
Technological innovations in cardiac electrostimulation: Professional updating and cultural evolution of nurses
Carlo Uran1, Pasquale Piscitelli2, Mariuccia falco3, Giovanna Bombace3, Palma Eterno3
1 Interventional cardiologist. Cardiology and Intensive Care Unit, “San Giuseppe e Melorio” Hospital, Santa Maria Capua Vetere, Italy
2 Registered nurse. Cardiology and Intensive Care Unit, “San Giuseppe e Melorio” Hospital, Santa Maria Capua Vetere, Italy
3 Graduate nurse. Cardiology and Intensive Care Unit, “San Giuseppe e Melorio” Hospital, Santa Maria Capua Vetere, Italy
Corresponding author: Dr. Carlo. Uran, Cardiology and Intensive Care Unit, “San Giuseppe e Melorio” Hospital, Santa Maria Capua Vetere, Italy. Email: carlura@libero.it

Cita questo articolo
Abstract
Cardiology made enormous advances in the treatment of extremely severe diseases such as heart failure. Specifically, interventional cardiology has been enriched, over the years, with increasingly complex aids that have contributed in improving the quality of life and survival of patients suffering from this disease. These advances in technique compel the interventional cardiologist being constantly updated on new procedures and therapy. As a result, both the ward nurses and those supporting the cardiologist in the surgery room, must acquire the knowledge that allows them to be always in step with the fast-changing times.
The aim of this commentary is to underlining the importance of a continuous updating of nurses by emphasizing that their role has been changing over the years and that these professionals, along with the physicians, must stay up-to-date regarding technological innovations, within the limits of their specific skills.
Keywords: Heart failure; Cardiac Contractility Modulation; Nurse updating
Introduction
Nurses of interventional Cardiology unit must acquire more and more skills because of the evolution of technology and subsequently of the complexity of implantable devices. The acquisition of skills is a continuous process and requires constant effort. Therefore, not only the physician, who remains the main operator, must constantly update himself on new techniques and procedures, but also nurses who assist him in and out the operating room, must acquire the scientific mentality that allows them to get highly specialized technical knowledges. In the field of interventional cardiology, advances in technology made care approach increasingly complex, before, during and after an interventional procedure. In such a large and constantly evolving field, nurses should necessarily acquire all the skills for the assistance process and should consequently have the ability to analyze, decide and execute the most appropriate and safe care services, supported by solid evidence of effectiveness. Cardiac Contractility Modulation (CCM) therapy, delivered by OPTIMIZER SMART®, is part of the non-pharmacological therapy for treatment of heart failure with reduced or moderately reduced ejection fraction, in symptomatic patients (NYHA class II-IV) despite optimized medical therapy [1]. It is an important technological innovation for the treatment of this severe disease. The CCM acts by delivering a high-energy non-excitatory bipolar signal, synchronized with local electrical activity, in the ventricular absolute refractory period, by means of two active-fixation leads, placed on the IVS and spaced from each other by no more than 1 cm. Both leads can have a sensing and therapy delivery function. In the implantation phase, is very important to be meticulous in positioning the leads so that they have a sensing greater than 4 mV at the PSA. In the short and long term, this treatment increases left ventricular contractility. As result, the CCM therapy improves clinical status, functional capacity, quality of life and prevents hospital admissions of carefully selected patients [2]. The selection of the patient to whom implant this device, takes place by evaluating his quality of life and the frequency of hospitalizations for heart failure. Quality of life is assessed by the MLWHFQ questionnaire. A score over 30 in a patient in NYHA II class is indicative of severe lack of autonomy and is a significant element in the decision to implant such device (Fig. 1). The interventional procedure does not differ from those implemented for the implantation of other cardiac devices. The difference is about the periodic checking of the implanted device, performed by the cardiologist with the help of a biomedical engineer, who analyze the data by a portable computer loaded with a specific software, by which, electrical parameters and therapy delivery time are tested. The therapy delivery time must be at least 7 hours per day and a parameter to pay attention to is the percentage of therapy delivery, which must be as high as possible and not fall below 80%. [3].
Discussion
Many papers describe implantation procedure and the role of nurses [4-5-6]. After the surgery, nurse takes the patient back to the ward and performs an ECG. Nurses who record the ECG should be able to understand whether the device is properly working or not. The typical ECG of a patient implanted with a CCM device shows a ‘spike’ in the absolute refractory period of cardiac cycle: the ‘R wave’ of QRS complex. (Fig. 2). Nurses should know that the presence of a ‘spike’ on the ‘R wave’ of the QRS complex is not a non-capturing sign or a sensing defect: it is the proper operating of the device itself. This knowledge is important in order not to alarm the patient and inappropriately alert the cardiologist. The day after implantation, nurses should check the surgical wound, evaluate whether there is a hematoma or not and if medical attention is required. Then the patient can undergo to a chest x-ray to evaluate the position of the leads and to exclude a PNx, if the subclavian vein puncture has been performed without echo guide [7]. OPTIMIZER SMART® is powered by a weekly-rechargeable battery through an induction mini-charger, rechargeable itself, delivered to the patient. At bedside, physician and nurses instruct the patient, with the assistance of biomedical engineer, regarding its use. It is important, in this phase, that nurses as well assist the patient and reassure him about the easiness of device recharging procedure. Patient should charge the device battery weekly and it is advisable to suggest him to always recharging the device on the same day and at the same time, specifying however that it is not a life-saving device, but an electrical therapy provider. This avoids the worry of postponing or anticipating the charging process. Nurses get involved in many ways in interventional procedures: they manage the pre-operation care and technical setup; help the physician in the surgical room; check the correct functioning of the device and, if complications are detected, alert the physician and look for a quick solution to them. In order to perform these tasks, nurses should know how the device acts and which complications might occur after intervention, so they can be able to deal with them without any anxiety. In 2014 in order to assess critical care nurses' knowledge and practice regarding implantable cardiac devices in Egypt, was published a paper by which authors showed that Critical care nurses have inadequate knowledge and practice regarding implantable cardiac devices [8]. Unfortunately, things have not changed over the years. In 2017, in order to assess cardiology nurses' knowledge and confidence in providing education and support to ICD recipients, Steffes et al. published a paper. The result was surprising: authors proved that the ICD knowledge of US nurses in 2015 was similar to that reported in the United Kingdom in 2004 [9-10], with limited knowledge about the complexities of modern ICD devices. Such deficits in knowledge may affect the quality of education provided to ICD recipients in preparing them to live safely with an ICD. A survey published in 2021 by Fitzimons et al, showed that many nurses felt not being living up to their job and emphasize the importance of in continuing cardiovascular nursing education and of their professional updating[11]. Nowadays, the nurses should be a complete professional and should have the technical and care skills required to obtain the best result in interventional procedures, as regard the new generation devices as well. Consequently, the interventional cardiology/electrostimulation nurses are required to have not only care skills, but also the knowledge of devices. In CCM therapy, electrical stimulation is delivered to the cardiac muscle during the absolute refractory period. In this phase, the electrical signals activate the mobilization of calcium ions in the cardiomyocytes. The mechanism of action of the CCM can be summarizing as follows: CCM signals applied during the absolute refractory period cause an increase of cytosolic calcium during the systole, resulting in improving the cardiac contraction [12]. The mechanism of action explains the typical ECG of a patient with CCM and the nurses must be able to recognize it in order not urgently alert the doctor. This is the reason why nurses as well should know it. Furthermore, nurses have to be aware about the effects of such therapy. A few seconds after the delivery of the therapy, normalization of the activity of the proteins that are involved in regulation of intracellular calcium, occurs. After a few hours, there is a progressive normalization of the abnormal expression of fetal gene program, which is a characteristic of heart failure. Reverse remodeling has been demonstrated within 3 months, with reduction of mechanical and neuro-hormonal stress and increase of left ventricular ejection fraction. CCM restores the structure and function of damaged cells to their normal state [13]. Due to this action, CCM improves clinical outcomes in terms of exercise tolerance and QOL at 6 months [14], and this is the reason why guidelines published in 2016 and the Consensus HFA ESC 2019, state that CCM can be considering in selected patients with HF [15]. In 2020, Giallauria et al. evaluated the three currently available randomized controlled trials of CCM therapy for treatment for patients with heart failure. This comprehensive meta-analysis made the authors conclude that CCM provides statistically significant and clinically meaningful benefits in measures of functional capacity and HF-related quality of life [16]. The latest ESC guidelines on heart failure (2021) suspend the judgment on CCM ('under evaluation'), since its effect on the long-term mortality rates of patients with heart failure has not evaluated yet in a randomized controlled multicenter trial [17]. However, it is noteworthy that some preliminary studies showed that CCM improves clinical outcome in terms of exercise tolerance and QOL. Besides, it improves long-term survival, compared with the mortality predicted by the Sattle Heart Failure Model Score and reduces hospitalizations by 75%. [18]. Due to these considerations, we highlighted that the cardiology nurses have not an adequate preparation. Because of this, patient care inevitably suffers. This is the reason why we believe that it is mandatory for the nurse to be updated both about procedures and about devices. They should have adequate knowledge about the indications and the mechanism of action of devices. Furthermore, as regard the CCM, it is mandatory for the cardiology nurses, the knowledge of the typical ECG of a patient implanted with such device.
Acknowledgement
The authors warmly thank Serena Costanza Uran for her collaboration in the translation
Funding statement
This paper did not receive any specific grant from funding agencies in the public, commercial, or not for profit sectors.
Competing interest statement
There are no competing interests for this study.
Authors’ contribution
Dr. C. Uran: Investigation, conceptualization, resources, preparation and translation of the paper. Dr. M Falco; P. Piscitelli; Dr. G. Bombace; Dr. P. Eterno: Preparation
References
- https://www.fda.gov/media/123038/download;
- Abraham WT, Smith SA. Devices in the management of advanced, chronic heart failure. Nat Rev Cardiol. 2013;10(2):98-110.
- Abraham W.T et al. A Randomized Controlled Trial to Evaluate the Safety and Efficacy of Cardiac Contractility Modulation. J Am Coll Cardiol HF 2018;
- Kim Rajappan, Cardiac Department, John Radcliffe Hospital, Headley Way, Headington, Oxford OX3 9DU, UK; Education in Heart Arrhythmias. Permanent pacemaker implantation technique: part I; http://dx.doi.org/10.1136/hrt.2007.132753
- Rajappan K. Permanent pacemaker implantation technique: part II. Heart. 2009;95(4):334-342. doi:10.1136/hrt.2008.156372
- Porfili A. Protocollo infermieristico per procedure di elettrostimolazione: impianto o sostituzione di Pacemker, Defibrillatori, Dispositivi per la terapia di re sincronizzazione cardiaca (CTR) Linee guida AIAC 10.2018
- Glikson M, Nielsen JC, Kronborg MB, et al. 2021 ESC Guidelines on cardiac pacing and cardiac resynchronization therapy. Eur Heart J. 2021;42(35):3427-3520. doi:10.1093/eurheartj/ehab364
- Nahla Shaaban Ali; Warda Youssef; Abdo Mohamed; Ali Hussein Nurses' knowledge and practice regarding implantable cardiac devices in Egypt. British Journal of Cardiac Nursing 10, No. 1. Published Online:26 Dec 2014https://doi.org/10.12968/bjca.2015.10.1.34
- Steffes SS, Thompson EA, Bridges EM, Dougherty CM. Knowledge of Implantable Cardioverter Defibrillator Purpose and Function Among Nurses in the United States. J Cardiovasc Nurs. 2017;32(3):304-310. doi:10.1097/JCN.0000000000000339
- Tagney J. Can nurses in cardiology areas prepare patients for implantable cardioverter defibrillator implant and life at home? Nurs Crit Care. 2004;9(3):104Y114
- Donna Fitzsimons, Matthew A Carson, Tina B Hansen, Lis Neubeck, Mu’ath I Tanash, Loreena Hill, The varied role, scope of practice, and education of cardiovascular nurses in ESC-affiliated countries: an ACNAP survey, European Journal of Cardiovascular Nursing, Volume 20, Issue 6, August 2021, Pages 572–579, https://doi.org/10.1093/eurjcn/zvab027
- Borggrefe, M.; D. Burkhoff (Jul 2012). “Clinical effects of cardiac contractility modulation (CCM) as a treatment for chronic heart failure”. Eur J Heart Fail. 14 (7): 703–712.
- Butter, C.; et al. (May 2008). “Cardiac Contractility Modulation Electrical Signals Improve Myocardial Gene Expression in Patients With Heart Failure” (PDF). J Am Coll Cardiol. 51 (18):1784–1789.
- Kuschyk et al. Cardiac Contractility Modulation treatment in patients with symptomatic heart failure despite optimal medical therapy and cardiac resynchronization therapy (CRT) International Journal of Cardiology 277 (2019) 173-177 .
- Petar M. Seferovic et al ”Clinical practice update on heart failure 2019: pharmacotherapy, procedures, devices and patient management. An expert consensus meeting report of The Heart Failure Association of the European Society of Cardiology.
- Giallauria F, Cuomo G, Parlato A, Raval NY, Kuschyk J, Stewart Coats AJ. A comprehensive individual patient data meta-analysis of the effects of cardiac contractility modulation on functional capacity and heart failure-related quality of life. ESC Heart Fail. 2020;7(5):2922-2932.
- McDonagh TA, Metra M, Adamo M, et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure [published correction appears in Eur Heart J. 2021 Oct 14;:]. Eur Heart J. 2021;42(36):3599-3726.
- “MAGGIC” Heart Failure Risc Calculator according to Pocock et al. Predicting survival in heart failure: a risk score based on 39372 patients from 30 studies, Eur Heart J (2013) 34(19) 1404-1413.

Figure 1. The Minnesota questionnarie 21 items

Figure 2. ECG of a patient with a CRT-D system, implanted with the CCM device

Table of abbreviations
Sleep Quality Related to Vigilance Among Nurses in Hospital: A Cross Sectional Study
Debbie Nomiko1*, Ernawati1, Bettywaty Eliezer1
1Nursing Department, Health Polytechnic Ministry of Health Jambi, Indonesia
Corresponding author: Debbie Nomiko, dr. Tazar Street, BuluranKenali, Kec. Telanaipura, Kota Jambi, Jambi 36361, Indonesia, Orcid :https://orcid.org/0000-0002-3623-7937, Phone: +62 812-7897-981, Email: debbiedebbienomiko@gmail.com

Cita questo articolo
ABSTRACT
Introduction: Sleep quality disorders may cause a decrease in concentration and work performance of individual. It is also believed that nurses with work shifts as health workers may run into sleep quality disorders. Several researches have shown the relationship between sleep quality and the work performance of nurses in shifts duty. This study aimed to determine the relationship of sleep quality and vigilance of nurses in shifts duty in Raden Mattaher hospital Jambi.
Methods: A cross sectional study was performed recruiting 97 nurses working shifts in 3 inpatients wards of the Raden Mattaher Hospital Jambi. Socio-demographic details and data nurses alertness were collected using ad hoc questionnaires, data sleep quality were collected using the Pittsburgh Sleep Quality Index. Relationships among sleep patterns and alertness variables were investigated. Data were analyzed by univariate and chi-square test (CI 95%). Statistical analysis was performed using the SPSS version 16.0.
Results: Results showed an average of 29.4 years of age. Respondents were mostly female, married with working time <5 years. The results of the bivariate analysis show there was not relationship between sleep quality and vigilance of nurses who undergoing shifts in Raden Mattaher hospital Jambi with p-value 0.35.
Conclusion: There was not a relationship between sleep quality and vigilance among nurses undergoing a shift in patients' rooms
Keywords: Nurses, Sleep Quality, Wakefulness, Shift Work Schedule
INTRODUCTION
The prevalence of sleep quality disorders every year tends to increase, one of the causes is fatigue due to excessive work volume [1–4]. Poor sleep quality may cause adverse effects workers physical and psychological health leading to negative consequence workplace such as mistakes and reduced performances [5–8]. Health professionals have been known to experience fatigue at times. The condition has also long been associated with reduced patient safety [9,10]; decreased satisfaction, health and well-being [11–13]; more conflict among team members [14]; risk of needle stick injuries [14,15] and increased staff turnover [10]. Nurses, the largest group of healthcare providers, are prone to relatively high acute burnout, chronic fatigue, and recovery from fatigue after shift changes [16]. It is closely related to the demands they face throughout the working day, such as physical, mental, emotional demands and pressures associated with shift and non-standard work schedules. These factors place hospital nurses very vulnerable to burnout and its accompanying effects [17].
Nurses are professional workers who use a shift work system, so it can be ascertained that sleep quality disorders can also occur in nurses who undergo shifts [18–20]. Shift work has an impact on disturbances in circadian rhythms [21], and the main one being sleep pattern disturbances that cause sleep deprivation and fatigue [22,23].
Vigilance is degree of readiness of a person in responding to something [24] A person's level of vigilance is needed at work. Accidents occur as a result of decreased levels of alertness [25]. Variables that affect the level of alertness are monotonous state, level of sleepiness, psychophysiology, distraction, and work fatigue. In the variable of sleepiness level, there are 3 indicator variables, namely, circadian rhythm, sleep quality, and sleep time [26,27]. Research results show that 78% of nurses who work shifts experience changes in sleep quality. Furthermore, poor sleep quality is one of the contributing factors to medical errors that occur in health services [28–30]. The impact of poor sleep quality has been widely studied. Sleep absence is an important predictive factor influencing the occurrence of various chronic diseases such as hypertension [31] and cardiovascular disease [32], and diabetes [33]. Nurses' inconsistent sleep habits can have a severe impact on their health as well as their ability to do their jobs [34,35].
METHODS
Trial design
A cross-sectional study was made at the Raden Mattaher Hospital Jambi.
Participants
The population in this study was all shift nurses in 3 inpatient installations at Raden Mattaher Hospital Jambi with a total sample of 97 people with the criteria of nurses in the inpatient installation, not leave, having at least a minimum nursing diploma.
Intervention
A study questionnaire was made to collect socio-demographic details and a 24 items questionnaire was implemented to collect nurses’ alertness data. to four point scored Likert scales (always, often, sometimes and never) were used for the self-assessment of nurses’ alertness before, during and after care activities, with particular attention to missed cares, mistakes and documentation management. Nurses’ sleep quality was assessed using the Pittsburgh Sleep Quality Index (PSQI) tool [36]. Authors declare that the PSQI (Indonesian version) permission to use was obtained by the copyright property.
The PSQI is widely considered the gold standard tool for sleep patterns evaluation and quality of sleep assessment. It provides a global score ranged from 0 to 21 where scores higher than 5 means poor sleep quality. Furthermore, it provides 7 sub-scores assessing sleep patterns: subjective sleep quality, sleep latency, sleep duration, habitual sleep efficiency, sleep disturbances, use of sleeping medications, and daytime dysfunctions. The PSQI questionnaire was translated into Indonesian and
tested for reliability with Cronbachs alpha result of 0.753. Data were collected by three interviewers who were unknown to the participants before the study.
Blinding
In this study, 3 enumerators were used to collect research data. The previous enumerators did not know the participants because they were students who had been trained by the researcher before collecting data.
Ethical Consideration
Before carrying out data collection, the researcher first took care of ethical permission. The authors state that this study followed all ethical clearance processes and was approved by the health research ethics committee of Jambi Universitys Faculty of Medicine and Health Sciences.
Statistical methods
Data were presented as numbers or percentages for categorical variables. Continuous data are expressed as the mean ± standard deviation (SD), or median with Interquartile Range (IQR). The chi square test and Fisher's exact test were performed to evaluate significant differences of proportions or percentages between two groups. Particularly Fisher's exact test was used where the chi square test was not appropriate. All tests with p-value (p)<0.05 were considered significant. Statistical analysis was performed using the SPSS version 16.0 application.
RESULTS
Ninety-seven out of one hundred twenty-two nurses working shifts in 3 wards) qualified nurses
completed their studies. The results of this study presented in the table 1.
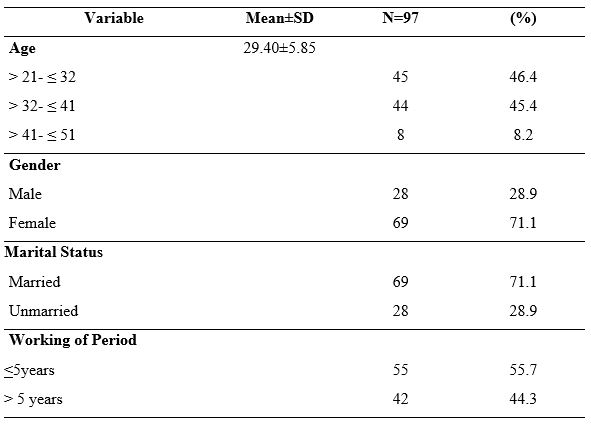
Table 1. Demographic Data of Nurses Undergoing Shift
Most of respondents were female (71.1%), married (71.1%) and have working of period < 5 years (55.7%). These results showed the average age of the respondents was 29.40 years, and the age range was between 21-51 years (SD 5.85).
Table 2 shows the results of the assessment of the seven components of the respondent's sleep quality, it was found that the component of the use of sleeping pills (using pills) had the highest score in terms of not using, namely 97.93%, the second highest score was the component of the subject's sleep quality, namely the subjective average of respondents stated 86.6% had good sleep quality. The results also showed that most of the respondents had sleep disturbances as much as 65%, and as many as 40% had sleep efficiency in the range of 75-84%.
That most nurses (86.6%) have good sleep quality based on subjective sleep quality. In the second component (sleep latency), most of the respondents (51.5%) had a sleep latency of 1-2 hours, and merely a small portion (7.2%) had a sleep latency of 5-6 hours.

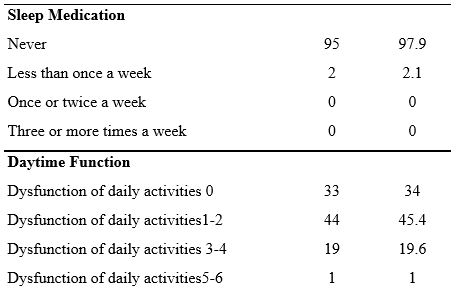
Table 2. Sleep Quality Components: Subjective and Objective Sleep Quality measures
In the third component (sleep duration), most of the respondents, as many as 32% of respondents, had sleep duration < 5 hours and only five respondents (5.2%) had sleep duration > 7 hours. Furthermore, 26.8% of the fourth component had a daily sleep efficiency > 85%, and only 14 respondents (14.4%) had a daily sleep efficiency of 14.4%. This result is slightly different from the previous study [49], which showed that 73.5% of nurses have sleep efficiency >85%.
Sleep quality in terms of sleep disturbance components shows that most of the respondents (67%) have sleep disorders with a score of 1-9, then for the use of sleeping pills, most of the respondents (97.93%) have never used sleeping pills at all.
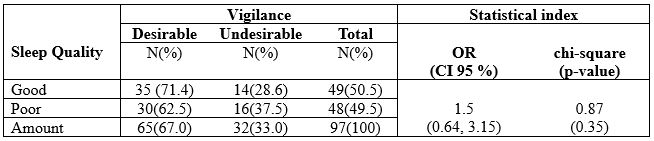
Table 3. The Correlation Between Sleep Quality and Vigilance Among Nurses undergoing Shift
The results of statistical tests obtained a p-value = 0.35, so it can be concluded that there was not a
significant relationship between sleep quality and vigilance among nurses who undergoing a shift in
the hospital.
DISCUSSION
Statistically it was found that in this study, there was no relationship between sleep quality and nurses' work alertness, although descriptively it can be reported that Nurses with good sleep quality tend to have good vigilance, and contrarily, nurses who have poor sleep quality tend to have less vigilance (see table 3). It significantly affects the productivity of nurses at work, where nurses in carrying out their work with good vigilance will work with good performance compared to nurses who are less alert.
Nurses who work night and rotating hours have been proven to have more trouble staying awake on duty and make twice as many mistakes as those who work day and evening shifts. More than 20% of workers in industrialized countries work shifts, and about 10% of them are diagnosed with sleep disorders [37]. Many factors affect sleep quality, one of which is shift work. Individuals who work shifts or shifts have difficulty adjusting to changing sleep schedules [6].
Poor sleep quality mainly occurs in nurses who use shift work systems. A study by Murphy et al., [38] found that shift work was significantly associated with poor sleep quality after controlling for variables of age, gender, and length of work.
This study also found almost the same proportion of respondents between respondents who had good and bad sleep quality, while most of the respondents had the desired of vigilance, which was around 67%. A systematic review study conducted by Dall’Ora et al. [39] found that shift characteristics are related to employee performance, and having sufficient rest time positively affects employee vigilance. Furthermore, Wahyuni [40] found a decrease in vigilance in night shift nurses with a proportion of decreased vigilance of 71.1%. However, statistically, it was not proven
to have a significant effect. The factor that influences the level of alertness before office hours is the
sleep quality. Lack of sleep results in a person's condition is less energetic and not enthusiastic [41].
We report that research data show that nurses predominately have a sleep latency of 1-2 hours, and only a small proportion (7.2%) have a sleep latency of 5-6 hours. Sleep latency is the length of sleep from start to fall asleep [42,43]. One of the factors that can affect sleep latency is bedtime habits that can disrupt a person's sleep and have an impact on increasing sleep latency [44].
This result is in line with the results of a previous study [45] that most respondents (60.3%) shift nurses experienced sleep disturbances less than once a week. Of all the sleep quality components, the sleep disturbance component had the highest mean of 1.44 with a standard deviation of 0.90 in a study of nurses undergoing shifts in Jordan [46].
Nurses’ poor sleep quality leads to a number of negative health outcomes. Nurses suffering from
poor sleep quality were more prone to develop burnout [47], depression and anxiety [48]. In addition, poor sleep could impair cognitive performance, such as concentration and memory, which may lead to poor work performance and even affect patients’ safety [49-51].
Effective measures, such as education on sleep hygiene [48], yoga [52] and cognitive-behavioral therapy for insomnia [53], should be considered to improve nurses’ sleep quality, quality of life, and patients’ safety.
CONCLUSION
The current study found that sleep quality was not a significant factor contributing to nurses' vigilance and medical error. Nevertheless, we still suggest that hospital managers should apply a 15-30 minute rest period during work shifts for nurses and pay attention to work rotation times, especially night shifts as a strategy to increase vigilance to prevent fatigue, sleepiness, and work errors.
LIMITATION OF STUDY
This study was only conducted in 3 hospital wards, so it cannot be compared with the same conditions in different hospitals. No intervention was carried out in this study to improve nurses' sleep quality and increase alertness while working. Other factors that influence Precautions, such as lighting conditions, environment, pills, caffeine, and other ingredients, were not studied.
Authors’ contribution
All authors equally contributed to preparing this article.
Acknowledgement
We express our gratitude to the director Director of Health Polytechnic, Ministry of Health Jambi, Indonesia for its support for the implementation of this research
Funding
This research received funding from the Development and Empowerment of Human Resources in Public Health (BPPSDMK) Indonesia
Conflict Of Interest
The authors declare that there was no conflict of interest in this research.
REFERENCES
- Deng X, Liu X, Fang R. Evaluation of the correlation between job stress and sleep quality in community nurses. Medicine. 2020;99(4).
- Boll J. Development of a Measure of Nurse Vigilance from the Patient’s Perspective: A Content Validity Study. 2014;
- Surani S, Hesselbacher S, Guntupalli B, Surani S, Subramanian S. Sleep quality and vigilance differ among inpatient nurses based on the unit setting and shift worked. Journal of patient safety. 2015;11(4):215–20.
- Kaliyaperumal D, Elango Y, Alagesan M, Santhanakrishanan I. Effects of sleep deprivation on the cognitive performance of nurses working in shift. Journal of clinical and diagnostic research: JCDR. 2017;11(8):CC01.
- Sayilan AA, Kulakaç N, Uzun S. Burnout levels and sleep quality of COVID-19 heroes. Perspect Psychiatr Care. 2020;57(3):1231–6.
- PA Potter AP. Fundamental Keperawatan. Jakarta: EGC; 2006.
- Tsai J-C, Chou K-R, Tsai H-T, Yen Y-C, Niu S-F. Effects of nocturnal sleep quality on diurnal cortisol profiles and attention in nurses: A cross-sectional study. Biological Research for Nursing. 2019;21(5):510–8.
- Di Muzio M, Diella G, Di Simone E, Pazzaglia M, Alfonsi V, Novelli L, et al. Comparison of Sleep and Attention Metrics Among Nurses Working Shifts on a Forward-vs Backward-Rotating Schedule. JAMA network open. 2021;4(10):e2129906–e2129906.
- Rainbow JG, Drake DA, Steege LM. Nurse health, work environment, presenteeism and patient safety. Western journal of nursing research. 2020;42(5):332–9.
- Smith-Miller CA, Shaw-Kokot J, Curro B, Jones CB. An integrative review. The journal of nursing administration. 2014;44(9):487–94.
- Asakura K, Asakura T, Satoh M, Watanabe I, Hara Y. Health indicators as moderators of occupational commitment and nurses’ intention to leave. Japan Journal of Nursing Science. 2020;17(1):e12277.
- Austin S, Fernet C, Trépanier S, Lavoie‐Tremblay M. Fatigue in new registered nurses: A 12‐month cross‐lagged analysis of its association with work motivation, engagement, sickness absence and turnover intention. Journal of nursing management. 2020;28(3):606–14.
- Bazazan A, Dianat I, Rastgoo L, Zandi H. Relationships between dimensions of fatigue and psychological distress among public hospital nurses. Health promotion perspectives. 2018;8(3):195.
- Han K, Trinkoff AM, Geiger-Brown J. Factors associated with work-related fatigue and recovery in hospital nurses working 12-hour shifts. Workplace health & safety. 2014;62(10):409–14.
- Fisman DN, Harris AD, Rubin M, Sorock GS, Mittleman MA. Fatigue increases the risk of injury from sharp devices in medical trainees results from a case-crossover study. Infection Control & Hospital Epidemiology. 2007;28(1):10–7.
- Barker LM, Nussbaum MA. Fatigue, performance and the work environment: a survey of registered nurses. Journal of advanced nursing. 2011;67(6):1370–82.
- Steege LM, Drake DA, Olivas M, Mazza G. Evaluation of physically and mentally fatiguing tasks and sources of fatigue as reported by registered nurses. Journal of Nursing Management. 2015;23(2):179–89.
- Reinke L, Özbay Y, Dieperink W, Tulleken JE. The effect of chronotype on sleepiness, fatigue, and psychomotor vigilance of ICU nurses during the night shift. Intensive care medicine. 2015;41(4):657–66.
- Geiger-Brown J, Rogers VE, Trinkoff AM, Kane RL, Bausell RB, Scharf SM. Sleep, sleepiness, fatigue, and performance of 12-hour-shift nurses. Chronobiology international. 2012;29(2):211–9.
- Ruggiero JS, Redeker NS, Fiedler N, Avi-Itzhak T, Fischetti N. Sleep and psychomotor vigilance in female shiftworkers. Biological research for nursing. 2012;14(3):225–35.
- Sun Q, Ji X, Zhou W, Liu J. Sleep problems in shift nurses: A brief review and recommendations at both individual and institutional levels. Journal of Nursing Management. 2019;27(1):10–8.
- Maurits LS, Widodo ID. Faktor dan Penjadualan Shift Kerja. Teknoin. 2008;13(2):18–22.
- Dong H, Zhang Q, Sun Z, Sang F, Xu Y. Sleep disturbances among Chinese clinical nurses in general hospitals and its influencing factors. BMC Psychiatry. 2017;17(1):1–9.
- Dorrian, J., Roach, Gregory.D., Fletcher, A., Dawson D. Simulated train driving: Fatigue, self awareness and cognitive disengagement. Applied Ergonomics. 2007;
- Desai A V., Haque MA. Vigilance monitoring for operator safety: A simulation study on highway driving. Journal of Safety Research. 2006;37(2):139–47.
- Zeng L-N, Yang Y, Wang C, Li X-H, Xiang Y-F, Hall BJ, et al. Prevalence of poor sleep quality in nursing staff: a meta-analysis of observational studies. Behavioral sleep medicine. 2020;18(6):746–59.
- Tu Z, He J, Zhou N. Sleep quality and mood symptoms in conscripted frontline nurse in Wuhan, China during COVID-19 outbreak: A cross-sectional study. Medicine. 2020;99(26).
- Arimura M, Imai M, Okawa M. Sleep, Mental Health and Errors in Nurses. Industrial health. 2010;48(6):811–7.
- Balas MC, Casey CM, Scott LD, Rogers AE. Maintain vigilance in the ICU. Nursing2020 Critical Care. 2007;2(4):38–44.
- Boughattas W, El Maalel O, Chikh R Ben, Maoua M, Houda K, Braham A, et al. Hospital night shift and its effects on the quality of sleep, the quality of life, and vigilance troubles among nurses. International Journal of Clinical Medicine. 2014;2014.
- Wang Y, Mei H, Jiang Y-R, Sun W-Q, Song Y-J, Liu S-J, et al. Relationship between duration of sleep and hypertension in adults: a meta-analysis. Journal of Clinical Sleep Medicine. 2015;11(9):1047–56.
- Cappuccio FP, Cooper D, D’Elia L, Strazzullo P, Miller MA. Sleep duration predicts cardiovascular outcomes: a systematic review and meta-analysis of prospective studies. European heart journal. 2011;32(12):1484–92.
- Alimoradi Z, Lin C-Y, Broström A, Bülow PH, Bajalan Z, Griffiths MD, et al. Internet addiction and sleep problems: A systematic review and meta-analysis. Sleep medicine reviews. 2019;47:51–61.
- Gómez-García T, Ruzafa-Martínez M, Fuentelsaz-Gallego C, Madrid JA, Rol MA, Martínez-Madrid MJ, et al. Nurses’ sleep quality, work environment and quality of care in the Spanish National Health System: observational study among different shifts. BMJ open. 2016;6(8):e012073.
- Kang J, Noh W, Lee Y. Sleep quality among shift-work nurses: A systematic review and meta-analysis. Applied nursing research. 2020;52:151227.
- Buysse DJ, Reynolds III CF, Monk TH, Berman SR, Kupfer DJ. The Pittsburgh Sleep Quality Index: a new instrument for psychiatric practice and research. Psychiatry research. 1989;28(2):193–213.
- Basent B. Shift-work sleep disorder. New England Journal of Medicine. 2005;353(5):519–21.
- Murphy R, Osterweil D, MscED CMD, Spivack BS, Zee PC. Improving Sleep Management in the Elderly. Citeseer; 2010.
- Dall’Ora C, Ball J, Recio-Saucedo A, Griffiths P. Characteristics of shift work and their impact on employee performance and wellbeing: A literature review. International journal of nursing studies. 2016;57:12–27.
- Wahyuni I, Dirdjo MM. Hubungan Kelebihan Waktu Kerja dengan Kelelahan Kerja dan Kinerja pada Perawat di Ruang Perawatan Intensif RSUD Abdul Wahab Sjahranie Samarinda. Borneo Student Research (BSR). 2020;1(3):1715–24.
- Budiawan W, Prastawa H, Kusumaningsari A, Sari DN. Pengaruh Monoton, Kualitas Tidur, Psikofisiologi, Distraksi, Dan Kelelahan Kerja Terhadap Tingkat Kewaspadaan. J@Ti Undip : Jurnal Teknik Industri. 2016;11(1).
- Rocha MCP da, Martino MMF De. Stress and sleep quality of nurses working different hospital shifts. Revista da Escola de Enfermagem da USP. 2010;44:280–6.
- Fietze I, Knoop K, Glos M, Holzhausen M, Peter JG, Penzel T. Effect of the first night shift period on sleep in young nurse students. European journal of applied physiology. 2009;107(6):707–14.
- Mubarok. Buku Ajar Kebutuhan Dasar Manusia : Teori & Aplikasi dalam Praktik. Jakarta: EGC; 2007.
- Safitrie A, Ardani MH. Studi Komparatif Kualitas Tidur Perawat Shift dan Non Shift di Unit Rawat Inap dan Unit Rawat Jalan. Prosiding Konferensi Nasional PPNI Jawa Tengah. 2013;17–23.
- Suleiman K, Al-Khaleeb T, Al-Kaladeh M, Sharour LA. The Effect of Shift Fluctuations on Sleep Quality among Nurses Working in the Emergency Room in Amman, Jordan. International Journal of Occupational Safety and Health. 2020;10(1):11–7.
- Giorgi, F., Mattei, A., Notarnicola, I., Petrucci, C., & Lancia, L. Can sleep quality and burnout affect the job performance of shift-work nurses? A hospital cross-sectional study. Journal of Advanced Nursing, 2018; 74, 698–708. doi:10.1111/jan.13484
- Baroni, A., Bruzzese, J. M., Di Bartolo, C. A., Ciarleglio, A., & Shatkin, J. P. Impact of a sleep course on sleep, mood and anxiety symptoms in college students: A pilot study. Journal of American College Health, 2018; 66, 41–50. doi:10.1080/07448481.2017.1369091
- Barbe, T., Kimble, L. P., & Rubenstein, C. Subjective cognitive complaints, psychosocial factors and nursing work function in nurses providing direct patient care. Journal of Advanced Nursing, 2018; 74, 914–925. doi:10.1111/ jan.13505
- Caruso, C. C. Negative impacts of shiftwork and long work hours. Rehabilitation Nursing, 2014; 39, 16–25. doi:10.1002/rnj.107
- Park, E., Lee, H. Y., & Park, C. S. Association between sleep quality and nurse productivity among Korean clinical nurses. Journal of Nursing Management. 2018; doi:10.1111/jonm.12634
- Fang, R., & Li, X. A regular yoga intervention for staff nurse sleep quality and work stress: A randomised controlled trial. Journal of Clinical Nursing, 2015; 24, 3374–3379. doi:10.1111/jocn.12983
- Kalmbach, D. A., Cheng, P., Arnedt, J. T., Anderson, J. R., Roth, T., Fellman-Couture, C., … Drake, C. L. Treating insomnia improves depression, maladaptive thinking, and hyperarousal in postmenopausal women: Comparing cognitive-behavioral therapy for insomnia (CBTI), sleep restriction therapy, and sleep hygiene education. Sleep Medicine, 2019; 55, 124–134. doi:10.1016/j.sleep.2018.11.019
![]() This work is licensed under a Creative Commons
This work is licensed under a Creative Commons
Attribution-NonCommercial-NoDerivatives 4.0 International License.
DEVELOPMENT AND EFFECTIVENESS OF AUGMENTED REALITY-BASED LEARNING FOR HEALTH SCIENCE STUDENTS: A SYSTEMATIC REVIEW
Lia Artika Sari1, Muhammad Rusdi2, Asrial2, Herlambang2
1 Doctorate student in Education MIPA Jambi University, Indonesia
2 Jambi University, Indonesia
Corresponding author: Lia Artika Sari Jl. Prof DR GA Siwabessy No.42, Buluran Kenali, Kec. Telanaipura, Kota Jambi, Jambi 36122, Indonesia, Tel: +6282196687959, Email: liaartikasari57@gmail.com, Orcid : https://orcid.org/0000-0002-5285-5356

Cita questo articolo
ABSTRACT
Background and Objective. The rapid development of technology makes it easier for teachers to continue to be interactively connected with students, for example, by using Augmented Reality technology. We conducted this review intending to investigate the diffusion and the effectiveness of AR technology as a learning media for students from various health fields.
Materials and Method. This systematic review was conducted using the Preferred Reporting Items for Systematic Reviews and Meta-Analyses Protocols) Checklist. We used some databases including PubMed, Google Scholar, Wiley Online Library, and Sciencedirect to search relevant literature with eligibility criteria, namely articles published in the period 201-2021, and discuss the development of Augmented Reality -based applications for learning students in the field of health
Results. The studies included are on the development of AR-based learning applications carried out to improve the clinical skills of health students (Medicine, Nursing, and Midwifery). Various types of application development are carried out including anatomy, Endotracheal Intubation, AR Prototype for Medical Surgery, Intravascular Neurosurgery, injection skills, and Laparoscopic.
Conclusion. The use of Augmented Reality as a learning medium really helps improve the understanding and skills of students majoring in health sciences.
Keywords: Development, Augmented Reality, Health-Science, Students
INTRODUCTION
The use of technology in the education of health science students has evolved over the years. These trends are mainly evolving in response to the challenges facing health education [1]. The use of simulation in health education has been applied in the last 50 years [2]. Augmented reality technology is an example of virtual reality technology developing rapidly in nursing education [3].
Augmented Reality (AR) technology refers to virtual elements to display the actual physical environment to create mixed-reality files in real-time. It complements and enhances the perceptions that humans acquire through their senses in the real world [4]. AR provides various levels of understanding and interaction, which can help students in e-learning activities [5]. For example, in an AR learning environment, motivational factors related to attention and learning satisfaction are rated higher than slide-based learning [6]. Today's development of smartphone technology makes AR technology more accessible to students and lecturers; for example, mobile learning (m-learning) using AR has become a trend [7].
Simulations using AR technology can replicate real-world aspects so that a safe learning environment is available for students where they can practice until the expected skill competencies are achieved [8]. Simulation has become an integral part of nursing curricula [9], which involves using patient simulators, trained people, real-life virtual environments, and role play [10].
Technological advances over time have increased the realism and authenticity of the simulated environment, leading to increased reactions, satisfaction, learning attitudes, cognitive and affective outcomes among health students in general [11].
Clinical health services have also used AR because it provides an internal picture of the patient, without the need for invasive procedures [12–15]. Medical students and professionals need more situational experience in clinical care, especially for patient safety, so this shows that there is a real need to continue developing the use of AR in health education.
The focus of studies on AR in recent years [16,17] has highlighted the belief that AR provides medical students with rich contextual learning to help achieve core competencies, such as decision making, work for effective teams, and creative adaptation of global resources to address local priorities [18], AR provides more authentic and engaging learning opportunities for various learning styles, providing students with a more personalized and exploratory learning experience [19]. The security of the patient will also be awake if an error occurs during skills training with AR [20].
Objective
This review was conducted to describe the development of AR technology as a learning medium for students from various health fields. This study is expected to be a reference material for teachers in learning strategies.
METHOD
Review Protocol
The research design is a Systematic Review, using the PRISMA-P 2009 (Preferred Reporting Items for Systematic Reviews and Meta-Analyses Protocols) Checklist.
Searching strategy
To search for literature using the PubMed database, Google Scholar, Wiley Online Library, and Sciencedirect using the keywords "Developing" AND "Augmented Reality" AND "Clinical practice" AND (Medical OR Nurse OR Midewifery) "College student".
We categorize the search into five categories that are considered to represent the topic of Augmented Reality development, namely AR typology, AR features and advantages, AR user perceptions, AR effectiveness in supporting learning, and AR design. Each category was analyzed to identify the best lessons, experiences, and evidence related to the design and development of AR.
Eligibility Criteria
The articles included in this review use the development method, with the subject of the trial being health students. In addition, the articles used are in English and full text, published in the period 2010–2020. Furthermore, the data obtained are then analyzed using quantitative descriptive methods and a narrative is produced that explains the study results.
The study results were documented to identify the effectiveness of using augmented reality in student health learning.
Study Type
The studies included in the criteria for this review are only limited to studies on the development
of Augmented Reality technology for student learning in the health sector. Articles entered are in English, full text, and is not a thesis or dissertation.
Type of Participant/Population Target
The participants used were health students (Medicine, Nursing, Midwifery) who did clinical practicum (Clinical Skill). There are no restrictions on age, gender, level/semester, as long as participants do clinical practicum learning (clinical skills).
Article Quality
Quality assessment was carried out on six journals that met the inclusion and exclusion criteria using the JBI Critical Appraisal Checklist criteria. Journals are good if they meet at least 80%, moderate if they meet 50–80% and weak if they meet less than 50% of the criteria. Articles are used in good to moderate categories for further data synthesis, namely, grouping similar extracted data according to the results to be measured to conclude.
RESULTS
Literature Identification and Selection
There were 319 articles identified from four databases (Pubmed, Google Scholar, ScienceDirect, and Wiley Online Library) relevant to the review topic, where the assessment or screening was based on the title and abstract of the articles obtained. 66 studies were removed because they were duplicate. After screening the title and abstract, 219 studies were removed due to irrelevant theme, not AR topic, and proceeding types. At the eligibility stage, 28 studies were not fit the inclusion criterias.
Critical Appraisal
Based on the JBI Critical Appraisal Checklist, six pieces of literature are in the excellent category, and two pieces of literature are in the weak category.
To maintain the quality of the literature studies made, this review only uses six good-quality journals, and then data extraction will be carried out (Figure 1).

Figure 1. PRISMA Flowchart: Strategy for Searching for Development of Augmented Reality in Educational Situations for Health-Science Students
After bearing the assessment, screening, and feasibility, the authors agreed to include six studies in this systematic review of the literature. Furthermore, the extraction of data from each of the included literature we describe in the following table displays the critical information needed with the theme of the study.
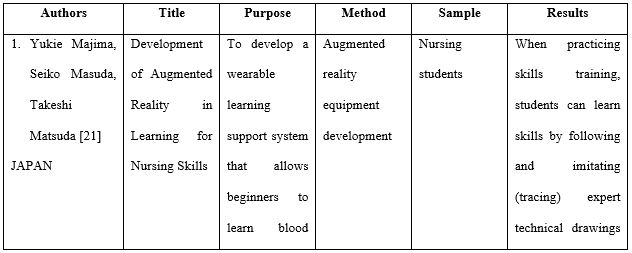
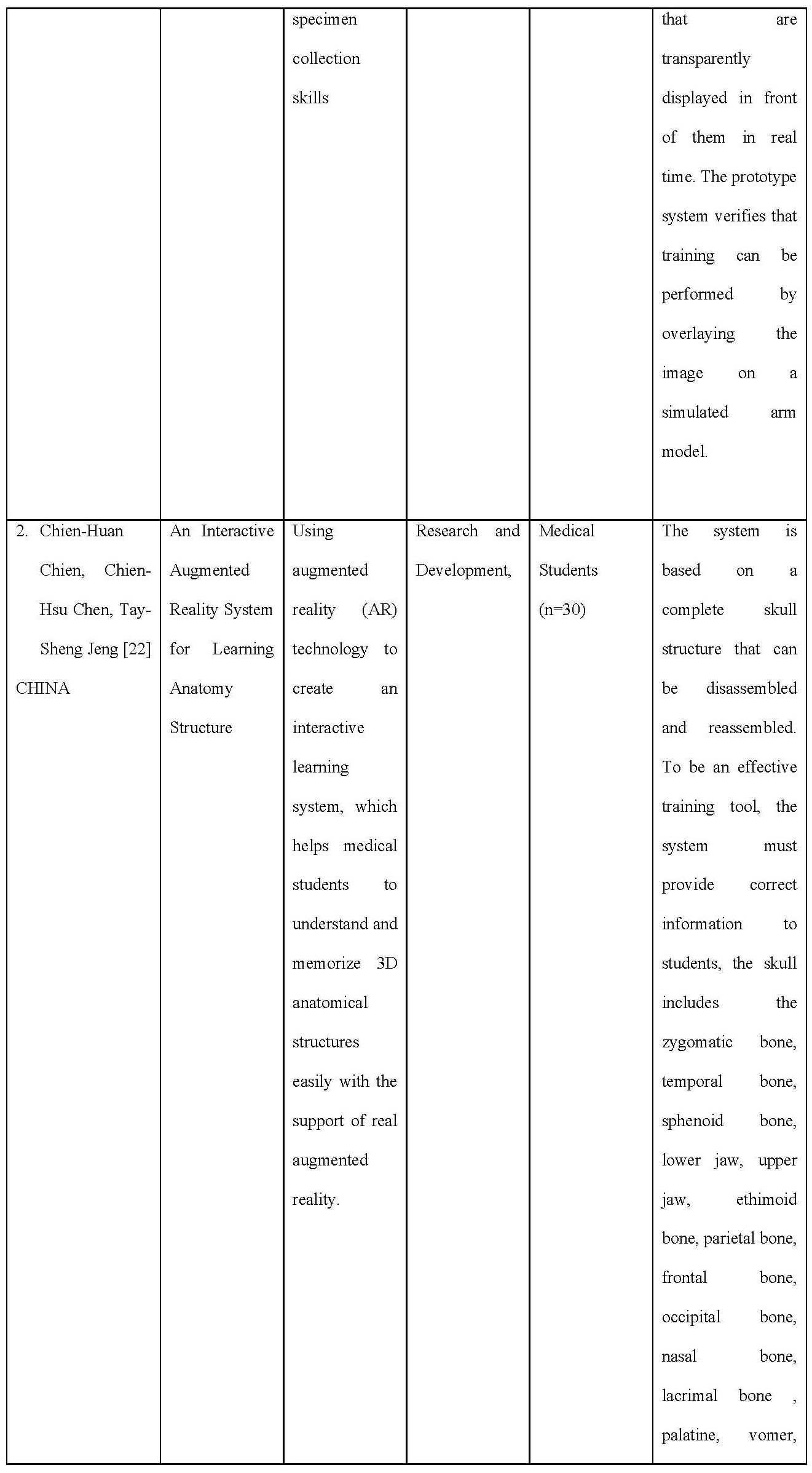


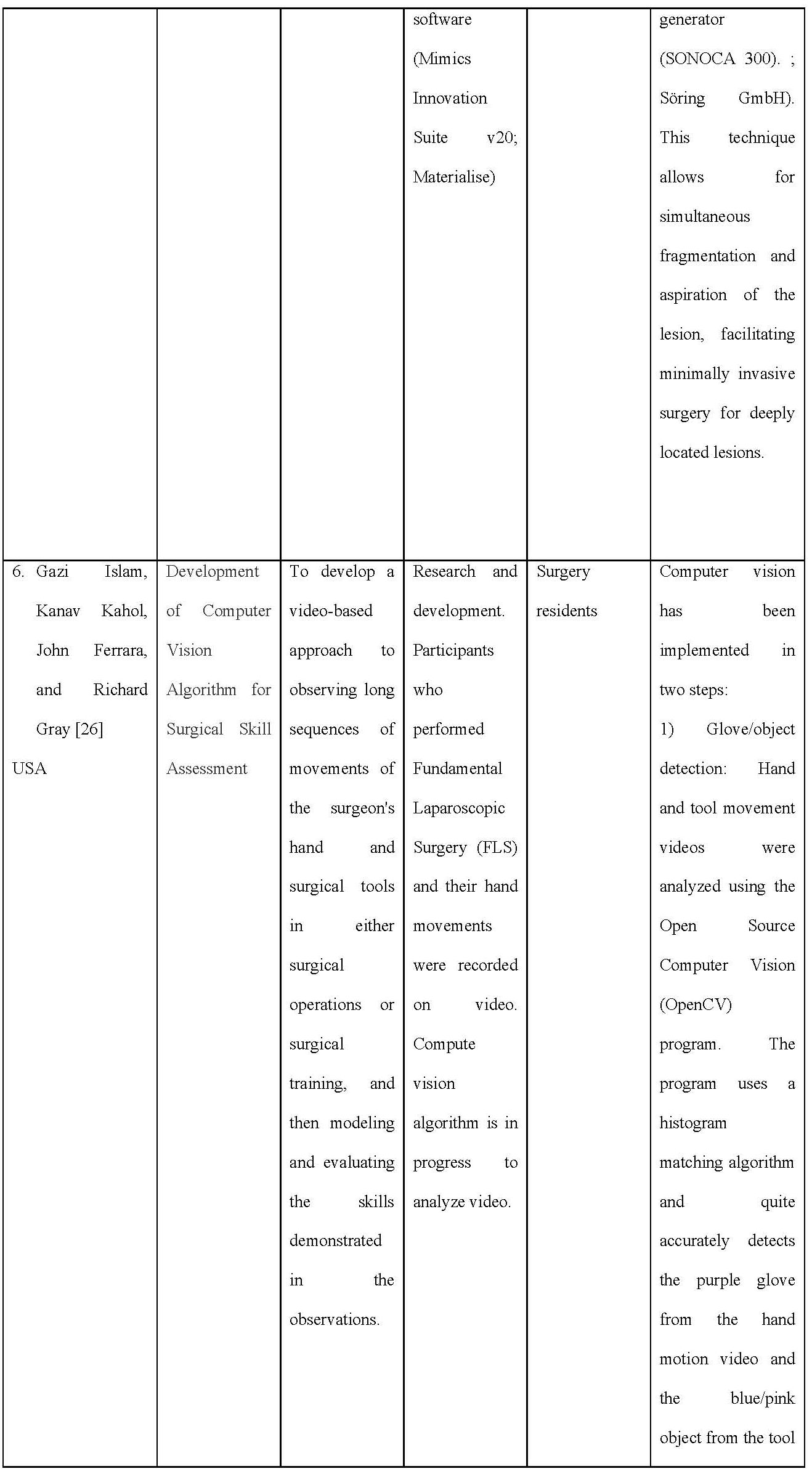

Table 1. Data Extraction on Included Articles
Characteristics of the studies included
The articles included in the inclusion criteria were six from several countries, including the USA as many as two articles, Canada 1 article, Sweden 1 article, Ireland 1 article, and Japan 1 article. Overall, the article taken is a study on the development of AR-based learning applications carried out to improve the clinical skills of health students (Medicine, Nursing, and Midwifery). Various types of application development are carried out including anatomy, Endotracheal Intubation, AR Prototype for Medical Surgery, Intravascular Neurosurgery, injection skills, and Laparoscopic.
Critical Appraisal
Based on the JBI Critical Appraisal Checklist, six pieces of literature are in the excellent category, and two pieces of literature are in the weak category. To maintain the quality of the literature studies made, this review only uses six good-quality journals, and then data extraction will be carried out.

Table 2. Summary of Critical appraisal based on JBI checklist
AR system design
In Majimas’ work, the learners can learn experts’ nursing skills without moving their lines of sight. When practicing skills training, learners can learn skills by following and imitating (tracing) the images of experts’ techniques that are dis-played transparently in front of them in real time. The prototype system verified that training is possible by overlaying images on a simulation arm model.
Chien and colleague The system is based on a complete structure of the skull which can be decomposed and reassembled. To be an effective training tool, the system has to provide correct information to the students, the skull includes zygomatic bone, temporal bone, sphenoid bone, mandible, maxilla, ethimoid bone, parietal bone, frontal bone, occipital bone, nasal bone, lacrimal bone, palatine, vomer, and inferior nasal concha.
Torregrosa and team developed an ARBOOK which includes a standard part of descriptive anatomy of the lower limb including osteology, arthrology, myology, nerve and vascular supply. Each part of the book includes bi-dimensional images and text about the muscles: origin insertion, vascular and nerve supply or action. It also includes a card for each anatomical figure that can be recognized by a digital webcam connected to a computer. The users can modify the actual position of the virtual structure by moving the card. To develop the ARBOOK, more than 100 TC images were needed and the images were processed by OsiriX software and 3D constructed. LabHuman and VMV3D companies performed the animation.
Drapkin study, an open-source T1 and T2 weighted simulated MRI dataset of a normal human brain constructed from a composite of 27 volumetric datasets of the same living subject was obtained from the BrainWeb simulated brain database. This dataset was viewed using GEHC MicroView software, version 2.1.2 (General Electric Healthcare, Little Chalfont, Buckinghamshire, UK). 3D models were constructed using MicroView to create isosurfaces based on gray scale values within a given region of interest to create a 3D mesh approximating the shape of a given internal brain structure. These computer graphic object composites were exported as a VTK PolyData file and edited using Maya software, version 2010 (Autodesk, San Rafael, CA) and were examined by two neuroanatomists and one neurologist for accuracy and compared to the Netter’s Atlas of Human Neuroscience. The final edited versions were imported back into MicroView 2.1.2 as Wavefront OBJ files and overlaid on top of the original MRI dataset. The final product was a set of digital 3D models of internal brain structures that can be freely rotated and zoomed by the user. To fabricate the 3D-printed models in Licci study, anonymized CT data set of a patient with enlarged CSF spaces was first downloaded from the picture archiving and communication system (PACS) and further processed with the medical segmentation software Materialise Mimics (Mimics Innovation Suite v20; Materialise). The DICOM CT data set consisted of native cross-sectional slices of bone and soft-tissue windows to display the relevant anatomical features. Further processing and segmentation of several anatomical structures according to tissue density (Hounsfield units) was worked out. The virtual cranial vault was designed with the help of the modeling software Materialise 3-Matics to be removable and equipped with realistic, neurosurgical burr holes for endoscopic access. The osseous skull was printed completely (2 parts) with a consumer Replicator+ 3D printer (MakerBot Industries) from polylactic acid (PLA; light gray), and the corresponding ventricle spaces were divided into 2 parts with a wall thickness of 3 mm in transparent PLA material. After printing a total of 5 skull models, the support structures were manually removed, and the two halves of the ventricular system were glued together. These were inserted into the skull model, and the cavity between the ventricular system and the bony skull was filled with 2-component silicone for stabilization.
In the Islam study, they proposed a novel video-based approach for observing continuous, long sequence of surgeon’s hand and surgical tool movements in both surgical operation or surgical training, and then modeling and evaluating the skill demonstrated in the observation. Hand movement of entire surgical procedure is captured using inexpensive video camera. Video data of the tool movement can also be obtained for minimal invasive surgery (MIS). Both of the video data are analyzed using computer vision algorithm and then integrated to correlate with user’s skill level.
For modeling the surgical skill, a stochastic approach is proposed that uses simple arithmetic mean and standard deviation of the processed data. Using this technique, observer-independent models can be developed through objective and quantitative measurement of surgical skills. Because of the non-contact nature of the tracking technique, the system is free from sterile issue and there is minimal interference with the skill execution, unlike other methods that employ instrumented gloves or sensor-based surgical tools.
AR for Nursing skills
There is one study that developed the teaching skills of nurses using AR technology. The skill learned in the study was performing intravenous injections [21].
AR for Anatomy learning
Three studies [22] developed learning methods based on AR technology. AR technology was used to create an interactive learning environment, which allows students to understand the 3D skull structure with visual support [14]. One of the studies gave their app the name ARBOOK, which can be presented in both, printed or electronic version. ARBOOK includes a standard part of descriptive anatomy of the lower limb including osteology, arthrology, myology, nerve and vascular supply [15]. Another study developed 3D Neuroanatomy Teaching Tool. The models were created of the ventricular system, thalamus, hypothalamus, pituitary gland, hippocam-pus, amygdala, fornix, caudate, putamen, globus pallidus, brainstem, cerebral peduncles, and cerebellar peduncles [16].
AR for Surgical training
There are two studies that develop training based on AR technology. The first study involved a neuroendoscopic ventricular lesion removal training [17], and the second study provided two laparoscopic graspers and performed the pegboard transfer exercise on the FLS [18].
DISCUSSION
It is undeniable that the advancement of Augmented Reality technology has had a significant impact on the health sciences. Professions requiring high precision and good psychomotor abilities certainly require more time to practice carrying out their actions. The presence of Augmented Reality technology in its various forms is proven to increase students' abilities and interests in dealing with the learning process.
Under certain conditions, especially during pandemic times where large-scale restrictions are imposed, direct meetings to carry out laboratory practicums are deemed possible, so there must be changes in strategies or effective learning methods for students in dealing with curriculum demands related to learning outcomes. A total of 6 eligible articles have been extracted to provide an overview of the development of Augmented Reality technology-based tools/tools in many health science fields, including Medicine, Nursing,/Midwifery. From the article, the discussion will be described based on the field of development, software and hardware used,
Development area
Anatomy Learning
Two articles develop applications for learning body anatomy based on Augmented Reality [18]. Tried to develop a 3D interactive learning environment of bone structure with visual support. This application is equipped with pop up labels and interactive displays in 3D to make it easier for users to see the position of each bone at various angles. In addition, users are also facilitated with the help of each label with information about the bone so that students no longer need to open books to look for information about the designated bone. To use this 3D application, students/users need hardware devices such as laptops/PCs equipped with cameras and pointers. For testing this device, Chien and colleagues used 30 medical students who had never taken anatomy courses to hope that the participants' responses to this application would be of better quality. At the evaluation stage, participants revealed that the developed application was fascinating because it could provide a complete picture of the displayed bone structure and explain each pop-up label, making it easier to understand and memorize. In addition, another exciting thing is that the reassembled function in the application allows students to see the inner structure of the bone.
Another application developed by Torregrosa and colleagues in 2014 called ARBOOK (Augmented Reality Book) focuses on the anatomical structure of the lower extremities. For its development, 100 TC photos/images are needed, then the images are processed using OsiriX software and 3D object creation. For validation, the questionnaire compiled for the ARBOOK evaluation consists of the categories of task motivation and attention, autonomous work, comprehensive spatial orientation, and 3D interpretation. . Next, an expert assessment will be carried out. Application testing involves first-year health students who have never taken an anatomy course. The test results show a significant difference between learning using ARBOOK and conventional learning. As has been stated in previous studies that the use of virtual materials in anatomy learning can provide good benefits for student learning achievement, especially regarding motivation and independence [27,28].
Augmented Reality technology was also developed in Neuroanatomy learning for MRI exercises developed by Drapkin and colleagues in 2015. The developed application makes the brain image display into a 3D shape. This 3D model begins by using MicroView to form a primary image in the form of isosurfaces and then form a 3D model similar to the shape of the actual brain. The graph is then exported in VTK PolyData file format and edited using Maya software. The editing results are then given to neuroanatomists and neuroscientists to assess the accuracy of the image shape and compared with images on the ATLAS neuroscience Netter. The final image is then placed on top of the actual brain image from the MRI. Next, we entered the pilot phase, which was conducted on participants who were medical students at level 1. The trials showed that this 3D neuroanatomy teaching tool effectively trains medical students to read brain MRI and effectively teach students to identify internal brain structures.
Surgery training
In contrast to learning the body's anatomical structure, surgical skills in surgery require hand-eye coordination, which can be achieved with continuous practice [29]. In surgery, one is not enough to see what other people are doing when performing surgery; that is, to become skilled, it is necessary to "watch and do" [30].
One of the six articles included in this review is an Augmented Reality-based simulation development study for Neuroendoscopic Ventricular Removal exercises [25]. In this development study, a 3D-printed model of synthetic body tissue was created. The idea is based on the limited material for practical surgery such as tumour removal. By using this 3D-printed model, it is hoped that it can accommodate all residents to do exercises repeatedly because this model is reusable.
Overall, the surveyed participants agreed or strongly agreed (Likert scores of 4 and 5) on the realistic nature of the anatomical model of the skull and ventricular system, the technical suitability of the model, the camera view, which was similar to the actual surgical view. Participants also agreed or strongly agreed that the content validity of the simulator is a valuable tool for enhancing surgical competence for neuro-endoscopic procedures that helps develop coordinating skills and represent an excellent practical exercise tool for ventricular tumour removal.
Other Augmented Reality-based surgical simulations are also included in this study. The development study conducted by Islam et al. [26] aims to create a video-based approach to observing surgeon hands and surgical instrument movements in surgery and surgical training. The data is captured with a video camera and then explored using a computer vision algorithm. Furthermore, by analyzing the basic statistical parameters, observer-independent performs objective and quantitative measurements of the surgical skills of the trainees. Computer vision is done through two steps, namely Glove/object detection and motion capture. This application is very suitable for remote assessment of student skills. Between the rater and the assessed, it is possible not to be in the room together; this allows the assessed participants to be calmer in the face of the assessment. Students can also receive virtual and interactive demonstrations of surgical procedures with surgeons carrying out the surgery so that students can experience real situations in the operating room.
Nursing skills
Majima, et all [21] developed a practicum learning system for nursing students based on Augmented Reality, especially in the act of taking blood specimens. In certain types of blood vessels, beginners find it difficult to insert the needle. It is the basis for this research. Through this development, beginners can learn the "art" in the veins and imitate the images displayed in front of them. In injection skills education, both instructors and students are usually very interested in holding a syringe. However, in reality, the teaching given is limited to fixation, and the left finger technique is taught, which is tailored to the characteristics of each patient's blood vessels that are difficult to insert a needle. How to repair and lengthen unstable blood vessels has not been entirely taught.
When practising skills training, students can learn skills by following and imitating (tracing) expert technical drawings transparently displayed in front of them in real-time. The prototype system verifies that training can be performed by overlaying the image on a simulated arm model.
CONCLUSION
The use of Augmented Reality as a learning medium really helps improve the understanding and skills of students majoring in health sciences. The many choices of models in application development provide opportunities for researchers to continue to innovate. Augmented Reality-based learning applications in the future become an absolute thing along with the increasing development of technology.
Limitation
Many databases not used in this review, such as Scopus, Ebsco, IEEE, and others, are very
credible for searching literature/articles. It is due to limited access to these databases. The use of gray literature such as google scholar conducted carefully with agreement of all authors.
The author also has limitations in understanding the software and programming languages used in the articles reviewed, so the authors cannot further discuss the application development process in the six articles reviewed.
Recommendation
This study provides a broad overview of the Augmented Reality-based application development process so that it can be a reference material for future teachers or researchers to be able to innovate in the development of Augmented Reality-based learning applications, for example, in the process of guiding final project students, or multiplying nursing action tutorials that are currently available. Not yet fully available in the form of an Augmented Reality application.
Funding
This systematic review does not get funding.
Conflict of Interest
The author declares there is no conflict of interest in this study.
REFERENCES
- Birt J, Stromberga Z, Cowling M, Moro C. Mobile mixed reality for experiential learning and simulation in medical and health sciences education. Information. 2018;9(2):31.
- Jones F, Passos-Neto CE, Braghiroli OFM. Simulation in medical education: brief history and methodology. Principles and practice of clinical research. 2015;1(2).
- Foronda CL, Alfes CM, Dev P, Kleinheksel AJ, Nelson Jr DA, O’Donnell JM, et al. Virtually nursing: Emerging technologies in nursing education. Nurse educator. 2017;42(1):14–7.
- Arena F, Collotta M, Pau G, Termine F. An Overview of Augmented Reality. Computers. 2022;11(2):28.
- Chiang THC, Yang SJH, Hwang G-J. Students’ online interactive patterns in augmented reality-based inquiry activities. Computers & Education. 2014;78:97–108.
- Di Serio Á, Ibáñez MB, Kloos CD. Impact of an augmented reality system on students’ motivation for a visual art course. Computers & Education. 2013;68:586–96.
- Khan T, Johnston K, Ophoff J. The impact of an augmented reality application on learning motivation of students. Advances in Human-Computer Interaction. 2019;2019.
- Jeffries PR. A framework for designing, implementing, and evaluating: Simulations used as teaching strategies in nursing. Nursing education perspectives. 2005;26(2):96–103.
- Aebersold M, Voepel-Lewis T, Cherara L, Weber M, Khouri C, Levine R, et al. Interactive anatomy-augmented virtual simulation training. Clinical simulation in nursing. 2018;15:34–41.
- Scalese RJ, Issenberg SB. Effective use of simulations for the teaching and acquisition of veterinary professional and clinical skills. Journal of veterinary medical education. 2005;32(4):461–7.
- Hamacher A, Kim SJ, Cho ST, Pardeshi S, Lee SH, Eun S-J, et al. Application of virtual, augmented, and mixed reality to urology. International neurourology journal. 2016;20(3):172.
- Bajura M, Fuchs H, Ohbuchi R. Merging virtual objects with the real world: Seeing ultrasound imagery within the patient. ACM SIGGRAPH Computer Graphics. 1992;26(2):203–10.
- Cameron C. How augmented reality helps doctors save lives. Read Write Web. 2010.
- De Paolis LT, Ricciardi F, Dragoni AF, Aloisio G. An augmented reality application for the radio frequency ablation of the liver tumors. In: International Conference on Computational Science and Its Applications. Springer; 2011. p. 572–81.
- Pandya A, Siadat M-R, Auner G. Design, implementation and accuracy of a prototype for medical augmented reality. Computer Aided Surgery. 2005;10(1):23–35.
- Rolland JP, Biocca F, Hamza-Lup F, Ha Y, Martins R. Development of head-mounted projection displays for distributed, collaborative, augmented reality applications. Presence: Teleoperators & Virtual Environments. 2005;14(5):528–49.
- Sielhorst T, Obst T, Burgkart R, Riener R, Navab N. An augmented reality delivery simulator for medical training. In: International workshop on augmented environments for medical imaging-MICCAI Satellite Workshop. 2004. p. 11–20.
- Frenk J, Chen L, Bhutta ZA, Cohen J, Crisp N, Evans T, et al. Health professionals for a new century: transforming education to strengthen health systems in an interdependent world. The lancet. 2010;376(9756):1923–58.
- Parmaxi A, Demetriou AA. Augmented reality in language learning: A state‐of‐the‐art review of 2014–2019. Journal of Computer Assisted Learning. 2020;36(6):861–75.
- Kobayashi L, Zhang XC, Collins SA, Karim N, Merck DL. Exploratory application of augmented reality/mixed reality devices for acute care procedure training. Western Journal of Emergency Medicine. 2018;19(1):158.
- Majima Y, Masuda S, Matsuda T. Development of Augmented Reality in Learning for Nursing Skills. In: MEDINFO 2019: Health and Wellbeing e-Networks for All. IOS Press; 2019. p. 1720–1.
- Chien C-H, Chen C-H, Jeng T-S. An interactive augmented reality system for learning anatomy structure. In: proceedings of the international multiconference of engineers and computer scientists. International Association of Engineers Hong Kong, China; 2010. p. 17–9.
- Ferrer-Torregrosa J, Torralba J, Jimenez MA, García S, Barcia JM. ARBOOK: Development and assessment of a tool based on augmented reality for anatomy. Journal of Science Education and Technology. 2015;24(1):119–24.
- Drapkin ZA, Lindgren KA, Lopez MJ, Stabio ME. Development and assessment of a new 3D neuroanatomy teaching tool for MRI training. Anatomical sciences education. 2015;8(6):502–9.
- Licci M, Thieringer FM, Guzman R, Soleman J. Development and validation of a synthetic 3D-printed simulator for training in neuroendoscopic ventricular lesion removal. Neurosurgical focus. 2020;48(3):E18.
- Islam G, Kahol K, Ferrara J, Gray R. Development of computer vision algorithm for surgical skill assessment. In: International Conference on Ambient Media and Systems. Springer; 2011. p. 44–51.
- Fairén M, Moyés J, Insa E. VR4Health: Personalized teaching and learning anatomy using VR. Journal of medical systems. 2020;44(5):1–11.
- Pringle RM, Dawson K, Ritzhaupt AD. Integrating science and technology: Using technological pedagogical content knowledge as a framework to study the practices of science teachers. Journal of Science Education and Technology. 2015;24(5):648–62.
- Rao A, Tait I, Alijani A. Systematic review and meta-analysis of the role of mental training in the acquisition of technical skills in surgery. The American Journal of Surgery. 2015;210(3):545–53.
- Herrlin S V, Wange PO, Lapidus G, Hållander M, Werner S, Weidenhielm L. Is arthroscopic surgery beneficial in treating non-traumatic, degenerative medial meniscal tears? A five year follow-up. Knee Surgery, Sports Traumatology, Arthroscopy. 2013;21(2):358–64.
![]() This work is licensed under a Creative Commons
This work is licensed under a Creative Commons
Attribution-NonCommercial-NoDerivatives 4.0 International License.
KNOWLEDGE AND ATTITUDES BETWEEN NURSES, MIDWIVES AND STUDENTS ABOUT VOLUNTARY TERMINATION OF PREGNANCY: A SCOPING REVIEW OF THE LITERATURE
Sofia Di Mario1, Andrea Minciullo2 & Lucia Filomeno3*
- RN, MSN, PhD Student; Department of Public Health and Infectious Diseases, Sapienza University of Rome, Piazzale Aldo Moro 5, 00185, Rome, Italy.
- RN, MSN, Gastroenterology and Digestive Endoscopy Unit, Campus Bio-Medico, 00128, Rome, Italy,
- RN, MSN, PhD Student; AOU Policlinico Umberto I – Department of Neurosciences and Mental Health, Viale dell’Università, 30, 00185, Rome, Italy.
* Corresponding author: Lucia Filomeno, Department of Neurosciences and Mental Health, AOU Policlinico Umberto I, Rome. E-mail: lucia.filomeno@uniroma1.it

Cita questo articolo
ABSTRACT
Background: Voluntary termination of pregnancy (VTP) is influenced by ethical convictions, religious orientations and knowledge of the law. The latter is essential for students to be improved in University curricula, in order to develop attitudes among future nurses and midwives with the objective to reduce stigma and reluctance in providing VTP. Previous research has shown that nursing and midwifery students' attitudes and knowledge can be improved.
Aim: The aim of this study is to describe literature regarding knowledge and perception about abortion and voluntary termination of pregnancy in several countries of the world among nurses, midwives and university students.
Methods: This is a scoping review of the literature conducted by following the recommendations of the PRISMA-ScR Statement. The authors selected studies in MEDLINE, Scopus, CINAHL, PsycINFO, Academic Search Index, Science Citation Index and ERIC, published in English and Italian in the last decade. Quality assessment was performed using the Jadad scale.
Results: Initially, 434 studies were selected. A total of 11 articles met the inclusion criteria. The articles included in the scoping review deal with the issue of abortion from different perspectives. From the analysis it emerged that the barriers for VTP are the lack or inadequate knowledge of the legislation and of the practical / technical phases of the procedure.
Conclusions: Health professionals and students have different perspectives and attitudes toward VTP. Nurses and midwives have inadequate knowledge of procedures and legislation. Therefore, it is recommended to implement university curricula on the topic.
Keywords: knowledge, attitudes, voluntary termination of pregnancy, nurses, midwives, students.
INTRODUCTION
Abortion, originated as birth control, is the termination of pregnancy before 20 weeks of gestation or with the foetus weight less than 500 gr at birth [1,2]. It can happen when at least three events occur: spontaneous or habitual abortion (also called Voluntary Termination of Pregnancy - VTP), criminal or illegal abortion, and therapeutic or legal abortion [3]. In the last decades of the 20th century, many countries all over the world legalised this practice. The World Health Organization (WHO) states that 3 out of 10 (29%) of all pregnancies, and 6 out of 10 (61%) of all unintended pregnancies, ended in an induced abortion [4]. In many societies, a deep conflict about the legality and morality of abortions manifests itself in restrictive laws and strong antiabortion attitudes. Women, including adolescents, with unwanted pregnancies often resort to unsafe abortion when they cannot access a safe one. Barriers to accessing safe VTP include: restrictive laws, poor availability of services, high cost, stigma, conscientious objection of health-care providers and unnecessary requirements, such as mandatory waiting periods, mandatory counselling, provision of misleading information, third-party authorization, and medically unnecessary tests that delay care [5,6]. Kumar et al. [7], defined abortion stigma as “a negative attribute ascribed to women who seek to terminate a pregnancy that marks them, internally or externally, as inferior to the ideals of womanhood”. According to this definition, women who experience VTP challenge social norms regarding female sexuality and maternity, and their doing so elicits stigmatising responses from the community. Where opposition to abortion is widespread, abortion-related stigma is likely to negatively influence women’s abortion experience.
Increased knowledge and improved attitudes among health care providers and university students have the potential to reduce stigma and reluctance to provide abortion [6]. In a recent study conducted by O'Shaughnessy et al. [8], it was reported that “low levels of knowledge among staff suggests that training is required to ensure the provision of a safe and effective VTP service”. Midwifery and Nursing schools do not provide termination of pregnancy education or, if they do, it is inadequate and so, most staff were left to navigate this procedure without support or prior practice.
Termination is only possible in the rarest of cases: when the pregnancy poses a serious risk to the woman’s life or in the event of foetal malformations [7]. In Italy, as in many countries, it is set at 12 weeks’ gestation according to the law No. 194 enacted on May 22nd, 1978. Before that date, VTP was considered illegal by the criminal code [9]. The law regulates VTP with the aim of guaranteeing the bio-psycho-social integrity and well-being of women. A woman can have an abortion within the first 90 days, or within the fourth and fifth months only for therapeutic reasons [9]. Conscientious objection status does not exempt the professional from assisting the woman before and after the procedure, but from carrying out only those procedures directed towards and aimed at the termination [10-13]. The nurse can raise a conscientious objection to assisting the VTP with a declaration that can be withdrawn at any time [9]. Termination is a woman’s right, and the staff involved must act in accordance with the law and the woman’s right to free choice. A better understanding of factors influencing perceptions may be useful in determining the curricula of university programs and in giving nurses and midwives the tools to cope with their own beliefs towards late abortions [14-16]. Thus, this review seeks to contribute to research on abortion stigma by exploring literature regarding attitude, knowledge and perception differences toward abortion among nursing, midwifery and students, assessing the scientific evidence available to date and thereby delineating directions for future research.
METHODS
Identification of Relevant Studies
A scoping review was chosen as the research methodology [17]. This supports what is referred to as a systematic approach to the synthesis of evidence, helping to identify gaps for future studies. In this case, the goal is to determine the strength of the evidence using a consistent best practice approach. The search of the international literature was conducted in accordance with the PRISMA-ScR Statement (PRISMA extension for Scoping Reviews)[18] and was conducted within some main databases of biomedical interest: MEDLINE, Scopus, CINAHL, PsycINFO, Academic Search Index, Science Citation Index and ERIC. The review was carried out from October 2021 to February 2022. The keywords used were “knowledge; attitude; perception; nurse; student; abortion; midwife and questionnaire”. The latter were useful in formulating the research question according to the PCC (Population, Concept and Context) methodology (Table 1).

Table 1. Clinical research question identified through the PCC methodology
Study Selection and Eligibility Criteria
Research question: “What are the differences in knowledge and attitudes between nursing and midwifery staff and the corresponding university students?”. The search string was created using the Boolean operators (AND and OR), the terms MeshTerms and the truncation function, to ensure maximum search sensitivity and specificity:
(Knowledge OR Attitude OR Perception) AND (Abortion) AND (Nurse OR Midwife OR Student) AND (Questionnaire OR Assessment)
The study population were nurses, midwives and nursing and midwifery students. The primary studies concerning the assessment of attitudes, perceptions and knowledge about abortion between the two groups and the efficacy and validity of these arguments within the degree programs were considered eligible. The studies included experimental or quasi-experimental studies and observational studies. Since grey literature (i.e., unpublished conference proceedings or theses or dissertations) was not considered, other potentially relevant studies were not included in this review.
The selection criteria listed below were met to identify suitable studies for the purpose of this review.
Inclusion criteria
- Literature from the last 10 years.
- Italian or English language.
- Experimental and observational studies: RCT (Randomised Controlled Trial), quasi-experimental research designs, pretest-posttest, cross-sectional.
- Nurses, midwives and corresponding university students.
Exclusion criteria
- Other healthcare professionals, physicians, medical students or students of other healthcare professionals.
- Grey
- Qualitative and mixed-methods studies.
Data Extraction
In the first phase, the results obtained from the research were imported into a software for the management of bibliographic references and duplicates were eliminated. In the second phase, each article uploaded to the database was carefully and independently examined. Initially, they were analysed by reading their title and abstract and, according to the previously established eligibility criteria, the irrelevant ones were excluded, while those relevant for full-text reading were selected. Thanks to the in-depth reading, it was possible to exclude the articles that did not answer the research questions. Two reviewers worked independently. The following data was collected for each article: study title, first author, year of publication, study sample and study design, objective, assessment and a summary of the results. The approach used to group the articles was thematic: the main objective of the thematic analysis is to identify similar concepts in the collected dataset, exploring their relationships of meaning. These reports can be used to further develop and corroborate the interpretation of theories that seek to investigate the phenomena studied [19].
Quality Assessment
The quality of the studies was assessed usingthe Jadad Scale [20], focusing on methods for random allocation, double blinding, and withdrawals and dropouts. Total scores ranged from 0 to 5 points, where studies with 0-2 points were considered poor quality and those with 3-5 points represented high-quality evidence [20].
RESULTS
Initially, 434 articles were selected with duplicates removed (Figure1). Of these, 11 met the inclusion criteria and underwent the review process. The main information of the relevant articles was organised in a data extraction table (Table 2). Studies were conducted in 11 different countries: Belgium, Ghana, Iran, Brazil, Israel, Spain, Ethiopia, Finland, Canada, Pakistan and South Korea. This demonstrates a notable absence of literature in Italy. The studies included a sample ranging from a minimum of 74 to a maximum of 647 participants. The most recent one dates to 2020, while the oldest one dates to 2010. From the analysis it emerged that the barriers for abortion treatment are the lack or inadequate knowledge of the legislation and of the practical / technical phases of the intervention [21-24]. The possession of skills is often not enough as in the study by Romina et al. [22] where it emerged that there was no significant relationship between the knowledge of the law and the care performance of health professionals while a statistically significant relationship was observed between their opinion of abortion and their active collaboration[22].

Figure 1. - PRISMA 2020 flow diagram for new systematic reviews which included searches of databases and registers only.
Personal and religious beliefs have been considered to have a profound influence on opinion and behaviour, in some cases resulting in the inability to take care of the patient for fear of remorse [21; 25-27]. The presence of moral and / or religious values in health workers was significantly correlated with the occurrence of the request for conscientious objection (CO) [21-26].



Table 2. Data Extraction Table.
In South Korea, where about half of the population declared themselves irreligious, Chung Mee Ko et al. [26] assessed the opinions of 167 nurses regarding CO; the majority replied that patients’ rights to health care should take priority over nurses’ right to refuse health care, concluding that the nursing profession should seriously consider whether it is necessary to insist on nurses’ right to CO and should be actively involved in the determination process of new abortion laws and related policies [26]. Nieminen et al. [6] studied CO among Finnish nursing students and practitioners. Most of them seemed to consider the continuation of adequate services to patients in the event of the introduction of CO as crucial, while emphasising the surgical act over patient support. Despite their views and beliefs, health workers sometimes faced a conflict with their commitment to care; in the work of Ben Natan et al. [15], they stated that bioethical dilemmas, as well as the reasons for abortion, influenced their ability to actively collaborate during the termination of pregnancy [15]. Nurses attitude and ability to actively participate in late abortions were found to be strongly conditioned by the level of religious observance [21-22]. The study by Roets et al. [28] found that in several neonatal intensive care units in Belgium, healthcare workers practicing late abortion had a high degree of tolerance towards late termination of pregnancy, regardless of the patient’s socio-demographic factors, so much so that they asked the institutions to provide for a change in legislation [28].
Ben Natan et al. [15], however, found that nursing students had more prejudices towards late abortions than experienced nurses, evidence in line with the study conducted by Assefa et al. [24] where it turned out that a predictor of a positive attitude towards VTP was seniority [24]. The role of health workers is very important, especially on a psychological level, even more so when they must help women to deal with a negative event such as a miscarriage. To this end, Engel et al. [27] suggested that health workers should receive specific training to be able to support women and their families [27]. Previous research has shown that university education programs do not provide the tools necessary to achieve the objectivity required in preparation for abortion and that this may have contributed to anti-abortion attitudes and misconceptions about legal regulations that are common among students10. Same results emerged from the work of Baig et al. [29] who studied the knowledge, attitudes and practices of midwives in post-abortion care services [29]. The work highlighted the need to provide comprehensive training and mentoring to midwives and students, building strong networks to enable the development of broader initiatives to reduce the stigma of abortion.
DISCUSSION
Although the total number of studies investigating abortion stigma among undergraduate students and nurses and midwives such as nurses and midwives is low, results indicate that knowledge, personal and religious beliefs significantly affect attitudes about VTP. This is in line with the findings by Madziyire et al. [10] where incomplete comprehension of abortion laws highlights the urgent need for providers education as a key step in reducing stigma and mortality associated with unsafe abortion [10]. Additionally, the lack of expertise evidenced by most of the studies, suggest that even nurses and midwives who have good intentions may unwittingly disseminate misinformation. One study underlined the fact that type of profession and seniority were important in providers’ knowledge about abortion. Also, being male and having high knowledge significantly influenced providers’ attitude. The same findings were highlighted by Hammarstedt et al. [30] who stated that gynaecologists and midwives were less restrictive towards legal abortion the more experience they had, being especially influenced by recently obtained experience within the last year [30]. Claims of conscientious objection must be ethically justified, and not become a strategy to hide prejudices or fear of lawsuits and moral accusations. Such an instrument cannot be an obstacle for women to have access to abortion [31]. Humanized care in the abortion process is part of the reproductive and sexual rights of women, and ensuring it is a duty of all health professionals.
Abortion laws and practice differ between cultures, religions and countries. The Finnish healthcare system is relatively liberal regarding the right for induced abortion until the 12° gestational week. Despite lively discussion, there is no legislation in this country on the possibility of CO [32]. Post-abortion care is important especially in countries like Pakistan, where half of pregnancies are unintended. Demand for abortions is high in Jamaica, but many doctors refer clients to another provider. Patient assessment is good, but support services need improvement [33]. This has been reported in other surveys in other countries. In Ghana, for example, only 45% of surveyed physicians said that they would perform abortions, whereas another 36% said that they would provide counselling prior to abortion but not the procedure itself [33]. Women deserve a well-prepared, informed personnel and similarly, students deserve a thoughtfully inclusive curriculum that accurately addresses ethical topics, as most programs do not require sexual health courses as a part of their curriculum [34-35].
CONCLUSION
The role of the health professional assisting the woman who decides to undergo a voluntary termination of pregnancy is very important, especially in the phases before and after the intervention. Assistance must always be provided with respect for the woman’s dignity, confidentiality and freedom of choice. Nurses need to provide a source of support for the woman by establishing a relationship based on trust. Health professionals and students have different perspectives and attitudes toward VTP. Nurses and midwives have inadequate knowledge of procedures and legislation. It is important that the health professional realises the crucial importance of their role in the woman’s grieving process to ensure good care.
Limitations of the study
Our study has some limitations that should be mentioned. In our analysis, only research articles published in English and Italian were included, which may have produced a language bias regarding the conclusion, as some scientific papers were published in other languages. Additionally, only studies published in peer-reviewed journals were included; this criterion was meant to ensure reporting quality but may mean that relevant grey literature was missed.
Practical implication
Nurse sneed to have adequate training in the bereavement context: they should know what interventions implement and what to avoid. The aim of the scoping review was to analyze the international panorama regarding abortion as a point of departure on which to develop an Italian study to compare legislation knowledge, attitudes and perspective differences among students and nurses and midwives. Therefore, it is recommended to implement university curricula on the topic.
Funding statement
This research did not receive any specific grant from funding agencies in the public, commercial, or not for profit sectors.
The authors declared no conflict of interest.
REFERENCES
- Lobo RA, Gershenson DM, Lentz GM, Valea FA. Comprehensive gynecology E-book. Elsevier Health Sciences, 2016.
- Echeverría BC, Serani MA, Arriagada U AM, Goic G A, Herrera CC, Quintana VC, et al. An ethical and medical perspective on the voluntary termination of pregnancy. 2015;143(11):1478–83. https://doi.org/10.4067/S0034-98872015001100014
- Narayan KS, Reddy M. Essentials of Forensic Medicine and Toxicology. JAYPEE Brothers MEDICAL P, 2017.
- World Health Organization. (2021). Access to medical abortion medicines in the South-East Asia Region-a status report.
- Bearak J, Popinchalk A, Ganatra B, Moller A-B, Tunçalp Ö, Beavin C, Kwok L, Alkema L. Unintended pregnancy and abortion by income, region, and the legal status of abortion: estimates from a comprehensive model for 1990–2019. Lancet Glob Health. 2020 Sep; 8(9):e1152-e1161. https://doi.org/10.1016/S2214-109X(20)30315-6
- Nieminen P, Lappalainen S, Ristimäki P, Myllykangas M, Mustonen A-M. Opinions on conscientious objection to induced abortion among Finnish medical and nursing students and professionals. BMC Medical Ethics. 2015 Mar 25;16(1):17. https://doi.org/10.1186/s12910-015-0012-1
- Kumar A, Hessini L, Mitchell EMH. Conceptualising abortion stigma. Culture, Health & Sexuality. 2009;11(6):625–39. https://doi.org/10.1080/13691050902842741
- O’Shaughnessy E, O’Donoghue K, Leitao S. Termination of pregnancy: Staff knowledge and training. Sexual&Reproductive Healthcare. 2021 Jun1;28:100613. https://doi.org/10.1016/j.srhc.2021.100613
- Italiana R. Legge 22 maggio 1978, n. 194. Norme per la tutela sociale della maternità e sull’interruzione volontaria della gravidanza. Gazzetta Ufficiale, 22. https://www.gazzettaufficiale.it/eli/id/1978/05/22/078U0194/sg
- Madziyire MG, Moore A, Riley T, Sully E, Chipato T. Knowledge and attitudes towards abortion from health care providers and abortion experts in Zimbabwe: a cross sectional study. Pan AfrMed J. 2019 Oct16;34:94. https://doi.org/10.11604/pamj.2019.34.94.18107
- Aragaw Y, Sinishaw W, Daba W, Mekie M. Attitude of Nursing and Midwifery students towards clinical practice and its associated factors in Northwest Ethiopia: a cross-sectional study. BMC Research Notes. 2019 Apr 3;12(1):205. https://doi.org/10.1186/s13104-019-4230-3
- Jafari H, Khatony A, Abdi A, Jafari F. Nursing and midwifery students’ attitudes towards principles of medical ethics in Kermanshah, Iran. BMC Medical Ethics. 2019 Apr 25;20(1):26. https://doi.org/10.1186/s12910-019-0364-z
- Biggs MA, Casas L, Ramm A, Baba CF, Correa SP. Medical and midwifery students’ views on the use of conscientious objection in abortion care, following legal reform in Chile: a cross-sectional study. BMC Medical Ethics. 2020 May 24;21(1):42. https://doi.org/10.1186/s12910-020-00484-4
- Glenton C, Sorhaindo AM, Ganatra B, Lewin S. Implementation considerations when expanding health worker roles to include safe abortion care: a five-country case study synthesis. BMC Public Health. 2017 Sep 21;17(1):730. https://doi.org/10.1186/s12889-017-4764-z
- Ben Natan M, Melitz O. Nurses’ and nursing students’ attitudes towards late abortions. Int Nurs Rev. 2011 Mar;58(1):68–73. https://doi.org/10.1111/j.1466-7657.2010.00840.x
- Harries J, Stinson K, Orner P. Health care providers’ attitudes towards termination of pregnancy: A qualitative study in South Africa. BMC Public Health. 2009 Aug 18;9(1):296. https://doi.org/10.1186/1471-2458-9-296
- Arksey H, O’Malley L. Scoping studies: towards a methodological framework. International Journal of Social Research Methodology. 2005 Feb 1;8(1):19–32. https://doi.org/10.1080/1364557032000119616
- Tricco AC, Lillie E, Zarin W, O’Brien KK, Colquhoun H, Levac D, et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Annals of Internal Medicine. 2018 Sep 4;169(7):467–73. https://doi.org/10.7326/m18-0850
- Allodola V.F. Metodi di ricerca qualitativa in MedicalEducation: Approcci, strumenti e considerazioni di rigore scientifico. Educ. Sci. Soc. 2014, 5, 121–144.
- Jadad AR, Moore RA, Carroll D, Jenkinson C, Reynolds DJ, Gavaghan DJ, et al. Assessing the quality of reports of randomized clinical trials: is blinding necessary? Control Clin Trials. 1996 Feb;17(1):1–12.https://doi.org/10.1016/0197-2456(95)00134-4
- De Roose M, Tency I, Beeckman D, Van Hecke A, Verhaeghe S, Clays E. Knowledge, attitude, and practices regarding miscarriage: A cross-sectional study among Flemish midwives. 2018 Jan;56:44–52. https://doi.org/10.1016/j.midw.2017.09.017
- Romina S, Alamshahi M, Moafi F, Mafi M, Hajnasiri H. Relationship of Knowledge and Attitude Towards Legal Abortion Laws with the Performance of Midwives in Qazvin, Iran. Health, Spirituality and Medical Ethics. 2019 Jun 10;6(2):17–23. http://dx.doi.org/10.29252/jhsme.6.2.17
- Cacique DB, Passini Junior R, Duarte Osis MJM, Oliveira HC, Padilha KM, Tedesco RP, et al. Perspectives of healthcare workers on the morality of abortion: a multicenter study in seven Brazilian public hospitals. Health Care Women Int. 2020 Jul;41(7):761–76. https://doi.org/10.1080/07399332.2019.1672169
- Assefa EM. Knowledge, attitude and practice (KAP) of health providers towards safe abortion provision in Addis Ababa health centers. BMC Women’s Health. 2019 Nov 14;19(1):138. https://doi.org/10.1186/s12905-019-0835-x
- Voetagbe G, Yellu N, Mills J, Mitchell E, Adu-Amankwah A, Jehu-Appiah K, et al. Midwifery tutors’ capacity and willingness to teach contraception, post-abortion care, and legal pregnancy termination in Ghana. HumResour Health. 2010 Feb23;8:2. https://doi.org/10.1186/1478-4491-8-2
- Ko CM, Koh CK, Lee YS. An ethical issue: nurses’ conscientious objection regarding induced abortion in South Korea. BMC Med Ethics. 2020 Oct 27;21(1):106. https://doi.org/10.1186/s12910-020-00552-9
- Engel J, Rempel L. Health Professionals’ Practices and Attitudes About Miscarriage. MCN Am J Matern Child Nurs. 2016 Feb;41(1):51–7. https://doi.org/10.1097/nmc.0000000000000207
- Roets E, Dierickx S, Deliens L, Chambaere K, Dombrecht L, Roelens K, et al. Healthcare professionals’ attitudes towards termination of pregnancy at viable stage. Acta ObstetGynecolScand. 2021 Jan;100(1):74–83. https://doi.org/10.1111/aogs.13967
- Baig M, Jan R, Lakhani A, Ali S, Mubeen K, Ali S, et al. Knowledge, Attitude, and Practices of Mid-Level Providers regarding Post Abortion Care in Sindh, Pakistan. Journal of Asian Midwives (JAM). 2017 Jun 1;4(1):21–34.
- Hammarstedt M, Jacobsson L, Wulff M, Lalos A. Views of midwives and gynecologists on legal abortion--a population-based study. Acta ObstetGynecolScand. 2005 Jan;84(1):58–64. https://doi.org/10.1111/j.0001-6349.2005.00695.x
- Madeiro A, Rufino A, Santos P, Bandeira G, Freitas I. Conscientious Objection and Legal Abortion: Medical Students’ Attitudes. Rev bras educ med. 2016 Mar;40:86–92. http://dx.doi.org/10.1136/medethics-2013-101482
- Gissler M, Ulander VM, Hemminki E, Rasimus A. Declining induced abortion rate in Finland: data quality of the Finnish abortion register. Int J Epidemiol. 1996 Apr;25(2):376–80. https://doi.org/10.1093/ije/25.2.376
- Fletcher H, Gordon-Strachan G, McFarlane S, Hamilton P, Frederick J. A survey of providers’ knowledge, opinions, and practices regarding induced abortion in Jamaica. Int J Gynaecol Obstet. 2011 Jun;113(3):183–6. https://doi.org/10.1016/j.ijgo.2010.12.022
- Baba CF, Casas L, Ramm A, Correa S, Biggs MA. Medical and midwifery student attitudes toward moral acceptability and legality of abortion, following decriminalization of abortion in Chile. Sexual&Reproductive Healthcare. 2020 Jun1;24:100502. https://doi.org/10.1016/j.srhc.2020.100502
- Burnes TR, Singh AA, Witherspoon RG. Sex Positivity and Counseling Psychology: An Introduction to the Major Contribution. The Counseling Psychologist. 2017 May 1;45(4):470–86. https://doi.org/10.1177%2F0011000017710216
![]() This work is licensed under a Creative Commons
This work is licensed under a Creative Commons
Attribution-NonCommercial-NoDerivatives 4.0 International License.
NUTRITION EDUCATION MODELS IN PREGNANCY TO INCREASE KNOWLEDGE AND DIETARY PATTERNS: A SYSTEMATIC REVIEW
Suryani*1, Muhammad Rusdi1, Asni Johari1, Solha Elrifda1
- Post-Graduate Program of Mathematic and Natural Science Education College, Jambi University, Indonesia
Correspondence: Suryani, Address : Dr. Tazar Street, Buluran Kenali, Kec. Telanaipura, Kota Jambi, Jambi 36361, Indonesia, Email : suryanipoltekkes3@gmail.com, Orcid : 0000-0001-6540-2607

Cita questo articolo
ABSTRACT
Background. The misconception of nutritional principles causes dietary oversight, resulting in an excess or deficit of energy and specific nutrients essential for the proper course of pregnancy and a child's healthy growth. This review aims to evaluate the effectiveness of nutrition education in improving knowledge and dietary change conducted in pregnant women.
Methods. This review study complies with the 2009 PRISMA guidelines. The studies included in this review are mainly studies with experimental designs. Databases used in searching relevant literatures such as PubMed, ScienceDirect, Willey online Library, Web of Science, Cochrane, and Proquest that were published from 2010 to 2021, full text, English version, experimental studies. Two review authors conducted studies screening based on the eligibility criteria, and extracted important points in the studies included. Quality of the studies included were assessed using EPHPP.
Results. A total of 10 studies were identified in this review. Six studies in the high quality, and four studies in moderate quality. Overall outcomes of the studies included are Knowledge, Attitude, practice, dietary practice, awareness, hemoglobin blood level, and Gestational Weight Gain (GWG).
Conclusion. Nutrition education in many methods has a power to improve knowledge, and dietary change of pregnant women. It implies the need for future large high quality trials using a standardized approach to measuring and reporting similar findings across studies.
Keywords : Pregnancy, Pregnant women, Education, Nutrition
INTRODUCTION
Pregnancy is one of the most notable moments in a person's life, and at that time, diet is essential [1]. So far, maternal malnutrition or failure to meet nutritional needs has caused specific health problems for both mothers and newborns [2]. Due to insufficient and unbalanced nutrition, problems such as anemia, osteomalacia, and pregnancy toxemia often arise, and the chances of stillbirth in newborns, premature delivery, congenital abnormalities, and mental retardation increase [3,4]. Furthermore, poor maternal nutritional quality causes developmental maladaptation in the fetus [5]. This results in long-term structural, physiological and metabolic changes and an increased risk of cardiovascular, metabolic, and endocrine diseases in adults [6].
Poor eating habits are a leading contributor to the development of overweight and obesity across the world [7,8]. The frequency of home-cooked meals has decreased over the last five decades, while consumption of foods produced outside the house (i.e., fast food and restaurant food), often higher in calories, fat, and salt, has grown [9,10]. Consumption of home-cooked meals regularly is linked to better diet quality over the lifespan [11,12]. As a result, increasing the frequency of home-prepared meal intake is a significant health habit to target for preventing overweight and obesity in adults and children, and it has been the topic of extensive research over the last two decades [13,14].
International authorities define pregnancy as a moment of highly nutritional needs to promote mother and fetal growth [15]. Nutritional support needed in pregnancy includes carbohydrates, fiber, protein, and micronutrients, such as vitamin A, vitamin B complex folate, and iron [16]. However, a study in Canada found that people have insufficient micronutrients through food, such as high levels of iron (97 percent), vitamin D (96 percent), and folate (70 percent) intake [17]. Therefore, stakeholders intended to present food and nutrition education to encourage a balanced diet based on food culture's valorization [18]. Food and nutrition education is an essential strategy for upgrading health because it encourages people to identify and tolerate their cultural discrepancies and empowers them to complete decisions concerning their health care [19]. Antenatal nutrition education is related to better eating patterns and a healthier pregnancy [20]. Healthy fetal growth and development, cognitive capacity, and immunological function are promoted by optimal nutrition throughout pregnancy [21]. Pregnant women's adherence to dietary guidelines decreases due to a lack of nutrition expertise and insufficient information from health providers [22]. Before and during pregnancy, the mother's behavior becomes a determining factor for both the mother and her child [23,24]. Many dietary mistakes can be caused by a lack of understanding of nutritional principles, resulting in an excess or deficit of energy and specific nutrients essential for the proper course of pregnancy and a child's healthy growth [25,26]. Adequate diet, in combination with sufficient physical activity and the avoidance of harmful habits, enhances the chances of a healthy pregnancy [27,28]. One of the previous systematic reviews on pregnant women's compliance in following dietary guidelines during pregnancy stated that knowledge was an essential predictor concerning adherence to the given nutritional guidelines [29].
It is essential to assess how successful nutrition educations are in improving the nutritional status of pregnant women especially their knowledge and dietary.
This systematic review aimed to assess the efficacy of nutrition education in knowledge and dietary change during pregnancy and their implications for future research. Therefore, the question for this review is, "what kind of nutritional education model is good for increasing knowledge and changes in the diet of pregnant women?".
METHODS
Design
When reporting this systematic review, the standards outlined in the Preferred Reporting Items for Systematic Reviews and Meta-Analyses statement were followed [30].
Eligibility Criteria
The participants, intervention, comparator, outcome, and study design (PICOS) criteria outlined in Table 1 were used to select studies for inclusion in this review.

Table 1. Studies Criteria based on PICOS
Type of Studies
The studies included in this review use experimental designs such as Randomized Controlled trials (RCT) and Quasi-experimental. Participants in the study should be pregnant women in any trimester of pregnancy.
Search Strategy
The following databases (platforms) were searched: PubMed, ScienceDirect, Willey online Library, Web of Science, Cochrane, and Proquest in the time frame between 2010 to 2021. We also searched the gray literature database for additional information such as Google Scholar, conference proceedings, and BASE. The keywords used are based on the Medical Subject Headings (MeSH) standard. Using Boolean operators and a combination of keywords used, namely: ((("pregnancy nutrition"[Title/Abstract]) OR ("pregnancy nutrition knowledge"[Title/Abstract])) AND ((("health education"[Title/Abstract]) OR ("nutritional education"[Title/Abstract])) OR ("health promotion"[Title/Abstract]))) AND (((("knowledge"[Title/Abstract]) OR ("attitude"[Title/Abstract])) OR ("practice"[Title/Abstract])) OR ("awareness"[Title/Abstract])).
Study selection
Two review authors independently assessed the titles and abstracts of the retrieved studies to see if they met the eligibility criteria (RUS and ASJ). The full-text publications for the remaining studies were obtained and evaluated for eligibility which obtained and read full texts of the studies that potentially met the inclusion criteria. The first ineligibility criterion from the following list determines why a publication was excluded: study design, population, intervention, and results. The first authors decided disagreements from review authors regarding the feasibility of the study (SUR and SOE), and this procedure was followed throughout the review.
Data Extraction and Quality Assessment
Two authors (SUR and SOE) independently extracted data in duplicate from studies that met the
inclusion criteria to avoid any chance of misinterpretation of conceptualizations in each study.
Data were synthesized in two ways: (1) research design and intervention strategies were presented. (2) the findings of each study were analyzed qualitatively by collecting the main findings with the design and intervention applied. Furthermore, data extraction was carried out to provide a brief description of the articles' substance, such as the characteristics of the respondents and the characteristics of the study. Data extracted included author, year, country, participant, study design, Intervention, outcome, and main findings. The researchers then examined each extraction and any discrepancies were discussed until consensus was reached.
The quality of the articles included was measured using an assessment tool for the Effective Public Healthcare Panacea Project (EPHPP) [31] which allows experts to apply this tool to articles on any public health topics. This tool uses STRONG, MODERATE, and WEAK categorizations based on the assessment results on eight components, namely Selection Bias, Study Design, Confounders, Blinding, Data Collection Methods, Withdrawals, and Drop-outs, Intervention Integrity, and Analyzes. Articles in the STRONG category are the article reached four strong from the EPHPP component without any of the components being considered weak, the MODERATE category if four components reach strong. One component is rated "weak," and for the WEAK category, it is given if two or more components reach a "weak" value.
Data synthesis
Data from the included studies could not be pooled for meta-analysis because to the substantial diversity in the methodological design of the investigations. Consequently, the narrative synthesis of the included study findings was provided using the Synthesis without Meta-analysis in Systematic Reviews: Reporting Guideline [32].
RESULTS
Search Results
The process of searching for articles up to the determination of articles that meet the inclusion requirements can be illustrated in Figure 1.

Figure 1. PRISMA Flowchart for Literature Search
Search results from five databases yielded 486 articles according to the keywords applied, and then 159 articles were eliminated because they were duplicates, leaving 327 articles. Furthermore, the screening stage was carried out on the remaining articles; as many as 295 articles were excluded because they did not discuss the nutrition status in pregnancy. At the end of the screening, ten articles met the inclusion criteria (Table 2). Those were included in the moderate and robust categories based on the EPHPP assessment tool for article quality assessment.



Table 2. Extraction of Literature Included
Description of studies included
The articles reviewed in this study are located in several countries such as Iran [37], Ethiopia [34], USA [41], Brazil [33], Palestine [36], and Somalia [39]. Study design including Randomized Controlled Trial (RCT) [33–35,38,39,42], and Quasy experimental [36],[37,40,41].
Characteristics of participants
All reviewed studies included pregnant women with variations in gestational age including below 36 weeks (Oliveira et al., 2018), below 16 weeks [34,35] below 20 weeks [41,42], 14-16 weeks [36], 6-10 weeks [38], 18 – 24 weeks [40], 14-20 [41]. Two studies were not applied the gestational age [37,39].
Description of interventions
Some studies provided booklet regarding Healthy Diet during Pregnancy [33], Counseling regarding dietary practice [34], Nutrition education (theoretical session, poster, brochures, flipchart, and whiteboard) [35,37,40], theoretical and practical [36], the nutrition‑education intervention based on Pender’s HPM [38], video health information [39], exercise, self-monitoring, facebook private group [41], web-based health information [42].
A booklet entitled “Healthy Diet during Pregnancy with Regional Foods (Alimentação Saudável na Gravidez com os Alimentos Regionais)” was used as the main intervention which contains the concept of healthy nutrition, allowed and avoided foods during pregnancy, the benefits of healthy dietary habits for mothers and babies, food hygiene, and recipes with regional foods. The intervention group participated in the individual intervention in a private room, in a single session, with an average duration of 20 minutes. During the meeting, the booklet was introduced, read, and the patients kept a copy to take home [33].
The counseling model has also been used in a study in Ethiopia. The intervention package was community-based guided counseling using the HBM and the TPB. The core content of counseling guide including meal frequency, portion size with increasing gestational age and taking diversified meals, consumption of iron/folic acid supplementation, iodized salt use, reducing of a heavy workload, taking day rest, use of impregnated bed nets, and health services. Counseling was given monthly using a counseling guide and leaflets with core contents. Individual Nutrition counseling was given through a home visit on non-working days. Each counseling session lasted for 40 to 60 minutes. Participants attended four counseling sessions during pregnancy. The first counseling was given before 16 weeks of gestation, the second and third counseling sessions were given during the second trimester of pregnancy, the fourth counseling was given during the early third trimester of pregnancy. The control group received nutrition education given by the health system [34].
Nutrition education intervention recorded in three studies was given to pregnant women between 1 and 4 months at baseline. The education was given every 15 days for 5 consecutive months. For intervention group, education intervention was given based on Health Belief Model theory: (1) susceptibility of the pregnant women and fetus to malnutrition due to inappropriate dietary practices nutrient deficiency or over nutrient intake; (2) severity of malnutrition such as wasting/thinness and overweight/obesity and high risk of fetus to intrauterine growth retardation, brain development, and cognitive function due to macro- and micronutrient deficiency; (3) benefits of right eating or dietary practices on women nutritional status and fetus health, (4) barriers to practice appropriate good dietary practices; and (5) self-confidence/efficacy to follow right dietary practices. The education was provided using theoretical session, poster, brochures, flipchart, and whiteboard. For the control group, nutrition education was given by trained community health volunteers based on the general usual nutrition education which is currently provided by health extension workers [35]. Fallah et al [37] conducted face-to-face nutritional education which contains two to four lessons based on a nutrition package by Iranian ministry of health. Another study by Shakeri [40] nutrition education conducted in groups of 12 people, held in 8 sessions each planned for three sections taking 90 minutes. An educational CD, educational booklet, tract, and pamphlet about the advantages of good nutrition for mothers and embryo, appropriate ways of doing activities during pregnancy, and false beliefs were given to the participants. Furthermore, lecture, question and answer, group discussion, and film screening methods were used to educate the patients. Paticipants in control group received the routine prenatal instructions [40].
The complementary nutritional intervention (CNI) program proposed by Al-Tell and colleague, it was developed based on the educational principles using the principles of health belief model that aimed to behavior change. The program composed of two parts that were presented within 16 hours and through 8 grouped sessions, in addition to another 2 individualized/ follow-up session for each woman. The content of the theoretical part consisted of 60% of program hours, and the practical part consisted of 40% of program hours. The study also used educational booklet for additional materials. It included information regard iron deficiency anemia in term of causes, complication, treatment inhibitors and promoters of iron absorption and examples of prepared meals rich of iron [36].
Khoigani and colleague conducted nutritional education based on the Pender’s HPM for intervention group, included three 45 – 60 minutes training sessions in 6 – 10, 18, and 26 weeks of pregnancy. Each participant had a meeting with the study nutritionist at the time of enrollment for nutritional assessment. In the first session, the dietary pattern, including the average daily servings of five food groups, was explained to the participants. In the second session, practical steps (goal‑setting techniques) to increase self‑efficacy [38].
Destephano et al evaluated the use of DVD to spread information about caesarean birth, episiotomy, nutrition and exercise, the father’s role, preparation and prevention, and pregnancy myths and facts. Each video topic ranged from 3 to 4 min in length, incorporated
traditional songs and poetry, and had English subtitles [39].
Baruth et al used the social cognitive theory to develop SELF intervention (Supporting hEaLthy Futures: Creating a Healthy Family by Investing in YourSELF). The intervention included four key components: Exercise is Medicine™, self-monitoring, opportunities for support, and walking groups (optional). In self monitoring, Participants were given a FitBit Charge to monitor their physical activity (daily) and an Eat Smart Precision digital scale (model ESBS-01) to monitor their weight. Participants were instructed to weigh themselves once a week using the scale provided, and enter their weight into their FitBit account [41].
Participants (control and intervention groups) in Olson et al [42] trials given access to the intervention website and to the placebo control website. The self-directed, integrated online and mobile phone behavioral intervention was designed using the Integrative Model of Behavior Prediction and the Behavior Model for Persuasive Design based on a non-electronic pregnancy lifestyle intervention. Participants in intervention group received access to three behavior change tools including a weight gain tracker, a diet and a physical activity goal-setting and self-monitoring tool, as well as, health information including tips, articles, frequently asked questions; a description of pregnancy and parenting-related resources available in the local community; a blogging tool; and an event and appointment reminder [42].
Quality Assessment
Assessment of the methodological quality of studies resulted in 6 studies with a high quality score [33–35,38,41,42] and 4 studies with a moderate quality score [36,37,39,40].
Description of Outcomes
Outcome measures reported in the included studies were Knowledge, attitude, practice [33–35,37,39,40], Dietary practices [34,35,38], Gestational Weight Gain (GWG) [41,43], behavior change [42], Hemoglobin blood level [36]. One study collected the result of outcomes measurement immediately after the intervention [39], Three studies conducted the evaluation in two times for 6 weeks [40], 5 months [36], and 8 months [42]. The rest of the studies evaluated the outcomes in the range of one to five months [33–35,37,38,41].
As mentioned in Oliveira et al study, the knowledge was considered adequate when used to prepare varied meals and/or juices, knew three or more types of regional foods, and mentioned at least two types of meals prepared with regional foods. The attitude was considered adequate when pregnant women prefer to use regional foods and know the advantages. The practice was considered adequate when pregnant women referred to use regional foods at least twice a day [33]. In Diddana study, knowledge measurement is based on the Health Belief Model consists of 15 nutrition question [35]. In Fallah study, Knowledge as a primary outcome was measured before the intervention and two posttests within three weeks interval [37]. Another study in Iran with knowledge and attitude as primary outcome completed the evaluation immediately and 6 weeks after the educational intervention for the samples of experimental and control groups [40].
For dietary practice outcome, assessment used a food frequency questionnaire (FFQ) collected between 36 to 37 weeks of gestation. Women who didn’t attend all counseling sessions were considered non-adherent to the guideline. But, women who withdraw from participating in the study were labeled as lost to follow up [34]. In Diddana study, dietary practice variable was collected by using 17 dietary habit questions [35].
DISCUSSION
Overview study included
This review provides evidence that interventions with a health education on pregnancy issue can improve pregnant women knowledge, attitude, practice, dietary pattern, awareness, hemoglobin level, and weight gain outcomes. There is somewhat more persuasive evidence that health education interventions are favorably linked with healthy living change during pregnancy of pregnant women as participants due to the number of RCTs that revealed significant findings. Because of the high variability of research designs and methodology utilized in the included papers, meta-analysis cannot be conducted. Furthermore, the goal of this evaluation was to serve as a first step in identifying evidence-based treatments that would help transfer prenatal nutrition research and guidelines into practice. Although the evidence highlighting the importance of nutritional status during pregnancy has been documented, and numerous practice guidelines, including the recently consolidated inter-professional practice guidelines, have existed for some time, there is still a significant gap in translating this evidence to pregnant women through health promotion efforts. Overall, there are few dietary promotion treatments during pregnancy, and only 10 interventions have been assessed on specified health outcomes, according to this analysis.
Overall, the studies comprised a wide range of pregnant women from six different nations, resulting in some findings. Furthermore, all of the research was done in a communal context. A previous evaluation noted that complete prenatal care treatments should be available in remote regions or with less infrastructure and that their duties and those of trained CHWs should be harmonized across nations to assure basic levels of care [44]. Pregnant women who did not take advantage of offered interventions, so missing out on the possibility of a better pregnancy outcome, exemplified the lack of access to services in remote regions [45].
We recommend that maternal and family health service managers at the national, state, and local levels devote resources to adapting and testing existing culinary nutrition programs or, as appropriate, developing new culinary nutrition programs tailored to these life stages, as a result of the potential benefits of culinary nutrition interventions during pregnancy and postpartum identified in this review. Culinary nutrition programs for pregnant or postpartum women might be incorporated into existing health education programs or offered separately. A workforce with culinary nutrition expertise in maternity and family health care would be required to support such initiatives.
Nutrition Education
For this group is included in the demographic group prone to nutrition and health concerns, nutrition education is crucial during pregnancy [46]. According to cross-sectional research, pregnant women's understanding of nutrition during pregnancy went from 53.9 percent to 97 percent after receiving nutrition education, while their pregnancy-specific dietary practices increased from 46.8 percent to 83.7 percent [47].
Besides knowledge, GWG is also an important issue to be discussed In both the short and long term, excessive GWG is linked to unfavorable health outcomes for mother and child health [48]. Excess GWG is linked to an increased risk of hypertensive disorders [49], glucose intolerance [50] and and poor delivery outcomes during pregnancy [51]. It also predicts more significant baby morbidity and fetal development, such as birth weight, big for gestational age, and macrosomia, among other things [52].
Olson et al., [42] In their experiment, a self-directed, integrated online and mobile phone behavior modification intervention failed to show a beneficial effect on the proportion of the sample with excessive total GWG when compared to an information-only placebo control condition (which is included in this review). It was most likely discovered because the intervention was self-directed. That may have been a wrong decision. Structured, personalized treatments were more likely to be successful in promoting dietary change, according to a recent assessment of the research on e-behavioral nutrition interventions [42].
One research included in this review, which focuses on the hemoglobin blood level as an outcome, was done in Palestine. Compared to the control group, the study found a substantial beneficial link between dietary behaviors and improved hemoglobin levels. Compared to the control group, there was also a good connection between maternal hemoglobin levels in the third trimester and tiredness levels in the study group [36]. According to review research, nutrition education such as counseling, web-based, and text messages may enhance pregnant women's adherence to iron supplements. The research also stressed the significance of a more extended trial period to assess the intervention's effectiveness correctly [53].
According to the World Health Organization, pregnant women who reside in areas with high nutritional deficits should get some primary nutritional treatment. Nutrition counseling on a healthy diet, energy and protein dietary supplements, iron and folic acid supplementation (all settings), calcium supplementation to reduce the risk of pre-eclampsia in settings where dietary calcium intake is low. Zinc supplementation is only recommended for pregnant women in the context of rigorous research, and multiple micronutrient supplementation is all recommended in settings where 20% or more of women are underweight. Nonetheless, in areas where nutritional shortages are common, several micronutrient supplements include iron and folic acid, may be recommended for maternal health [54].
CONCLUSION
Nutrition education in many methods has a power to improve knowledge, and dietary change of pregnant women. However, there is a need for future large high quality trials using a standardized approach to measuring and reporting similar findings across studies. A future study might use a double-blind RCT approach with larger sample size and a variety of nutritional outcomes. Longer duration in implementing the trials will improve the outcomes of the study as expected.
Limitation
Our study has several flaws, including a lack of access to the most often recommended databases for searching relevant literature and, ultimately, trial trials. Some research relied on self-reported outcome measures, which might be vulnerable to various biases (e.g., recall bias and response bias). Because some of the studies are of intermediate quality, their conclusions should be read with care. We should also consider that non-English paper were not considered and included in this review, with a potential bias to not identify as many eligible studies as possible.
Conflict of interest statement
The author(s) declares no conflict of interest.
Funding statement
This research did not receive any specific grant from funding agencies in the public, commercial, or not for profit sectors.
Acknowledgements
We express our gratitude to the director of Jambi University for its support for the implementation of this research and President of Jambi University, Indonesia
REFERENCES
- Ho A, Flynn AC, Pasupathy D. Nutrition in pregnancy. Obstetrics, Gynaecology & Reproductive Medicine. 2016;26(9):259–64.
- Woldeamanuel GG, Geta TG, Mohammed TP, Shuba MB, Bafa TA. Effect of nutritional status of pregnant women on birth weight of newborns at Butajira Referral Hospital, Butajira, Ethiopia. SAGE open medicine. 2019;7:2050312119827096.
- Sokulmez P OA. Effects of General Health and Nutritional Status of Pregnant Adolescents on Newborn Health. Journal of Turkish Society of Obstetrics & Gynecology. 2014;11(1).
- Momin M, Jain V, Momin S, Kulkarni V. Nutritional Management for Pregnant Women-an extended role of Pharmacist. Journal of Pharmacy Research. 2012;5(12).
- Fleming TP, Watkins AJ, Velazquez MA, Mathers JC, Prentice AM, Stephenson J, et al. Origins of lifetime health around the time of conception: causes and consequences. The Lancet. 2018;391(10132):1842–52.
- Sebastiani G, Andreu-Fernández V, Herranz Barbero A, Aldecoa-Bilbao V, Miracle X, Meler Barrabes E, et al. Eating Disorders During Gestation: Implications for Mother’s Health, Fetal Outcomes, and Epigenetic Changes. Frontiers in pediatrics. 2020;8:587.
- Ronto R, Wu JHY, Singh GM. The global nutrition transition: trends, disease burdens and policy interventions. Public health nutrition. 2018;21(12):2267–70.
- Popkin BM. Global changes in diet and activity patterns as drivers of the nutrition transition. In: Emerging societies-coexistence of childhood malnutrition and obesity. Karger Publishers; 2009. p. 1–14.
- Smith LP, Ng SW, Popkin BM. Trends in US home food preparation and consumption: analysis of national nutrition surveys and time use studies from 1965–1966 to 2007–2008. Nutrition journal. 2013;12(1):1–10.
- Juul F, Hemmingsson E. Trends in consumption of ultra-processed foods and obesity in Sweden between 1960 and 2010. Public health nutrition. 2015;18(17):3096–107.
- Sweetman C, McGowan L, Croker H, Cooke L. Characteristics of family mealtimes affecting children’s vegetable consumption and liking. Journal of the American Dietetic Association. 2011;111(2):269–73.
- Wolfson JA, Bleich SN. Is cooking at home associated with better diet quality or weight-loss intention? Public health nutrition. 2015;18(8):1397–406.
- Lavelle F, Hollywood L, Caraher M, McGowan L, Spence M, Surgenor D, et al. Increasing intention to cook from basic ingredients: A randomised controlled study. Appetite. 2017;116:502–10.
- Herbert J, Flego A, Gibbs L, Waters E, Swinburn B, Reynolds J, et al. Wider impacts of a 10-week community cooking skills program-Jamie’s Ministry of Food, Australia. BMC public health. 2014;14(1):1–14.
- Berti C, Decsi T, Dykes F, Hermoso M, Koletzko B, Massari M, et al. Critical issues in setting micronutrient recommendations for pregnant women: an insight. Maternal & child nutrition. 2010;6:5–22.
- Jun S, Gahche JJ, Potischman N, Dwyer JT, Guenther PM, Sauder KA, et al. Dietary supplement use and its micronutrient contribution during pregnancy and lactation in the United States. Obstetrics and gynecology. 2020;135(3):623.
- Dubois L, Diasparra M, Bédard B, Colapinto CK, Fontaine-Bisson B, Morisset A-S, et al. Adequacy of nutritional intake from food and supplements in a cohort of pregnant women in Québec, Canada: the 3D Cohort Study (Design, Develop, Discover). The American journal of clinical nutrition. 2017;106(2):541–8.
- Pava-Cárdenas A, Vincha KRR, Vieira VL, Cervato-Mancuso AM. Promoting healthy eating in primary health care from the perspective of health professionals: a qualitative comparative study in the context of South America. BMC nutrition. 2018;4(1):1–11.
- Sharma P, Rani MU. Effect of digital nutrition education intervention on the nutritional knowledge levels of information technology professionals. Ecology of food and nutrition. 2016;55(5):442–55.
- Ota E, Hori H, Mori R, Tobe‐Gai R, Farrar D. Antenatal dietary education and supplementation to increase energy and protein intake. Cochrane Database of Systematic Reviews. 2015;(6).
- Hanson MA, Bardsley A, De‐Regil LM, Moore SE, Oken E, Poston L, et al. The International Federation of Gynecology and Obstetrics (FIGO) recommendations on adolescent, preconception, and maternal nutrition:“Think Nutrition First”#. International Journal of Gynecology & Obstetrics. 2015;131:S213–53.
- Lee A, Newton M, Radcliffe J, Belski R. Pregnancy nutrition knowledge and experiences of pregnant women and antenatal care clinicians: A mixed methods approach. Women and Birth. 2018;31(4):269–77.
- Marques AH, O’Connor TG, Roth C, Susser E, Bjørke-Monsen A-L. The influence of maternal prenatal and early childhood nutrition and maternal prenatal stress on offspring immune system development and neurodevelopmental disorders. Frontiers in neuroscience. 2013;7:120.
- Gernand AD, Schulze KJ, Stewart CP, West KP, Christian P. Micronutrient deficiencies in pregnancy worldwide: health effects and prevention. Nature Reviews Endocrinology. 2016;12(5):274–89.
- Borge TC, Aase H, Brantsæter AL, Biele G. The importance of maternal diet quality during pregnancy on cognitive and behavioural outcomes in children: a systematic review and meta-analysis. BMJ open. 2017;7(9):e016777.
- Fadare O, Amare M, Mavrotas G, Akerele D, Ogunniyi A. Mother’s nutrition-related knowledge and child nutrition outcomes: Empirical evidence from Nigeria. PloS one. 2019;14(2):e0212775.
- Lindqvist M, Lindkvist M, Eurenius E, Persson M, Ivarsson A, Mogren I. Leisure time physical activity among pregnant women and its associations with maternal characteristics and pregnancy outcomes. Sexual & Reproductive Healthcare. 2016;9:14–20.
- Aşcı Ö, Rathfisch G. Effect of lifestyle interventions of pregnant women on their dietary habits, lifestyle behaviors, and weight gain: a randomized controlled trial. Journal of Health, Population and Nutrition. 2016;35(1):1–9.
- Caut C, Leach M, Steel A. Dietary guideline adherence during preconception and pregnancy: A systematic review. Maternal & child nutrition. 2020;16(2):e12916.
- Moher D, Liberati A, Tetzlaff J, Altman DG, Group P. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS medicine. 2009;6(7):e1000097.
- Armijo‐Olivo S, Stiles CR, Hagen NA, Biondo PD, Cummings GG. Assessment of study quality for systematic reviews: a comparison of the Cochrane Collaboration Risk of Bias Tool and the Effective Public Health Practice Project Quality Assessment Tool: methodological research. Journal of evaluation in clinical practice. 2012;18(1):12–8.
- Campbell M. E McKenzie J. Sowden A, Katikireddi SV, E Brennan S, Ellis S, Hartmann-Boyce J, Ryan R, Shepperd S, Thomas J, et al Synthesis without meta-analysis (SWiM) in systematic reviews: Reporting guideline BMJ. 2020;368:l6890.
- Oliveira SC de, Fernandes AFC, Vasconcelos EMR de, Ximenes LB, Leal LP, Cavalcanti AMTS, et al. Effect of an educational intervention on pregnancy: a cluster-randomized clinical trial. Acta Paulista de Enfermagem. 2018;31:291–8.
- Demilew YM, Alene GD, Belachew T. Effect of guided counseling on dietary practices of pregnant women in west Gojjam zone, Ethiopia. Plos one. 2020;15(5):e0233429.
- Diddana TZ, Kelkay GN, Dola AN, Sadore AA. Effect of nutrition education based on health belief model on nutritional knowledge and dietary practice of pregnant women in Dessie Town, Northeast Ethiopia: A cluster randomized control trial. Journal of Nutrition and Metabolism. 2018;2018.
- AL-TELL MA, EL-GUINDI FK, SOLIMAN NM, EL-NANA H. Effect of nutritional interventions on anemic pregnant women’s health using health promotion model. The Medical Journal of Cairo University. 2010;78(2).
- Fallah F, Pourabbas A, Delpisheh A, Veisani Y, Shadnoush M. Effects of nutrition education on levels of nutritional awareness of pregnant women in Western Iran. International journal of endocrinology and metabolism. 2013;11(3):175.
- Goodarzi-Khoigani M, Moghadam MHB, Nadjarzadeh A, Mardanian F, Fallahzadeh H, Mazloomy-Mahmoodabad S. Impact of nutrition education in improving dietary pattern during pregnancy based on pender’s health promotion model: A randomized clinical trial. Iranian journal of nursing and midwifery research. 2018;23(1):18.
- DeStephano CC, Flynn PM, Brost BC. Somali prenatal education video use in a United States obstetric clinic: A formative evaluation of acceptability. Patient Education and Counseling. 2010;81(1):137–41.
- Shakeri M. The effect of educational program based on basnef model on the nutritional behavior of pregnant women. Int Res J Applied Basic Sci. 2013;5(12):1606–11.
- Baruth M, Schlaff RA, Deere S, Walker JL, Dressler BL, Wagner SF, et al. The feasibility and efficacy of a behavioral intervention to promote appropriate gestational weight gain. Maternal and child health journal. 2019;23(12):1604–12.
- Olson CM, Groth SW, Graham ML, Reschke JE, Strawderman MS, Fernandez ID. The effectiveness of an online intervention in preventing excessive gestational weight gain: the e-moms roc randomized controlled trial. BMC pregnancy and childbirth. 2018;18(1):1–11.
- Olson CM. Behavioral nutrition interventions using e-and m-health communication technologies: a narrative review. Annual review of nutrition. 2016;36:647–64.
- Nishimwe C, Mchunu GG, Mukamusoni D. Community‐based maternal and newborn interventions in Africa: Systematic review. Journal of Clinical Nursing. 2021;
- Konje ET, Magoma MTN, Hatfield J, Kuhn S, Sauve RS, Dewey DM. Missed opportunities in antenatal care for improving the health of pregnant women and newborns in Geita district, Northwest Tanzania. BMC pregnancy and childbirth. 2018;18(1):1–13.
- Teweldemedhin LG, Amanuel HG, Berhe SA, Gebreyohans G, Tsige Z, Habte E. Effect of nutrition education by health professionals on pregnancy-specific nutrition knowledge and healthy dietary practice among pregnant women in Asmara, Eritrea: a quasi-experimental study. BMJ Nutrition, Prevention & Health. 2021;bmjnph-2020.
- Zelalem A, Endeshaw M, Ayenew M, Shiferaw S, Yirgu R. Effect of nutrition education on pregnancy specific nutrition knowledge and healthy dietary practice among pregnant women in Addis Ababa. Clinics in Mother and Child Health. 2017;14(3):265.
- Goldstein RF, Abell SK, Ranasinha S, Misso M, Boyle JA, Black MH, et al. Association of gestational weight gain with maternal and infant outcomes: a systematic review and meta-analysis. Jama. 2017;317(21):2207–25.
- Boyle A, Timofeev J, Halscott T, Desale S, Driggers RW, Ramsey PS. Is 40 the new 30?: pregnancy outcomes by degree of weight gain among obesity subclasses. Obstetrics & Gynecology. 2014;123:41S.
- Berntorp K, Anderberg E, Claesson R, Ignell C, Källén K. The relative importance of maternal body mass index and glucose levels for prediction of large-for-gestational-age births. BMC pregnancy and childbirth. 2015;15(1):1–8.
- Wu Y, Wan S, Gu S, Mou Z, Dong L, Luo Z, et al. Gestational weight gain and adverse pregnancy outcomes: a prospective cohort study. BMJ open. 2020;10(9):e038187.
- Chen C-N, Chen H-S, Hsu H-C. Maternal prepregnancy body mass index, gestational weight gain, and risk of adverse perinatal outcomes in Taiwan: a population-based birth cohort study. International journal of environmental research and public health. 2020;17(4):1221.
- Gomes F, Bergeron G, Bourassa MW, Dallmann D, Golan J, Hurley KM, et al. Interventions to increase adherence to micronutrient supplementation during pregnancy: a protocol for a systematic review. Annals of the New York Academy of Sciences. 2020;1470(1):25.
- World Health Organization (WHO). Mainstreaming nutrition through the life-course. Essential Nutrition Actions. 2019.
![]() This work is licensed under a Creative Commons
This work is licensed under a Creative Commons
Attribution-NonCommercial-NoDerivatives 4.0 International License.
The influence of mobile app in Glycemic Control and Prevention of Hypoglycemics in Diabetic management: A Systematic Review
Netha Damayantie1* Muhammad Rusdi2, Syamsurizal2, Ummi Kalsum3
1 Student of Doctoral Programme faculty of Mathematic and and science, Jambi University
2 Chemical Education Study Program, Teacher Training and Education Faculty, Jambi University
3Public Health Study Program, Medicine and Health Sciences Faculty, Jambi University
* Corresponding author: Netha Damayantie, Jl. Jambi - Muara Bulian No.KM. 15, Mendalo Darat, Kec. Jambi Luar Kota, Kabupaten Muaro Jambi, 36129, Indonesia, Orcid : https://orcid.org/0000-0002-5628-2700. Email: netha.dam.57@gmail.com

Cita questo articolo
Abstract
Background. The use of technology in the treatment of diabetes can facilitate the medium of communication between nurses and clients in data collection to create a comfortable life for patients. The use of mobile health technology in diabetic education is an innovative learning method that can engage patients and influence positive health behaviors.
Aim. This study aims to find out the influence of mobile-based education applications in the Haemoglobin A1c control and prevention of hypoglycemia in patients with type 2 diabetes mellitus.
Methods. Database search for article are from four databases such as Pubmed, Sciencedirect, Proquest, and Cochrane is limited to the publication of the last ten years from 2010 to 2021 and full text article in English. Authors individually screened the titles and abstracts, then full articles in order to obtain papers that met inclusion criteria
Results. a total of 664 references were found. After duplicates were removed, 391 potentially relevant references remained from the database searches. Eight articles were finally designated as articles to be reviewed and use RCT design. Most studies put a Haemoglobin A1c (HbA1c) as a primary outcomes, and hypoglycemia as a secondary outcomes. Through the use of mobile app, there are reductions in HbA1c which affect the hypoglycemia events in Type 2 DM patients.
Conclusion. Mobile application can enhance HbA1c and hypoglycemia control among T2DM patients. Because providing patient education face to face is time-consuming, the use of mobile application may be an effective complement or alternative for healthcare professionals to manage the rapidly increasing number of diabetes patients.
Keywords: Mobile app, Type 2 DM, Glycemic control, Hypoglicemia prevention
Introduction
Diabetes mellitus, particularly type 2, is a global health issue in the worldwide. The International Diabetes Federation (IDF) estimated an escalation of diabetes prevalence from 424.9 million in 2017 to about 628.6 million by 2045 [1]. More than 10,3 million people had diabetes mellitus in Indonesia [2]. Ninety percent (90%) of diabetes cases is type 2 diabetes mellitus with characteristics of insulin sensitivity disorders and/or impaired insulin secretion [3]. The prevalence of diabetes mellitus in Indonesia based on doctor's diagnosis in the population aged ≥15 years has increased from 1.5% in 2013 to 2.0% in 2018 [4,5]. Administration of insulin therapy causes the main side effect of hypoglycemia. Another side effect is the immune response to insulin which can lead to insulin allergies or insulin resistance [3]. Hypoglycemia is a condition in which glucose levels in the blood decrease below the value of 70 mg / dl or less [6,7].The prevalence of hypoglycemia with type II diabetes mellitus patients can reach 70-80%, which has a serious impact on morbidity, mortality, and quality of life [8]. Severe occurrence of hypoglycemia in type 2 diabetes mellitus patients reaches 3-73 episodes per 100 patients annually [6]. A common phenomenon in the clinical practice is that many patients argue that mild hypoglycemia as a consequence of hypoglycemic control [9]. In addition, many patients misunderstand the symptoms of hypoglycemia as a symptom of ketoacidosis, because they need to reduce or delay insulin administration [10]. Patients attempted to lower blood sugar levels without knowing the effects of using the drug where patients may experience severe hypoglycemia as the result. One of the reasons for the lack of patient knowledge about hypoglycemia is the lack of information provided by healthcare professionals [11]. Shreds of evidence have shown that the potential use of smartphone-based technology has helped people with diabetes in self-care management by staying connected with health care providers. Futuristic features are provided with all the ease to understand and use [12,13]. A well-suited App could transform a mobile phone into a medical device helping ease the burden of diabetes, preventing complications, and improving a patient’s quality of life. However, an overwhelming number of products and services are available to patients with diabetes. Patients and providers must recognize the characteristics of these products and services to capitalize on the advantages while avoiding harmful deficiencies [14]. The use of technology in the treatment of diabetes can facilitate the medium of communication between nurses and clients in data collection to create a comfortable life for patients. An important goal of treatment with electronic media is to enable patients the opportunity to maintain effective they education without interruption [12]. Interest in mobile health apps in supporting self-management of health arises because it is easily accessible, portable, low cost, convenient for users, and has a widespread. Furthermore, 50% of smartphone users will have at least one mobile health app [13]. The use of mobile health technology in diabetic education is an innovative learning method that can engage patients and influence positive health behaviors [14].
This review aims to collate and provide evidence related to mobile application for Glycemic Control, and prevention of hypoglycemia of Diabetes Melitus patients.
Methods
Design
This study is a systematic review based on Preferred Reporting Items for Systematic Reviews and Meta-Analyzes (PRISMA). PRISMA is an evidence-based minimum set of items for reporting in systematic reviews and meta-analyses. PRISMA focuses on the reporting of reviews evaluating randomized trials, but can also be used as a basis for reporting systematic reviews of other types of research, particularly evaluations of interventions. Authors must use PRISMA as a guideline and theory underlying aims to help authors improve the reporting of systematic reviews and meta-analyses (PRISMA Statement, 2015).
Eligibility
Inclusion criteria for this systematic review are (1) adult-elderly patients (18-85 years), (2) uncomplicated or non co morbid diabetes mellitus patients, and (3) patients who are conscious and cooperative (4) study design that include in this review is randomized control trials (RCT). Exclusion criteria in this systematic review are (1) patients experiencing complications (stroke, heart, kidney), and (2) patients who have dementia and aphasia.
Search Methods
Database search for article are from four databases such as Pubmed, Sciencedirect, Proquest, and Cochrane is limited to the publication of the last ten years from 2010 to 2021 and full text article in English. Keywords used in the article search of all databases are combination of "diabetes mellitus" OR “Type 2 DM” AND "glycemic control” OR “Hypoglicemia prevention” OR “HbA1c” AND "health education" AND “m-health" OR “Mobile app”. The next step after the articles that meet the criteria are collected is to analyze and form the articles according to the specified inclusion and exclusion criteria. The article search process was carried out in August 2021. The article search uses keywords that have been determined by the researchers and limits the inclusion and exclusion criteria. The data obtained are then selected one by one by the researchers to determine the suitability of the articles desired by the researchers and delete the same articles or those that do not fit the criteria. After getting the articles according to the researchers, the articles are analyzed one by one and grouped to get the results. The next step is to discuss based on the points obtained from the selection results.
Critical appraisal
The included quantitative studies were appraised using the McMaster Critical Review Form for quantitative studies [18]. The critical appraisal process was undertaken independently by the two authors. Discrepancies in scoring were then resolved through discussions until consensus was achieved.
There are 13 question items that can be answered with yes, no, and not addressed options. Scores are given as a percentage, and one point for each question item if available. 90% were categorized as high quality, 70% medium, and low quality for the rest.
Data Abstraction
Two authors independently reviewed the abstracts of studies retrieved from the database Search and read the full-text of potentially relevant articles. For studies that met the inclusion criteria, data extraction was independently conducted by two investigators using our data extraction tool adapted from existing guidelines and other review articles of mobile application for DM [19,20]. Using this tool we extracted the general and mobile app features of the papers including the outcome, study design, characteristics of the intervention, evaluation method and main findings. Disagreements in data extraction were solved by a third investigator.
Data Analysis/ Synthesis
Data of the studies included were synthesized thematically in order to understand the effectiveness of mobile application. Thematic analysis involves discovering, interpreting and reporting patterns and clusters of meaning within the data. Using this frame-work and by reading the included articles several times, themes were identified. Subsequently, these themes were further examined for their similarities, differences and contradictions. The subject matter of the findings from the quantitative studies was examined, and the resulting information was placed under the qualitative themes. This integration of quantitative findings to the qualitative themes was completed by the first author. The second author reviewed the matched themes and quantitative studies. Any disagreement was resolved through mutual discussion. Due to the heterogeneity and insufficient number of the studies included, we could not conduct meta-analyses.
Results
Search Results
Combining the output of the searches in the various databases, a total of 664 references were found. After duplicates were removed, 391 potentially relevant references remained from the database searches. 283 articles removed by reasons of irrelevant, review/report, not full text, book chapter. Eight articles were finally designated as articles to be reviewed. PRISMA flowchart for Study selection can be presented in Figure 1.

Figure 1. PRISMA flowchart for Study selection
The main focus of this systematic literature review is the effects of mobile app on hypoglycemia prevention. However, to optimize the interpretation of these effects, we will first clarify the methodological quality and characteristics of the studies, as well as the characteristics of the mobile app under review. The authors developed tables for data analysis with the type of diabetes addressed in the review article, the types of technology used for the intervention along with outcomes measured. The most common health outcome measure was hemoglobin A1c (A1c), and hypoglycemia may present in secondary outcome. This shared data element allowed comparison between the varying interventions addressed in these reviews.
In Table 1 we reported the articles included in our study.






Table 1. Data extraction of studies included
The result of Critical review
The results of the critical appraisal of the studies are presented in Table 2, respectively. The data that contributed to the generation of these themes are presented narratively in the following results subsection, with the appropriate source references identified.

Table 2. Critical review for Quantitative studies included
Critical appraisal of quantitative research studies: As outlined in Table 2, all of the studies had a clear purpose and relevant literature reviews. All of the studies reported appropriate conclusions, given their study purpose.
Table 2 shows the value of Cohen's kappa coefficient in each article with a range of 0.41 to 0.806 with a moderate to strong category. This coefficient is the result of two reviewers who evaluate each article separately.
Study Characteristics
Most of the selected reviews used research from locations around the globe. Articles that meet the inclusion criteria come from several countries including China [21–23], USA [24,25], Norway [26], Japan [27], and France [28]. The mean age range reported was from 38 to 68 years old. Duration of the intervention was 3 months [27], 6 months [21,22,26], 9 months [23], and 12 months [24,25,28]. The number of participants involved in the study was in the range of 54 to 665 patients divided into intervention and control groups.
Outcomes Measured, Primary Focus
Primary outcomes
Change in HbA1c level after 1 year was chosen as the primary outcome because it is the main target measure when treating diabetes and is frequently used when evaluating interventions. HbA1c data were collected through the GPs and were assessed primarily with the Siemens DCA Vantage Analyzer a maximum of 2 weeks before or after the follow-up to reduce measurement bias [26].
In the study of Waki and colleague, HbA1c as a primary outcome was measured from baseline to 3-month follow-up for each patient with an intention-to-treat analysis in intervention and control groups [27].
The primary outcome of Quinn [25] study was change in glycated hemoglobin comparing control usual care (UC) and maximal treatment (Coach primary care providers portal with decision support (CPDS) at baseline versus 12 months. Medical chart reviews were used to ascertain patient data. For patients without a glycated hemoglobin within 4 months of the desired measurement, a glycated hemoglobin test was offered at no charge at baseline to determine eligibility and at 12 months. At baseline, glycated hemoglobin was measured using one device, the Bayer DCA 2000, by trained staff blinded to patient group assignment. At follow-up, if glycated hemoglobin was not ascertained within 14 days of the 12-month time point, reminders were provided to patients and physicians to complete the test. Glycated hemoglobin level at intermediate time points (3, 6, and 9 months) was collected from patients’ medical charts [24,25].
Franc et al. determined the primary outcomes of their study was the mean change in HbA1c from baseline to 12 months (primary endpoint), and the occurrence of hypoglycemia. An independent ‘‘Hypoglycemia Adjudication Committee’’ validated the classification of all declared hypoglycaemic episodes. A severe hypoglycemic episode means that the patient required the indispensable assistance of a third person. A symptomatic hypoglycemic episode refers to those symptoms of hypoglycemia associated with rapid recovery after self-administration of sugar [28].
The primary outcome in Xu et al study [22] was diabetic symptom scores. It was assessed by the diabetes symptom grading and quantitative scale according to the Guidelines for the Clinical Research of Chinese Medicine New Drugs. Secondary outcome was blood glucose level including fasting blood glucose, 2-h postprandial blood glucose (2 hPG), and glycated hemoglobin (HbA1c) at baseline and 6 months after intervention. Serum HbA1c level reflects a patient’s blood glucose concentration during the previous 2–3 months, so it was taken into consideration as an essential indicator [22].
The primary outcome in Zhang et al. study [29] was glucose control, including the changes (from baseline to months 3 and 6) in the HbA1c level. The major adverse event was hypoglycemia. Hypoglycemia was defined as BG ≤3.9 mmol/L [21].
In the Sun study, there were intervention and control groups. Primary outcome was self-administered blood glucose level. HbA1c level was measured at 3 and 6 months [23].
The primary outcome of Quinn study [24] was the change in HbA1c (% of total hemoglobin) in the control group versus in the intervention group, at baseline versus at 12 months. HbA1c levels were recorded at baseline and at 3, 6, 9, and 12 months. Patient data were retrieved from medical charts [24].
Intervention Features
We will describe a mobile application intervention based on each of the studies that we included in this review. Holmen et al., [26]: To increase self-management comprised of 3 intervention groups: the Few Touch Application (FTA) intervention group, the FTA with health counseling (FTA-HC) intervention group, and the control group. The FTA-HC group received health counseling for the first 4 months of the project period. The health counseling was based on the transtheoretical model of stages of change and a problem-solving model, and used motivational interviewing as a counseling technique. The health counseling in the present study was part of the mHealth intervention.
Waki et al., [27]. DialBetics is composed of 4 modules. First is the data transmission module: patients’ data—blood glucose, blood pressure, body weight, and pedometer counts. Second is the evaluation module: data are automatically evaluated following the Japan Diabetes Society (JDS) guideline’s targeted values. Third is the communication module: about meals, and advice on lifestyle modification. Fourth is dietary evaluation: patients’ photos of meals are sent to the server.
Quinn et al., [25]. The mobile software allowed patients to enter diabetes self-care data (blood glucose values, carbohydrate intake, medications, other diabetes management information) on a mobile phone and receive automated, real-time educational, behavioral, and motivational messaging specific to the entered data. The patient web portal augmented the mobile software application and consisted of a secure messaging center (for patient-provider communication), personal health record with additional diabetes information (e.g., laboratory values, eye examinations, foot screenings), learning library, and logbook to review historical data.
Franc et al., [28]. A reference nurse initiates the patient to the use of the DIABEO app on his smartphone. The patient enters relevant data (glycemia, physical activity, and ingested carbohydrates) and DIABEO calculates the insulin dose (an eventual dose adaptations). These data are sent every 2 h to a platform that is continuously visible by the reference nurse and the investigator.
Xu et al., [22]. The smartphone app for diabetes management was composed of 4 modules: syndrome differentiation, body differentiation and health preservation, thesaurus, and interactive follow-up. A reminder message would be received if the patients forget to complete that in time. The diabetes educators can track the data from the app and provide specific guidance and suggestions for the clients.
Zhang et al., [21]. Welltang app mainly comprises 4 parts: education, self-management (including records of SMBG, diet, exercise, medication, body weight, and other diabetes data), patient community, and communication between patients and clinicians. For clinicians, Welltang mainly provided the real-time uploading of data from patients.
Quinn et al., [24]. Mobile diabetes management software application (MDMA) allowed patients to enter diabetes self-care data (blood glucose values, carbohydrate intake, medications, and other diabetes management information) on a mobile phone and receive automated, real-time messages that were educational, behavioral, motivational, and specific to the entered data.
Sun et al., [23]. Patients uploaded the glucometer data to the mHealth management app which was then automatically transmitted to the medical server (glucometer was connected to the mobile phone via Bluetooth). The medical teams sent medical advice and reminders to patients to monitor their glucose levels via the personal messaging app or telephonically every 2 weeks.
Discussion
This systematic review provides an overview of studies on mobile applications in improving HbA1c and hypoglycemic control among T2DM patients. The highest decrease in HbA1c was 1.9% which is relatively high compared to several previous studies, which found a decrease in HbA1c of 0.49% [30] and 0.51% [31]. There was no subgroup analysis in studies involving patients in different age groups. In general, it can be concluded that mobile application interventions can provide the same benefits for younger (<55 years) or older (≥55 years) T2DM patients. It is inconsistent with findings from a previous systematic review [30], which suggested that ST interventions were more effective for younger T2DM patients than older patients. The mobile applications in the included studies are complex and generally include more than one component. Almost all studies evaluate mobile applications related to lifestyle modification and self-monitoring of blood glucose. Therefore, it is logical to conclude that a decrease in HbA1c is associated with improving the patient's lifestyle. Although quality improvement programs are usually multi-component, they are more oriented towards targeting changes in health care provider behavior or service delivery models [32]. Interventions using mobile applications have a stronger focus on empowering patient behavior change. A systematic review Barreira et al., [33] showed that exercise effectively reduced HbA1c. Of the four included studies, which have included a component of exercise adherence monitoring [23,26,27], this suggests that a mobile application may be an effective adjunct to controlling HbA1c, or It is more common to enhance lifestyle modification efforts among type 2 DM patients. These studies also suggest considering the mobile application as a complementary intervention that can be used in diabetes self-care strategies more effectively through lifestyle modification and self-monitoring blood glucose. In the included studies, self-monitoring of blood glucose was also included as part of a mobile application intervention, while its effectiveness in controlling DM was uncertain.
A previous systematic review study Xu et al., [34] concluded that SMBG only contributed to a 0.46% decrease in HbA1c. Available evidence suggests that SMBG can promote self-management, increase medication adherence rates, and improve the patient's ability to detect hypoglycemia [35]. However, the UK National Institute for Health and Care Excellence guidelines state that SMBG is not recommended as part of routine DM management but should be considered in subgroups of patients, such as those receiving insulin therapy and patients prone to hypoglycemia [36]. Current clinical practice guidelines recommend close monitoring of HbA1c and titration of drug therapy instead [37]. It was difficult for us to find relevant literature on mobile applications to reduce the risk of hypoglycemia in both type 1 and type 2 DM patients. Several studies that we included in this review made hypoglycemia a secondary outcome. The results obtained from the two studies stated that there was no significant difference between the intervention group and the control group. Reports of signs and symptoms of hypoglycemia occurred only once or twice in 1 year of follow-up [25,28]. However, post hoc analyses of the Action to Control Cardiovascular Risk in Diabetes (ACCORD) trial indicated an increased hypoglycemia risk in type 2 diabetic participants with poorer glycemic control than subjects with more desirable HbA1c levels, irrespective of assigned treatment group [38]. Based on this statement, it can be concluded that from all studies included in this review, the mobile application can provide an effect on controlling hypoglycemia levels in Type 2 DM patients, although it is not clearly stated how the mechanism is. Little is known about the relationship between glycemic control and hypoglycemia in the usual care setting, where clinical decision-making about treatment intensity occurs and is modified throughout a patient's life [39].
Based on the two studies included in this review, it appears that there is no significant effect of the use of mobile phone applications on the quality of life of people with diabetes. The possible cause of no significant change in the quality of life before and after using the application is the age of the participants, most of which are in the elderly who feel less interested in using technology, especially smartphone-based [26]. The elderly need more intensive guidance regarding the use of technology applications, usually the elderly ask to be accompanied by family members or people who care for them. For the elderly who feel the exhaustion of their illness, they often hand over the responsibility to the people who take care of them [40,41].
Conclusion
In conclusion, mobile application can enhance HbA1c and hypoglycemia among T2DM patients. Because providing patient education face to face is time-consuming, the use of mobile application may be an effective complement or alternative for healthcare professionals to manage the rapidly increasing number of diabetes patients. Because providing patient education face to face is time-consuming, the use of mobile application as an educational media may be an effective complement or alternative for healthcare professionals to manage the rapidly increasing number of diabetes patients. The evidence suggests that organizations, diabetes educators, policy makers, and payers should consider these solutions in the design of diabetes self-management education and support services for population health and value-based care models. With the widespread adoption of mobile phones, digital health solutions that incorporate evidence-based, behaviorally designed interventions can improve the reach of and access to diabetes self-management education and ongoing support.
Limitation
We have identified several limitations in this study, including limited access to several good-quality databases, which are expected to provide broader search results. In addition, studies that matched our inclusion criteria were also very limited with regard to hypoglycemic control. We also considered potential bias related to different intervention/app, duration of intervention, and the limited numbers of RCTs included. Also, in the search strategy, some important databases are missing.
Funding statement
This research did not receive any specific grant from funding agencies in the public, commercial, or not for profit sectors.
Competing interests statement
There are no competing interests for this study.
REFERENCES
- J.E. Shaw , R.A. Sicree PZZ. Global estimates of the prevalence of diabetes for 2010 and 2030. Australia; 2010.
- Kementrian Kesehatan RI. Suara Dunia Perangi Diabetes. Jakarta; 2018.
- Decroli E. Diabetes Mellitus Tipe 2. I. Kam, Alaxander; Efendi Y, editor. Padang; 2019.
- Kementrian Kesehatan RI. Laporan Nasional hasil Riskesdas 2013. Jakarta: Badan Penelitian dan Pengembangan kesehatan; 2013.
- Kementerian Kesehatan RI. Laporan Nasional Riskesdas 2018. Jakarta: Badan Penelitian dan Pengembangan kesehatan; 2019.
- ADA. Standars Of Medical Care In Diabetes — 2017 Standards of Medical Care in Diabetes d 2017. The Journal of Clinical and Applied Research and Education. 2017;40(January):S48–56.
- Soelistijo SA, Novida H, Rudijanto A, Soewondo P, Suastika K, Manaf A, et al. Konsensus Pengelolaan Dan Pencegahan Diabetes Melitus Tipe 2 Di Indonesia 2015. Edisi I. Buku Konsensus DM Tipe-2. Jakarta: PB Perkeni; 2015. 11–14 p.
- Setyohadi B. Kegawatdaruratan Penyakit Dalam. Jakarta: Pusat Penerbitan Ilmu Penyakit Dalam; 2011.
- Sudoyo, A.W; Alwi, SB; Marcellus,S S. buku Ajar Ilmu Penyakit Dalam. 1st ed. Jakarta: EGC; 2007.
- Hudak, Carolyn. M; Gallo B. Keperawatan kritis Pendekatan Holistik. 8th ed. Jakarta: EGC; 2012.
- Sutawardana JH. Phenomenology Study The Experience Of Persons With Diabetes Mellitus. Nurseline Journal. 2016;1(1):159–75.
- Arnhold M, Quade M, Kirch W. Mobile applications for diabetics: a systematic review and expert-based usability evaluation considering the special requirements of diabetes patients age 50 years or older. Journal of medical Internet research. 2014;16(4):e2968.
- Brzan PP, Rotman E, Pajnkihar M, Klanjsek P. Mobile applications for control and self management of diabetes: a systematic review. Journal of medical systems. 2016;40(9):1–10.
- Rose KJ, Petrut C, L’Heveder R, de Sabata S. IDF Europe’s position on mobile applications in diabetes. Diabetes research and clinical practice. 2019;149:39–46.
- Tavsanli NG, Karadacovan A, Saygili F. The use of videophone technology (telenursing) in the glycaemic control of diabetic patients: a randomized controlled trial. Journal of Diabetes Research and Clinical Metabolism. 2013;2(1):1.
- Miller AS, Cafazzo JA, Seto E, Seto E. A Game Plan: Gamification Design Principles in mHealth Applications for Chronic. Health Informatics Journal. 2014;1–10.
- Kho SES, Lim SG, Hoi WH, Ng PL, Tan L, Kowitlawakul Y. The development of a diabetes application for patients with poorly controlled type 2 diabetes mellitus. CIN - Computers Informatics Nursing. 2019;37(2):99–106.
- Law M, Stewart D, Pollock N, Letts L, Bosch J, Westmorland M. Critical review form–quantitative studies. McMaster University: Occupational Therapy Evidence-Based Practice Research Group. 1998;
- Liberati A, Altman DG, Tetzlaff J, Mulrow C, Gøtzsche PC, Ioannidis JPA, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. Journal of clinical epidemiology. 2009;62(10):e1–34.
- Sun C, Malcolm JC, Wong B, Shorr R, Doyle M-A. Improving glycemic control in adults and children with type 1 diabetes with the use of smartphone-based mobile applications: a systematic review. Canadian journal of diabetes. 2019;43(1):51–8.
- Zhang L, He X, Shen Y, Yu H, Pan J, Zhu W, et al. Effectiveness of Smartphone App–Based Interactive Management on Glycemic Control in Chinese Patients With Poorly Controlled Diabetes: Randomized Controlled Trial. Journal of medical Internet research. 2019;21(12):e15401.
- Huiwen XU, Yuan Y, Li Y, En TAKASHI AK. Effect of a traditional Chinese medicine theory-based mobile app on improving symptoms in patients with type 2 diabetes mellitus: A randomized controlled trial. Journal of Integrative Nursing. 2021;3(3):97–105.
- Sun C, Sun L, Xi S, Zhang H, Wang H, Feng Y, et al. Mobile phone–based telemedicine practice in older chinese patients with type 2 diabetes mellitus: randomized controlled trial. JMIR mHealth and uHealth. 2019;7(1):e10664.
- Quinn CC, Shardell MD, Terrin ML, Barr EA, Park D, Shaikh F, et al. Mobile diabetes intervention for glycemic control in 45-to 64-year-old persons with type 2 diabetes. Journal of Applied Gerontology. 2016;35(2):227–43.
- Quinn CC, Shardell MD, Terrin ML, Barr EA, Ballew SH, Gruber-Baldini AL. Cluster-randomized trial of a mobile phone personalized behavioral intervention for blood glucose control. Diabetes care. 2011;34(9):1934–42.
- Holmen H, Torbjørnsen A, Wahl AK, Jenum AK, Småstuen MC, Årsand E, et al. A mobile health intervention for self-management and lifestyle change for persons with type 2 diabetes, part 2: one-year results from the Norwegian randomized controlled trial RENEWING HEALTH. JMIR mHealth and uHealth. 2014;2(4):e3882.
- Waki K, Fujita H, Uchimura Y, Omae K, Aramaki E, Kato S, et al. DialBetics: a novel smartphone-based self-management support system for type 2 diabetes patients. Journal of diabetes science and technology. 2014;8(2):209–15.
- Franc S, Hanaire H, Benhamou P-Y, Schaepelynck P, Catargi B, Farret A, et al. DIABEO system combining a mobile APP software with and without Telemonitoring versus standard care: a randomized controlled trial in diabetes patients poorly controlled with a Basal-Bolus insulin regimen. Diabetes Technology & Therapeutics. 2020;22(12):904–11.
- Li X, Yu S, Zhang Z, Radican L, Cummins J, Engel SS, et al. Predictive modeling of hypoglycemia for clinical decision support in evaluating outpatients with diabetes mellitus. Current Medical Research and Opinion. 2019;35(11):1885–91.
- Hou C, Carter B, Hewitt J, Francisa T, Mayor S. Do mobile phone applications improve glycemic control (HbA1c) in the self-management of diabetes? A systematic review, meta-analysis, and GRADE of 14 randomized trials. Diabetes care. 2016;39(11):2089–95.
- Wu IXY, Kee JCY, Threapleton DE, Ma RCW, Lam VCK, Lee EKP, et al. Effectiveness of smartphone technologies on glycaemic control in patients with type 2 diabetes: systematic review with meta‐analysis of 17 trials. Obesity Reviews. 2018;19(6):825–38.
- Tricco AC, Ivers NM, Grimshaw JM, Moher D, Turner L, Galipeau J, et al. Effectiveness of quality improvement strategies on the management of diabetes: a systematic review and meta-analysis. The Lancet. 2012;379(9833):2252–61.
- Barreira E, Novo A, Vaz JA, Pereira AMG. Dietary program and physical activity impact on biochemical markers in patients with type 2 diabetes: A systematic review. Atencion primaria. 2018;50(10):590–610.
- Xu Y, Tan DHY, Lee JY. Evaluating the impact of self‐monitoring of blood glucose frequencies on glucose control in patients with type 2 diabetes who do not use insulin: a systematic review and meta‐analysis. International journal of clinical practice. 2019;73(7):e13357.
- Berard LD, Blumer I, Houlden R, Miller D, Woo V. Monitoring glycemic control. Canadian journal of diabetes. 2013;37:S35–9.
- Chung WK, Erion K, Florez JC, Hattersley AT, Hivert M-F, Lee CG, et al. Precision medicine in diabetes: a consensus report from the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetes care. 2020;43(7):1617–35.
- Nolan K, Shearn P, Gholitabar M, Richardson J. NICE Update NICE public health guidance update.
- Lipska KJ, Warton EM, Huang ES, Moffet HH, Inzucchi SE, Krumholz HM, et al. HbA1c and risk of severe hypoglycemia in type 2 diabetes: the Diabetes and Aging Study. Diabetes care. 2013;36(11):3535–42.
- Hong S, Preswala L, Harris YT, Romao I, Ross DW, Paz HA, et al. Hypoglycemia in Patients with Type 2 Diabetes Mellitus and Chronic Kidney Disease. Kidney360. 2020;
- Androutsou T, Kouris I, Anastasiou A, Pavlopoulos S, Mostajeran F, Bamiou D-E, et al. A smartphone application designed to engage the elderly in home-based rehabilitation. Frontiers in Digital Health. 2020;2:15.
- Paiva JO V, Andrade RMC, de Oliveira PAM, Duarte P, Santos IS, Evangelista AL de P, et al. Mobile applications for elderly healthcare: A systematic mapping. PloS one. 2020;15(7):e0236091.
![]() This work is licensed under a Creative Commons
This work is licensed under a Creative Commons
Attribution-NonCommercial-NoDerivatives 4.0 International License.
Nurses' experiences and emotions in the face of changes caused by the COVID-19 pandemic: a phenomenological study
Sara Muzzicato1, Lorenza Garrino2, Vincenzo Alastra2, Valeria Miazzo1
- Opera San Camillo Foundation, Turin
- Master Executive Narrative Practices in Care Professions, COREP, Turin
*Corresponding author: Sara Muzzicato, Department of Rehabilitation, Recovery and Functional Rehabilitation Level 2, Fondazione Opera San Camillo, Turin. Email: sara.muzzicato@gmail.com
Cita questo articolo
ABSTRACT
Introduction: Following the Covid-19 pandemic, healthcare personnel had to face a very difficult period linked to the healthcare emergency, with important repercussions from a professional and personal point of view. These aspects have been explored by numerous researches on an international level, but only a small number of articles have investigated the phenomenon in the Italian context. The aim of this research is to describe the experience of healthcare workers in a Covid ward, exploring their emotional responses.
Materials and Methods: The study consists of a qualitative research with a phenomenological approach according to Giorgi. Narrative interviews were used with healthcare workers who worked in a Covid ward at the San Camillo health centre in Turin, a hospital specialising in second level functional recovery and re-education.
Results: Through the field research, 12 interviews were collected, involving 9 nurses and 3 social-health workers, working in a ward dedicated to the care of Covid-19 patients. The common themes that emerged concerned: the beginning of the Covid operator's "journey", characterised by a profound change in professional life since the beginning of the pandemic; the whirlwind of emotions and feelings experienced (fear, feeling blocked, annulled, powerless, depersonalised by suits and masks, anguish due to both physical and psychological isolation, etc.); relations with family members and friends; the relationship with the patient's family; relations with the operators' families; the risk of contagion and the fear of infecting oneself and one's loved ones; the group as a handhold for not giving up, as a point of strength, union and trust; the awareness of change with the desire to take one's own life back into one's own hands, taking advantage of the good things this time can give.
Conclusions: The research highlights the ability of the operators to identify positive aspects in the experiences lived, the union and trust in the group and the support of the family despite the strong fear of contagion. There are also important suggestions to reinforce strategies for dealing with such health emergencies and the importance for each individual in feeling accompanied throughout the process, in the difficult challenges they face.
Keywords: Covid-19, Experiences, Nursing, Narrative, Phenomenological approach.
INTRODUCTION
On 31 December 2019, Chinese Health Authorities reported to the World Health Organisation a cluster of cases of pneumonia of unknown aetiology in the city of Wuhan, in China's Hubei province. On 9 January 2020, the Centre for Disease Control and Prevention of China reported that a new coronavirus (SARS-CoV-2)[1] was identified as the causative agent of the respiratory disease later named Covid-19. China made public the genome sequence that enabled a diagnostic test and on 30 January 2020, the World Health Organisation (WHO)[2] declared the Coronavirus outbreak in China to be an "International Public Health Emergency" [3,4]. From then on, the word 'COVID-19' has indicated the disease associated with the SARS-CoV-2 virus (severe acute respiratory syndrome coronavirus 2), characterised by mild symptoms (fever, sore throat, fatigue, muscle pain, loss of taste and smell) or more severe symptoms (pneumonia, respiratory failure)[5]. Such symptoms have often led to the need for intensive care[6,7], thus causing high pressure on hospitals struggling to cope with too many patients to care for [8]. In this catastrophic scenario linked to the epidemic, Italy was one of the countries most affected[9]. Between the beginning of February and 30 November 2020, 1,651,229 positive Covid-19 cases were diagnosed by Regional Reference Laboratories and reported to the Italian National Institute of Health (NIH) - Italian National Integrated Surveillance System by 20 December 2020[10].
The pandemic has had different intensities and lethality in Italy compared to the rest of Europe. Differences in lethality rates are explained by: demographics, as mortality tends to be higher in older populations with co-morbidities; characteristics of the healthcare system, where there are organisational shortcomings, initial delays in understanding the severity of the emergency, deficits in infection tracking systems, hospitals overwhelmed by admissions, etc.; differences in the number of people tested; and different levels of virus aggressiveness[11].
Italy faced an unprecedented health crisis, with serious shortages of health professionals and difficulties in procuring personal protective equipment. New organisational models had to be implemented and hospital inpatient facilities had to be rapidly transformed into units suitable for the care of pandemic patients[12].
The NIH weekly bulletin of 28 April 2020 stated that 47.4% of the cases of infection among healthcare personnel were nurses[13].
In Italy[14] according to the provincial records, 40 nurses died, 32 of whom with the Covid-19 disease (positive swab), 4 with Covid-related illness (for whom the viral pathology was a favourable factor) and 4 (positive in any manner) for whom the mode of death was suicide[15]. A different view of the same phenomenon is reported by the monitoring as of 15 June 2020 conducted by INAIL (Italian National Institute for Insurance against Accidents at Work). INAIL, considering the accident reports referring only to insured workers, certified that there were a total of 236 deaths from Covid-19, of which 40% were healthcare professionals and 61% were nurses. In this complex epidemiological and healthcare framework, healthcare personnel reported the consequences of significant psychophysical stress with experiences and emotions still largely to be explored. Arasli et al. (2020)[16] explored experiences during the Covid-19 pandemic through testimonies written by nurses on social media through qualitative research. The study showed a high level of stress among healthcare professionals related to the risk and fear of becoming infected. Labrague et al. (2020)[17], through a quantitative study conducted in a region of the Philippines, highlighted high dysfunctional levels of anxiety in frontline nurses, while recording an increase in their resilience. On the Italian scene, Catania et al. (2020)[18] carried out qualitative research involving nurses from all regions of the peninsula. This study highlighted the enormous impact of COVID-19 on nurses, the need to identify new working practices, and highlighted the high-risk nature of nursing, exacerbated by the difficulty in Personal Protective Equipment (PPE) availability. In addition to reporting the high levels of stress experienced by the interviewees, the element of narratives also highlighted the resilience of the nursing community. Qualitative research was conducted by De Vito et al.[19], through the narratives of paediatric doctors and nurses in the paediatric emergency room of the Regina Margherita hospital. The authors emphasise how much the number of admissions in the paediatric sector had fallen, reflecting profoundly on changes in care, but also on the relationship itself with and between patients.
The results of the study show how the act of describing helped participants to process and understand their experience. Storytelling provided a cathartic means for participants to reformulate the events they experienced, rationalising them and making sense of them. In the Turin landscape, the experiences of nursing students were investigated. Garrino et al. (2021)[20], through a qualitative study, emphasised the changes induced by Covid-19 in nursing education. The need to use distance learning and the impossibility of doing internships during the pandemic period created many difficulties in training students. The narrative approach[21] and reflective thinking[22] aim to capture the latent aspects and hidden meanings of the complex pandemic reality[23,24].
The aim of the research is to describe the experience of health workers on a Covid ward, exploring their experiences and emotions.
MATERIALS AND METHODS
Study design
In this study, a qualitative methodology was used to investigate subjective phenomena, based on the assumption that fundamental truths about reality are rooted in people's lived experiences. This method allows for exploration of experiences by the person who has them, attempting to describe the meanings that the individual creates and gives to that experience, understanding the structure, nature and form, as perceived by the individual[25]. This survey aims to understand the experience of nurses and social workers during the first wave in a ward caring for Covid-19 patients, and who are now called upon again to provide the same type of care, in order to find out how the workers in question have responded to a pandemic emergency which, in addition to involving the work aspect, has invaded the personal sphere.
Background
The San Camillo hospital, as a hospital specialising in second-level functional recovery and rehabilitation, provides intensive rehabilitation treatment in the post-acute phase of the illness. The hospital has five departments that fulfil this function.
In November 2020, during the second wave of the pandemic, two wards were dedicated to the care of Covid patients. The health workers of these two wards, defined as 'COVID staff', had to cope with this new situation with various difficulties that have also characterised many healthcare facilities in Italy, but in this second phase they were able to use sufficient and appropriate PPE. The COVID wards of the facility were designed for a maximum capacity of 20 beds and intended for the care of patients coming from the intensive care units of other hospitals and in the sub-acute phase. Other patients in the early stages of the disease came directly from the emergency rooms of local hospitals, which could not cope with all the demand at that time. During admission, the intention was to stabilise the clinical condition and ventilatory support consisted of a Venturi mask or nasal cannulae, not having the tools provided in intensive care, such as assisted ventilation or intubation of the patient. The hospitalisation continued until the swab was negative, although the symptoms had already receded. Few of these patients died in the facility. The research was conducted in only one of the two Covid departments (with the participation of three respondents who worked in the second department, but who had worked sporadic shifts in the Covid department under consideration).
Participants
In this study, nurses and social workers (OSS) working in the Covid ward of the San Camillo hospital in Turin agreed to participate. Participants include the researcher (MS), in the role of observer-participant.
Mode of data collection
The study was based on a collection of semi-structured interviews consisting of 11 open-ended questions (Box 1) and proposed directly to the persons involved by email[26,27]. Respondents participated on a voluntary basis. Non-probabilistic, purposive sampling continued until data saturation, collected between 15 December 2020 and 15 January 2021. The questions for the semi-structured interviews were elaborated with the narrative interview method[28] and were chosen through the "SIFA" method, in order to try to explore each sphere of interest regarding Feelings, Ideas, Functions/Activities of the client, Expectations[29].
Methods of data analysis
For data analysis, the phenomenological method according to Giorgi (2008)[30] was used (Box 2). The interviews were read over and over again, seeking personal assessments through a suspension of judgement. Subsequently, an attempt was made to find common areas of meaning describing the most important themes reported by the interviewees[31,32]. The analysis was conducted independently by researchers S.M., L.G., V.A. and V.M. They then compared their work using the triangulation method[33]. During the analysis, the researchers reflected on their own values and suspended judgements, knowledge and ideas about the phenomenon under study[34].
Ethical consideration
The persons involved voluntarily agreed to answer the interview and signed an informed consent on the use and processing of the data. The research was authorised by the Health Directorate and the General Directorate of the San Camillo Hospital.
RESULTS
Through field research, 12 interviews were collected. Table 1 shows the socio-demographic data of the participants.
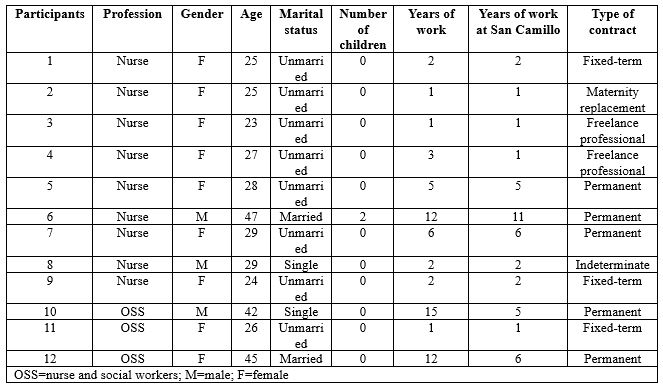
Table 1 - Social and personal data of participants
The average age of those involved is 30, with a minimum age of 23 and a maximum age of 47. All operators were professionally trained in Italy. None have postgraduate or Master's degrees. Several main and recurring themes emerged from the analysis of the interviews. These macro-categories bring us back to the experience of the participants. Terminology as presented and written by the interviewees themselves is reported, outlining the importance of the meanings expressed by them. The following themes emerged: the beginning of the Covid worker's 'journey' and the whirlwind of emotions and feelings that accompanied that (fear, feeling stuck, helpless, powerless, concerns for one's family in relation to the risk of contagion and the fear of infecting oneself and loved ones), the group as a foothold to keep going, a point of strength, union and provider of trust, the awareness of change, the cognition of time and the constructive vision of the experience (table 2).
Table 2 – Main themes emerging from the analysis
The start of the Covid worker's 'journey'
The interviews reveal the profound change that occurred in the participants' professional lives at the beginning of the pandemic. Most of them talk about the impossibility of choosing whether to work in a Covid department or not, often indicating it as a decision linked to a sense of duty fulfilment.
[...] "It wasn't really a personal choice to join the Covid team... I happened to be there, and I was probably OK with that." [...] (interview 1)
[...] "I didn't really have a choice in deciding whether I could work closely with Covid-positive patients... So compared to my start in a Covid department, I can't even explain how it came about." [...] (interview 3)
Participants underline the initial impact they had following the news, accompanied by a set of feelings that were difficult to deal with at the time and to talk about later. They describe thoughts, emotions and sensations and there are often conflicting feelings, accompanied by fear, anxiety and stress.
[...] "Literally thrown into the deep end... My thoughts were questions. Why? Why? Why? So many questions that had no answers." [...] (interview 8)
[...] "I'm still trying to figure it out... on the front line in a Covid ward... I wasn't chosen, I found myself there almost by accident." [...] (interview 7)
In the interviews, the theme of travel emerges significantly, as a symbol of uncertainty and restlessness in trying to know and explore unknown places; as well as the theme of battle, almost as if they had to fulfil a destiny already written in their professional profile.
[...] "I didn't feel chosen, I felt enlisted in an impromptu army for an impromptu battle... I was there, so I had to fight... I had the fear and adrenaline of those who leave without knowing the destination and the consequences of their journey." [...] (interview 4)
A whirlwind of emotions and feelings: fear, feeling stuck, helpless, powerless
Concerning the emotions felt during this long experience by the health workers, many of them found themselves facing different difficulties, multiple fears and feelings, one of the main ones being isolation, not only physical but also psychological.
[...] "I avoided even the contact allowed by the Decrees, I isolated myself completely, more than was necessary... All you can do is wake up in the morning and wonder when it will end... I would have liked to live fully, not at the mercy of anxiety and worry. [...] (interview 1)
[...] "I would arrive home drained, feeling nothing but tiredness that muffled all the outside world." [...] (interview 2)
[...] "I see myself as someone who put aside feelings and sensations to face a big battle, so today I don't even remember what I was feeling... We have lost all consciousness, we no longer saw well, we no longer heard well, we no longer spoke much..." [...] (interview 3)
Respondents write that they feel alone in this battle, misunderstood, stuck and aimless, depersonalised, helpless due to the suits and masks, powerless before an invisible enemy so difficult to defeat.
[...] "When I finish a shift, I feel like I have finished a test under stress... as though I had passed a test... many times I felt like I hadn't made it, as though the ground was sinking from under my feet, other times I felt empty, as though under that suit there was almost nothing left... as if I had failed, as if I hadn't done enough." [...] (interview 4)
[...] "I remember the fear... and the tiredness because I had been alone in facing that new beginning so physically and psychologically intense... The whole condition of isolation puts a lot of pressure on you psychologically... I felt powerless, a nobody before something so big... I felt like a wrapper, a container whose contents had been disposed of along with the protective suit." [...] (interview 5)
The family and the risk of contagion: the fear of infecting oneself and one's loved ones
A topic that is repeated in almost every narrative is the importance of family affection. This theme is often addressed in the interviews, emphasising the importance that health workers attached to the support given by their loved ones, but at the same time linked to the constant fear of infecting themselves and consequently their families.
[...] "If I get infected will I be sick? And at home? If mum and dad get ill? Who will take care of Granny if we are sick? What if Granny gets sick?" [...] (interview 1)
[...] "I was afraid though, afraid of not being up to it and afraid of infecting myself and my loved ones." [...] (interview 2)
[...] "The biggest fear I had was that I would get worse and that I could infect my partner... that last idea drove me mad." [...] (interview 5)
There was a high level of stress among the interviewees, which, despite everything, also contributed to an increase in attention and precautions regarding safety regulations, the correct use of personal protective equipment and the correct way of disposing of it.
[...] "At the onset, I didn't have tumultuous emotions, it was the people next to me who were really very worried and I honestly experienced their emotion... The first thing I think about when I start my shift is that I must not get sick, so I must do everything I can to avoid infection." [...] (interview 3)
[...] "I try to be focused because you can let your guard down due to tiredness and then risk getting infected." [...] (interview 12)
Conflict with PPE: distancing, anonymity and protection
The interviews reveal the perceptions of nurses and social workers obliged to wear "all those layers of latex", exploring their experiences in relation to the care provided to their patients on the Covid ward. Nurses and social workers talk of overalls, double gloves, double masks, footwear, goggles and face shields which, while vital for working on Covid wards, have raised barriers between staff and patients.
[...] "A person covered from head to toe without knowing what he looks like or not remembering his name, as if he wasn't human... and all I know of this person are his brown eyes surrounded by a mask and a big suit." [...] (interview 1)
[...]“"Halfway between astronauts and aliens!" [...] (interview 2)
[...]“I never imagined that I would keep my physical and moral distance from a patient in such a way that I could become one of the many operators, just any operator, someone easily replaceable... I didn't use to feel naked unless wearing a gown, visor and mask, whereas now I do." [...] (interview 3)
[...]“"So many little white men, completely covered by overalls, gowns, masks, gloves and visor, almost clumsy in their movements and practically indistinguishable from each other... What I miss most is being able to show my smile to the patients, free from masks, and to shake their hands, free from those multiple layers of gloves." [...] (interview 5)
[...]“Living diving suits... it's as though there were a thousand barriers, a thousand layers separating us...a gentle caress with double latex gloves is not the same..."[...] (interview 6)
The group as a foothold for not giving up: strength, unity and trust
From the interviews, it emerges that the group has been a strong point, an important support for the health workers to go on and not give up.
[...] "I have never believed in the motto 'unity is strength' as I do now... in April there were so many brave little soldiers, in November we were one giant soldier...I don't feel alone, never; I feel escorted, I feel that someone is looking out for me as I am looking out for someone else... the working group has become a family... I would get through this as long as I had this team to rely on." [...] (interview 4)
[...] "I am grateful to her for that moment, for understanding me and giving me strength when she was probably also on her last legs. We hugged each other when we left the hospital, amidst tears. I don't think I could have done it without her that day." (Interview 6)
[...] "We have been able to overcome some difficult moments only thanks to our unity. (Interview 7)
According to the interviewees, coping with such a complex period with one's team helped to increase cohesion, strengthen group dynamics and was often the driving force needed to cope with stressful situations.
[...] "The wonderful team I have the honour of sharing this experience with has become very cohesive. We all worked together for the same goal on the same road, holding hands, hugging ideally, supporting each other, experiencing the same feelings, falling down and helping each other up." [...] (interview 3)
[...]“"I believe that the greatest strength came from the working group, which I have never before felt close to me, or rather part of me... in the group set up for the Covid emergency, I really found a rock to rely on. We work with common principles, side by side to achieve the same goals. What I perceive between us is harmony, respect and sharing"[...] (interview 5)
Awareness of change: time, self-work, constructive view of the experience
What emerges from the interviews is the strength and the desire to take charge of one's own life again, the desire to make it through this pandemic, trying to find a positive side, not to throw everything away, to seize what good can come from this experience. From the words of those interviewed, one can see a devastating past and present, which has affected people greatly, but also a future full of hope.
[...] "I hope to be myself with some more awareness, especially about what was taken for granted before Covid... I'm happy to still feel like myself, to not want to give in to the suffering that Covid forced us to face every day." [...] (interview 2)
[...]“"I worked on myself like we all did...The nurse I loved to be is here somewhere, she is not gone... My job will go back to that wonderful normality I loved, with some more experience, some scars that won't go away, some indelible memories..."[...] (interview 4)
[...]“"I hope to still be the same, with more experience on my shoulders. Of course, the pandemic has changed everything and everyone, but life goes on and you have to think about facing the next enemy."[...] (interview 8)
[...]“"I hope to see myself proud of what I have done, I hope to have left a good memory in the people I have met and I will be able to say this one is gone too." [...] (interview 12)
DISCUSSION
The aim of this study was to describe the experience of healthcare workers in a Covid ward, exploring their emotional experiences and attempting to capture the meanings that the individual creates and gives to that experience, understanding the structure, nature and form, as perceived by the individual. This survey collected the experiences of nurses and social and health workers who worked in a ward for the treatment of patients affected by Covid-19, in order to know how they responded to an emergency situation that not only involved the work aspect but also invaded the personal sphere. From the data collected, it emerges that the pandemic is immediately experienced by health workers as insidious, bringing uncertainties and anxiety, emotions and feelings that can be traced back to a scenario reminiscent of a battle. You feel overwhelmed by a storm, you prepare for the arrival of a real 'enemy' [19], you find yourself united by the same feelings, but at the same time alone and ill-prepared, forced to take the to the field with the few weapons available. This describes the whirlwind of emotions, fears, worries, feelings of helplessness, a mixture of negative feelings in which there is rarely any slight hope for the future. In the interviews, all subjects tell of their fears: of becoming sick and infected, of being isolated, of not being ready to face the big changes in the work structure. This issue is dealt with extensively by Catania et al.[18] and by De Vito et al.[19], highlighting how the narratives of the nurses, also working in different wards, underline the common theme of the physical and psychological impact that the change in work organisation had on the same individual workers and on team work. In the study by Arasli et al[16], 'fear' and 'risk' were two of the most frequently used words by nurses in social media during the pandemic. Among the feelings experienced there is certainly no lack of anxiety, which is expressed several times in the narratives considered in this study and is also widely described in the article by Labrague et al.[17]. From the data collected it emerges how the entire pandemic situation forces nurses and social and health workers to create a different way of being workers, a situation that almost imposes a different way of directing the therapeutic relationship no longer mediated by touch, words, reciprocal dialogue and the security of familiar clothing, but hindered by the trappings of a distancing "dress" and by the impossibility of speech that bring out a problematic core of objectification of care. This aspect emphasises how to deal with health emergencies, without at the same time renouncing the humanity of the therapeutic relationship that characterises this profession. All the images described in the interviews are of 'detachment' from one's own body which, within the innumerable protective layers within which it is forced, finds itself taking on a form unknown to the eyes of the subjects themselves. These people are the same as those who performed acts of care, but in doing so they all felt equal and experienced a human closeness made up only of glances. From the narratives of this research, a strong spirit of adaptation and resilience emerges in nurses, aspects also described by Catania et al.[18] and Labrague et al.[17]. This theme was widely taken up in the interviews, allowing us to outline through these nurses "made of suits and personal protective equipment", an image in which latex and nitrile are transformed into a material capable of absorbing a shock without breaking, to face and overcome a traumatic and extreme event, to give hope in the future. Wu Y. et al. [35] show that doctors and nurses working in Covid wards experienced lower levels of anxiety, depression and burnout than those working in their usual wards, with a response to the pandemic characterised by a high level of adaptation and resilience. The participants of our study emphasised that the team proved to be the most important strength in overcoming daily difficulties within the Covid department. The objectives for which the group meets and works together and the dynamics of consolidation of the process that forms the working group, from interaction to integration[35], are essentially described in both processes and activities: the group intervenes whenever someone is in difficulty; a hand is always extended towards the other when one finds oneself lost in what should be a known world but has become an unexplored labyrinth. The feeling of belonging to the group is found to be a decisive positive factor also among the students of the article by Garrino et al.[20], which underlines how the comparison between peers and the support provided by peers are a decisive element to deal positively with the practical traineeship experience.
Another important theme that emerged from the interviews was time. A time that sometimes expands, sometimes shrinks, but which must be lived anyway[19]. In fact, the impact of the pandemic marked a deep rift between what was before and what would be after. This perception had different effects. On the one hand, it made them feel stuck and unable to imagine the future from such an uncertain present; on the other hand, it allowed them to discover new physical spaces and adopt new or renewed daily habits which helped them to imagine a possible future. The perspectives described are linked to fear, but also to the hope that normality will be re-established, both on the horizon of care and in daily life. These reflections represent an added value that contributes to a greater understanding of oneself and the role that one's experiences played during the emergency. Narratives have been a useful tool for making sense and meaning of the experiences associated with the pandemic experience[19].
CONCLUSIONS
The research explored the lived experiences of a small group of health workers working in a Covid ward during the pandemic in November 2020. Telling stories was a chance to give shape to the situations experienced, continuing to plan oneself, giving new meaning and significance to one's existence. Narrative and mutual listening practices were recognised as very useful and effective in capturing and understanding meanings, emotions and representations about one's professional role and wider existential issues. This research provides evidence to improve the strategies to deal with a health emergency by listening to personal experiences and thoughts, by accepting the emotions and feelings felt by the care professionals, experiences and representations that, many times, in these situations the caregiver may struggle to express or, even, prefers to keep hidden under his uniform. It can be concluded that narrative medicine used in care environments, in situations where there is no space and time for the individual, offers the possibility to improve and increase the communication and cooperation skills of all; to develop new knowledge of each operator to improve the relationship with others; to give meaning and value to the experience of care of health workers and help them to process and alleviate, as far as possible, the emotional stress that accompanies them in the difficult path of care.
LIMITATIONS
Data were collected by sending an interview outline via email. This method was chosen due to the lack of opportunities to conduct the interview due to the national lock-down and to allow the interviewees to express themselves freely and openly without time constraints. this deprived the research of elements concerning the conducting and interaction aspects that usually characterise face-to-face interviews.
CONFLICTS OF INTEREST AND FUNDING SOURCES
No funding sources were used to support the project. There is no conflict of interest.
DECLARATIONS
No formal approval by the Local Ethics Committee was required for this study.
REFERENCES
- Tutto sulla pandemia di SARS-CoV-2; 16 gennaio 2020. Disponibile a:https://www.epicentro.iss.it/coronavirus/sars-cov-2. Ultimo accesso 28 febbraio 2022.
- Coronavirus disease (COVID-19) pandemic. Disponibilea: https://www.who.int/emergencies/diseases/novel-coronavirus-2019. Ultimo accesso 7 marzo 2022.
- Tufekci Z. Pandemic mistakes we keep repeating. The Atlantic. 26 febbraio, 2021. Disponibile a: https://www.theatlantic.com/ideas/archive/2021/02/how-public-health-messaging-backfired/618147/. Ultimo accesso 20 febbraio 2022.
- WHO Director-General’s opening remarksat the media briefing on COVID19; 23 ottobre 2020. Disponibile a:https://www.who.int/director-general/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19---23-october-2020. Ultimo accesso 20 gennaio 2022. Ultimo accesso 10 febbraio 2022.
- Contini C., Di Nuzzo M., Barp N., Bonazza A., De Giorgio R., Tognon M., et al.The novel zoonotic COVID-19 pandemic: An expected global health concern. J. Infect. Dev. Ctries. 2020, 14, 254–264.
- Covid-19: mortalità in terapia intensiva; 2 ottobre 2020. Disponibile a: https://www.med4.care/covid-19-mortalita-in-terapia-intensiva/. Ultimo accesso 7 marzo 2022.
- Porcheddu R., Serra C., Kelvin D., Kelvin N., Rubino S. Similarity in Case Fatality Rates (CFR) of COVID-19/SARS-CoV-2 in Italy and China. J. Infect. Dev. Ctries. 2020, 14, 125–128.
- Galimberti F., Boseggia S.B., Tragni E. Consequences of COVID-19 pandemic on healthcare services. SEFAP Università degli Studi di Milano 2021; 13 (1): 5-16. Disponibile a: http://www.sefap.it/web/upload/GIFF2021_1_5_16.pdf. Ultimo accesso 10 febbraio 2022.
- Impatto dell’epidemia COVID-19 sulla mortalità totale della popolazione residente periodo gennaio-novembre 2020; 30 dicembre 2020. Disponibile a: https://www.epicentro.iss.it/coronavirus/pdf/Rapp_Istat_Iss_gennaio-novembre-2020.pdf- Ultimo accesso 20 gennaio 2022.
- La mortalità totale in Italia nell’anno della pandemia; 16 febbraio 2021. Disponibile a: https://www.unive.it/pag/fileadmin/user_upload/dipartimenti/economia/doc/eventi/EconomicsTuesdayTalks/ett_20210216_corsetti.pdf. Ultimo accesso 4 marzo 2022.
- Sun P., Lu X., Xu C., Sun W., Pan B. Understanding of COVID-19 based on current evidence. J. Med. Virol. 2020, 92, 548–551.
- Epidemia COVID-19; 30 aprile 2020. Disponibile a: https://www.epicentro.iss.it/coronavirus/bollettino/Bollettino-sorveglianza-integrata-COVID-19_28-aprile-2020.pdf. Ultimo accesso 20 gennaio 2022.
- COVID-19, l’impatto della pandemia: analisi degli infermieri deceduti; 15 luglio 2020. Disponibile a: https://www.fnopi.it/2020/07/15/covid19-analisi-deceduti-infermieri. Ultimo accesso 20 gennaio 2022.
- Rizzo C., Campagna I., Pandolfi E., Croci I., Russo L., Ciampini S., et al. Knowledge and Perception of COVID-19 Pandemic during the FirstWave (Feb–May 2020): A Cross-Sectional Study among Italian HealthcareWorkers. International Journal of Environmental Research and Public Health. 2021; 18, 3767.
- Monitoraggio sugli operatori sanitari risultati positivi a COVID-19 dall’inizio dell’epidemia fino al 30 aprile 2020: studio retrospettivo in sette regioni italiane; marzo 2021. Disponibile a https://www.inail.it/cs/internet/docs/alg-pubbl-monitoraggio-operatori-sanitari-studio.pdf. Ultimo accesso 7 marzo 2020.
- Arasli H., Furunes T., Jafari K., Saydam M.B., Degirmencioglu Z. Hearing the Voices of Wingless Angels: A Critical Content Analysis of Nurses' COVID-19 Experiences. International Journal of Environmental Research and Public Health. 2020; 16;17(22):8484. doi: 10.3390/ijerph17228484.
- Labrague L.J., De Los Santos J.A.A. COVID-19 anxiety among front-line nurses: Predictive role of organisational support, personal resilience and social support. Journal of Nursing Management. 2020 Oct; 28(7):1653-1661. doi: 10.1111/jonm.13121.
- Catania G., Zanini M., Hayter M., Timmins F., Dasso N., Ottonello G., et al. Lessons from Italian front-line nurses' experiences during the COVID-19 pandemic: A qualitative descriptive study. Journal of Nursing Management. 2021;29(3):404-411. doi: 10.1111/jonm.13194.
- De Vito B., Castagno E., Garrone E., Tardivo I., Conti A., Luciani M., et al. Narrating care during the COVID-19 pandemic in a paediatric emergency department. Reflective Practice. 2021: 1-12 doi: 10.1080/14623943.2021.2013190.
- Garrino L., Ruffinengo C., Mussa V., Nicotera R., Cominetti L., Lucenti G., et al. Diari di bordo: l’esperienza di tirocinio pre-triage COVID 19 degli studenti in infermieristica. Journal of Health Care Education in Practice. 2021; 3, 67-79.
- Charon R. Narrative medicine - Honoring the Stories of Illness. New York: Oxford University Press. it. Medicina narrativa. Onorare le storie dei pazienti. Milano, Raffello Cortina Editore 2019.
- Mortari L. Ricercare e riflettere. Roma: Carocci Editore. 2009.
- Sodano L. Emozioni Virali. Roma: Il Pensiero Scientifico Editore.
- Bosco F., Chiarlo M., Tizzani D., Cavicchi Z.F. Abbracciare con lo sguardo. Roma: Il Pensiero Scientifico Editore. 2020.
- Polit D.F., Beck C.T. Fondamenti di ricerca infermieristica. Seconda edizione Milano: McGraw-Hill Education. 2018; 3.
- Liehr P., Takahashi R., Liu H., Nishimuna C., Summers L.C. Bridging distance and culture with a cyberspace method of qualitative analysis. AdvNurs Sci. 2004; 27(3):176-186.
- Hamilton R.J., Bowers B.J. Internet recruitment and e-mail interviews in qualitative studies. Qual Health Res. 2006; 16:821- 835.
- Atkinson R. L’intervista narrativa. Milano: Raffaello Cortina Editore.
- Hogan-Quigley B., Palm M.L., Bickley L.B. Valutazione per l'assistenza infermieristica. Rozzano: Casa Editrice Ambrosiana. 2017.
- Giorgi A.P., Giorgi B. Phenomenological psychology: The Sage handbook of qualitative research in psychology. 2016. doi: 3402/qhw.v11.30682
- Garrino L. La Medicina narrativa nei percorsi di ricerca e di cura in Finiguerra I., Garrino L., Picco E., Simone P. Narrare la malattia rara. Esperienze e vissuti delle persone assistite e degli operatori. Torino: Edizioni Medico-Scientifiche.
- Mortari L., Zannini L. La ricerca qualitativa in ambito sanitario. Roma: Carocci Editore. 2017.
- Streuber Speziale H.J., Carpenter D.R. La ricerca qualitativa: un imperativo umanistico. Napoli: Idelson-Gnocchi. 2005.
- Mortari L., Ghirotto L. I metodi dalla ricerca qualitativa. Roma: Carocci Editore. 2019.
- Wu Y., Wang J., Luo C., Hu S., Lin X., Anderson A.E., et al. A Comparison of Burnout Frequency Among Oncology Physicians and Nurses Working on the Frontline and Usual Wards During the COVID-19 Epidemic in Wuhan, China. Journal of Pain and Symptom Management.2020;60.
- Quaglino G.P., Casagrande S., Castellano A.M. Gruppo di lavoro, lavoro di gruppo. Milano: Raffaello Cortina Editore. 1992.
Box 1 – Interview outline
1. Could you tell me how your adventure in the Covid ward started?
2. What was the first thought that came into your mind when you were chosen as Covid-19 worker?
3. How do you think your way of working has changed compared to before?
4. If you saw yourself through the eyes of a patient, how would you describe yourself?
5. How do you feel and what do you think when you finish your shift and leave the hospital?
6. And what do you think and feel when you have to start a shift?
7. has anything changed in the working group compared to previous months? If so, what?
8. Can you tell me an episode that made you think you could deal with all this with your team?
Box 2 – Giorgi's method (2008)
A. Read the whole description of the experience with the aim of making sense of it all
B. Rereading the descriptions to discover the essences of the experience. Observe every time a transaction takes place in meaning. Make these meaning units or themes abstract
C. Examine units of meaning for redundancy, clarification or elaboration. Relate units of meaning to each other and to the meaning of the whole
D. Reflect on the units of meaning and extrapolating the essence of the experience for each participant. Transform each unit of meaning into scientific language
![]() This work is licensed under a Creative Commons
This work is licensed under a Creative Commons
Attribution-NonCommercial-NoDerivatives 4.0 International License.
How to Trust your Intuition when You're Making a Decision
Once I gave the headphones a thorough once-over exam, I tried them on. As I mentioned, they have a classic over-the-ear style and just looking at them, the padding on the ear pieces seem adequate and the peak of the headband seemed to be a bit lacking, but you don’t really know comfort unless you try on the product. So, I slipped the headphones on and found them to be exquisitely comfortable. Once I gave the headphones a thorough once-over exam, I tried them on. As I mentioned, they have a classic over-the-ear style and just looking at them, the padding on the ear pieces seem adequate and the peak of the headband seemed to be a bit lacking, but you don’t really know comfort unless you try on the product. So, I slipped the headphones on and found them to be exquisitely comfortable.
If no one hates you, no one is paying attention. If attention is what you want for vanity, confidence, or, hell — to make a decent living — then know that it’s not instantaneous. Every single person that you’re currently paying attention to, at some point in their lives.
You need to be true to yourself
Just like every other human on the planet, I have epically awesome days and days when life just turne against me. And while I can’t stand most self-help (see: tired quotes over stock photography on Instagram), sometimes I need a little pick-me-up. And most of the time, in order to get out of a slump (because my brain leans more into math/science than anything else), I need to drop a logic bomb on my ass.
Yes, this is a long article. But here’s the thing — if you’re reading this in your inbox and are already like, “fuck this!” delete it. No hard feelings. If you’re reading this in a browser on a website, and you see how tiny the scroll-bar is because of how far you still have to scroll to get to the bottom, close this tab and go back to 140-character tidbits of advice. Still with me? Phew. Just had to weed out all the folks from points: #1, #4 and #8. Welcome friends, onward we go.
Never give up and stay strong
If no one hates you, no one is paying attention. If attention is what you want for vanity, confidence, or, hell — to make a decent living — then know that it’s not instantaneous. Every single person that you’re currently paying attention to, at some point in their lives, was in your exact position. They kept at it and worked enough so that others started listening. Also know that if no one is watching, you can experience true freedom. Dance in your underwear. Write entirely for yourself. Like there’s a going-out-of-business sale. Find yourself — not in some coming-of-age hippie way involving pasta and ashrams— but in a way that helps you draw your own line in the sand for what matters and what doesn’t. Do what you want to do, just because you want to do that thing. This will build confidence that will come in handy later.


Once I gave the headphones a thorough once-over exam, I tried them on. As I mentioned, they have a classic over-the-ear style and just looking at them, the padding on the ear pieces seem adequate and the peak of the headband seemed to be a bit lacking, but you don’t really know comfort unless you try on the product. So, I slipped the headphones on and found them to be exquisitely comfortable. Once I gave the headphones a thorough once-over exam, I tried them on. As I mentioned, they have a classic over-the-ear style and just looking at them, the padding on the ear pieces seem adequate and the peak of the headband seemed to be a bit lacking, but you don’t really know comfort unless you try on the product. So, I slipped the headphones on and found them to be exquisitely comfortable.
If no one hates you, no one is paying attention. If attention is what you want for vanity, confidence, or, hell — to make a decent living — then know that it’s not instantaneous. Every single person that you’re currently paying attention to, at some point in their lives, was in your exact position. They kept at it and worked enough so that others started listening. Also know that if no one is watching, you can experience true freedom. Dance in your underwear. Write entirely for yourself. Like there’s a going-out-of-business sale. Find yourself — not in some coming-of-age hippie way involving pasta and ashrams— but in a way that helps you draw your own line in the sand for what matters and what doesn’t. Do what you want to do, just because you want to do that thing. This will build confidence that will come in handy later.
Everyday inspired by the Beauty of the Mountains
Take your time.
I’ve got a Fujifilm X100s. It runs about $1300. It’s easily the best camera I’ve ever owned. I take care of it as best as I can, but I don’t let taking care of it impact the photography. Let me elaborate on that a bit better. You’ll get better at each section of what we talked about slowly. And while you do, you’ll be amazed at how much easier it all is and how the habit forms. The best way to get better at photography is start by taking your camera everywhere. If you leave your house, your camera leaves with you. The only exception is if you’re planning for a weekend bender — then probably leave it at home. Other than that, always have it slung over your shoulder. It would probably help to get an extra battery to carry in your pocket. I’ve got three batteries. One in my camera, one in my pocket, one in the charger.
When it dies, swap them all.
For me, the most important part of improving at photography has been sharing it. Sign up for an Exposure account, or post regularly to Tumblr, or both. Tell people you’re trying to get better at photography. Talk about it. When you talk about it, other people get excited about it. They’ll come on photo walks with you. They’ll pose for portraits. They’ll buy your prints, zines, whatever.
Clouds come floating into my life, no longer to carry rain or usher storm, my sunset sky.
— Rabindranath Tagore
Breathe the world.
I’ve got a Fujifilm X100s. It’s easily the best camera I’ve ever owned. I take care of it as best as I can, but I don’t let taking care of it impact the photography. Let me elaborate on that a bit better. You’ll get better at each section of what we talked about slowly. And while you do, you’ll be amazed at how much easier it all is and how the habit forms. The best way to get better at photography is start by taking your camera everywhere. If you leave your house, your camera leaves with you. The only exception is if you’re planning for a weekend bender — then probably leave it at home. Other than that, always have it slung over your shoulder. It would probably help to get an extra battery to carry in your pocket. I’ve got three batteries. One in my camera, one in my pocket, one in the charger. When it dies, swap them all.
For me, the most important part of improving at photography has been sharing it. Sign up for an Exposure account, or post regularly to Tumblr, or both. Tell people you’re trying to get better at photography. Talk about it. When you talk about it, other people get excited about it. They’ll come on photo walks with you. They’ll pose for portraits. They’ll buy your prints, zines, whatever.
Heavy hearts, like heavy clouds in the sky, are best relieved by the letting of a little water.
— Christopher Morley
Enjoy the morning.
The best way to get better at photography is start by taking your camera everywhere. If you leave your house, your camera leaves with you. The only exception is if you’re planning for a weekend bender — then probably leave it at home. Other than that, always have it slung over your shoulder. It would probably help to get an extra battery to carry in your pocket. I’ve got three batteries. One in my camera, one in my pocket, one in the charger. When it dies, swap them all.
For me, the most important part of improving at photography has been sharing it. Sign up for an Exposure account, or post regularly to Tumblr, or both. Tell people you’re trying to get better at photography. Talk about it. When you talk about it, other people get excited about it. They’ll come on photo walks with you. They’ll pose for portraits. They’ll buy your prints, zines, whatever.
It’s easily the best camera I’ve ever owned. I take care of it as best as I can, but I don’t let taking care of it impact the photography. You’ll get better at each section of what we talked about slowly. And while you do, you’ll be amazed at how much easier it all is and how the habit forms.
There are absolutely no rules of architecture for a castle in the clouds and this is real.
— Gilbert K. Chesterton
Free your mind.
The best way to get better at photography is start by taking your camera everywhere. If you leave your house, your camera leaves with you. The only exception is if you’re planning for a weekend bender — then probably leave it at home. Other than that, always have it slung over your shoulder. It would probably help to get an extra battery to carry in your pocket. I’ve got three batteries. One in my camera, one in my pocket, one in the charger. When it dies, swap them all.
I’ve got a Fujifilm X100s. It’s easily the best camera I’ve ever owned. I take care of it as best as I can, but I don’t let taking care of it impact the photography. Let me elaborate on that a bit better. You’ll get better at each section of what we talked about slowly. And while you do, you’ll be amazed at how much easier it all is and how the habit forms.
For me, the most important part of improving at photography has been sharing it. Sign up for an Exposure account, or post regularly to Tumblr, or both. Tell people you’re trying to get better at photography. Talk about it. When you talk about it, other people get excited about it. They’ll come on photo walks with you. They’ll pose for portraits. They’ll buy your prints, zines, whatever.
How to Appreciate the Little Things in Life and be Happy
Just the other day I happened to wake up early. That is unusual for an engineering student. After a long time I could witness the sunrise. I could feel the sun rays falling on my body. Usual morning is followed by hustle to make it to college on time. This morning was just another morning yet seemed different.
Witnessing calm and quiet atmosphere, clear and fresh air seemed like a miracle to me. I wanted this time to last longer since I was not sure if I would be able to witness it again, knowing my habit of succumbing to schedule. There was this unusual serenity that comforted my mind. It dawned on me, how distant I had been from nature. Standing near the compound’s gate, feeling the moistness that the air carried, I thought about my life so far.
Your time is limited, so don't waste it living someone else's life. Don't be trapped by dogma – which is living with the results of other people's thinking.
Steve Jobs
I was good at academics, so decisions of my life had been pretty simple and straight. Being pretty confident I would make it to the best junior college of my town in the first round itself, never made me consider any other option. I loved psychology since childhood, but engineering was the safest option. Being born in a middle class family, thinking of risking your career to make it to medical field was not sane. I grew up hearing ‘Only doctor’s children can afford that field’ and finally ended up believing it. No one around me believed in taking risks. Everyone worshiped security. I grew up doing the same.
‘Being in the top will only grant you a good life’ has been the mantra of my life. But at times, I wish I was an average student. I wish decisions would have not been so straightforward. Maybe I would have played cricket- the only thing I feel passionate about. Or maybe I would have studied literature (literature drives me crazy). Isn’t that disappointing- me wishing to be bad at academics. It’s like at times I hate myself for the stuff I am good at.
When you step out of these four walls on a peaceful morning, you realize how much nature has to offer to you. Its boundless. Your thoughts, worries, deadlines won’t resonate here. Everything will flow away along with the wind. And you will realize every answer you had been looking for, was always known to you. It would mean a lot to me if you recommend this article and help me improve.
Assessing the outcome of admissions: Pilot study in a High Intensity Psychiatric Residential Facility
Pierluigi Ricchiuto1, Stefania Impicci2, Martina Schiano3
1.Nurse at the Department of Emergency and Acceptance, Emergency Department - OBI, Asl Napoli 2 Nord, Santa Maria delle Grazie Hospital, Pozzuoli.
2.Nurse at "Casa Rossa" Residential Rehabilitation Centre. Area Vasta 2 - Ancona.
3.Nurse at UOS Clinical Risk, AORN - Ospedale dei Colli, Monaldi Hospital, Naples.
*Corresponding Author: Pierluigi Ricchiuto, Department of Emergency and Acceptance, Emergency Department - OBI, Asl Napoli 2 Nord, Santa Maria delle Grazie Hospital, Pozzuoli.
Email: pierluigi.ricchiuto@aslnapoli2nord.it
Cita questo articolo
ABSTRACT
Background: The Italian health system related to mental disorders is currently experiencing a period of radical reforms. This process began in 1978 with the adoption of the law 180 which produced a radical reform in mental health care. The problems of the continuous confrontation with increasing levels of expenditure are reflected in the search for models to improve both the efficiency and effectiveness of the health care system. Among these, the value creation model proposes to optimize the relationship between effectiveness, quality, and appropriateness of care on the one hand, and efficiency, cost and how resources are used on the other. The intervention involves redesigning services on the principles of recovery; implementing treatments supported by scientific evidence; encouraging processes of social inclusion. The proposed rehabilitation interventions are recovery oriented that place the person at the center of his rehabilitation path, motivating him in assuming responsibility for the treatment proposed during hospitalization.
Objective: Evaluate the impact of the organisational reorganisation of the DSM S.R.R Regional Health Service of Ancona Area Vasta 2 by introducing evidence-based and recovery-oriented practices through the evaluation of clinical outcomes and psychosocial functioning.
Methods: Longitudinal descriptive observational study with evaluation of a cohort of 13 patients, hospitalized in residential and semi-residential care at SRP1 “Casa Rossa” Area Vasta 2 of Ancona, by administration of a questionnaire (HoNOS) at the time of recruitment (February 2019), at 6 months (August 2019) and at 12 months (February 2020). The 12 items of the questionnaire were grouped into four subsets: behavioural problems (items 1-3), deficits and disabilities (items 4-5), psychopathological symptoms (items 6-8) and relational/environmental problems (items 9-12).
Results: Survey results show a reduction in mean scores at 6 and 12 months compared to baseline in all subscales.
Conclusions: Intensive mental health residential facilities need to put more effort into evaluating effectiveness in practice, using appropriate tools for outcome assessment and analysis of results. It is possible, in daily clinical practice, to evaluate the outcome of admissions in order to satisfactorily describe the changes induced during the period of hospitalization.
Keywords: outcome of care, mental health, psychiatric facility, biopsychosocial.
INTRODUCTION
The Department of Mental Health (DSM in Italian) is the set of facilities and services whose task is to take charge of the demand for care, assistance and protection of mental health; it is the body which governs, coordinates and manages Community Psychiatry, guaranteeing the unity and integration of psychiatric services within the area of competence defined by ASUR Marche [1]. Moreover, the DSM's task is to promote mental health and quality of life in the target population; to guarantee primary and secondary prevention of mental disorders with the early detection of situations of distress and tertiary prevention with the reconstruction of the affective, relational, social and work fabric [2]. The typology of psychiatric residential facilities is distinguished both by the level of therapeutic-rehabilitative intervention, related to the level of impairment of the patient's functions and abilities (and its treatability), and by the level of care intensity offered, related to the overall degree of autonomy. Psychiatric residential facilities for intensive therapeutic rehabilitation treatment (SRP1) are facilities for patients with severely impaired personal and social functioning. These structures play a transitional role, aimed at reintegrating the patient into his/her usual living environment (generally family) [3,4]. The intervention areas of SPR1 concern the clinical psychiatric, psychological, rehabilitation, resocialisation and coordination areas. The new organisation of the Psychiatric Residential Facilities (SRP in Italian) of the Area Vasta 2 DSM is part of the new organisation suggested by the Unified Conference Agreement of 17 October 2013 [5] and subsequently accepted at regional level by D.G.R.M. 1331/14 [6], where the concept of residency is declined in a different way of managing psychological distress. The user is no longer placed in a purely medical dimension, but an individual project is built in agreement with other professionals. Therefore, the care pathway must be configured as a project characterised by: unity, continuity, multidisciplinarity, high organisational complexity, relevant professional specificity and ability to manage sociomedical integration [7]. It is based on the integration of specific activities such as: clinical and rehabilitation activities, care activities, family and social mediation, networking and coordination. The realisation of this pathway implies a strong investment in team work, understood as a multi-professional group able to develop an accurate reading of the patient's biopsychosocial dimension, to integrate the observation data and to modulate a coherently articulated therapeutic planning. Thus, the 'biopsychosocial' model systematically employs biological, psychological and social factors, including their complex interactions, in the understanding of psychophysical health and the choice of therapeutic intervention [8]. Consequently, by focusing on the unitary and global approach to the person, the biopsychosocial model is the one most conducive to an interdisciplinary approach between the various professions, such as doctors, psychologists, social workers and educators. For patients with severe mental illnesses, controlling symptoms, regaining a positive sense of self, dealing with stigma and discrimination, and trying to lead a productive and satisfying life is increasingly referred to as an ongoing process of recovery [9]. Equally important is to enhance personal attitudes and skills such as communication skills, enthusiasm and willingness to learn, cultural background and to develop the practice of outcome assessment among practitioners. Patient care in residential psychiatric facilities is therefore linked to a practice oriented towards therapeutic continuity and is implemented through individual projects [10]. In past years, at national and regional level, activity data have shown a progressive lengthening of hospital stays, with a consequent reduction in patient turnover. In this sense, psychiatric residency has often taken on the function of a 'housing solution' rather than being functional to the 'individual treatment project', generating the danger that SRPs are used for forms of new institutionalisation. All SRPs should therefore provide for light residential care with assistance, which facilitates the transition from the structure to the territory [3].
There is a need for evidence-based assessment and rehabilitation activities in order to provide residents with the possibility of being involved in social interactions outside of the facilities, and possibly with opportunities for sheltered work and social integration. Indeed, work, social relationships and independence are aspects of quality of life recognised as important by both patients and their treating physicians [11]. Well-designed rehabilitation plans, adapted to the needs of each patient, are mandatory to foster the development of independence, increase the likelihood of discharge and ultimately improve quality of life [12]. The development of the clinical pathways model requires addressing fundamental clinical and organisational aspects [13]:
- organising a reception/assessment function for demand and requests from psychiatric services;
- the centrality of the sending Mental Health Centre (CSM in Italian);
- the centrality of family;
- the involvement of the GP to be implemented from the earliest stages of the patient's contact with the structure;
- the definition and organisation of individualised therapeutic-rehabilitation paths;
- facilitating access procedures for all DSM operators;
- defining criteria for a maximum length of stay consistent with the level of rehabilitation intensity (18/24 months for rehabilitation facilities, 36 months for care facilities).
The result of the change process was to orientate the whole Structure to adopt principles, develop policies and implement actions, in order to help people with mental disabilities to remain in their life context, trying to achieve the best possible biopsychosocial functioning compatible with functional deficits, persistent psychopathology and relapses.
MATERIALS AND METHODS
Study design
Longitudinal descriptive observational study by administering the HoNOS questionnaire after the reorganisation of the psychiatric residential facilities of the Department of Mental Health of the Ancona Vasta 2 Area.
Population and settings
The pilot study was conducted at SRP1 "Casa Rossa" Area Vasta 2 of Ancona and involved 13 patients admitted to SRP1 Casa Rossa - AN ASUR Marche.
Inclusion criteria
Residential and semi-residential patients.
Ethical consideration
After explaining the purpose, the study was authorised by the Director of the DSM.
The study protocol was developed in accordance with the guidelines of the Declaration of Helsinki. Participation in the study was voluntary: patients were provided with a consent form for data processing and an information and consent form for the study. Only after obtaining consent and ensuring that the patient understood the purpose of the study was the paper-based HONOS questionnaire administered.
Data were collected after obtaining informed consent from each patient. The confidentiality of the data collected was guaranteed by ensuring the anonymity of all participants and avoiding the use of any personal identifiers.
The surveys, carried out in a homogeneous way by the Coordinator of the Operating Unit with over thirty years of working experience (twenty years of experience in the mental health area) took place in a protected environment, with a standardised method: a room specifically dedicated to surveys and data collection, no outside involvement and respect for the patient’s privacy.
Survey instrument
The validated Italian version of the Health of the Nation Outcome Scales [14] was used. The HoNOS scale is a multidimensional outcome and severity assessment tool developed specifically for routine use in mental health services, suitable for the assessment of clinical and psychosocial problems [15,16]. It consists of 12 items that the therapist assesses according to the severity of the problems. Each item represents a clinical problem area and is rated on a 5-point Likert scale. Relevant items include:
1.Hyperactive, aggressive, destructive or agitated behaviour;
2.Deliberately self-harming behaviour;
3.Problems related to drug or alcohol use;
4.Cognitive problems;
5.Problems of somatic illness or physical disability;
6.Problems of somatic illness or physical disability;
7.Problems related to depressed mood;
8.Other mental and behavioural problems;
9.Relational problems;
10.Problems in activities of daily living;
11.Problems in living conditions;
12.Problems in the availability of resources for work or leisure activities.
Each of the twelve items in the questionnaire is given a score from 0 to 4, where:
- a score of 0 indicates that no problem has been found;
- a score of 1 indicates that the problem is present, but because of its reduced severity no intervention is needed;
- a score of 2 indicates that a problem of mild severity is present, for which intervention (rehabilitation, care or therapy) is required;
- score 3 indicates the presence of a problem of moderate severity;
- a score of 4 indicates that a serious or very serious problem is present.
Unknown information was given a score of 9. The twelve scores can be added together to obtain an estimate of total severity or evaluated individually.
Study procedures and data collection
The reconversion project of SRP1 "Casa Rossa" took place in accordance with the principle of gradualness and with the participation of all operators through weekly meetings specifically planned by the nursing coordinator. Subsequently, patients were assessed three times over a one-year period by administration of the HoNOS questionnaire, at recruitment (February 2019), at 6 months (August 2019) and at 12 months (February 2020). Patients excluded from care were not included in the study. After data collection, the 12 items of the HoNOS scale were grouped into four subscales:
1.behavioural problems (items 1-3),
2.deficits and disabilities (items 4-5),
3.psychopathological symptoms (items 6-8)
4.relational/environmental problems (items 9-12).
Statistical analyses
Data was expressed as mean and standard deviation (SD) or median and interquartile range (IQR) in the case of numerical variables, while in the case of qualitative variables, it was expressed as absolute numbers or percentages.
The normality of the data was checked with the Shapiro-Wilk test, where with a p-value > 0.05 there is evidence of normally distributed data.
The difference between the averages of the total score and the scores of the four subscales, at the three follow-up points, was statistically evaluated with an analysis of variance model for repeated measures, in the case of normally distributed residuals; in the case of non-normally distributed data, the non-parametric Friedman test was applied.
For the scales with statistically significant differences in scores, multiple comparisons were made retrospectively between the groups (baseline, 6 months, 12 months) maintaining the 5% significance level with Bonferroni correction. Statistical analyses were carried out using the software R-CRAN v.3.6.2 for Windows.
RESULTS
Table 1 shows the demographic and clinical characteristics of the cohort of patients examined in the study.

Table 1. Descriptive statistics for demographic and clinical variables.
The mean with the standard deviation and the median with the interquartile range of the total score and the scores of the items of the 4 sub-scales, at baseline and in the two surveys at follow-up, are shown in table 2 and figure 1.
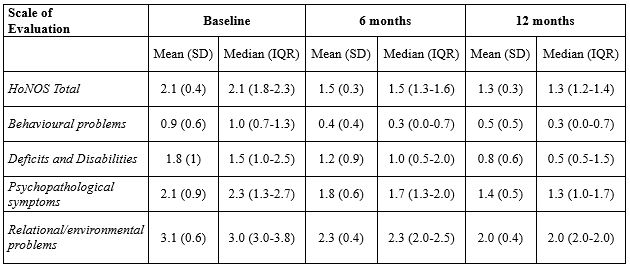
Table 2. Mean, standard deviation, median and interquartile range of Total Scale and 4 Subscales scores at baseline, 6 months and 12 months.
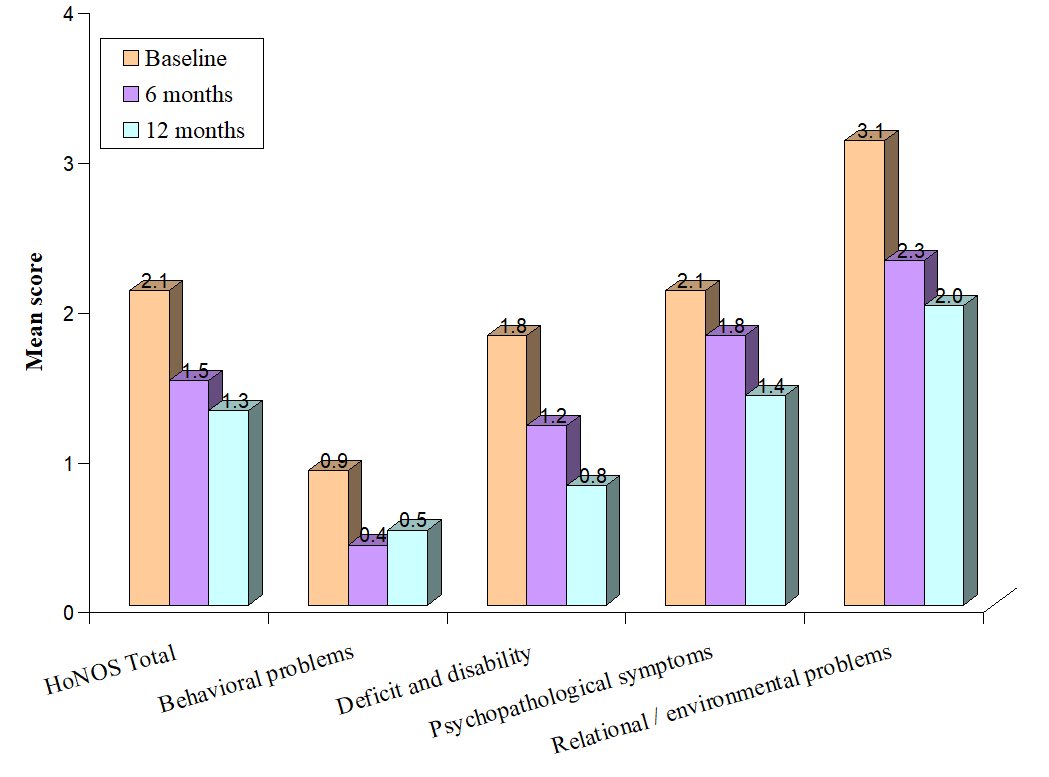
Figure 1. Average total score and average score of the 4 sub-scales.
The residuals of the analysis of variance model are distributed in accordance with the Normal random variable for the subscales of "deficit and disability" and "psychopathological symptoms" (p-value>0.05); the scale HoNOS Total, that of behavioural problems and of relational/environmental problems do not present normally distributed residuals (table 3).
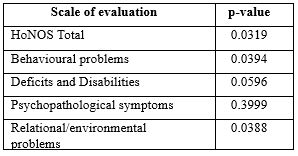
Table 3. P-value Shapiro-Wilk normality test
The statistical significance (p-value) of the differences between the averages of the total score and the scores of the four subscales at the three follow-up points are given in Table 4; the results show a statistically significant difference between the averages at the 95% confidence level.
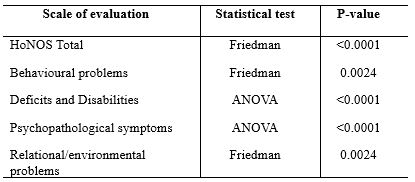
Table 4. Statistical significance of ANOVA and Friedman's Test.
Table 5 shows the p-values of multiple retrospective comparisons between the groups (baseline, 6 months, 12 months) while maintaining the 5% significance level with the Bonferroni correction.

*P-value <0.05 Statistically significant difference
Table 5. P-value of pairwise retrospective comparisons of scores on the HoNOS Total scale and the 4 subscales at baseline, 6 months and 12 months.
DISCUSSION
The study performed predates the SARS-CoV2 pandemic and involved a cohort of 13 patients admitted to SRP1 Casa Rossa in Ancona. The mean age at recruitment and at disease onset was 46 and 19 years respectively, 69% of patients were male, 46% had a caregiver and 38.5% had undertaken other rehabilitation pathways. The results of the study show a reduction in the average HoNOS scale scores at 6 and 12 months compared to baseline in the four subscales considered. Considering the HoNOS scale in its entirety, there was a considerable decrease in the score from an overall mean of 2.1 at baseline to 1.3 at the end of the 12-month study period (Table 2). In all subscales considered, this decrease is statistically significant. The analysis of the data showed that the adjustment of the organisational set-up produces greater improvements especially in the initial phase (after 6 months) with a very significant decrease in average scores. After 6 months from the start of the study there is a stabilisation of the average HoNOS Total and subscale scores. Table 5 shows the p-values of the multiple comparisons between the groups; the scores of the groups compared were statistically significant with the exception of the scores taken at 6 and 12 months for the subscales of "behavioural problems", "deficits and disabilities" and "relational/environmental problems" and the scores taken at 6 months and at baseline for "psychopathological symptoms".
Similarly to a study by Buratti et al. [17], it is important to underline that, in the face of a clear prevalence of pharmacological treatments, the items that undergo a clear improvement are precisely those on which the drug has a direct effect (e.g. items concerning behavioural problems, deficits and disabilities and psychopathological symptoms), while the items concerning problems that would also require the use of other types of treatments (e.g. relational, environmental items) show a smaller decrease in average scores. Other data in the literature demonstrate the importance of using the HoNOS scale for assessing outcomes in patients with mental illness. A first longitudinal study in 3 times (14 months) was carried out in the Mental Health Services of the A.O. Ospedale Niguarda Ca' Granda in order to contribute to the validation of the Italian version of the HoNOS scale and to make operators aware of the importance of a standardised assessment of outcomes. With regard to the results on improvement (clinically significant criterion of 7 points), improved patients correspond to 45.3% of the sample after 14 months from the start of the study [16]. Two other longitudinal studies [18,19] in three stages and with a two-year follow-up, were implemented in a Mental Health Centre in Rome where the following were analysed: the relationship between the severity detected by HoNOS and the ICD-9-CM diagnosis; the convergence between the two instruments; the relationship between HoNOS severity and the types of interventions used by the Mental Health Centre (psychiatric interview, psychological interview, psychotherapy, pharmacotherapy, home visits, rehabilitation, insertion in residential facilities) in order to assess the distribution of resources and finally the improvement of patients in one year. The results found convergence between HoNOS and ICD-9, appropriate use of interventions in relation to the specificity and severity of the diagnosis, and an improvement in patients with a significant decrease in mean scores.
Further studies have involved the Mental Health Departments of the A.O. Ospedale Niguarda Ca' Granda as part of the introduction of a tool to formalize the Individual Treatment Plan (I.T.P.) in which the HoNOS scale is used for assessment and final evaluation of the chosen treatment [19,20]. In this research several aspects were evaluated: the type of intervention foreseen (counselling, intake, treatment), the treatments carried out (pharmacotherapy, psychotherapy, work placement, family involvement, etc.), the outcome of the intervention (re-evaluation at 6 months in case of intake and treatment), drop-out, costs, the role of the case manager and the impact on the work of the operators. The results showed a statistically and clinically significant improvement in severity scores even though there was a medical/nursing imbalance in the treatments provided. The number of psychological, social and rehabilitation treatments is still too low. In psychiatric services, the professional figure and services of psychiatrists predominate, to the detriment of the scarce presence of psychologists/psychotherapists, despite the fact that psychotherapy has been shown to bring about greater and more constant changes over time than the use of medication alone [19]. For this reason, one of the innovative elements in the study was to go beyond the medical-centric model in favour of interdisciplinary teamwork. In community psychiatry, all professionals must be united by a single aim: to provide patients with opportunities to use the skills learned in rehabilitation programmes in natural environments and to increase the quality of their lives. In order to ensure such integration, it is necessary to establish and implement an interdisciplinary and multidisciplinary team, whose operation is ensured by individual and collective tasks, well-defined performance standards, supervision and continuous on-the-job training [21]. It becomes a moral duty to assess whether in one's own reality, with one's own patients, colleagues, organisational difficulties and shortcomings, one can achieve the same results as in experimental effectiveness studies. It is possible, in everyday clinical practice, to routinely assess the outcome of hospitalisation using a scale such as the HoNOS, because not only is it simple and quick to fill in, but above all because it satisfactorily describes the changes induced by the period of hospitalisation.
CONCLUSIONS
In recent decades, mental health care has seen a shift from symptom management to the promotion of quality of life within psychiatric facilities: both patients and their relatives consider quality of life as one of the main goals of mental health care [22]. Rehabilitation facilities should be aimed at social integration; provide for a maximum length of stay of 24 months, with a 24-hour presence of health and psycho-socio-educational staff; provide for areas of involvement of patients and relatives [5]. The results of this pilot study show how an organisational reorganisation aimed at adopting principles, developing policies and implementing actions to help people with mental disabilities can improve the quality of hospitalisation and consequently the quality of life of patients with mental disorders. Achieving the best possible biopsychosocial functioning compatible with functional deficits, persistent psychopathology and relapses, involving the family and the general practitioner from the earliest stages of the patient's contact with the facility are fundamental aspects of a care pathway for patients with mental disorders. At the end of a residential treatment programme, there should be a continuation of rehabilitation and care treatment by the mental health centres (CSM) in the region, where there is support and home visits through a single and integrated socio-health pathway with re-evaluation over time of patients under treatment for mental disorders. The evaluative approach should not be seen by practitioners as an inquisitorial control, but as an opportunity geared towards improving care, the severity of patients and the outcome of their treatment. The use of HoNOS in Psychiatric Facilities should not be considered as a goal, but as a starting point for a journey towards a more adequate clinical practice for the management of patients with mental disorders, which favours the effectiveness of treatments and the self-reflection of professionals [16].
LIMITATIONS OF THE STUDY
Despite the supervision of the nursing coordinator and the medical director of the facility, a potential information bias due to the detector effect (degree of subjective evaluation of information) is present and cannot be eliminated. The main limitation is the small sample size, which does not allow confounding factors such as diagnosis, age at onset, etc. to be taken into account in the statistical analysis. Although the results show a reduction in mean scores at 6 and 12 months compared to baseline, a longer observation period would be desirable to allow further evaluations of the effectiveness of the biopsychosocial intervention.
POSSIBLE FUNDING
This research has not received any form of funding.
CONFLICTS OF INTEREST
The authors declare that they received no funding for the following study and have no financial interest in the subject matter or the results obtained.
REFERENCES
- La rete dei servizi per la salute mentale disponibile al seguente url: https://www.salute.gov.it/portale/saluteMentale/dettaglioContenutiSaluteMentale.jsp?lingua=italiano&id=168&area=salute%20mentale&menu=vuoto#:~:text=Il%20Dipartimento%20di%20salute%20mentale,Azienda%20sanitaria%20locale%20(ASL). Data ultima consultazione 04/01/2022
- Amaddeo, F., Bacigalupi, M., de Girolamo, G., Di Munzio, W., Lora, A., & Semisa, D. (1998). Attivitá e interventi del Dipartimento di Salute Mentale. Epidemiologia e Psichiatria Sociale. Monograph Supplement, 7(S2), 13–30.
- Cerati, G., Ciancaglini P., Ferrannini L., Merckling D. (2015) http://www.nuovarassegnastudipsichiatrici.it/attachments/article/140/NRSP-Vol.12-13-I-programmi-di-residenzialita-leggera-tra-recente-normativa-nazionale-ed-esperienze.pdf. Data ultima consultazione 27/02/2022
- Lora A., Starace F., Di Munzio W., Fioritti A. (2014). Italian community psychiatry in practice: description and comparison of three regional systems. J Nerv Ment DIs. 202(6):446-50
- Allegato A – Accordo tra il Governo, le Regioni e le Province autonome di Trento e di Bolzano, le Province, i Comuni e le Comunità montane sul documento concernente “Le strutture residenziali psichiatriche”. Rep. Atti n. 116/CU del 17 ottobre 2013
- G.R.M. 1331/14- Regione Marche. 25 novembre 2014
- Percudani M., Cerati G. et al. (2012). I modelli regionali nelle politiche di salute mentale. Sistema Salute, 56, 2, 2012: pp. 192-204
- Hatala A.R. (2012). The Status of the “Biopsychosocial” Model in Health Psychology: Towards an Integrated Approach and a Critique of Cultural Conceptions. Open Jurnal of Medical Psychology. 1, 51-62
- Markowitz F. E. (2001). Modeling processes in recovery from mental illness: relationships between symptoms, life satisfaction, and self-concept. J Health Soc Behav. 42(1):64-70
- Borrel-Carriò F., Suchman A.L., Epstein R.M. (2004). The biopsychosocial model 25 years later: principles, pratice, and scientific inquiry. Ann Fam Med. 2(6): 576-82
- Angermeyer MC, Holzinger A, Kilian R, Matschinger H (2001) Quality of life—as defined by schizophrenic patients and psychiatrists. Int J Soc Psychiatry 47:34 –42
- Picardi, A., Rucci, P., de Girolamo, G., Santone, G., Borsetti, G., & Morosini, P. (2006). The quality of life of the mentally ill living in residential facilities. European Archives of Psychiatry and Clinical Neuroscience, 256(6), 372–381.
- Deliberazione n. 7/17513 del 17 Maggio 2004: Piano regionale Triennale per la Salute Mentale in attuazione del Piano Socio Sanitario Regionale 2002-2004
- Preti A., Pisano A., Cascio MT., et al. (2012). Validation of the Health of the Nation Outcome Scales as a routine measure of outcome in early intervention programmes. Early Interv Psychiatry. 6(4):423-31
- Wing J., Curtis R.H., Beevor A.S., Park B.G., Hadden S. & Burns A. (1998). Healt of the Nation Outcome Scales (HoNOS): research and development. British Journal of Psychiatry 172, 11-18
- Lora A., Bai G., Bianchi S., Bolongaro G., Civenti G., Erlicher A., Maresca G. Monzani E., Panetta B., Von Morgen D., Rossi F., Torri V. & Morosini P. (2001). La versione italiana della HoNOS (“Healt of the Nation Outcome Scales”), una scala per la valutazione della gravità e dell’esito nei servizi di salute mentale. Epidemiologia e Psichiatria Sociale 10, 198-212
- Buratti, E., Vigorelli, M., Gallucci, M., Moranti, C., Schiavolin, S., & Peri, Y. (2006). Valutazione con HoNOS (Health of the Nation Outcome Scales) nei servizi territoriali di Niguarda a Milano: uno studio longitudinale. Relazione presentata al VI Congresso Nazionale S.P.R.-Italia “Tra Scilla e Cariddi”, Reggio Calabria
- Vigorelli, M., Correale, A., Criconia, M., Bolzoni, C., Stirone, V., & Schlosser, S. (2008). Accoglimento nei primi colloqui, profili diagnostici e di cura: una ricerca sul campo in 2° area. Relazione presentata alla Giornata di studio “Il servizio conosce se stesso? Ricerca sugli esiti e appropriatezza degli interventi”, DSM, Roma B
- Vigorelli M. (2010). Ricerca multistrumentale in psicoterapia, valutazione in psicosomatica e nei servizi psichiatrici: gruppo di ricerca coordinato da Marta Vigorelli. Ricerca in Psicoterapia / Research in Psychotherapy; 2(13): 287-321
- Manfrè, S., Simoncini, L., Scordari, S., Segato, C., Vigorelli, M., & Re, E. (2009). Pratica clinica strutturata e valutazione di esito: l’esperienza del DSM di Milano Niguarda. Psichiatria di Comunità, 8(4), 31–40
- Moxham L., Patterson C., Taylor E., Perlman D., Sumskis S., Brighton R. (2017) A multidisciplinary learning experience contributing to mental health rehabilitation. Disabil Rehabil. 39(1):98:103.
- Salvi G., Leese M., Slade M. (2005). Routine use of mental health outcome assessments: choosing the measure. British Journal of Psychiatry, 182(2), 146-152
![]() This work is licensed under a Creative Commons
This work is licensed under a Creative Commons
Attribution-NonCommercial-NoDerivatives 4.0 International License.
The Effect of Spirotive Relaxation Techniques in Reducing the Level of Osteoarthritic Pain in the Elderly: Quasi Experiment Design
Abbasiah1*, Monalisa1, Yunike1, Mohd Syukri1, Dewi Masyitah1
- Department of Nursing, Health Polytechnic of Jambi, Indonesia.
* Corresponding author: Abbasiah, H. Department of Nursing, Health Polytechnic of Jambi, Indonesia; Agus Salim Street, Kota baru Jambi, 36129 Indonesia. Orcid: https://orcid.org/0000-0001-7692-7337. Email: ummiabbasiah35@gmail.com

Cita questo articolo
Abstract
Introduction: Pain is a common issue in the elderly. Osteoarthritis is often encountered in the elderly and contributes significantly to pain. Pain complaints involve multifactorial and often face many hindrances in the management.
Objective: This study aims to determine the effect of spirotive relaxation techniques in reducing osteoarthritis pain scale in the elderly.
Methods: This quasi-experimental study used the Pre-Post Test Control Group Design, conducted in the Penyengat Olak and Sungai Duren Community Health Center, Jambi Province, Indonesia, from September to November 2021. Sixty-four elderly participants in this study were divided into Spirotive relaxation exercise and dhikr as the intervention group and the control group given Spirotive relaxation exercise only. Data analysis used t-test and independent t-test at a significant level of 95%.
Results: There are differences in pain levels of the intervention group before and after Spirotive relaxation exercise and dhikr. Before the intervention, pain levels were moderate to severe, and pain levels were mild to moderate after the intervention. Similar results were also obtained in the control group given Spirotive relaxation exercise only with a significant reduction in pain. The independent test results showed a p-value = 0.207, indicating no difference in osteoarthritis pain in the intervention and control groups.
Conclusion: Spiritual relaxation exercises have been shown to reduce pain levels in the elderly with osteoarthritis. There are also differences in the level of joint pain scale in the intervention and control groups. It suggests that public health centers provide non-pharmacological inspirational interventions as an additional therapy for the elderly.
Keyword: Osteoarthritic, Pain, Spirotive, Elderly
Introduction
Various health problems will arise along the ageing process and rising age. It is mainly a physical inconveniences problem, such as ailments of musculoskeletal function [1]. Pain in the joints frequently becomes an obstacle for the elderly to carry out daily activities [2,3]. Osteoarthritis is the most common joint disease, which increases in age. The ageing process exerts a shrinking effect on human muscle fibres. Muscle strength will undoubtedly decrease due to the shrinkage of muscle mass impacting the weakness in activity or movement, thereby reducing the quality of life. In addition, it also affects bone mass diminishes. The elderly with regular exercise do not encounter the same loss as the sedentary elderly [4].
Approximately 20% of the world's population obtains joint pain at 55 years old. The current increase in the elderly population goes hand in hand with an increase in the number of cases of joint pain [5,6]. Accordingly, the prevalence of joint disease in Indonesia is 7.3%, of which 45.58% arises in the 56-65 age group, 82.54% is discovered in the female group, and 53.26% complains of knee pain [7].
Knee Osteoarthritis (OA) is a common progressive multifactorial joint disease characterized by chronic pain and functional disability [4]. Knee OA accounts for almost four-fifths of the burden of OA worldwide and increases with obesity and age [6]. Knee arthroplasty is considered an effective treatment at an advanced stage of the disease. However, which is responsible for substantial health costs [5]. Many researchers have shifted their focus to the prevention and treatment in the early stage of the disease [2]. Accordingly, it is essential to understand the prevalence, incidence, and modifiable risk factors of knee OA to provide efficacious preventive strategies [3,8].
Non-pharmacological management of osteoarthritis pain in the elderly include Spirotive Relaxation Exercise (SRE) and dhikr [9]. Spirotive relaxation is a combination and modification of progressive muscle relaxation and spiritual relaxation (dhikr) interventions. Relaxation begins with dhikr, then relaxes muscle tension. Those activities are expected to obtain His grace in the form of peace, tranquillity, happiness, health and physical fitness. [10].
Spiritual Relaxation (Dhikr) involves praising, remembering, and submitting supplications to God in resignation [11]. Medically, it has been proven that dhikr will automatically stimulate the secretion of endorphins to feel happiness and comfort [12]. Yusuf et al. [11] found changes in psychological well-being in the treatment group before and after the dhikr intervention.
The Spirotive Relaxation Exercise (SRE) is based on the Comfort theory of Kolcaba [13]. Comfort is the main goal in nursing because it is closely related to healing [14–16]. According to Yusuf, et al [11] Spiritual Relaxation intervention can provide comfort by doing SRE and spiritual relaxation (dhikr). Sound waves during dhikr will stimulate auditory receptors. Furthermore, the stimulus will be forwarded to the temporal lobe to catch the point of God (circuit of God). The prefrontal cortex will respond to stimuli at the point of God for the process of forming positive perceptions, both emotionally and spiritually. The amygdala will respond to the prefrontal cortex to the hippocampus as feedback. In addition, the amygdala also stimulates the hypothalamus through the hypothalamic-pituitary-adrenal (HPA) axis to secrete corticotrophin-releasing factor (CRF).
SRE induces muscle contraction of the skeletal fibers, leading to muscle tension [17,18]. In this case, the central nervous system (CNS) involves the sympathetic nervous system and the parasympathetic nervous system [19]. Several organs are affected by these two nervous systems [20]. Sympathetic and parasympathetic nerves work reciprocally. Activation of the parasympathetic nervous system, also called Trophotropic, provides a desire to rest and physical improvement of the body [20,21]. The feeling of comfort and relaxation may reduce even eliminate pain [18,22–24].
Gonçalves, et al [25] stated that dhikr could reduce joint pain in the elderly with knee osteoarthritis. Another study stated that being more active may reduce pain and the risk of functional impairment or disability [26].
Joint pain is a subjective experience that impacts the quality of life and impaired functional activities of the elderly. Therefore, adequate treatment is needed. Non-pharmacological intervention SRE has the potential to reduce the intensity of osteoarthritis pain. To the best of our knowledge, this has never been studied. Therefore, this study aims to determine the effectiveness of Spirotive Relaxation Exercises to reduce osteoarthritis pain in the elderly.
Methods
Research design
The research design used in this study was Experimental with a Quasi Experiment Design in Pre-Post Test Control Group approach. This study revealed a causal relationship by involving the control group and the experimental group.
Research Time and Place
The study was conducted in the working area of the Penyengat Olak and Sungai Duren Community Health Center, Jambi Province, Indonesia, from September to November 2021.
Participants
The participants in this study were all the elderly in the Penyengat Olak Health Center (n=32 people) and the elderly at the Sungai Duren Health Center (n=32 people).
Intervention
SRE is administered independently for 45 minutes twice a week for four weeks. SRE measurement used SOP, While the pain level was measured using the WOMAC Questionnaire. In this index, 24 parameters consisting of pain, stiffness, physical and social function were evaluated using WOMAC. The higher value obtained indicates the magnitude of the patient's functional limitations. The higher the value obtained indicates the magnitude of the patient's functional limitations.
In comparison, the lower value indicates improved functional ability. WOMAC parameters include (1) the presence of pain, which aspects are assessed when walking, climbing stairs, doing activities at night, at rest and when supporting (2) the presence of stiffness in the morning and stiffness throughout the day (3) the state of physical function Patients have difficulty going downstairs, difficulty going upstairs, difficulty from sitting to standing, difficulty standing, difficulty sitting on the floor, difficulty walking on a flat surface, difficulty getting in and out of a vehicle, difficulty shopping, difficulty wearing socks, difficulty lying in bed, difficulty taking off socks, difficulty sitting, difficulty doing heavy tasks and difficulty doing light tasks. WOMAC produces an algorithmic value obtained from a questionnaire to measure pain and disability in patients' knees. In the questionnaire, the answers were given a 0 - 4. Each score represents the patient's perceived state. Details of the WOMAC questionnaire can be seen in the table. Furthermore, the scores of the 24 questions are added up divided by 96 and multiplied by 100% to find out the total score and categorized as Mild (0-40%), moderate (40%-70%), and severe (70%-100%). The greater the score, the more severe the pain and disability of the knee [27,28].
The Assessment of pain is based on stiffness and physical function with mild, moderate, and severe categories. The intervention group was given SRE and reciting dhikr, while the control group only received SRE.
Outcomes
The output of this study was to determine the level of pain and the differences in pain levels before and after giving spirotive relaxation exercises.
Sample size
The sample in the current study was 64 participants divided into two groups, 32 participants as group intervention and 32 participants as group control. The minimum sample size was determined using the GPower software version 3.1.9.4, where the effect size d = 0.63, alpha = 0.05, at power 0.80 with a sample ratio of 1:1. The sample size for group 1 was 32 and group 2 was 32 for a total of 64. The sample was randomly selected. The sample size in the study initially involved 124 potential participants, whereas 60 people did not meet the criteria. The inclusion criteria for the sample were 45-80 years old, a minimum education level of Elementary School (SD), and no cognitive impairment (MMSE score >23). At the same time, the elderly with limited range of motion and bed rest were excluded.
Randomisation
Participants were selected from the total population using a simple random technique. Sample selection includes determining prospective participants, selecting participants, and reporting participants to researchers. Enumerators received a briefing on applying the sample selection mechanism for the provision of SRE and dhikr.
Blinding
The included samples were selected blindly. The enumerator who had been assigned by the researcher did not previously know the potential participants.
Ethical Consideration
No economic incentives were offered or provided for participation in this study. The study was performed under the ethical considerations of the Helsinki Declaration by the Health Research Ethics Commission of the Ministry of Health, Jambi, and registration number: LB.02.06/2/59/2021.
Statistical analysis
Description of participant characteristics (age, gender, education level, and occupation) and osteoarthritis pain before and after the intervention is based on univariate analysis results. Data are presented as numbers and percentages for categorical variables. Continuous data were expressed as mean ± standard deviation (SD) or median with Interquartile Range (IQR). The normality test used the Kolmogorov-Smirnov test with Lilliefors significance correction.
In bivariate analysis, a t-test was used to assess the effect of spiritual healing and dhikr in the intervention and control groups. In contrast, an independent t-test was used to determine differences in osteoarthritis pain intensity between the two study groups. All tests with p-value (p)<0.05 were considered significant. Statistical analysis was performed using SPSS version 16.0.
Results
The characteristics of respondents are presented in table 1 below :

Table 1. Characteristics of Respondents
Characteristics of respondents from the two groups are based on gender, primarily female, 62.5% from the intervention group, and 68.7% from the control group. The characteristics of respondents based on age were mainly in the elderly group (60-74) years, 56.3% in the intervention group, and 53.1% in the control group. Based on education level, most respondents were junior high school, as much as 53% in the intervention group and 50% in the control group. Characteristics of respondents based on the type of work show that most respondents did not work, as much as 87.5% in the intervention group and 90.7% in the control group.
The description of osteoarthritis pain in the intervention group before and after the intervention presented in table 2 below:

Table 2. Description of pain scale before and after spirotive intervention in the intervention group
Table 2 shows that the scale of osteoarthritis pain before the SRE was mild pain (6.3%), moderate pain (46.9%), and severe pain (46.9%). The osteoarthritis pain scale felt by respondents after the SRE was mild pain (37.5%), moderate pain (56.3%), and severe pain (6.3%).
The description of osteoarthritis pain in the control group before and after the intervention presented in table 3 below:

Table 3. Description of pain scale before and after spirotive intervention in the control group
Table 3 shows that the scale of osteoarthritis pain before SRE was 15.6% in mild pain, 65.6% in moderate pain, and 18.8% in severe pain. After the intervention, it was found that participants felt mild pain (59.4%), moderate pain (37.5%), and severe pain (3.1%).
Furthermore, the data normality test was carried out using the Kolmogorov-Smirnov test to determine the distribution of research data. The results of the data normality test are presented in table 4 below:

Table 4. Data Normality Test
Table 4 shows that the p-value of the intervention group > 0.05, as well as the p-value of the control group > 0.05, so it can be concluded that the data is normally distributed.
The condition of painful scale before and after the intervention in Group 1 and Group 2 can be seen in the table 5 below:

Table 5. Frequency distribution of Group Intervention and Group Control before and after interventions
Table 5 shows a significant decrease in pain level in both groups before and after the intervention with a p-value <0.05. Based on the t independent test, it was found that the p-value for the pre-test (<0.005) and the post-test was 0.207. The post-test value showed no difference between the two research groups.
Discussions
The t-test result of pre-post intervention revealed a decrease in pain. In both the intervention and control groups, the p-value was <0.05. The independent t-test showed differences in the two groups before the intervention with a p-value <0.05, but after the intervention (post-test), the p-value was >0.05. It indicates that SRE and dhikr therapy may reduce knee OA pain in the elderly.
Older people with osteoarthritis often run into joint pain [29,30]. These complaints are often found in geriatric care in the community and clinic. This study provides an SRE intervention with a combination of spiritual techniques: dhikr (spirotive) to reduce joint pain in the elderly with osteoarthritis [24]. Joint disease is a degenerative process and causes pain in the elderly [31]. Pain itself can be caused by several conditions, including rheumatoid arthritis, gout (uric acid), and osteoarthritis [32]. SRE is a technique for reducing muscle tension by a simple and systematic process of stretching a group of muscles and then relaxing back [33].
SRE focuses on maintaining a deep form of relaxation, applying contraction and relaxation of various muscle groups from the feet up or from the head down. This method will realise where the muscles are located and increase awareness of the body's muscle response [34,35]. SRE may reduce pain, anxiety, depression, improve sleep quality, and reduce fatigue [36].
Religious relaxation (dhikr) is a technique that includes a belief factor. In this study, we used the element of Islamic belief with the repeated praise of God's name submissively [11]. Religious relaxation: dhikr is one of the efforts to meet the psychological needs of the elderly through the fulfillment of spiritual needs. It is also a practice of prayer to God by continuously remembering God name submissively. The essence of dhikr is praying for forgiveness, praising and glorifying God, being grateful, takbir to humble before God. Finally, eliminate ourselves and our ego against God's ego in all the activities we do [37].
Dhikr relaxes the body and produces impulses sent through afferent nerve fibers. Physiologically, spiritual therapy by dhikr or remembering God's name causes the brain to work. When the brain gets external stimulation, it will produce neuropeptides chemicals to provide comfort. The substances will be involved and absorbed in the body, providing feedback in comfort. Psychologically dhikr will balance serotonin and norepinephrine levels in the body. This phenomenon is natural morphine that works in the brain and will cause the heart and mind to feel calm compared to before dhikr [37].
The results of this study must be interpreted cautious because the limitations of this study are: the patient was not directly supervised by the researcher in doing dhikr. It is difficult to determine the quality of dhikr performed by a person, and there are no clear parameters to determine it. Supposedly, the acceptable quality of dhikr will give a calming effect. It could result in no difference in pain levels between the two groups after the intervention. In future studies, supervision should be conducted strictly when the intervention ensues. The strength of this study lies in its RCT design, using an intervention that has never been done before in patients with osteoarthritis pain.
Conclusion
SRE has been proven to reduce joint pain scale in the elderly with osteoarthritis, and there are also differences in joint pain scale levels in the intervention and control groups.
It is suggested that the community health centers may use SRE as an additional therapy for the elderly. Increasing the capacity of elderly health assistance needs to be carried out by the community health centers to increase the knowledge and behavior of the elderly in overcoming problems related to their degenerative conditions.
The limitations
The limitations of this study include a small sample and only involving respondents in one country, namely Indonesia, so it cannot compare the intervention responses in each different ethnic group.
Acknowledgement
We would like to express our gratitude to the director of the Midwifery Department of Jambi health polytechnic who has supported this research.
Funding statement
This research did not receive any specific grant from funding agencies in the public, commercial, or not for profit sectors.
Competing interests statement
There are no competing interests for this study.
References
- Gignac MAM, Davis AM, Hawker G, Wright JG, Mahomed N, Fortin PR, et al. “What do you expect? You’re just getting older”: a comparison of perceived osteoarthritis‐related and aging‐related health experiences in middle‐and older‐age adults. Arthritis Care & Research: Official Journal of the American College of Rheumatology. 2006;55(6):905–12.
- Glyn-Jones S, Palmer AJR, Agricola R, Price AJ, Vincent TL, Weinans H, et al. Osteoarthritis. The Lancet. 2015;386(9991):376–87.
- Peat G, Thomas MJ. Osteoarthritis year in review 2020: epidemiology & therapy. Osteoarthritis and Cartilage. 2021;29(2):180–9.
- Hunter DJ, Bierma-Zeinstra S. Osteoarthritis. The Lancet. 2019;393(10182):1745–59.
- McAlindon TE, Bannuru R, Sullivan MC, Arden NK, Berenbaum F, Bierma-Zeinstra SM, et al. OARSI guidelines for the non-surgical management of knee osteoarthritis. Osteoarthritis and cartilage. 2014;22(3):363–88.
- Vos T, Allen C, Arora M, Barber RM, Bhutta ZA, Brown A, et al. Global, regional, and national incidence, prevalence, and years lived with disability for 310 diseases and injuries, 1990–2015: a systematic analysis for the Global Burden of Disease Study 2015. The lancet. 2016;388(10053):1545–602.
- Kemenkes RI. Hasil utama RISKESDAS 2018. Kementerian Kesehatan Badan Penelitian dan Pengembangan Kesehatan. Jakarta; 2018.
- Cui A, Li H, Wang D, Zhong J, Chen Y, Lu H. Global, regional prevalence, incidence and risk factors of knee osteoarthritis in population-based studies. EClinicalMedicine. 2020;29:100587.
- Hidayat S, Mumpuningtias ED, Indriyani R. The Combination Therapy of Self-Surrender Exercise and Distraction Against Osteoarthritis Pain Scale of Elderly In Coastal Area. STRADA Jurnal Ilmiah Kesehatan. 2020;9(2):1212–22.
- Chamsi-Pasha M, Chamsi-Pasha H. A review of the literature on the health benefits of Salat (Islamic prayer). The Medical journal of Malaysia. 2021;76(1):93–7.
- Yusuf A, Sriyono S, Kurnia ID. The Beneficience Of Religious Relaxation: Dzikir To Increase Phsycological Wellness Of Elder. Jurnal Ners. 2008;3(1):81–6.
- Patimah I, Suryani S, Nuraeni A. Pengaruh Relaksasi Dzikir terhadap Tingkat Kecemasan Pasien Gagal Ginjal Kronis yang Menjalani Hemodialisa. Jurnal Keperawatan Padjadjaran. 2015;3(1).
- Kolcaba K. Katharine Kolcaba’s comfort theory. Nursing theories and nursing practice. 2015;381–92.
- Kolcaba KY. A theory of holistic comfort for nursing. Journal of advanced nursing. 1994;19(6):1178–84.
- Narayanasamy A, Clissett P, Parumal L, Thompson D, Annasamy S, Edge R. Responses to the spiritual needs of older people. Journal of advanced nursing. 2004;48(1):6–16.
- Kolcaba K. Comfort theory and practice: a vision for holistic health care and research. Springer Publishing Company; 2003.
- Baird CL, Murawski MM, Wu J. Efficacy of guided imagery with relaxation for osteoarthritis symptoms and medication intake. Pain management nursing. 2010;11(1):56–65.
- de Lorent L, Agorastos A, Yassouridis A, Kellner M, Muhtz C. Auricular acupuncture versus progressive muscle relaxation in patients with anxiety disorders or major depressive disorder: a prospective parallel group clinical trial. Journal of acupuncture and meridian studies. 2016;9(4):191–9.
- Akmeşe ZB, Oran NT. Effects of progressive muscle relaxation exercises accompanied by music on low back pain and quality of life during pregnancy. Journal of midwifery & women’s health. 2014;59(5):503–9.
- Kegel AH. Progressive resistance exercise in the functional restoration of the perineal muscles. American journal of obstetrics and gynecology. 1948;56(2):238–48.
- Dhyani D, Sen S, Raghumahanti R. Effect of progressive muscular relaxation on stress and disability in subjects with chronic low back pain. IOSR Journal of Nursing and Health Science. 2015;4(1):40–5.
- Zulvana Z, Eka MMH. Spirotif Relaxation Improve Anxiety and Sleep Quality in Elderly [Internet]. The 9th International Nursing Conference 2018. “Nurses at The Forefront in Transforming Cre, Science, and research.” 2018. Available from: http://eprints.ners.unair.ac.id/815/3/Spirotif Relaxation Improve Anxiety and Sleep Quality in Elderly.pdf
- Mualimah N, Nurbaeti I, Palupi P. The Effectiveness Of Dhikr To Intensity Of Pain During Active Phase In Mothers Getting Inducing Labour. Jurnal Keperawatan Padjadjaran. 2020;8(2):184–92.
- Ulfiiana E, Mujtaba AH, Nihayati HE. Effect of Psycho Religious Dhikr Therapy on the Level of Anxiety in Elders Living in the Orphanage. Journal of Computational and Theoretical Nanoscience. 2021;18(1–2):313–8.
- Gonçalves JPB, Lucchetti G, Menezes PR, Vallada H. Religious and spiritual interventions in mental health care: a systematic review and meta-analysis of randomized controlled clinical trials. Psychological medicine. 2015;45(14):2937–49.
- Egan BA, Mentes JC. Benefits of physical activity for knee osteoarthritis: a brief review. Journal of gerontological nursing. 2017;36(9):9–14.
- Brown GA. AAOS clinical practice guideline: treatment of osteoarthritis of the knee: evidence-based guideline. JAAOS-Journal of the American Academy of Orthopaedic Surgeons. 2013;21(9):577–9.
- Carlson VR, Ong AC, Orozco FR, Hernandez VH, Lutz RW, Post ZD. Compliance with the AAOS guidelines for treatment of osteoarthritis of the knee: a survey of the American Association of Hip and Knee Surgeons. JAAOS-Journal of the American Academy of Orthopaedic Surgeons. 2018;26(3):103–7.
- Wilcox S, Brenes GA, Levine D, Sevick MA, Shumaker SA, Craven T. Factors related to sleep disturbance in older adults experiencing knee pain or knee pain with radiographic evidence of knee osteoarthritis. Journal of the American Geriatrics Society. 2000;48(10):1241–51.
- Neogi T. The epidemiology and impact of pain in osteoarthritis. Osteoarthritis and cartilage. 2013;21(9):1145–53.
- Hawker GA, Stewart L, French MR, Cibere J, Jordan JM, March L, et al. Understanding the pain experience in hip and knee osteoarthritis–an OARSI/OMERACT initiative. Osteoarthritis and cartilage. 2008;16(4):415–22.
- Fu K, Robbins SR, McDougall JJ. Osteoarthritis: the genesis of pain. Rheumatology. 2018;57(suppl_4):iv43–50.
- Gurudut P, Jaiswal R. Comparative Effect of Graded Motor Imagery and Progressive Muscle Relaxation on Mobility and Function in Patients with Knee Osteoarthritis: A Pilot Study. [Internet]. Alternative Therapies in Health and Medicine. 2020. Available from: https://europepmc.org/article/med/33128533
- Baird CL, Sands L. A pilot study of the effectiveness of guided imagery with progressive muscle relaxation to reduce chronic pain and mobility difficulties of osteoarthritis. Pain Management Nursing. 2004;5(3):97–104.
- Bernstein DA, Carlson CR, Schmidt JE. Progressive relaxation. Stress Management. 2007;88.
- Kobayashi S, Koitabashi K. Effects of progressive muscle relaxation on cerebral activity: an fMRI investigation. Complementary therapies in medicine. 2016;26:33–9.
- Hidayat S. Dzikir Khafi untuk Menurunkan Skala Nyeri Osteoartritis Pada Lansia. Journal Of Health Science (Jurnal Ilmu Kesehatan). 2014;1(1):13–22.
![]() This work is licensed under a Creative Commons
This work is licensed under a Creative Commons
Attribution-NonCommercial-NoDerivatives 4.0 International License.