Saida, Rahmawati*, Wa Ode Syahrani Hajri
Department of Nursing, Medical of Faculty, Halu Oleo of University, Kendari, Indonesia
* Corresponding author: Rahmawati, Kampus Hijau Bumi Tridharma, Anduonohu, Kec. Kambu, Kota Kendari, Sulawesi Tenggara 93232, Indonesia, Orcid : https://orcid.org/0000-0002-6826-5393. Email: saida@uho.ac.id
Cita questo articolo
Abstract
Introduction: Non-communicable diseases (NCDs) are diseases that are not caused by bacterial infection and are the main cause of death in the world. The increase in NCDs cases also occurred in Southeast Sulawesi Province (Indonesia), including Kendari City. The purpose of this study was to analyze the determinants of proxies related to the performance of Integrated Non-Communicable Diseases Development Post (INCDDP) cadres in Kendari City, Indonesia.
Materials and Methods: A cross-sectional study carried out in Kendari City, Southeast Sulawesi Province (Indonesia), with a population of all INCDDP cadres in the working area of PHC Abeli, Lepo-Lepo, and Perumnas. The sample consisted of 56 responders. Data were analyzed univariate and bivariate statistics, using the chi-square test. Multivariate using logistic regression.
Results: The results of the research on the performance of INCDDP cadres were awards (p = 0.079), cadre training history (p = 0.031), infrastructure (p = 1.0) and knowledge (p = 0.007). The factor most related to the performance of INCDDP cadres was cadre knowledge (p = 0.019) with the coefficient of determination (R2) = 27.4%.
Conclusion: Cadre performance is related to awards, cadre training history, infrastructure and cadre knowledge. The most related factor to INCDDP cadre performance is cadre knowledge.
Keywords: Health-Cadres, Non-Commnicable Diseases, Performance, Health Services
Introduction
Non-communicable diseases (NCDs) have become an enormous public health problem, especially in Indonesia [1]. It is marked by a shift in disease patterns which is often referred to as an epidemiological transition characterized by increased mortality and morbidity due to NCDs such as stroke, heart disease and diabetes mellitus [2].
NCDs account for 41 million deaths each year, equivalent to 71% of all deaths globally [3]. The 2018 Basic Health Research (BHR) results show an increase in the prevalence of NCDs compared to the 2013 BHR results [4]. NCDs cases in Southeast Sulawesi in 2018 were still relatively high [4,5]. In 2019, the number of hypertension sufferers in Kendari city was 13,807 cases, and DM patients were 2876 cases [6].
The high number of NCDs cases in Kendari City requires severe treatment by increasing the Public Health Center (PHC) role through the Integrated Non-Communicable Diseases Development Post (INCDDP), significantly expanding the part of cadres in the context of preventing and controlling NCDs. INCDDP is a form of community participation in activities for early detection, monitoring, and early follow-up of NCDs risk factors independently [7], routinely, integrated, and continuously [8]. The high number of PTM cases in Kendari City (Indonesia) requires serious handling by increasing the role of the Puskesmas through the Integrated Non-Communicable Disease Development Post (INCDDP), significantly expanding the role of cadres in the context of preventing and controlling PTM. INCDDP is a form of community participation in activities for early detection, monitoring, and early follow-up of PTM risk factors independently [7], routinely, integrated, and continuously [8].
In improving the skills of cadres, it is necessary to support the development of health workers, especially community nurses [9]. One of the intervention strategies that can be applied as community nurses as educators or educators is to provide health education to high-risk community groups and health cadres and change public health behavior. Following this research, nurses are expected to be able to empower cadres by increasing the knowledge and skills of cadres as mover in the community. One of the ways to increase knowledge and skills is through community-based education programs. This is intended to improve the quality of cadres in providing counseling and management to patients and families of NCDs patients, as well as the community [10–12].
The role of INCDDP cadres is as an implementer of NCDs risk factor control for the surrounding community. The functions of cadres are as coordinator of INCDDP implementation, community mobilizer to participate in INCDDP, monitoring of measurement of NCDs risk factors, counsellor for INCDDP participants, recorder of results of INCDDP activities [13].
There are still many problems in service at INCDDP related to the capacity of cadres. In theory, three factors affect a person’s performance: individual elements consisting of abilities and expertise, background, and demographics. The second is psychological factors consisting of perceptions, attitudes, learning and motivation. The last is organizational factors, namely resources, leadership, rewards, structure and job design. These three factors can be classified into intrinsic factors, while extrinsic factors include political, economic and social factors [14].
The results of previous studies stated a relationship between cadre performance with attitudes, motivation, rewards, job design, and there was no relationship between HR and the role of stakeholders [15]. It is in line with other research states that the support of health cadres and family support by using INCDDP in the Ballaparang working area of Makassar City [16]. Kendari City has 15 PHCs, 13 of which have INCDDP. INCDDP cadres have a very big role in the prevention and early detection of risk factors for NCDs in the community [6].
The purpose of this study was to analyze the factors related to the performance of INCDDP cadres in Kendari City (Indonesia).
Materials and Methods
Trial design
This type of research is an observational analytic with a cross-sectional design to analyze the determinants of the proxy factors related to the performance of INCDDP cadres in Kendari City (Indonesia).
Participants
This research was carried out in October 2021 at 3 (three) Puskesmas in Kendari City (Indonesia) consisting of Abeli, Lepo-Lepo, and Perumnas Health Centers involving 56 INCDDP cadres with criteria including cadres who were present at the time of the study, cadres with active status participating in Integrated Non-Communicable Diseases Development Post (INCDDP) activities, while the inactive Cadres are expelled.
Intervention
The dependent variable in this study is the performance of cadres with the objective criteria of “good” and “bad”. While the independent variables are cadre training, infrastructure, knowledge, awards with “good” and “less” objective criteria. Collecting data on cadre performance variables using a questionnaire, and cadre training variables, infrastructure, knowledge, awards, also using questionnaires. on each variable, consisting of 10 questions with an alternative scoring as follows: if the respondent answers yes then it is given a score of 1 and if the respondent answers no it is given a score of zero. All questionnaires in this study used previous research questionnaires that had been tested for validity and reliability. The questionnaire received an award from the Kiting PR research. et al, [15], questionnaire of knowledge, training and infrastructure adoption from Handayani RO. et al, research [17].
Outcomes
Knowing the performance of cadres, training history, rewards, infrastructure, and knowledge.
Sample size
The number of participants in this study was 56 people. The age of the sample in this study was between 26-67 years, all of whom were female because all Integrated Non-Communicable Diseases Development Post (INCDDP) cadres were female. The sampling method in this study was total sampling because the number of Integrated Non-Communicable Diseases Development Post (INCDDP) candidates was very small.
Statistical analysis
Data are presented as numbers and percentages for categorical variables. Continuous data were expressed as mean ± standard deviation (SD) or median with Interquartile Range (IQR). The bivariate analysis uses the chi-square test, and multivariate uses logistic regression. Logistic regression test is used because the data scale used is categorical or binomial. in the multivariate test, there is R2 or R square also referred to as the coefficient of determination which explains how far the dependent data can be explained by independent data. All tests with p-value (p)<0.05 were considered significant. Statistical analysis was performed using the SPSS version 16.0 application.
Ethical Consideration
No economic incentives were offered or provided for participation in this study. The study was performed in accordance with the ethical considerations of the Helsinki Declaration. This study obtained ethical feasibility under the Health Research Ethics Committee of the College of Medicine, Halu Oleo University, number: 183/UN29.17.1.3/ETIK/2021.
Result
The distribution of the characteristics of the results of this study is showed in Table 1:
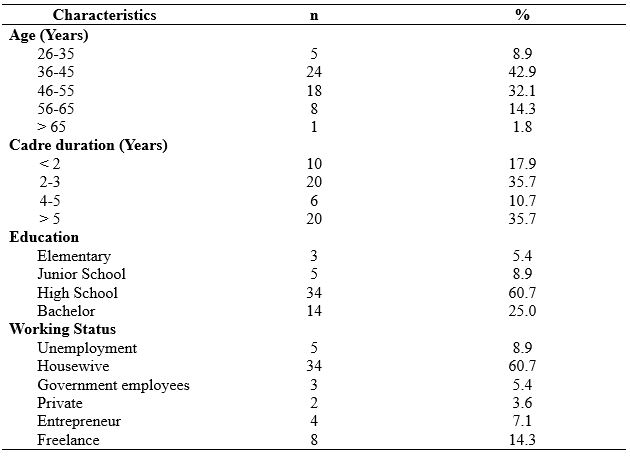
Table 1. Frequency Distribution Based on Characteristics of Respondents
Table 1 shows the frequency distribution of 56 respondents based on age characteristics, primarily aged 36-45 years as many as 24 (42.9%), the highest length of being a cadre is 2-3 years, and > 5 years each is 20 (35.7%), the highest level of education is high school graduates as many as 34 (60.7%). The most elevated employment status is as a housewife as much as 34 (60.7%).
The distribution of research variables is presented in table 2. Table 2 shows the frequency, distribution by knowledge, perception of vulnerability, and compliance, there were 29 cadres (52.8%) who performed well, 26 cadres (46.4%) had attended training, 45 cadres (80.4%) stated that they had received awards, there were 48 cadres (85.7%) who indicated that infrastructure facilities were not available. Meet the minimum requirements, and 36 cadres (64.3%) have good knowledge.
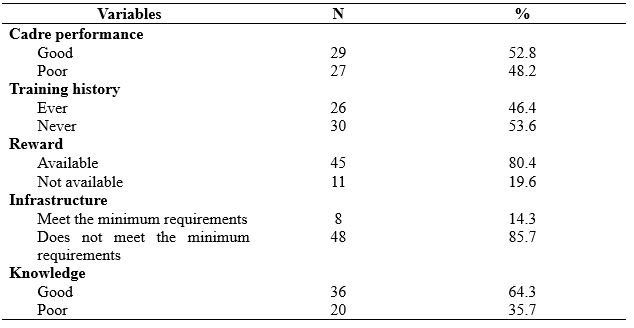
Table 2. Frequency Distribution by Knowledge, perception of vulnerability, and compliance
The distribution of the relationship between research variables can be presented in the following table 3:
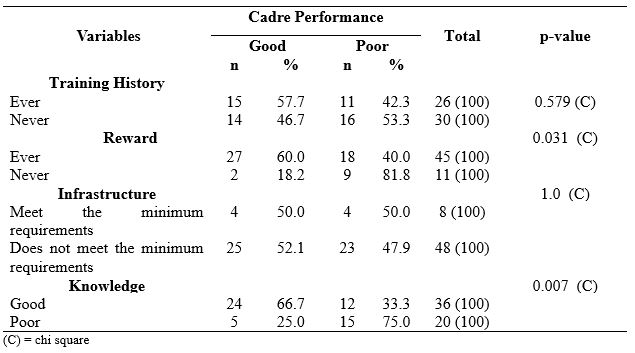
Table 3. Relationship between variables
Table 3 shows that of the 26 respondents who have a good training history, there are 15 cadres (57.7%) who perform well and 11 cadres (42.3%) who perform poorly, then from 30 respondents who have a history of lack of training, there are 16 cadres (53.3%). Underperforming and 14 cadres (46.7%) performed well. The chi-square test showed a p = 0.579, indicating no significant relationship between training history and the performance of INCDDP cadres.
Forty-five respondents assessed the availability of the award, as many as 27 cadres (60.0%) with good performance and 18 cadres (40.0%) with less performance. Then from 11 respondents who assessed that the award did not exist, nine cadres (81.8%) with poor performance and two cadres (18.2%) performed well. The chi-square test shows the p = 0.031, indicating a significant relationship between rewards and the implementation of INCDDP cadres.
Eight respondents assessed the minimum requirements of infrastructure, four cadres (50.0%) with good performance and four cadres (50.0%) with poor performance. Of the 48 respondents who assessed that the infrastructure did not meet the minimum requirements, 23 cadres (47.9%) underperforming and 25 cadres (52.1%) performed well. The chi-square test shows that the p = 1.0 indicates no significant relationship between infrastructure and the performance of INCDDP cadres.
Of the 36 respondents who have good knowledge, there are 24 cadres (66.7%) with good performance and 24 cadres (33.3%) with poor performance; then from 20 respondents who have less knowledge, there are 15 cadres (75.0%) with poor performance and five cadres (25.0 %) perform well. The chi-square test showed a p = 0.007, indicating a significant relationship between knowledge and performance of INCDDP cadres.
Multivariate data analysis using logistic regression test is presented in table 4.
The results of the multivariate analysis showed that the Wald value of the knowledge variable was the largest with a significant value (p = 0.090).
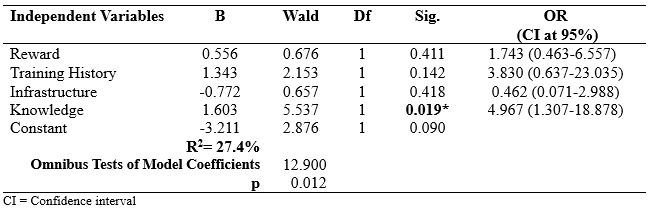
Table 4. Multivariate Analysis of INCDDP Cadre Performance
The value of R2 = 27.4% indicates that this model can explain the effect variable (INCDDP cadre performance) of 27.4%, while 72.6% is influenced by other variables not examined.
The value of chi square = 12,900 with sig. 0.012 in Degree of Feedom 4 the value of chi square table = 9.49. it can be seen that the p value < 0.05, so it can be ascertained that the addition of the independent variable has a real effect on the model, in other words other models are declared FIT
Discussion
1.Reward
The purpose of this study was to analyze the factors related to the performance of INCDDP cadres in Kendari City (Indonesia). The existence of cadres should receive fair and sincere recognition and appreciation [18]. Recognition of the existence of cadres from cadre coaches in the sub-district needs to be realized by prioritizing free health services and the presence of cadre uniforms [19]. The hierarchy of human needs starts from primary needs (physiological needs and safety needs) to be dominant until these needs are felt to be sufficiently fulfilled [20].
Appreciation for the work done is a desire from selfish needs, manifested in praise, gifts (in the form of money or not), announced to his co-workers [21]. Therefore, giving awards for cadre loyalty will be very helpful to maintain the activeness of Posbindu cadres; giving tasks that are not boring with praise, completing attributes while on duty will increase cadre performance [22].
In this study, it was found that of the overall respondents, more than half had received awards from the government through the Puskesmas or the Kendari city health office. Indeed, this greatly influenced the motivation of Posbindu cadres in working. It is statistically proven that cadres who have a history of receiving awards tend to perform well and vice versa.
It is stated that usually, a person will feel mistreated if the treatment is seen as a dangerous thing. In working life, this perception is associated with various things, namely incentives and the number of hours worked [23]. The provision of incentives is a basic payment to motivate employees to be more advanced in work with more excellent skills and responsibilities [24]. Incentives are one type of award that is associated with work performance [25].
The award should be given to human resources, in this case, Posbindu PTM cadres who perform well to increase the spirit of work. Other cadres will see and will encourage other cadres to work better so that performance improves. Therefore, the performance of PTM Posbindu cadres will significantly increase if awards are given to their human resources.
In line with the findings of Renate Pah Kiting [15] stated that there is a relationship between rewards and performance (p=0.013 OR=10.400). Furthermore, Renate et al. said that cadres who received awards ten times would have the opportunity to have better performance compared to cadres who did not accept awards.
2.Training
The commitment of cadres to the responsibilities and functions of the INCDDP program in the Anambas Islands is quite good. It is evidenced by the continued implementation of the INCDDP program even though it is still constrained by several problems such as limited tools and materials and has never received special training. Therefore, support and commitment from cadres are very vital in the implementation of the INCDDP program. In the results of his research, it is stated by [26] that INCDDP cadres who always consistently run INCDDP with or without training will motivate other cadres to take an active role and try to help active cadres with what has been exemplified.
In this study, only a few respondents had ever been sent to receive training, although some of the cadres who had attended the training section stated that they were not under the assignment field at INCDDP. This condition will undoubtedly affect cadres’ performance where when doing work. They do not look professional due to their lack of knowledge.
There is a difference in the proportion of cadres who received training and whose performance was considered “good” compared to cadres whose performance was “good” but did not receive training. The result shows that the more often cadres attend training, the better their performance [27]. Cadre training is carried out to increase the knowledge and skills of cadres. It will be achieved if the training section is carried out correctly. Puspasari A stated that the quality of cadre training is a factor causing cadres’ low knowledge and skills level in carrying out their roles and duties. Therefore, training activities should be carried out regularly with a distance that is not too long.
The training should always start with the importance of an INCDDP cadre’s goals so that interest and strong desire to make decisions and take action in implementing PTM Posbindu activities arise. It is expected that cadres will work with higher motivation and feel satisfied with their work so that it has a direct impact on increasing performance [28].
3.Infrastructure
Not all of the INCDDP in the working area of the PHC have complete kits; it requires them to use alternate tools at implementation. The Posbindu kit contains tools for checking blood sugar, cholesterol, uric acid, measuring height and then a body fat analyzer. Digital devices have never been calibrated, and this, of course, has fatal consequences in calculating the inspection results. Based on the inspection, the digital sphygmomanometer is broken, which give abnormal results in measurement.
Regarding the damaged digital INCDDP equipment, it is also following the research of Astuti et al. [29] that the number of NCDs INCDDP equipment is damaged/error. These tools include; body fat scale analyzer, measuring blood sugar and measuring total cholesterol. Likewise, research by Pranandari et al. [30] concluded that the infrastructure for the NCDs Posbindu in Banguntapan District, Bantul Regency for examining NCDs risk factors in the form of examination strips was not sufficient. Nova Silviyani’s research [31] states that the statistical results obtained a p of 0.05 = (0.05), so it can be noted that there is no significant relationship between infrastructure and Posbindu performance.
In motivating the work, it should provide suitable facilities and infrastructure to carry out tasks. However, as complained by the cadre coach at the Kendari City District level, inadequate facilities and infrastructure such as tables, chairs, scales, stationery and especially the Posbindu place will hinder the performance of Posbindu cadres [32].
Posbindu activities will not be able to run correctly if adequate facilities do not support them. The provision of work facilities is that the work facilities provided must be sufficient and follow the duties and functions. Moreover, it must be implemented and available at the right time and place. Therefore, Posbindu facilities are everything that can support the implementation of Posbindu activities such as a fixed place or location, routine funds for giving additional food (PMT), the necessary tools, for example, kitchenware, KMS, tables, chairs, register books and others [33].
4.Knowledge
Knowledge of health cadres is an essential factor in supporting the ability of cadres to provide services. This study shows that several cadres have a low level of knowledge. There needs to be an effort to increase the knowledge of cadres, where one of the steps that can be taken is to provide health education and training to health cadres [34],[35].
Cadre knowledge is the extent to which cadres understand their duties and roles in INCDDP activities, including preparation before implementation, during implementation and after the implementation of INCDDP for the elderly. Knowledge of health cadres about INCDDP services is obtained from the information they obtain both from official sources, meaning from the health office that fosters them, from informal sources, and activities aimed at increasing cadre knowledge such as training, seminars and so on [36].
It is evident from the results of statistical tests that there is a relationship between knowledge and the performance of Posbindu cadres in the working area of the Puskesmas in Kendari City. Hence, there is a tendency for cadres who have an excellent ability to do their jobs well.
It is in line with research [37] which examines the relationship between knowledge and length of work with the skills of cadres in assessing the growth curve of toddlers at the Posyandu, Tegalsari Village, Candisari District, Semarang City. This study shows that the level of knowledge of cadres about the growth curve of toddlers is primarily adequate, where one of the factors related to this knowledge is the level of education of cadres, most of whom are in high school.
We assume the level of education of cadres varies from elementary school to high school level. This level of schooling dramatically affects the attitude and ability of cadres in capturing information conveyed by officers both when training and visits to INCDDP.
5.Multivariate test results
In Table 4, there is a significant positive correlation between the Performance and Knowledge of INCDDP Cadres (OR=4.987; p=0.019). it can be explained that after going through a simultaneous test between the performance of cadres and all independent variables (knowledge, training, infrastructure, and awards) it was found that only the knowledge of cadres was significant while the other 3 variables were not significant. Knowledge of cadres dominates the motivation of cadres to improve their performance, so even though infrastructure is available, if cadres do not have knowledge of what to do, then cadres’ performance tends to be poor.
Implications of research results for nursing and clinical practice is to be valuable information for health service providers, especially community health centers to maximize the performance of nurses in assisting cadres when providing services to the community.
Conclusion
Cadre performance is related to awards, cadre training history, infrastructure and cadre knowledge. The most related factor to INCDDP cadre performance is cadre knowledge.
There is a need to increase advocacy to the legislative body regarding the importance of getting more budget for PHC and the need to improve health funds budgeted through the Regional Revenue and Expenditure Budget (APBD) to support the implementation of services and the need to formulate regulatory policies to tackle financing for cadres immediately. It is necessary to carry out periodic training for cadres, and it is hoped that INCDDP cadres will continue to explore knowledge and experience to improve performance in the implementation of INCDDP activities and always be positive in every action carried out at INCDDP and need to improve and improve facilities and infrastructure to meet basic service needs.
Limitations of Study
The limitations of this study include the very limited number of subjects, and this research only involves one region or 1 region so the results may be different when compared to other regions or regions in Indonesia.
Acknowledgement
We would like to thank the Chairperson of the research institute and community service who have supported this research.
Funding statement
This research did not receive any specific grant from funding agencies in the public, commercial, or not for profit sectors.
Competing interests statement
There are no competing interests for this study.
References
- Kemenkes RI. Rencana Aksi Nasional Penyakit Tidak Menular 2015-2019. Kementerian Kesehatan RI. Jakarta; 2017.
- World Health Organization (WHO). Global status report on noncommunicable diseases. World Health Organization. Italia; 2010. 176 p.
- WHO. Noncommunicable diseases. World Health Organization; 2018.
- Kementerian Kesehatan Republik Indonesia. Riset Kesehatan Dasar. Jakarta: Balitbangkes RI; 2018. Available from: https://kesmas.kemkes.go.id/assets/upload/dir_519d41d8cd98f00/files/Hasil-riskesdas-2018_1274.pdf “Accessed December 21,2021”
- Dinas Kesehatan Provinsi Sulawesi Tenggara. Profil Kesehatan Propinsi Sulawesi Tenggara. Kendari: Bidang P2PL Dinas Kesehatan Prov. Sultra; 2020. Available from: https://farmalkes.kemkes.go.id/ufaqs/dinas-kesehatan-provinsi-sulawesi-tenggara/“Accessed December 28,2021”
- Dinas Kesehatan Kota Kendari. Profil Dinas Kesehatan Kota Kendari. Kendari: Bidang P2PL Dinas Kesehatan Kota Kendari; 2019. Available from: https://siasiksehat.kendarikota.go.id/profil-kesehatan-kota-kendari/“Accessed December 21,2021”
- Dinkes Kabupaten Demak. Kegiatan Posbindu PTM. Demak; 2018. Available from: https://dinkes.demakkab.go.id/download/“Accessed December 21,2021”
- Kemenkes RI. Petunjuk Teknis Pos Pembinaan Terpadu Penyakit Tidak Menular (POSBINDU PTM). In Jakarta: Direktorat Jenderal Pengendalian Penyakit dan Penyehatan Lingkungan Direktorat Pengendalian Penyakit Tidak Menular; 2012.
- Iriarte‐Roteta A, Lopez‐Dicastillo O, Mujika A, Ruiz‐Zaldibar C, Hernantes N, Bermejo‐Martins E, et al. Nurses’ role in health promotion and prevention: A critical interpretive synthesis. Journal of Clinical Nursing. 2020;29(21–22):3937–49.
- Halcomb E, Williams A, Ashley C, McInnes S, Stephen C, Calma K, et al. The support needs of Australian primary health care nurses during the COVID‐19 pandemic. Journal of nursing management. 2020;28(7):1553–60.
- Halcomb E, McInnes S, Williams A, Ashley C, James S, Fernandez R, et al. The experiences of primary healthcare nurses during the COVID‐19 pandemic in Australia. Journal of Nursing Scholarship. 2020;52(5):553–63.
- Blay N, Sousa MS, Rowles M, Murray‐Parahi P. The community nurse in Australia. Who are they? A rapid systematic review. Journal of nursing management. 2021;
- Kementerian Kesehatan RI. Modul Pelatihan Posbindu PTM. Jakarta: Direktorat PPTM, Direktorat Jenderal PP dan PL; 2013.
- Andriani K, Bisri RS MS. Analisis Faktor Faktor Yang Mempengaruhi Kinerja Tenaga Kesehatan Pada Penerapan Program Keluarga Sadar Gizi di Kabupaten Sukoharjo. Manajemen Bisnis Syariah. 2013;1(7).
- Kiting RP, Ilmi B, Arifin S. Faktor Yang Berhubungan Dengan Kinerja Kader Posbindu Penyakit Tidak Menular. Jurnal Berkala Kesehatan. 2017;1(2):106.
- Nasruddin NR. Faktor-faktor yang mempengaruhi pemanfaatan pos pembinaan terpadu penyakit tidak menular (POSBINDU PTM) Di Wilayah Kerja Puskesmas Ballaparang Kota Makassar Tahun 2017. Universitas Islam Negeri Alauddin Makassar; 2017. Available from: http://repositori.uin-alauddin.ac.id/6515/1/NURIZKA RAYHANA_opt.pdf.“Accessed December 28,2021”
- Handayani RO, Suryoputro A, Sriatmi A. Faktor-Faktor Yang Berhubungan Dengan Praktik Kader Dalam Pelaksanaan Posyandu Lansia di Kelurahan Sendangmulyo Kecamatan Tembalang Kota Semarang. Jurnal Kesehatan Masyarakat (Undip). 2018;6(1):81–92.
- Husniyawati YR, Wulandari RD. Analisis motivasi terhadap kinerja kader Posyandu berdasarkan teori Victor Vroom. Jurnal Administrasi Kesehatan Indonesia. 2016;4(2):126–35.
- Bunawar KMS. Hubungan Penghargaan, Tanggung Jawab, Pengawasan, Hubungan Interpersonal terhadap Motivasi Kerja Kader Posyandu di Wilayah Kerja Puskesmas Sungai Bengkal Kabupaten Tebo Tahun 2017. Scientia Journal. 2019;8(1):249–55.
- Tay L, Diener E. Needs and subjective well-being around the world. Journal of personality and social psychology. 2011;101(2):354.
- Profita AC. Beberapa faktor yang berhubungan dengan keaktifan kader posyandu di Desa Pengadegan Kabupaten Banyumas. Jurnal Administrasi Kesehatan Indonesia. 2018;6(2):68–74.
- Isaura V. Faktor-faktor yang berhubungan dengan kinerja kader posyandu di wilayah kerja Puskesmas Tarusan Kecamatan Koto XI Tarusan Kabupaten Pesisir Selatan tahun 2011. Padang: Fakultas Kedokteran Universitas Andalas (skripsi tidak diterbitkan). 2011; Available from: http://repository.unand.ac.id/17532/1/FAKTOR.pdf. “Accessed December 20,2021”
- Siagian SP. Manajemen Sumber Daya Manusia. Jakarta: Bumi Aksara; 2006.
- Bangung W. Manajemen sumber daya manusia. Bandung: erlangga. 2012;
- Larasati S. Manajemen Sumber Daya Manusia. Deepublish; 2018.
- Primiyani Y, Masrul M, Hardisman H. Analisis Pelaksanaan Program Pos Pembinaan Terpadu Penyakit Tidak Menular di Kota Solok. Jurnal Kesehatan Andalas. 2019;8(2):399.
- Puspasari A. Faktor-faktor yang mempengaruhi kinerja kader posyandu dikota Sabang Provinsi Nanggroe Aceh Darussalam. Skripsi. Institut Pertanian Bogor; 2002. Available from: https://repository.ipb.ac.id/handle/123456789/14771. “Accessed December 20,2021”
- Handarsari E, Syamsianah A, Astuti R. Peningkatan Pengetahuan dan Ketrampilan Kader Posyandu di Kelurahan Purwosari Kecamatan Mijen Kota Semarang. In: PROSIDING SEMINAR NASIONAL & INTERNASIONAL. 2015. Available from: https://jurnal.unimus.ac.id/index.php/psn12012010/article/view/1646. “Accessed December 25,2021”
- Astuti ED, Prasetyowati I, Ariyanto Y. Gambaran Proses Kegiatan Pos Pembinaan Terpadu Penyakit Tidak Menular di Puskesmas Sempu Kabupaten Banyuwangi (The Description of Activity Process for the Integrated Development Post of Non-Communicable Disease (IDP of NCD) at Sempu Public Health Centre i. Pustaka Kesehatan. 2016;4(1):160–7.
- Pranandari LL, Arso SP, Fatmasari EY. Analisis implementasi program pos pembinaan terpadu penyakit tidak menular (posbindu PTM) di Kecamatan Banguntapan Kabupaten Bantul. Jurnal Kesehatan Masyarakat (Undip). 2017;5(4):76–84.
- Silviyani N, Setyawati VAV. Faktor-Faktor yang Berhubungan dengan Kinerja Posyandu Lansia di Wilayah Puskesmas Miroto Semarang. Skripsi Semarang: Universitas Dian Nuswantoro. 2015; Available from: https://core.ac.uk/download/pdf/35382833.pdf. “Accessed December 2,2021”
- Syahmasa. Analisis Hubungan Faktor Demografi dan Motivasi Dengan Kinerja Kader Dalam Berperan Serta Meningkatkan Pelyanan Keperawatan Di Posyandu Wilayah Puskesmas Kecamatan Cipayung Jakarta Timur Tahun 2002. 2002. Available from: https://lib.ui.ac.id/detail?id=72143&lokasi=lokal. “Accessed December 2,2021”
- Siagian S. Teori dan Praktek Kepimpinan. Jakarta: PT. Rineka Cipta; 2003.
- Nurhidayah I, Hidayati NO, Nuraeni A. Revitalisasi Posyandu melalui Pemberdayaan Kader Kesehatan. Media Karya Kesehatan. 2019;2(2).
- Lindner JR, Dooley KE. Agricultural education competencies and progress toward a doctoral degree. Journal of Agricultural Education. 2002;43(1):57–68.
- Jayusman TAI, Widiyarta A. Efektivitas Program Pos Pembinaan Terpadu (POSBINDU) Penyakit Tidak Menular (PTM) Di Desa Anggaswangi Kecamatan Sukodono Sidoarjo. Dinamika Governance: Jurnal Ilmu Administrasi Negara. 2017;7(2).
- Syamsianah A, Winaryati E. Hubungan Pengetahuan dan Lama Kerja Dengan Ketrampilan Kader Dalam Menilai Kurva Pertumbuhan Balita di Posyandu Kelurahan Tegalsari Kecamatan Candisari Kota Semarang. Jurnal Gizi. 2013;2(1).
Appendix A
QUESTIONNAIRE
Instruction :
1. Fill in the blanks with honest answers
2. Put a tick (X) on the multiple choice answer
3. Put a tick (√ ) on the available answer choices
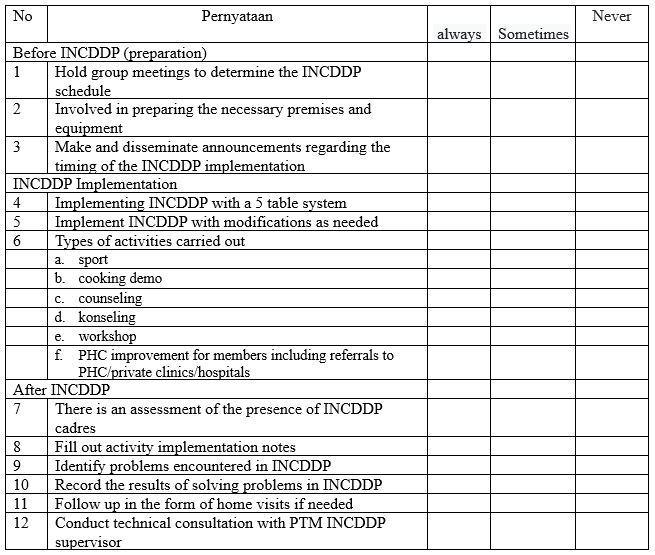
A. Cadre performance
B. INCDDP Cadre Training
Have you ever received training for INCDDP cadres?
a. Yes
b. No
C. Awards
1. Have you ever received an award in the form of a charter or award while being a INCDDP cadre?
a. Yes
b. No
2. Have you ever received an award in the form of funds while being a INCDDP cadre?
a. Yes
b. No
3. Do you get a uniform to carry out INCDDP activities?
a. Yes
b. No
4. Do you always receive an award if you are active in INCDDP activities?
a. Yes
b. No
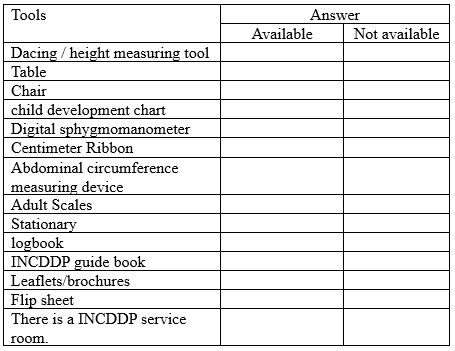
D. Facilities and infrastructure
E. Knowledge