Pierluigi Ricchiuto1, Stefania Impicci2, Martina Schiano3
1.Nurse at the Department of Emergency and Acceptance, Emergency Department – OBI, Asl Napoli 2 Nord, Santa Maria delle Grazie Hospital, Pozzuoli.
2.Nurse at “Casa Rossa” Residential Rehabilitation Centre. Area Vasta 2 – Ancona.
3.Nurse at UOS Clinical Risk, AORN – Ospedale dei Colli, Monaldi Hospital, Naples.
*Corresponding Author: Pierluigi Ricchiuto, Department of Emergency and Acceptance, Emergency Department – OBI, Asl Napoli 2 Nord, Santa Maria delle Grazie Hospital, Pozzuoli.
Email: pierluigi.ricchiuto@aslnapoli2nord.it
Cita questo articolo
ABSTRACT
Background: The Italian health system related to mental disorders is currently experiencing a period of radical reforms. This process began in 1978 with the adoption of the law 180 which produced a radical reform in mental health care. The problems of the continuous confrontation with increasing levels of expenditure are reflected in the search for models to improve both the efficiency and effectiveness of the health care system. Among these, the value creation model proposes to optimize the relationship between effectiveness, quality, and appropriateness of care on the one hand, and efficiency, cost and how resources are used on the other. The intervention involves redesigning services on the principles of recovery; implementing treatments supported by scientific evidence; encouraging processes of social inclusion. The proposed rehabilitation interventions are recovery oriented that place the person at the center of his rehabilitation path, motivating him in assuming responsibility for the treatment proposed during hospitalization.
Objective: Evaluate the impact of the organisational reorganisation of the DSM S.R.R Regional Health Service of Ancona Area Vasta 2 by introducing evidence-based and recovery-oriented practices through the evaluation of clinical outcomes and psychosocial functioning.
Methods: Longitudinal descriptive observational study with evaluation of a cohort of 13 patients, hospitalized in residential and semi-residential care at SRP1 “Casa Rossa” Area Vasta 2 of Ancona, by administration of a questionnaire (HoNOS) at the time of recruitment (February 2019), at 6 months (August 2019) and at 12 months (February 2020). The 12 items of the questionnaire were grouped into four subsets: behavioural problems (items 1-3), deficits and disabilities (items 4-5), psychopathological symptoms (items 6-8) and relational/environmental problems (items 9-12).
Results: Survey results show a reduction in mean scores at 6 and 12 months compared to baseline in all subscales.
Conclusions: Intensive mental health residential facilities need to put more effort into evaluating effectiveness in practice, using appropriate tools for outcome assessment and analysis of results. It is possible, in daily clinical practice, to evaluate the outcome of admissions in order to satisfactorily describe the changes induced during the period of hospitalization.
Keywords: outcome of care, mental health, psychiatric facility, biopsychosocial.
INTRODUCTION
The Department of Mental Health (DSM in Italian) is the set of facilities and services whose task is to take charge of the demand for care, assistance and protection of mental health; it is the body which governs, coordinates and manages Community Psychiatry, guaranteeing the unity and integration of psychiatric services within the area of competence defined by ASUR Marche [1]. Moreover, the DSM’s task is to promote mental health and quality of life in the target population; to guarantee primary and secondary prevention of mental disorders with the early detection of situations of distress and tertiary prevention with the reconstruction of the affective, relational, social and work fabric [2]. The typology of psychiatric residential facilities is distinguished both by the level of therapeutic-rehabilitative intervention, related to the level of impairment of the patient’s functions and abilities (and its treatability), and by the level of care intensity offered, related to the overall degree of autonomy. Psychiatric residential facilities for intensive therapeutic rehabilitation treatment (SRP1) are facilities for patients with severely impaired personal and social functioning. These structures play a transitional role, aimed at reintegrating the patient into his/her usual living environment (generally family) [3,4]. The intervention areas of SPR1 concern the clinical psychiatric, psychological, rehabilitation, resocialisation and coordination areas. The new organisation of the Psychiatric Residential Facilities (SRP in Italian) of the Area Vasta 2 DSM is part of the new organisation suggested by the Unified Conference Agreement of 17 October 2013 [5] and subsequently accepted at regional level by D.G.R.M. 1331/14 [6], where the concept of residency is declined in a different way of managing psychological distress. The user is no longer placed in a purely medical dimension, but an individual project is built in agreement with other professionals. Therefore, the care pathway must be configured as a project characterised by: unity, continuity, multidisciplinarity, high organisational complexity, relevant professional specificity and ability to manage sociomedical integration [7]. It is based on the integration of specific activities such as: clinical and rehabilitation activities, care activities, family and social mediation, networking and coordination. The realisation of this pathway implies a strong investment in team work, understood as a multi-professional group able to develop an accurate reading of the patient’s biopsychosocial dimension, to integrate the observation data and to modulate a coherently articulated therapeutic planning. Thus, the ‘biopsychosocial’ model systematically employs biological, psychological and social factors, including their complex interactions, in the understanding of psychophysical health and the choice of therapeutic intervention [8]. Consequently, by focusing on the unitary and global approach to the person, the biopsychosocial model is the one most conducive to an interdisciplinary approach between the various professions, such as doctors, psychologists, social workers and educators. For patients with severe mental illnesses, controlling symptoms, regaining a positive sense of self, dealing with stigma and discrimination, and trying to lead a productive and satisfying life is increasingly referred to as an ongoing process of recovery [9]. Equally important is to enhance personal attitudes and skills such as communication skills, enthusiasm and willingness to learn, cultural background and to develop the practice of outcome assessment among practitioners. Patient care in residential psychiatric facilities is therefore linked to a practice oriented towards therapeutic continuity and is implemented through individual projects [10]. In past years, at national and regional level, activity data have shown a progressive lengthening of hospital stays, with a consequent reduction in patient turnover. In this sense, psychiatric residency has often taken on the function of a ‘housing solution’ rather than being functional to the ‘individual treatment project’, generating the danger that SRPs are used for forms of new institutionalisation. All SRPs should therefore provide for light residential care with assistance, which facilitates the transition from the structure to the territory [3].
There is a need for evidence-based assessment and rehabilitation activities in order to provide residents with the possibility of being involved in social interactions outside of the facilities, and possibly with opportunities for sheltered work and social integration. Indeed, work, social relationships and independence are aspects of quality of life recognised as important by both patients and their treating physicians [11]. Well-designed rehabilitation plans, adapted to the needs of each patient, are mandatory to foster the development of independence, increase the likelihood of discharge and ultimately improve quality of life [12]. The development of the clinical pathways model requires addressing fundamental clinical and organisational aspects [13]:
- organising a reception/assessment function for demand and requests from psychiatric services;
- the centrality of the sending Mental Health Centre (CSM in Italian);
- the centrality of family;
- the involvement of the GP to be implemented from the earliest stages of the patient’s contact with the structure;
- the definition and organisation of individualised therapeutic-rehabilitation paths;
- facilitating access procedures for all DSM operators;
- defining criteria for a maximum length of stay consistent with the level of rehabilitation intensity (18/24 months for rehabilitation facilities, 36 months for care facilities).
The result of the change process was to orientate the whole Structure to adopt principles, develop policies and implement actions, in order to help people with mental disabilities to remain in their life context, trying to achieve the best possible biopsychosocial functioning compatible with functional deficits, persistent psychopathology and relapses.
MATERIALS AND METHODS
Study design
Longitudinal descriptive observational study by administering the HoNOS questionnaire after the reorganisation of the psychiatric residential facilities of the Department of Mental Health of the Ancona Vasta 2 Area.
Population and settings
The pilot study was conducted at SRP1 “Casa Rossa” Area Vasta 2 of Ancona and involved 13 patients admitted to SRP1 Casa Rossa – AN ASUR Marche.
Inclusion criteria
Residential and semi-residential patients.
Ethical consideration
After explaining the purpose, the study was authorised by the Director of the DSM.
The study protocol was developed in accordance with the guidelines of the Declaration of Helsinki. Participation in the study was voluntary: patients were provided with a consent form for data processing and an information and consent form for the study. Only after obtaining consent and ensuring that the patient understood the purpose of the study was the paper-based HONOS questionnaire administered.
Data were collected after obtaining informed consent from each patient. The confidentiality of the data collected was guaranteed by ensuring the anonymity of all participants and avoiding the use of any personal identifiers.
The surveys, carried out in a homogeneous way by the Coordinator of the Operating Unit with over thirty years of working experience (twenty years of experience in the mental health area) took place in a protected environment, with a standardised method: a room specifically dedicated to surveys and data collection, no outside involvement and respect for the patient’s privacy.
Survey instrument
The validated Italian version of the Health of the Nation Outcome Scales [14] was used. The HoNOS scale is a multidimensional outcome and severity assessment tool developed specifically for routine use in mental health services, suitable for the assessment of clinical and psychosocial problems [15,16]. It consists of 12 items that the therapist assesses according to the severity of the problems. Each item represents a clinical problem area and is rated on a 5-point Likert scale. Relevant items include:
1.Hyperactive, aggressive, destructive or agitated behaviour;
2.Deliberately self-harming behaviour;
3.Problems related to drug or alcohol use;
4.Cognitive problems;
5.Problems of somatic illness or physical disability;
6.Problems of somatic illness or physical disability;
7.Problems related to depressed mood;
8.Other mental and behavioural problems;
9.Relational problems;
10.Problems in activities of daily living;
11.Problems in living conditions;
12.Problems in the availability of resources for work or leisure activities.
Each of the twelve items in the questionnaire is given a score from 0 to 4, where:
- a score of 0 indicates that no problem has been found;
- a score of 1 indicates that the problem is present, but because of its reduced severity no intervention is needed;
- a score of 2 indicates that a problem of mild severity is present, for which intervention (rehabilitation, care or therapy) is required;
- score 3 indicates the presence of a problem of moderate severity;
- a score of 4 indicates that a serious or very serious problem is present.
Unknown information was given a score of 9. The twelve scores can be added together to obtain an estimate of total severity or evaluated individually.
Study procedures and data collection
The reconversion project of SRP1 “Casa Rossa” took place in accordance with the principle of gradualness and with the participation of all operators through weekly meetings specifically planned by the nursing coordinator. Subsequently, patients were assessed three times over a one-year period by administration of the HoNOS questionnaire, at recruitment (February 2019), at 6 months (August 2019) and at 12 months (February 2020). Patients excluded from care were not included in the study. After data collection, the 12 items of the HoNOS scale were grouped into four subscales:
1.behavioural problems (items 1-3),
2.deficits and disabilities (items 4-5),
3.psychopathological symptoms (items 6-8)
4.relational/environmental problems (items 9-12).
Statistical analyses
Data was expressed as mean and standard deviation (SD) or median and interquartile range (IQR) in the case of numerical variables, while in the case of qualitative variables, it was expressed as absolute numbers or percentages.
The normality of the data was checked with the Shapiro-Wilk test, where with a p-value > 0.05 there is evidence of normally distributed data.
The difference between the averages of the total score and the scores of the four subscales, at the three follow-up points, was statistically evaluated with an analysis of variance model for repeated measures, in the case of normally distributed residuals; in the case of non-normally distributed data, the non-parametric Friedman test was applied.
For the scales with statistically significant differences in scores, multiple comparisons were made retrospectively between the groups (baseline, 6 months, 12 months) maintaining the 5% significance level with Bonferroni correction. Statistical analyses were carried out using the software R-CRAN v.3.6.2 for Windows.
RESULTS
Table 1 shows the demographic and clinical characteristics of the cohort of patients examined in the study.

Table 1. Descriptive statistics for demographic and clinical variables.
The mean with the standard deviation and the median with the interquartile range of the total score and the scores of the items of the 4 sub-scales, at baseline and in the two surveys at follow-up, are shown in table 2 and figure 1.
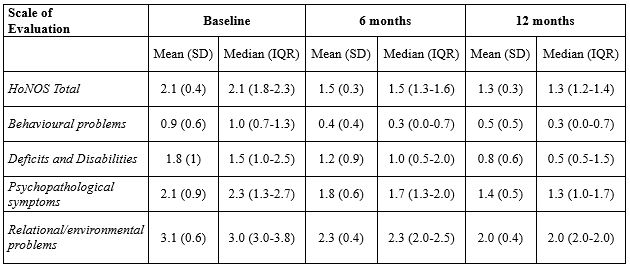
Table 2. Mean, standard deviation, median and interquartile range of Total Scale and 4 Subscales scores at baseline, 6 months and 12 months.
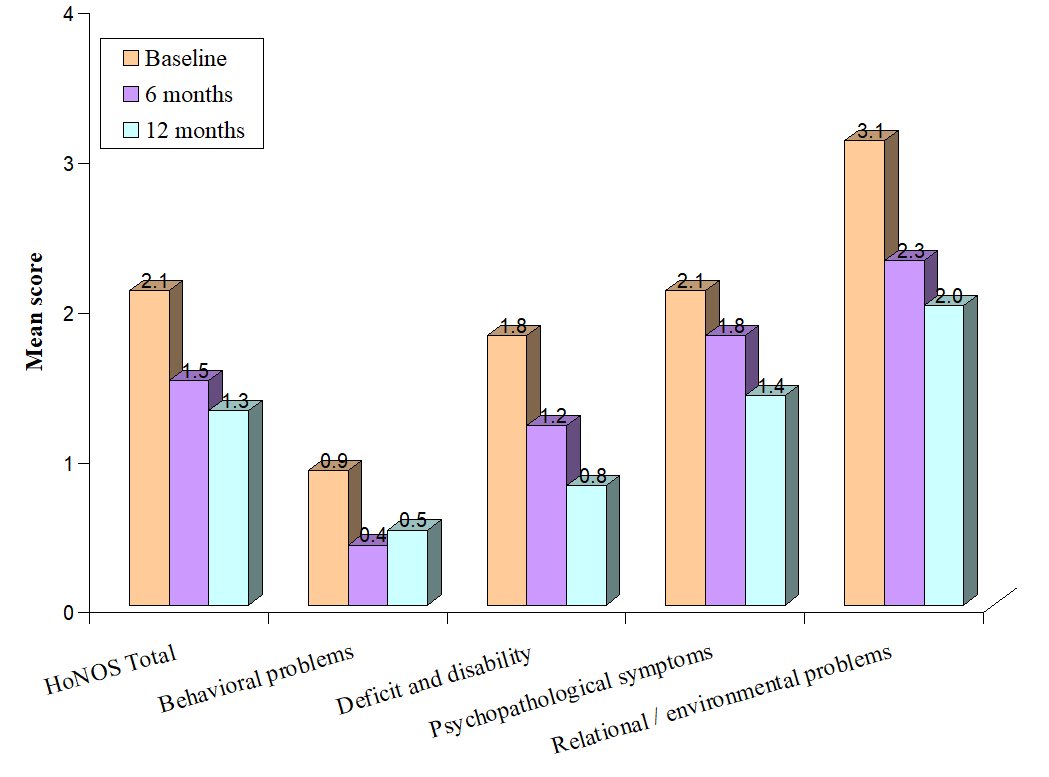
Figure 1. Average total score and average score of the 4 sub-scales.
The residuals of the analysis of variance model are distributed in accordance with the Normal random variable for the subscales of “deficit and disability” and “psychopathological symptoms” (p-value>0.05); the scale HoNOS Total, that of behavioural problems and of relational/environmental problems do not present normally distributed residuals (table 3).
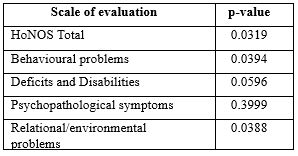
Table 3. P-value Shapiro-Wilk normality test
The statistical significance (p-value) of the differences between the averages of the total score and the scores of the four subscales at the three follow-up points are given in Table 4; the results show a statistically significant difference between the averages at the 95% confidence level.
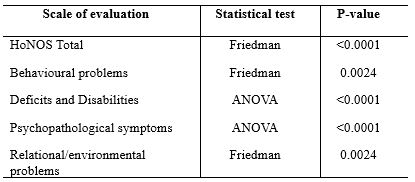
Table 4. Statistical significance of ANOVA and Friedman’s Test.
Table 5 shows the p-values of multiple retrospective comparisons between the groups (baseline, 6 months, 12 months) while maintaining the 5% significance level with the Bonferroni correction.

*P-value <0.05 Statistically significant difference
Table 5. P-value of pairwise retrospective comparisons of scores on the HoNOS Total scale and the 4 subscales at baseline, 6 months and 12 months.
DISCUSSION
The study performed predates the SARS-CoV2 pandemic and involved a cohort of 13 patients admitted to SRP1 Casa Rossa in Ancona. The mean age at recruitment and at disease onset was 46 and 19 years respectively, 69% of patients were male, 46% had a caregiver and 38.5% had undertaken other rehabilitation pathways. The results of the study show a reduction in the average HoNOS scale scores at 6 and 12 months compared to baseline in the four subscales considered. Considering the HoNOS scale in its entirety, there was a considerable decrease in the score from an overall mean of 2.1 at baseline to 1.3 at the end of the 12-month study period (Table 2). In all subscales considered, this decrease is statistically significant. The analysis of the data showed that the adjustment of the organisational set-up produces greater improvements especially in the initial phase (after 6 months) with a very significant decrease in average scores. After 6 months from the start of the study there is a stabilisation of the average HoNOS Total and subscale scores. Table 5 shows the p-values of the multiple comparisons between the groups; the scores of the groups compared were statistically significant with the exception of the scores taken at 6 and 12 months for the subscales of “behavioural problems”, “deficits and disabilities” and “relational/environmental problems” and the scores taken at 6 months and at baseline for “psychopathological symptoms”.
Similarly to a study by Buratti et al. [17], it is important to underline that, in the face of a clear prevalence of pharmacological treatments, the items that undergo a clear improvement are precisely those on which the drug has a direct effect (e.g. items concerning behavioural problems, deficits and disabilities and psychopathological symptoms), while the items concerning problems that would also require the use of other types of treatments (e.g. relational, environmental items) show a smaller decrease in average scores. Other data in the literature demonstrate the importance of using the HoNOS scale for assessing outcomes in patients with mental illness. A first longitudinal study in 3 times (14 months) was carried out in the Mental Health Services of the A.O. Ospedale Niguarda Ca’ Granda in order to contribute to the validation of the Italian version of the HoNOS scale and to make operators aware of the importance of a standardised assessment of outcomes. With regard to the results on improvement (clinically significant criterion of 7 points), improved patients correspond to 45.3% of the sample after 14 months from the start of the study [16]. Two other longitudinal studies [18,19] in three stages and with a two-year follow-up, were implemented in a Mental Health Centre in Rome where the following were analysed: the relationship between the severity detected by HoNOS and the ICD-9-CM diagnosis; the convergence between the two instruments; the relationship between HoNOS severity and the types of interventions used by the Mental Health Centre (psychiatric interview, psychological interview, psychotherapy, pharmacotherapy, home visits, rehabilitation, insertion in residential facilities) in order to assess the distribution of resources and finally the improvement of patients in one year. The results found convergence between HoNOS and ICD-9, appropriate use of interventions in relation to the specificity and severity of the diagnosis, and an improvement in patients with a significant decrease in mean scores.
Further studies have involved the Mental Health Departments of the A.O. Ospedale Niguarda Ca’ Granda as part of the introduction of a tool to formalize the Individual Treatment Plan (I.T.P.) in which the HoNOS scale is used for assessment and final evaluation of the chosen treatment [19,20]. In this research several aspects were evaluated: the type of intervention foreseen (counselling, intake, treatment), the treatments carried out (pharmacotherapy, psychotherapy, work placement, family involvement, etc.), the outcome of the intervention (re-evaluation at 6 months in case of intake and treatment), drop-out, costs, the role of the case manager and the impact on the work of the operators. The results showed a statistically and clinically significant improvement in severity scores even though there was a medical/nursing imbalance in the treatments provided. The number of psychological, social and rehabilitation treatments is still too low. In psychiatric services, the professional figure and services of psychiatrists predominate, to the detriment of the scarce presence of psychologists/psychotherapists, despite the fact that psychotherapy has been shown to bring about greater and more constant changes over time than the use of medication alone [19]. For this reason, one of the innovative elements in the study was to go beyond the medical-centric model in favour of interdisciplinary teamwork. In community psychiatry, all professionals must be united by a single aim: to provide patients with opportunities to use the skills learned in rehabilitation programmes in natural environments and to increase the quality of their lives. In order to ensure such integration, it is necessary to establish and implement an interdisciplinary and multidisciplinary team, whose operation is ensured by individual and collective tasks, well-defined performance standards, supervision and continuous on-the-job training [21]. It becomes a moral duty to assess whether in one’s own reality, with one’s own patients, colleagues, organisational difficulties and shortcomings, one can achieve the same results as in experimental effectiveness studies. It is possible, in everyday clinical practice, to routinely assess the outcome of hospitalisation using a scale such as the HoNOS, because not only is it simple and quick to fill in, but above all because it satisfactorily describes the changes induced by the period of hospitalisation.
CONCLUSIONS
In recent decades, mental health care has seen a shift from symptom management to the promotion of quality of life within psychiatric facilities: both patients and their relatives consider quality of life as one of the main goals of mental health care [22]. Rehabilitation facilities should be aimed at social integration; provide for a maximum length of stay of 24 months, with a 24-hour presence of health and psycho-socio-educational staff; provide for areas of involvement of patients and relatives [5]. The results of this pilot study show how an organisational reorganisation aimed at adopting principles, developing policies and implementing actions to help people with mental disabilities can improve the quality of hospitalisation and consequently the quality of life of patients with mental disorders. Achieving the best possible biopsychosocial functioning compatible with functional deficits, persistent psychopathology and relapses, involving the family and the general practitioner from the earliest stages of the patient’s contact with the facility are fundamental aspects of a care pathway for patients with mental disorders. At the end of a residential treatment programme, there should be a continuation of rehabilitation and care treatment by the mental health centres (CSM) in the region, where there is support and home visits through a single and integrated socio-health pathway with re-evaluation over time of patients under treatment for mental disorders. The evaluative approach should not be seen by practitioners as an inquisitorial control, but as an opportunity geared towards improving care, the severity of patients and the outcome of their treatment. The use of HoNOS in Psychiatric Facilities should not be considered as a goal, but as a starting point for a journey towards a more adequate clinical practice for the management of patients with mental disorders, which favours the effectiveness of treatments and the self-reflection of professionals [16].
LIMITATIONS OF THE STUDY
Despite the supervision of the nursing coordinator and the medical director of the facility, a potential information bias due to the detector effect (degree of subjective evaluation of information) is present and cannot be eliminated. The main limitation is the small sample size, which does not allow confounding factors such as diagnosis, age at onset, etc. to be taken into account in the statistical analysis. Although the results show a reduction in mean scores at 6 and 12 months compared to baseline, a longer observation period would be desirable to allow further evaluations of the effectiveness of the biopsychosocial intervention.
POSSIBLE FUNDING
This research has not received any form of funding.
CONFLICTS OF INTEREST
The authors declare that they received no funding for the following study and have no financial interest in the subject matter or the results obtained.
REFERENCES
- La rete dei servizi per la salute mentale disponibile al seguente url: https://www.salute.gov.it/portale/saluteMentale/dettaglioContenutiSaluteMentale.jsp?lingua=italiano&id=168&area=salute%20mentale&menu=vuoto#:~:text=Il%20Dipartimento%20di%20salute%20mentale,Azienda%20sanitaria%20locale%20(ASL). Data ultima consultazione 04/01/2022
- Amaddeo, F., Bacigalupi, M., de Girolamo, G., Di Munzio, W., Lora, A., & Semisa, D. (1998). Attivitá e interventi del Dipartimento di Salute Mentale. Epidemiologia e Psichiatria Sociale. Monograph Supplement, 7(S2), 13–30.
- Cerati, G., Ciancaglini P., Ferrannini L., Merckling D. (2015) http://www.nuovarassegnastudipsichiatrici.it/attachments/article/140/NRSP-Vol.12-13-I-programmi-di-residenzialita-leggera-tra-recente-normativa-nazionale-ed-esperienze.pdf. Data ultima consultazione 27/02/2022
- Lora A., Starace F., Di Munzio W., Fioritti A. (2014). Italian community psychiatry in practice: description and comparison of three regional systems. J Nerv Ment DIs. 202(6):446-50
- Allegato A – Accordo tra il Governo, le Regioni e le Province autonome di Trento e di Bolzano, le Province, i Comuni e le Comunità montane sul documento concernente “Le strutture residenziali psichiatriche”. Rep. Atti n. 116/CU del 17 ottobre 2013
- G.R.M. 1331/14- Regione Marche. 25 novembre 2014
- Percudani M., Cerati G. et al. (2012). I modelli regionali nelle politiche di salute mentale. Sistema Salute, 56, 2, 2012: pp. 192-204
- Hatala A.R. (2012). The Status of the “Biopsychosocial” Model in Health Psychology: Towards an Integrated Approach and a Critique of Cultural Conceptions. Open Jurnal of Medical Psychology. 1, 51-62
- Markowitz F. E. (2001). Modeling processes in recovery from mental illness: relationships between symptoms, life satisfaction, and self-concept. J Health Soc Behav. 42(1):64-70
- Borrel-Carriò F., Suchman A.L., Epstein R.M. (2004). The biopsychosocial model 25 years later: principles, pratice, and scientific inquiry. Ann Fam Med. 2(6): 576-82
- Angermeyer MC, Holzinger A, Kilian R, Matschinger H (2001) Quality of life—as defined by schizophrenic patients and psychiatrists. Int J Soc Psychiatry 47:34 –42
- Picardi, A., Rucci, P., de Girolamo, G., Santone, G., Borsetti, G., & Morosini, P. (2006). The quality of life of the mentally ill living in residential facilities. European Archives of Psychiatry and Clinical Neuroscience, 256(6), 372–381.
- Deliberazione n. 7/17513 del 17 Maggio 2004: Piano regionale Triennale per la Salute Mentale in attuazione del Piano Socio Sanitario Regionale 2002-2004
- Preti A., Pisano A., Cascio MT., et al. (2012). Validation of the Health of the Nation Outcome Scales as a routine measure of outcome in early intervention programmes. Early Interv Psychiatry. 6(4):423-31
- Wing J., Curtis R.H., Beevor A.S., Park B.G., Hadden S. & Burns A. (1998). Healt of the Nation Outcome Scales (HoNOS): research and development. British Journal of Psychiatry 172, 11-18
- Lora A., Bai G., Bianchi S., Bolongaro G., Civenti G., Erlicher A., Maresca G. Monzani E., Panetta B., Von Morgen D., Rossi F., Torri V. & Morosini P. (2001). La versione italiana della HoNOS (“Healt of the Nation Outcome Scales”), una scala per la valutazione della gravità e dell’esito nei servizi di salute mentale. Epidemiologia e Psichiatria Sociale 10, 198-212
- Buratti, E., Vigorelli, M., Gallucci, M., Moranti, C., Schiavolin, S., & Peri, Y. (2006). Valutazione con HoNOS (Health of the Nation Outcome Scales) nei servizi territoriali di Niguarda a Milano: uno studio longitudinale. Relazione presentata al VI Congresso Nazionale S.P.R.-Italia “Tra Scilla e Cariddi”, Reggio Calabria
- Vigorelli, M., Correale, A., Criconia, M., Bolzoni, C., Stirone, V., & Schlosser, S. (2008). Accoglimento nei primi colloqui, profili diagnostici e di cura: una ricerca sul campo in 2° area. Relazione presentata alla Giornata di studio “Il servizio conosce se stesso? Ricerca sugli esiti e appropriatezza degli interventi”, DSM, Roma B
- Vigorelli M. (2010). Ricerca multistrumentale in psicoterapia, valutazione in psicosomatica e nei servizi psichiatrici: gruppo di ricerca coordinato da Marta Vigorelli. Ricerca in Psicoterapia / Research in Psychotherapy; 2(13): 287-321
- Manfrè, S., Simoncini, L., Scordari, S., Segato, C., Vigorelli, M., & Re, E. (2009). Pratica clinica strutturata e valutazione di esito: l’esperienza del DSM di Milano Niguarda. Psichiatria di Comunità, 8(4), 31–40
- Moxham L., Patterson C., Taylor E., Perlman D., Sumskis S., Brighton R. (2017) A multidisciplinary learning experience contributing to mental health rehabilitation. Disabil Rehabil. 39(1):98:103.
- Salvi G., Leese M., Slade M. (2005). Routine use of mental health outcome assessments: choosing the measure. British Journal of Psychiatry, 182(2), 146-152
![]() This work is licensed under a Creative Commons
This work is licensed under a Creative Commons
Attribution-NonCommercial-NoDerivatives 4.0 International License.