Arvida Bar1, Monalisa2*, Netha Damayantie3, Halimah4
1,2,3,4Department of Nursing, Health Polytecnic of Jambi, Indonesia
* Corresponding author: Monalisa, Jl. Dr. Tazar, Buluran Kenali, Kec. Telanaipura, Kota Jambi, Jambi 36361, Indonesia, Orcid: https://orcid.org/0000-0002-4879-3893
Email: monalisa.poltekkes@gmail.com
Phone: +62 821-8656-3003

Cite this article
ABSTRACT
Introduction. Music has been widely recognized for its effectiveness in controlling anxiety and pain. However, in particular groups such as children, the implementation may be challenging, especially regarding the type of music selection. The aim of the study is to evaluate the music therapy efficacy on pain and anxiety management in pediatric care to improve the management of pain and anxiety in the pediatric population.
Methods. This review was written according to the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) statement. In assessing the impact of music therapy as a method of pain and anxiety management in pediatric care, a database tracking was conducted for articles publicized between 2000 and 2022. The databases used including Sciencedirect, Cochrane library, PubMed, and Wiley online library. Articles were deemed if the study subjects ranged in age from 0 to 21 years old, the intervention was live or recorded music, and the study took place in an inpatient background.
Results. 1,129 publications were discovered. In final search of literature, there are 12 articles included in this review. There is consistent and consequential evidence that music may relieve pain and anxiety in hospitalized children before and during procedures. The type of music that is widely used is classical and traditional instrumental music. In addition, there were only two studies using nursery rhymes.
Conclusion. The patient’s preference in choosing music for children enables them to determine the appropriateness of therapy. Classical music can be the main choice in applying music therapy in reducing anxiety and pain in children.
Keywords: Pediatric; music; pain; anxiety; inpatient; nurse
INTRODUCTION
Extreme anxiety may harm a child’s physical and psychological health, cause adverse postoperative outcomes that hinder recuperation, rehabilitation and reduce a child’s alliance in self-care [1–3]. Hospitalized children may experience anxiety due to daily activities, recurring convulsions, loss of control, or loneliness [4–6]. According to the current study, compelling pain and anxiety management are critical to healing [7,8]. Untreated pain and anxiety may cause diverted recovery, extended hospitalization, impaired physical growth and development, faked personality, and a lifelong nervousness of medical providers and treatments to be inducted [6,9–12].
There are multiple hindrances to implementing sufficient management of child care. Many parents and healthcare providers fear the side effects of pain and anxiety remedies [13–16]. Since 1999, the U.S. pediatric mortality rate, ages 0 to 19, has nearly tripled due to illicit prescription opioids [18]. Due to the risks and harmful effects of sole reliance on pharmacological treatments, Governments and healthcare providers are striving for alternative non-pharmacological modalities for manipulating pain and anxiety, particularly in children [19].
Music, touch, and nurse-led distraction techniques are non-pharmacological therapies currently widely used in pediatric care [20]. This therapy is effective in helping reduce the dose and duration of pain and anxiety medications and improve pain and anxiety scores; thus, nurses can continue to maintain their autonomy [21,22]. Focusing on music therapy turns out that this therapy has the potential to reduce or even eliminate the need for pharmacological therapy (18). Music also impacts human emotional and physiological responses by diverting attention from the symptoms of pain and anxiety that arise (19). The theory best known as the mechanism of pain, Gate Control, posits that pain receptors collaborate to transmit pain signals to the brain [23]; thus, distractions such as music can block specific pain pathways and reduce the amount of pain felt. Music therapy sessions allow individuals to express their pain and anxiety in healthy ways, such as through improvised songs and playing instruments [24,25]. Music has been used in clinical settings such as general practice (medical and dental) and more specialized settings such as surgery and related medical professions (such as physiotherapy and speech therapy). It is essential to recognize differences between the clinical practice of music therapists, who are certified, and the use of music by lay practitioners, who are not explicitly trained or have some background in music psychology or clinical psychology [26,27].
Previous systematic reviews of randomized controlled trial studies concluded the excellent efficacy of music therapy for children in controlling pain and anxiety when facing medical procedures. However, these studies could have clearly shown the type of music and therapy delivery method, which is still a big question [28]. Another review study found that the evidence for the effectiveness of using music to reduce dental anxiety in children is inconclusive and of limited quality [27]. The present review study aims to assess the effect of music therapy on pain and anxiety management in pediatric care to improve pain and anxiety management in the pediatric population from existing literature published from 2000 to 2022. The time-lapse choosen to updating studies in previous review. Review question including what types of music most used? What method used to deliver the music?
METHODS
Review Protocol
Following the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) 2020 guidelines, we conducted a systematic review of the literature consisting of Randomized Controlled Trials (RCTs) that apprised the effectiveness of music therapy in alleviating pain and anxiety in pediatric care [29].
Eligibility Criteria
We removed duplicates and uploaded articles to the web-based bibliography and database manager. It was then distributed to the team members, and a single reviewer initially reviewed the title and abstract. The following step was a full-text review by two reviewers. Additional reviewers were organized to deal with contentions to reach a consensus. The inclusion criteria include subjects ranged in age from 0 to 21, using live or recorded music in a hospital setting, effective or ineffective in alleviating pain and anxiety, and the full text was available in English. Articles are excluded if located in an outpatient setting, such as an emergency department or venipuncture clinic; music therapy by a music therapist; in labour or involving pregnant adolescents; during surgery or under general anaesthesia, or occurs in the neonatal intensive care unit (NICU) or pediatric intensive care unit (PICU). Babies treated in the NICU must be excluded because premature babies’ nervous systems are immature, so they respond to pain differently from full-term babies. Although not all babies treated in the NICU are premature, several articles do not always distinguish between premature and full-term babies born in the NICU. Theses or dissertations, conference articles, comments, editorial reports, and poster presentations are exempt.

Table 1. PICOS statement
Information source
A medical librarian searched a database for articles published in the previous ten years, from 2000 to 2022, in May 2022. Sciencedirect, Cochrane library, PubMed, and Wiley online library were all searched.
Search Strategy
PubMed, Sciencedirect, Wiley Online Library, and the Cochrane Library were among the databases searched. Furthermore, we also search on the list of references in the article that meet the criteria to broaden the search results further. In creating a comprehensive search strategy for each database, the following search terms were used: (1) pediatric, child, adolescent, infant, infant, toddler, adolescent, adolescent, male, female, (2) pain, tone, voice (3) anxiety (4) hospitalization, hospitalization, procedure, postoperative, surgery. A review of all included study references was also conducted. We also add filters to each database, including publication type and research design.

Table 2. Search String
Data Collection
Two authors independently screened the title and abstract to suit the inclusion criteria, if it was not clear, then they continued by reading the main text. No automation tools were used in selection literatures.
Data Extraction
To extract the required data, we followed the McMaster Critical Review Form-Quantitative Studies v. 2.0 and added some information that we think is important. The data we extracted included authors, countries, outcomes, study designs, participants, interventions, evaluation methods, and main findings. Two authors performed data extraction independently. The finalization of the extraction process was read and endorsed by the first author.
Quality of the Study
Study quality was assessed by two authors independently using the Critical Appraisal Skills Program (CASP) for the Randomized Controlled Trial [30]. This tool consists of 11 questions which are divided into four sections with the choices of Yes, No, and Can’t Tell checklist columns. We categorize the quality of studies into High, Medium, and Low. High quality studies if you have answers YES 10 – 11/11, medium quality if you have answers YES 7 – 9/11, and Low quality if answers YES ≤6/11.
Study Risk of Bias Assessment
The risk of bias or validity in the process and results of a systematic review is reflected in its methodological quality. The Cochrane Handbook 5.2.0 was used to reckon methodological quality. Two authors independently assessed the risk of bias in the included studies. In the circumstance of a disagreement, refer it to the corresponding author for arbitration. The Cochrane bias risk assessment tool was used to evaluate the risk of RCTs, which possessed random sequence generation, allocation concealment, blinding of subjects and researchers, blinding of outcome assessment, insufficient outcome data, and selective reporting.
RESULTS
Study Selection
A systematic electronic search identified that 1,129 publications were discovered through backward searching of relevant papers. The full-text screening was conducted on 783 articles. A total of 692 articles failed to meet eligibility criteria at the full-text screening stage, and only 12 articles were finally eligible for further analysis. The search results follow the PRISMA 2020 flow diagram (Fig. 1).
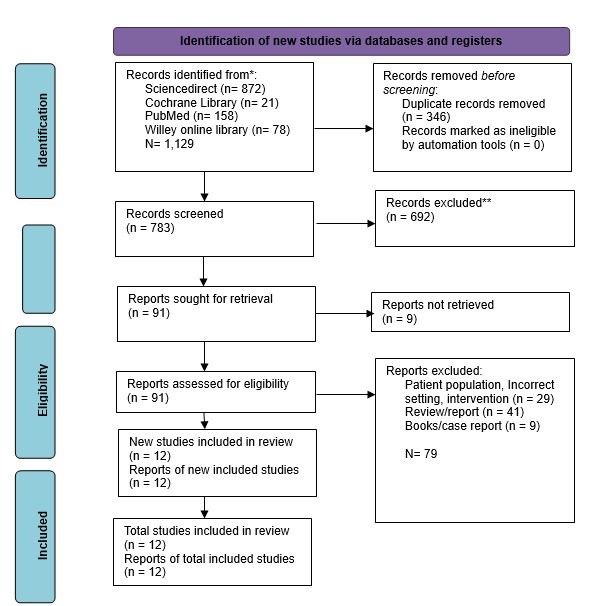
Figure 1. PRISMA flow diagram for literature search


Table 3. Characteristics of studies included.
Study Characteristics
Eleven randomized controlled trials (RCTs) and one quasi-experimental study met the inclusion criteria and was analyzed. The studies included 543 participants ranging in age from seven days to 18 years. The research was conducted in eight countries: India (8.33%, n=1) [31], Brazil (8.33%, n=1) [32], Iran (16.67%, n=2) [33,34], South Korea (8.33%, n=1) [35], the United Kingdom (UK) (8.33%, n=1) [36], Vietnam (8.33%, n=1) [37], the United States (US) (16.67%, n=2) [38,39], Turkey (8.33%, n=1) [25], and China (16.67%, n=2) [40,41].
Studies reported the implementation of music therapy before a procedure (n =5, 41.67%), during a procedure (n =4, 33.33%), after a procedure (n =6, 50%), or at any time during a hospitalization (n =2 16.67%), music-based interventions were used. The time spent listening to music ranged from 1 minute to at least 30 minutes. Most of the studies (n=7, 58.3%) used recorded music with headphones (n=7, 58.3%); one used speakers and ambient music.
The studies in the analysis scrutinized the effects of music-based interventions on pain (n=5, 41.67%) and anxiety (n=5, 41.67%). Some studies found a consequential lowering in pain scores in the music group (n=3), while others found no significant reduction (n=2). Before and during procedures, all studies conveyed a significant reduction in anxiety scores in the music group (n=5). Only one study discovered no significant lessening in anxiety scores in the music group following surgery.
Study quality
Based on the results of the study quality assessment which consisted of thirteen questions, only four studies were in the High Quality category, and eight other studies were in the Medium Quality category.

Table 4. Summary of quality assessment
Risk of Bias in Studies
Based on the bias assessment, all studies are in the low category in the Bias in measurement of the outcome domain. For overall bias, there are four studies that are in the Some Concerns category, and eight studies that are in the Low risk of bias category.

Figure 2. Traffic-light plot for RoB in individual study
Effect on Anxiety
There are eight studies [25,32,34,35,37,38,40] who analyzed the effect of music on pediatric anxiety in dealing with hospital care situations. The measurements of participants’ anxiety levels used a variety of instruments, including The Observational Scale of Behavioral Distress (OSBD), the modified Yale Preoperative Anxiety Scale (mYPAS), and The Spielberger State-Trait Anxiety Inventory (STAIC). Overall there was a significant decrease in anxiety in the studies that analyzed the effects of this music intervention.
Effect on Pain
There are nine studies [25,31,33,36–41] who analyzed the effect of music on the level of pain experienced by pediatricians. However, two studies showed insignificant results in reducing experienced pain [31,41]. The instruments used to measure pain include Wong-Baker Faces (WB-FACES), Visual Analog Scale (VAS), Numeric rating scale (NRS), and The Children’s Hospital of Eastern Ontario Pain Scale (CHEOPS).
DISCUSSION
Non-pharmacologic methods are widely used as forms of pain, fear, and vomiting control for children in the hospital setting. There are several medical procedures in the hospital that can provide an unpleasant experience, especially in Pediatric care. This review evaluated the impact of music therapy as a corroborative strategy for pain and anxiety control in hospitalized children. The publications’ central theme was statistically meaningful evidence that music can decline anxiety before and during procedures [32,34,35,37,38,40,41]. However, results concerning pain, often viewed as physiologic analogs to pain, were mixed [31,32,36–39,41]. Music-based interventions are also secure for hospitalized children, according to the evidence. Only one RCT reported any negative effects, deemed minor and mostly related to headphone affliction or no refinement in pain or anxiety scores [37].
It is crucial to explore patient factors that contributed to music interventions’ success in employing this review’s findings. Several studies have emphasized the importance of patient discretion in deciding on music for children [32,37,39,41]. Researchers have allowed two-year-olds to choose the type of music they want to listen to in several research studies [37,39,41]. According to one study, this sovereignty contributed to lower pain and anxiety levels in music groups [37]. In another study, subjects were reluctant to listen to researcher-selected music, resulting in significant sample loss [32]. It reflects a broader healthcare shift towards patient-centered care over the past decades, recognizing the importance of patient preferences in achieving positive health outcomes[24]. Music-based interventions deliver tangible ways for children to partake directly in care giving and manage challenging situations.
It is also important to regard the kit for implementing musical interventions. There is a high reliance on pre-recorded audio delivered through headphones. It exemplifies the viability and cost-effectiveness of music interventions in the hospital. The costs associated with the equipment needed to play music are relatively affordable, and several previous studies suggest that nurses may execute interventions without formal internship [32,35,37,39,41].
Music treatment is unassailable, affordable, and uncomplicated to learn, and hospital nurses can use it efficiently [42]. Music in nursing practice can be used unattended or in concurrence with other methods, such as jaw relaxation [43] and therapist guidance [44]; it can be used in a variety of sets, circumstances, and people for a miscellany of pursuits [43–47]. According to studies, 20-90 minutes of music therapy is an adequate remedy time. The following types of music were played: Sedative music [48], researcher-supplied music and subject-preferred music, smoothing music, and easy-listening music are all examples of sedative [46].
Music therapy may activate the natural analgesia in the human body that leads to alleviating pain, known as Endorphine [49]. Endorphine is a neuro hormone provoking pleasant sensations. The pain will be relieved along with parasympathetic system activation, which leads to the relaxation of the body. Aside from feel-good chemicals, nor-adrenaline and serotonin contribute enormously to pain relief via attenuated transmission of the brain’s descending impulse. The descending control system is a sensory neuron fiber that runs from the midbrain (precisely the peri-aqueductal gray matter) to the inter-neuronal inhibitory system [50–52]. The system will remain active in response to the stimulus of soft music, which inhibits the transmission of the pain stimulus. Music therapy has been shown to stimulate the axons or nerve fibers on the ascending tracts of RAS neurons (Reticular Activating System). The stimulus is transmitted to the cerebral cortex, limbic system, and corpus callosum through the autonomous nervous and neuro-endocrine systems. When one is immersed in soft music, the limbic system is aroused, causing it to secrete phenylethylamine (neuroamin), which controls impulse and mood emotion. Music stimulates the parasympathetic nervous system to work on the sympathetic nerves, causing the switch to alpha-type brain waves to yield soothing outcomes on the autonomic nervous system [53–55].
The physiological justification backs up the study’s finding that music therapy has a positive effect on reducing or relieving anxiety and pain in children. Nurses ought to employ a combination of pharmacologic and non-pharmacologic interventions to relieve pain and avoid the medication’s unwanted side effects [56]. It lays the hypothetical underpinnings for skillful or qualified nurses to gain new knowledge of other methods effective in relieving pain and anxiety, such as the use of music therapy, in health-care facilities. It echoes the assertion made by Huang, Good, and Zauszniewski [48] that music therapy is one of the interventional techniques that has concrete proof nursing theories to proficiently alleviate anxiety and pain.
Indeed although all considerations included in this integrator writing survey are of tall or great quality, it is conceivable that the comes about might have been impacted by pondering confinements. For case, a few ponder utilized a little test measure or did not incorporate a test estimate calculation. Test estimate was famous when evaluating the quality of each article. In expansion, most things did not dazzle the analysts, spectators, or members. Even though blinding in the investigation is critical to play down any conceivable inclination, it is troublesome to do so with music-based mediations, especially live music.
Two studies used an invalidated pain or anxiety scale in the study population, which was highlighted when appraising the precision of each article [37,41]. Because pain and anxiety are subjective, they are challenging to assess. Standardized pain and anxiety scales are used by providers to assess pain and anxiety, especially in nonverbal or nonresponsive patients. CHEOPS, FACES, FPS-R, NRS, and VAS pain scales were used in the studies. The m-YPAS and STAIC anxiety scales were used in the studies. While there are numerous pain and anxiety scales available, a validated and user-friendly pain or anxiety scale may not always be obtainable or ubiquitously used for the workforce being ascertained.
A wide age range of participants was used in multiple studies. From infancy to adolescence, children’s emotions, personalities, behavior, and speech will grow and develop. The way children react to stimuli like pain and anxiety will vary based on their developmental stage and age. Despite the fact that the studies only looked at children aged 0 to 18, the use of such a wide age range of individuals makes the reliability analysis of the findings questionable.
LIMITATION
In our search for full-text articles, we only collected 12 articles due to the limited access we faced, which prevented us from further exploring the magnitude of the effect of music therapy on pain and anxiety in children in the form of a meta-analysis. Some of the studies we include are also in the Some Concern category, so using the results of this study requires caution. However, we believe that nurses can apply music therapy autonomously in managing pain and anxiety in children as a form of nursing implementation and improving the quality of care.
CONCLUSION
For children in the hospital, pain, and anxiety often come to them in various incredibly invasive medical procedures. Music therapy can be the first choice for nurses to offer children with minimal side effects and is friendly to children’s conditions. Physiologically, music therapy can trigger natural analgesics in the body through neurohormones that have a calming effect. Based on studies that apply music therapy, the type of music generally used in classical music is delivered through headphones. Future studies can further examine how music therapy influences chronic pain conditions in children.
Conflict of Interests
There is no conflict of interest.
Ethical Approval
Ethics approval Ethical approval will not be required because this study will retrieve and synthesize data from already published studies.
Acknowledgments
We would like to express our gratitude to all parties, particularly the director of Health Polytechnic of Jambi.
Author’s Contribution
All authors equally contributed to preparing this article.
Funding/Support
This research did not receive any specific grant from funding agencies in the public, commercial, or not for profit sectors.
REFERENCES
- van der Heijden MJE, Jeekel J, Rode H, Cox S, van Rosmalen J, Hunink MGM, et al. Can live music therapy reduce distress and pain in children with burns after wound care procedures? A randomized controlled trial. Burns. 2018;44(4):823–33.
- Anggerainy SW, Wanda D, Nurhaeni N. Music therapy and story telling: Nursing interventions to improve sleep in hospitalized children. Comprehensive child and adolescent nursing. 2019;42(sup1):82–9.
- Zhu X, Haegele JA, Healy S. Movement and mental health: Behavioral correlates of anxiety and depression among children of 6–17 years old in the US. Mental Health and Physical Activity. 2019;16:60–5.
- Gomes GLL, Fernandes M das GM, Nóbrega MML da. Hospitalization anxiety in children: conceptual analysis. Revista brasileira de enfermagem. 2016;69:940–5.
- Li WHC, Chung JOK, Ho KY, Kwok BMC. Play interventions to reduce anxiety and negative emotions in hospitalized children. BMC pediatrics. 2016;16(1):1–9.
- Delvecchio E, Salcuni S, Lis A, Germani A, Di Riso D. Hospitalized children: anxiety, coping strategies, and pretend play. Frontiers in public health. 2019;7:250.
- Gogoularadja A, Bakshi SS. A Randomized study on the efficacy of music therapy on pain and anxiety in nasal septal surgery. International Archives of Otorhinolaryngology. 2020;24:232–6.
- Cırık V, Efe E. THE EFFECT OF MUSIC THERAPY IN CHILDREN’S HEALTH. Journal of Educational & Instructional Studies in the World. 2018;8(2).
- Chow CHT, Van Lieshout RJ, Schmidt LA, Dobson KG, Buckley N. Systematic review: audiovisual interventions for reducing preoperative anxiety in children undergoing elective surgery. Journal of pediatric psychology. 2016;41(2):182–203.
- Lerwick JL. Minimizing pediatric healthcare-induced anxiety and trauma. World journal of clinical pediatrics. 2016;5(2):143.
- Fronk E, Billick SB. Pre-operative anxiety in pediatric surgery patients: Multiple case study analysis with literature review. Psychiatric Quarterly. 2020;91(4):1439–51.
- Johnson AA, Berry A, Bradley M, Daniell JA, Lugo C, Schaum-Comegys K, et al. Examining the effects of music-based interventions on pain and anxiety in hospitalized children: An integrative review. Journal of Pediatric Nursing. 2021;60:71–6.
- Bawa M, Mahajan JK, Aggerwal N, Sundaram J, Rao KLN. Barriers to pediatric pain management in children undergoing surgery: A survey of health care providers. Journal of Pain & Palliative Care Pharmacotherapy. 2015;29(4):353–8.
- Katende G, Mugabi B. Comforting strategies and perceived barriers to pediatric pain management during IV line insertion procedure in Uganda’s national referral hospital: A descriptive study. BMC pediatrics. 2015;15(1):1–8.
- Greenfield K, Carter B, Harrop E, Jassal S, Bayliss MJ, Renton K, et al. Healthcare professionals’ experiences of the barriers and facilitators to pediatric pain management in the community at end-of-life: a qualitative interview study. Journal of Pain and Symptom Management. 2022;63(1):98–105.
- Sabeti F, Mohammadpour M, Pouraboli B, Tahmasebi M, Hasanpour M. Health Care Providers’ experiences of the non-pharmacological pain and anxiety management and its barriers in the Pediatric Intensive Care Units. Journal of Pediatric Nursing. 2021;60:e110–6.
- Rudd RA, Aleshire N, Zibbell JE, Gladden RM. Increases in drug and opioid overdose deaths—United States, 2000–2014. Morbidity and mortality weekly report. 2016;64(50 & 51):1378–82.
- Gaither JR, Shabanova V, Leventhal JM. US national trends in pediatric deaths from prescription and illicit opioids, 1999-2016. JAMA network open. 2018;1(8):e186558–e186558.
- Bizzio R, Cianelli R, Villegas N, Hooshmand M, Robinson M, Hires KA, et al. Exploring non-pharmacological management among anesthesia providers to reduce preoperative distress in children. Journal of pediatric nursing. 2020;50:105–12.
- Giordano F, Zanchi B, De Leonardis F, Rutigliano C, Esposito F, Brienza N, et al. The influence of music therapy on preoperative anxiety in pediatric oncology patients undergoing invasive procedures. The Arts in Psychotherapy. 2020;68:101649.
- Uggla L, Bonde L, Hammar U, Wrangsjö B, Gustafsson B. Music therapy supported the health‐related quality of life for children undergoing haematopoietic stem cell transplants. Acta paediatrica. 2018;107(11):1986–94.
- Mondanaro JF, Sara GA, Thachil R, Pranjić M, Rossetti A, Sim GE, et al. The effects of clinical music therapy on resiliency in adults undergoing infusion: a randomized, controlled trial. Journal of Pain and Symptom Management. 2021;61(6):1099–108.
- Melzack R, Wall PD. Pain Mechanisms: A New Theory: A gate control system modulates sensory input from the skin before it evokes pain perception and response. Science. 1965;150(3699):971–9.
- Finnerty R. Music therapy as an intervention for pain perception. Anglia Ruskin University, Cambridge, England. 2006;
- Bulut M, Alemdar DK, Bulut A, Şalcı G. The effect of music therapy, hand massage, and kaleidoscope usage on postoperative nausea and vomiting, pain, fear, and stress in children: A randomized controlled trial. Journal of Perianesthesia Nursing. 2020;35(6):649–57.
- Stegemann M. therapy and other music-based interventions in pediatric health care: An overview. Medicines;
- Ainscough SL, Windsor L, Tahmassebi JF. A review of the effect of music on dental anxiety in children. European Archives of Paediatric Dentistry. 2019;20(1):23–6.
- Klassen JA, Liang Y, Tjosvold L, Klassen TP, Hartling L. Music for pain and anxiety in children undergoing medical procedures: a systematic review of randomized controlled trials. Ambulatory pediatrics. 2008;8(2):117–28.
- Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. International Journal of Surgery. 2021;88:105906.
- Programme CAS. CASP randomised controlled trial checklist. 2018.
- Balan R, Bavdekar SB, Jadhav S. Can Indian classical instrumental music reduce pain felt during venepuncture? The Indian Journal of Pediatrics. 2009;76(5):469–73.
- Franzoi MAH, Goulart CB, Lara EO, Martins G. Music listening for anxiety relief in children in the preoperative period: a randomized clinical trial. Revista latino-americana de enfermagem. 2016;24.
- Sabzevari A, Kianifar H, Jafari SA, Saeidi M, Ahanchian H, Kiani MA, et al. The effect of music on pain and vital signs of children before and after endoscopy. Electronic physician. 2017;9(7):4801.
- Kazemi S, Ghazimoghaddam K, Besharat S, Kashani L. Music and anxiety in hospitalized children. Journal of Clinical and Diagnostic Research. 2012;6(1):94–6.
- Kim SJ, Oh YJ, Kim KJ, Kwak Y-L, Na S. The effect of recorded maternal voice on perioperative anxiety and emergence in children. Anaesthesia and intensive care. 2010;38(6):1064–9.
- Longhi E, Pickett N, Hargreaves DJ. Wellbeing and hospitalized children: can music help? Psychology of music. 2015;43(2):188–96.
- Nguyen TN, Nilsson S, Hellström A-L, Bengtson A. Music therapy to reduce pain and anxiety in children with cancer undergoing lumbar puncture: a randomized clinical trial. Journal of Pediatric Oncology Nursing. 2010;27(3):146–55.
- Noguchi LK. The effect of music versus nonmusic on behavioral signs of distress and self-report of pain in pediatric injection patients. Journal of Music Therapy. 2006;43(1):16–38.
- Suresh S, De Oliveira GS, Suresh S. The effect of audio therapy to treat postoperative pain in children undergoing major surgery: a randomized controlled trial. Pediatric Surgery International. 2015;31(2):197–201.
- Liu Y, Petrini MA. Effects of music therapy on pain, anxiety, and vital signs in patients after thoracic surgery. Complementary therapies in medicine. 2015;23(5):714–8.
- Yu H, Liu Y, Li S, Ma X. Effects of music on anxiety and pain in children with cerebral palsy receiving acupuncture: A randomized controlled trial. International Journal of Nursing Studies. 2009;46(11):1423–30.
- Wang C-F, Sun Y-L, Zang H-X. Music therapy improves sleep quality in acute and chronic sleep disorders: A meta-analysis of 10 randomized studies. International journal of nursing studies. 2014;51(1):51–62.
- Good M, Anderson GC, Ahn S, Cong X, Stanton‐Hicks M. Relaxation and music reduce pain following intestinal surgery. Research in nursing & health. 2005;28(3):240–51.
- Gutgsell KJ, Schluchter M, Margevicius S, DeGolia PA, McLaughlin B, Harris M, et al. Music therapy reduces pain in palliative care patients: a randomized controlled trial. Journal of pain and symptom management. 2013;45(5):822–31.
- Chaput-McGovern J, Silverman MJ. Effects of music therapy with patients on a post-surgical oncology unit: A pilot study determining maintenance of immediate gains. The Arts in Psychotherapy. 2012;39(5):417–22.
- Allred KD, Byers JF, Sole M Lou. The effect of music on postoperative pain and anxiety. Pain Management Nursing. 2010;11(1):15–25.
- Wurjatmiko AT. The effects of music therapy intervention on the pain and anxiety levels of cancer patient: A systematic review. International Journal of Nursing Education. 2019;11(4):14–8.
- Huang S-T, Good M, Zauszniewski JA. The effectiveness of music in relieving pain in cancer patients: a randomized controlled trial. International journal of nursing studies. 2010;47(11):1354–62.
- Aktaş YY, Karabulut N. The use of cold therapy, music therapy and lidocaine spray for reducing pain and anxiety following chest tube removal. Complementary therapies in clinical practice. 2019;34:179–84.
- Cowen R, Stasiowska MK, Laycock H, Bantel C. Assessing pain objectively: the use of physiological markers. Anaesthesia. 2015;70(7):828–47.
- McInnis PM, Braund TA, Chua ZK, Kozlowska K. Stress-system activation in children with chronic pain: a focus for clinical intervention. Clinical Child Psychology and Psychiatry. 2020;25(1):78–97.
- Wei Y, Liang Y, Lin H, Dai Y, Yao S. Autonomic nervous system and inflammation interaction in endometriosis-associated pain. Journal of Neuroinflammation. 2020;17(1):1–24.
- Riganello F, Cortese MD, Arcuri F, Quintieri M, Dolce G. How can music influence the autonomic nervous system response in patients with severe disorder of consciousness? Frontiers in neuroscience. 2015;9:461.
- Akimoto K, Hu A, Yamaguchi T, Kobayashi H. Effect of 528 Hz music on the endocrine system and autonomic nervous system. Health. 2018;10(09):1159.
- Yamashita K, Kibe T, Ohno S, Kohjitani A, Sugimura M. The effects of music listening during extraction of the impacted mandibular third molar on the autonomic nervous system and psychological state. Journal of Oral and Maxillofacial Surgery. 2019;77(6):1153-e1.
- Yaban ZS. Usage of non-pharmacologic methods on postoperative pain management by nurses: Sample of turkey. International Journal of Caring Sciences. 2019;12(1):529–41.
![]() This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.