of Agree, Not Sure and Disagree while factors data was obtained using 5 likert scale of strongly agree, agree, Not Sure, disagree and stongly disagree.
Procedure for data collection
The data was collected over a period of 4 weeks. All pregnant women were qualified to be included in the study hence need to randomly select about 20 manageable women during the antenatal visit (two Antenatal clinics per week) out of more than 60 attendance to prevent disruption of antenatal clinic activities and efficiency in data collection. The selected 20 women having been informed about the study and consent gained were administered the pretest. The education intervention which is already prepared materials on what Caesarean section is, when is it needed, types, and how to prepare for a Caesarean section are included in the module of training. The questionnaires were administered at the end of the intervention, that is, post-test.
Statistical analysis
Descriptive analysis like percentages and frequency tables were used to present the summary of the data, Cronbach’s alpha was utilised to test reliability of the instrument and Spearman correlation was used to test the hypotheses – relationship between knowledge and attitude at a 0.05 level of significance. Data were analyzed using the statistical package for social sciences (SPSS) version 20. The knowledge variable was defined by assigning points based on the affirmative response of Yes or No. For example if the number of participants who has correct answer to the questions is below 50%, 1point is assigned, if they are between 50-75% 2 points is assigned while 3points is assigned for participants between 76-100%. The maximum obtainable points of 8 knowledge items is 24 points while the minimum is 8 points. Therefore knowledge is graded thus: 1-8(Low knowledge).9-16 (Medium knowledge) while 17-24 (High Knowledge). The Perception and attitude were scored based on 3 points likert scales thus: Agree(3), Disagree (2) and Not Sure (1). the maximum obtainable score for Perception (7 items) is 21 and the minimum is 7. The maximum obtainable scores for attitude is 30 while the minimum is 10. Factors questionaires were graded on 5 points likert scales. The maximum obtainable mark is 35 while the minimum is 7.
Ethical considerations
Letter of introduction and intention of the study was taking to the Primary Health Care Authority and written permission was obtained. The study is not an invasive study, no formal approval by the Local Ethics Committee was required for this study hence no protocol number was indicated on the letter but the reference number PHCA/AK-S/020/124. However, the participants informed consent were obtained and willingness to participate was expressed before inclusion in the study. All participants were assured anonymity and confidentiality.
Results
Table 1 revealed the socio-demographic characteristics of the respondents.
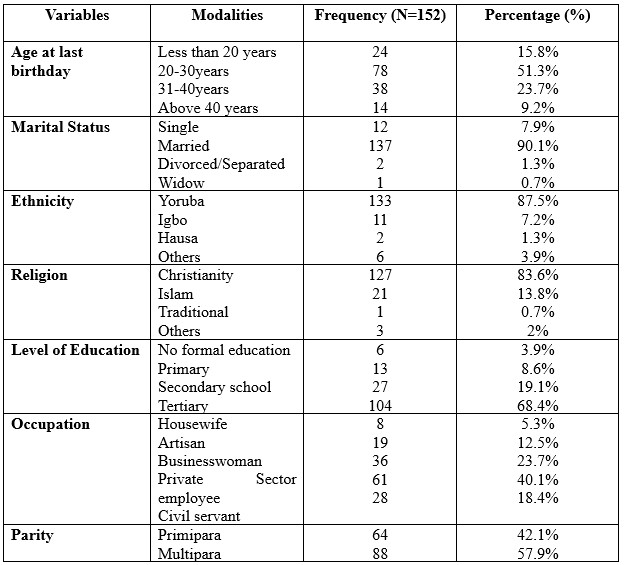
Table 1. Socio-demographic characteristics of the 152 respondents.
The respondents are 152 in number. Of the 152 respondents, 51.3% of the participants fall in the
age group between 20-30 years, and 90.1% are married. 87.5% are Yoruba and 83.6% are Christians. Findings further showed that 68.4% had tertiary education, 40.1% were private sector employees and 57.9% were multipara.
Table 2 above shows the knowledge of childbearing mothers on Caesarean section. Before the intervention, the participants had medium knowledge, that is, the score of 16 which is 66.7% of the responses from study participants while after the intervention, the participants had high knowledge of Caesarean section, that is, the score of 24 which is (100%) of obtainable knowledge scores.
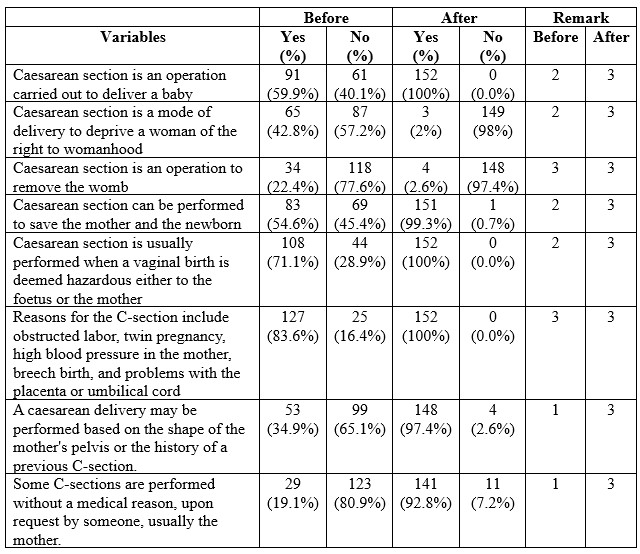
Table 2. Knowledge of 152 childbearing mothers on Caesarean section
Table 3 below shows the perception of childbearing mothers toward Caesarean section. The training improves the perception of mothers toward Caesarean as a method mode of delivery. All the respondents (100%) stated that vaginal delivery is a natural and acceptable mode of delivery.
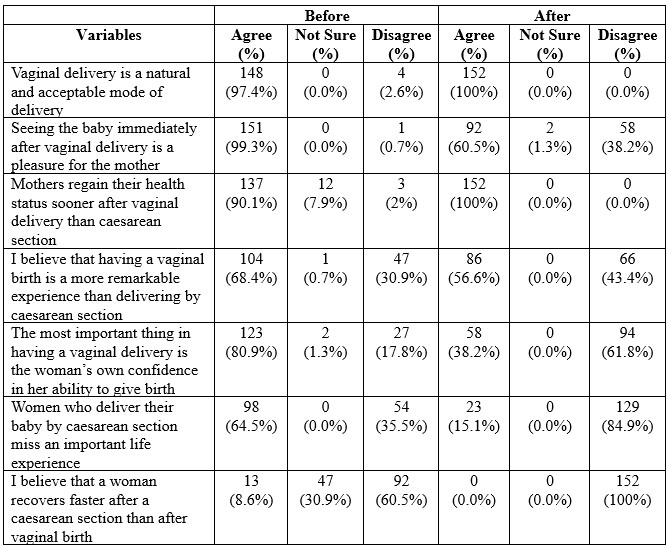
Table 3. Perception of 152 childbearing mothers toward Caesarean section.
Table 4 below shows the attitude of childbearing mothers towards Caesarean section as the accepted mode of delivery among women. Before the training, many mothers had negative attitudes towards Caesarean but this improves after the training.
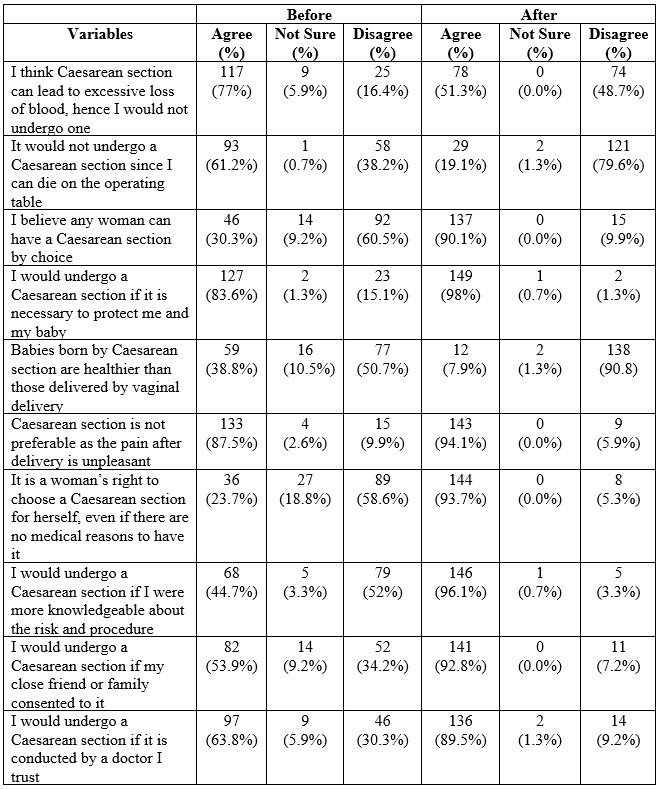
Table 4. The attitude of 152 childbearing mothers towards Caesarean section.
Table 5 above shows factors for not accepting Caesarean section as the mode of delivery among women. The women stated that fear of death, fear of pain, cost of the operation, cultural belief, being a subject of ridicule by friends, husband disapproval, and religion for not accepting Caesarean section as the mode of delivery among the women.

Table 5. Factors for not accepting Caesarean section as the mode of delivery among 152 women.
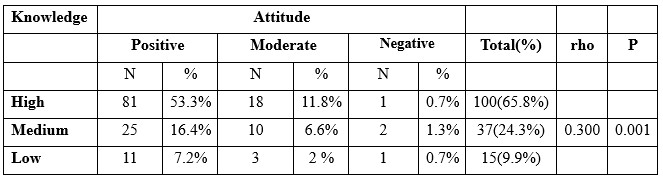
Table 6. Spearman correlation between knowledge and attitude of pregnant women towards caesarean section delivery.
Spearman correlation analysis test was carried out to determine the relationship between knowledge and attitudes, obtained p < 0.001 indicating that p <0.05. H0 is rejected and H1 is accepted, it can be concluded that there is a significant relationship between knowledge and attitude of pregnant women towards caesarean section delivery. It is found that rho = 0.300 and the direction of positive correlation (+). It can be concluded that the strength of the correlation between knowledge and attitude is low, which means that even though in this study there is a significant relationship between the two variables, there are still many factors that influence knowledge and attitude. The results of this study also show a positive correlation direction (+), which means that the relationship between knowledge and unidirectional attitude – meaning that the higher one’s knowledge, the better the attitude.
Discussion of findings
The discussions made on the findings of this study are presented in accordance with the research questions. The sub-headings under which the discussions are provided show in specific what each research question seeks to find.
Demographic characteristics of respondents
Findings from this study revealed that the average age of the respondents is 27 years. The majority (90.1%) were married and multipara and the population were dominated by Yoruba and Christians. More than half of the respondents had tertiary education. This was similar to the study of [19] on the attitude of pregnant women in southwestern Nigeria. The findings are in line with the study of [19]on the perception and attitude of pregnant women towards Caesarean section delivery in the University of Port-Harcourt Teaching Hospital, Rivers State, in which the majority of respondents between the age group of 25-29 years, and 85.9% were married.
Knowledge of childbearing mother on Caesarean section
Based on the findings from this study, it was revealed that there was an increase in the knowledge of mothers after the educational intervention on Caesarean section. The increased level of knowledge among pregnant women may be attributed to the educational intervention and information provided during the training. This is in consonant with the study of [20,21,22] who reported that majority of the women have good knowledge about caesarean section. The study of [23] on pregnant women’s knowledge, perception, and attitudes towards the Caesarean section also showed that the majority of women had adequate knowledge and were aware of all of the factors concerning Caesarean section deliveries. This study was in contrast with the study of [24] who reported good knowledge of 17.4% on Caesarean section delivery. [25] also found that there was a low overall knowledge of mothers about the modes of delivery.
Perception of the Childbearing Mothers towards Caesarean section
The findings from this study revealed that the majority of mothers had a poor perception of a Caesarean section before the training; however, there was an increase in the mothers’ score on the perception of Caesarean section among childbearing mothers after the intervention. Childbearing mothers still believe that vagina delivery is a natural delivery and has joy attached to it, and most women still prefer it over Caesarean section[25]. The study of [27] reported that having a Caesarean section takes away from the joy of giving birth and was of the view that Caesarean section births are not natural and should be reserved for those with medical issues or those who fear pain.
The attitude of Childbearing Mothers toward Caesarean section
The findings from this study revealed improved scores in the attitude of mothers toward Caesarean section. The majority of the mothers reported that they would opt for Caesarean section if it is necessary to protect them and their babies, and they believe it is a woman’s right to choose a Caesarean section for herself, even if there are no medical reasons to have it. They were also of the opinion that Caesarean section is not preferable as the pain associated with it post-delivery is unpleasant. Although before the training majority thought Caesarean section can lead to excessive loss of blood and they could die on the operating table. This assertion corresponds to the finding of [23] who submitted that the fear of death, complications, and other negative perceptions about Caesarean section make women unwilling to opt for it. The study of [28] on perception and attitude towards Caesarean section in Niger/Delta reflected that 83.2% of mothers would accept Caesarean section if it is a necessity that will protect them and their babies [29].
Factors for not accepting Caesarean section as the mode of delivery among the women
Findings from this study revealed fear of death, fear of pain, cost of the operation, being seen as a failure, cultural belief, husband disapproval, and religion were the factors revealed by the mothers for not accepting Caesarean section as the mode of delivery. [31] listed fear of death, denial of womanhood, expensive mode of delivery, and the possibility of being exposed to insults as reasons for opposing Caesarean section for delivery. [29] stated maternal autonomy, women empowerment and gender inequality as several women often need to take permission from their husbands and/or religious leaders before making health-related decisions[29]. According to [30] women’s decision-making in consultation with relatives is the main influencer to accept elective caesarean section.
Discussion of the hypothesis
The primary objective of this study was to investigate the existence of a significant relationship between pregnant women’s knowledge and attitudes toward cesarean delivery before and after training. The secondary objective of the study was to describe the levels of knowledge and attitude of childbearing mothers about cesarean section before and after the educational intervention and the factors for not accepting cesarean section as a mode of delivery among women. Based the inferential statistics carried out in this study, it was revealed that there is a significant difference between the pre and post-intervention knowledge of Caesarean section, and pre and post-intervention attitudes of pregnant women towards Caesarean section delivery. Similarly, [32] found a significant difference between pre and post-intervention knowledge and pre and post-intervention attitudes of pregnant women to Caesarean section. Contrary to these findings, there was no significant association between knowledge about Caesarean section and respondents’ characteristics in relation to age, marital status, occupation, and previous place of delivery [33].
Conclusions
Nigerian women are unwilling to have Caesarean section because of the general belief that abdominal delivery is a reproductive failure on their part regardless of the feasibility of vaginal birth after a Caesarean section and the decreasing mortality from Caesarean sections. The primary objective of this study was to investigate the existence of a significant relationship between pregnant women’s knowledge and attitudes toward cesarean delivery before and after training. The secondary objective of the study was to describe the levels of knowledge and attitude of childbearing mothers about cesarean section before and after the educational intervention and the factors for not accepting cesarean section as a mode of delivery among women. The study revealed an increase in the mothers’ knowledge about Caesarean section after the intervention. In addition, both perception and attitude towards Caesarean section improved following the intervention. The researchers found a significant relationship between the knowledge and attitude of pregnant women towards Caesarean section delivery before and after the intervention. It was concluded that the childbearing mothers still believe that vagina delivery is a natural delivery and there is joy attached to it, most women would only agree to have Caesarean section if the need arises but they would still prefer spontaneous vagina delivery.
Recommendations
Based on the findings, the following recommendations are made:
- There is still a need for awareness programs to increase women’s and community’s understanding about Caesarean section in Nigeria.
- Our society needs further enlightenment on the advantages of antenatal care attendance and hospital deliveries as the problem is rooted in our culture.
- Local, State and Federal Governments should subside the costs of maternity services through an all-inclusive National Health Insurance Scheme. This will go a long way to encourage women to accept Caesarean section when the need arises.
Limitations
The research was carried out in just one health center (Iloro Comprehensive Health Center) in Akure Local government are of Ondo State due limited funds. Future research should utilise more facilities to enhance generalisation.
Conflicts of interest and sources of funding:
None declared. This research did not receive any specific grant from funding agencies in the public, commercial, or not for profit sectors.
Author contributions: All authors equally contributed to the conduct of this study and to preparing this article.
Acknowledgments
The authors appreciate the Management of Basic Health Centre Iloro, Akure, Ondo State, Nigeria, and all the mothers that participated in the study for their cooperation.
References
- Cunningham, F.G., MacDonald, P.C., Gant, N.F., Leveno, K.J, Gilstrap, L.C. & Hankins, G. (2017). Caesarean delivery and Caesarean In: Cunningham, et al, editors. Williams Obstetrics, 20th edition. Stamford, CF: Appleton & Lange; p. 509-31.
- Kerr-Wilson R. (2018). Caesarean section on demand. In: Current Obstetrics and Gynaecology. Harcourt Publishers: 126-28.
- Gomen, R., Tamir, A. & Degani, S. (2014). Obstetricians’ opinions regarding patient choice in caesarean delivery. Obstet Gynecol.;99(4):577 -80.
- Ohanson, R.B., EI-Timini, S., Rigby, C., Young, P. & Jones P. (2019). Caesarean section by choice could fulfi11the inverse care law. Eur J Obstet Gynecol Reprod BioI.;97(1):20-2.
- Ezeonu,P. O.. Ekwedigwe, K. C., Isikhuemen,M. E., Eliboh,M. O., Onoh, R. C., Lawani,L. O., Ajah,L. O. & Dimejesi,E. I. (2017). Perception of Caesarean Section among Pregnant Women in a Rural Missionary Hospital.Advances in Reproductive Sciences, Vol.5 No.3.
- Egwuatu, V.B. & Ezeh, I.O. (2018). Vaginal delivery in Nigeria Women after a previous section. Int J Gynaecol Obstet.;32: 1-6
- Coleman, V.H., Lawrence, H. & Schulkin, J. (2019). Rising Cesarean Delivery Rates. The Impact of Cesarean Delivery on Maternal Request. CME review article 4. ObstetGynecol survey.; 64: 2.
- Penna, L. (2014). Caesarean section on request for non-medical indications. Current Obstet. Gynaecol.; 14: 220-223.
- Naa Gandau, B.B., Nuertey, B.D., Seneadza, N.A.H. et al. Maternal perceptions about caesarean section deliveries and their role in reducing perinatal and neonatal mortality in the Upper West Region of Ghana; a cross-sectional study. BMC Pregnancy Childbirth 19, 350 (2019). https://doi.org/10.1186/s12884-019-2536-8
- Danon, D., Sekar, R., Hack, K.E & Fisk, N.M. (2013). “Increased stillbirth in uncomplicated monochorionic twin pregnancies: a systematic review and meta-analysis”. Obstetrics & Gynecology. 121 (6): 1318–26. doi: 10.1097/AOG.0b013e318292766b. PMID 23812469. S2CID 5152813.
- Onah H.E. & Ugona M.C. (2014). Preference for Caesarean section or symphysiotomy for obstructed labour among Nigerian women. IJOG 2004; 84: 70-91.
- Ezechi, O.C., Fasuba, O.B., Kalu, B.E., Nwokolo, C.A. & Obiesie, L.O. (2014). Caesarean Delivery: Why the aversion? Trop J ObstetGynaecol.; 21 (2): 164-167.
- Chigbu, C. & Iloabachie, G. (2017). The burden of Caesarean section refusal in a developing country setting. BJOG: An International Journal of Obstetrics & Gynaecology; 114: 1261 – 1265.
- Bonney, E.A. & Myers, J.E. (2015). Caesarean section: Techniques and complications. Obstet. Gynaecol Rep Med; 21(4): 97 – 102. http://.dx.doi.org/10.1016/j.ogrm.
- Etuk, S.J. & Ekanem, A.D. (2017). Socio-demographic and Reproductive Characteristics of women who default from orthodox obstetrics care in Calabar, Nigeria. Int. J. Gynaecol. Obstet; 73: 57-60.
- Awoyinka, B.S., Ayinde, O.A & Omigbodun, A.O. (2016). Acceptability of Caesarean delivery to Antenatal patients in a tertiary health facility in south west Nigeria. J Obstet Gynaecol.; 26(3); 208-210.
- United Nations – World Population Prospects: Akure, Nigeria Metro Area Population 1950-2023: -Akure – Historical Population Data https://www.macrotrends.net/cities/21978/akure/population; Retrieved 2023-03-08.
- Colton T., Statistics in Medicine. Little Brown & Co. 1974.
- Faremi, A., Ibitoye I., Olatubi M., Koledoye, P. & Ogbeye G. (2014). Attitude of pregnant women in south western Nigeria towards caesarean section as a method of birth. Int J Reprod Contracept Obstet Gynecol.;3(3):709-714. DOI: 10.5455/2320-1770.ijrcog20140970.
- Robinson-Bassey, G. & Uchegbu, J. (2017). Perception and attitude of pregnant women towards caesarean section delivery in University Of Portharcourt Teaching Hospital, Rivers State. International Journal for Research in Health Sciences and Nursing, Volume-2, Issue-4.
- Orukwowu, U. & Ene-Peter, J. (2022). The Knowledge and Attitude of Pregnant Women towards Cesarean Section in the University of Port Harcourt Teaching Hospital (UPTH). IPS Journalof Basic and Clinical Medicine, 1(3), 1–12. https://doi.org/10.54117/ijbcm.v1i3.3
- Al Sulamy, A. , Yousuf, S. & Thabet, H. (2019) Knowledge and Attitude of Pregnant Women toward Elective Cesarean Section in Saudi Arabia. Open Journal of Nursing, 9, 199-208. doi: 4236/ojn.2019.92020.
- Dorkenoo, J.E. & Abor, P.A. (2021). Pregnant women’s knowledge, perception and attitudes towards caesarian section among obstetrics unit attendants in a teaching hospital. Res. J. of Health Sci. Vol 9(3). http://dx.doi.org/10.4314/rejhs.v9i3.2.
- Saoji, A., Nayse, J., Kasturwar, N. & Reiwani, N. (2017). Women’s knowledge, perception and potential demands towards caesarean section. National Journal of Community Medicine 2(2): 244-248.
- Nusrat, N., Nisar, A. S. & Ahson, M. (2019). Knowledge, attitude and preferences of pregnant women towards modes of delivery. Journal of Liaquat University of medical and Health Sciences, 8 (3): 228-233.
- Gamble, J.A. & Creedy, D.K. (2015). Women’s preference for a caesarean section: incidence and associated factors. Birth. 28(2):101-10.
- Dorkenoo, J.E. & Abor, P.A. (2021). Pregnant women’s knowledge, perception and attitudes towards caesarian section among obstetrics unit attendants in a teaching hospital. Res. J. of Health Sci. Vol 9(3). http://dx.doi.org/10.4314/rejhs.v9i3.2.
- Sunday-Adeoye, I. & Kalu, C.A. (2011). Pregnant Nigerian women’s view of cesarean section Nigerian Journal of Clinical Practice; 14(3), 276-279.
- Abah, M.G. & Umoh, A.V. (2015). Perception and attitude towards Caesarean section by pregnant women attending antenatal clinic in a Niger Delta tertiary facility. DOI: 10.47837/CMJ.19770126.201531167.
- Bam V, Lomotey AY, Kusi-Amponsah Diji A, Budu HI, Bamfo-Ennin D, Mireku G. Factors influencing decision-making to accept elective caesarean section: A descriptive cross-sectional study. Heliyon. 2021 Aug 11;7(8):e07755. doi: 10.1016/j.heliyon.2021.e07755. PMID: 34430742; PMCID: PMC8365447.
- Adewuyi, E.O., Auta, A. & Khanal, V. (2018). Prevalence and factors associated with underutilization of antenatal care services in Nigeria: A comparative study of rural and urban residences based on the 2013 Nigeria demographic and health survey. PLoS One;13:e0197324.
- Ashimi, A.O., Amole, T.G. & Aliyu, L.D. (2013). Knowledge and attitude of pregnant Women to caesarean section in a semi-urban community in northwest Nigeria. Journal of the West African College of Surgeons; 3(2), 46-61.
- Afaya, R.A., Bam, V., Apiribu, F., Agana, V.A. & Afaya, A. (2018) Knowledge of Pregnant Women on Caesarean Section and their Preferred Mode of Delivery in Northern Ghana, NUMID HORIZON: An International Journal of Nursing and Midwifery,; 2(1), 62-73.
![]() This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
THE IMPACT OF INTRODUCING A NURSING EDUCATION PROTOCOL ON THE INCIDENCE OF CLOSTRIDIUM DIFFICILE INFECTIONS IN THE HOSPITAL ENVIRONMENT: A QUASI-EXPERIMENTAL STUDY
Darija Knežević1*, Duška Jović1 & Miroslav Petković2
1. Department of Nursing, University of Banja Luka, Faculty of Medicine, Banja Luka, the Republic of Srpska, Bosnia and Herzegovina
2. Department of Microbiology and Immunology, University of Banja Luka, Faculty of Medicine, Banja Luka, the Republic of Srpska, Bosnia and Herzegovina
* Corresponding author: Darija Knežević, 1.Department of Nursing, University of Banja Luka, Faculty of Medicine, Banja Luka, the Republic of Srpska, Bosnia and Herzegovina. E-mail: darija.a.knezevic@med.unibl.org

Cite this article
ABSTRACT
Introduction: Increased virulence of Clostridium difficile and use of antimicrobial drugs in recent years represent a challenge in the treatment of these infections in healthcare institutions. Improving the overall knowledge on prevention and control of C. difficile infections (CDI) among nurses may be one strategies to help reduce the CDI incidence rate in hospital settings.
Objective: The research objective was to develop, implement and evaluate a protocol for the prevention of CDI in hospital environment through nurses’ education.
Materials and Methods: This study utilized a quasi-experimental pretest–post-test design, which was carried out in tertiary care hospital, Banja Luka, Bosnia and Herzegovina. The educational modules contained detailed description of prevention measures to prevent CDI transmission, and C. difficile toxins in faces were identified using laboratory enzyme immunoassays.
Results: The research included 60 nurses. There was a statistically significant difference (p=0.001) in the evaluation of knowledge in relation to professional experience and education level before the intervention. Nurses showed highly significant (p<0.001) better knowledge about C. difficile and CDI prevention on the test after the education. Before the education of nurses and technicians on preventive measures, CDI incidence was 11.04 per 10,000 patient – days, and after the education 6.49.
Conclusion: The study results showed that continuous medical education about CDI can have contribute to increasing knowledge and awareness about the importance of CDI prevention.
Keywords: Clostridium difficile, infection, prevention, nurses, education.
INTRODUCTION
Hospital-associated diarrhoeas are most often the result of an infection caused by Clostridium difficile (CDI), and the prevention of these infections has public health significance. Decreasing the CDI rate is challenging due to the complex pathogenesis, a many number of colonized patients and the presence of infectious spores [1,2]. The spreading of CDI is a consequence of the uncontrolled use of antibiotics and inappropriate control of hospital-acquired infections (HAI) [3-5]. Therefore, the prevention and control of CDI in healthcare institutions nowadays requires two basic approaches: preventing horizontal spreading of C. difficile and decreasing the risk of CDI in case the infection spreads. The first approach to CDI control involves isolating the infected patient and cleaning and disinfecting the hospital environment according to the guidelines [6,7]. Another approach is to control the use of antibiotics [8,9]. Strategies and guidelines for the prevention of CDI are based on a bundle of measures or a set of data that lead to the best possible outcome. The CDI prevention bundle consists of individual elements or interventions, as it follows: diagnostic testing, empirical control, contact isolation, hand hygiene and disinfection of the hospital environment. Successful implementation of the CDI prevention bundle depends on several persons: physicians, nurses, caregivers, personnel in charge of hygiene, family members and others who are in contact with patients [10]. Considering the high incidence of CDI, healthcare professionals should be familiar with the latest guidelines in the treatment and prevention of CDI [11,12]. Faecal microbiota transplantation (FMT), also called faecal transplantation or faecal bacteriotherapy, is one of the more important, newer approaches to the treatment of CDI. FMT is the infusion of a suspension of faces from a healthy donor into the colon of the CDI patient [13,14]. Nurses have an important role in the modern approach to the treatment of CDI patients, such as FMT and primarily if those patients are housed in an intensive care unit (ICU). Enteric preventive measures and proper isolation of patients with CDI are crucial care procedures [15,16]. Nurses should be alert that after FMT, antibiotic exposure can still lead to recurrent CDI [17]. There is evidence that educational interventions improve the knowledge and practice of nurses with regard to infection prevention both in hospitals and nursing homes [18,19]. Educational interventions included evidence-based information on the etiology, epidemiology, diagnosis, treatment, transmission and prevention of CDI, such as hand hygiene, isolation measures and the use of antibiotics [20-22]. Staff education is one of the most successful measures to prevent the spread of C. difficile, which should include not only medical staff (nurses and physicians), but also non-medical staff, especially those responsible for maintaining the hygiene of the hospital environment [23]. Spagnolo et al. (2018) presented in their research how a multidisciplinary approach to the prevention of CDI, which included several interventions, one of which was the education of nurses and hygiene personnel, proved to be successful in controlling the epidemic in one Italian hospital [24]. However, recent studies published that health workers are not properly following the CDI prevention measures. Some of the possible reasons include more and more complex preventive procedures that lead to confusion and gaps [25–27].
Data from the literature indicate that certain individual and socio-demographic factors, including knowledge, length of service or work experience, gender and type of profession influence adherence to infection prevention and control procedures [28]. However, even when hospital infection prevention protocols are followed, outbreaks of any infectious disease, including CDI, may occasionally occur. Therefore, it is important for nurses to update their knowledge on how to prevent HAI, and about the control and management of infections in healthcare facilities [29]. Continuous educational programmes, professional training and ensuring the availability of the necessary guidelines represent essential steps for improving the knowledge and practice of nurses in relation to the prevention of HAI [30]. Different educational strategies are being used to improve nurses’ knowledge and practice of infection control. Some of the most often used methods include quasi-experimental research in which control and target groups are subjected to both didactic and practical sessions, training based on pre-prepared scenarios, e-learning with a questionnaire and focus group discussions, and computer-assisted learning in infection control education [31]. Due to the rapid pace of scientific discoveries, technological innovations and social changes, knowledge quickly becomes outdated. Andragogy is a useful model for planning and facilitating adult learning [32]. Problem-based learning (PBL) is also an effective educational strategy that can improve critical thinking skills in infection prevention and control [33,34].
Nurses make the largest group of health workers in the healthcare system. They provide services in hospitals seven days a week throughout the year and are in close contact with patients and their families. Nurses working in different hospital departments play an important role in HAI prevention [35]. The present relevant literature has only a few published studies that evaluate the knowledge, perception and practice of nurses regarding CDI [36]. A recently conducted study from Bosnia and Herzegovina showed that nurses’ knowledge about CDI prevention is not at a satisfactory level, which indicates an increasing need for educating nurses about this issue [37].
Therefore, the present study was planned bearing in mind the importance of nurses in CDI prevention, and the importance of an educational intervention on the behaviour of nurses in the practice of infection control.
Objective: The research objective was to develop, implement and evaluate an educational module for the prevention of CDI in the hospital environment through the education of nurses in order to improve the level of knowledge and practice among them.
MATERIALS AND METHODS
Design
The research design used in this study was quasi-experimental design with one group design pretest-posttest approach.
Research Time and Place
The study was conducted in the University Clinical Centre of the Republic of Srpska (UKC RS) in Bosnia and Herzegovina, from April to June 2020.
Study Population
The target population consisted of nurses working in ICU, Clinic for Internal Diseases, Clinic for General and Abdominal Surgery, Clinic for Infectious Diseases and Clinic for Oncology.
Based on a G*Power 3.1.9.4 program calculation of medium effect size, power set at 0.80, and a set at 0.05, a minimum of 47 participants is required. Considering a typical dropout rate of 10% for the experimental design used, 57 is the minimum required sample. The scope in the study initially included 75 participants, but excluded 15 with incomplete answers. A final sample of 60 was reached of nurses who have fully completed the education program, pretesting, and post-testing. Participants were selected from the total population using a simple random technique.
Inclusion and Exclusion Criteria for Nurses population
According to the defined criteria for inclusion in the study, the subjects were nurses providing direct care to patients, of all educational profiles, employed at these clinics, aged 18-65, having passed the state exam (nurses licensed to practice) and working 8 and 12 hours shifts. Nurses working on administrative assignments were not included in the study, according to the defined criteria. The criteria for exclusion at the study were the nurses with incomplete answers.
Inclusion and Exclusion Criteria for Patients population
The study included patients with CDI who were older than 18 years of age and hospitalised at the Intensive Care Unit (ICU), Clinic for Internal Diseases, Clinic for General and Abdominal Surgery, Clinic for Infectious Diseases and Clinic for Oncology, from July to December 2019 (before the intervention) and from July to December 2020 (after the intervention). These clinics were selected for the purpose of the study because they treated patients with increased risk for CDI and had an increased incidence of C. difficile infections in 2019.
A case of hospital-acquired CDI (HA-CDI) was defined according to the criteria of the C. difficile Study Group of the European Society of Clinical Microbiology and Infectious Diseases as follows: any patient who developed symptoms of diarrhoea at least 48 hours after admission to the hospital (HA-CDI case with hospital onset); any patient who was admitted with symptoms of diarrhoea at the hospital with an onset of symptoms in the community within 4 weeks following discharge from the hospital (HA-CDI case with community onset) and patients who had stool samples positive for CD toxin A or B or positive for toxin-producing CD [25]. Only the first positive test for C. difficile in patients during the current hospitalization was included in the study. If patients had more than one positive test during the study period, we included only the first episode. Paediatric population of CDI patients, was not included in the study, along with community-acquired CDI.
Educational Intervention
The educational modules contained detailed description of prevention measures against the transmission of the C. difficile in hospital settings in accordance with the guidelines [6,7], and their implementation would affect the patient’s safety during hospitalisation and the treatment outcome. Each educational module was based on adult learning theories for interactive, self-directed learning, which developed interactive teaching, increased the motivation and interest of nurses, and at the same time made it easier to follow and remember the issue [31-33]. For more successful learning, we used numerous teaching aids (blackboard, flip chart, computers and LCD projector, moderation cards, models and figures). Each didactic session would start with a previously prepared Microsoft Office PowerPoint and video presentations followed by interactive group learning (discussions, case studies, and practical examples). The acquisition of planned knowledge and skills was the foundation for evaluating the success of each educational module.
Knowledge Assessment and Outcome Measures
Anonymous survey questionnaires in the form of a test to examine the knowledge and attitudes of nurses about CDI and its prevention were designed for the needs of this research based on the modified version of the questionnaire by Brady et al. [38] with additional questions about new prevent and treatment methods e.g. FMT according to the guidelines [6,7].
The knowledge was evaluated using multiple-choice questions with only one correct answer. The tests that were offered to the respondents at the beginning of the educational modules (previous test for evaluation of the baseline knowledge) and at the end of the session (final test to evaluate what was learned) were the same. These tests contained 10-15 questions divided into two parts, the first part: included questions about the social and demographic characteristics of the respondents, the second part: included questions related to the evaluation of knowledge about CDI and its prevention. Tests before and after the educational modules were numbered to correlate with each subject’s responses and were not correlated across modules for individual participants. We tested the hypothesis that after the training, the nurses’ knowledge about the prevention and control of CDI in hospital settings was significantly higher than the baseline knowledge.
Evaluation of CDI
The diagnosis of CDI is based on clinically identified diarrhoea and laboratory findings. The toxins of C. difficile in faeces were identified using laboratory enzyme immunoassays.
Ethical Considerations
The study was performed in accordance with the ethical considerations of the Helsinki Declaration. The study was approved by the Ethics Committee of the University of Banja Luka, Medical Faculty No: 18/4.4/20. Written consent for was obtained from all the subjects (nurses) who participated in the study. All data collected were confidential and used only by this study.
Statistical analysis
Descriptive statistics and percentages were used to calculate the answers to the questions. A correct answer to each question was graded with “1”, and an incorrect answer with “0”. The final score of knowledge was obtained by dividing the sum of correct answers by the number of questions, and multiplying the quotient of these two numbers by 10. In that way, it was possible to get a range of scores between 0 and 10. The incidence rate of hospital-associated CDI was calculated as the ratio of the number of infections/10,000 patient days. The incidence defined considering 10,000 according to European Society of Clinical Microbiology and Infectious Diseases (ESCMID) CDI-related guidance documents and the European Centre for Disease Prevention and Control (ECDC) protocol for CDI surveillance in acute care hospitals. Patient-days was calculated by summing the number of days in which a bed is occupied overnight by patients hospitalized during the surveillance period [39]. The level of knowledge before the education was described using Kruskal-Wallis test or one-way analysis of variance (ANOVA). To evaluate the effects of the reality based education program, Wilcoxon rank-sum were used for differences in knowledge before and after the education. Statistical hypotheses were tested at the significance level (alpha) of p˂0.05. Statistical analysis was done using IBM SPSS Statistics 26 software.
RESULTS
The characteristics of respondents in this study include gender, age, education level and years of experience. The age intervals were defined on the basis of the median value for the age of the respondents. The intervals of years of experience were determined based on the fact that we wanted to show whether the length of years in practice affects knowledge about CDI. The following is the frequency distribution of the respondents’ characteristics in this study:

Table 1. Demographic characteristics of study participants
The research included 12 (20%) nurses working at the ICU, and at clinics for internal medicine, abdominal surgery, infectious diseases and oncology. The majority of interviewed nurses were female – 51 (85%), with an average age of 31.06 ± 10.74 years. The highest percentage of respondents completed secondary medical school (70%) and most of them had professional experience of 1-15 years – 33 (55%) of them (Table 1).
Level of knowledge among participants with various lengths of work in the profession before application of the educational interventions, is presented in table 2:

Table 2. The level of knowledge among participants with various lengths of work in the profession before application of the educational interventions
Table 2 presents the descriptive statistics of the respondents’ baseline, theoretical knowledge before education on CDI in relation to the years of work experience in practice. There was a statistically significant difference (p=0.001) in the evaluation of knowledge in relation to years of experience in practice, meaning that knowledge about CDI was the highest among respondents with >15 years of experience in practice, and the lowest among those who had <1 years of experience.
Level of knowledge among participants with various education levels before application of the educational interventions, can be seen in table 3:

Table 3. The level of knowledge among participants with various education levels before application of the educational interventions
We determined a statistically significant difference in the average assessment of knowledge about CDI and the prevention of infections caused by this microorganism, in relation to the level of education (7.5 ± 1.0) (Table 3).
Based on the normality test, the statistical test used for the knowledge is Wilcoxon’s matched-pairs test, with the results as shown in the figure 1.
Figure 1 presented the nurses showed highly significant (p<0.001) better knowledge about C. difficile and CDI on the Module 1and 2 tests after the education. On the Module 1, the mean value of the total score on the knowledge test about C. difficile and CDI was significantly higher after the education (8.29 ± 1.18) compared to mean values of the total score on the test that was performed before the education (5.01 ± 2.00). The mean value of the total score on the CDI prevention knowledge test was significantly higher after the education (8.70 ± 0.67) compared to the mean values of the total score on the test that was performed before the education (4.5 ± 2.13) (Module 2).
SD=standard deviation; *** p<0.001; Wilcoxon’s matched-pairs test

Figure 1. Mean values of the total score of the Module 1 and 2 tests before and after the education
CDI incidence before and after the nurses’ education on CDI prevention measures, is presented in table 4.

Table 4. CDI incidence before and after the nurses’ education on CDI prevention measures
Before the education, in the period from 1 July to 31 December 2019, there were 74 patients diagnosed with CDI hospitalised at the UKC RS, whereas after the education of nurses on CDI prevention, in the period from 1 July to 31 December 2020, there were 42 patients diagnosed with CDI hospitalised at the UKC RS. Before the education of nurses on CDI prevention measures, the CDI incidence was 11.04 per 10,000 patient – hospital days. After education on CDI prevention measures, the incidence was 6.49 (Table 4).
DISCUSSION
CDI represents a challenging problem in the acute care environment. Nurses play in important role in the early recognition, diagnosis and rapid treatment of patients with this bacterial infection [40]. Due to the changing epidemiology and increased virulence of C. difficile, it was necessary to educate nurses on the implementation of contact prevention measures when in contact with patients with CDI in order to prevent the transmission of C. difficile to hospitalised patients, their families, and the nurses themselves. The targeted CDI prevention programme included the development and implementation of an evidence-based protocol [6,7] to improve compliance with prevention measures (hand hygiene, contact isolation, cleaning equipment and surfaces, taking care of patients).
Continuous education of medical staff about CDI represents the foundation in risk management in order to reduce the number of infections, as it enables the transfer of know-how, the development of appropriate procedures and leads to better internal communication. Health care personnel education on CDI could be more important than isolating infected patients in single rooms [41].
The results of this study, the nurses demonstrated better knowledge of C. difficile, prevention and control of CDI after the education. Other studies that also evaluated the impact of educational interventions in improving knowledge about infection prevention among nurses had similar results [42-44].
There is evidence to support the fact that both baseline knowledge, and the knowledge gained after an educational intervention on infection prevention, vary with the level of education, type of work, and years of professional experience [22,45]. The results presented here also showed that there is a statistically significant correlation with the level of nurses’ education and years of professional experience in relation to the level of knowledge about the prevention and control of CDI.
After reviewing the reference literature, we noticed that the knowledge of health workers about CDI, the ways of transmission and prevention differs between countries. The research conducted in England [46], USA [12,47] and South Africa [48] confirmed that nurses’ knowledge about CDI is not satisfactory. The research conducted in Poland demonstrated that despite the average score of 6.85 obtained for correct answers to questions that evaluated the knowledge of medical workers, this value was not satisfactory due to differences in the level of knowledge among different groups. Nurses showed a slightly higher level of knowledge than other health workers [45].
In order to recognize a patient with CDI, healthcare professionals should know how to recognise risk factors, as well as the symptoms present in patients. In the research of Legenza et al. the main barrier in recognising a patient with CDI was insufficient knowledge. Thirteen (50%) participants were not able to describe the risk factors for the occurrence of CDI, which could speed up the diagnosis [48].
The results of the research conducted by Aldeyab et al. [49] provided further evidence that a series of CDI control measures, focusing on risky antibiotics (reduction of quinolone antibiotics), education of staff, patients and their families, implementation of prevention measures and isolation, led to a significant reduction in the incidence of infection in three hospitals in Ireland. The research conducted by Wong-McClure et al. [50] showed similar situation, where infection control strategies implemented proved to be effective in achieving outbreak control and in maintaining the baseline C. difficile incidence rate following it.
Even though our educational modules intended for nurses included a part of units which referred to the use of antimicrobial agents, as the main risk factor for CDI, during the introduction of the protocol the use of high-risk antimicrobial agents was not limited because nurses do not prescribe antibiotics. However, numerous efforts in CDI prevention published in the literature report that antibiotic stewardship programs significantly reduce the incidence of infections and colonization with antibiotic-resistant bacteria and CDI in hospitalised patients [51].
The present study results showed that after educating nurses about CDI prevention measures, the incidence of CDI decreased, but it cannot be claimed that the education itself had an effect on the reduction of this hospital infection. However, some other studies have confirmed that education of nurses about CDI prevention along with control of antibiotic use in patient care can lead to reduction of CDI in acute care hospitals [52-54].
CONCLUSION
The knowledge test on C. difficile has confirmed statistically significant differences among nurses, and in prevention and control of CDI after the education compared to the average values of the total score on the test before the education. The study results showed that continuous medical education about CDI can have contribute to inreasing knowledge and awareness about the importance of CDI prevention.
Limitations
This study had several limitations. One limitation of this study is that we recruited nurses from a single hospital and specific findings may only generalize to settings with similar CDI prevention practices and a similar workflow. Consequently, repeated studies using this education program with nurses from other hospitals are needed. The study focuses on both competencies and skills in nurses. The initial plan for our study was to reduction of CDI. During the study, we did not monitor risk factors for CDI such as patient age, severity of the primary disease, and total antibiotic consumption, which would be necessary for this type of study.
Contact prevention measures, such as the use of personal protective equipment, frequent hand washing and disinfection of surfaces, maintaining distance and isolation of patients have been particularly strengthened since the beginning of the COVID-19 pandemic. It would be good to monitor how well nurses actually practice hand hygiene because epidemiological studies show that most HAI are caused by microorganisms that contaminate the hands of nursing staff. According to some authors, a properly adopted hand washing procedure reduces the risk of CDI infection by half [55]. Additionally, the total sample of subjects included less male persons, which could have influenced the results. However, conducting this type of study can provide guidelines to the hospital infection monitoring and control team so that not only nurses but also other health professionals and persons in charge of hospital hygiene can be educated about CDI in the future. It would be good if this type of CDI education for nurses would be repeated every 6 months and the educational modules are revised according to the new CDI prevention guidelines.
Funding statement
No funding sources were used to support the project.
Conflict of interest
The authors declare no conflict of interest.
Authors’ contribution
All authors equally contributed to preparing this article.
Acknowledgements
The authors would like to express special thanks to all participants in this study.
REFERENCES
- Barker AK, Ngam C, Musuuza JS, Vaughn VM, Safdar N. Reducing Clostridium difficile in the Inpatient Setting: A Systematic Review of the Adherence to and Effectiveness of C. difficile Prevention Bundles. Infect Control Hosp Epidemiol. 2017;38(6):639-50.
- Nasiri MJ, Goudarzi M, Hajikhani B, Ghazi M, Goudarzi H, Pouriran R. Clostridioides [Clostridium] difficile infection in hospitalized patients with antibiotic-associated diarrhea: A systematic review and meta-analysis. 2018;50:32-7.
- Teng C, Reveles KR, Obodozie-Ofoegbu OO, Frei CR. Clostridium difficile Infection Risk with Important Antibiotic Classes: An Analysis of the FDA Adverse Event Reporting System. Int J Med Sci. 2019;16(5):630-5.
- Büchler AC, Wicki M, Frei R, Hinic V, Seth-Smith HMB, Egli A, et al. Matching Clostridioides difficile strains obtained from shoe soles of healthcare workers epidemiologically linked to patients and confirmed by whole-genome sequencing. J Hosp Infect. 2022;126:10-15.
- Landelle C, Verachten M, Legrand P, Girou E, Barbut F, Brun-Buisson C. Contamination of healthcare workers’ hands with Clostridium difficile spores after caring for patients with C. difficile infection. Infect Control Hosp Epidemiol. 2014;35(1):10-5.
- Tschudin-Sutter S, Kuijper EJ, Durovic A, Vehreschild MJGT, Barbut F, Eckert C, et al. Guidance document for prevention of Clostridium difficile infection in acute healthcare settings. Clin Microbiol Infect. 2018;24(10):1051-4.
- McDonald LC, Gerding DN, Johnson S, Bakken JS, Carroll KC, Coffin SE, et al. Clinical Practice Guidelines for Clostridium difficile Infection in Adults and Children: 2017 Update by the Infectious Diseases Society of America [IDSA] and Society for Healthcare Epidemiology of America [SHEA]. Clin Infect Dis. 2018;66(7):e1-e48.
- Schoyer E, Hall K. Environmental Cleaning and Decontamination to Prevent Clostridioides difficile Infection in Health Care Settings: A Systematic Review. J Patient Saf. 2020;16(3S Suppl 1):S12-S15.
- Ramai D, Noorani A, Ofosu A, Ofori E, Reddy M, Gasperino J. Practice measures for controlling and preventing hospital associated Clostridium difficile infections. Hosp Pract (1995). 2019;47(3):123-9.
- Musuuza JS, Hundt AS, Carayon P, Christensen K, Ngam C, Haun N, et al. Implementation of a Clostridioides difficile prevention bundle: Understanding common, unique, and conflicting work system barriers and facilitators for sub-process design. Infect Control Hosp Epidemiol. 2019;40(8):880-8.
- Balsells E, Filipescu T, Kyaw MH, Wiuff C, Campbell H, Nair H. Infection prevention and control of Clostridium difficile: A global review of guidelines, strategies, and recommendations. J Glob Health. 2016;6(2):020410.
- Fayerberg E, Bouchard J, Kellie SM. Knowledge, attitudes and practice regarding Clostridium difficile: A survey of physicians in an academic medical center. Am J Infect Control. 2013;41(3):266-9.
- Kelly BJ, Tebas P. Clinical Practice and Infrastructure Review of Fecal Microbiota Transplantation for Clostridium difficile Infection. Chest. 2018;153(1):266-77.
- Rao K, Safdar N. Fecal microbiota transplantation for the treatment of Clostridium difficile infection. J Hosp Med. 2016;11(1):56-61.
- Guillemin I, Marrel A, Beriot-Mathiot A, et al. How do Clostridium difficile infections affect nurses’ everyday hospital work: a qualitative study. Int J Nurs Pract. 2015; 21(suppl 2):38-45.
- Knežević D, Petković M. Faecal transplantation and Clostridioides difficile infection. Scr Med. 2021;52(3):215-23.
- Liubakka A, Vaughn BP. Clostridium difficile Infection and Fecal Microbiota Transplant. AACN Adv Crit Care. 2016;27(3):324-37.
- Hammond DA, Hughes CA, Painter JT, Pennick RE, Chatterjee K, Boye B, Meena N. Impact of Targeted Educational Interventions on Clostridium difficile Infection Treatment in Critically Ill Adults. Hosp Pharm. 2016 Dec;51(11):901-6.
- Kakkar SK, Bala M, Arora V. Educating nursing staff regarding infection control practices and assessing its impact on the incidence of hospital-acquired infections. J Educ Health Promot. 2021 Jan 28;10:40.
- Koo E, McNamara S, Lansing B, Olmsted RN, Rye RA, Fitzgerald T, et al. Making infection prevention education interactive can enhance knowledge and improve outcomes: Results from the Targeted Infection Prevention [TIP] Study. Am J Infect Control. 2016;44(11):1241-6.
- Mody L, Krein SL, Saint S, Min LC, Montoya A, Lansing B, et al. A targeted infection prevention intervention in nursing home residents with indwelling devices: a randomized clinical trial. JAMA Intern Med. 2015;175(5):714-23.
- Barker AK, Ngam C, Musuuza JS, Vaughn VM, Safdar N. Reducing Clostridium difficile in the Inpatient Setting: A Systematic Review of the Adherence to and Effectiveness of C. difficile Prevention Bundles. Infect Control Hosp Epidemiol. 2017;38(6):639-50.
- Kato H, Hagihara M, Asai N, Shibata Y, Yamagishi Y, Iwamoto T, et al. A systematic review and meta-analysis of decontamination methods to prevent hospital environmental contamination and transmission of Clostridioides difficile. 2022;73:102478.
- Spagnolo AM, Sartini M, Battistella A, Casini B, Lo Pinto G, Schinca E, et al. A Clostridium difficile outbreak in an Italian hospital: The efficacy of the multi-disciplinary and multifaceted approach. J Prev Med Hyg. 2018;59(2):E132-E138.
- European Surveillance of Clostridioides [Clostridium] difficile infections. Surveillance protocol version 2.4. European Centre for Disease Prevention and Control. Stockholm: ECDC; 2019. Available at: ecdc.europa.eu/sites//files/documents/clostridium-difficile-infections-EU-surveillance-protocol-vers2.4.pdf. Last accessed: 2 Mart 2022.
- Vonberg RP, Kuijper EJ, Wilcox MH, Barbut F, Tüll P, Gastmeier P, et al. Infection control measures to limit the spread of Clostridium difficile. Clin Microbiol Infect. 2008;14 Suppl 5:2-20.
- Tsioutis C, Birgand G, Bathoorn E, Deptula A, ten Horn L, Castro-Sánchez E, et al. Education and training programmes for infection prevention and control professionals: mapping the current opportunities and local needs in European countries. Antimicrob Resist Infect Control. 2020;9(1):183.
- Abalkhail A, Alslamah T. Institutional Factors Associated with Infection Prevention and Control Practices Globally during the Infectious Pandemics in Resource-Limited Settings. Vaccines (Basel). 2022;10(11):1811.
- Yoshikawa A, Tashiro N, Ohtsuka H, et al. Protocol for educational programs on infection prevention/control for medical and healthcare student: A systematic review and meta-analysis. PLoS One. 2022;17(10):e0276851.
- Asfaw N. Knowledge and practice of nurses towards prevention of hospital acquired infections and its associated factors. International Journal of Africa Nursing Sciences. 2021;16:100333.
- Gaikwad U N, Basak S, Kulkarni P, Sande S, Cahavan S, et al. Educational Intervention to Foster Best Infection Control Practices Among Nursing Staff. Int J Infect. 2018;5(3):e81531.
- Knowles MS, Holton EF, Swanson RA, Robinson PA. The adult learner: The definitive classic in adult education and human resource development. 9nd ed. Oxfordshire: Routledge. 2020.
- Cole M. Problem-based learning — a case for infection control. British Journal of Infection Control. 2005;6(6):16-9.
- Choi Y-R, Lee Y-N, Kim D, Park WH, Kwon DY, Chang SO. An e-Problem-Based Learning Program for Infection Control in Nursing Homes: A Quasi-Experimental Study. International Journal of Environmental Research and Public Health. 2022;19(20):13371.
- Kakkar SK, Bala M, Arora V. Educating nursing staff regarding infection control practices and assessing its impact on the incidence of hospital-acquired infections. J Educ Health Promot. 2021;10:40.
- Finnimore K, Smyth W, Carrucan J, Nagle C. Nurses’ knowledge, practices and perceptions regarding Clostridioides difficile: Survey results. Infect Dis Health. 2023 Feb;28(1):39-46.
- Miljković I, Topuz A. The knowledge of nurses about prevention of infections caused by the bacteria Clostridium difficile. Biomedicinska Istraživanja. 2021;12(1),61–8.
- Brady RR, Rodrigues MA, Harrison R, Rae C, Graham C, Poxton IR, et al. Knowledge of Clostridium difficile infection among UK health-care workers: development of a knowledge assessment tool. Scott Med J. 2012;57(3):124-30.
- Krutova M, Kinross P, Barbut F, et al. How to: Surveillance of Clostridium difficile infections. Clin Microbiol Infect. 2018;24(5):469-75.
- Keske LA, Letizia M. Clostridium difficile infection: essential information for nurses. Medsurg Nurs. 2010;19(6):329-33.
- Domeniconi G, Serafino S, Migone De Amicis M, Formica S, Lanzoni M, Maraschini A, et al. Clostridium difficile infection epidemiology and management: Comparison of results of a prospective study with a retrospective one in a reference teaching and research hospital in Northern Italy. Am J Infect Control. 2016;44(11):1214-18.
- Kim E, Kim SS, Kim S. Effects of infection control education for nursing students using standardized patients vs. Peer role-play. Int J Environ Res Public Health. 2021;18(1):107.
- Korashy Osman F, Mohamed El Banna H, Youssef Sharaf A, Fathy Mohammed Y. The Effects of Educational Interventions on Nurses’ Knowledge and Practices in Hemodialysis Unit Regarding Infection Control Practices. Egypt J Hosp Med. 2021;84(1):1739-48.
- Gomarverdi S, Khatiban M, Bikmoradi A, Soltanian AR. Effects of a multi-component educational intervention on nurses’ knowledge and adherence to standard precautions in intensive care units. J Infect Prev. 2019;20(2):83-90.
- Kiersnowska ZM, Lemiech-Mirowska E, Semczuk K, Michałkiewicz M, Sierocka A, Marczak M. Level of Knowledge of Medical Staff on the Basis of the Survey in Terms of Risk Management, Associated with Clostridioides difficile Infections. Int J Environ Res Public Health. 2021;18(13):7060.
- Burnett E, Corlett J. Understanding risk perceptions and responses of the public and health care professionals toward Clostridium difficile: A qualitative interpretive description study. Am J Infect Control. 2017;45(2):133-8.
- Legenza L, Barnett S, Rose W, Safdar N, Emmerling T, Peh KH, et al. Clostridium difficile infection perceptions and practices: A multicenter qualitative study in South Africa. Antimicrob Resist Infect Control. 2018;7:125.
- Klatte JM, Myers AL, Livingston RA, Jackson MA. Pediatric physicians’ knowledge, attitudes, and beliefs regarding Clostridium difficile-associated disease prevention, testing, and treatment. Am J Infect Control. 2012;40(6):577.
- Aldeyab MA, Devine MJ, Flanagan P, Mannion M, Craig A, Scott MG, et al. Multihospital Outbreak of Clostridium difficile Ribotype 027 Infection: Epidemiology and Analysis of Control Measures. Infect Control Hosp Epidemiol. 2011;32(3):210-9.
- Wong-McClure RA, Ramírez-Salas E, Mora-Brenes N, Aguero-Sandí L, Morera-Sigler M, Badilla-Vargas X, et al. Long term effect of infection control practices and associated factors during a major Clostridium difficile outbreak in Costa Rica. J Infect Dev Ctries. 2013;7(12):914-21.
- Baur D, Gladstone BP, Burkert F, Carrara E, Foschi F, Döbele S, et al. Effect of antibiotic stewardship on the incidence of infection and colonisation with antibiotic-resistant bacteria and Clostridium difficile infection: a systematic review and meta-analysis. Lancet Infect Dis. 2017;17(9):990-1001.
- Jarodiya V, Singh T, Khan ZH. Decreasing Hospital Clostridium difficile Infections: Impact of an Educational Module. Am J Gastroenterol. 2019;114:S117.
- Pate K, Reece J, Smyre A. A Multifaceted Approach to the Prevention of Clostridioides [Clostridium] Difficile. Clin Nurse Spec. 2019;33(2):75-81.
- Fabre V, Markou T, Sick-Samuels A, Rock C, Avdic E, Shulder S, et al. Impact of Case-Specific Education and Face-to-Face Feedback to Prescribers and Nurses in the Management of Hospitalized Patients with a Positive Clostridium difficile Test. Open Forum Infect Dis. 2018;5(10):ofy226.
- Kiersnowska ZM, Lemiech-Mirowska E, Michałkiewicz M, Marczak M. Hand hygiene as the basic method of reducing Clostridium difficile infections (CDI) in a hospital environment. Ann Agric Environ Med. 2021;28(4):535-40.
![]() This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
Single-centre descriptive study of adverse events reported after anti-COVID vaccination
Fabio Giancane1, Angelo Cianciulli1, Silvia De Chiara2, Alessandra Iannelli2,
Marika Finizio4, Rosetta Frammartino1, Andrea Lombardi1,
Domenico Ciro Cristiano1, Francesco Gravante3, Francesco Petrosino1*
1.Nurse, AOU ‘San Giovanni di Dio e Ruggi d’Aragona’, Salerno
2.Pharmacist, AOU ‘San Giovanni di Dio e Ruggi d’Aragona’, Salerno
3.Nurse, Local Health Unit of Aversa, Caserta
4.Nursing graduate, University of Salerno
*Corresponding author: Francesco Petrosino, AOU ‘San Giovanni di Dio e Ruggi d’Aragona’, Salerno. Email: f.petrosino75@gmail.com
Cite this article
ABSTRACT
Introduction: In Italy, approximately 80.5% of the population has completed the primary anti-COVID vaccination cycle with approximately 141 million doses administered. With the introduction of new measures to counter the spread of COVID-19, including compulsory vaccination for certain categories of people, the population expressed fears about the safety and adverse effects of SARS-CoV-2 vaccines. Several factors, such as gender and age, could have influenced the outcomes associated with the vaccine. Our single-centre work seeks to provide such evidence with respect to Pfizer/BioNTech’s BNT162b2 (Comirnaty) and AstraZeneca’s AZD1222 (Vaxzevria) vaccines.
Materials and Methods: Single-centre descriptive study carried out on a sample of subjects who underwent anti-COVID vaccination at the ‘San Giovanni di Dio e Ruggi d’Aragona’ AOU vaccination centre in Salerno. Patients who reported a suspected adverse reaction after receiving a dose of vaccine were included in the study. The regional vaccine platform SORESA and the VigiFarmaco portal were used to collect the data.
Results: During the period covered by the study, 126,928 doses of SARS-CoV-2 vaccine were administered. The Pfizer-BioNTech vaccine group comprised 124,138 administrations. The AstraZeneca vaccine group consisted of 2,790 administrations. 287 post-vaccination adverse reaction reports entered in the National Pharmacovigilance Network were considered. In most of the reactions reported, for both vaccines considered, the symptomatology was attributable to local reactions at the injection site. At the systemic level, however, we noted the prevalence of non-specific events such as fever, headache and diffuse arthromyalgia.
Conclusions: Based on our results and comparison with the literature, the data collected on the vaccines considered in the study suggest a favourable safety profile for their large-scale use. The rate of minor adverse events turned out to be low, with similarly reassuring data compared to serious adverse events, such as not to justify hesitation towards vaccination for COVID-19 disease control.
Keywords: SARS-CoV-2; Surveillance system; COVID-19 vaccination; mRNA; Viral vector; Adverse events following immunisation
INTRODUCTION
Pathogenic viral outbreaks and complex interactions with humans and animals have, over the centuries, caused the transmission of viruses between different species (jumping), posing a great threat to human health and safety[1-3]. Globalisation has increasingly favoured pathogenic transmission between continents, causing different pandemics, in particular viral pandemics[4]. A new public health crisis that threatened the world in 2019 was the spread of the new coronavirus (2019-nCoV) or severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) declared a pandemic by the World Health Organisation (WHO) in March 2020[5]. The rapid spread of the COVID-19 disease has focused researchers’ attention on the repurposing of existing approved drugs that inhibit viral entry, endocytosis, genome assembly, transmission and replication[6]. Most of the available information has been obtained through studies on other members of this family (SARS and MERS)[7]. Many researchers are currently working on the development of various types of specific drugs to treat this disease worldwide[8, 9]. Therefore, the current treatment given to COVID-19 patients is only based on their symptoms[10, 11]. Exposure to a pathogen such as SARS-CoV-2 generates an antibody response that changes over time and in different individuals (antibody kinetics)[12, 13]. It is believed that the limited pre-existing natural immunity to this virus was responsible for the explosive increase in cases[14, 15]. A previous infection, on the other hand, could play a key role in ensuring protection against new infections, and the literature can provide evidence of such protective correlations through longitudinal cohort studies[16-19]. In the absence of specific drugs, only global vaccination has made it possible to contain the spread of the virus, reducing the number of serious clinical cases and hospitalisations[20-22]. In December 2020, the first vaccines against COVID-19 developed with different technologies received Emergency Use Authorisation (EUA) from the US Food and Drug Administration (FDA). Subsequently, globally, they were licensed in 117 countries in North and South America, the United Kingdom, Europe, Africa, Asia and Oceania[23, 24].
In Italy, mRNA vaccines and the adenovirus vaccine AZD1222 have been widely administered. Time saving during the development of COVID-19 vaccines was achieved through unprecedented levels of public financial support, increased tolerance for risky investments in technology and process, and studies on mRNA transport methodology[25-27]. The Italian Medicines Agency defines pharmacovigilance and vaccine vigilance as “a complex set of activities aimed at continuously assessing all information relating to the safety of medicinal products and ensuring that the benefit/risk (B/R) ratio remains favourable over time.” Our country has a pharmacovigilance system that, for many years now, has devoted special attention and a special organisational structure precisely to monitoring what happens after a vaccine is administered. It is an open, dynamic system to which everyone (health professionals, patients, parents, citizens) can send their reports contributing to the monitoring of the safe use of vaccines and medicines in general. Furthermore, the system has full transparency and offers access to aggregated data, which can be queried on the AIFA website. The National Pharmacovigilance Network (NFP) suddenly came into the spotlight when several new vaccines received emergency authorisation and were launched on a large scale at the end of 2020. Vaccines have undergone rigorous clinical testing and evaluation by the authorities, but with the use of new technologies [28] and rapid, large-scale administration of vaccines, the importance of a well-functioning international system of post-marketing safety surveillance has been emphasised[29, 30]. The surveillance of vaccine safety and the collection of reports on suspected adverse events after immunisation (AEFI) [31] is the responsibility of national vaccine regulatory systems, including national regulatory authorities (NRAs) and national immunisation programmes (NIPs). Passive surveillance, defined as the collection and analysis of unsolicited reports of suspected adverse events in the form of individual case safety reports (ICSRs) that are sent to a central database or a health authority, is the basis of safety surveillance for immunisation programmes, in order to identify rare events, evaluate clusters of reports and detect safety signals for further and subsequent studies [32, 33]. Although the identification and quantification of adverse events related to anti-COVID vaccination is not always easy to understand, especially in such a broad context as a pandemic, the analysis of the available data can be an important moment for risk estimation and subsequent safety assessments[34-36].
This paper describes reports of reactions that were observed after administration of the COVID vaccine. Investigating the meaning and causes of these reactions is the task of pharmacovigilance. Investigating every event that appears after a vaccination serves to gather as much information as possible and increase the possibility of identifying truly suspicious events whose nature is important to understand, or which have never been observed before, with the aim of ascertaining whether there is a causal link with the vaccination. In this way, regulatory authorities such as AIFA can verify the safety of vaccines in the real world, confirming what has been observed in pre-authorisation studies and possibly identifying new potential adverse reactions, especially if they are rare (1 in 10,000) and very rare (less than 1 in 10,000). A large number of reports, therefore, does not imply that the vaccine is more dangerous, but is an indication of the high capacity of the pharmacovigilance system to monitor safety.
The anti-Sars-CoV-2 vaccination campaign, which started on 27 December 2020, saw the participation of the ‘San Giovanni di Dio e Ruggi d’Aragona’ AOU of Salerno in ‘Vaccine Day’, the symbolic start date of the vaccination campaign in Italy and across Europe. In what was analysed by this work, in order to make this event – historic for all healthcare worldwide – possible, an organisational and coordination process was implemented that ensured high daily vaccination numbers and minimal risks for users, in full compliance with the quality standards of Public Health.
Several factors, such as gender and age, may have influenced the clinical outcomes associated with the vaccine[37]. To date, in Italy, about 80.5% (48 million subjects) of the population have completed the COVID-19 primary vaccination cycle with about 141 million doses administered. This followed the introduction of new measures to combat the spread of COVID-19, including the compulsory vaccination of certain categories of persons[38].
MATERIAL AND METHODS
Study design
In this paper, we will provide a surveillance report on vaccines administered at the ‘San Giovanni di Dio e Ruggi d’Aragona’ University Hospital (AOU ‘Ruggi’) in Salerno with respect to specific targets:
1.to conduct a descriptive observational study of subjects undergoing vaccination with Pfizer/BioNTech’s BNT162b2 (Comirnaty) and AstraZeneca’s AZD1222 (Vaxzevria) between 27 December 2020 and 30 November 2021
2.to conduct a descriptive analysis of all reports of suspected adverse drug reactions attributed to COVID-19 vaccination (Adverse Events and Severe Adverse Events Following Immunisation, AEFI and sAEFI), collected through the AIFA form and/or the VigiFarmaco system of the Italian Drug Agency (severity, concomitant use of drugs, outcome)
3.to assess the role and statistical association between reported reactions and previously identified variables (age, gender, dose).
Participants
The descriptive observational study was carried out on a sample of subjects who received the vaccine at the ‘San Giovanni di Dio e Ruggi d’Aragona’ AOU vaccination centre in Salerno in the period between 27 December 2020 and 30 November 2021. Patients who reported a suspected adverse reaction after receiving a dose of vaccine were included in the study.
Sample Size
The sample size was evaluated using the GPower software version 3.1.9.7[39]. Power analysis was conducted for a two-tailed t-test, with an effect size = 0.50, a probability of type I error = 0.05, a test power = 0.95 and a sample size ratio of 1:1. The sample size for group 1 is 105 and for group 2 it is 105 for a total of 210 items. For the goodness-of-fit χ2 test, with an effect size = 0.3, a probability of the type 1 error = 0.05, a power of the test = 0.95 and GdL = 1, the sample size for the group is 143 (172 with 2 degrees of tolerance).
Data collection
For the vaccination population, data were obtained from the SINFONIA platform (Sistema Informativo Sanità Campania) and the VigiFarmaco portal for adverse event reporting. They were collected anonymously, formatted, narrowed down to the vaccines of interest for this study and entered into a database using Microsoft Corporation Excel software.
Data analysis
The collected data were processed with SPSS ® (Statistical Package for Social Science – Chicago, IL, USA) statistical software for Windows, version 26.0. A descriptive analysis of the general characteristics of the study population was performed, using absolute frequencies and percentages. Data were stratified by age group, gender and period of administration. For continuous variables, results were expressed as mean ± standard deviation (SD), and as median and Interquartile range (RIQ) for numeric variables. Paired and unpaired data were analysed using Student’s t-test. The Kolmogorov-Smirnov test, which is more appropriate when the sample size is >50, was used to check normality. The Q-Q diagram and the values of skewness and kurtosis were also evaluated. The categorical variables were summarised using frequencies and percentages, and we used the chi-square (χ2) test to compare the categorical variables between the groups.
The Phi coefficient was used to measure the strength of association between the dichotomous variables, while Pearson’s linear correlation coefficient was used to assess the degree of relationship between the variables age and severity.
All tests with p-value (p) < 0.05 were considered statistically significant.
Ethical consideration
Due to the nature of this study, no formal approval to the relevant Ethics Committee was required. The study was conducted in accordance with the principles of the Declaration of Helsinki. The data were extracted from databases for which the processing information had been signed in advance and analysed for the time strictly necessary to achieve the purposes for which they were collected, in compliance with the Regulation (EU) 2016/679 (GDPR) on privacy and guarantee of anonymity. Authorisation for their use was provided by the Corporate Privacy Officer and the legal representative of the organisation.
RESULTS
During the period covered by the study, 126,928 doses of SARS-CoV-2 vaccine were administered. Those who had already received the first dose went to the centre for the administration of the second dose of vaccine. Some of them also received the third dose.
In Table 1, the general trend of the Vaccination Centre is shown, while in Table 2, the trend per macro area (Vaccination Type and Dose) is shown.

Table 1. General performance of the Vaccination Centre

Table 2. Performance by macro area of the Vaccination Centre, with order of priority of categories
A proportion of the vaccinated subjects (404) switched from AstraZeneca to Pfizer-BioNTech due to changes in the Italian Regulatory Authority’s declarations [40] or because they had suffered increased D-dimer levels [41]after the first AZD dose.
The Pfizer-BioNTech vaccine group (BNT) comprised 124,138 administrations (47.8% men and 52.2% women) with a mean age of 49.11±20.94 years (range: 12-101) and a median age of 51 years (RIQ: 31-64).
The distribution is superimposable between first dose (50.6%) and second dose (47.2%). Only 2.2% of the subjects received the third dose.
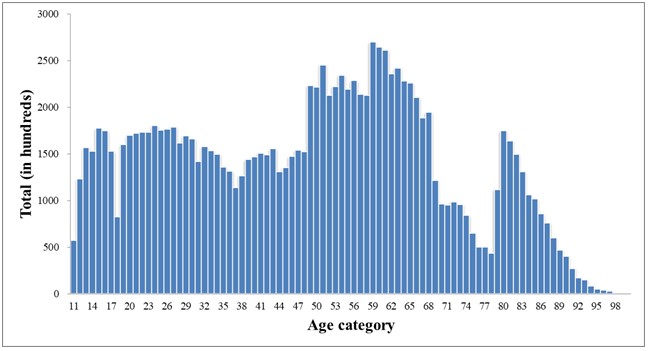
Figure 1. Age distribution BNT Group
The AstraZeneca vaccine group (AZD) consisted of 2,790 administrations (57.7% men and 42.3% women), with a mean age of 47.46±11.77 (range: 18-76 years) and a median age of 49 years (RIQ: 38-57). 58.7% of the sample received the first dose and 41.3% the second dose.

Figure 2. Age distribution AZD Group
The enrolled population was stratified by age decades. The Pfizer-BioNTech group consisted predominantly (18.9%) of individuals aged between 60 and 69 years (Figure 3), whereas the AstraZeneca group comprised more people (23.1%) aged between 40 and 49 years (Figure 4). In particular, several subjects were unable to receive AstraZeneca mainly due to thrombotic risk (e.g. high D-dimer value, coagulation impairment, etc.) and age limitation (initially subjects over 18 years of age were eligible and later over 60 years of age), according to the recommendations in force in Italy. Our study therefore examined the AEFIs and sAEFIs attributed to the SARS-CoV-2 vaccination and recorded by the nursing staff or pharmacists responsible for vaccine preparation and pharmacovigilance at the AOU ‘San Giovanni di Dio e Ruggi d’Aragona’ Vaccine Centre.
At the time of its closure on 30 November 2021, we verified that 287 post-vaccination adverse reaction reports had been entered into the National Pharmacovigilance Network. The data show that the percentage of reported sAEFIs are significantly lower than the risks related to COVID-19 (data from the COVID-19 Integrated Surveillance in Italy).
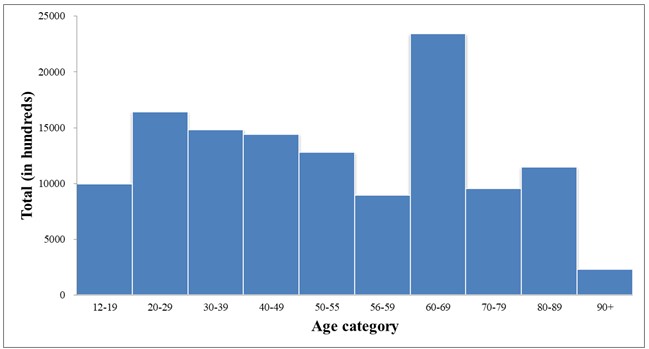
Figure 3. Distribution by age group BNT Group

Figure 4. Age distribution AZD Group
Most of the reported adverse events were classified as non-serious (90.9%) and to a lesser extent as serious (9.1%); in most cases, the outcome was complete resolution or improvement of symptoms. The distribution of reports per type of vaccine follows the distribution of administrations (92% for Pfizer-BioNTech and 8% for AstraZeneca).
The average age of persons reporting a suspected adverse event was 62±22.21 years (range: 15-99). As already observed in the National Surveillance Reports on anti-COVID-19 vaccines, also in what was analysed by this work, the reporting rates for the 2nd dose are lower than for the 1st dose and significantly lower for the 3rd dose. Although these are not absolute incidence rates, the data indicate an overall absence of significant sAEFI events such as to be an alert for regulators to serious safety issues with administered vaccines. On the other hand, in contrast to the overlapping exposure between the genders (52% of doses administered in females and 48% in males), one can note the asymmetric distribution of reports with respect to gender, with 71.1% of reports concerning women and 27.9% concerning men, regardless of the vaccine and the dose administered.
In our statistical analysis, in order to determine whether there were age differences between those who reported a post-vaccination adverse reaction, we performed an independent samples t-test.
To test for normality, we used the Kolmogorov-Smirnov test with Lilliefors correction, which was non-significant for both men (p = 0.071) and women (p = 0.058). Visual inspection of the Q-Q plot shows that age is normally distributed, with a skewness of -0.445 (ES = 0.271, | z | = 1.64) and kurtosis of -0.634 (ES = 0.535) for men and a skewness of 0.006 (ES = 0.171, | z | = 0.035) and kurtosis -0.902 (ES = 0.341) for women[42-43]. Having ascertained the normality of the sample distribution, we evaluated the hypothesis of equality of variance by means of Levene’s test. This turns out to be statistically non-significant (F = 0.255, p = 0.614) and it is therefore possible to use the assumption of homogeneous variance of the age of males and females.
The results suggest that the difference in mean age between the two groups is not significantly different (t(279) = 1.769, p = 0.078). We then looked at whether the 287 subjects in our sample were as likely as the Italian population to have non-serious (81.8%) or serious (18.1%) reactions[44].
We conducted a χ2 test for goodness of fit against the theoretical distribution model. In this case, the results obtained suggest that the two categories do not distribute themselves according to the expected probability (χ2(1) = 15.88, p < 0.001). In particular, in our reference sample, non-serious reactions are more frequent (90.9%) than serious reactions (9.1%). We then conducted a χ2 test to test whether men and women were equally likely to have non-serious or serious reactions. The test results suggest that men and women were equally distributed within the two categories of the severity status variable (χ2(1) = 2.83, Phi = -0.100, p = 0.093). In other words, there is no evidence of linear dependence between gender and the occurrence of a serious adverse reaction, with a small linkage effect between the two variables, as suggested by the value close to 0 for the Phi coefficient. We also conducted a χ2 test to test whether there was a relationship between the number of doses received and the occurrence of a severe reaction. These results also suggest that the groups are equally distributed within the two categories of the severity status variable (χ2(2)= 0.418, p = 0.811, V = 0.038). In other words, dose and severity of the reaction are independent in distribution. Finally, Pearson’s linear correlation coefficient was calculated to investigate the correlation between the variables age and severity considering the reported adverse reaction (r = -0.279, p = 0.01).
The results suggest that as age decreases, there is a weak correlation with the presentation of a severe reaction. In this analysis, the source variable (severity) was coded into a nominal dichotomous qualitative variable with value 0 (no severe reaction) and 1 (severe reaction).
Below are some of the reactions detected and their incidence in relation to the total number of detections (Figure 5).
Figure 6 shows some detected reactions and their incidence for the Pfizer-BioNTech vaccine and Figure 7 for AstraZeneca.

Figure 5. All types of adverse events observed on our sample.

Figure 6. All types of adverse events observed by Comirnaty vaccine.

Figure 7. All types of adverse events observed by Vaxzevria vaccine.
Finally, Figure 8 shows the reports of sAEFI aggregated by symptomatology. It can be noted that,

Figure 8. All types of severe adverse events observed.
Figure 8 shows the reports of severe AEFIs aggregated by symptomatology. It can be seen that, in addition to overlapping with the AEFIs in terms of typology, they are characterised by events attributable to general pathologies. For all reported sAEFIs, the outcome was improvement of symptoms.
DISCUSSIONS
Our study examined AEFIs and sAEFIs spontaneously reported at the AOU ‘San Giovanni di Dio e Ruggi d’Aragona’ in Salerno through the AIFA pharmacovigilance system and attributed to anti-COVID vaccination. Our data, although related to a small sample, demonstrate the few reports of serious reactions and the low risk of outcomes when compared to historical pandemic data and in line with national data. In contrast to an overlapping exposure between the sexes with respect to total administrations, AEFIs were predominantly reported in the female sex (71%). The percentage of sAEFI is almost overlapping between the sexes, with a prevalence for Pfizer-BioNTech’s Comirnaty vaccine (78%) at the first dose (77%). In most of the AEFIs reported, for both vaccines considered, the symptomatology was attributable to local reactions at the injection site (e.g. pain, swelling, redness). At the systemic level, however, we noted the prevalence of non-specific events such as fever, headache and diffuse arthromyalgia. The same applies to reactions reported as serious; the latter, identified as such due to the prolonged observation period at the vaccination centre, in rare cases led to the hospitalisation of those involved. All these reports resulted in an improvement in symptoms. In line with the literature, our study showed that the onset of AEFI can be influenced by gender. This could be related to the opposite role of sex hormones [42] as well as pharmacokinetic parameters that may differ between males and females [43].
Disease control efforts by health authorities should seriously consider the relationship between the risks involved in immunising the population versus the benefits against the disease[45]. While there is no general acceptable risk threshold, the number of deaths worldwide from COVID-19, the risk of collapse of health systems, shutdowns and damage to economies, should lead epidemiologists, health organisations and governments to set this threshold as soon as possible.
CONCLUSIONS
Based on our results and the comparison with the literature[46, 47], both vaccines showed a favourable safety profile, with reassuring data that does not justify hesitation towards vaccination for COVID-19 disease control[48-50]. We therefore highlighted the few differences in the incidence and type of AEFI and sAEFI associated with Pfizer/BioNTech’s Comirnaty (BNT162b2) and AstraZeneca’s Vaxzevria (AZD1222). For these reasons, the guidelines issued by many countries, such as Italy, whose main objective is to increase the number of vaccinated persons with a ‘fourth dose’ to protect the over 60s and the frailest of the population. It is therefore necessary to disseminate surveillance and public health data to counter vaccination hesitancy in the general population and the reluctance of “no vax” subjects towards vaccinations, also in view of possible future pandemic events.
LIMITS
The study has some limitations. Pharmacovigilance information is based on a voluntary and passive reporting system that may not capture every single event related to AEFI and sAEFI. Direct verification is not always possible to determine whether every reported adverse reaction is actually related to the vaccine. In particular, the lack of reporting could lead to an underestimation of all the adverse events that actually occurred.
Another limitation of the study is that, to the exclusion of age and gender, other individual characteristics were not taken into account, such as underlying or previous diseases (myocarditis, autoimmune or immune-mediated diseases, oncological pathologies) or chronically taken medications, which might instead predispose vaccinated subjects to be susceptible to AEFIs and sAEFIs.
ACKNOWLEDGEMENTS
We thank Prof Francesco De Caro (UOC Risk Assessment Management and Reporting) and Dr Maria Grazia Lombardi (UOC Pharmacy), AOU ‘San Giovanni di Dio e Ruggi d’Aragona’, Salerno.
FUNDING
This research did not receive any external funding or support.
CONFLICTS OF INTEREST
The authors declare that they have no conflicts of interest associated with the study.
AUTHORS’ CONTRIBUTION
FG and AC were responsible for the conception and design of the study; SDC and AI performed the data collection; FG and FP performed the data analysis; MF and RF were responsible for drafting the manuscript; AL and DCC made critical revisions to the article.
REFERENCES
- Sharma A, Tiwari S, Deb MK, Marty JL. Severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2): a global pandemic and treatment strategies. Int J Antimicrob Agents. 2020;56(2):106054.
- Reperant LA, Osterhaus ADME. AIDS, Avian flu, SARS, MERS, Ebola, Zika… what next?. Vaccine. 2017;35(35 Pt A):4470-4474.
- Reperant LA, Cornaglia G, Osterhaus AD. The importance of understanding the human-animal interface: from early hominins to global citizens. Curr Top Microbiol Immunol. 2013; 365:49-81.
- Liu J, Dai S, Wang M, Hu Z, Wang H, Deng F. Virus like particle-based vaccines against emerging infectious disease viruses. Virol Sin. 2016;31(4):279-287.
- Wang C, Horby PW, Hayden FG, Gao GF. A novel coronavirus outbreak of global health concern [published correction appears in Lancet. 2020 Jan 29;:]. Lancet. 2020;395(10223):470-473.
- Muralidar S, Ambi SV, Sekaran S, Krishnan UM. The emergence of COVID-19 as a global pandemic: Understanding the epidemiology, immune response and potential therapeutic targets of SARS-CoV-2. Biochimie. 2020;179:85-100.
- Chan-Yeung M, Xu RH. SARS: epidemiology. Respirology. 2003;8 Suppl(Suppl 1):S9-S14.
- Parums DV. Editorial: Current Status of Oral Antiviral Drug Treatments for SARS-CoV-2 Infection in Non-Hospitalized Patients. Med Sci Monit. 2022;28:e935952.
- Zarandi PK, Zinatizadeh MR, Zinatizadeh M, Yousefi MH, Rezaei N. SARS-CoV-2: From the pathogenesis to potential anti-viral treatments. Biomed Pharmacother. 2021;137:111352.
- Hosoki K, Chakraborty A, Sur S. Molecular mechanisms and epidemiology of COVID-19 from an allergist’s perspective. J Allergy Clin Immunol. 2020;146(2):285-299.
- Huang C, Wang Y, Li X, et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China [published correction appears in Lancet. 2020 Jan 30;:]. Lancet. 2020;395(10223):497-506.
- Huang AT, Garcia-Carreras B, Hitchings MDT, et al. A systematic review of antibody mediated immunity to coronaviruses: kinetics, correlates of protection, and association with severity. Nat Commun. 2020;11(1):4704.
- Grifoni A, Sidney J, Vita R, et al. SARS-CoV-2 human T cell epitopes: Adaptive immune response against COVID-19 [published correction appears in Cell Host Microbe. 2022 Dec 14;30(12):1788]. Cell Host Microbe. 2021;29(7):1076-1092.
- Wallinga J, Teunis P. Different epidemic curves for severe acute respiratory syndrome reveal similar impacts of control measures. Am J Epidemiol. 2004;160(6):509-516.
- Dan JM, Mateus J, Kato Y, et al. Immunological memory to SARS-CoV-2 assessed for up to 8 months after infection. Science. 2021;371(6529):eabf4063.
- Qu G, Li X, Hu L, Jiang G. An Imperative Need for Research on the Role of Environmental Factors in Transmission of Novel Coronavirus (COVID-19). Environ Sci Technol. 2020;54(7):3730-3732.
- Wu Y, Kang L, Guo Z, Liu J, Liu M, Liang W. Incubation Period of COVID-19 Caused by Unique SARS-CoV-2 Strains: A Systematic Review and Meta-analysis [published correction appears in JAMA Netw Open. 2022 Sep 1;5(9):e2235424]. JAMA Netw Open. 2022;5(8):e2228008.
- Zhou F, Yu T, Du R, et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: a retrospective cohort study [published correction appears in Lancet. 2020 Mar 28;395(10229):1038] [published correction appears in Lancet. 2020 Mar 28;395(10229):1038]. Lancet. 2020;395(10229):1054-1062.
- Seow J, Graham C, Merrick B, et al. Longitudinal observation and decline of neutralizing antibody responses in the three months following SARS-CoV-2 infection in humans. Nat Microbiol. 2020;5(12):1598-1607.
- Moreira ED Jr, Kitchin N, Xu X, et al. Safety and Efficacy of a Third Dose of BNT162b2 Covid-19 Vaccine. N Engl J Med. 2022;386(20):1910-1921.
- Tarke A, Coelho CH, Zhang Z, et al. SARS-CoV-2 vaccination induces immunological T cell memory able to cross-recognize variants from Alpha to Omicron. Cell. 2022;185(5):847-859.e11.
- Wajnberg A, Amanat F, Firpo A, et al. Robust neutralizing antibodies to SARS-CoV-2 infection persist for months. Science. 2020;370(6521):1227-1230.
- van Riel D, de Wit E. Next-generation vaccine platforms for COVID-19. Nat Mater. 2020;19(8):810-812.
- Cai C, Peng Y, Shen E, et al. A comprehensive analysis of the efficacy and safety of COVID-19 vaccines. Mol Ther. 2021;29(9):2794-2805.
- Hahn WO, Wiley Z. COVID-19 Vaccines. Infect Dis Clin North Am. 2022;36(2):481-494.
- Nakagami H. Development of COVID-19 vaccines utilizing gene therapy technology. Int Immunol. 2021;33(10):521-527.
- Wallace M, Moulia D, Blain AE, et al. The Advisory Committee on Immunization Practices’ Recommendation for Use of Moderna COVID-19 Vaccine in Adults Aged ≥18 Years and Considerations for Extended Intervals for Administration of Primary Series Doses of mRNA COVID-19 Vaccines – United States, February 2022. MMWR Morb Mortal Wkly Rep. 2022;71(11):416-421.
- Rauch S, Jasny E, Schmidt KE, Petsch B. New Vaccine Technologies to Combat Outbreak Situations. Front Immunol. 2018;9:1963.
- Black S, Eskola J, Siegrist CA, et al. Importance of background rates of disease in assessment of vaccine safety during mass immunisation with pandemic H1N1 influenza vaccines [published correction appears in Lancet. 2010 Jan 30;375(9712):376]. Lancet. 2009;374(9707):2115-2122.
- Klein NP, Lewis N, Goddard K, et al. Surveillance for Adverse Events After COVID-19 mRNA Vaccination. JAMA. 2021;326(14):1390-1399.
- Dudley MZ, Halsey NA, Omer SB, et al. The state of vaccine safety science: systematic reviews of the evidence. Lancet Infect Dis. 2020;20(5):e80-e89.
- Rudolph A, Mitchell J, Barrett J, et al. Global safety monitoring of COVID-19 vaccines: how pharmacovigilance rose to the challenge. Ther Adv Drug Saf. 2022;13:20420986221118972.
- Kochhar S, Salmon DA. Planning for COVID-19 vaccines safety surveillance. Vaccine. 2020;38(40):6194-6198.
- Soiza RL, Scicluna C, Thomson EC. Efficacy and safety of COVID-19 vaccines in older people. Age Ageing. 2021;50(2):279-283.
- Kamidani S, Rostad CA, Anderson EJ. COVID-19 vaccine development: a pediatric perspective. Curr Opin Pediatr. 2021;33(1):144-151.
- Menni C, Klaser K, May A, et al. Vaccine side-effects and SARS-CoV-2 infection after vaccination in users of the COVID Symptom Study app in the UK: a prospective observational study. Lancet Infect Dis. 2021;21(7):939-949.
- COVID-19 vaccine safety: the AIFA annual report.
- Dumyati G, Jump RLP, Gaur S. Mandating COVID-19 Vaccine for Nursing Home Staff: An Ethical Obligation. J Am Med Dir Assoc. 2021;22(10):1967-1968.
- Faul F, Erdfelder E Fau – Lang A-G, Lang Ag Fau – Buchner A, Buchner A. G*Power 3: a flexible statistical power analysis program for the social, behavioral, and biomedical sciences. (1554-351X (Print)).
- https://www.aifa.gov.it/documents/20142/1289678/Comunicato_AIFA_n.627.pdf.
- Sharifian-Dorche M, Bahmanyar M, Sharifian-Dorche A, Mohammadi P, Nomovi M, Mowla A. Vaccine-induced immune thrombotic thrombocytopenia and cerebral venous sinus thrombosis post COVID-19 vaccination; a systematic review. J Neurol Sci. 2021;428:117607.
- Läärä E. Statistics: Reasoning on Uncertainty, and the Insignificance of Testing Null. Annales Zoologici Fennici. 2009;46:138-57.
- Kim HY. Statistical notes for clinical researchers: assessing normal distribution (2) using skewness and kurtosis. Restor Dent Endod. 2013;38(1):52-4.
- Rapporto sulla Sorveglianza dei vaccini anti-COVID.
- Kislaya I, Machado A, Magalhães S, et al. COVID-19 mRNA vaccine effectiveness (second and first booster dose) against hospitalisation and death during Omicron BA.5 circulation: cohort study based on electronic health records, Portugal, May to July 2022. Euro Surveill. 2022;27(37):2200697.
- Tran Kiem C, Andronico A, Bosetti P, et al. Benefits and risks associated with different uses of the COVID-19 vaccine Vaxzevria: a modelling study, France, May to September 2021. Euro Surveill. 2021;26(26):2100533.
- Fiolet T, Kherabi Y, MacDonald CJ, Ghosn J, Peiffer-Smadja N. Comparing COVID-19 vaccines for their characteristics, efficacy and effectiveness against SARS-CoV-2 and variants of concern: a narrative review. Clin Microbiol Infect. 2022;28(2):202-221.
- Troiano G, Nardi A. Vaccine hesitancy in the era of COVID-19. Public Health. 2021;194:245-251.
- Joshi A, Kaur M, Kaur R, Grover A, Nash D, El-Mohandes A. Predictors of COVID-19 Vaccine Acceptance, Intention, and Hesitancy: A Scoping Review. Front Public Health. 2021;9:698111. Published 2021 Aug 13.
- Hudson A, Montelpare WJ. Predictors of Vaccine Hesitancy: Implications for COVID-19 Public Health Messaging. Int J Environ Res Public Health. 2021;18(15):8054. Published 2021 Jul 29.
![]() This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.

ANALYSIS OF PSYCHOSOCIAL STATUS AND QUALITY OF LIFE IN THE ELDERLY WITH OSTEOARTHRITIS DURING THE COVID-19 PANDEMIC: A CROSS SECTIONAL STUDY
Mohd Syukri1*, Dewi Masyitah1, Mashudi1, Lailatul Fadilah2
1. Department of Nursing, Health Polytechnic, Ministry of Health Jambi, Indonesia
2. Department of Nursing, Health Polytechnic, Ministry of Health Banten, Indonesia
* Corresponding author: Mohd Syukri, Jl. Dr. Tazar, Buluran Kenali, Kec. Telanaipura, Kota Jambi, Jambi 36361, Indonesia, Orcid: https://orcid.org/0000-0003-2061-5531
Email: syukrimuh290@gmail.com

Cite this article
ABSTRACT
Introduction: Along with increasing age, there will also be an increasing tendency to get sick and have physical limitations (disabilities) due to a drastic decline in physical abilities. These conditions are the leading cause of high mortality and morbidity in the elderly, especially during the Covid-19 pandemic. The current study aims to analyze the relationship between psychosocial status and the quality of life of the elderly with osteoarthritis during the Covid-19 pandemic.
Materials and Methods: This cross-sectional study was located at a nursing home in Jambi, involving 351 randomly selected participants. Measure the psychosocial status of the elderly using the Indonesian version of the Self Reporting Questionnaire (SRQ) and the quality of life using the Indonesian version of the World Health Organization Quality of Life-Old (WHOQOL – OLD) questionnaire.
Results: Most elderly have a good quality of life, as many as 229 (65.1%), while a poor quality of life, as many as 30 people (8.5%). In the psychosocial variables, most respondents did not experience mental health disorders, as many as 260 people (74.1%). The Mann-Whitney test showed a significant relationship between Quality of Life and Psychosocial Status, in particular we obserbed in subjects without mental disorders in comparison to subjects with mental disorders a better quality of life, i.e. the elderly who do not suffer from mental disorders will show a tendency for a good quality of life.
Conclusions: Psychosocial status related to quality of life in the elderly with osteoarthritis during the Covid-19 pandemic. The elderly who do not suffer from mental disorders will show a tendency for a good quality of life.
Keywords: Elderly; Covid-19; Psychosocial; Quality of life
INTRODUCTION
Qualified elderly are elderly who, through the aging process, remain healthy and optimal physically, socially, and mentally to remain prosperous throughout life and participate in improving the quality of life as members of society [1,2]—osteoarthritis in the elderly results in limitations in carrying out daily activities independently. A study revealed that 2.6% of the elderly experienced total dependence, 1.2% with moderate support, and 96.3% with mild reliance [3]. Dependence, coupled with lifestyle changes, is one of the factors causing stress in the elderly [4,5].
The elderly with osteoarthritis who experience stress tend to experience sadness, and the body becomes weak, with reduced appetite and interest in all things [6,7]. As a result, they will experience delays in treatment, especially in the second year of the Covid-19 pandemic, where there is a statistical increase in cases in various parts of the world, including some areas in Indonesia, where the elderly are a group that is vulnerable to infection. The number of deaths continues to increase, especially in the elderly group [8–10]. If this condition is allowed to drag on, it will trigger depression. In addition, the elderly will find it difficult to motivate themselves to recover. The adaptation process that must undertake to all the changes experienced makes the elderly vulnerable to psychological disorders such as unstable emotional conditions, depression, or anxiety, and it may reduce the quality of life of the elderly [11,12].
Crisis in the elderly can be expressed as a condition of psychosocial disorders with characteristics including dependence on others, isolating themselves, or withdrawing from social activities for various reasons. The reasons include undergoing retirement, severe and prolonged illness, the death of a spouse, and undergoing health protocols during the Covid-19 period, where everyone must keep their distance and isolate themselves [6,13]. For the elderly, changing roles in the family, socio-economic, and social community resulted in setbacks in adapting to the new environment and interacting with the social environment [11,14].
Quality of life is a strategic issue that reflects the condition of the elderly in enjoying the rest of their life and preparing to die peacefully. Therefore, factors affecting the quality of life of the elderly should be accommodated by the elderly, families, and health providers [15,16]. One of the health service providers on the first line is the Public Health Center (PHC). PHC as a health service provider and acting as a center for community health development in its working area should develop health programs based on problems that develop in the community [17,18].
Psychological factors, as assessed by the Geriatric Depression Scale, and sociodemographic characteristics, such as marital status, income and leisure activities, had an impact on quality of life [19]. Other studies show that apart from social demographic factors, social organization and social support affect the quality of life of the elderly [20], and the ability to perform daily routine activities is the strongest predictor [21]. In addition to the aforementioned factors, it is necessary to explore the effects of the psychosocial status of the elderly during the Covid-19 pandemic because the elderly are prone to depression. Preliminary research shows an increase in depression, post-traumatic anxiety, and adjustment disorders in the elderly, and the risk of suicide increases sharply. Stress can also lower the body's immunity, worsening the condition of the elderly who are already physically weak. Patients with a previous psychiatric disorder will tend to experience worsening [3,20].
The elderly group is very vulnerable to contracting Covid-19, plus declining physical health conditions are increasingly impacting the decline in the quality of life of the elderly, increasing mortality rates in the elderly group. For this reason, it is necessary to survey psychosocial health status, response, and quality of life during the Covid-19 pandemic. This study explores the psychosocial problems of the elderly with osteoarthritis during the Covid-19 pandemic.
MATERIALS AND METHODS
Study design
The type of research is analytic observational using the research design is cross sectional study.
Study Population
This study was conducted at the Jambi Nursing Home involving 351 randomly selected participants with the following sample criteria including age 55 years, living in Jambi Nursing Home for at least one year.
Instruments
Psychosocial status was measured using the Indonesian version of the Self-Reporting Questionnaire (SRQ), which consisted of 29 questions about the respondent's condition during the last 30 days [21]. The Indonesian version of the SRQ-20 has 5 dimensions, namely energy, cognitive, depression, physiology, and anxiety. The YES answers to items 1 to 20 (symptoms of neurosis) indicated a psychological problem, and item number 21 meant using a psychoactive substance. One YES answer from items 22 to 24 (psychotic symptoms) indicates a severe problem and needs further treatment. One YES answer to items 25-29 indicates the presence of symptoms of PTSD (Post Traumatic Stress Disorder).
Psychosocial status was categorized into suffering and not suffering from mental disorders. A mental disorder is declared if at least 5 neurotic symptoms are found or there is at least 1 psychotic or PTSD (Post Traumatic Stress Disorder) symptom on the Self-Reporting Questionnaire (SRQ). Meanwhile, it is declared not suffering from mental disorders if there are only 4 items of neurotic symptoms and there are no psychotic symptoms or PTSD (Post Traumatic Stress Disorder) symptom on the Self-Reporting Questionnaire (SRQ). The variable “Psychosocial status” assigning the scores: 1 = suffering and 0 = not suffering for mental disorders.
Measurement of quality of life used the Indonesian version of the World Health Organization Quality of Life-Old (WHOQOL – OLD) questionnaire, which contains the respondents' living conditions in the last four weeks consisting of 26 questions [22]. The variable “Quality of Life”, assigning the scores: 1 = poor, 2= moderate, 3 = good, and 4 = very good for each subject.
The Indonesian version of the World Health Organization Quality of Life-Old (WHOQOL – OLD) questionnaire consists of the Herth Hope Index, Perceived Social Support from Friends (PSS-Fr), Perceived Social Support from Family (PSS-Fa) [22]. The Indonesian version of the WHOQOL-BREFF questionnaire has been tested for validity and reliability by Priastana et al. [22] with a rcount value (0.361) and a Cronbach Alpha value = 0.965, so researchers do not need to test the validity and reliability again.
Sample size
The number of samples involved was 351 participants who were randomly selected from the population. Calculating the number of samples is determined using the Slovin formula [23], where from 2.880 people in the population, d = 0.05, the number of samples is 351.
Ethical Consideration
No economic incentives were offered or provided for participation in this study. The study protocol matched the Declaration of Helsinki ethical guidelines for clinical studies. This research has been approved by the Health Research Ethics Commission of the Health Polytechnic of the Jambi Ministry of Health with the number LB.02.06/2/111/2022.
Statistical analysis
Data are presented as number and percentage for categorical variables, and continuous data expressed as the mean ± standard deviation (SD) or median with Interquartile Range (IQR). The results of data normality analysis using the Kolmogorov Smirnov test showed that the data were not normally distributed. We found the relationship between Quality of Life and Mental disorders using the Mann–Whitney test (ordinal data vs dichotomous).
We considered all tests with P-value< 0.05 as significant. The statistical analysis was performed by SPSS software version 16.0.
RESULTS
The distribution of the characteristics of the research respondents is presented in table 1.

Table 1. Distribution of the Respondents characteristics
Table 1 show that most respondents were 55-64 years, as many as 186 (53%). Most sexes are male, with as many as 225 (64.1%) respondents. Most respondents had a high school education, with 227 (64.7%).
Table 2 shows that most elderly have a good quality of life, as many as 229 (65.1%), while a poor quality of life, as many as 30 people (8.5%).
In the psychosocial variables, most respondents did not experience mental health disorders, as many as 260 people (74.1%).
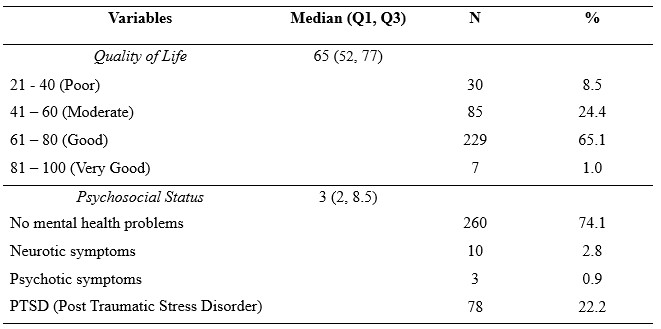
Table 2. Distribution of study variables
Table 3 shows that of the 91 respondents who do have mental disorders, there are 46 respondents with a moderate quality of life category. Of the 260 respondents with not mental disorders, there are 218 respondents have a good quality of life category
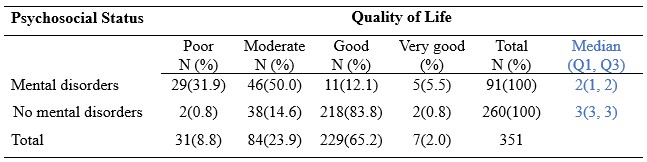
Table 3. Relationship between Psychosocial Status and Quality of Life in the Elderly
The Mann-Whitney test showed a significant relationship between Quality of Life and Psychosocial Status, in particular we obserbed in subjects without mental disorders in comparison to subjects with mental disorders a better quality of life (median: 3 vs 2, p<0.0001), i.e. the elderly who do not suffer from mental disorders will show a tendency for a good quality of life.
DISCUSSION
Elderly stress arises from anxiety about various diseases, including Covid-19. The current study aims to analyze the relationship between psychosocial conditions and the quality of life of the elderly with osteoarthritis during the Covid-19 pandemic.
The results of this study reported that on the psychosocial variables of the elderly, most of the elderly did not experience mental health disorders, as many as 260 people (74.1%) and the elderly and around 25.9% of the elderly experienced mental disorders ranging from PTSD (Post Traumatic Stress Disorder), neurotic and psychotic. Mental disorders experienced by the elderly include the elderly avoiding interacting with other people, decreasing interest in routine activities, always remembering the impact of Covid-19 and feeling disturbed, lack of appetite, not sleeping well, and feeling anxious. Symptoms of this health disorder significantly interfere with the quality of life of the elderly [24].
Anxiety, as a symptom of stress in the elderly in the Covid-19 pandemic situation, should receive support from spouses and family members by being willing to listen to the complaints of the elderly, being able and having time always to be near and accompany the elderly. Elderly family members are also responsible and act as friends of the elderly in dealing with their day-to-day. Likewise, in elderly stress, there is family support to maintain health by supporting the health of the elderly [25].
The increasing number of Covid-19 cases harms everyone's mentality, especially the elderly. SARS-CoV-2 is highly contagious. Even some cases develop into respiratory failure, which will progress to death. Deterioration of the patient's condition is more common in the elderly and those with previous co morbidities (hypertension, diabetes, heart disease) [26,27]. The elderly group (elderly) has physical and psychological weaknesses during the Covid-19 pandemic. About 20% of deaths with Covid-19 in China are over 60 years old [28].
The effects of quarantine are loneliness, sadness, and prolonged stress. Preliminary research suggests an increase in depression, post-traumatic stress, adjustment disorders in the elderly, and the risk of suicide [29]. Stress lowers immunity. This situation can worsen the condition of the elderly, who are already physically weak. Patients with previous psychiatric conditions will tend to experience worsening, one of which is the problem of osteoarthritis [30].
The main problem often experienced by the elderly with osteoarthritis is joint pain. Pain will increase when doing activities, which limits a person's activities. The decrease in physical activity will affect the patient's daily life activities and the quality of his life. A further consequence of osteoarthritis is decreased functional activity, especially difficulty rising to a sitting position, walking, and going up and down stairs [31,32]. The elderly with osteoarthritis will experience joint and muscle dysfunction, so they will experience limited movement, decreased strength, and muscle balance. About 18% experience difficulties and limitations in activities, loss of function of work capacity, and decreased quality of life [33,34].
According to Hong's study [35], the elderly with osteoarthritis have a poorer quality of life than the elderly without osteoarthritis. This condition is associated with decreased physical function due to joint inflammation caused by joint damage. Therefore, it is highly recommended that families take care of the mental health of the elderly during Covid-19 so that it does not affect their physical health. Maintaining the mental health of the elderly during the Covid-19 pandemic requires assistance from all parties. Families, health workers, the government, and the elderly must cooperate. In addition, the knowledge, attitude, and behavior of the elderly need to be improved to deal with the Covid-19 pandemic. Adaptation and survival are the keys to overcoming this pandemic condition [29].
The primary strategy is to ensure that the elderly always maintain physical distance, wash their hands, use masks, eat nutritious foods, and do light exercise [36,37]. Other activities that can be done indoors, such as reading books, painting, or watching movies, can still be done. Explanations should be given as concisely as possible to the elderly. If the elderly understand, they will feel safe and peaceful and improve their quality of life. Social relations with family and friends must still be carried out through communication tools. Emotional support is crucial for the elderly who live alone. They are prone to anxiety and confusion during this uncertain period [9,38].
Visits to the doctor should be replaced with telemedicine. Patients can consult via Whatsapp, telephone, short message, Zoom, or any application. All planned surgeries should be postponed, such as cataracts, hernias, and kneecap replacements [38]. Any redundant information about Covid-19 should be reduced to prevent panic and misunderstanding. Information should focus on preventive measures, not on myths alone. Health information, updates about Covid-19, and psychological consultations should be provided by telephone or online by the government [30,39]. Although the elderly may appear weak from the outside, the family must try to give them a sense of freedom, respect, and genuine care. The elderly must still be involved in decision-making [40].
The World Health Organization (WHO) emphasizes the importance of psychosocial needs for the elderly [38]. The government is expected to provide basic needs for the elderly, especially those less well off financially and psychologically. The items that is important to prepare including food, medicines, and disinfectants. The need for security is essential and should not be ignored [41].
The strength of this study is that the two questionnaires used, namely the Self Reporting Questionnaire (SRQ) and the World Health Organization Quality of Life-Old (WHOQOL – OLD) questionnaire, have used the Indonesian version of the questionnaire to reduce research bias.
CONCLUSION
Psychosocial status related to quality of life in the elderly with osteoarthritis during the Covid-19 pandemic. The elderly who do not suffer from mental disorders will show a tendency for a good quality of life.
LIMITATIONS
The research location only involves 1 place so that it cannot compare the results of similar studies in different populations, so in the future research must be carried out involving several regions. Another limitation is the cross-sectional research design because it only measures the current condition of the variables, so it can cause research results to be biased.
FUNDING STATEMENT
This research did not receive any specific grant from funding agencies in the public, commercial, or not for profit sectors.
COMPETING INTERESTS STATEMENT
There are no competing interests for this study.
AUTHORS’ CONTRIBUTION
All authors equally contributed to preparing this article.
REFERENCES
- do Nascimento RJ, Barbosa Filho VC, Rech CR, Brasil RB, Junior RC, Streit IA, et al. Changes in Health-Related Quality of Life and Physical Activity Among Older Adults in the First-Wave COVID-19 Outbreak: A Longitudinal Analysis. Journal of Aging and Physical Activity. 2021;30(3):389–96.
- Ragni E, Mangiavini L, Viganò M, Brini AT, Peretti GM, Banfi G, et al. Management of Osteoarthritis During the COVID‐19 Pandemic. Clinical Pharmacology & Therapeutics. 2020;108(4):719–29.
- Pramono YS, Yuniarti Y, Anggraini L. Hubungan Derajat Insomnia Dengan Pemenuhan Kebutuhan Activity Of Daily Living Pada Lansia Di Panti Sosial Budi Sejahtera Banjarbaru 2019. Dinamika Kesehatan: Jurnal Kebidanan dan Keperawatan. 2019;10(2):916–27.
- Lábadi B, Arató N, Budai T, Inhóf O, Stecina DT, Sík A, et al. Psychological well-being and coping strategies of elderly people during the COVID-19 pandemic in Hungary. Aging & Mental Health. 2022;26(3):570–7.
- Nimitha KJ, Singh B, Srivastava RN, Kumar R. SYMPOSIUM Health Related Quality Of Life And Depression In Older Adults With Knee Osteoarthritis Pain-Cross-Sectional Telephonic Survey In Covid 19 Pandemic. Indian journal of psychiatry. 2022;64(Suppl 3):S634.
- Giacalone A, Rocco G, Ruberti E. Physical health and psychosocial considerations during the COVID-19 outbreak. Psychosomatics. 2020;61(6):851–2.
- Dubey S, Biswas P, Ghosh R, Chatterjee S, Dubey MJ, Chatterjee S, et al. Psychosocial impact of COVID-19. Diabetes & Metabolic Syndrome: clinical research & reviews. 2020;14(5):779–88.
- Onder G, Rezza G, Brusaferro S. Case-fatality rate and characteristics of patients dying in relation to COVID-19 in Italy. Jama. 2020;323(18):1775–6.
- Lee K, Jeong G-C, Yim J. Consideration of the psychological and mental health of the elderly during COVID-19: A theoretical review. International journal of environmental research and public health. 2020;17(21):8098.
- Akat M, Karataş K. Psychological effects of COVID-19 pandemic on society and its reflections on education. Electronic Turkish Studies. 2020;15(4).
- Min Fui W, Abdul Majid H, Ismail R, Su TT, Maw Pin T, Said MA. Psychosocial factors associated with mental health and quality of life during the COVID-19 pandemic among low-income urban dwellers in Peninsular Malaysia. PloS one. 2022;17(8):e0264886.
- Bidzan-Bluma I, Bidzan M, Jurek P, Bidzan L, Knietzsch J, Stueck M, et al. A Polish and German population study of quality of life, well-being, and life satisfaction in older adults during the COVID-19 pandemic. Frontiers in psychiatry. 2020;11:585813.
- Wiraini TP, Zukhra RM, Hasneli Y. Hubungan Dukungan Keluarga Dengan Kualitas Hidup Lansia Pada Masa COVID-19. Health Care: Jurnal Kesehatan. 2021;10(1):44–53.
- Muliani R, Jayanti TN, Dirgahayu I, Safarudin I, Anri A. Psychosocial Support in Increasing COVID-19 and Mental Health in The Elderly. JCES (Journal of Character Education Society). 2021;4(1):135–47.
- Zulka AN, Suryaningsih Y, Wulandari PNM, Putri DA. Evaluasi Manajemen Penyakit dan Psychological Well Being Lansia di Masa Pandemi Covid 19. The Indonesian Journal of Health Science. 2022;14(1):84–91.
- Juwita R. Meningkatkan Kualitas Hidup Lansia Pasca Pandemi Covid 19. Jurnal Mitra Prima. 2022;4(2).
- Rayani D, Purqoti DNS. Kecemasan Keluarga Lansia Terhadap Berita Hoax Dimasa Pandemi COVID-19. Realita: Jurnal Bimbingan dan Konseling. 2020;5(1).
- Syahruddin S. Kebugaran Jasmani Bagi Lansia Saat Pandemi Covid-19. JUARA: Jurnal Olahraga. 2020;5(2):232–9.
- Alexandre T da S, Cordeiro RC, Ramos LR. Factors associated to quality of life in active elderly. Revista de saude publica. 2009;43:613–21.
- Guida C, Carpentieri G. Quality of life in the urban environment and primary health services for the elderly during the Covid-19 pandemic: An application to the city of Milan (Italy). Cities. 2021;110:103038.
- Idaiani S, Suryaputri IY, Mubasyiroh R, Indrawati L, Darmayanti I. Validity of the Self Reporting Questionnaire-20 for Depression Based on National Health Survey. 2021;
- Priastana IKA, Kusumaningtiyas DPH. Quality of Life in The Elderly Viewed from Hope, Friend Support, and Family Support. STRADA Jurnal Ilmiah Kesehatan. 2020;9(2):1670–5.
- Sugiyono. Metode penelitian pendidikan pendekatan kuantitatif, kualitatif dan R&D. Alfabeta; 2013.
- Widyaningrum DA, Umam FN. Pengaruh Nyeri Sendi Terhadap Kualitas Tidur dan Kualitas Hidup Pada Lansia Penderita Osteoartritis. Jurnal Keperawatan. 2020;13(2):7.
- Intarti WD, Savitri NPH. Manfaat Relaksasi Yoga Dan Swedish Massage Terhadap Stress Lansia Saat Pandemi Covid-19. Jurnal Bina Cipta Husada. 2021;17(1):96–112.
- Banerjee D. ‘Age and ageism in COVID-19’: Elderly mental health-care vulnerabilities and needs. Asian journal of psychiatry. 2020;51:102154.
- Jing Z, Li J, Wang Y, Ding L, Tang X, Feng Y, et al. The mediating effect of psychological distress on cognitive function and physical frailty among the elderly: evidence from rural Shandong, China. Journal of affective disorders. 2020;268:88–94.
- Wu Z, McGoogan JM. Characteristics of and important lessons from the coronavirus disease 2019 (COVID-19) outbreak in China: summary of a report of 72 314 cases from the Chinese Center for Disease Control and Prevention. jama. 2020;323(13):1239–42.
- Perrotta F, Corbi G, Mazzeo G, Boccia M, Aronne L, D’Agnano V, et al. COVID-19 and the elderly: insights into pathogenesis and clinical decision-making. Aging clinical and experimental research. 2020;32(8):1599–608.
- Armitage R, Nellums LB. COVID-19 and the consequences of isolating the elderly. The Lancet Public Health. 2020;5(5):e256.
- Peat G, McCarney R, Croft P. Knee pain and osteoarthritis in older adults: a review of community burden and current use of primary health care. Annals of the rheumatic diseases. 2001;60(2):91–7.
- Jakobsson ULF, Hallberg IR. Pain and quality of life among older people with rheumatoid arthritis and/or osteoarthritis: a literature review. Journal of clinical nursing. 2002;11(4):430–43.
- Neogi T. The epidemiology and impact of pain in osteoarthritis. Osteoarthritis and cartilage. 2013;21(9):1145–53.
- McCaffrey R, Freeman E. Effect of music on chronic osteoarthritis pain in older people. Journal of advanced nursing. 2003;44(5):517–24.
- Hong J-Y, Han K, Shin D-H, Chun EM. Quality of life analysis and smoking correlation in symptomatic spine osteoarthritis: a nationwide health survey analysis of an elderly population with EQ-5D. PLoS One. 2016;11(3):e0151315.
- Meng H, Xu Y, Dai J, Zhang Y, Liu B, Yang H. Analyze the psychological impact of COVID-19 among the elderly population in China and make corresponding suggestions. Psychiatry research. 2020;289:112983.
- Girdhar R, Srivastava V, Sethi S. Managing mental health issues among elderly during COVID-19 pandemic. Journal of geriatric care and research. 2020;7(1):32–5.
- Banerjee D. The impact of Covid‐19 pandemic on elderly mental health. International journal of geriatric psychiatry. 2020;35(12):1466.
- Petretto DR, Pili R. Ageing and COVID-19: what is the role for elderly people? Vol. 5, Geriatrics. MDPI; 2020. p. 25.
- Liu K, Chen Y, Lin R, Han K. Clinical features of COVID-19 in elderly patients: A comparison with young and middle-aged patients. Journal of Infection. 2020;80(6):e14–8.
- Papadopoulos V, Li L, Samplaski M. Why does COVID‐19 kill more elderly men than women? Is there a role for testosterone? Andrology. 2021;9(1):65–72.
![]() This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
Cardiopulmonary Resuscitation (CPR) during COVID-19 Pandemic
Aprianto Daniel Pailaha1*
1 Professional Nurse Study Program, Department of Nursing, Faculty of Health Sciences, Brawijaya University, Malang, Indonesia
*Corresponding Author: Ns. Aprianto Daniel Pailaha, S.Kep., Professional Nurse Study Program, Department of Nursing, Faculty of Health Sciences, Brawijaya University, Malang, Indonesia. Email: apriantodanielpp@gmail.com
ORCHID ID: https://orcid.org/0000-0002-9456-6616

Cite this article
ABSTRACT
Introduction: The COVID-19 infection has a high rate of mortality and morbidity and is extremely contagious. COVID-19 has raised attention to safety issues involving healthcare workers who perform CPR. The risk of transmission produces a dilemma to perform cardiopulmonary resuscitation (CPR) within the COVID-19 pandemic. Additionally, patient and/or family preferences, as a factor associated with Do-Not-Resuscitate (DNR). This commentary wants to provide an overview or other perspectives that may be the subject of further research so that there will be evidence base practice for health workers, especially nurses in code blue situations.
Discussion: COVID-19 pandemic has clearly had a significant impact on the epidemiology and outcome of cardiac arrest in both out-of-hospital and in-hospital settings. All potential COVID-19 patients should be offered the advantage of CPR by attempting to revive them after taking all required safety precautions, and the patient should only be confirmed dead after CPR has been performed. Provision of further information regarding CPR to patients and/or families for consideration, including the advantages and disadvantages of CPR, before making a final decision regarding the administration of CPR. COVID-19 patients with a poor prognosis might benefit from Do-Not-Resuscitate (DNR) but this is causes dilemmas in nursing profession.
Conclusion: Although the survival rate for COVID-19 patients is poor, it is anticipated that CPR attempts will still be performed during the COVID-19 pandemic by following several guidelines. COVID-19 patients with a poor prognosis might benefit from Do-Not-Resuscitate (DNR) if the patient and/or family who are accountable provide their approval and everything is in order. As a nurse, we must respect the decisions that patients or families make because it is their right and their authority.
Keywords: CPR; Cardiac Arrest; DNR; COVID-19; Nursing
INTRODUCTION
The COVID-19 pandemic is extremely challenging health care systems worldwide and increasing principal ethical issues, especially concerning a prospect need for health care in the context of scarce resources and crisis capacity. Cardiac arrest is defined as the sudden cessation of cardiac mechanical activity, confirmed by the absence of signs of circulation. Lack of blood flow to the brain and other vital organs can cause loss of consciousness, powerlessness, or death if not treated properly [1]. Cardiac arrest is associated with pneumonia in COVID-19 patients, myocardial injury has a poor percentage of outcomes, whereas other Cardiovascular Disease (CVD) cases without myocardial injury are relatively vulnerable [1,2]. The COVID-19 patients may experience respiratory dysfunction and a subsequent change in tissue oxygenation that directly affects the cardiovascular system and results in serious issues including myocarditis, myocardial injuries, acute myocardial infarction, heart failure, cardiac dysrhythmia, and thromboembolism [3]. COVID-19 infection has a high mortality and morbidity rate and is highly contagious. COVID-19 has raised attention to safety issues involving healthcare workers attempting CPR. Among the several aerosol-producing procedures performed on patients, CPR is strongly associated with a variety of aerosol-generating procedures, including chest compression, positive pressure ventilation, and the respiratory tract maneuver. This will trigger extremely concerned about being infected with COVID-19 because considering that the COVID-19 virus is very dangerous for vulnerable populations.
Several inpatients experiencing cardiac arrest are administered cardiopulmonary resuscitation (CPR), provided advance instructions are available or the patient has a documented Do-Not-Resuscitate (DNR) status [4]. Despite the fact that attitudes regarding CPR have changed due to the COVID-19 pandemic, the majority of respondents reported that they would be prepared to do CPR if they encountered a cardiac arrest incident. Notably, independent of usual circumstances, people are more inclined to perform CPR without mouth-to-mouth resuscitation. There were other factors that affected CPR during the COVID-19 pandemic, however the two of that had been determined to be of considerable increasing significance were the fear of contracting COVID-19 and the fear of spreading COVID-19 to others, which were assessed at 78% and 29%, respectively [5,6]. This is a separate consideration for health workers, especially nurses in implementing CPR in cases of cardiac arrest during the COVID-19 pandemic.
When a new pandemic begins, the infection in healthcare facilities spreads easily. In April 2020, as many as 22,073 cases of COVID-19 among healthcare professionals were reported to the WHO. On February 2020, there were 1716 healthcare professionals in China who had contracted SARS-CoV-2. As many as 3300 people were infected as of early March, and at least 22 of them died in China. As of March 2020, about 2600 people were infected in Italy, and 13 of them had died [7]. When performing CPR during the COVID-19 pandemic, there are several factors that need to be considered carefully to ensure the safety of the rescuers, the patients, and the surroundings. The purpose of writing comments on this article is to provide an opinion regarding the administration of CPR in cardiac arrest in patients with COVID-19 or during this COVID-19 pandemic.
The resuscitation guidelines, in force considering 2015, have consequently been adapted to this new situation, e.g., for Basic Life Support (BLS), mouth-to-mouth ventilation in addition to chest compression are encouraged to bystanders. For Advanced Life Support (ALS), bag-masks or Supraglottic Airway (SGA) ventilation are considered appropriate options to tracheal intubation [8]. Recently, updates have been issued, considerably with the aid of using the International Liaison Committee on Resuscitation (ILCOR), European Resuscitation Council (ERC), and the American Heart Association (AHA). Briefly, the principle modifications advise that lay rescuers have to consider chest compressions only, except for children, and all life support providers must use PPE all through resuscitation and favor early tracheal intubation to minimize aerosols.
The risk of transmission of the SARS-CoV-2 virus to initial responders performing cardiopulmonary resuscitation (CPR) produce a dilemmas to manage CPR within the COVID-19 pandemic. A better knowledge of this could enable identification of which individuals are less likely to benefit from CPR, and inform discussion of a Do Not Resuscitate (DNR). This aims to provide an overview or other perspectives that may be the subject of further research so that there will be evidence base practice for health workers, especially nurses in code blue situations.
DISCUSSION
1. CPR and COVID-19 Additional Considerations
The new regulations for performing high-quality CPR during the COVID-19 pandemic have been introduced to lower the risk of COVID-19 transmission. In order, the American Heart Association (AHA), European Resuscitation Council (ERC), International Liaison Committee on Resuscitation (ILCOR), and other resuscitation associations have been released a modification guidelines or recommendations for the COVID-19 pandemic concerns into account [9-11]. Several modification and recommendation implemented since the COVID-19 pandemic:
1) International Liaison Committee on Resuscitation (ILCOR)
Treatment recommendations from ILCOR for performing CPR to address cardiac arrest problems in patients with COVID-19 [12].
a) Cardiopulmonary resuscitation and chest compressions may produce aerosol.
b) Rescuers consider public-access defibrillation and compression-only.
c) Rescuers who are committed, competent, and trained may choose to give children rescue breaths in addition to chest compressions (good practice statement).
d) Should wear personal protection equipment during resuscitation
e) Rescuers consider defibrillation before donning aerosol-generating personal protection equipment.
2) European Resuscitation Council (ERC)
The following new recommendation of Basic Life Support (BLS) are advised by the European Resuscitation Council for patients with confirmed or suspected COVID-19 [12,13].
a) Should have prior training in appropriate use of PPE
b) Consider to compression-only CPR if bag-mask ventilation is difficult or not available
c) Use a high-efficiency particulate air (HEPA) filter during bag-mask ventilation
d) Use two hands to hold the mask and the person doing compressions can squeeze the bag when they pause after 30 compressions
e) Use PPE (surgical mask, eye protection, apron, and gloves) before defibrillation because not an aerosol-generating procedure
3) American Heart Association (AHA)
The American Heart Association (AHA) introduced new recommendation for Basic Life Support (BLS) in COVID-19 patients both in‑and out‑of‑hospital cardiac arrest [13].
a) Significantly reduce the risk of infection with vaccination and boosters.
b) CPR is considered to be an aerosol-generating procedure (AGP) such as hest compressions, defibrillation, bag-valve-mask (BVM) ventilation, intubation, and positive pressure ventilation.
c) Should wear PPE such as N95 mask, gloves, gown, eye protection, positive pressure ventilation.
d) PPE must be donned before performing components of resuscitation.
If patients have any signs and symptoms, bystanders should give defibrillation only and without chest compression unless they have PPE. As a result, the estimated death rates for CPR are extremely low, and the use of barriers such as PPE was strongly recommended to reduce the risk of COVID-19 transmission. Cardiopulmonary Resuscitation (CPR) attempts such as chest compression only and defibrillation only as procedures with an increased risk of COVID-19 transmission. Tracheal intubation and mouth-to-mouth or mouth-to-mask ventilation were associated with a high risk of COVID-19 transmission. Although previous research has shown that compression-only CPR is as effective as combined compressions and ventilations, this could not be the case for COVID-19 patients because they suffer from primary respiratory failure.
The European Resuscitation Council (ERC) COVID-19 guidelines encourage continuing resuscitation efforts for cardiac arrests that occur both inside and outside of hospitals while also attempting to reduce risk to the person providing treatment. The COVID-19 guidelines focus specifically on patients with COVID-19. Those providing treatment should conduct a dynamic risk assessment, which may include current COVID-19 prevalence, the patient's presentation, the probability that treatment will be effective and efficient, the accessibility of personal protective equipment (PPE), and personal risks for those providing treatment [14]. The proportion of patients with shockable rhythms decreased, as did the use of automated external defibrillators. The use of supraglottic airways increased, while the rate of intubation decreased. Overall, there was a increase rates return of spontaneous circulation, survival to admission, and survival to discharge.
2. CPR Outcomes during COVID-19 Pandemic
According to recent research, in-hospital cardiac arrest (IHCA) among COVID-19 patients was 9.39%, with 9% ROSC and 2% survival to hospital discharge. Accordingly, the average rate of out-of-hospital cardiac arrest (OHCA) survival to discharge is 8.8% [15]. But among COVID-19 patients, two more investigations on both in- and out-of-hospital CA showed a 0% survival rate to hospital discharge rate [16,17]. The primary CPR success rate among COVID-19 patients was low, especially for those with asystole or bradycardia [3,18]. This harmful infection has influenced the CPR efficacy because there are additional considerations for the CPR attempt. Therefore, the COVID-19 pandemic has largely influenced CPR procedures. Apart from the various factors involved in performing CPR, another thing that must be considered is the ability and capability to perform CPR through training [19]. Participation in training such as Basic Trauma Cardiac Life Support (BTCLS) or Advanced Cardiac Life Support (ACLS) will help nurses gain more knowledge, experience, and skills when it comes to performing CPR on cardiac arrest patients.
Continuous cardiopulmonary resuscitation (CPR) training and quality control systems, such as monitoring morbidity and mortality, are also recommended [20]. Every nurse, especially those working in emergency room, needs to have the necessary training to administer first aid in accordance with protocol. As a result, nurses may feel more confident and competent to provide CPR in situations of cardiac arrest.
Data from in-hospital cardiac arrests caused by COVID-19 are less commonly reported. According to a multicenter cohort study from 68 Intensive Care Units in the United States found that 14.0% (701/5019) of patients had an in-hospital cardiac arrest, 57.1% (400/701) received CPR, and 7.0% (28/400) survived to hospital discharge with normal or mildly impaired neurological status [21]. According to data from 136 patients in China, about 113 (83.1%) of them required CPR, and ROSC occurred in 18 (13.2%) of the patients, 4 (2.9%) survived for at least 30 days, and one patient had a favorable neurological outcome at 30 days [22]. COVID-19 pandemic has clearly had a significant impact on the epidemiology and outcome of cardiac arrest in both out-of-hospital and in-hospital settings.
3. Nursing Decision-Making
Nursing is patient-centered care. A nursing profession requires to follow an ethical code, which allowed to provide great nursing care. Therefore, the nursing profession intends to maintain and improve health care in society. The key point is that a lower survival rate in CPR was reported at the start of the COVID-19 pandemic compared to previous years. All intervention decisions must involve informed and involved patients and/or families, according to national and institutional policy [23]. However, patient and/or family preferences, as a factor associated with Do-Not-Resuscitate (DNR). Provision of further information regarding CPR to patients and/or families for consideration, including the advantages and disadvantages of CPR, before making a final decision regarding the administration of CPR.
It is critical for determine personal goals and preferences regarding a resuscitation attempt. The mortality rate for COVID-19 patients who seemed to be critically ill was significant and increased with age, comorbidities, and symptom severity. The AHA recommends taking these considerations into account when weighing the risk versus the benefit of initiating resuscitation. Furthermore, many different institutions have strongly advised patients with poor prognoses to consider DNR. When considering DNR, COVID-19 positivity by itself cannot be a factor except when it is accompanied by irreversible multi-organ dysfunction [16,24]. All potential COVID-19 patients should be offered the advantage of CPR by attempting to revive them after taking all required safety precautions, and the patient should only be confirmed dead after CPR has been performed. The statement emphasized the need for all professionals to consider every cardiac arrest victim who presents to the emergency room as a possible COVID-19 suspect during the pandemic and to wear the proper PPE. The CPR method should be performed with the fewest number of essential medical professionals present, ideally in a single-person room with the door closed.
It is noteworthy that CPR, in some cases, has been initiated by nurses, but the decision-making process for non-resuscitation is made by the physician and based on the discussion between the all-team members, considers not being useful the CPR maneuvers for some cases. It depends on the nurse, among other actions, the functionality of the stop cart, with availability of materials necessary for this type of assistance, technical procedures for venipuncture, preparation and administration of medications, supervision of the technical professionals of the nursing team and possible relay in resuscitation maneuvers.
4. Ethical Approaches and DNR
The reality requires reflection with a professional ethical focus on the duty of updating professionals, as provided for in the Code of Ethics for Nursing Professionals, and which determines that the patient has the right to get preserve of correct information, to be heard in their needs, and to get preserve of resolute humanized care. These conclusions are based on bioethical reflection and acknowledgement that not all nurses working in palliative care for COVID-19 patients with DNR are able to provide communication that supports this choice, either by acting in accordance with protocol or by providing nursing care without considering or updating the practice of euthanasia. In this situation, struggling to take into consideration the knowledge of those involved or neglecting to listen to the patient and family interferes with their ability to communicate effectively and their autonomy, leading to conflicts and challenges in the management of nursing care.
According to qualitative research, in Maryland there are 31 nurses who worked for COVID-19 patients in the acute care units, in depth-interview the nurse mentioned that “They really push that DNR and that’s like a part of my distress, because I know I’m very patient-family centered in my thinking…because it’s futile they tell the family this person should be DNR. They’re over 70, we’re not going to escalate care…The family has to believe whatever we tell them…so hopefully they’re right, because they don’t have a choice, the family or the patient.[25]” Knowing the DNR order causes the nurse to experience moral distress. Rather than enhancing services, prepare for end-of-life care is something that is very difficult. Of course, as a nurse, you want to do the best for patients and their families, but not in the event of a DNR, because It is the patient and family's authority. Besides, disagreement about the proper use of end-of-life care is one of the triggers of moral distress when providers encourage families to do DNR.
According to qualitative research, in Philippines there are 12 nurses who worked in COVID-19 ward of several hospitals, the nurse mentioned that “Occasionally, family members decide against intubation because they do not wish to witness their family member suffer further and add to the agony of the patient [26].” Severe symptoms of COVID-19 prompt families to put their loved ones out of the misery and sign DNR forms. In this case, nurses support symptom-free death and suffering reduction through assisting patients and families.
According to qualitative research, in United States there are 7 ICU nurses, in interview session the nurse mentioned that "Patient was a DNR or DNI maxed out on BiPAP (bilevel positive airway pressure support) and developed respiratory arrest. I, the nurse, and the intensivist thoroughly explained the situation to the family and encouraged transition to comfort care, yet the family refused. The patient suffered for another day and a half before she died. I was furious at the family and heartbroken for the patient, she deserved a more dignified death than she received [27].” The nurse was not explicit use term “moral distress” but describe about condition when they experienced moral-constraint distress because they perceived the life-sustaining treatments provided were contrary to the patient’s wishes and contributing to the patient’s suffering because they were constrained by a DNR order. Surrogate decision-making are not reflect the fully patient’s wishes.
Evidence has emerged illustrating ethical dilemmas in conducting DNR discussions during the COVID-19 pandemic [28]. Based on some of the qualitative research findings in several countries, it shows that DNR status causes moral distress due to opposition, and disagreement about DNR. Moreover, nurses have to support symptom-free death and suffering reduction for patients and their families. Additionally, nurses believe that the DNR is not in line with the patient's intentions and that the surrogate decision-making certainly does not properly represent the patient's preferences. Some of the responses given by nurses depend on the assessment of the ethics held. This can be considered valid or correct if it is based on strong evidence.
CONCLUSIONS
Even when cardiopulmonary resuscitation is administered, cardiac arrest is common in critically ill COVID-19 patients and is associated with poor survival. COVID-19 patients with a poor prognosis might benefit from Do-Not-Resuscitate (DNR) if the patient and/or family who are accountable provide their approval and everything is in order. In fact, CPR efforts are still possible if there is a chance of surviving the patient. Although the survival rate for COVID-19 patients is poor, it is anticipated that CPR attempts will still be performed during the COVID-19 pandemic by following several guidelines in order to help people COVID-19 patients to survive using the American Heart Association (AHA), European Resuscitation Council (ERC), International Liaison Committee on Resuscitation (ILCOR), and other resuscitation associations modification guidelines or recommendations for the COVID-19 pandemic. However, patient and/or family preferences, as a factor associated with Do-Not-Resuscitate (DNR) in several cardiac arrest conditions. Nursing profession have to reflection and uphold ethical as provided for in the Code of Ethics for Nursing Professionals. DNR status causes moral distress due to opposition, and disagreement. Surrogate decision-making certainly does not properly represent the patient's preferences. As nurse, we have to support symptom-free death and suffering reduction for patients and their families, and respect the decisions that patients or families make because it is their right and their authority.
CONFLICT OF INTERESTS DISCLOSURE
The author declares that there is no conflict of interests
ETHICAL APPROVAL
Not applicable
FUNDING
Not applicable
REFERENCES
- Shao F, Xu S, Ma X, et al. In-hospital cardiac arrest outcomes among patients with COVID-19 pneumonia in Wuhan, China. Resuscitation 2020;151:18–23; doi: 10.1016/j.resuscitation.2020.04.005.
- Guo T, Fan Y, Chen M, et al. Cardiovascular Implications of Fatal Outcomes of Patients With Coronavirus Disease 2019 (COVID-19). JAMA Cardiol 2020;5(7):811; doi: 10.1001/jamacardio.2020.1017.
- Goodarzi A, Khodaveisi M, Abdi A, et al. Cardiopulmonary Resuscitation Outcomes of Patients with COVID-19; a One-Year Survey. Arch Acad Emerg Med 2021;9(1); doi: 10.22037/AAEM.V9I1.1381.
- Garg H, Jha S. Cardiopulmonary Resuscitation during COVID-19 Pandemic: Outcomes, Risks, and Protective Strategies for the Healthcare Workers and Ethical Considerations. Indian Journal of Critical Care Medicine 2020;24(9):868–872; doi: 10.5005/jp-journals-10071-23544.
- AL-shiakh S, Tran QK, Caggiula A, et al. Attitudes among healthcare professionals towards cardiopulmonary resuscitation during COVID-19. Am J Emerg Med 2022;52:34–42; doi: 10.1016/j.ajem.2021.11.017.
- Chong K-M, Chen J-W, Lien W-C, et al. Attitude and behavior toward bystander cardiopulmonary resuscitation during COVID-19 outbreak. PLoS One 2021;16(6):e0252841; doi: 10.1371/journal.pone.0252841.
- Jin YH, Huang Q, Wang YY, et al. Perceived infection transmission routes, infection control practices, psychosocial changes, and management of COVID-19 infected healthcare workers in a tertiary acute care hospital in Wuhan: A cross-sectional survey. Mil Med Res 2020;7(1); doi: 10.1186/s40779-020-00254-8.
- Baert V, Jaeger D, Hubert H, et al. Assessment of changes in cardiopulmonary resuscitation practices and outcomes on 1005 victims of out-of-hospital cardiac arrest during the COVID-19 outbreak: registry-based study. Scand J Trauma Resusc Emerg Med 2020;28(1); doi: 10.1186/s13049-020-00813-x.
- Kundra P, Vinayagam S. COVID-19 cardiopulmonary resuscitation: Guidelines and modifications. J Anaesthesiol Clin Pharmacol 2020;36(5):39; doi: 10.4103/joacp.JOACP_257_20.
- Chojecka D, Pytlos J, Zawadka M, et al. How to Maintain Safety and Maximize the Efficacy of Cardiopulmonary Resuscitation in COVID-19 Patients: Insights from the Recent Guidelines. J Clin Med 2021;10(23):5667; doi: 10.3390/jcm10235667.
- Fazel MF, Mohamad MHN, Sahar MA, et al. Readiness of Bystander Cardiopulmonary Resuscitation (BCPR) during the COVID-19 Pandemic: A Review. Int J Environ Res Public Health 2022;19(17):10968; doi: 10.3390/ijerph191710968.
- Nolan JP, Monsieurs KG, L.Bossaert, et al. European Resuscitation Council COVID-19 guidelines executive summary. Resuscitation 2020;153:45–55; doi: 10.1016/j.resuscitation.2020.06.001.
- Kundra P, Vinayagam S. COVID-19 Cardiopulmonary Resuscitation: Guidelines and Modifications. J Anaesthesiol Clin Pharmacol 2020;36(5):S39–S44; doi: 10.4103/joacp.JOACP_257_20.
- Perkins GD, Graesner JT, Semeraro F, et al. European Resuscitation Council Guidelines 2021: Executive summary. Resuscitation 2021;161:1–60; doi: 10.1016/j.resuscitation.2021.02.003.
- Nguyen D, Sarani N, Marshall K, et al. CODE BLUE-19: A Proposed Protocol to Mitigate COVID-19 Transmission in the Emergency Department when Receiving Out-of-hospital Cardiac Arrest Patients. Western Journal of Emergency Medicine 2020;21(6); doi: 10.5811/westjem.2020.7.48436.
- Sultanian P, Lundgren P, Strömsöe A, et al. Cardiac arrest in COVID-19: characteristics and outcomes of in- and out-of-hospital cardiac arrest. A report from the Swedish Registry for Cardiopulmonary Resuscitation. Eur Heart J 2021;42(11):1094–1106; doi: 10.1093/eurheartj/ehaa1067.
- Thapa SB, Kakar TS, Mayer C, et al. Clinical Outcomes of In-Hospital Cardiac Arrest in COVID-19. JAMA Intern Med 2021;181(2):279; doi: 10.1001/jamainternmed.2020.4796.
- Hayek SS, Brenner SK, Azam TU, et al. In-hospital cardiac arrest in critically ill patients with covid-19: multicenter cohort study. BMJ 2020;m3513; doi: 10.1136/bmj.m3513.
- Sukarwan A, Peristiowati Y, Ellina AD. The Role of Emergency Nurses in Cardiopulmonary Resuscitation (CPR) of Cardiac Arrest Patients: A Literature Review. ENDLESS : International Journal of Future Studies 2021;4(1):148–158; doi: 10.54783/endless.v4i1.53.
- Taha HS, Shaker MM, Abdelghany MM. Cardiopulmonary resuscitation during the COVID-19 pandemic: a scientific statement on CPR management protocol of Kasr Al-Ainy University Hospital is presented. The Egyptian Heart Journal 2020;72(1):73; doi: 10.1186/s43044-020-00106-9.
- Hayek SS, Brenner SK, Azam TU, et al. In-hospital cardiac arrest in critically ill patients with covid-19: multicenter cohort study. BMJ 2020;371:m3513; doi: 10.1136/bmj.m3513.
- Phattharapornjaroen P, Nimnuan W, Sanguanwit P, et al. Characteristics and outcomes of out-of-hospital cardiac arrest patients before and during the COVID-19 pandemic in Thailand. Int J Emerg Med 2022;15(1); doi: 10.1186/s12245-022-00444-2.
- Connellan D, Diffley K, McCabe J, et al. Documentation of Do-Not-Attempt-Cardiopulmonary-Resuscitation orders amid the COVID-19 pandemic. Age Ageing 2021;50(4):1048–1051; doi: 10.1093/ageing/afab075.
- Nguyen D, Sarani N, Marshall K, et al. CODE BLUE-19: A Proposed Protocol to Mitigate COVID-19 Transmission in the Emergency Department when Receiving Out-of-hospital Cardiac Arrest Patients. Western Journal of Emergency Medicine 2020;21(6); doi: 10.5811/westjem.2020.7.48436.
- Silverman HJ, Kheirbek RE, Moscou-Jackson G, et al. Moral distress in nurses caring for patients with COVID-19. Nurs Ethics 2021;28(7–8):1137–1164; doi: 10.1177/09697330211003217.
- Jimenez OJB, Trajera SM, Ching GS. Providing End-of-Life Care to COVID-19 Patients: The Lived Experiences of ICU Nurses in the Philippines. Int J Environ Res Public Health 2022;19(19); doi: 10.3390/ijerph191912953.
- Morley G, Copley DJ, Field R, et al. RESPONDER: A qualitative study of ethical issues faced by critical care nurses during the COVID-19 pandemic. J Nurs Manag 2022; doi: 10.1111/jonm.13792.
- Hanna K, Cannon J, Gabbay M, et al. End of life care in UK care homes during the COVID-19 pandemic: a qualitative study. BMC Palliat Care 2022;21(1); doi: 10.1186/s12904-022-00979-4.
![]() This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.