Francesco Saverio Auricchio¹*, Maria Russo²,
Maddalena Lettieri¹, Nicolas Craparotta¹
¹Department of Translation Medical Sciences, University Federico II, Naples.
²San Giovanni di Dio Civil Hospital of Frattamaggiore, Asl Naples 2 North, Naples.
*Corresponding author: Francesco Saverio Auricchio, Department of Translation Medical Sciences, University Federico II, Naples.
Email: francescosaverio.auricchio@unina.it

Cite this article
ABSTRACT
Introduction: In recent years, with the rapid advancement of technology, tools capable of minimising discomfort for the diabetic patient are becoming increasingly popular, thereby increasing adherence to treatment. The use of technology improves glycometabolic compensation and quality of life.
Objective: The aim of the present study is to verify, in the group using the Flash Glucose Monitoring system, improved diabetes management and satisfaction in insulin-treated patients.
Materials and Methods: A retrospective cross-sectional study was performed through the administration of the “Diabetes Treatment Satisfaction Questionnaire”. The study was performed from January to July 2019. 82 validated questionnaires were administered in the Italian version. Participants were 47 women (39 Type 1 Diabetes Mellitus and 8 Type 2 Diabetes Mellitus) and 35 men (19 Type 1 Diabetes Mellitus and 16 Type 2 Diabetes Mellitus).
Results: Results show that subjects with the Flash Glucose Monitoring system have greater satisfaction than those using the Self-Monitoring of Blood Glucose system. Patients using Flash Glucose Monitoring showed 83.9% satisfaction, while patients using Self-Monitoring of Blood Glucose showed 33.3% complete satisfaction. The average glycosylated haemoglobin of the group of subjects using Flash Glucose Monitoring was 53.2 mmol/mol, while that of subjects with self-monitoring of capillary blood glucose was 60.3 mmol/mol.
Conclusions: The adoption of new technologies has benefits for the patient that positively affect quality of life. The study showed better glycometabolic compensation in the group of patients using Flash Glucose Monitoring. Diabetes carries significant costs to public health, and prevention and improvement of care could be a primary goal for the community and health systems.
Keywords: Diabetes mellitus; Telemedicine; Technology; Flash glucose monitoring; Self-monitoring of blood glucose
INTRODUCTION
Diabetes mellitus is a chronic disease characterised by increased concentration of glucose in the blood. The vast majority of diabetes cases fall into two broad aetiopathogenic categories. In one category, Type 1 Diabetes Mellitus (DMT1), the cause is an absolute lack of insulin secretion due to an autoimmune pathological process that occurs in the pancreatic islets and/or genetic alterations. In the other category, Type 2 Diabetes Mellitus (DMT2), the cause is a combination of resistance to insulin activity and an inadequate compensatory insulin secretory response. In the latter category, a degree of hyperglycemia sufficient to cause pathological and functional alterations in various target tissues, but without clinical symptoms, may be present for a long time before diabetes is detected [1].
DMT2 is considerably the most frequent form of diabetes (it affects 90% of cases) and is typical of middle age. It emerges as a multifactorial disease that involves both genetic predisposition and multiple environmental factors [2]. In 2021, the International Diabetes Federation (IDF) estimated that 537 million were diagnosed with diabetes mellitus and predicted that this figure will reach 643 million by 2030 and 783 million by 2045. In addition, the IDF estimated that, in 2021, 541 million people had reduced glucose tolerance. The number of children and adolescents living with diabetes is constantly increasing. In 2021, more than 1.2 million children and adolescents were diagnosed with Type 1 Diabetes Mellitus.
Direct health expenditures due to diabetes are already close to $1 trillion and will exceed this figure by 2030. The 10th edition of the IDF Diabetes Atlas also shows that hyperglycaemia in pregnancy affects about one in six pregnancies. Another cause for alarm is the consistently high percentage (45%) of people with undiagnosed diabetes, which is predominantly type 2. This highlights the urgent need to improve the ability to diagnose people with diabetes, many of whom do not know they have the condition, and to provide appropriate and timely care to all people with diabetes as soon as possible [3]. One-fifth of people with type 1 diabetes are in low- and lower-middle-income countries. The residual life expectancy of a 10-year-old child diagnosed with Type 1 Diabetes Mellitus in 2021 ranged from an average of 13 years in low-income countries, to 65 years in high-income countries [4].
Diabetes therapy is often substitutive and is based on partly frequent or continuous insulin administrations. The objective of replacement therapy is to maintain blood glucose concentrations in a physiological range, trying to avoid or in any case limit both episodes of hypoglycaemia and hyperglycaemia. It is therefore necessary to continuously harmonise insulin therapy, nutrition and exercise, also taking into account the hyperglycaemic effect of stress, intercurrent diseases and, in the case of the child, even in changes in a growing body [5]. To be able to live with your diabetes, without being overwhelmed by it, you need good blood sugar control. To judge the effectiveness of the control, it is necessary to measure the reactions of the body to the treatment, even if you are not on drug therapy, but proper care is based on lifestyle changes and physical activity [6]. Through monitoring, it is possible to intervene in the most appropriate way, bringing or maintaining blood glucose levels as close as possible to the reference values [7]. The American Diabetes Association (ADA) recommends that all diabetics try by any and all means to maintain blood sugar control so as to reduce the risk of complications [8].
Diabetes, a systemic disease not to be overlooked, has chronic complications that can also be disabling and fatal. Diabetes presents macrovascular complications, including coronary heart disease, stroke, and peripheral vascular disease, and microvascular complications, such as end-stage renal disease, retinopathy, and neuropathy, along with lower limb amputations. Complications are responsible for much of the health spending associated with diabetes. There is also a growing recognition of a diverse set of causal conditions, including cancers, ageing-related outcomes (e.g. dementia), infections, and liver disease [9]. Daily monitoring of diabetes, due to frequent capillary sampling obtained by finger prick, is painful and this can make it difficult to adhere to a diabetes management plan. In recent years, thanks to the increasing number of technologies available for glycaemic monitoring and insulin administration, there has been a real revolution in the care of people with diabetes mellitus [10].
The Flash Glucose Monitoring (FGM) system avoids inconvenience to patients due to repeated capillary punctures, providing continuous measurement of blood glucose [11] through a system consisting of a small circular sensor applied to the back of the arm that, at intervals of one minute, measures glucose in the interstitial fluid, by means of a small filament inserted under the skin and held in place by a small adhesive pad. Using this circuit, the patient is able to detect blood glucose in real time, and wirelessly transmit all the information necessary to evaluate the glycaemic trend.
The purpose of this study is to look at the impact of the FGM system on glycaemic control in insulin-treated diabetic patients, verifying whether those who use the FGM system have better diabetes management, as well as a better degree of satisfaction than those who use Self-monitoring of Blood Glucose (SMBG).
MATERIALS AND METHODS
The following cross-sectional study was carried out by administering a questionnaire validated in its Italian version, found in the international literature. The Italian adaptation of the “Diabetes Treatment Satisfaction Questionnaire” (DTSQ) was used [12]. This questionnaire has been specifically designed to measure satisfaction with diabetes treatments and can be used in both patients with type 1 diabetes and those with type 2 diabetes. The level of treatment satisfaction in the two patient groups (FGM and SMBG) and the frequency of perception of episodes of hypoglycaemia and hyperglycaemia were analysed and compared. The study began in January 2019 and was completed in July of the same year. 82 questionnaires of the validated Italian version of the DTSQ were administered. The questionnaire includes 8 questions, 6 of which are added together in a single score that varies between 8 (very unsatisfied) and 36 (very satisfied). The remaining two questions, used individually, explore the perceived frequency of episodes of hypo- and hyperglycaemia [13], through an incremental score of 1 (never) to 6 (very often). We also investigated the personal characteristics of the sample (gender and age), the type of diabetes (DMT1 and DMT2), the methods of glycaemic control (SMBG and FGM) and the value of glycosylated haemoglobin (HbA1c).
The questionnaires were administered online, on Facebook™ social media and through the Google Forms™ platform, within special groups dedicated to the diabetic patient, namely Diabetica: il gruppo sul diabete tipo 1, Diabete.com, Diabetici Insieme. The survey was conducted through the use of convenience sampling. Adherence to the questionnaire was voluntary and the questionnaire was made anonymous at source. The consent to the participation and use of the data was considered acquired at the time of sending the questionnaire. The data were analysed in aggregate form. Approval by the Local Ethics Committee was not required for this type of study.
The following inclusion criteria were defined: subjects of both sexes, patients with DMT1, patients with DMT2, patients on pharmacological treatment, patients aged > 6 years. The following exclusion criteria were defined: patients aged < 6 years, patients not pharmacologically treated or patients who follow only a diet and/or physical activity.
Statistical analyses
The data collected were processed through the use of the “LibreOffice6.2™” package for descriptive statistical analysis. The same data were analysed with the statistical software “RStudio™” for the analysis of the variables under analysis. Data are presented as number and percentage for categorical variables and continuous data are expressed as mean ± standard deviation (SD), median and interquartile range (IQR). The confidence interval (CI) was calculated for mean age and HbA1c. The different variables were analysed and correlated to assess whether there were differences in diabetes management and satisfaction in the two patient groups (SMBG and FGM). The chi-squared test was performed for the two levels of satisfaction obtained in relation to the two types of treatment. The Shapiro-Wilk test was used to determine whether the variables were distributed normally and, subsequently, the non-parametric Wilcoxon-Mann-Whitney test was carried out for unpaired data, since the variables were not distributed normally. All tests with a p-value <0.05 were considered significant.
RESULTS
The sample consisted of 82 diabetic subjects, of whom 58 (70.7%) had a diagnosis of DMT1, while 24 (29.3%) had a diagnosis of DMT2.
The subjects included in the study had a variable age. The mean age was 37.5 years (95% CI: 34.1-40.9; SD=15.4). The study included the distribution of patients according to sex.
The analysis of the data showed greater participation in the completion of the questionnaire by females (47 subjects, equal to 57.3% of the sample) compared to males (35 subjects, equal to 42.7% of the sample). For the purposes of the study, patients were divided according to the type of glycaemic monitoring: SMBG and FGM. On analysing the data, it was observed, as is known, that the glycemic self-monitoring system using capillary puncture is the most widespread system.
Of the 82 subjects who participated in the study, 51 subjects used the SMBG system (62.2%) and 31 subjects (37.8%) used the FGM system. The different levels of satisfaction for the related types of monitoring were also analysed.
For the evaluation of the different levels of satisfaction, of a maximum score of 36 (sum of the maximum scores of each score), a score < 12 was considered as totally unsatisfactory, a score between 12 and 24 as partially satisfactory and finally a score between 24 and 36 as satisfactory. The scores obtained were categorised and analysed.
The results, extrapolated from the questions investigating objective data, were stratified according to gender and are reported in Table 1.

Table 1. Characteristics of 82 diabetic patients stratified by gender.
The effectiveness of diabetes treatment should not be assessed solely on the basis of HbA1c levels as it should also focus on patient-reported outcomes such as patient satisfaction, well-being and quality of life. The DTSQ was developed to assess patient satisfaction in the treatment of diabetes.
Table 2 shows the results obtained from the questionnaire.

Table 2. Summary of the percentages of responses obtained from the DTSQ questionnaire administered to 82 diabetic patients (the score for each field ranges from 1 to 6, where 1 means “very dissatisfied” and 6 means “very satisfied”).
Table 3 shows the results obtained from the DTSQ, stratified into three categories: “Satisfaction yes”, “Partial satisfaction”, “Satisfaction no”,
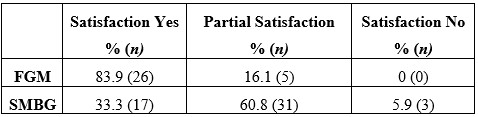
Table 3. Results obtained according to the evaluation criteria of the scale used (score < 12 = totally unsatisfactory, score between 12 and 24 = partially satisfactory, score between 24 and 36 = satisfactory).
Subjects with the FGM system show greater satisfaction than those using the SMBG system. Patients using Flash Glucose Monitoring showed 83.9% satisfaction, 16.1% partial satisfaction and 0% total dissatisfaction. Patients using capillary glucose self-monitoring, on the other hand, showed complete satisfaction for 33.3% of the sample (1 out of 3), partial satisfaction for the treatment equal to 60.8% and total dissatisfaction equal to 5.9% (Table 3).
The results obtained show that the FGM group had a dissatisfaction (satisfaction no) value of 0. The purpose of the study was to demonstrate a significant difference in satisfaction in the two different monitoring groups. The results obtained by the partially satisfied (partial satisfaction), considered as negative and not sufficient, were merged with those of the not satisfied (satisfaction no). Table 4 shows the new classification.

Table 4. Comparison between the results obtained for “satisfaction yes” and the combined results of “satisfaction no” and “partial satisfaction”
In Table 4 the results obtained for “partial satisfaction” were considered as negative values and therefore added to the values obtained for “satisfaction no”.
Table 4 shows a significant relationship between the groups and the satisfaction variable. In particular, the chi-squared test showed a significantly higher presence of satisfaction in the FGM group compared to the SMBG group (19.74, 83.9% vs 33.3%, chi-squared=19.74, p<0.0001). In other words, there is significantly greater treatment satisfaction in diabetic patients using the FGM monitoring system compared to the traditional method (SMBG). Differences in glycosylated haemoglobin were also analysed in the two patient groups. The mean glycosylated haemoglobin of the FGM group was 53.2 mmol/mol (95% CI: 49.0-57.4), while that of subjects with self-monitoring of capillary blood glucose was 60.3 mmol/mol (95% CI: 55.9-64.6).
For inferential analysis, the Wilcoxon-Mann-Whitney nonparametric test was used for two independent samples, as the data distributions were not normal. The different variables covered by the research were compared in relation to the monitoring system used by the patient (Table 5). Statistical analysis of both samples (SMBG and FGM) was performed. The samples were first analysed independently and then compared.

Table 5. Comparison between SMBG and FGM samples, regarding the different variables considered in our study, such as Satisfaction yes, HbA1c, Hyperglycaemia, Hypoglycaemia, tot DTSQ Satisfaction.
In the study sample, as seen in the descriptive statistical analysis, there was some difference between the glycosylated haemoglobins of the two groups. This comparison parameter was analysed using the Wilcoxon-Mann-Whitney test. The test showed that the difference is statistically significant, p-value= 0.029.
Another variable under study was the analysis of the frequency of perception of episodes of both
hypoglycaemia and hyperglycaemia. The frequencies of these perceptions were compared for the two classes of patients by performing an inferential analysis. With regard to the comparison of the perception of hypoglycaemic episodes, the test did not show a statistically significant difference, p-value = 0.22. The test also showed no statistically significant significance when comparing the perception of hyperglycaemic episodes, p-value = 0.30.
Finally, the degree of patient satisfaction in relation to the type of monitoring was investigated.
As seen above during the descriptive statistical analysis, there was a significant difference in satisfaction in the two groups. Statistical inference was performed to test whether the relationship between monitoring systems and satisfaction was statistically significant. The non-parametric Wilcoxon-Mann-Whitney test was chosen for two independent samples (p-value Shapiro-Wilk test = 0.024, so the distribution is not normal).
The test showed a statistically significant difference between the two groups (p-value < 0.0001).
DISCUSSION
Based on the material found in the international scientific literature, the results obtained from the study show a good match in measuring the satisfaction of diabetic patients with blood glucose monitoring. Flash glucose monitoring allows frequent glucose checks with increased time in range and reduced time in hyper- and hypoglycaemia [14]. The use of innovative tools, capable of providing greater patient comfort, is helpful in achieving better outcomes and better management of a chronic condition such as diabetes. The Impact study showed that FGM was able, in comparison to conventional systems, to increase the frequency of monitoring (up to 15 scans per day), reduce the time spent in hypoglycaemia and result in no increase in glycosylated haemoglobin at six months. FGM decreases hypoglycaemia in patients with DMT1 by an average of 74 minutes per day, with a 38% reduction compared to the control group in the 6 a.m. to 11 p.m. time slot and a 40% reduction in the time spent in hypoglycaemia in the 11 p.m. to 6 a.m. period [15].
A retrospective study, conducted in the US, and a meta-analysis, conducted in the US and Canada, showed that, with the use of the FGM system, glycosylated haemoglobin was significantly reduced in DMT2 [16].
The FGM system tends to improve treatment satisfaction, can lead to improved glycaemic control in patients with DMT2 undergoing multi-injection therapy, without increasing the frequency of hypoglycaemia [17], improving daily glycaemic control and self-care behaviour [18].
The research included the administration of the DTSQ in order to be able to analyse possible differences between the two monitoring groups and confirmed what has been stated by the various studies in the literature. The analysed sample is not representative of the entire population of diabetics as it comes from the online patient groups only, however, the patients belong to different settings as well as to different regions. In agreement with the findings in the literature, this research has shown that the use of the FGM system improves the quality of life and satisfaction of patients and promotes their well-being. The FGM system not only benefits the patient, who has greater awareness of glucose trends throughout the day, but also benefits the physician himself, who can better monitor diabetes compensation, hypoglycaemic and hyperglycaemic load in order to make the necessary changes to drug treatment [19]. Research has shown the benefits of using innovative monitoring systems.
This system is easy to wear and, with a painless scan, allows the measurement of glucose levels in the interstitial fluids of people with diabetes mellitus, even through clothing. Each scan shows both the current glucose value and the glucose data for the last 8 hours. A trend arrow helps the patient to assess the trend of blood sugar: whether it is increasing or decreasing and at what rate. These graphs allow adult patients and parents of children with diabetes to take all the necessary steps to avoid serious glycaemic imbalances. Indeed, the FGM system avoids repetitive fingertip pricks for blood glucose measurement, which cause pain, embarrassment and discomfort to the patient, and consequently allows more frequent glucose monitoring. This allows optimal management of the disease and its complications, helping to prevent, and thus reduce, episodes of hypoglycaemia and hyperglycaemia. In this regard, an additional variable was considered in the study, which involved analysing the frequency of perception of episodes of both hypoglycaemia and hyperglycaemia for the two classes of patients by performing an inferential analysis. However, the difference was not statistically significant. In addition to the limited sample size, this is due to the problems of perception of the problem and the type of data collected (self-reported).
The burden of caring for people with diabetes is considerable and the cost grows exponentially as co-morbidities increase, with hospitalisation being the main cost factor. The FGM system promotes the self-care of patients with diabetes mellitus and can help prevent acute disease-related events such as ketoacidosis and severe hypoglycaemia, thus reducing hospitalisations. Investing resources in new technologies, and thus in treatments and devices that reduce diabetes-related events, is a cost-effective strategy and thus amounts to reducing costs for the SSN (National Health Service).
The FGM system also fits well with the recent development of new digital technologies. Thanks to these advances, while on the one hand we have witnessed the increasing development of telecommunication, enabling the user to take advantage of health services through remote communication [20], on the other hand there have been significant advances in medical and technological studies, from the combination of which Telemedicine was born. It guarantees greater continuity of care, better quality of life and savings in terms of health expenditure. This enables simple and immediate doctor-patient communication, reducing outpatient visits as well as offering personalised and effective care management. Women treated with telemedicine feel better cared for through the continuous exchange of information between doctor and patient [21]. With the use of these new tools and technologies, the aim is to achieve a more sustainable management of diabetes and a more rational and modern approach to remotely managed care. Moreover, it should not be overlooked that the use of such systems allows the concept of patient empowerment to take hold, which is fundamental in the management of chronic diseases, as it enables the patient’s active participation in the treatment decision-making process.
CONCLUSIONS
The adoption of new technologies to detect blood glucose has benefits for the patient that positively influence quality of life. The improved control of the disease, linked to increased frequency of glucose monitoring, allows the reduction of glycosylated haemoglobin levels, thus achieving improved glycometabolic control. The study showed that there was a statistically significant difference in glycosylated haemoglobins between the two groups (FGM and SMGB). Glycosylated haemoglobin provides a good indication of the amount of glucose present in the blood over the past few months and is therefore a valid test for diagnosing and monitoring diabetes and, above all, diabetes management. The use of the FGM system, as confirmed by the study, allows the improvement of the quality of life of people with diabetes mellitus as well as better management of the disease. Reducing morbidity and mortality and improving the quality of life of people with diabetes mellitus is one of the current challenges for healthcare professionals.
LIMITATIONS OF THE STUDY
Although the study conducted confirmed what is already widely found in the literature, it is not without its limitations. The limitations of the study are related to the way the questionnaire was administered and the choice of sampling, which was carried out according to a non-probabilistic method that does not give all units of the population the same probability of being part of the sample. Indeed, convenience sampling was chosen for data collection. With convenience sampling, patients are not recruited randomly, so the resulting sample is subject to bias. Further limitations are represented by the sample size, which is especially useful to allow generalisation of the results, and the administration of the questionnaire to paediatric patients and young adults up to 18 years of age. For this class of patients, 8 were aged < 18 years (9.8 % of the sample), 3 were aged < 10 years (3.7 % of the sample). It is likely that the answer to the questionnaire was provided by the parent, who therefore has a system of perception of the problem that is not the patient’s own. A further study with a larger sample size would be needed to demonstrate the statistically significant reduction between perceptions of hypoglycaemic and hyperglycaemic episodes in subjects using the FGM system compared to those using the SMGB.
FUNDING
The authors did not receive any external funding to support this research.
AUTHORS’ CONTRIBUTION
All the authors contributed to the same extent to the realisation of the research.
CONFLICT OF INTEREST
The authors declare that they have no conflicts of interest.
LEGEND ACRONYMS AND ABBREVIATIONS
ADA = American Diabetes Association; DMT1 = Type 1 Diabetes Mellitus; DMT2 = Type 2 Diabetes Mellitus; DTSQ = Diabetes Treatment Satisfaction Questionnaire; FGM = Flash Glucose Monitoring; HbA1c = Glycosylated Hemoglobin; CI = Confidence Interval; IDF = International Diabetes Federation; IQR= Interquartile Scrap; SMBG = Self-monitoring of Blood Glucose; SSN = National Health Service
REFERENCES
- American Diabetes Association. Diagnosis and classification of diabetes mellitus. Diabetes Care 2014; 37(Suppl. 1): (S81–S90)2, 1993.
- Leslie RDG. Causes of diabetes. Genetic and environmental factors. Wiley & Sons, Chicester, 1993.
- Dianna J. Magliano, Edward J. Boyko. IDF Diabetes Atlas 10th edition scientific committee. Brussels: International Diabetes Federation; 2021.
- Gabriel A Gregory, Thomas I G Robinson, Sarah E Linklater, Fei Wang, Stephen Colagiuri, Carine de Beaufort et al. Global incidence, prevalence, and mortality of type 1 diabetes in 2021 with projection to 2040: a modelling study. Lancet Diabetes Endocrinol. 2022 Oct; 10(10):741-760.
- Lo Scalzo A, Abraha I, Bonomo MA, Chiarolla E, Migliore A, Paone S et al. Flash Continuous Glucose Monitoring Systems – Rapid HTA report for diabetes subjects in insulin therapy. Agenas: Rome, 2018.
- Fox C, Kilvert A. Il diabete di tipo 2. Tutte le risposte a portata di mano. Versione italiana a cura di Edoardo Mannucci e Caterina Lamanna. Ercules Comunicazioni, 2012.
- American Diabetes Association (ADA). Standards of Medical Care in Diabetes. Diabetes Care 2018; 41, Suppl. 1, 2018.
- Implication of Diabetes Control and Complication Trial. Diabetes Care, 2004.
- Wenqi Fan, Haipeng Pang, Zhiguo Xie, Gan Huang, and Zhiguang Zhou. Circular RNAs in diabetes mellitus and its complications. Front Endocrinol (Lausanne). 2022; 13: 885650.
- Mariarosaria De Luca, Michele Modestino, Olimpia Iacono, Anna De Simone, Vincenzo Guardasole, Angelo Foglia. Advanced hybrid closed-loop: review of the current systems available in Italy for the treatment of type 1 diabetes mellitus. JAMD 2022| VOL. 25 | N° 2: 121.
- Yaron M, Roitman E, Aharon-Hananel G, Landau Z, Ganz T, Yanuv I et al. Effect of Flash Glucose Monitoring Technology on Glycemic Control and Treatment Satisfaction in Patients With Type 2 Diabetes. Diabetes Care. 2019 Apr 29.
- Nicolucci A, R Giorgino, D Cucinotta, G Zoppini, M Muggeo, S Squatrito et al. Validation of the Italian version of the WHO-Well-Being Questionnaire (WHO-WBQ) and the WHO-Diabetes Treatment Satisfaction Questionnaire (WHO-DTSQ). Diabetes Nutr Metab. 2004 Aug;17 (4):235-43.
- Nicolucci A. L’uso dei questionari sulla qualità della vita. G It Diabetol Metab ,2006.
- Timothy C Dunn, Yongjin Xu , Gary Hayter , Ramzi A Ajjan. Real-world flash glucose monitoring patterns and associations between self-monitoring frequency and glycaemic measures: A European analysis of over 60 million glucose tests. Diabetes Res Clin Pract. 2018 Mar;137:37-46.
- Bolinder J, Antuna R, Geelhoed-Duijvestijn P, Kroger J, Weitgasser R. Novel glucose-sensing technology and hypoglycaemia in type 1 diabetes: a multicentre, non-masked, randomised controlled trial. Lancet, 2016.
- Anders L Carlson, Timothy Dilon Daniel, Andrea DeSantis, Serge Jabbour, Esra Karslioglu French , Davida Kruger et al. Flash glucose monitoring in type 2 diabetes managed with basal insulin in the USA: a retrospective real-world chart review study and meta-analysis. BMJ Open diabetes Res Care. 2022 Jan; 10(1):e002590.
- Marianna Yaron, Eytan Roitman, Genya Aharon-Hananel, Zohar Landau, Tali Ganz, Ilan Yanuv et al. Effect of Flash Glucose Monitoring Technology on Glycemic Control and Treatment Satisfaction in Patients With Type 2 Diabetes. ADA Volume 42,Issue 7, 2019 July.
- Reng-Na Yan, Ting-Ting Cai1, Lan-Lan Jiang 1, Ting Jing 1, Ling Cai , Xiao-Jing Xie et al. Real-Time Flash Glucose Monitoring Had Better Effects on Daily Glycemic Control Compared With Retrospective Flash Glucose Monitoring in Patients With Type 2 Diabetes on Premix Insulin Therapy. Front Endocrinol (Lausanne).2022 Feb 10;13:832102.
- Concetta Irace, Sergio Di Molfetta. Il monitoraggio in continuo della glicemia: stato dell’arte. Aggiornamento in tema di tecnologie. Dicembre 2022| Vol 34.| N° 4.
- Michael J. Ackerman, Rosemarie Filart, Lawrence P. Burgess, Insup Lee, and Ronald K. Poropatich.Developing Next-Generation Telehealth Tools and Technologies: Patients, Systems, and Data Perspectives.Telemedicine and e-Health.Feb 2010.93 95.
- Ming W, Lucy H Mackillop, Andrew J Farmer, Lise Loerup, Katy Bartlett, Jonathan C Levy et al. Telemedicine Technologies for Diabetes in Pregnancy: A Systematic Review and Meta-Analysis J Med Internet Res 2016; 18 (11):e290.
![]() This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.