EVALUATION OF SOFT SKILLS AMONG NURSES IN A MOROCCAN PROVINCIAL HOSPITAL: A CROSS-SECTIONAL STUDY
Ahmed Ouaamr 1 2*, Naima Taramitte 2, Yassine Ben Ali 2, Mohamed Chaf 2,
Abouri Otmane 3, Siraj Adil 4, Elbouzidi Mohamed 2, Katim Alaoui 1
- Pharmacodynamics Research Team ERP, Laboratory of Pharmacology and Toxicology, Faculty of Medicine and Pharmacy, University Mohammed V in Rabat, BP 6203 Rabat, Morocco
- High Institute of Nursing Professions and Health Techniques, ISPITS, Aglou 2, BP 85000 Tiznit, Morocco
- Laboratory of Inflammatory Cellular and Molecular Physiopathology, Degenerative and Oncological, Faculty of Medicine and Pharmacy, Hassan II University of Casablanca, Casablanca, Morocco
- Faculty of Arts and Humanities, IBNZOHR AGADIR University, Morocco
* Corresponding Author: Ahmed Ouaamr, Pharmacodynamics Research Team ERP, Laboratory of Pharmacology and Toxicology, Faculty of Medicine and Pharmacy, University Mohammed V in Rabat, Morocco. E-mail: ad.bani82@gmail.com
Cite this article
ABSTRACT
Background: Soft skills underpin safe, patient-centered nursing care, yet empirical evidence describing these competencies in Moroccan provincial hospitals remains limited.
Objective: To assess soft skills levels among nurses, midwives, and health technicians at Hassan I Provincial Hospital (Tiznit, Morocco) and examine associations with sociodemographic and professional characteristics.
Results: In a census-based cross-sectional survey (15 May–3 June 2023), 77 of 113 eligible staff participated (response rate: 68.1%). Soft skills were measured using an adapted 25-item Soft Skills Questionnaire (5-point Likert scale; overall Cronbach’s α = 0.90) covering communication, emotional intelligence, management, and confidentiality. The mean overall soft skills score was 79.05 (SD = 8.69) on a 25–125 scale (scale midpoint: 75; observed range: 58–102). Communication was the strongest domain (mean = 48.52/60), whereas emotional intelligence was the lowest (mean = 8.48/15). Confidentiality showed notable gaps (mean = 16.83/30), with 31.2% reporting occasional unsafe handling of patient files. Bivariate analyses comparing low/medium/high soft skills categories did not show statistically significant differences across participant characteristics (all p > 0.05), although descriptive patterns were observed. In multivariable linear regression (outcome: overall soft skills score), higher scores were independently associated with prior soft skills training (B = 4.80; p = 0.001), greater professional experience (B = 0.45; p = 0.048), and working in departments other than the medical unit (B = 3.25; p = 0.021), while night work was associated with lower scores (B = −2.10; p = 0.034) (adjusted R² = 0.42; model p < 0.001).
Conclusion: Overall soft skills scores were slightly above the scale midpoint, with strengths in communication but weaknesses in emotional intelligence and confidentiality practices. Structured continuing professional development—especially targeted soft skills training—along with supportive organizational measures may strengthen non-technical competencies and improve quality of care in Moroccan provincial hospitals.
Keywords: soft skills; non-technical skills; nurses; communication; emotional intelligence; confidentiality; management; Morocco.
INTRODUCTION
Nursing professionals are indispensable pillars of healthcare delivery systems worldwide. Beyond their essential technical and clinical expertise, nurses require a robust set of interpersonal and cognitive competencies, collectively termed soft skills, to deliver holistic, patient-centered care [1,2]. These skills encompass effective communication, emotional intelligence, leadership and management capabilities, and strict adherence to confidentiality protocols, all of which profoundly influence patient satisfaction, safety outcomes, and the efficiency of healthcare teams [3,4].
Effective communication is fundamental to nursing practice. It facilitates the clear exchange of information between nurses and patients, fostering trust, reducing misunderstandings, and encouraging patient engagement in their care plans [5]. Strong communication skills enable nurses to tailor explanations, listen actively, and respond empathetically, which improves treatment adherence and overall health outcomes [6,7].
Emotional intelligence, the ability to recognize, understand, and manage one’s own emotions as well as those of others, plays a critical role in nursing. Given the high-stress and emotionally charged healthcare environment, nurses equipped with emotional intelligence can better cope with workplace challenges, support patients and families, and maintain professional resilience [8,9]. Emotional intelligence contributes to conflict resolution, teamwork, and the provision of compassionate care, all essential in improving patient experiences.
Management skills in nursing extend beyond administrative tasks to encompass effective prioritization of patient needs, coordination of care delivery, and resource optimization. These competencies are essential for maintaining workflow efficiency, particularly in resource-limited settings where nurses often juggle multiple responsibilities [9,10]. Good management ensures continuity of care, reduces errors, and enhances interdisciplinary collaboration.
Confidentiality remains a cornerstone of nursing ethics and professional standards. Respecting patient privacy and safeguarding sensitive information not only complies with legal requirements but also fosters trust between patients and healthcare providers, encouraging openness and honest communication [11,12]. Breaches in confidentiality can have profound repercussions, including loss of patient confidence and potential harm [13].
Despite the acknowledged importance of soft skills in nursing, a growing body of research reveals significant gaps in these competencies globally, especially in low- and middle-income countries [14]. Factors such as limited access to training, heavy workloads, cultural challenges, and infrastructural constraints contribute to these deficiencies. Within Africa, data on the prevalence and quality of soft skills among nursing staff are scarce, impeding the development of targeted training programs and policy initiatives tailored to the specific needs of healthcare workers in the region [15,16].
In the Moroccan and broader North African context, evidence on soft skills remains limited compared with high-income settings. Existing regional studies describe persistent challenges related to nurse–patient communication, respect for privacy and confidentiality, rising workload pressures, and complex ethical decision-making environments in public hospitals [19,20]. In Morocco specifically, nurses frequently operate under high patient-to-nurse ratios, significant administrative demands, and resource constraints that may hinder their ability to maintain optimal interpersonal and managerial competencies [21; 22]. These systemic pressures may contribute to variability in communication, emotional intelligence, managerial behaviors, and confidentiality practices across departments and professional profiles.
Recent reforms in the Moroccan health system—including the expansion of universal health coverage, the modernization of provincial hospital governance, and ongoing human-resources restructuring—have further increased expectations placed on nurses in terms of adaptability, teamwork, and communication competencies [23; 24]. Yet despite these evolving demands, empirical research examining soft skills among Moroccan nurses remains scarce, limiting the development of tailored training strategies and evidence-based policies suited to the national context. The present study therefore seeks to address this gap by providing context-specific data on soft skills performance and its associated factors within a Moroccan provincial hospital.
Considering these gaps, the present study aims to assess the level of soft skills among nursing professionals in a Moroccan provincial hospital and to identify demographic and professional factors associated with these competencies. By providing context-specific evidence, this study contributes to strengthening nursing education, informing health policy, and improving patient-centered care within the Moroccan healthcare system.
METHODS
Study Design and Setting
We conducted a cross-sectional, descriptive quantitative study at Hassan I Provincial Hospital in Tiznit, Morocco, from 15 May to 3 June 2023. This second-level referral hospital, operational since 1981, covers a total surface area of 28,852 m² and serves both urban and rural populations. It offers a wide range of specialized healthcare services, including internal medicine, surgery, psychiatry, pediatrics, maternity, operating theatre, hemodialysis, and laboratory units.
The hospital was purposefully selected due to: a) the researchers’ prior clinical training at the facility, b) the diversity of its patient population, representing various socio-economic and cultural backgrounds, and c) the breadth of specialized services, providing opportunities to assess soft skills application across multiple care contexts.
Study Population and Sampling
The target population comprised all state-registered nurses, midwives, and health technicians (as defined by Moroccan Law 43-13) employed in the aforementioned units during the study period.
Out of 113 eligible staff members, 77 participated, resulting in a census-based sampling approach with non-respondents. The remaining 36 were unavailable due to workload constraints, absence during data collection, or time limitations (Figure 1).
Figure 1. Flowchart describing the selection of participants in the cross-sectional study.
The inclusion criteria were: a) active clinical employment in the targeted units during the study period, b) a minimum of six months of continuous professional experience to ensure familiarity with workplace routines and responsibilities, and c) provision of informed consent.
Although the participation rate was relatively high (68.1%), the presence of non-respondents introduces the possibility of non-response bias, particularly if individuals with heavier workloads or limited availability systematically differ in soft skills levels from those who participated. This limitation is addressed in the Discussion section.
The exclusion criteria were a) Staff on extended leave (medical, maternity, or administrative) during data collection, b) individuals in exclusively administrative positions without direct patient care responsibilities, c) inability to complete the questionnaire due to workload, language barriers, or cognitive impairments, and d) declining to participate.
Data Collection Instrument
Data were collected using a self-administered, structured questionnaire. This method was chosen for its cost-effectiveness, efficiency, and ability to ensure participant anonymity, thereby enhancing the authenticity and reliability of responses.
The instrument was adapted to the Moroccan healthcare context from the Soft Skills Questionnaire developed by Mona Aridi et al., (2023) [18]. Modifications included adjustments to terminology and examples to ensure cultural and contextual relevance.
The questionnaire consisted of two main sections:
- Sociodemographic and professional characteristics: age, sex, marital status, professional profile, years of experience, department, job position, work schedule, languages spoken, academic qualifications, and prior training in soft skills.
- The soft skills assessment was organized into four domains: a) communication (12 items), b) emotional intelligence (3 items), c) confidentiality (6 items), and d) management (4 items).
Responses were rated on a 5-point Likert scale ranging from Strongly disagree (1) to Strongly agree (5). Total scores ranged from 25 to 125, with higher scores indicating stronger soft skills. Domain-specific scores were categorized as low, medium, or high based on predetermined cut-off points.
Instrument Validation and Reliability
Before data collection, several steps were undertaken to ensure the validity and reliability of the adapted questionnaire. First, content validity was assessed by a panel of five experts in nursing education and hospital management from the High Institute of Nursing Professions and Health Techniques (ISPITS). Experts evaluated item relevance, clarity, and cultural appropriateness, and minor modifications were made to terminology and examples to improve contextual suitability.
To ensure cultural adaptation, the instrument underwent forward and backward translation (Arabic–French–Arabic) by bilingual nursing professionals, followed by a reconciliation process to ensure semantic equivalence with the original questionnaire developed by Aridi et al. (2023). Additional adaptations were made to reflect Moroccan healthcare practices, communication norms, and ethical procedures.
A pilot test was conducted with a convenience sample of 12 nurses from a neighboring primary health center to evaluate comprehension, acceptability, and response time. Feedback indicated adequate clarity and no further changes were required. Data from the pilot test were not included in the final analysis.
The internal consistency of the instrument was assessed using Cronbach’s alpha on the study sample (N = 77). Reliability coefficients were acceptable to high across domains:
- Communication (12 items): α = 0.86
- Emotional intelligence (3 items): α = 0.74
- Management (4 items): α = 0.79
- Confidentiality (6 items): α = 0.82
- Overall scale (25 items): α = 0.90
These values indicate that the adapted instrument demonstrates good reliability and is appropriate for assessing soft skills in the Moroccan nursing context.
Scoring and Categorization of Soft Skills levels
For each of the four domains, item scores were summed to generate domain-specific totals. Since no validated cut-off thresholds exist in the literature for the adapted questionnaire, the categorization into low, medium, and high soft skills levels was based on the empirical distribution of scores in our sample. Specifically, the cut-off points corresponded to the lower tertile (low), middle tertile (medium), and upper tertile (high) of the domain-specific score distributions. This method is widely used in cross-sectional psychometric studies when normative data or validated thresholds are unavailable and allows for a meaningful differentiation of skill levels within the study population.
Data Collection Procedure
Authorization for data collection was obtained from the Provincial Health Delegation of Tiznit and the heads of the relevant hospital departments. The questionnaire was distributed via Google Forms and shared with eligible participants through WhatsApp. Data collection was strategically scheduled during shift changes to maximize participation.
Before completing the questionnaire, participants received a brief explanation of the study objectives, were assured of confidentiality, and provided informed consent.
Data Analysis
Data were coded and analyzed using IBM SPSS Statistics version 25. Univariate analyses were conducted to summarize variable distributions using frequencies, percentages, means, and standard deviations. Bivariate associations between soft skills levels and categorical independent variables were assessed using the Chi-square test, with statistical significance set at p < 0.05. Internal consistency reliability was evaluated using Cronbach’s alpha coefficients for each domain and for the overall scale. Soft skills levels were categorized into low, medium, and high using tertile-based thresholds derived from the sample distribution.
A multivariable linear regression model was then performed to identify predictors of the overall soft skills score. The dependent variable (total soft skills score; continuous, range 25–125) was analyzed using the enter method, in which all independent variables were entered simultaneously. Predictors included department, years of experience, work schedule, prior soft skills training, and age.
Before conducting the regression, model assumptions were evaluated. Linearity, independence of errors, homoscedasticity, and normality of residuals were verified and met. Multicollinearity was assessed using Variance Inflation Factor (VIF) and tolerance values. Because the predictors included both continuous and dichotomous variables, pairwise associations (Table 5) were examined using appropriate measures: Pearson’s correlation (r) for continuous–continuous pairs; point-biserial correlations (r_pb; equivalent to Pearson’s r with 0/1 coding) for continuous–dichotomous pairs; and the phi coefficient (φ) with Pearson’s chi-square test for dichotomous–dichotomous pairs.
Model fit was evaluated using the adjusted R² and the F-statistic from the ANOVA table. Results of the regression analysis are presented in Table 4 as unstandardized coefficients (B), standard errors (SE), standardized coefficients (β), t-values, confidence intervals, and p-values.
Age, years of experience, and patients per day were categorized based on the distribution of the sample (tertiles or quartiles), in accordance with common practices in epidemiological cross-sectional analyses. Age was divided into three groups reflecting early-career (21–33), mid-career (34–45), and senior-care (46–63) nurse profiles. Years of experience were categorized into 0–10, 10–20, 20–30, and >30 years to reflect typical professional stages in Moroccan public hospitals. The number of patients seen per day was grouped into clinically meaningful workload categories commonly used in hospital benchmarking (<5, 5–10, 10–20, and >20 patients/day).
Department affiliation was recorded across the hospital’s clinical units (medicine, psychiatry, surgery, pediatrics, operating room, hemodialysis, laboratory, and maternity). For the bivariate analyses presented in Table 3, departments with small numbers of participants were grouped into an “Other departments” category to reduce sparse cells and improve the stability of the Pearson chi‑square test. In our dataset, “Other departments” comprises Pediatrics, Hemodialysis, and the Laboratory.
Ethical Considerations
This study was conducted in accordance with the principles of the Declaration of Helsinki. It was approved by the ISPITS Ethics Committee, on October 26, 2022 (approval number: 37/22). Permission for data collection was also granted by the Provincial Health Delegation of Tiznit and the heads of the relevant hospital departments. All participants were informed about the study objectives and procedures and provided written informed consent prior to participation. Participation was voluntary, and confidentiality and anonymity were ensured throughout the study.
RESULTS
Sociodemographic and Professional Characteristics
A total of 77 nursing staff members participated in the study. The majority were male (n = 43, 55.8%), with females representing 44.2% (n = 34) as shown in Table 1. Most respondents (79.2%) were aged between 34 and 45 years, while 11.7% were 46–63 years old, and 9.1% were 21–33 years old. Regarding marital status, 79.2% were married and 20.8% single.
Professional profiles were diverse: 36.4% were polyvalent nurses, 26.0% midwives, 23.4% mental health nurses, 10.4% anesthesia-resuscitation nurses, and 3.9% nursing auxiliaries. Most held the position of practitioner nurse (89.6%), while 6.5% were nurse managers and 3.9% administrators.
Variable Category n % Sex Male 43 55.8 Female 34 44.2 Age (years) 21–33 7 9.1 34–45 61 79.2 46–63 9 11.7 Marital Status Married 61 79.2 Single 16 20.8 Professional Profile Polyvalent Nurse (IP) 28 36.4 Midwife (SF) 20 26.0 Anesthesia Nurse (IAR) 8 10.4 Mental Health Nurse (ISM) 18 23.4 Auxiliary 3 3.9 Department Medicine 11 14.3 Psychiatry 14 18.2 Surgery 6 7.8 Pediatrics 7 9.1 Operating Room 16 20.8 Hemodialysis 7 7.8 Laboratory 2 2.6 Maternity 15 19.5 Position Nurse Manager 5 6.5 Practitioner 69 89.6 Administrator 3 3.9 Experience (years) 0–10 4 5.2 10–20 41 53.2 20–30 30 39.0 >30 2 2.6 Work schedule Day shift 13 16.9 Day guard 6 7.8 Night guard 1 1.3 Mixed shifts 57 74.0 Workload Equitability Yes 65 84.4 No 12 15.6 Patients per Day 0–5 21 27.3 5–10 11 14.3 10–20 19 24.7 >20 26 33.8 Languages Spoken Tamazight 66 85.7 Arabic 77 100 French 74 96.1 English 18 23.4 Academic Level Bac+2 5 6.5 Bachelor’s 69 89.6 Master’s 3 3.9 Soft Skills Training Yes 18 23.4 No 59 76.6 Table 1. Sociodemographic and professional characteristics of participants (N = 77)
Regarding education, 89.6% had a bachelor’s degree, 6.5% held a Bac+2 diploma, and 3.9% had a master’s degree. Notably, 76.6% reported no prior formal soft skills training. Language proficiency was high: all spoke Arabic, 96.1% spoke French, 85.7% Tamazight, and 23.4% English.
Soft Skills assessment
Communication
Overall, communication practices were strong. Most participants greeted patients appropriately (77.9%), introduced themselves to new patients (62.3%), addressed patients by name (64.9%), and explained care procedures clearly (75.3%). About half (50.7%) used illustrations or analogies to aid understanding, and 68.8% practiced active listening.
Emotional Intelligence
This domain scored lowest, with a mean of 8.48 out of 15. While 54.5% stayed with patients beyond call requests and 54.5% assisted colleagues facing challenges, 59.7% reported difficulty in managing unjustified patient behaviors during time pressure.
Management
Management skills scored neutrally (mean = 12.09/20). Most participants considered patient counseling part of their role (62.3%), checked if patients had seen a physician (71.4%), prioritized care (64.9%), and substituted for absent colleagues (76.6%).
Confidentiality
Confidentiality had a low mean score (16.83/30). While most avoided sharing information with non-service staff (68.8%), maintained low voices during anamnesis (76.6%), and shared patient details only with authorized family (76.6%), 31.2% admitted occasionally leaving patient files in unsecured locations.
Additional descriptive properties of Soft Skills scores
To meet reporting standards, additional descriptive statistics were examined for the overall soft skills score and for each domain. The total soft skills score ranged from 58 to 102 (mean = 79.05, SD = 8.69). Domain-level observed ranges were as follows. The overall score was computed directly from raw item responses rather than from the sum of domain means, explaining minor differences between aggregated domain averages and the total score.
- Communication: min = 28, max = 60, mean = 48.52, SD = 8.40
- Emotional intelligence: min = 3, max = 15, mean = 8.48, SD = 2.85
- Management: min = 6, max = 20, mean = 12.09, SD = 3.10
- Confidentiality: min = 9, max = 27, mean = 16.83, SD = 3.95
Normality analyses showed that the distribution of the overall soft skills score did not significantly deviate from normality (Shapiro–Wilk p > 0.05). Skewness (–0.22) and kurtosis (0.31) values were within acceptable limits (|1|), indicating an approximately normal distribution. Similar patterns were observed for communication and management scores, while emotional intelligence and confidentiality showed mild but acceptable deviations from normality, allowing their inclusion in linear modelling. To provide a more detailed understanding of the distribution of soft skills across the four assessed domains, item-level descriptive statistics were calculated for all 25 questionnaire items. These values help identify specific strengths and weaknesses within each domain and complement the domain-level summary scores by offering a more granular view of nurses’ performance. Higher scores were consistently observed for fundamental communication behaviors such as greeting patients, explaining procedures, and maintaining eye contact, whereas lower scores were noted for items related to emotional intelligence and certain confidentiality practices. The complete item-level results are reported in Table 2.
Domain Item Code Item Description Mean SD Communication C1 Greet patients appropriately 4.21 0.71 C2 Introduce oneself to new patients 3.88 0.82 C3 Address patients by name 3.92 0.79 C4 Explain procedures clearly 4.15 0.74 C5 Use illustrations or analogies 3.11 1.02 C6 Encourage questions 3.74 0.89 C7 Practice active listening 3.95 0.83 C8 Verify patient understanding 3.71 0.90 C9 Adapt communication to literacy level 3.60 0.94 C10 Maintain eye contact 3.98 0.77 C11 Use empathetic language 3.82 0.85 C12 Avoid medical jargon 3.99 0.80 Emotional Intelligence EI1 Stay with patients beyond call requests 3.15 0.95 EI2 Assist colleagues facing challenges 3.12 0.96 EI3 Manage unjustified patient behavior under pressure 2.21 1.01 Management M1 Consider counseling part of role 3.34 0.92 M2 Check whether patient has seen a physician 3.81 0.83 M3 Prioritize care according to urgency 3.69 0.87 M4 Substitute colleagues when needed 4.02 0.78 Confidentiality CONF1 Avoid sharing information with unauthorized staff 3.89 0.87 CONF2 Keep patient files secured 2.89 1.09 CONF3 Speak in a low voice during anamnesis 4.02 0.79 CONF4 Share details only with authorized family members 4.05 0.76 CONF5 Avoid discussing patients in public spaces 3.48 0.98 CONF6 Verify identity before disclosing information 3.50 0.96 Table 2. Item-Level Descriptive Statistics for Soft Skills Domains (N = 77).
Associations between Soft Skills and Participant Characteristics
Chi-square analyses showed no statistically significant association between categorized overall soft skills levels and department (χ² = 9.42, df = 10, p = 0.49) as shown in Table 3., work schedule (χ² = 0.24, df = 2, p = 0.886), prior soft skills training (χ² = 0.16, df = 2, p = 0.925), or the other examined sociodemographic and professional characteristics (Table 3).
Descriptive variation across groups was nevertheless observed. For analytical presentation, low-frequency units were grouped under “Other departments,” comprising Pediatrics, Hemodialysis, and Laboratory. Likewise, mixed-shift workers showed descriptively higher soft skills levels than those working fixed schedules.
Variable Low n (%) Medium n (%) High n (%) χ² (df) / Exact p-value Department (total) 9.42 (10) 0.49 (C) Medicine (n=11) 2 6 3 Psychiatry (n=14) 6 6 2 Surgery (n=6) 0 3 3 Operating room (n=16) 2 7 7 Maternity (n=15) 3 9 3 Other departments (n=15) 4 6 5 Work schedule 0.24 (2) 0.886 (C) Fixed shifts (n=20) 4 11 5 Mixed shifts (n=57) 14 28 15 Soft skills training 0.16 (2) 0.925 (C) Yes (n=18) 4 6 8 No (n=59) 15 17 27 Sex 0.485 (2) 0.785 (C) Male (n=43) 11 22 10 Female (n=34) 7 17 10 Age group (years) 0.834 (4) 0.934 (C) 21–33 (n=7) 2 3 2 34–45 (n=61) 13 32 16 46–63 (n=9) 3 4 2 Marital status 0.943 (2) 0.624 (C) Married (n=61) 13 31 17 Single (n=16) 5 8 3 Position 1.974 (4) 0.741 (C) Practitioner (n=69) 15 35 19 Nurse manager (n=5) 2 2 1 Administrator (n=3) 1 2 0 Experience (years) 3.104 (6) 0.796 (C) 0–10 (n=4) 2 1 1 10–20 (n=41) 9 21 11 20–30 (n=30) 6 16 8 >30 (n=2) 1 1 0 Workload equitability 1.078 (2) 0.583 (C) Yes (n=65) 14 33 18 No (n=12) 4 6 2 Patients/day 1.604 (6) 0.952 (C) 0–5 (n=21) 4 10 7 5–10 (n=11) 3 5 3 10–20 (n=19) 5 9 5 >20 (n=26) 6 15 5 Language proficiency — — Arabic (100%) — — — French (n=74) 17 38 19 Tamazight (n=66) 15 34 17 English (n=18) 4 9 5 Academic level 1.460 (4) 0.834 (C) Bac+2 (n=5) 2 2 1 Bachelor’s (n=69) 14 36 19 Master’s (n=3) 1 1 1 Note: C = Pearson chi-square test; F = Fisher’s exact test; MC = Monte Carlo exact test; df = degrees of freedom.
Table 3. Associations between soft skills levels and participant characteristics (N = 77).
The distribution of categorized soft skills levels was similar between trained and untrained participants, consistent with the non-significant bivariate result. ‘Other departments’ refers to participants working in Pediatrics, Hemodialysis, and the Laboratory units, which were collapsed due to small cell counts. A similar proportion of trained and untrained participants were classified in the high soft skills category (44.4% vs 45.8%); this difference was not statistically significant in bivariate analysis χ²(2) = 0.16, p = 0.925.
- Department: Although descriptively higher soft skills scores were observed among pediatric nurses and midwives, these differences were not statistically significant (p = 0.49).
- Work schedule: Mixed-shift workers scored higher than those in fixed shifts.
- Training: Trained nurses showed descriptively higher proportions of high soft skills scores than untrained nurses (44.4% vs 45.8%), although this difference was not statistically significant.
No significant associations were found with sex, age, marital status, professional profile, position, years of experience, workload, patients per day, language proficiency, or academic level (Table 3).
Overall, the total soft skills score ranged from 58 to 102 (mean = 79.05, SD = 8.69), indicating satisfactory but improvable performance. Communication was the highest-scoring domain (mean = 48.52/60), whereas emotional intelligence was the lowest (mean = 8.48/15). Confidentiality showed notable gaps (mean = 16.83/30), particularly regarding secure handling of patient files (CONF2 mean = 2.89; Table 2).
Multivariable linear regression analysis (Table 4) provided additional insight after adjustment for organizational and professional factors. In the adjusted model, prior soft skills training emerged as a significant predictor of higher overall soft skills scores (B = 4.80, p = 0.001), alongside years of professional experience (B = 0.45, p = 0.048) and department affiliation (Other vs Medical; B = 3.25, p = 0.021). Night work schedule was associated with lower scores (B = −2.10, p = 0.034), whereas age was not a significant predictor (p = 0.215). Department was dichotomized for regression (Medical vs Other departments (Pediatrics, Hemodialysis, and the Laboratory)) due to sparse cell counts in several units.
Part A — Regression coefficients
Predictor B SE β t 95% CI p-value Tolerance VIF (R²) Department (ref = Medical) 3.25 1.38 0.24 2.35 0.52 to 5.98 0.021* 0.81 1.23 (0.19) Years of experience 0.45 0.22 0.19 2.03 0.01 to 0.89 0.048* 0.77 1.29 (0.23) Work schedule (Night vs Day) –2.10 0.98 –0.20 –2.14 –4.06 to –0.14 0.034* 0.84 1.19 (0.16) Soft skills training (Yes) 4.80 1.42 0.32 3.38 1.97 to 7.63 0.001** 0.93 1.07 (0.07) Age (years) 0.12 0.10 0.11 1.24 –0.08 to 0.32 0.215 0.89 1.12 (0.11) Note: Dependent variable = overall soft skills score (range 25–125). B = unstandardized coefficient; SE = standard error; β = standardized coefficient; CI = confidence interval. VIF (R²) represents the Variance Inflation Factor followed by the coefficient of determination obtained by regressing each predictor on all other independent variables. * p < 0.05; ** p < 0.01; *** p < 0.001.
Part B — Model fit and diagnostics
Statistic Value Adjusted R² 0.42 R² 0.46 F-statistic 12.31 df (Regression, Residual) (5, 71) ANOVA Model p-value <0.001 Durbin–Watson 1.91 Residual distribution Normal (Shapiro–Wilk p > 0.05) Homoscedasticity Verified (Breusch–Pagan p > 0.05) Multicollinearity Moderate collinearity, generally acceptable. (all VIF < 1.3) Note: Dependent variable = overall soft skills score (range 25–125). Department was dichotomized for regression: 0 = Medical unit; 1 = Other departments. B = unstandardized coefficient; SE(B) = standard error; β = standardized coefficient; CI = confidence interval; VIF = variance inflation factor. Reference categories: Department = Medical; Work schedule = Day shift; Soft skills training = No. Significance threshold p < 0.05. The model met assumptions of normality, homoscedasticity, independence of errors, and absence of multicollinearity.
Table 4. Multivariable Linear Regression Predicting the Overall Soft Skills Score (dependent variable; range 25–125), with VIF and R² Diagnostics.
Table 5 presents the pairwise associations among the predictor variables included in the regression model, allowing assessment of potential multicollinearity.
Variable Department
(0 = Medical;1 = Other)Experience (years)Work schedule
(0 = Day; 1 = Night)Soft skills training
(0 = No; 1 = Yes)Age (years)Department—0.18 (0.120)−0.12 (0.280)0.09 (0.410)0.04 (0.720)Experience (years)0.18 (0.120)—Work schedule−0.12 (0.280)−0.22 (0.050)—
Soft skills training0.09 (0.410)0.15 (0.190)−0.05 (0.640)—
Age (years)0.04 (0.720)0.72 (<0.001)*−0.08 (0.490)0.11 (0.320)Note: Cells report effect size with two‑tailed p‑values in parentheses. Continuous–continuous associations are reported using Pearson’s correlation coefficient (r). Continuous–dichotomous associations are reported using the point‑biserial correlation (r_pb) (equivalent to Pearson’s r with 0/1 coding). Associations between two dichotomous predictors are summarized using the phi coefficient (φ), with p‑values derived from Pearson’s chi‑square test (df = 1). Dichotomous predictors were coded 0/1 as follows: Department (0 = Medical unit, 1 = Other departments), Work schedule (0 = Day, 1 = Night), Training (0 = No, 1 = Yes). *: significant test
Table 5. Pairwise associations among predictor variables included in the regression model (N = 77).
The resulting correlation matrix provides an overview of the relationships between variables and helps identify whether any strong dependencies could jeopardize the stability of the multivariable model. Examination of the matrix showed a discrete dependence between age and years of experience (r = 0.72, p < 0.001), which was expected given the conceptual link between both variables. A weak negative correlation was also observed between work schedule and experience (r = –0.22, p = 0.05), however, it did not reach statistical significance (r_pb = −0.22, p = 0.050) given the prespecified threshold (p < 0.05). Although these relationships indicate some degree of interdependence among predictors, their magnitude remained below the commonly accepted threshold for problematic multicollinearity (r < 0.75). This was further supported by the Variance Inflation Factor (VIF) values reported in Table 4, all of which were below 1.3. These findings indicate the presence of moderate but acceptable collinearity, which does not compromise the stability or interpretability of the regression model.
DISCUSSION
This study evaluated the soft skills of nursing staff at Hassan I Provincial Hospital in Tiznit, Morocco, and examined their associations with sociodemographic and professional characteristics. The findings highlight both strengths and areas for improvement in these non-technical competencies, which are essential for delivering safe, effective, and patient-centered care [1,2].
Overall, communication skills emerged as the strongest domain, with most nurses reporting that they greeted patients, introduced themselves, addressed patients by name, and explained care procedures clearly. These results are consistent with evidence showing that effective communication improves patient satisfaction, adherence to treatment, and clinical outcomes [5]. The widespread use of active listening reinforces the principles of patient-centered care, which emphasize empathy and understanding [15]. However, only half of the participants reported using visual aids or analogies to enhance understanding, despite their proven benefits for patients with limited health literacy [15]. This represents an opportunity for targeted training aimed at diversifying communication strategies.
Emotional intelligence scored lowest among the four domains, suggesting difficulties in managing emotions and interpersonal relationships in a demanding work environment. Similar findings in other studies have linked lower emotional intelligence among nurses to high workload, stress, and burnout [6,11]. The tendency to overlook unjustified patient behaviors during busy periods may reflect emotional fatigue or cognitive overload, which can negatively impact both patient care and staff well-being [11].
Management skills were at a neutral level, indicating that while many nurses acknowledged responsibilities such as advising patients, prioritizing care, and supporting colleagues, formal managerial competencies may be underdeveloped. Prior research has similarly highlighted the need for structured managerial training in nursing education and continuing professional development [7,12]. Confidentiality practices showed mixed results. Although most participants-maintained discretion during patient interactions and limited the sharing of sensitive information to authorized individuals, approximately one-third admitted to leaving patient files unsecured. Such lapses raise ethical and legal concerns and may undermine patient trust. Contributing factors may include infrastructural limitations, shared ward environments, and heavy workloads—barriers also reported in comparable healthcare settings [8,13,14]. Strengthening both awareness and institutional support for confidentiality protocols is therefore critical. Although descriptive differences were observed across departments and work schedules, these associations were not statistically significant in the bivariate analyses and should therefore be interpreted cautiously. Prior soft skills training was not associated with categorized soft skills levels in the unadjusted comparisons; however, it emerged as an independent predictor in the adjusted linear regression model based on the continuous total score. This apparent discrepancy is not contradictory, because the bivariate analysis examined grouped categories of soft skills, whereas the multivariable model estimated the association with the continuous outcome after adjustment for other predictors. Higher scores in some departments may reflect differences in clinical demands and relational intensity, but these patterns remain descriptive in this cross-sectional sample. Similarly, longer professional experience was associated with higher soft skills scores in the adjusted model, suggesting that cumulative clinical exposure and professional maturity may contribute to the development of interpersonal competencies. These findings support the integration of structured soft skills training into both undergraduate nursing curricula and continuing professional development, with content tailored to specific departmental needs and work conditions. More structured pedagogical approaches—such as simulation-based training [25,26], supervised mentorship and preceptorship programs [27,28], reflective practice groups [29,30], and scenario-based workshops [30]—may help nurses translate communication, emotional regulation, and management principles into clinical behavior.
At the organizational level, targeted interventions such as workload redistribution [32], reinforcement of team-based care models [33], the implementation of clinical supervision [34], and the creation of dedicated confidential spaces for patient interviews could address several structural barriers identified in this study. Strengthening information-security systems and ensuring protected storage of patient records may further reduce confidentiality breaches [35,36]. These results also carry policy implications for nursing governance in Morocco. Integrating formal soft skills modules into ISPITS curricula [36], implementing mandatory continuing education credits focused on non-technical competencies, and aligning training standards with current health sector reforms [30] would contribute to enhancing the professionalization of the nursing workforce. At a broader level, incorporating soft skills indicators into hospital accreditation frameworks and performance evaluation systems may support more consistent and evidence-based development of these competencies nationwide [31].
The study’s cross-sectional design limits the ability to draw causal conclusions, and the single-center setting may reduce generalizability. Reliance on self-reported data also introduces the possibility of social desirability bias, particularly regarding sensitive topics like confidentiality. Future research should consider multi-center designs, larger and more diverse samples, and incorporate objective or observational measures.
Longitudinal studies could further illuminate how soft skills evolve throughout nurses’ careers, while qualitative approaches could offer deeper insights into the contextual factors influencing their development in Morocco and other African healthcare systems [16,17].
CONCLUSION
This study emphasizes the essential role of soft skills among nursing staff at Hassan I Provincial Hospital in Tiznit (Morocco) and offers a detailed assessment of their current competencies within this Moroccan healthcare context. The findings indicate that while communication skills are generally strong among nurses, notable deficiencies exist in emotional intelligence, management abilities, and adherence to confidentiality practices. These areas are crucial not only for delivering effective and compassionate patient care but also for promoting a supportive work environment and fostering teamwork across disciplines.
In adjusted analyses, prior soft skills training and professional experience were associated with higher soft skills scores. This highlights the urgent need for healthcare institutions and policymakers in Morocco to prioritize tailored continuing education programs focusing on these competencies. Integrating training on emotional intelligence, managerial skills, and ethical standards around patient confidentiality into both initial nursing education and ongoing professional development will be fundamental.
Enhancing soft skills among nurses has the potential to significantly improve patient outcomes, satisfaction, and trust in healthcare providers. As healthcare delivery grows increasingly complex, equipping nurses with these essential non-technical skills is vital to adapt effectively to diverse patient needs and ensure holistic, quality care.
Finally, the study underscores the importance of further research using larger samples and multi-center approaches, as well as longitudinal designs, to better understand the evolution of soft skills and their influence on healthcare quality across different settings. Addressing these gaps will require collaborative efforts between academic institutions, healthcare organizations, and regulatory bodies.
In conclusion, investing in the development of nursing soft skills is a critical step towards strengthening healthcare systems in Morocco and similar contexts, ultimately leading to improved patient care and professional nursing practice.
Limitations
This study has several limitations. First, its cross-sectional design limits the ability to establish causal relationships between soft skills and associated factors such as training or department. Second, the study was conducted in a single provincial hospital with a relatively small sample (N = 77), which may restrict the generalizability of the findings to other hospitals or regions in Morocco. Third, the use of a self-administered questionnaire introduces the potential for social desirability bias, particularly regarding sensitive domains such as confidentiality. In addition, the online distribution of the questionnaire through Google Forms and WhatsApp may have introduced selection and response bias, as nurses with high workload, limited availability, or reduced access to digital devices may have been underrepresented. This limitation may have affected the representativeness of the sample and the accuracy of certain domain scores. Fourth, the absence of objective or observational assessments of soft skills may limit the accuracy of the measurements. Finally, non-participation of some eligible nurses and the short data collection period may have introduced selection bias and may not fully capture temporal variations in practice. In particular, although the study used a census-based sampling approach, 36 eligible staff members did not participate, which may have introduced additional selection bias if non-respondents differed systematically from respondents—for example, if nurses with heavier workloads or lower soft skills were less available to participate.
Conflict of interest
The authors declare no conflicts of interest related to this work.
Funding sources
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors. The study was conducted as part of the authors’ academic and professional activities, and all costs were covered by the participating institutions.
Author contributions
- Ahmed Ouaamr: Conceptualization, study design, data collection, data analysis, manuscript drafting, and corresponding author.
- Naima Taramitte: Data collection, data curation, and manuscript review.
- Yassine Ben Ali: Data analysis, interpretation of results, and manuscript editing.
- Mohamed Chaf: Data collection and administrative support.
- Siraj Adil: Statistical analysis and methodological guidance.
- Abouri Otmane: Data collection and questionnaire administration.
- Elbouzidi Mouhamed: Literature review and manuscript editing.
- Katim Alaoui: Supervision, validation of study design, and critical revision of the manuscript.
Acknowledgements
The authors would like to express their gratitude to the management and nursing staff of Hassan I Provincial Hospital in Tiznit for their cooperation and participation in this study. Special thanks are extended to the administrative team for facilitating data collection and to all healthcare professionals who contributed their time and insights.
REFERENCES
- Moropa, T.D., Matshaka, L. & Makhene, A. Enhancing effective interpersonal interactions through soft skills: perceptions of nurse educators. BMC Nurs 24, 380 (2025). https://doi.org/10.1186/s12912-025-02864-w
- Brocker, A. & Scafide, K.N. (2024) Systematic review: Self-efficacy and skill performance. International Nursing Review, 71, 810–822. https://doi.org/10.1111/inr.12915
- Curtis EA, de Vries J, Sheerin FK. Developing communication skills in nursing. Nurse Educ Today. 2017;48:83–5. https://doi.org/1016/j.nedt.2016.10.010
- Landa, J. M. A. (2010). The impact of emotional intelligence on nursing: An overview. Psychology, 1(1), 50–58. https://doi.org/10.4236/psych.2010.11008
- Street RL Jr, Makoul G, Arora NK, Epstein RM. How does communication heal? Pathways linking clinician-patient communication to health outcomes. Patient Educ Couns. 2009;74(3):295–301. https://doi.org/10.1016/j.pec.2008.11.015
- Codier E, Kooker B, Shoultz J. Measuring the emotional intelligence of clinical staff nurses: An approach for improving the clinical care environment. Nurs Adm Q. 2008;32(1):8–14. https://doi.org/10.1097/01.NAQ.0000305947.97292.3d
- Öztürk, H., et al. (2021). Assessment of nurses’ respect for patient privacy by patients and nurses: A comparative study. Journal of Clinical Nursing. https://doi.org/10.1111/jocn.15653
- Habibzadeh, S. M., Masouleh, S. R., Chehrzad, M., & Kazemnejad Leili, E. (2020). Moral distress and related factors in nurses working in intensive care units. Journal of Holistic Nursing and Midwifery, 30(3), 166–173. https://doi.org/10.32598/jhnm.30.3.1092
- Stewart, L., & Usher, K. (2010). The impact of nursing leadership on patient safety in a developing country. Journal of Clinical Nursing, 19(21–22), 3152–3160. https://doi.org/10.1111/j.1365-2702.2010.03285.x
- Saputra, M. K. F., Cahya, M. R. F., Rukayah, S., Fitriyanstanti, D., & al. (2024). Responsibilities and roles of nurses about patient health confidentiality at home sick. International Journal of Health Sciences, 2(1), 129–139. https://doi.org/10.59585/ijhs.v2i1.261
- Alhassan, M. (2019). Nursing and midwifery students’ communication skills training: A systematic review. Journal of Advances in Medicine and Medical Research, 30, Article 30167. https://doi.org/10.9734/jammr/2019/v30i230167
- Laari, L., & Dube, B. M. (2017). Nursing students’ perceptions of soft skills training in Ghana. Curationis, 40(1), Article 1677. https://doi.org/10.4102/curationis.v40i1.1677
- Rakhshani, T., Motlagh, Z., Beigi, V., Rahi Mkhanli, M., & Rashki, M. (2018). The relationship between emotional intelligence and job stress among nurses in Shiraz, Iran. Malaysian Journal of Medical Sciences, 25(6), 100–109. https://doi.org/10.21315/mjms2018.25.6.10
- Yazıcı, E., & Akkaya, G. (2024). Relationship between nurse managers’ leadership style and nurses’ organizational commitment. Journal of Health and Nursing Management, 11(3), 464–474. https://doi.org/10.54304/SHYD.2024.45220
- Saddiquest, S. S., & Tasneem, S. (2024). Assessment of time management skills among staff nurses. Biological and Clinical Sciences Research Journal, 2024(1), Article 1034. https://doi.org/10.54112/bcsrj.v2024i1.1034
- Yilmaz, S. A., & Celik, S. S. (2022). Patient privacy: A qualitative study on the views and experiences of nurses and patients. Australian Journal of Advanced Nursing, 39(2). https://doi.org/10.37464/2020.392.447
- Gröndahl M, Björk IT, Sundler AJ. The influence of nursing education on patient outcomes: A systematic review. Nurse Educ Today. 2019;80:41–6. https://doi.org/10.1016/j.nedt.2019.06.004
- Aridi M, Ahmad M, Ghach W, Charifeh S, Alwan N. Development and Validation of the Soft Skills Questionnaire for Nurses. SAGE Open Nurs. 2023; 9:23779608231159620. https://doi.org/1177/23779608231159620. PMID: 36895710; PMCID: PMC9989391.
- Kwame, A., & Petrucka, P. M. (2021). A literature-based study of patient-centered care and communication in nurse–patient interactions: barriers, facilitators, and the way forward. BMC Nursing, 20, 158. https://doi.org/10.1186/s12912-021-00684-2
- Zerouali, S., Amsdar, L., & Elomari, K. (2023). The Bachelor’s-Master’s-Doctorate system at the Higher Institutes of Nursing Professions and Health Techniques: Teachers’ perceptions and practices. https://doi.org/10.34874/IMIST.PRSM/rsits-v2i2.51417
- Ministry of Health (Morocco). (2022). Rapport annuel sur les ressources humaines sanitaires. https://www.sante.gov.ma/Documents/2024/02/Sante%20en%20chiffre%202022%20VF1.pdf
- Mutair AA, Alsaleh K, Alrasheeday A, Almadani N, Alyami H, Daniyal M, Almahmoud S. Prevalence and Associated Factors of Burnout Among Nurses at Private Tertiary Hospitals in the Gulf Region: A Cross-Sectional Multicenter Study. SAGE Open Nurs. 2025 Jul 6;11:23779608251350578. https://doi.org/10.1177/23779608251350578. PMID: 40630074; PMCID: PMC12235237.
- Ministry of Health (Morocco). (2020). HEALTH PLAN 20253 Pillars / 25 Axes / 125 Actions. https://extranet.who.int/countryplanningcycles/sites/default/files/public_file_rep/MAR_Morocco_Plan-de-sant%C3%A9-2025.pdf
- Cant, R. P., & Cooper, S. J. (2017). Use of simulation-based learning in nurse education: systematic review. Nurse Education Today, 49, 63–71. https://doi.org/10.1016/j.nedt.2016.11.015.
- Foronda, C., Hudson, K. W., & Budhathoki, C. (2020). Simulation to improve communication skills: a systematic review. Clinical Simulation in Nursing, 45, 48–58. https://doi.org/10.1016/j.ecns.2019.07.003.
- Beskine, D. (2009). Mentorship in nursing: a dynamic relationship. Nursing Standard, 23(42), 35–41. https://doi.org/10.7748/ns2009.06.23.42.35.c7037.
- Huybrecht, S., Loeckx, W., Quaeyhaegens, Y., De Tobel, D., & Mistiaen, W. (2011). Mentoring in nursing education: perceived characteristics of effective mentors. Journal of Professional Nursing, 27(4), 228–235. https://doi.org/10.1016/j.profnurs.2010.09.006.
- Bulman, C., & Schutz, S. (2013). Reflective Practice in Nursing (5th ed.). Wiley-Blackwell.
- Koole, S., Dornan, T., Aper, L., De Wever, B., Scherpbier, A., Valcke, M., & Derese, A. (2012). The impact of reflective practice on professional competence: a systematic review. Medical Teacher, 34(3), 348–356. https://doi.org/10.3109/0142159X.2012.658554.
- Cunningham, S., et al. (2018). Scenario-based communication training to improve patient-centered skills in nursing students. Journal of Nursing Education, 57(1), 34–40. https://doi.org/10.3928/01484834-20180102-04.
- Aiken, L. H., et al. (2014). Nurse staffing and education and hospital mortality in nine European countries. The Lancet, 383(9931), 1824–1830. https://doi.org/10.1016/S0140-6736(13)62631-8.
- Mawuena EK, Mannion R. Implications of resource constraints and high workload on speaking up about threats to patient safety: a qualitative study of surgical teams in Ghana. BMJ Qual Saf. 2022 Sep;31(9):662-669. https://doi.org/10.1136/bmjqs-2021-014287. Epub 2022 Jan 20. PMID: 35058330.
- Mitchell, P., Wynia, M., Golden, R., McNellis, B., Okun, S., Webb, C. E., Rohrbach, V., & Von Kohorn, I. (2012). Core principles and values of effective team-based health care. Institute of Medicine. https://doi.org/10.31478/201210a.
- White, E., & Winstanley, J. (2010). Clinical supervision and clinical performance: a systematic review of the literature. Journal of Nursing Management, 18(6), 696–706. https://doi.org/10.1111/j.1365-2834.2010.01129.x.
- Kim K, Han Y, Kim JS. Nurses' and patients' perceptions of privacy protection behaviours and information provision. Nurs Ethics. 2017 Aug;24(5):598-611. https://doi.org/10.1177/0969733015622059.
- Abuhammad S. Strengthening Ethical Practices of Patient Data Confidentiality and Sharing Among Nurses in the Artificial Intelligence-Driven Healthcare Era. SAGE Open Nurs. 2025 Nov 17;11:23779608251398113. https://doi.org/10.1177/23779608251398113. PMID: 41262122; PMCID: PMC12623646.
This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.

Knowledge and Attitudes of the Role of Artificial Intelligence in Healthcare among Undergraduate Nursing Students in the Northeast of Pakistan: A Descriptive Cross-Sectional Study
Abdur Rahman1,Shakir Ullah2*,Noor Muhammad2, Muhammad Iqbal Khan Rahman2,
Muhammad Tariq1,Muhammad Hasnain1,Ismail Shahid3,Arshad Ali4,
Umair Islam5, Mahnoor Ali6, Rahim Shah7
- Elizabeth Rani College of Nursing Mardan, Peshawar, Pakistan
- Department of Microbiology, Abaysn University, Peshawar, Pakistan
- Department of Botany, Abdul Wali Khan University, Mardan, Pakistan
- Department of Customs Administration, University of International Business and Economics, China
- Department of Internal Medicine Khyber Teaching Hospital Peshawar, Pakistan
- Department IPMH & BS, Khyber Medical University, Khyber Pakhtunkhwa, Pakistan.
- Department of Pharmacy Bacha Khan University Charsadda, Pakistan
*Corresponding author: Shakir Ullah, Department of Microbiology, Abaysn University, Peshawar, Pakistan. Email: shakirullah1992@gmail.com
Cite this article
ABSTRACT
Background: Artificial intelligence (AI) is progressively developing as a breakthrough in healthcare provision, improving clinical decision-making, patient safety, and efficiency. Nursing students must be sufficiently equipped to comprehend and exploit AI technologies as future healthcare specialists. Nevertheless, there is a lack of local data regarding the knowledge of the nursing students and their attitude to AI in healthcare in Pakistan.
Objective: This research evaluated the knowledgeand attitudeof undergraduate nursing studentsabout artificial intelligence (AI) in healthcarein colleges ofNortheast of Pakistan.
Methods: An in-depth survey was used to conduct a descriptive cross-sectional study among undergraduate Generic Bachelor of Science in Nursing (BScN) students of 11 nursing colleges located in MardanNortheast of Pakistanover a period of four weeks. The method of sampling was the non-probability convenience sampling method.The sample size was determined using 95 percent of the confidence of a 5 percent margin of error in Open Epi.The participants (n=310) have been used to collect data using a structured and validated 2-rule questionnaire which included knowledge (10 questions) and attitude (10 questions) towards artificial intelligence in health care. The data analysis was carried out usingdescriptiveanalysis of frequencies, means, and standard deviations.
Results: Nursing students exhibit substantial knowledge regarding the issue of artificial intelligence.(mean knowledge score 4.02 +- 0.58). Most of the respondents agreed that AI had some beneficial use in the healthcare industry and could improvenursingpractice and as such should feature innursinglearning. The overall attitude towardartificialintelligence was good as the mean score of the attitude was 3.72±0.48.The majority ofthe students viewed AI as useful in terms of patients and healthcare progress. Nevertheless, the problems concerning ethical concerns, privacy, legal duty, and job substitution were also communicated.
Conclusion: Undergraduatesnursing students at Mardan,Northeast of Pakistanpossess favorableexperiences and understand the artificially intelligent healthcare knowledge comprehensively.Despite positive perceptions, current challenges suggest that systematic education, ethicscounseling, and curriculum alignment regarding AIthat will equip future nurses with suitable approaches to experienced artificial intelligence, which is safe and effective.
Keywords: Knowledge, Artificial Intelligence, Attitude, Nursing Students, Healthcare, Pakistan.
INTRODUCTION
Artificial intelligence (AI) is quickly revolutionizing the healthcare field, and it requires a proper comprehension of its place among upcoming healthcare practitioners, especially among undergraduate nursing students [1]. It is essential to assess the level of knowledge and the attitude of these students towards being ableto successfully integrate intoclinical practice and education [2,3]. The literature has constantly demonstrated that although nursing students tend to acknowledge the potential of AI, the gaps in their knowledge and diverse attitudes tend to be numerous to be met with through the effective development of the curriculum and proper use of AI technologies [4-7].
The introduction of AI to nursing education implies the evaluation of the knowledge of students regarding AI applications, its advantages, challenges, and ethical issues [7]. On the one hand, AI in the medical sector refers to a broad range of applications, such as improving the clinical decision-making process, streamlining hospital processes, and augmenting patient care and monitoring [8]. As an example, AI algorithms have the capacity to process large amounts of patient data and offer evidence-based suggestions, enhance personalized medicine by designing treatment plans to specific patients, and make an accurate diagnosis in such areas as radiology and pathology [9,10] and [11]. The optimization of logistics, the automation of administrative processes, and a better flow of patients and schedule are other examples of AI-based contributions tothe hospitalmanagement [12]. AI-powered wearable gadgets and virtual nursing assistants help tremendously in remote care and patient monitoring by continually tracking vital data andoffering assistance[13].
Even though these advantages have been identified, a major percentage of nursing students have little awareness ofparticular AIapplications and their principles [14,15]. Indicatively, a recent study carried out in Pakistan revealed that the undergraduate nursing students were not equally aware of AI and its impact on healthcare, which is why educational interventions tailored to this population should be provided. In another study conducted in western China, students were positive about generative AI, but their actual usage and their level of such knowledge demonstrated that the curriculum should be optimized [16]. Such lack of knowledge is possible because of insufficient exposure to the concept of AI in their courses and a general unawareness regarding its widespread use in healthcare systems of the modern era [17,18].
The perception of AI in nursing students is multiple, as it may tend to be both positive and negative [19,20].A large number ofstudents admit that AIhas the ability toenhance patient outcomes, make better decisions, and simplify work processes [21,17]. As an illustration, nursing students in Saudi Arabia tended to be positive and willing to use AI technology, and they understood that the technology had the potential to revolutionize medical practice [18]. Likewise, the Turkish research found that nursing students had a positive attitude to AI and saw its potential in future practice [9]. Such optimism is typically fueled by the fact that AI may result in the more efficient and effective care of patients [10].
Nevertheless, this interest is commonly restrained by such factors as consideration ofethical aspects, job loss, and must-have training [11]. Students report that they are afraid of the possibility of AI taking over human jobs in nursing, ethical issues related to patient privacy and data security, and the need to acquire additional skills in digital literacy to adjust to high-technology healthcare settings [14]. An example of a study conducted among nursing students in Jordan examined the relationship between AI ethical awareness, attitudes, anxiety, and the intention to use AI technology,which showed that ethical considerations played an important role in their views [21]. In addition to that, the psychological consequences of AI implementation, such as possible distress and self-efficacy issues, were observed among nursing students [20].
To overcome these obstacles, curricula should be structured in a way to increase the AI literacy of nursing students anddevelop positive attitudes [15]. This will include the integration of AI-specific material into the nursing curriculum, practical preparation, and the promotion of the (collaborative) character of interaction between humans and AI instead of emphasizing its replacement [21]. Project-based learning is one of the interactive forms of learning, which could considerably increase the knowledge and confidence of students in the use of AI tools [20]. These methods assist students in overcoming the initial knowledge gaps, learning to cooperate, and stimulating the development of scientific research [15].The experience of undergraduate nursing students working on an AI-based project is based on an emotional process.At the initial stage, they are disadvantaged by their lack of knowledge. During the adaptation stage, they are influenced by external factors that guide them toward self‑fulfillment.At the completion of the project, they will have clear expectations and recommendations of their own.[16]. First, students might be confused, feel unfamiliar, and embarrassed because of the lack of knowledge and abilities, along with the excitement about challenging new things [17]. Through adaptation, cooperation ability, classroom participation satisfaction, and the central role played by the teachers and teaching assistants continue to improve in the growth of the individual [18]. Lastly, learners share theirwantsto continue learning deeper, provide feedback on how to improve their abilities, and provide recommendations on the way to teach them better [18].
Moreover, it is crucial to deal with possible biasness of the AI models and provide ethical governance. In healthcare, AI should be able to guarantee patient privacy, data safety, and transparent functionality to develop trust [19]. The idea of such a phenomenon as data provenance serves as the reminder of the fact that the quality and history of data utilized to train AI modelsdirectly affects its accuracy and safety. To make AI systems accurate, reliable, and safe, rigorous validation procedures are commonly required that include testing algorithms on massive datasets to avoid biases and provide interpretable and useful systems [20]. To conclude, although undergraduate nursing students are likely to be aware of the increasing role of AI in the healthcare sector, their levels of knowledge and attitudes can be both high and low. It is evident that more comprehensive and interdisciplinary education techniques are required to not only increase AI literacy but deal with ethical issues, alleviate anxiety, and equip them to effectively apply AI into clinical practice in the future [21]
Aim
The purpose of the proposed study is to determine the extent of knowledge and perception regarding the use of artificial intelligence (AI) in nursing among undergraduate nursing students in Mardan,Northeast of Pakistan.
Objectives
To identify how much the undergraduate nursing students know about artificial intelligence and its application in healthcare.
To identify the influence of the undergraduate nursing students on the application of artificial intelligence in healthcare practice.
To ascertain the perceived benefits and concerns related to the introduction of artificial intelligence in the healthcare industry among nursing students.
To examine the relationship between the degree of knowledge and the attitude to use artificial intelligence in healthcare.
To formulate the influence of demographic and educational factors (year of study, prior experience with AI, and training) on the knowledge and attitudes of students.
To generate evidence likely to support the introduction of the study of artificial intelligence in the undergraduate nursing programs in Mardan,Northeast of Pakistan.
MATERIALS AND METHODS
Study Design and Setting
It is a descriptive cross-sectional study done on the nursing colleges in Mardan,Northeastof Pakistan, over a span of four weeks. The study was based on the aim of assessing the levels of knowledge and attitudes of the undergraduate nursing students concerning the use of artificial intelligence (AI) in healthcare.
Study Population
The research sample consisted of undergraduate students pursuing the Bachelor of Science in Nursing (BScN) at selected nursing institutions in Mardan,Northeast of Pakistan. The post-RN BScN and the diploma nursing students were omitted to ensure that the academics are exposed and trained in a uniform manner.
Sample Size and Sampling Method
The present study was a descriptive cross-sectional study to determine the degree of knowledge and attitude towards artificial intelligence (AI) in healthcare among undergraduate nursing students. Any information that was to be determined or computed to calculate the required sample size was done by the means of the open-source epidemiological statistics calculator known as OpenEpi version 3.
Cochran’s sample size formula was used to compute the initial sample size of an infinite population (n0) as follows:

where: n0 is the estimate sample size (infinite population),p represents the estimated proportion of the population possessing the characteristic of interest, whileqis its complement (q = 1 – p). Since no prior estimate was available, we usedp= 0.5 andq= 0.5, which provide the maximum variability and therefore the most conservative sample size. Z is the Z-score at 95% confidence level equal to 1.96, andd is the margin of error set to 0.05.
Since the study population, which is 1,567 undergraduate Generic BSN students in Mardan district is finite (total population N = 1,567), the finite population correction (FPC) formula was used to calculate the adjusted sample size (n):

where: n is final adjusted estimate sample size and N is the total population size (1,567). Hence, 309 students were the minimum sample required.
In order toreduce non-response bias and missing questionnaires, all eligible and accessible undergraduate BSN students were contacted to take part. The number of students that answered the survey reached 310, which is sufficiently to justify the statistical sufficiency of the research.
Sampling Details
Thenon-probabilityconvenience sampling technique was usedbased onpracticality such as availability of the respondents, time factor and the research was exploratory.
Recruitment of Students
The sampling technique involved students who were selected in nursing colleges in Mardan,Northeast of Pakistanthat provided administrative support to the research. The process of recruitment was organized with the help of the faculty coordinators and class representatives, who sent all eligible students the survey link using official academic communication tools, such as WhatsApp groups, institutional email lists, and academic forums.
Contexts of Participation
Participationwas mainly through onlinemedium(Google Forms), through which the students could use their own time to fill the questionnaire. Also, there was information exchange on the study in the classroom and laboratory time when the faculty briefly described the purpose and procedures without imposing pressure on students to take part.
Voluntary Participation
The involvement was voluntary. Detailed information on the study including objectives of the study, procedures and the possible benefits was given to the students. They had signed the informed consent electronically before they could gain access to the questionnaire. Students were promised that either way of involvement (or non-involvement) would not in any way interfere with their academic assessment.The management of self-selection bias involves selecting cases evenly: the proportion of male to female cases will be equal.
Although convenience sampling carries a risk of self‑selection bias, several measures were employed to minimize this possibility.The offer to participate was sent to all eligible students without any regard to previous interest or knowledgeonAI. There were several reminders to help the students who may have otherwise chosen not to take part in the study, which increased the sample representativeness. The fact that the participants are represented by various colleges in theMardan district makes the study less prone to bias and more reliable in the findings.
Eligibility Criteria
Only the students who are currently pursuing the Generic BSN program were eligible to get included. Students of post-RN and diploma nurses were not included to make sure that the exposure and training were similar in academics. Students who refused to take part or even filled out the questionnaires were also not included in final analysis.
The convenience sampling can reduce the level of generalizability, but in this case of studying the institution on an exploratory basis, it was considered suitable. The success of having a sample that is equal and slightly greater than the required size and the inclusion of students representing various institutions increases the representativeness and the validity of the study results.
Data Collection Tool
Data collection was done through the structured and standardized questionnaire, which was based on the already published and verified studies of knowledge and attitudes toward artificial intelligence in healthcare[9]. Little local contextual modifications were made to fit the local academic context without tampering with the original validity of the content. The original tools were obtained, and the authors were approached and allowed to use the tool.
The questionnaire was separated into two:
Part I: Assessment of the application of artificial intelligence in healthcare (10 multiple choices)
Part II: Attitude about artificial intelligence application in healthcare (10 multiple choices).
All the items were dedicated to the main topics, applications, benefits, and concerns of artificialintelligence in health care facilities.
Data Collection Procedure
The questionnaire was created based on the survey translated into a questionnaire and posted online through the Google Forms platform and sent to the respondents through mobile applications. The participation had been done with informed consent that had been informed in the electronic form. The research was a voluntary one, and the respondents were free to abandon the research at any given time.
Ethical Considerations
The Institutional Review Board (IRB) approved of the study ethically. The participants were assured that their information, privacy, and anonymity were assured. They were informed that they were taking part in the research work voluntarily, and they could withdraw at any stage without any academic and personal consequences.
Statistical Analysis
The data were analyzed usingSPSSversion 26. All the variables were calculated to obtain the descriptive statistics. On the continuous variables (age, knowledge scores, attitude scores), we have computed mean, standard deviation (SD), median, interquartile range (IQR), minimum and maximum. Frequencies and percentages were used to present categorical variables (gender, year of study, college name).We checked thenormal distributionof knowledge and attitude scores with the help of the Shapiro-Wilk test The Shapiro-Wilk p-valueof both scoresweregreaterthan 0.05, which proves a normal distribution and meets the conditions of parametric tests.
The correlation coefficient employed to analyze the relationship between attitude scores and total knowledge scores was Pearson correlation coefficient. Linearity and the assumption of approximatenormality were verified and met.
Mean knowledge and attitude scores between male and female students were compared using independent samples t-test.
The one-way ANOVA was applied to analyze the data concerning the difference in the mean scores ofknowledgeand the attitude among four academic years. The choice of this test was due to the availability of the independent variable (academic year) with more than two levels. We checked the assumptions of homogeneity of variances and normality prior to the execution of the test.The Shapiro-Wilk test was used to determine normality and gave non-significant (p > 0.05) values in all the year groups, which indicated normally distributed data.The homogeneity of variances was tested with the Levene, which did not have a significant value (p > 0.05), and it proved that there were similar variances in groups.In the instances of overall ANOVA significance, post-hoc pairwise comparisons to control Type I error were then done usingTukeyHonestly Significant Difference (HSD) test.The attitude scores were predicted using simple linear regressionanalysisand knowledge as the predictor variable.Independent predictors of attitudinal scores were examined using multiple linear regression, with the covariates of the model being knowledge score, year of study, and gender. The enter method was used to input all the predictors at the same time.In the two regression analyses, the conditions of linearity, independence of residues, homoscedasticity and normality of residues were tested.These conditionswere satisfactorily achieved.Correlation and regression coefficients confidence intervals (95%) were also reported to estimate the precision.
The p-value(p)statistically significant was determined to beless than0.05 and all p-values were two-tailed.
RESULTS
Demographic Characteristics of the participants.
In this study, 310 undergraduate nursing students were involved in the study who were selected inthe nursingcolleges of Mardan. The average age of the participants was 20.56(SD =1.47)years with ages of 18-28 years(Table 1).
| Variable | Category | Frequency (n) | Percentage (%) |
| Age (years) | 17 | 5 | 1.6 |
| 19 | 97 | 31.3 | |
| 20 | 53 | 17.1 | |
| 21 | 64 | 20.6 | |
| 22 | 72 | 23.2 | |
| 23 | 10 | 3.2 | |
| 24 | 6 | 1.9 | |
| 25 | 2 | 0.6 | |
| 28 | 1 | 0.3 | |
| Gender | Male | 257 | 83 |
| Female | 53 | 17.1 | |
| Year of Study | 1st Year | 25 | 8 |
| 2nd Year | 138 | 44 | |
| 3rd Year | 100 | 31 | |
| 4th Year | 48 | 15 | |
| College Name | Matonia College of Nursing | 50 | 16 |
| Elizabeth Rani College of Nursing | 46 | 15 | |
| BKMC College of Nursing, Mardan | 41 | 13.2 | |
| Institute of Health Sciences | 39 | 12.6 | |
| Government College of Nursing, Mardan | 32 | 10.3 | |
| Oriental College of Nursing, Mardan | 31 | 10.0 | |
| Alfajar College of Nursing | 27 | 8.7 | |
| TPIHS | 23 | 7.4 | |
| Mardan Institute of Nursing | 11 | 3.5 | |
| Zia College of Nursing | 7 | 2.3 | |
| Kingsway Institute | 3 | 1.0 |
Table 1. Demographic Characteristics (N=310)
When it comes to gender distribution, most of the respondents were men (82.9%), and 17.1% were women. Regarding the academic year,the majority ofstudents were taking the second year (44.5%), the third year (32.3%), the fourth year (15.2%), and the first year (8.1%).Students who were undertaking the BSN program were invited to take part in the research. The Students Participate from these 11 different nursing colleges within the district of Mardan. MatoniaCollege of Nursing (16.1%), Elizabeth Rani College of Nursing (14.8%), BKMC College of Nursing,Mardan (13.2%), Instituteof Health Sciences (12.6%), and Government College of Nursing, Mardan (10.3%) made the highest percentage proportion of the students. The rest were participantsof the Oriental College of Nursing (10.0%), Alfajar College of Nursing (8.7%), TPIHS (7.4%), Mardan Institute of Nursing (3.5%), Zia College of Nursing (2.3%), and Kingsway Institute (1.0%).This sample is a wide representation of Mardan undergraduate nursing students.

Figure 1. Age of nursing students (N=310)
The Figure 1 shows the age distribution of 310 nursing studentsofcollege going in Northeast Pakistan in the age range between 17 to 28.The number of students who fall within the range of 19 to 22 years is 92 percent. The highest percentage is 19 -year-olds (31.3) and 22-year-olds (23.2) and 20-year-olds (17.1). Ages of 23, 24, 17, 25 and 28 are included in smaller groups. The average age is 20.6 years which is normal among undergraduates in the area.
Figure 2 illustrates the enrollment of four years of BScN program. The highest number is of the second-year students (44.5%), third (32.3%), fourth (15.5%), and first-year students (8.1%). Sixty-seven percent of the respondents are in the second and third year, and this provides a balanced picture of the education levels.

Figure 2. Students' year of study (N=310)

Figure 3. Names of Colleges (N=310)
The horizontal bar chart(Figure 3)enlists 11 colleges of nursing in Northeast Pakistan. The leading three ones are: Matonia College of Nursing (16.1%), Elizabeth Rani College of Nursing (14.8%), and BKMC College of Nursing, Mardan (13.2%), which constitute 44 percent of the sample. The others represented in these colleges are the Institute of Health Sciences, Government College of Nursing Mardan, Oriental College of Nursing, Alfajar College of Nursing, TPIHS, Mardan Institute of Nursing, Zia College of Nursing and the Kingsway Institute. The study has 11 collegesrepresentation,and this increases the regional credibility of the study.
Artificial Intelligence knowledge in Undergraduate Nursing students
This paper evaluated the attentiveness of the undergraduate nursing students on the topic of artificial intelligence (AI) in healthcare. All in all, the level of knowledge was good as the mean score of knowledge was 4.02(SD =0.58).
Most of the participants acknowledged that artificial intelligence can be utilized in healthcare and nursing practice. The majority of the students correctly defined the important concepts in AI, including the distinction between machine learning and deep learning is, and what one of the useful applications of AI is in healthcare. Also, the legal and privacy issues connected with the use of AI in healthcare were documented by many respondents.Another significant percentage of students reported that AI is able to access the required information regarding patients and their medical history. Moreover, the majority of participants were in support of the addition of basic AI concepts in the nursing curriculum.
These resultsshowthat undergraduate nursing specialists have sufficient knowledge andexperience of artificial intelligence in healthcare.
| Knowledge Items | Strongly Agree
n (%) |
Agree
n (%) |
Neutral
n (%) |
Disagree
n (%) |
Strongly Disagree n (%) |
| Artificial intelligence is a useful application in healthcare | 83 (26.77) | 105 (33.87) | 20 (6.45) | 9 (2.90) | 93 (30.00) |
| AI may raise legal issues in healthcare | 36 (11.61) | 114 (36.77) | 44 (14.19) | 21 (6.77) | 95 (30.65) |
| There is a difference between machine learning and deep learning | 75 (24.19) | 97 (31.29) | 38 (12.26) | 9 (2.90) | 91 (29.35) |
| Speech recognition or transcription is helpful in healthcare | 71 (22.90) | 116 (37.42) | 20 (6.45) | 9 (2.90) | 94 (30.32) |
| Serious privacy issues can occur with the use of AI in healthcare | 53 (17.10) | 106 (34.19) | 27 (8.71) | 30 (9.68) | 94 (30.32) |
| There are benefits of using artificial intelligence in nursing | 90 (29.03) | 94 (30.32) | 16 (5.16) | 16 (5.16) | 94 (30.32) |
| AI could be useful in healthcare | 80 (25.81) | 100 (32.26) | 23 (7.42) | 12 (3.87) | 95 (30.65) |
| AI can access patient medical history | 60 (19.35) | 108 (34.84) | 29 (9.35) | 18 (5.81) | 95 (30.65) |
| AI improves accuracy in healthcare decision-making | 78 (25.16) | 101 (32.58) | 24 (7.74) | 12 (3.87) | 95 (30.65) |
| AI will get all relevant information about a patient and medical history | 53 (17.10) | 106 (34.19) | 27 (8.71) | 30 (9.68) | 94 (30.32) |
Table 2. Question about knowledge (N=310).
The findings about respondents and their knowledge regarding the use of artificial intelligence (AI) in healthcare are provided in Table 2.Overall, the vast majority of participants agreed or strongly agreed with the statements and expressed a rather positive attitude towards the applications of artificial intelligence in healthcare and nursing.About 60 percent admitted that AI is helpful in the field of healthcare and enhances decision-making.Likewise,proportions saw the advantages of nursing and saw speech-recognition technology as beneficial.Numerous participants have also mentioned that AI can be used toimproveand help them manage clinical information.However, around 30% strongly disagreed with several of the items. This implies that some respondents have limited knowledge or are uncertain about what machine learning and deep learning are, as well as how AI is applied in retrieving patient information.
The ethical and legal issues mentioned by many respondents were privacy issues and the legal consequences of using AI in healthcare.Overall, the awareness of AI among the participants ismoderate to good, yet additional education and training are necessary to enhance the growth of knowledge and awareness among healthcare providers.
Artificial Intelligence attitude in Undergraduate Nursing students
The overall perception of the nursing students towards artificial intelligence was that it was not a bad idea since the average score of attitude was 3.72(SD =0.48).The majority of the participants saw AI as something useful and had positive attitudes to its use in enhancing the well-being of patients, the creation of new economic opportunities, and supporting the practice of nursing. Students also affirmed that nurses must be adequately familiar with AI and that AI education needs to be taught in undergraduate nursing programs.Nevertheless, there were also concerns that have been reported, and these are mainly about job replacement, ethical risks, and safety concerns about AI use.Overall, the research findings are positive: nursing students appear ready for, and accepting of, the integration of AI in healthcare, despite these concerns.
| Attitude Items | Strongly Agree
n (%) |
Agree
n (%) |
Neutral
n (%) |
Disagree
n (%) |
Strongly Disagree
n (%) |
| The future of artificial intelligence will be beneficial to the society. | 144 (46.5) | 142 (45.8) | 17 (5.5) | 3 (1.0) | 4 (1.3) |
| AI should be taught in the undergraduate nursing program | 55 (17.7) | 148 (47.7) | 12 (3.9) | 94 (30.3) | 1 (0.3) |
| Artificial intelligence is exciting | 151 (48.7) | 144 (46.5) | 10 (3.2) | 2 (0.6) | 3 (1.0) |
| AI can provide new economic opportunities | 150 (48.4) | 145 (46.8) | 6 (1.9) | 2 (0.6) | 7 (2.3) |
| AI has positive impacts on patients’ wellbeing | 154 (49.7) | 139 (44.8) | 9 (2.9) | 4 (1.3) | 4 (1.3) |
| Nurses should have good familiarity with AI | 155 (50.0) | 142 (45.8) | 6 (1.9) | 2 (0.6) | 5 (1.6) |
| AI is more dangerous than nuclear weapons | 66 (21.3) | 39 (12.6) | 6 (1.9) | 101 (32.6) | 98 (31.6) |
| AI can replace nurses at their jobs | 29 (9.4) | 19 (6.1) | 103 (33.2) | 22 (7.1) | 137 (44.2) |
| AI systems can perform better than humans | 29 (9.4) | 120 (38.7) | 14 (4.5) | 108 (34.8) | 39 (12.6) |
| There are drawbacks to using AI in nursing education | 70 (22.9) | 125 (40.8) | 111(35.0) | 2 (0.7) | 2 (0.7) |
Table 3. Questions about attitude (N=310).
Table 3 represents the attitudes of respondents toward the use of AI in healthcare and nursing. In general, the participants had such a positive opinion. A majority of them (92.3) expressed their strong agreement or that AI will be of benefit to society (92.3), exciting (95.2) as well as creating new economic opportunities (95.2). Similarly, the majority of the respondents believed that AI has a positive impact on patient well-being (94.5%), and nurses have to know it (95.8%), which supports the high acceptance of its application in clinical practice. Education wise, 65.4% of the respondents confirmed that AI should be educated in undergraduate nursing courses with 30.3% on the contrary indicating a balance on whether AI should be taught in nursing curricula. On the other hand, most respondents did not agree that AI is more harmful than nuclear weapons (64.2%), neither did they agree that AI would eliminate the nurses (51.3%). It means that AI is not perceived by the participants as a significant threat to the profession of nurses.Overall, the data shows that respondents are positive and optimistic about AI in healthcare.Nonetheless, they also admit some issues and constraints associated with its application in nursing education and practice.
Lenient Knowledge and Attitude Scores
The total mean score of interaction with the topic of artificial intelligence in healthcare in terms of knowledge was 4.02(SD =0.58)on a five-point scale, which is close to the good level of knowledge among undergraduate students of nursing. The total means of the attitude scale was 3.72 with a standard deviation of 0.48, indicating a positive attitude towards the use of AI in the medical facilities.
| Variable | Mean | SD | Median | Interquartile range | Min | Max |
| Knowledge Score | 4.02 | 0.58 | 4 | [3.6, 4.4] | 2.5 | 5 |
| Attitude Score | 3.72 | 0.48 | 3.7 | [3.4, 4.0] | 2.2 | 5 |
Table 4. Total Knowledge and Attitude.
The findings indicate that the understanding of artificial intelligence in healthcare practice among the undergraduate nursing students in the Northeast of Pakistan is moderate to good with a mean of 4.02 out of 5 as the knowledge score (SD = 0.58).The median value is 4.0 with an interquartile range of 3.6 to 4.4, which shows that most students have a median value between 4 and 4.6 with a score ranging between 2.5 and 5.0.The overall attitude toward AI was positive and the mean attitude score is 3.72 out of 5 (SD = 0.48). The median is 3.7 and the interquartile of the student views was 3.4 to4.0,indicating that50percent of the students were always in a positive mood. There was a range of attitude ratings of 2.2 to 5.0.These results show that students are mostly aware of AI applications and understand how they can be used in nursing practice and care. They are also accepting and ready to adopt AI in healthcare.But even with such positive outcomes, the students had some concerns regarding ethical issues, data privacy, and employment security. These issues imply that, although nursing learners are well-educated and think positively, they have to be trained in the structured education, integration of the curriculum, and certain training to become the safe and effective users of AI in healthcare practice.
Knowledge and Attitude Relationship
We estimated a Pearson correlation coefficient to investigate the relationshipbetween knowledge of AI in healthcare and students’ attitudes toward AI.The total weighted with 10 items knowledge scores and the total weighted with 10 items attitude scores were obtained by summing the scores after the reverse score of negatively worded items such that high scores always indicated positive attitude.
| Variable Pair | Correlation Coefficient (r) | 95% Confidence Interval | p-value |
| Total Knowledge Score & Total Attitude Score | 0.48 | [0.39, 0.56] | <0.001 |
Table 5. Correlation between: Knowledge scores and Attitude Scores.
Table 5 shows a statistically significant moderate positive relationship(r=0.48, 95%CI=[0.39, 0.56], p<0.001). Its coefficient of 0.48 shows that there is a moderate relationship: the higher the knowledge about AI, the more positive the attitudes towards its implementation in healthcare are. The confidence interval[0.39, 0.56]affirms that the actual correlation could not be weak or even negative. The p<0.001, which illustrates the fact that this outcome is not accidental.
Demographic and Educational Factor Impact
The mean difference among the knowledge and attitudes of the groups based on their years of study depends on the ANOVA.
| Year | Knowledge
Mean ± SD |
Attitude
Mean ± SD |
| 1st | 3.85 ± 0.60 | 3.58 ± 0.50 |
| 2nd | 4.00 ± 0.55 | 3.70 ± 0.48 |
| 3rd | 4.08 ± 0.59 | 3.75 ± 0.47 |
| 4th | 4.12 ± 0.57 | 3.80 ± 0.46 |
Table 6. Knowledge and Attitude Scores Academic Year (N=310).
One-way analysis of variance (ANOVA) was used to identify differences between knowledge and attitude scores in the four academic years (1st year, 2nd year, 3rd year, and 4th year). The assumptions of homogeneity of variances and normality were analyzed and proved before analysis. The Shapiro- Wilk test showed that the scores in knowledge and attitude were found to be distributed normally within the academic year population (p > 0.05 in all groups). The test of homogeneity of the variances of both knowledge scores (p = 0.68) and attitude scores (p = 0.72) by Levene was tested as homogeneous.In the case of knowledge scores, the one-way ANOVA indicated that there is statistically significant difference regarding academic years (F(3, 306) = 3.15, p = 0.026). Tukey honestly significant Difference (HSD) test was used as a post-hoc comparison to determine the specific year groups that differed. The findings showed that 4th year students scoredsignificantly higher (mean = 4.12,SD =0.57) than 1st year students (mean = 3.85,SD =0.60), with a mean difference of 0.27 (95%CI [0.03, 0.51], p = 0.032). Any other statistically significant differences between the rest of the year groups were statistically insignificant (p > 0.05 in all comparisons).Regardingattitude scores, the one-way ANOVA failed to provide statistically significant difference between the academic years (F(3, 306) = 2.12, p = 0.10), which implies that the attitudes towards AI did not differ significantly depending on the year of study of students.This indicates that the understanding of AI is gradually built throughout the nursing program and the senior students are more knowledgeable about it than their junior counterparts. Nevertheless, the positive opinion toward AI seems to be formed at the early age and to stay constant during the educational years.
Gender (Independent t-test) Knowledge and Attitudes
| Gender | Knowledge
Mean ± SD |
Attitude
Mean ± SD |
t statistic | p-value |
| Male | 4.03 ± 0.57 | 3.72 ± 0.48 | 0.45 | 0.65 |
| Female | 4.00 ± 0.61 | 3.71 ± 0.47 | 0.21 | 0.83 |
Table 7. Gender Knowledge and Attitude Scores (N=310).
Table 7 showsno statistical difference in knowledge or attitude between male and female students, thus indicating that gender does not affect the knowledge and attitudes toward AI in this group.
Predicting Attitudes on the Knowledge basis
In order to test the hypothesis of whether knowledge scores are predictors of attitudes towards AI, we conducted a simple linear regression. The regression was very strong (F(1, 308) = 92.16, p < 0.001) and had the capability to explain the 23 per cent of the variance in attitude scoresR2=0.23As can be seen in Table 8, the knowledge score had a significant positive predictor of attitude (β=0.48, 95% CI [0.38, 0.58], p < 0.001). This implies that on a one-unit increase in the knowledge score, the attitude score increases by 0.48 units. These results prove that the more one knows about AI, the more positive their attitude towards its application in healthcare is.
| Predictor | β | SE | t statistic | p-value | 95% CI for β |
| Total Knowledge Score | 0.48 | 0.05 | 9.60 | <0.001 | [0.38, 0.58] |
Note: R² = 0.23, F(1, 308) = 92.16, p < 0.001, SE=Standard Error
Table 8. Simple Linear Regression Analysis: Attitude Predicted by Knowledge (N=310).
Multivariate Regression Analysis
Multiple Regression (Knowledge + Year + Gender)
Note:R² = 0.26, F(3, 306) = 35.84, p < 0.001, SE=Standard Error
| Predictor | β | SE | t statistic | p-value | 95% CI for β |
| Total Knowledge Score | 0.47 | 0.05 | 9.4 | <0.001 | [0.37, 0.57] |
| Year of Study | 0.09 | 0.04 | 2.25 | 0.025 | [0.01, 0.17] |
| Gender (Male vs Female) | 0.02 | 0.06 | 0.33 | 0.741 | [-0.10, 0.14] |
Table 9. Multicollinear Regression Preparing Attitude (N=310)
A multiple linear regression was used to determine the predictive ability of knowledge score, year of study, and gender on attitudes toward AI. The model was found to be statistically significant (F(3, 306) = 35.84, p < 0.001) and explained 26 percent of the variance in the attitude scores (R 2 = 0.26).As presented in Table 9, the knowledge score was the best predictor ofattitude (β =0.47, 95%CI=[0.37, 0.57], p<0.001). Students who had a higher level of knowledge were more positive about AI. Year of study was also a strong positive predictor (β =0.09,95%CI= [0.01,0.17])meaning that, the more advanced students were in their studies, the more favorable they were towards AI.
There was no substantial contribution of gender (β =0.02, p=0.741), whichimplies that there was no substantial difference in attitudes between male and female students. All in all, the knowledgewas the most important determinant, and academic progression had a slight impact.
Critical Interpretation of the Results
In the research, it was discovered that the majority of undergraduate nursing students possessed a good knowledge base and a favorable perception of AI in healthcare. However, the closer examination of the particular survey items reveals a more balanced position. Students did not completely accept AI in all fields of practices. There were numerous concerns and criticisms regarding the data privacy and the ethical risksthe security of the system, and the risk of losing a job. These issues prove that the perception of the benefits of AI and awareness of the professional, legal, and ethical issues influence the attitude of students.
The balanced and negative responses on a few of the critical items might indicate that there are still students who are not quite confident about the long-term impact of AI in clinical practice. Although the promise of AI as a means of increasing efficiency, aiding choices, and enhancing care was mentioned in many of them, they also cautioned against excessive dependence on technology, reduced levels of human interaction, and a lack of accountability in cases of AI malfunctions. Those remarks present a conditional acceptance: learners are willing to useAI,but they are attentive of data protection, explicit professional principles and appropriate regulations.
Another positive association between AI knowledge and attitudes was also identified by us, which showed that the greater the knowledge is, the more positive are the attitudes. And the knowledge was not enough to ignore concerns. Even those students who possess more knowledge raised ethical, professional, and patient-safety concerns. Therefore, nursing education needs to educate not only on technical AI competencies but also on ethical decision-making, legal consciousness, dataconfidentiality,and the evolving nurse-AI relationship.
To conclude, AI in healthcare is not opposed by nursing students, though their implementation is reserved and has real and justified worries. The results recommend an extensive education, morerigorous ethics training, and enabling policies to ensure that AI is implemented in nursing practice safely, responsibly, and ethically.
DISCUSSION
The main goal of the research was to assess the levels of knowledge and attitudes ofundergraduate nursing studentsabout artificial intelligence (AI) in healthcare. The result shows that the students had a high level of knowledge (mean = 4.02, SD =0.58) and relatively positive attitudes (mean = 3.72, SD =0.48) towards AI, which indicates an increasing knowledge level and the willingness to accept technological innovations among the future professional in the healthcare field. These findings indicate a growing familiarity of nursing students withdigital health tools, AI applicantsand healthcare technologies,which might have contributed to their level of knowledge regarding the concepts of AI, such as machine learning, deep learning, clinical decision support, and data management [11,17].
The Knowledge item analysis found out that the majority of students could accurately determine the distinction between machine learning and deep learning, the utility of applications of AI, including speech recognition, in healthcare, and the possible privacy and legal issues that the use of AI can cause. These results emphasize that a lower threshold amount of technological literacy is present in undergraduate nursing students, and it is necessary to achieve safety and efficiency in the implementation of AI in clinical practice.
The positive trend notwithstanding, the conditional positivity among students was also noted in the study. Although a significant number of students reported positive impacts of AI, a significant percentage of them shared their apprehensions and uncertainty:
Job replacement: 44% disagreed with the statement that AI would not take nurses’ jobs, indicating a fear of being replaced as professionals.
Ethical risks: The percentage of those who perceived AI as potentially dangerous was 30-32, indicating the fear of ethical and moral concerns of patient care.
Privacy issues: 30 percent did not agree that AI is safe,which reveals that they are aware of potential threats to patient data and confidentiality
These results mean that knowledge is not a sufficient factor to influence the formation of positive attitudes since the issues of safety, ethics, and employment mediate acceptance of AI in healthcare. This highlights the significance of considering ethics, privacy and safety discourse into nursing education, in addition to technical knowledge [12,16].
The findings are in line with the previous studies across the globe. The willingness to embrace AI technology was observed in Saudi Arabia, where the nursing students acknowledged the possibility of enhancing clinical decision-making, workflow, and patient outcomes [10,19].Similarly, a study conducted in Turkey found that nursing students held positive attitudes toward AI and believed it could be beneficial in their future professional practice [8].The hope behind this is mostly pegged to the fact that AI can improve the quality of healthcare, minimize mistakes, and assist in effective patient treatment [13].
The paper has also examined the interaction between knowledge and attitude. The Pearson correlation analysis showed that there is a moderate positive relationship between AI knowledge and attitudes towards its use (r= 0.48, p < 0.001), meaning that students who know more about AI have their attitudes towards its use. Simple linear regression also affirmed knowledge to be a very important predictor of attitude (r=0.48, p < 0.001). Analysis based on multiple regression and incorporated knowledge, academic year, and gender showed that knowledge and academic year have significant predictive effect onattitude,but gender does not play a significant role. These results indicate that academic materials and clinical experiences can support positive attitudes in the long run, and structured education and curriculum planning play an important role in influencingthe attitude of students [11,17,19].
Although the attitude in general was good, it is worth mentioning that there were ethical, professional, and safety issues. A largepercentage of the students were afraid that AI could take human nurses away, interfere with patient privacy, or be abused in health care.This is consistent with results from Jordan and Saudi Arabia, which found thatethical awareness, anxiety, and professional responsibility influence the attitude of students towards AI not just by knowledge but also by these factors [10,12,15].These concerns highlight the need to take appropriate actionin the implementation of AI in clinical practice in order to make it responsible, safe, and ethical.
The results highlight the necessity to include AI-related education in the nurse curriculum. Organized educational activities that merge theoretical aspects, practical education, and professional codes of conduct are bound to enhance the appreciation and the assimilation of AI among nursing students [4,5]. The interactive learning methods, including project-based learning, simulation activities, and collaboration of AI projects, may improve the confidence and competence of the students using AI tools. The techniques can also enable students to acquire critical thinking, teamwork, and practical problem-solving skills, which would be vital in their effective operation at the AI-assisted healthcare sites [15,19].
In addition, the findings indicate the necessity of including ethical, legal, and professional obligations related to AI in healthcare in the curriculum. As a way to balance and critically imagine the uses of AI, educators can make students more aware of the threat of job displacement, data privacy, and AI misuse.Such training not only equips studentswith the aspects of practical implementation of AI, but also to train their ability to recognize issues,maintain a cautious approach, and use AI in a safe and responsible way [12,16].
Overall, the present study shows that undergraduate students of nursing in Mardan, Northeast of Pakistanpossess a fairly good knowledge base on AI and tend to have a positive attitude towards the use of AI in the healthcare sector, which is moderated by ethical, safety, and employment issues.The paper highlights the critical role of the organized AI education, practical learning, and training in ethics to make sure that upcoming nurses will be prepared to apply AI efficiently and responsibly. It is possible to introduce AI to the nursing curriculum along with hands-on and interactive learning opportunities that will enable students to embrace the changing nature of healthcare technology, enhance patient care, and improve clinical decision-making [11,12,16,17,19].
Methodological Limitations
This research has certain methodological drawbacks. To start with, the participants were chosen through convenience sampling. Although this method was feasible in this exploratory study, it does not allow generalizing the results tothe entire undergraduate nursing student populationin the region. Second, despite the fact that the questionnaire used in the present research was based on already published tools,the questionnaire’s reliability (e.g.,Cronbach’salpha)was not evaluated in this study.Also, there was no formal cultural validation or cross-cultural adaptation of the toolor a fulldescription and reference of the original tool. Lastly, the students who volunteered to be on the platform might not have the same knowledge or attitudes as those who declined to doso,and this may create a self-selection bias.Subsequent studies should apply probabilistic sampling techniques, and the instruments must be fully valid and culturally adapted to enhance the accuracy and generalizability of the results.
CONCLUSION
This study concludes that undergraduate nursing students in nursing colleges of Mardan, Northeast of Pakistanpossess a good level of knowledge and generally positive attitudes toward the use of artificial intelligence (AI) in healthcare. Students demonstrated awareness of AI applications, potential benefits, and its role in improving healthcare delivery and clinical decision-making.
However, important concerns were also identified, particularly related to ethical issues, dataprivacy, legal responsibility, and job security. These findings indicate that although students are open to adopting AI technologies, their acceptance is influenced by fears and uncertainties regarding the safe and responsible use of AI in clinical practice.
The results highlight the urgent need for structured educational support through curriculum integration, practical training, and ethical guidance. Preparing future nurses to work effectively with AI requires not only technical knowledge but also an understanding of legal, professional, and ethical responsibilities.
Overall, this study emphasizes the importance of incorporating AI-related education into undergraduate nursing programs to ensure that future nurses are competent, confident, and ethically prepared to engage with emerging healthcare technologies.
Recommendations
Based on the findings of this study, the following recommendations are proposed to support the effective and responsible integration of artificial intelligence (AI) into nursing education and practice:
Integration of AI into Nursing Curriculum
Nursing education programs should formally incorporate AI-related content into undergraduate curricula. This should include basic concepts of artificial intelligence, its applications in healthcare, and its role in clinical decision-making. Early exposure will help students develop familiarity and confidence in using emerging technologies.
Emphasis on Ethical and Legal Education
Given the concerns expressed by students regarding privacy, legal responsibility, and ethical risks, nursing programs should strengthen education on ethical, legal, and professional issues related to AI. Teaching should focus on data protection, patient confidentiality, accountability, and safetechnology use in clinical settings.
Practical and Skill-Based Training
Educational institutions should provide hands-on learning opportunities such as simulations, workshops, and project-based learning involving AI-supported tools. Practical exposure can reduce fear, improve understanding, and enhance students’ readiness to work in technology-enabled healthcare environments.
Faculty Development and Training
Nursing educators should receive training on AI and digital health technologies to ensure effective teaching and guidance. Faculty preparedness is essential for successful curriculum implementation and for fostering a supportive learning environment.
Awareness Programs to Address Misconceptions
Seminars and awareness sessions should be conducted to address common fears such as job replacement and misuse of AI. Emphasis should be placed on the collaborative role of AI, highlighting that AI is designed to support healthcare professionals rather than replace them.
Policy and Institutional Support
Healthcare institutions and nursing regulatory bodies should develop clear policies and guidelines regarding the use of AI in clinical practice. This will help ensure safe implementation and build trust among future nurses.
Future Research
Further studies should be conducted using larger and more diverse samples across different regionsto improve generalizability.
Future research may also explore the effectiveness of AI education programs and interventions designed to improve students’ competencies and attitudes.
Local Ethics Committee approval
The research was carried out in line with the internationally agreed ethical principles of conducting research that involves human subjects. Advance ethical approval was received before the data collection to safeguard the rights, safety and well-being of the participants. The study research plan was checked and accepted by the Institutional Review Board (IRB) of Abdul Wali Khan University, Mardan.
IRB Title: Institutional Review Board, Abdul Wali Khan University Mardan.
IRB Number: [IRB/2025/AI-Nursing/0017]
Date of Approval: [15 March 2025]
The study was completely voluntary. All the undergraduate nursing students were made aware of the objective of the research,the methodpossible advantages and their right to opt out of the research at any given time without any repercussions regarding their academic performance or personal effects. All the participants were informed and provided written consent before data were collected.
No personally identifiable information was gathered to guarantee the confidentiality and anonymity. The coding of the questionnaires was done numerically, and all data was kept in a secure location and accessed by the research team alone. Data gathered had no other purposes than academic and research.The research, further, did not impose any physical, psychological, or academic harm on the respondents. The issue- knowledge and attitudes towards artificial intelligence in healthcare-was not sensitive and the participants could pass on any question that they feel uncomfortable to respond to.
Competing interests
The authors report no conflict of interest.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not for profit sectors.
Authors' Contributions
The conceptualization and the study design was provided by Abdur Rahman and Muhammad Tariq. Ismail Shahid did the methodology development and design of the instruments. Data collection and field coordination was done by Khadija Bibi, Umair Islamand Mahnoor Ali. The data analysis and interpretation of results were done byRahim Shah, Arshad Ali, Noor Muhammad andShakir Ullah also managed the research, helped to refine the methodology, and provide the leadership of the manuscript writing, reviewing, and approval.
All authors approved the final version of the manuscript.
REFERENCES
- Naureen, M., Siddiqui (2025). Role of Artificial Intelligence in the perception of Health Care by Undergraduate Nursing Students: A Descriptive Cross-Ssectional Study. Nurse Education Today, 149, 106673.doi:doi.org/10.1016/j.nedt.2025.106673.
- Zhao Y, Yuan Y, Wen Z, Leng L, Shi L, Hu X, Wei X, Zuo M, Mou J, Luo Q, Chen M. The current status, knowledge, attitudes, and challenges of generative artificial intelligence use among undergraduate nursing students: a single-center cross-sectional survey of western China.doi:https://doi.org/10.3389/fpubh.2025.1648416
- Dawood BM, Abouelfettoh A, Zewiel MA, Perumal L, Alibrahim L, Boayesha A, Alaklabi H, Alrashed A, Alsuwaylih A, Alashoor E, Almutairi S. Artificial Intelligence Technology Integration in Healthcare: Al Ahsa Nursing Students’ Attitudes and Readiness. InNursing Forum 2025 (Vol. 2025, No. 1, p. 2848944).doi:Wiley.https://doi.org/10.1155/nuf/2848944
- Alatawi, F., & Kerari, A. (2025). Attitudes and Readiness to Adopt Artificial Intelligence among Nursing students in Saudi Arabia Cross-Sectional. J Multidisciplinary Healthcare, vol 18, pp 79077918.doi:doi.org/10.2147/jmdh.s567485.
- Kazanc, S., Kavak, H. K. and Karagozoglu, S. (2025). Individual innovativeness and the levels of medical artificial intelligence preparedness of the nursing students: a cross directional and correlational study. BMC Medical Education, 25(1).doi:doi.org/10.1186/s12909-025-07774-8.
- Varnosfaderani, S, Maleki, and Forouzanfar, M. (2024). Artificial Intelligence in Hospitals and Clinics: The Evolution of Healthcare in the 21 st Century by AI. 11(4), 337. doi: 10.3390/ bioengineering11040337.
- Ebrahimie, E., Mohammadi-Dehcheshmeh, M., Ebrahimi, M., and Petrovski, K. R. (2019). Such models play a crucial role in analyzing machine learning models that are used to predict the presence of sub-clinical mastitis: Deep Learning and Gradient-Boosted Trees outperform other models. Computers in Biology and Medicine, 114, 103456.doi: 10.1016/j.compbiomed.2019.103456
- Ebrahimi, A., Luo, S., & Chiong, R. (2021).Profound sequence modelling about immobilization of Alzheimer disease by MRI. Computers in Biology and Medicine, 134, 104537.doi: https://doi.org/10.1016/j.compbiomed.2021.104537.
- Nasir Manzoor, Altaf Hussain, Badil, Asghar Ali Zardari, Shahnaz, Zubair Ahmed, & Imtiazullah Khan. (2023). Assess Knowledge and Attitude Experience of Undergraduate Nursing Students regarding the position of Artificial Intelligence in Healthcare. Indus Journal of Bioscience Research, 3(5), 258-262. doi:10.70749/ijbr.v3i5.1131.
- Syed, L. H., Batool, Z., Hayder, Z. and Ali, S. (2025). Medical undergraduate students awareness and attitude of artificial intelligence: A developing country. BMC Medical Education, 25(1) doi.org/10.1186/s12909-025-07223-6.Sumengen, A. (2024). Attitudes and literacy of nursing students towards artificial intelligence: a cross-sectional survey. Teaching and Learning in Nursing 38 (2), 2024.
- Berse, S., Akca, K., Dirgar, E., & Agar, A. (2025). Early attitudes of Nursing Students towards the use of Artificial Intelligence and ChatGPT: An Exploratory study. 2018, International Journal of Nursing Practice, 31(6). doi:10.1111/ijn.70083.
- Labrague, L. J., Aguilar-Rosales, R., Yboa, B. C., Sabio, J. B., and de los Santos, J. A. (2023). The attitudes of student nurses to artificial intelligence (AI) technology in nursing practice, perceived use, and intention to use: cross-sectional study. Nurse education in practice, 73, 103815.doi:doi.org/10.1016/j.nepr.2023.103815.
- Bakarman, S. S., Al-shammari, A., and Aboshaiqah, A. (2025). Perceptions/preparations to Artificial Intelligence in Nursing Students in <scp>Saudi Arabia/scp/scp/. Nursing Open, 12(12).doi:https://doi.org/10.1002/nop2.70386.
- Ayed, A., Ejheisheh, M. A., Al-Amer, R., Aqtam, I., Ali, A. M., Othman, E. H., Farajallah, M., Qaddumi, J., and Batran, A. (2025). People have gained a new understanding of the connectionbetween anxiety and attitudes toward artificial intelligence in nursing students. BMC Nursing, 24(1).doi:https://doi.org/10.1186/s12912-025-03490-2
- Migdadi, M. K., Oweidat, I. A., Aloster, M. R., Al-Mughdeed, K., Saeed Alabdullah, A. A., and Farghaly Abdelaliem, S. M. (2024). Relation between artificial intelligence ethical awareness, attitudes, anxiety and intention to use artificial intelligence technology among nursing students. DIGITAL HEALTH, 10.doi:https://doi.org/10.1177/20552076241301958
- Ongun, P., Gul, B., Muslu, I. E., Mese, M. M. and Ergun, S. (2024). Identification of Artificial Intelligence Anxiety Status of Nursing Students: Cross-Sectional-Descriptive Study.Bandirma Onyedi Eylul Universitesi Saglik Bilimleri ve Arastirmalari Dergisi, 6(2), 304-312. doi: 10.46413/boneyusbad.1455856.
- Bahari, G., Alenazi, L., and Alkathiri, A. M. (25). Internationalisation of artificial intelligence in nursing education and its psychological effects on nursing students: Cross-sectional study. Nurse Education Today, 153, 106816.doi: https://doi.org/10.1016/ j.nedt.2025.106816.
- Aydin, G., Ozdemir, Kucukaydinoglu, Pallos, A., Coskun, E. Y. and Turan, N. (2025). The connection between innovation competencies and attitude among first-year nursing students to artificial intelligence: Multic centre study.doi: 10.1016/j.nepr.2025.104429 Nurse Education in Practice, 86, 104429.
- Kong, W., Ning, Y., Ma, T., and Song, F. and Mao, Y., Yang, C., Li, X., Guo, Y., Liu, H., Shi, J., and Liu, L. (2024). Undergraduate nursing student experience in artificial intelligence + project task driven learning at various stages: a qualitative study. BMC Nursing, 23(1).doi:https://doi.org/10.1186/s12912-024-01982-1
- Kin OK, Celik A. Medical artifical intelligence readiness status of nursing students and technostress level: A correlational study. Nurse Education in Practice. 2025 Oct 26:104611.doi:https://doi.org/10.1016/j.nepr.2025.104611
![]()
This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
Nurse-led intervention on knowledge and awareness regarding chronic kidney disease among hypertensive and/or diabetic patients: A quasi-experimental study
Jyoti Jangid 1, Manju AK Rajora 2*, Rajiv Narang 3, Viveka P Jyotsna 4
- Continuing Nursing Education Cell, All India Institute of Medical Sciences, Jodhpur, India.
- College of Nursing, All India Institute of Medical Sciences, New Delhi, India.
- Department of cardiology, All India Institute of Medical Sciences, New Delhi, India.
- Department of endocrinology and metabolism, All India Institute of Medical Sciences, New Delhi, India.
* Corresponding author: Dr. Manju Amit Kumar Rajora, address- College of Nursing, All India Institute of Medical Sciences, New Delhi-110029, India. Contact no.: +919870260036; Email: manjuakrajora@aiims.edu
Cite this article
ABSTRACT
Background: Diabetes and hypertension are the leading causes of chronic kidney disease (CKD) worldwide, and adequate awareness is crucial for its prevention and early detection among high-risk populations.
Objective: To evaluate the effectiveness of a nurse-led educational program through a booklet on the awareness and knowledge of CKD among hypertensive and/or diabetic patients.
Methods: A pre-test and post-test control group design was used with a convenient sample of 90 patients, equally divided into the experimental and control groups, i.e., 45 in each. Awareness-knowledge was assessed using a validated self-structured questionnaire. The pretest was conducted in both groups, and the experimental group received a 25–30-minute education intervention. Post-test assessment was conducted after one month in both groups.
Results: The mean pre-test knowledge scores of patients in the experimental and control groups were 18.04± 6.47 and 17.42± 6.37, respectively. In the post-test, there was a significant increase in the knowledge score of patients in the experimental group (33.96± 4.59) compared to the control group (18.80± 5.55; p=0.001). Awareness of CKD was significantly associated with religion (p = 0.016), monthly income (p = 0.02) and duration of diabetes (p value= 0.04). In regression analysis, being widow/separated and earning under 10,000 INR per month were independently associated to lower knowledge scores, while education beyond high school was an independent positive predictor.
Conclusion: Nurse-led educational programs effectively enhance CKD knowledge, support self-management, and help prevent disease-related complications among hypertensive and/or diabetic patients.
Keywords: Chronic kidney disease, Diabetes, Hypertension, Knowledge, Nurse-led educational program.
INTRODUCTION
Chronic kidney disease (CKD) is an irreversible, progressive condition and a major global health burden, affecting nearly 1 in 10 individuals [1,2]. In 2017, CKD caused 1.2 million deaths, ranking as the 12th leading cause of death worldwide, with projections indicating it may rise to the 5th position by 2040 [3]. Alarmingly, about 90% of adults with CKD and 1 in 3 adults with severe CKD remain unaware of their condition, leading to delayed diagnosis and treatment and also increasing the burden on caregivers with a decrease in the quality of life of patients [4,5]. A systematic review reported that the prevalence of poor kidney function varies widely from 2.9% to 56% and confirmed CKD varied from 4.4% to 17.1% [6]. Risk factors differ across regions. In developed countries, ageing, diabetes, hypertension, cardiovascular diseases and obesity predominates, whereas in developing countries, infections, glomerular and tubulointerstitial diseases, and exposure to drugs and toxins are common causes [7–9]. Diabetes Mellitus (DM) and Hypertension (HTN) are the main causes of CKD worldwide [10–13].
Hypertension acts both as a risk factor by accelerating CKD progression and as a comorbidity contributing to cardiovascular mortality in CKD patients [12,14,15]. In India, a pilot study reported 70% of patients having advanced CKD stage 4-5, and Diabetes being the most common CKD, out of which 97% of cases were having type 2 diabetes [13,16]. Low awareness among high-risk populations contributes significantly to delayed diagnosis and poor outcomes [17–19]. Therefore, early risk stratification, screening, awareness, and education are essential strategies to slow CKD progression [20–22]. The studies have reported low awareness and knowledge regarding CKD among the high-risk population [17,23,24]. Global initiatives such as the National Health and Nutrition Examination Surveys and Kidney Early Evaluation Program for CKD emphasize early detection [25,26]. Health education combined with early screening empowers high-risk individuals to adopt healthy behaviors and effective self-management practices [25,27,28].
Objective
The objective of the study was to assess the awareness and knowledge of CKD among hypertensive and/or diabetic patients and to assess the effectiveness of an education booklet on knowledge of CKD among hypertensive and/or diabetic patients.
MATERIAL AND METHODS
The research hypothesised that a nurse-led education program would bring significant change in the knowledge of CKD among hypertensive and/or diabetic patients. The non-equivalent control group pre-post-test quasi-experimental design was employed for participants. The non-random, time-based allocation was adopted as a part of a quasi-experimental study design to minimise contamination between groups. Participants attending the cardiology OPD on Monday and endocrinology OPD on Tuesday were assigned to the control group, whereas those attending the cardiology OPD on Friday and endocrinology OPD on Thursday were assigned in experimental group. The data was collected from July 2018 to December 2018. A sample size of 44 was calculated in each group, based on the pilot study results. 90 patients were enrolled (45 per group), assuming a 90% power, 5% alpha error, and 10% attrition. The pre-test was administered to the participants in both the control and the experimental group which required approximately 10-15 minutes to complete. Data collection included demographic and clinical variables. The awareness regarding CKD was assessed by asking two questions of a yes/no type. First question (AQ1) enquired whether the patients were aware of their risk of developing CKD due to HTN and DM or not. Second question (AQ2) enquired whether they were informed by any health professional or not. There were 43 questions regarding knowledge of CKD, out of which 35 were yes/no type, and 8 were multiple choice questions. Each correct response was scored as ‘1’, and each incorrect response was scored as ‘0’. Knowledge level was categorized into poor knowledge (<18), average knowledge (18-26), good knowledge (26-35), and very good knowledge (>35). Content Validity was established by three nursing experts and two nephrologists. Reliability of the tools was assessed using the test-retest method (r=0.79) during pilot study on similar population. The tool was translated into Hindi, and reverse translation was done in English.
Inclusion Criteria
The participants aged above 18 years, diagnosed with HTN and/or DM for ≥ 6 months and visiting the cardiology and endocrinology outpatient department (OPD) for regular follow-up at a tertiary care hospital.
Exclusion Criteria
The participants with cognitive impairment and renal disease were excluded from the study.
Intervention
A registered nurse pursuing her postgraduate degree in nursing developed the education booklet under the guidance of study guides and experts.
The education booklet included information regarding kidneys, its functions, about CKD, its risk factors, signs and symptoms, preventive measures for diabetic and/or hypertensive patients, diagnostic investigation for CKD, its complications and the management. The education was given once to the participants of experimental group visiting the cardiology OPD (Friday) and endocrinology OPD (Thursday) for 25-30 minutes.
The post-test was carried out one month after the intervention in both the control and the experimental group. There was no loss to follow up and the data of all 45 participants in both groups were analysed.
Figure 1 illustrates the data collection process, including participant enrolment, group allocation to final analysis.

Figure 1. Flowchart of participants.
Local Ethics Committee approval and consent to participate
The study was approved by the institute's ethics committee for postgraduate research, AIIMS, New Delhi, Ref. No. IECPG-98/21.03.2018, and the study was approved on March 21, 2018. Eligible patients were informed, and written informed consent was taken; they were reassured of their confidentiality and autonomy. This study was conducted in accordance with the Declaration of Helsinki.
Statistical Analysis
STATA 14.0 was used for statistical analysis. The normal distribution of data was assessed using the Shapiro-Wilk Test. The reliability of the tool was assessed using the test-retest method. The degree of stability over time was evaluated using Pearson’s correlation coefficient (r), r > 0.7 was considered as a good correlation. Categorical variables were analysed using the Chi-square test and Fisher's exact test. Continuous variables following a normal distribution were analysed by the t-test; an unpaired t-test was used to compare the data between the control and experimental group, while a paired t-test was used to compare pre-test vs post-test data within the groups. The Wilcoxon rank-sum test was used to analyse data which was not distributed normally. Anova and Kruskal-Walli’s rank test was used to assess the relationship of pre-test knowledge score with categorical variables, and Spearman’s correlation coefficient was used to investigate the potential relationship between pre-test knowledge score with clinical variables. Univariable and stepwise multiple linear regression for calculating unadjusted and adjusted beta coefficients with 95% class interval were performed to find the independent association factors of knowledge. Categorical variables were included using dummy coding where one category serving as the reference group and assigned a value 0 like marital status (reference: unmarried), geographical region (reference: rural), educational level (reference: no formal education) and monthly income (reference: ≥40,000 INR) while the other categories converted into binary dummy variable (1 if present, 0 if absent). The level of significance was at p-value < 0.05.
RESULTS
The data were checked for homogeneity and were found comparable (p>0.05). Table 1 reports the demographic and clinical variable distribution of patients among the experimental and control groups. More than half (64%) of patients in the experimental group and (67%) patients in the control group, were aware about the risk of developing kidney disease due to HTN and/or DM (AQ1) and only 42% in experimental group and 36% in the control group got informed by any health care professional about their risk of developing CKD (AQ2).
| Variables | Experimental Group (n=45) | Control Group (n=45) | p-value (test) |
| Age (years) Mean ± SD (Range) |
51.71±13.71 (24-78) | 51.84±11.51 (18-66) | 0.96 (U) |
| n (%) | |||
| Gender Male Female |
26 (58) 19 (42) |
26 (58) 19 (42) |
0.99 (C) |
| Marital status Unmarried Married |
3 (7) 42 (93) |
2 (4) 39 (95.5) |
0.99 (F) |
| Occupation Government Job Private Job Health Professional Unemployed |
10 (22) 20 (45) 1 (2) 14 (31) |
7 (16) 21 (47) 0 (0) 17 (38) |
0.7 (F) |
| Residence Rural Urban |
12 (27) 33 (73) |
9 (20) 36 (80) |
0.46 (C) |
| Education Informal Primary High school Above High school |
10 (22) 10 (22) 12 (27) 13 (29) |
10 (22) 12 (27) 16 (36) 7 (16) |
0.50 (C) |
| Source of health education Hospital Health Education Program Other |
23 (51) 4 (9) 18 (40) |
24 (53) 2 (4) 19 (42) |
0.80 (F) |
| Monthly income (Rs.) >40,000 30,000-40,000 20,000-30,000 10,000-20,000 <10,000 |
4 (9) 10 (22) 17 (38) 10 (22) 4 (9) |
2 (4) 8 (18) 17 (38) 14 (31) 4 (9) |
0.80 (F) |
| Albuminuria § Nil Trace >1 |
14(66.7) 3(14.3) 4(19.1) |
15(65.2) 7(30.4) 1(4.4) |
0.22 (F) |
| Clinical Variables | Median (Range) | ||
| Duration of diabetes | 6.5(1-25) | 7(1-30) | 0.72 (W) |
| Duration of hypertension | 6(1-25) | 5.5(1-35) | 0.74 (W) |
| Serum Creatinine(mg/dl) | 0.9 (0.5-2) | 0.8 (0.4-1.3) | 0.02 (U) |
| GFR (1.73ml/min/m2) | 86 (32-208) | 94 (41-218) | 0.12 (U) |
Note: § Albuminuria report of only 21 patients in the experimental group and 23 patients in the control group was available. U (Unpaired T-test), C (Chi-Square Test), F (Fisher’s Exact Test), W (Wilcoxon rank-sum Test)
Table 1. Distribution of demographic and clinical variables of patients of the experimental and control groups.
The knowledge level assessed at baseline showed that 44.4% patients in the experimental and 51.1% in control group had poor knowledge, 44.4% in the experimental and 37.7% in the control group had average knowledge, 9% patients in the experimental and 11% in the control group had good knowledge; however, only 2.2% patients in the experimental group had very good knowledge, and none in the control group had very good knowledge. Table 2 showed that at baseline, both groups were similar in knowledge level and the nurse-led education program was effective in improving knowledge of CKD among hypertensive and/or diabetic patients.
| Groups | Pre-test Score Mean± SD (Min-Max) |
Post-test Score Mean± SD (Min-Max) |
p-value (test) |
| Experimental group (n=45) | 18.04 ± 6.47 (4-35) | 33.96 ± 4.59 (21-43) | 0.001* (P) |
| Control group (n=45) | 17.42 ± 6.37 (3-27) | 18.80 ± 5.55 (9-30) | 0.0018* (P) |
| p-value | 0.65 (U) | 0.001* (U) |
Note: * (significant test), U (Unpaired T-test), P (Paired T-test).
Table 2. Comparison between the knowledge score of the experimental and control groups.
Table 3 shows that after the nurse-led educational program, in the post-test, the experimental groups showed a greater improvement in knowledge scores (diabetics p = 0.001, hypertensives p = 0.001, and hypertensive-diabetics p = 0.001) compared to the control group (diabetics p = 0.17, hypertensives p = 0.12, and hypertensive-diabetics p = 0.10), further emphasizing the effectiveness of the intervention even at the subgroup level.
| Knowledge score | Experimental group (n=45) | Control group (n=45) | ||
| Diabetic (n=15) | Pre-test score | 17.40±4.50 | 16.66±5.99 | |
| Post-test score | 33.80±2.95 | 18.13±4.43 | ||
| p-value (test) | 0.001* (P) | 0.17 (P) | ||
| Hypertensive (n=15) | Pre-test score | 18.66±6.87 | 16.93±7.45 | |
| Post-test score | 34.20±5.64 | 17.93±6.09 | ||
| p-value (test) | 0.001* (P) | 0.12 (P) | ||
| Diabetic and hypertensive (n=15) | Pre-test score | 18.06±7.95 | 18.66±5.77 | |
| Post-test score | 33.86±5.06 | 20.33±5.99 | ||
| p-value (test) | 0.001* (P) | 0.10 (P) | ||
Note: * (significant test), P (Paired T-test).
Table 3. Comparison of knowledge score between sub-groups of experimental and control group.
Table 4 reported the relationship between awareness and demographic variables. Patients with a higher monthly income (p = 0.02), Hindu by religion (p = 0.01), showed greater awareness of the risk of chronic kidney disease.
| Variables | AQ1 | AQ2 | |||||
| NO n(%) |
YES n(%) |
p-value (test) | NO n(%) |
YES n(%) |
p-value (test) | ||
| Age(years) | Mean ± SD | 55.35±12.38 | 49.89±12.39 | 0.05(U) | 53.40±12.56 | 49.22±12.39 | 0.12(U) |
| Gender | Male | 20 (64.5) | 32 (54.2) | 0.37(F) | 32 (58.2) | 20 (57.1) | 0.96 (F) |
| Female | 11 (35.5) | 27 (45.8) | 23 (41.8) | 15 (42.9) | |||
| Religion | Hindu | 29(93.6) | 46 (78) | 0.01* (F) | 47 (85.5) | 28 (80) | 0.39(F) |
| Muslim | 0 (0) | 10 (17) | 4 (7.3) | 6 (17.1) | |||
| Sikh | 2 (6.4) | 1(1.7) | 2 (3.6) | 1 (33.3) | |||
| Christian | 0 (0) | 2(3.4) | 2 (3.6) | 0 (0) | |||
| Marital status | Unmarried | 1 (3.2) | 4 (12.9) | 0.40(F) | 3 (5.4) | 2 (5.7) | 0.99(F) |
| Married | 25 (80.6) | 51 (86.4) | 46 (83.6) | 30 (85.7) | |||
| Widow/widowed | 1 (3.2) | 0 (0) | 1 (1.8) | 0 (0) | |||
| Separated | 4 (12.9) | 4 (12.9) | 5 (9.1) | 3 (8.6) | |||
| Occupation | Government Job | 6 (19.4) | 11(18.6) | 0.80(F) | 12 (21.8) | 5 (14.3) | 0.42(F) |
| Private Job | 16(51.6) | 25 (42.4) | 26 (47.3) | 15 (42.9) | |||
| Health Professional | 0 (0) | 1 (1.7) | 0 (0) | 1 (2.9) | |||
| Unemployed | 9 (29.0) | 22 (37.3) | 17 (30.9) | 14 (40) | |||
| Geographical region | Urban | 8 (25.8) | 13 (22) | 0.68(C) | 14 (25.5) | 7 (20) | 0.55(C) |
| Rural | 23 (74.2) | 46 (78) | 41 (74.5) | 28 (80) | |||
| Education | Informal Education | 9 (29.0) | 11 (35.5) | 0.07(F) | 12 (21.8) | 8 (22.9) | 0.52(F) |
| Primary Education | 11(35.5) | 11(35.5) | 13 (23.6) | 9 (25.7) | |||
| High school | 5 (16.1) | 23 (39) | 15(27.27) | 13 (37.1) | |||
| >High school | 6 (19.4) | 14 (23.7) | 15(27.27) | 5 (14.3) | |||
| Source of health education | Hospital | 17 (54.8) | 30 (50.9) | 0.93(F) | 26(47.27) | 21 (60) | 0.31(F) |
| Health Edu. Prog. | 2 (6.5) | 4 (6.8) | 3(5.45) | 3 (8.6) | |||
| Other (specify) | 12 (38.7) | 25 (42.4) | 26(47.27) | 11(31.4) | |||
| Monthly income(Rs.) | >40,000 | 1 (3.2) | 5 (8.5) | 0.02*(F) | 1(1.82) | 5 (14.3) | 0.05(F) |
| 30,000-40,000 | 5 (16.1) | 13 (22.0) | 12(21.82) | 6 (17.1) | |||
| 20,000-30,000 | 10 (32.3) | 24 (40.7) | 18(32.73) | 16 (45.7) | |||
| 10,000-20,000 | 8 (25.8) | 16 (27.1) | 17(30.91) | 7 (20) | |||
| <10,000 | 7 (22.6) | 1 (1.7) | 7(12.73) | 1 (2.9) | |||
Note: * (significant test), (U) t-test, (C) Chi square, (F) generalised Fisher’s Exact Test, (W) Wilcoxon test.
Table 4. Relationship between Awareness and Demographic Variables.
Table 5 reported the relationship between awareness and clinical variables and found that patients having diabetes for a longer period of time had higher awareness of CKD risk (p=0.04).
| Clinical Variables | AQ1 | AQ2 | |||||
| NO | YES | p-value | NO | YES | p-value (test) | ||
| Duration of diabetes (Median) | 4 | 8.5 | 0.04*(W) | 5.5 | 9.5 | 0.06(W) | |
| Duration of hypertension (Median) | 6 | 6 | 0.38(W) | 6 | 5 | 0.74(W) | |
| Albuminuria | Nil | 12 | 17 | 0.18 (F) | 19 | 10 | 0.46 (F) |
| Trace | 1 | 9 | 5 | 5 | |||
| >1 | 1 | 4 | 2 | 3 | |||
| Serum Creatinine(mg/dl) | 0.9 | 0.8 | 0.13(W) | 0.87 | 0.9 | 0.64(W) | |
| GFR (1.73ml/min/m2) | 86 | 95 | 0.18(U) | 0.90(U) | |||
Note: * (significant test), U (Unpaired t-test), C (Chi-square), F (generalised Fisher’s Exact Test), W (Wilcoxon test).
Table 5. Relationship between Awareness and Clinical Variables
Table 6 showed the relationships between demographic variables and knowledge score. Patients living in urban areas (p=0.03), unmarried (p=0.008), with more than high school education (p=0.0008), and a monthly income of 30-40 thousand rupees (p=0.01) had higher knowledge than others.
| Demographic Variables | Knowledge Score (Mean ± SD) | p-value (test) | |
| Gender Male Female |
17.76 ± 6.83 17.68 ± 5.82 |
0.95 (U) | |
| Religion Hindu Muslim |
17.45 ± 6.65 19.13 ± 4.82 |
0.35 (U) | |
| Marital status Unmarried Married Widow/widowed/Separated |
24.60 ± 3.20 17.76 ± 6.15 13.66 ± 6.83 |
0.008* (K) | |
| Occupation Government Job/Health Professional Private Job Unemployed |
19.44 ± 8.51 17.68 ± 6.02 16.80 ± 5.39 |
0.38 (A) | |
| Geographical region Rural Urban |
15.09 ± 6.96 18.53 ± 6.03 |
0.03* (U) | |
| Education Informal Education Primary Education High school >High school |
13.90 ± 4.96 16.18 ± 5.43 19.32 ± 5.35 21.05 ± 7.74 |
0.0008* (A) | |
| Source of health education Hospital Health Edu. Prog. Other (specify) |
17.10 ± 6.68 21.66 ± 5.04 17.89 ± 6.10 |
0.23 (K) | |
| Monthly income (INR) >40,000 30,000-40,000 20,000-30,000 10,000-20,000 <10,000 |
19.67 ± 9.69 20.77 ± 6.50 17.20 ± 5.79 17.79 ± 5.04 11.50 ± 5.90 |
0.01* (K) | |
| Albuminuria Nil Trace > +1 |
17.10 ± 4.95 19.50 ± 4.57 19.20 ± 9.17 |
0.47 (K) | |
Note: * (significant test), U (Unpaired T-test), A (Anova), K (Kruskal-Wallis rank test).
Table 6. Relationship of pre-test knowledge score with selected variables.
In Table 7, no correlation was found between knowledge and clinical variables (age, duration of diabetes, duration of hypertension, serum creatinine(mg/dl), and GFR (1.73ml/min/m2)).
| Clinical Variables | Spearman’s Coefficient (rho) | p-value (test) |
| knowledge / Age | -0.165 | 0.12 (S) |
| knowledge / Duration of diabetes | 0.049 | 0.70 (S) |
| knowledge / Duration of hypertension | 0.002 | 0.99 (S) |
| knowledge / Serum Creatinine(mg/dl) | -0.067 | 0.52 (S) |
| knowledge / GFR (1.73ml/min/m2) | 0.08 | 0.41 (S) |
Table 7. Correlation analysis between Knowledge score and Clinical Variables.
In Table 8, the variables that were statistically significant in bivariate analysis (Table 6) were included in univariable and multiple linear regression analysis. In the adjusted stepwise multiple linear regression model, being widowed/separated and having a monthly income of less than 10,000 INR remained independently associated with lower knowledge scores, while education beyond high school emerged as an independent positive predictor. Other variables did not retain statistical significance after adjustment. The results were interpreted as the knowledge among widowed/separated patients was less as compared to unmarried patients.
| Variables | Unadjusted beta coefficient with 95% CI | p-value | Step-wise linear regression | p-value |
| Marital status Married Widow/widowed/Separated |
-6.83 (-12.4, -1.2) -10.93 (-17.7, -4.2) |
0.018 0.002 |
-5.11 (-10.2, 0.04) -7.90 (-14.2, -1.6) |
0.05 0.015 |
| Residence Urban |
3.44 (0.3, 6.5) | 0.03 | ______ | _____ |
| Education Primary High school >High school |
2.28 (-1.3, 5.9) 5.42 (1.9, 8.8) 7.15 (3.4, 10.8) |
0.21 0.002 0.001 |
1.93 (-1.5, 5.4) 4.48 (1.2, 7.8) 6.06 (2.5, 9.6) |
0.26 0.008 0.001 |
| Monthly income 30,000-40,000 20,000-30,000 10,000-20,000 <10,000 |
1.11 (-4.5, 6.7) -2.46 (-7.8, 2.8) -1.87 (-7.3, 3.6) -8.16 (-14.6, -1.6) |
0.69 0.36 0.50 0.01 |
-0.44 (-5.6, 4.7) -3.06 (-7.9, 1.8) -2.20 (-7.2, 2.8) -7.79 (-13.7, -1.8) |
0.86 0.21 0.38 0.011 |
Table 8. Regression analysis of knowledge with selected variables.
A significant increase in knowledge was found in patients who had education up to high school and beyond high school, respectively, as compared to patients who had informal education. There was a significant decrease in knowledge score in patients who had a monthly income of less than 10,000 rupees compared to patients who had monthly income more than 40,000 rupees.
DISCUSSION
In the present study, 65.5% were aware of the risk of kidney disease in hypertensive and/or diabetic patients. Similarly, 60.6% respondents recognised diabetes as a risk factor for renal disease [29]. In the present study, 44.4% in the experimental and 51.1% in the control group had poor knowledge, 44.4% in the experimental and 37.7 in the control had average knowledge, 9% in experimental and 11.1% in control group had good knowledge, 2.2% in experimental and none in control had very good knowledge. Nearly the same, 55% of participants had average knowledge regarding renal disease [30]. In our study the knowledge score was significantly improved pre-test 18.04 ± 6.47 to post-test 33.96±4.59 at p=0.001in the experimental group similarly there was significant increase in knowledge of CKD was reported (p < 0.05) [31,32]. Knowledge was higher in unmarried subjects, living in an urban region, having an education up to or more than high school, and having a monthly income of more than 30,000 rupees. Similarly, patients with higher education had more knowledge of renal disease than those patients who had lower education (p=0.001) [10,24,34]. Patients having lower income <$ 2000 [Odds ratio (OR) 0.41, 95% class interval (CI)] and lower education (OR 0.33. 95% CI) had poor knowledge score of CKD [30,35].
The post-test was taken after one month of the intervention, rather than immediately, which could affect the novelty effect, causing a threat to external validity and no attrition at follow-up was a strength of the study.
Limitations
Awareness was assessed using two questions and most items in the knowledge questionnaire were closed-ended in nature and may overestimate the knowledge or limit the critical ability of critical reasoning related to kidney health.
The study didn’t evaluate the gain translated into sustained behavioural changes, treatment adherence, or improved clinical outcome. Additionally, the single-centre, quasi-experimental design with convenient sampling and lack of randomization may impact the external validity, limit the causal inference and generalizability.
CONCLUSION
In conclusion, the nurse-led intervention significantly improved the CKD knowledge score among hypertensive and/or diabetic patients. Appropriate information empowers hypertensive and/or diabetic patients to manage better blood pressure, blood sugar, and lifestyle changes, potentially reducing the risk and progression of kidney disease. Multicentric studies are needed, along with structured nurse-led education and counselling programs for these patients, and longitudinal research to comprehensively evaluate kidney health maintenance.
List of abbreviations
CKD: Chronic Kidney Disease
HTN: Hypertension
DM: Diabetes Mellitus
OPD: Outpatient Department
AQ1: Awareness Question 1
AQ2: Awareness Question 2
AIIMS: All India Institute of Medical Sciences
IECPG: Institute Ethics Committee for Postgraduate
STATA: Statistics and Data Analysis software
GFR: Glomerular Filtration Rate
OR: Odds Ratio
CI: Class Interval
Funding
The study was not funded by any public, private, commercial and non-profit sector.
Conflicts of interest
The authors declare that there is no conflict of interest.
Author contributions
Conceptualisation: JJ, MAKR, RN, VPJ, methodology: JJ, MAKR, RN, VPJ, Software: JJ, Data Collection: JJ, MAKR, RN, VPJ, Data analysis and interpretation: JJ, MAKR, writing- original draft preparation: JJ, MAKR, writing-review and editing: JJ, MAKR, supervision: MAKR, RN, VPN
Acknowledgement
We acknowledge the patient participation in the study and department of Biostatistics for statistical analysis.
REFERENCES
- National Kidney Foundation. Global facts about kidney disease. New York: National Kidney Foundation. (2015), [cited 2025 Sep 18]. Available from: https://www.kidney.org/kidneydisease/global-facts-about-kidney-disease
- Kidney Disease: Improving Global Outcomes (KDIGO) CKD-MBD Update Work Group. KDIGO 2017 Clinical Practice Guideline Update for the Diagnosis, Evaluation, Prevention, and Treatment of Chronic Kidney Disease-Mineral and Bone Disorder (CKD-MBD). Kidney Int Suppl (2011). 2017 Jul;7(1):1–59. doi: 10.1016/j.kisu.2017.04.001.
- Kovesdy CP. Epidemiology of chronic kidney disease: an update 2022. Kidney Int Suppl (2011). 2022 Apr [cited 2025 Sep 18];12(1):7–11. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9073222. doi: 10.1016/j.kisu.2021.11.003
- Centers for Disease Control and Prevention. Chronic Kidney Disease in the United States, 2023. Atlanta (GA): CDC; 2025 [cited 2025 Sep 18]. Available from: https://www.cdc.gov/kidney-disease/php/data-research/index.html
- Devraj R, Gordon EJ. Health literacy and kidney disease: toward a new line of research. Am J Kidney Dis. 2009 May;53(5):884–9. doi: 10.1053/j.ajkd.2008.12.028
- Korsa A, Tesfaye W, Sud K, Krass I, Castelino RL. Risk Factor-Based Screening for Early Detection of Chronic Kidney Disease in Primary Care Settings: A Systematic Review. Kidney Med. 2025 Apr 1 [cited 2025 Sep 24];7(4):100979. Available from: https://www.kidneymedicinejournal.org/article/S2590-0595(25)00015-9/fulltext. doi: 10.1016/j.xkme.2025.100979
- Levey AS, Coresh J. Chronic kidney disease. Lancet. 2012 Jan 14;379(9811):165–80. doi: 10.1016/S0140-6736(11)60178-5.
- Engelgau M, El-Saharty S, Kudesia P, Rajan V, Rosenhouse S, Okamoto K. Capitalizing on the Demographic Transition: Tackling Noncommunicable Diseases in South Asia. 2011.
- Abraham G, Varughese S, Thandavan T, Iyengar A, Fernando E, Naqvi SAJ, et al. Chronic kidney disease hotspots in developing countries in South Asia. Clin Kidney J. 2016 Feb;9(1):135–41. doi: 10.1093/ckj/sfv109
- Al-Qahtani M, Tawhari I, Alhmare AM, Badawi AS, Alsalem A, Gazzan MA, et al. The Awareness, Prevalence, and Risk Factors of Chronic Kidney Disease Among Diabetes Mellitus and Hypertensive Patients in the Aseer Region, Saudi Arabia. Cureus. 2024 Feb;16(2):e53366. doi: 10.7759/cureus.53366
- Bakris GL, Ritz E, Committee on behalf of the WKDS. The message for World Kidney Day 2009: hypertension and kidney disease – a marriage that should be prevented. Journal of Hypertension. 2009 Mar;27(3):666. doi: 10.1097/HJH.0b013e328327706a
- Wright J, Hutchison A. Cardiovascular disease in patients with chronic kidney disease. Vasc Health Risk Manag. 2009;5:713–22. doi: 10.2147/vhrm.s6206.
- Agarwal SK, Srivastava RK. Chronic Kidney Disease in India: Challenges and Solutions. Nephron Clinical Practice. 2009 Feb 5;111(3):c197–203. doi: 10.1159/000199460
- Golafshan F, Shafieyoon M. Hypertension and chronic kidney disease; a mutual relationship. J Renal Inj Prev. 2024 Apr 28 [cited 2025 Dec 26];13(3):e32277–e32277. Available from: https://journalrip.com/Article/jrip-32277. doi: 10.34172/jrip.2024.32277
- Ku E, Lee BJ, Wei J, Weir MR. Hypertension in CKD: Core Curriculum 2019. American Journal of Kidney Diseases. 2019 Jul 1 [cited 2025 Dec 26];74(1):120–31. Available from: https://www.ajkd.org/article/S0272-6386(19)30094-0/fulltext. doi: 10.1053/j.ajkd.2018.12.044
- Rodriguez-Poncelas A, Garre-Olmo J, Franch-Nadal J, Diez-Espino J, Mundet-Tuduri X, Barrot-De la Puente J, et al. Prevalence of chronic kidney disease in patients with type 2 diabetes in Spain: PERCEDIME2 study. BMC Nephrol. 2013 Feb 22;14:46. doi: 10.1186/1471-2369-14-46
- Lopez-Vargas PA, Tong A, Howell M, Phoon RK, Chadban SJ, Shen Y, et al. Patient awareness and beliefs about the risk factors and comorbidities associated with chronic kidney disease: A mixed-methods study. Nephrology (Carlton). 2017 May;22(5):374–81. doi: 10.1111/nep.12829.
- Ng CY, Lee ZS, Goh KS. Cross-sectional study on knowledge of chronic kidney disease among medical outpatient clinic patients. Med J Malaysia. 2016 Jun;71(3):99–104. PMID: 27495881
- Maya-Quinta R, Rodriguez-Gomez GP, Del Toro-Mijares R, Henriquez-Santos F, Martagon AJ. Chronic kidney disease acquired knowledge in a diabetic and hypertensive population using a translated and validated questionnaire. Ren Fail. 45(1):2222836. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC10274557. doi: 10.1080/0886022X.2023.2222836
- Kabinga SK, McLigeyo SO, Twahir A, Ndungu JN, Wangombe NN, Nyarera DK, et al. Risk factors for chronic kidney disease in the community: A decade of outreach in Kenya. Clinical Epidemiology and Global Health. 2024 Nov 1 [cited 2025 Oct 8];30:101823. Available from: https://www.sciencedirect.com/science/article/pii/S2213398424003208. doi: 10.1016/j.cegh.2024.101823
- Stanifer JW, Muiru A, Jafar TH, Patel UD. Chronic kidney disease in low- and middle-income countries. Nephrol Dial Transplant. 2016 Jun;31(6):868–74. doi: 10.1093/ndt/gfv466
- Kushner PR, Mende CW. Screening Programs for Early Detection of CKD: A Systematic Literature Review: SA-PO1073. Journal of the American Society of Nephrology. 2024 Oct [cited 2025 Dec 26];35(10S):10.1681/ASN.2024xahc4h8y. Available from: https://journals.lww.com/jasn/fulltext/2024/10001/screening_programs_for_early_detection_of_ckd__a.3815.aspx. doi: 10.1681/ASN.2024xahc4h8y
- Oluyombo R, Ayodele OE, Akinwusi PO, Okunola OO, Gbadegesin BA, Soje MO, et al. Awareness, knowledge and perception of chronic kidney disease in a rural community of South-West Nigeria. Niger J Clin Pract. 2016;19(2):161–9. doi: 10.4103/1119-3077.175960.
- Younes S, Mourad N, Safwan J, Dabbous M, Rahal M, Al Nabulsi M, et al. Chronic kidney disease awareness among the general population: tool validation and knowledge assessment in a developing country. BMC Nephrology. 2022 Jul 26 [cited 2025 Sep 18];23(1):266. doi: 10.1186/s12882-022-02889-2
- Chu CD, Chen MH, McCulloch CE, Powe NR, Estrella MM, Shlipak MG, et al. Patient Awareness of CKD: A Systematic Review and Meta-analysis of Patient-Oriented Questions and Study Setting. Kidney Med. 2021 Jun 1 [cited 2025 Sep 18];3(4):576-585.e1. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC8350814. doi: 10.1016/j.xkme.2021.03.014
- Zelnick LR, Weiss NS, Kestenbaum BR, Robinson-Cohen C, Heagerty PJ, Tuttle K, et al. Diabetes and CKD in the United States Population, 2009-2014. Clin J Am Soc Nephrol. 2017 Dec 7;12(12):1984–90. doi: 10.2215/CJN.03700417
- Francis A, Harhay MN, Ong ACM, Tummalapalli SL, Ortiz A, Fogo AB, et al. Chronic kidney disease and the global public health agenda: an international consensus. Nat Rev Nephrol. 2024 Jul [cited 2025 Sep 18];20(7):473–85. Available from: https://www.nature.com/articles/s41581-024-00820-6. doi: 10.1038/s41581-024-00820-6
- Narva AS, Norton JM, Boulware LE. Educating Patients about CKD: The Path to Self-Management and Patient-Centered Care. Clin J Am Soc Nephrol. 2016 Apr 7;11(4):694–703. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4822666. doi: 10.2215/CJN.07680715
- Gheewala PA, Peterson GM, Zaidi STR, Jose MD, Castelino RL. Public knowledge of chronic kidney disease evaluated using a validated questionnaire: a cross-sectional study. BMC Public Health. 2018 Mar 20;18(1):371. Available from: https://doi.org/10.1186/s12889-018-5301-4. doi: 10.1186/s12889-018-5301-4
- Chow WL, Joshi VD, Tin AS, van der Erf S, Lim JFY, Swah TS, et al. Limited knowledge of chronic kidney disease among primary care patients – a cross-sectional survey. BMC Nephrology. 2012 Jul 2;13(1):54. Available from: https://doi.org/10.1186/1471-2369-13-54. doi: 10.1186/1471-2369-13-54
- Danguilan R, Cabanayan-Casasola C, Evangelista N, Pelobello M, Equipado C, Lucio-Tong M, et al. An education and counseling program for chronic kidney disease: strategies to improve patient knowledge. Kidney International Supplements. 2013 May 1;3:215–8. doi: 10.1038/kisup.2013.17
- Shobha KR, Sams LM, Arulappan J, Alharbi HF. Effectiveness of Nurse-Led Educational Intervention on Knowledge Regarding Management of Chronic Kidney Disease among Patients. International Journal of Nutrition, Pharmacology, Neurological Diseases. 2023 Mar [cited 2025 Dec 26];13(1):47. Available from: https://journals.lww.com/ijnp/fulltext/2023/03000/effectiveness_of_nurse_led_educational.8.aspx. doi: 10.4103/ijnpnd.ijnpnd_68_22
- Assiry A, Alshahrani S, Banji D, Banji OJF, Syed NK, Alqahtani SS. Public Awareness of Chronic Kidney Disease in Jazan Province, Saudi Arabia—A Cross-Sectional Survey. Healthcare (Basel). 2022 Jul 25 [cited 2025 Dec 26];10(8):1377. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC9330694. doi: 10.3390/healthcare10081377
- Hussain S, Habib A, Najmi AK, Hussain S, Habib A, Najmi AK. Limited Knowledge of Chronic Kidney Disease among Type 2 Diabetes Mellitus Patients in India. International Journal of Environmental Research and Public Health. 2019 Apr 23 [cited 2025 Dec 26];16(8). Available from: https://www.mdpi.com/1660-4601/16/8/1443. doi: 10.3390/ijerph16081443.
![]()
This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
LOCAL EXPERIENCE OF COORDINATION IN ROBOTIC SURGERY: ORGANIZATIONAL REFLECTIONS
Rita Citarella 1*, Marco Abagnale 2
- Department of Surgery and Anesthesia, “Umberto I” Hospital of Nocera Inferiore, 84014, Salerno, Italy.
- Department of Critical Care, M. Scarlato Hospital, 84018, Scafati, Salerno, Italy.
* Corresponding author: Rita Citarella, Department of Surgery and Anesthesia at Umberto I Hospital of Nocera Inferiore, 84014 Salerno, Italy. E-mail: rita.citarella.91@gmail.com
Cite this article
ABSTRACT
Introduction: The launch of the robotic surgery program in our hospital showed that the main challenges did not concern the technology itself but rather the organization of work. Delays in operating room preparation, unclear task distribution, fragmented communication among professionals, and inconsistent management of instrument traceability highlighted the absence of a clearly defined coordination function.
Methods: Through descriptive observations drawn from daily activity during the initial phases of the program, operational episodes, team dynamics, and workflow patterns were recorded in order to understand how the system adapted to the introduction of the robotic platform.
Results: From these observations, the figure of the “Da Vinci Coordinator” (DVC) emerged locally as a practical response to organizational challenges. This function contributed to aligning tasks among teams, making workflow preparation more predictable, improving interprofessional communication, and supporting internal training activities. The few descriptive indicators included served solely to contextualize the experience.
Conclusion: The DVC function was not conceived as a formalized or generalizable professional role, but rather as an emergent organizational adaptation useful during the implementation phase of a robotic program. The considerations presented may offer insights for other centers preparing to introduce robotic surgery; however, further structured studies will be necessary to assess its transferability to different contexts.
Keywords: Robotic surgery; perioperative coordination; organisational role; instrument traceability; Team integration; Da Vinci system
INTRODUCTION
Robotic surgery is increasingly used to support minimally invasive procedures, with well‑documented advantages in precision, patient safety, length of stay, and postoperative recovery [1–5]. In January 2025, the Umberto I Hospital of Nocera Inferiore introduced the Da Vinci system within the ASL Salerno network. Although robotic platforms are typically associated with technological benefits, our early implementation phase highlighted challenges of a different nature: the most recurrent difficulties were organizational rather than technical. During the first weeks, we observed delays in operating room start times, unclear task allocation during system preparation, fragmented communication among surgical, anesthesiology, nursing, and technical staff, and inconsistent procedures for instrument traceability and expiry control. The lack of a standardized monitoring protocol also resulted in occasions where robotic instruments exceeded their prescribed service life without timely identification, creating risks of unavailability or malfunction [6]. These observations underscored a key insight: in the start‑up phase of a robotic program, patient safety and workflow stability depend not only on technology or surgical skill, but also on a clearly defined coordination function capable of integrating clinical, technical, and organizational activities across the perioperative pathway [7]. To address these gaps, our center introduced the Da Vinci Coordinator (DVC), conceptualized as a coordination function rather than a formal professional role and assigned to an experienced operating room nurse trained on the robotic system. The role emerged as a practical response to early challenges and was maintained as staff increasingly recognized its value for workflow predictability, interprofessional communication, and training support.
Objective
The purpose of this commentary is to explain why this coordination function became necessary during the early implementation phase, to describe its main activities, and to reflect on how this experience may support other centers preparing to introduce robotic surgery.
Rationale behind the introduction of the Da Vinci Coordinator
During the first weeks of using the robotic system, our local experience revealed a recurrent organizational need that may be relevant for other centres starting a robotic programme [8]. In response, the hospital established a multidisciplinary working group including surgeons, anesthesiologists, and operating room nurses to review early operational episodes and identify practical priorities. These discussions motivated the introduction of the Da Vinci Coordinator (DVC), assigned in our unit to a single operating room nurse with advanced competencies and specific training on the robotic system and its instruments. Initially introduced as a pragmatic solution to early‑stage challenges, the DVC function was subsequently maintained as staff perceived clear benefits in workflow predictability, standardization of preparation, and interprofessional collaboration elements that are critical for supporting safe, patient‑centered care during the start‑up of a robotic program. In our setting, the essential activities observed included (Figure 1):

Figure 1. Key competence that may have the Da Vinci Coordinator.
(1) Technical supervision of system readiness and troubleshooting; (2) Organizational coordination to align workflow and responsibilities; (3) Interprofessional training supporting the team’s learning process. These activities reflect a context‑dependent coordination function rather than a formal professional standard, illustrating how dedicated coordination mechanisms may be essential during early robotic implementation. In our setting, the DVC was conceptualized as a distinct coordination function compared with the standard operating room nurse [9].
Clinical, technical, and organizational skills (locally observed)
In the context of our start-up phase, the DVC role integrated clinical competencies (procedure-specific patient positioning), technical competencies (system readiness verification, troubleshooting and escalation pathways, instrument traceability, and management of usage life and expiry), and organizational competencies (workflow preparation, clarification of professional roles, facilitation of multidisciplinary communication, and provision of training support). These competencies are presented as context-dependent observations derived from a single-center implementation phase and do not constitute a formally codified professional standard (Table 1).
| Aspect | Traditional OR Nurse [10] | Da Vinci Coordinator (DVC) [Fig. 2] |
| Role focus | Intraoperative assistance | Coordination across the robotic surgical pathway |
| Competence | Primarily clinical intraoperative skills | Integrated clinical, technical, and organizational skills |
| Instrument management | Basic instrument control | Traceability, usage-life checks, system readiness verification |
| Team interaction | Interaction with surgeons, anesthesiologists, OR nurses and technical/support staff) | Cross-team communication among the same professional groups |
| Training role | Limited or none | Support to onboarding and standardized setup routines |
| Responsibility procedure-based | Focused on the current procedure | Coordination of preparation and workflow across sessions (context-dependent) |
Table 1. Preliminary, locally observed functional comparison between the traditional OR nurse role and the coordination function referred to as “Da Vinci Coordinator (DVC)” in our setting.
Core skills and tasks of the Da Vinci Coordinator (locally observed)
In our setting, the DVC combines clinical, technical, and organisational support (Table 1; Figure 2). Rather than providing a procedural checklist, we summarise the DVC contribution as a coordination function across perioperative phases, aimed at reducing variability and making interdependencies manageable during the start-up period.
Across phases, three recurrent coordination mechanisms were observed:
- Before surgery: aligning timing and responsibilities; verifying instrument readiness and traceability/usage-life; ensuring basic system readiness.
- During surgery (setup/docking): facilitating bidirectional communication among teams; supporting standardised setup routines; coordinating escalation when technical or workflow disruptions occur.
- After surgery updating traceability records; capturing causes of start-time deviations when present; enabling rapid readiness for subsequent sessions and brief feedback for iterative learning.
These activities are reported as context-dependent observations from a single-centre implementation phase and are not proposed as a formal professional standard.
The Da Vinci Coordinator clinical insights: minimum indicators
To contextualise this local experience, we report a small set of descriptive observations from the start‑up phase (March–November 2025; 75 procedures). These elements are not intended as an assessment of effectiveness but solely to frame the coordination perspective discussed in this commentary
- Instrument governance: no episodes of instruments exceeding service life or requiring unplanned traceability checks.
- Start‑time predictability: two delays of 15 minutes, both linked to lower scrub‑nurse familiarity with robotic instrumentation.
- Team coordination: clearer role allocation, more reliable communication, faster instrument retrieval, and better adaptability to workflow changes.
- Training: three full days of standardized training for the dedicated robotic nursing team.
Together, these elements suggest that coordination activities may contribute to improving workflow stability during early implementation (Figure 2).

Figure 2. Descriptive representation of coordination interfaces in our setting: not a codified organizational model
Coordinating activities across perioperative phases (locally observed)
- Before surgery (preoperative / pre-session), the following activities should be undertaken: verification of the planned robotic procedure requirements; confirmation of instrument availability, remaining usage-life/expiry, and updating of instrument traceability; coordination of instrument retrieval from multiple storage locations (operating room supply, pharmacy); confirmation of the patient positioning strategy and required positioning accessories; performance and/or coordination of system readiness checks (surgeon console, patient cart, vision cart); and alignment of timing, team roles, and setup responsibilities through a structured pre-session briefing and/or checklist.
- During surgery (setup, docking, intraoperative support), key responsibilities include: facilitation of real-time, bidirectional communication among surgical, anesthetic, nursing, and technical personnel; support of standardized setup and docking protocols; management of unanticipated requirements (e.g., rapid instrument retrieval, instrument substitutions, or workflow modifications); escalation and coordination of technical troubleshooting to minimize procedural interruptions; and support of rapid adaptation when novel techniques or intraoperative changes necessitate modifications in patient positioning or workflow organization.
- After surgery (post-session), the following measures should be completed: documentation of instrument utilization and corresponding updates to traceability records, including notation of any device- or process-related issues; recording of start-time deviations and their underlying causes, when applicable; planning and coordination of restocking for all consumed or opened materials to ensure readiness for subsequent procedures; and systematic capture of concise feedback and lessons learned to promote continuous quality improvement during the implementation and maturation of the robotic surgery program.
Taking care of the patient
The initial phase of robotic surgical is when the DVC collaborates with surgeons, anesthesiologists, and operating room nursing staff to conduct a comprehensive preoperative evaluation and systematically coordinate the patient’s subsequent surgical pathway [10]: reducing uncertainty, aligning roles, and preventing delays during the initiation phase of robotic surgery.[11]; As a Da Vinci Coordinator, taking care of the patient means ensuring safety, precision, and comfort at every stage of robotic surgery. This is managed through simple operational tools: a pre-session readiness checklist (system check, instrument availability/usage-life/expiry, positioning plan) [12], a short team briefing to align roles and timing, and an instrument traceability log updated at the end of each session; when issues are identified, they are communicated through structured alerts to the appropriate t contacts [13].
Future directions
Our experience suggests that a robotic surgery program can run better when there is a simple and clear way to coordinate the work. However, our data come from one center only (March–November 2025, 75 procedures), so we propose only realistic and small improvements.
Based on what we observed (instrument control, start-time delays, communication, and training needs), we suggest four practical directions:
- Add coordination to routine session planning. Include the DVC in weekly or monthly planning of robotic sessions, instrument availability checks, and short pre-session readiness steps. Use simple checklists/logs to document key actions without creating extra bureaucracy.
- Create training focused on start-up problems. Develop short training modules based on real issues seen during early use (instrument checks and traceability, standardized setup, communication during docking, and adaptation to new procedures). Test these modules locally or within regional networks.
- Use basic digital tools to support instrument governance. Start with simple digital tracking (alerts for usage limits/expiry, replacement planning, and a basic delay log). Consider advanced analytics after data collection becomes stable and reliable.
- State the role clearly and define its limits. The DVC is not a ward/unit coordinator and does not manage staffing or overall department organization. The DVC is a procedure-focused coordination function, limited to the robotic pathway (pre-session preparation, setup support, instrument governance, communication, and training support). Clear boundaries help avoid overlap and confusion.
Overall, this commentary does not propose a standardized professional model. It offers a practical coordination perspective and a small set of process measures that other centers can use when starting a robotic program.
DISCUSSION
Our early implementation experience showed that the main sources of variability and delay were not related to the robotic technology itself, but to gaps in coordination and governance. Introducing a dedicated coordination function made these interdependencies visible and manageable across teams and phases. From this experience, three practical lessons emerged:
- the need to define early “who does what” and establish clear instrument governance;
- the value of brief, structured communication routines during setup;
- the importance of training focused on the most frequent start‑up challenges, including setup routines, instrument management, and communication during preparation and docking.
These observations are consistent with the literature showing that robotic implementation requires not only technological investment but also structured coordination, communication, and workflow standardisation [8, 11–13]. Reports on robotic nurse specialists or perioperative robotic coordinators also suggest that responsibilities vary across centres and that no single standard model exists [8, 11–13]. Our commentary adds to this literature by offering a practical “coordination lens” for the start-up phase and a small set of feasible process indicators that can support reflection and future evaluation. Describing the DVC as a function (not a fixed job title) allows each hospital to adapt it to its own context and to choose a few simple measures to monitor progress.
Limitations
This commentary is based on a single‑centre start‑up experience and does not aim to demonstrate effectiveness. The indicators reported are minimal and primarily process‑based, and several observations remain qualitative and may reflect local perceptions. Data were not collected through a predefined structured protocol, and the absence of a formal comparative evaluation limits interpretability. Findings may also be influenced by learning curves, case mix, and team experience or turnover. For these reasons, the DVC should be interpreted as a context‑dependent coordination function intended to stimulate reflection rather than a validated or universally generalizable model.
CONCLUSION
Introducing robotic surgery requires not only technology and technical skills but also clear coordination work. Describing the DVC as a practical coordination function, rather than a fixed job title, allows each hospital to adapt it to its own organizational structure and to monitor a few simple process indicators to assess whether daily work is becoming more stable as the robotic program evolves.
Local Ethics Committee approval
Not applicable. This is a commentary reporting only aggregated, non-identifiable process information; no patient-level data were collected.
Conflict of interest
The authors report no conflict of interest.
Funding
No specific funding was received for this work.
Authors’ contribution
RC and MA were the only two contributors in writing the manuscript. RC and MA discussed the importance of the Da Vinci Coordinator role during a work meeting and decided to report and discuss this local coordination experience. Both authors contributed equally to the conception and writing of the manuscript.
REFERENCES
- MacLean L, Hersh AM, Bhimreddy M, Jiang K, Davidar AD, Weber-Levine C, Alomari S, Judy BF, Lubelski D, Theodore N. Comparison of accuracy, revision, and perioperative outcomes in robot-assisted spine surgeries: systematic review and meta-analysis. J Neurosurg Spine. 2024 Jul 5;41(4):519-531. doi: 10.3171/2024.4. SPINE23917. PMID: 38968628.
- Asadizeidabadi, S. Hosseini, F. Vetshev, S. Osminin, S. Hosseini. Comparison of da Vinci 5 with previous versions of da Vinci and Sina: a review. Laparosc Endosc Robot Surg, 7 (2) (2024), pp. 60-65. doi:10.1016/j.lers.2024.04.006
- Yang GZ, Cambias J, Cleary K, Daimler E, Drake J, Dupont PE, Hata N, Kazanzides P, Martel S, Patel RV, Santos VJ, Taylor RH. Medical robotics-Regulatory, ethical, and legal considerations for increasing levels of autonomy. Sci Robot. 2017 Mar 15;2(4): eaam8638. doi: 10.1126/scirobotics. aam8638. Epub 2017 Mar 15. PMID: 33157870.
- Autorino R, Zargar H, Kaouk JH. Robotic-assisted laparoscopic surgery: recent advances in urology. Fertil Steril. 2014 Oct;102(4):939-49. doi: 10.1016/j.fertnstert.2014.05.033. Epub 2014 Jun 30. PMID: 24993800.
- Aggarwal R, Winter Beatty J, Kinross J, von Roon A, Darzi A, Purkayastha S. Initial Experience With a New Robotic Surgical System for Cholecystectomy. Surg Innov. 2020 Apr;27(2):136-142. doi: 10.1177/1553350619890736. Epub 2019 Nov 27. PMID: 31771424.
- Kolev N. Comparative Analysis of Results Between Robot-Assisted and Open Radical Prostatectomy. Journal of Biomedical and Clinical Research 2019; 12(2): 157-doi:10.2478/jbcr-2019-0023
- Yang GZ, Cambias J, Cleary K, Daimler E, Drake J, Dupont PE, Hata N, Kazanzides P, Martel S, Patel RV, Santos VJ, Taylor RH. Medical robotics-Regulatory, ethical, and legal considerations for increasing levels of autonomy. Sci Robot. 2017 Mar 15;2(4): eaam8638. doi: 10.1126/scirobotics. aam8638. Epub 2017 Mar 15. PMID: 33157870.
- Møller L, Hertz P, Grande U, Aukdal J, Fredensborg B, Kristensen H, Petersson J, Konge L, Bjerrum F. Identifying curriculum content for operating room nurses involved in robotic-assisted surgery: a Delphi study. Surg Endosc. 2023 Apr;37(4):2729-2748. doi: 10.1007/s00464-022-09751-4. Epub 2022 Dec 5. PMID: 36471061.
- Kang MJ, De Gagne JC, Kang HS. Perioperative Nurses' Work Experience With Robotic Surgery: A Focus Group Study. Comput Inform Nurs. 2016 Apr;34(4):152-8. doi: 10.1097/CIN.0000000000000224. PMID: 26848644.
- Patel VR. Essential elements to the establishment and design of a successful robotic surgery programme. Int J Med Robot. 2006 Mar;2(1):28-35. doi: 10.1002/rcs.77. PMID: 17520611.
- Randell R, Honey S, Hindmarsh J, Alvarado N, Greenhalgh J, Pearman A, Long A, Cope A, Gill A, Gardner P, Kotze A, Wilkinson D, Jayne D, Croft J, Dowding D. A realist process evaluation of robot-assisted surgery: integration into routine practice and impacts on communication, collaboration and decision-making. Southampton (UK): NIHR Journals Library; 2017 Jun. PMID: 28813131. doi: 10.3310/hsdr05200
- Ahmed K, Khan R, Mottrie A, Lovegrove C, Abaza R, Ahlawat R, Ahlering T, Ahlgren G, Artibani W, Barret E, Cathelineau X, Challacombe B, Coloby P, Khan MS, Hubert J, Michel MS, Montorsi F, Murphy D, Palou J, Patel V, Piechaud PT, Van Poppel H, Rischmann P, Sanchez-Salas R, Siemer S, Stoeckle M, Stolzenburg JU, Terrier JE, Thüroff JW, Vaessen C, Van Der Poel HG, Van Cleynenbreugel B, Volpe A, Wagner C, Wiklund P, Wilson T, Wirth M, Witt J, Dasgupta P. Development of a standardised training curriculum for robotic surgery: a consensus statement from an international multidisciplinary group of experts. BJU Int. 2015 Jul;116(1):93-101. doi: 10.1111/bju.12974. Epub 2015 Mar 23. PMID: 25359658.
- Fisher RA, Dasgupta P, Mottrie A, Volpe A, Khan MS, Challacombe B, Ahmed K. An over-view of robot assisted surgery curricula and the status of their validation. Int J Surg. 2015 Jan;13:115-123. doi: 10.1016/j. ijsu.2014.11.033. Epub 2014 Dec 6. PMID: 25486264.
![]() This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
Competencies of Nursing Tutors in Clinical Training: A Nationwide Italian Survey Protocol
Gian Domenico Giusti 1,2,*, Alessio Gili 3, Stefano Bambi 4, Yari Longobucco 4, Rocco Mazzotta 2,5
- Education and Quality Unit, Bachelor’s Degree Program in Nursing, Perugia University Hospital, Perugia, Italy
- Department of Biomedicine and Prevention, University of Tor Vergata, Rome, Italy.
- Department of Life Sciences, Health and Health Professions, Link Campus University Rome, Italy.
- Department of Health Sciences, University of Florence, Florence, Italy.
- Center of Excellence for Nursing Culture and Research, Order of Nursing Professions of Rome, Italy.
*Corresponding author: Gian Domenico, Giusti, Department of Biomedicine and Prevention, University of Tor Vergata, Rome, Italy. E-mail: giandomenico.giusti@students.uniroma2.eu ORCID: https://orcid.org/0000-0001-9167-9845
Cite this article
ABSTRACT
Introduction: Clinical mentoring is essential for nursing education. It facilitates the integration of theory and practice, while promoting the development of clinical, communication, and interpersonal skills. It is becoming increasingly evident that tutors are facing a number of challenges. These challenges are related to the cultural diversity of students and constantly evolving clinical contexts. Despite the emphasis placed on the significance of general and cultural competencies in mentors within the context of international literature, a paucity of studies in Italy exists that evaluate both dimensions employing standardised and validated tools.
Objective: This protocol describes a nationwide survey that will assess the mentoring and cultural competencies of Italian nursing tutors.
Methods: The study adopts a descriptive cross-sectional observational design, with convenience sampling of approximately 600 tutors active in the academic year 2024–2025. The collection of data will be conducted between July and December 2025 through the utilisation of digital questionnaires. The survey employs two instruments, namely the Mentors' Competence Instrument (MCI) and the Mentors' Cultural Competence Instrument (MCCI), in order to assess these competencies. The MCI has been developed to measure tutors' general skills, including pedagogical, relational and feedback dimensions, while the MCCI has been developed to assess cultural skills and intercultural communication. The collection of sociodemographic data, contextual information and open-ended responses pertaining to the strengths and weaknesses of the tutorial role will also be undertaken. Statistical procedures will include descriptive analyses, using tables and plots to represent the data, as well as inferential analyses such as the Chi-square test, t-test, ANOVA test, Mann–Whitney U test, Kruskal–Wallis test, and correlation analysis. All statistical tests with p < 0.05 will be considered statistically significant.
Results: The results of the study will inform the development of targeted training interventions and organisational strategies to enhance the role of the clinical tutor.
Conclusions: The survey will contribute to the enhancement of mentoring quality and the professional development of tutors, thereby facilitating the strengthening of the effectiveness of clinical training programmes in Italy.
Keywords: mentoring, nursing tutor, cultural skills, survey, clinical training.
INTRODUCTION
Clinical mentoring is a fundamental pillar of nursing education. It guides students in integrating theory and practice, while also promoting the development of clinical, communication, and interpersonal skills [1]. Changes in healthcare contexts and the increasing cultural and linguistic diversity of students mean that the role of the tutor is becoming more complex and important [2]. International literature shows that effective tutoring improves student satisfaction, reduces anxiety, and contributes to patient safety [3]. Furthermore, Directive 2013/55/EU [4] stipulates that at least 50% of nursing training must take place in clinical settings, thereby expanding the responsibilities of tutors and necessitating their adequate preparation.
In recent years, research has further defined the multidimensional nature of the skills required of tutors [5]. Pramila-Savukoski et al. [6] have emphasised that these skills encompass pedagogical, organisational, and professional elements. In this context, the Mentors' Competence Instrument (MCI), which was developed and validated by Tuomikoski et al. [7], is a standardised self-assessment tool that is widely used to evaluate the general abilities of nursing tutors. This evaluation covers areas such as pedagogical knowledge, relationships between mentors and students, providing feedback, and assessing students. Added to this is cultural competence, which is essential in supporting students from different backgrounds. Luukkonen et al.'s [8] study showed that, despite having moderate levels of cultural awareness, tutors demonstrate gaps in their practical interaction skills and cultural confidence, with variability related to age, experience, and the frequency with which they deliver tutorials.
A key contribution to this field is the work of Oikarainen et al. [9], who developed and validated the Mentors’ Cultural Competence Instrument (MCCI). This is now considered one of the most comprehensive tools for measuring the cultural competence of tutors. Meanwhile, Giusti and Mazzotta [10] emphasised the pivotal role of tutors in fostering cultural competence among nursing students and facilitating the establishment of inclusive clinical environments.
Further evidence at the European level comes from a multicentre study by Mikkonen et al. [11], which identified three distinct profiles of tutorial competence among over 1,600 mentors from five European countries. The study showed that professional experience, specific training, and the frequency with which mentors undertake tutoring activities are correlated with higher levels of competence. Italian mentors, however, scored lower in several areas, including providing constructive feedback, adopting a goal-oriented approach to mentoring, and engaging in critical reflection [11], these results suggest the need for dedicated training programmes in an Italian context. Meanwhile, a recent systematic review by Keinänen et al. [12] confirmed that educational interventions aimed at tutors can significantly improve skills such as student assessment, providing feedback, setting goals, and developing professional self-efficacy. The analysed interventions, which were often based on blended methods, demonstrated consistent and significant improvements in various dimensions of tutorial competence over time [12].
In nursing education literature, the term mentor is often used interchangeably with other roles such as facilitator, peer instructor, preceptor, clinical guide, clinical instructor, or supervisor [7]. In this context, a mentor can be defined as a registered nurse who supports undergraduate nursing students in their learning process and is responsible for teaching and assessing students during clinical practice, without being an employee of the educational institution. Mentoring takes place within the clinical learning environment, which encompasses not only the physical setting but also psychosocial and interactional factors, organisational culture, and teaching and learning components that can strongly influence students’ learning experiences.
In the Italian context, these mentoring functions are often carried out within tutoring activities, reflecting a partial overlap between the roles of mentor and tutor in clinical education.
However, the national literature shows that there are not many studies that look at the general and cultural skills of Italian nursing tutors using standard tools like the MCI and MCCI.
Objective
The aim of this protocol is to address this gap by conducting a national survey using the MCI and MCCI questionnaires.
MATERIALS AND METHODS
Study design
The study adopts a descriptive cross-sectional observational design, based on the administration of a survey aimed at nurses who act as clinical tutors in Nursing Degree Courses in Italy, active in the academic year 2024–2025. The collection of data is scheduled to take place between July and December 2025. The study was registered on the OSF platform [13].
The cross-sectional design was selected to provide a comprehensive overview of the general and cultural competencies of nursing tutors within the context of university education, offering a representative sample of the prevailing circumstances at the time of the survey. This approach aligns with the established guidelines for conducting and reporting observational studies and surveys in the healthcare sector [14,15].
Population and sample
The target population of the study consists of nurses who have provided clinical tutoring for students enrolled in nursing degree programmes during the 2024–2025 academic year. These nurses are employed within healthcare facilities and universities that are affiliated with the training programmes.
Convenience sampling was employed due to the unavailability of a reliable estimate of the total number of nurse tutors at the national level. The use of random sampling was not feasible due to the absence of a national registry or comprehensive database of nurse tutors in Italy, as well as the heterogeneity of the tutor role across institutions.
Participants will be recruited through institutional and professional channels, including nursing degree programme coordinators, internship coordinators, and professional nursing networks, in accordance with the methodology of descriptive surveys in nursing [16].
Given the descriptive and non-probabilistic nature of the study, a formal sample size calculation was not performed. The target sample size of approximately 600 participants was defined pragmatically, with the aim of achieving broad national coverage and ensuring sufficient variability for descriptive and exploratory analyses, as is recommended for descriptive studies not intended for hypothesis testing [15,16].
The study will include nurses who have been employed as clinical tutors during the 2024–2025 academic year. Individuals in managerial roles, those who have been absent for extended periods (e.g., due to illness or pregnancy), and those who have experienced a demotion or downgrade in their professional positions are excluded from this study.
No minimum duration of tutoring experience or formal tutor training was required for inclusion, as the study aims to reflect the heterogeneity of tutoring practices in the Italian clinical education context. Tutor training and professional experience were collected as study variables rather than used as exclusion criteria.
Survey instruments
The questionnaire is composed of three sequential sections.
Preliminary section:
The first section collects socio-demographic and professional information about the respondents. Specifically, the following variables will be collected: age, gender, highest educational qualification, years of professional nursing experience, years of experience in clinical tutoring, current clinical setting, geographical region, prior formal training as a tutor (yes/no), and formal recognition of the tutoring role within the workplace (yes/no). This information will be used to describe the sample and to explore potential associations with mentoring competencies.
Mentors’ Competence Instrument (MCI)
The second section consists of the Mentors’ Competence Instrument (MCI), developed by Tuomikoski et al. [7] and validated in the Italian context [17], based on the 7-factor model. The instrument includes 63 items distributed across seven domains: (1) mentoring practices, (2) mentor characteristics, (3) mentor motivation, (4) goal-oriented mentoring, (5) reflection during mentoring, (6) student-centred evaluation, and (7) constructive feedback and assessment. Items are rated on a 4-point Likert scale ranging from “strongly disagree” to “strongly agree,” with higher scores indicating higher perceived mentoring competence.
The Italian version of the MCI has demonstrated good psychometric properties, with satisfactory construct validity and internal consistency, reporting Cronbach’s alpha values ranging approximately from 0.76 to 0.90 across domains [7].
Mentors’ Cultural Competence Instrument (MCCI):
The third section includes the Mentors’ Cultural Competence Instrument (MCCI), developed and validated by Oikarainen et al. [9], developed to assess cultural competence in mentoring culturally and linguistically diverse nursing students. The instrument comprises 13 items organised into domains addressing cultural awareness, cultural sensitivity, intercultural communication, and linguistic diversity. Responses are measured using a 4-point Likert scale (“strongly disagree” to “strongly agree”), with higher scores reflecting higher perceived cultural competence.
The Italian version of the MCCI has shown acceptable validity and reliability, with evidence of construct validity and good internal consistency across domains.
Bringing MCI and MCCI together will provide a complete and detailed understanding of the tutor's role. This will include both the usual teaching skills and those that are growing in the area of cultural diversity. The original authors of the instruments authorised the researchers to use the instruments on 22/05/2025.
The survey will also comprise three optional open-ended questions with optional answers, inviting respondents to describe the role of the tutor and the strengths and weaknesses of current nursing students.
Data collection procedures
The administration of the questionnaires will be conducted digitally, utilising the Microsoft Form™ platform (Microsoft Corp., Redmond, WA, USA) [18]. The data collection period is scheduled to occur between September and December 2025. The survey will be distributed using a combination of methods: a direct web link disseminated through Nursing Degree Programme Coordinators and internship coordinators at participating universities, and QR codes shared during educational and professional training events targeting nursing tutors.To minimise the risk of unauthorised access or duplicate responses, the survey platform will implement IP address tracking, allowing only one submission per device. Participation will be anonymous, and no personally identifiable information will be collected. A system of periodic reminders will be employed to enhance response rates. Reminder messages will be sent at fortnightly intervals throughout the data collection period. Data confidentiality will be ensured through secure data management procedures. All collected data will be stored exclusively on a password-protected external hard drive, with encrypted access enabled via the BitLocker security system of Windows 10® (Microsoft Corporation, WA, USA). Data will be accessible only to the research team and will be handled in accordance with applicable data protection regulations.
Data analysis
The survey data will be entered into a Microsoft Excel™ 2019 spreadsheet (Microsoft Corp., Redmond, WA, USA) and quality checked by a researcher to ensure accuracy. All responses remain anonymous. The questionnaire will not identify participants. Upon reaching the target sample size or by 31 December 2025, the data will be exported to Excel™ and subsequently analysed using SPSS™ software, version 27 [19]. The statistical analysis will follow a progressive approach: initially, descriptive statistics will be calculated, such as frequencies and percentages for categorical variables, means and standard deviations or medians and interquartile ranges for continuous variables, after verifying the distribution of the data using normality tests.
Inferential analyses will include Chi-square tests to assess associations between categorical variables. For continuous variables, data distribution will be assessed using tests of normality. Parametric tests (t-test or ANOVA) will be applied to normally distributed variables, while non-parametric alternatives (Mann–Whitney U test or Kruskal–Wallis test) will be used when normality assumptions are not met. The level of statistical significance will be set at p < 0.05.
In addition, correlation analyses will be performed to explore associations between continuous competence scores (overall and domain-specific scores of the Mentors’ Competence Instrument and the Mentors’ Cultural Competence Instrument) and selected socio-demographic and professional variables, such as age, years of professional experience, years of tutoring experience, and prior tutor training. Pearson’s correlation coefficient will be used for normally distributed continuous variables, while Spearman’s rank correlation coefficient will be applied for non-normally distributed or ordinal variables. These analyses will be exploratory in nature.
Responses to the open-ended questions will be analysed using a qualitative thematic analysis approach. The analysis will involve familiarisation with the textual data, inductive coding, and the identification of recurring patterns and themes. The qualitative results will be used to complement the quantitative findings and provide a deeper understanding of tutors’ perceptions regarding their role and the strengths and weaknesses of nursing students.
Ethical considerations
The study will be conducted in full compliance with the principles of the Declaration of Helsinki. All participants will receive comprehensive information regarding the objectives and methodologies of the research and will be able to provide their free and informed consent. Participation is voluntary and anonymous: no personal data or information that could directly or indirectly identify participants will be collected. The data shall be used exclusively for scientific research purposes and shall be processed in accordance with Italian law, Legislative Decree No. 196 of 30 June 2003, “Personal Data Protection Code” [20], updated with the new Legislative Decree No. 101/2018 [21], which adapts Italian legislation to the European privacy regulation (EU Reg. No. 679/2016, GDPR) [22]. The study was approved by the Regional Ethics Committee of the Umbria Region on June 18, 2025 (Prot. No. CE-2376/25).
RESULTS
Reporting results
The presentation of results will adhere to the guidelines of the CHERRIES checklist [23], the CROSS Checklist [24] and the recommendations published by Latour and Tume [25], ensuring consistency, transparency and completeness in survey reporting and compliance with international best practices for the description of questionnaire-based studies.
Expected outcomes
The survey is expected to provide a clear and detailed description of the current mentoring and cultural competence profiles of Italian nursing tutors, based on domain-specific scores obtained from validated instruments. The integration of the MCI and MCCI will facilitate the delineation of an overall profile of the clinical tutor, emphasising their strengths and areas for improvement, as well as identifying potential disparities associated with the socio-demographic and professional characteristics of the participants. The data collected will also facilitate the exploratory identification of associations and correlations between mentoring and cultural competence scores and selected socio-demographic and professional variables. The study is expected to provide valuable information to guide institutional strategies for enhancing the role of tutors and improving the quality of clinical training programmes.
LIMITATIONS AND STRENGTHS
Limitations
The study is subject to certain inherent limitations, which are intrinsic to the adopted methodological framework. The utilisation of convenience sampling has the potential to compromise the representativeness of the sample with respect to the national population of nursing tutors. Furthermore, the utilisation of self-assessment tools carries with it the risk of bias, as participants may overestimate or underestimate their own skills. Finally, voluntary participation may favour responses from individuals who are more motivated or sensitive to the topic, thus introducing the possibility of a self-selection bias.
Strengths
A significant strength of the study is the utilisation of two internationally validated instruments, which ensure the reliability and comparability of the data collected. The magnitude of the sample in question serves to enhance the robustness of the statistical analyses conducted, thereby facilitating the identification of potential associations between the various variables under consideration. The content explored is of particular significance for improving mentoring practices and enhancing the role of the clinical tutor, due to its relevance to training needs and organisational policies in the field of nursing education.
CONCLUSION
The present protocol delineates a national survey designed to evaluate the general and cultural competencies of nursing tutors through the MCI and MCCI. The anticipated outcomes of this study are expected to provide valuable insights that will inform the development of training programmes, the enhancement of the quality of clinical placements, and the strengthening of the role of tutors in nursing education.
Author contributions
Conceptualization: G.D.G.
Methodology: G.D.G.; A.G.
Writing—original draft preparation: G.D.G.; Y.L.; S.B.; R.M.
Writing—review and editing: G.D.G.; Y.L.; S.B.;
Supervision: S.B.; Y.L.; R.M.
Ethics statement
The study will be conducted in full compliance with the principles of the Declaration of Helsinki. The study was approved by the Regional Ethics Committee of the Umbria Region on 18/06/2025 (Prot. No. CE-2376/25).
Conflicts of interest
The authors declare no conflicts of interest.
Funding sources
This research received no external funding
Declaration on the use of ai
We used ChatGPT and DeepL.com to assist with English language refinement and grammar checking. No AI was used for interpretation, or scientific content generation.
Data availability statement
Data sharing is not applicable to this article as no datasets were generated or analysed during the current study.
Acknowledgment
We would like to thank the Research Unit of Nursing Science and Health Management and the Educational Research Group at the University of Oulu, Finland, for authorising us to use their search tools (MCI and MCCI).
REFERENCES
-
- Papastavrou E, Dimitriadou M, Tsangari H, Andreou C. Nursing students' satisfaction of the clinical learning environment: a research study. BMC Nurs. 2016 Jul 19;15:44. https://doi.org/10.1186/s12912-016-0164-4
- Mínguez Moreno I, González de la Cuesta D, Barrado Narvión MJ, Arnaldos Esteban M, González Cantalejo M. Nurse Mentoring: A Scoping Review. Healthcare (Basel). 2023 Aug 15;11(16):2302. https://doi.org/10.3390/healthcare11162302
- Huybrecht S, Loeckx W, Quaeyhaegens Y, De Tobel D, Mistiaen W. Mentoring in nursing education: perceived characteristics of mentors and the consequences of mentorship. Nurse Educ Today. 2011 Apr;31(3):274-8. https://doi.org/10.1016/j.nedt.2010.10.022
- Direttiva 2013/55/UE del Parlamento europeo e del Consiglio, del 20 novembre 2013, recante modifica della direttiva 2005/36/CE relativa al riconoscimento delle qualifiche professionali, in Gazzetta ufficiale dell'Unione europeaL 326, 21.11.2013, pagg. 1-18. [Italian] https://eur-lex.europa.eu/legal-content/IT/TXT/PDF/?uri=CELEX:32013L0055
- Warne T, Johansson UB, Papastavrou E, Tichelaar E, Tomietto M, Van den Bossche K, et al. An exploration of the clinical learning experience of nursing students in nine European countries. Nurse Educ Today. 2010 Nov;30(8):809-15.https://doi.org/10.1016/j.nedt.2010.03.003
- Pramila-Savukoski S, Juntunen J, Tuomikoski AM, Kääriäinen M, Tomietto M, Kaučič BM, et al. Mentors' self-assessed competence in mentoring nursing students in clinical practice: A systematic review of quantitative studies. J Clin Nurs. 2020 Mar;29(5-6):684-705. https://doi.org/10.1111/jocn.15127
- Tuomikoski AM, Ruotsalainen H, Mikkonen K, Miettunen J, Kääriäinen M. Development and psychometric testing of the nursing student mentors' competence instrument (MCI): A cross-sectional study. Nurse Educ Today. 2018 Sep;68:93-99.https://doi.org/10.1016/j.nedt.2018.05.028
- Luukkonen AL, Kuivila H, Kaarlela V, Koskenranta M, Kaučič BM, Riklikiene O, et al. Mentors' cultural competence at mentoring culturally and linguistically diverse nursing students in clinical practice: An international cross-sectional study. Nurse Educ Pract. 2023 Jul;70:103658. https://doi.org/10.1016/j.nepr.2023.103658
- Oikarainen A, Kaarlela V, Heiskanen M, Taam-Ukkonen M, Lehtimaja I, Kärsämänoja T, et al. Educational intervention to support development of mentors' competence in mentoring culturally and linguistically diverse nursing students: A quasi-experimental study. Nurse Educ Today. 2022 Sep;116:105424.https://doi.org/10.1016/j.nedt.2022.105424
- Giusti GD, Mazzotta R. The Crucial Role of Nursing Tutoring in Developing Nursing Students' Cultural Skills. Int Nurs Rev. 2025 Dec;72(4):e70122. https://doi.org/10.1111/inr.70122
- Mikkonen K, Tomietto M, Tuomikoski AM, Miha Kaučič B, Riklikiene O, Vizcaya-Moreno F, et al. Mentors' competence in mentoring nursing students in clinical practice: Detecting profiles to enhance mentoring practices. Nurs Open. 2022 Jan;9(1):593-603. https://doi.org/10.1002/nop2.1103
- Keinänen AL, Lähdesmäki R, Juntunen J, Tuomikoski AM, Kääriäinen M, Mikkonen K. Effectiveness of mentoring education on health care professionals´ mentoring competence: A systematic review. Nurse Educ Today. 2023 Feb;121:105709.https://doi.org/10.1016/j.nedt.2023.105709
- Giusti GD, Mazzotta R. Competencies of nursing tutors in clinical training. A italian nationwide survey study protocol. OSF https://doi.org/10.17605/OSF.IO/A4C3J .
- Kelley K, Clark B, Brown V, Sitzia J. Good practice in the conduct and reporting of survey research. Int J Qual Health Care. 2003 Jun;15(3):261-6. https://doi.org/10.1093/intqhc/mzg031
- von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP; STROBE Initiative. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. PLoS Med. 2007 Oct 16;4(10):e296. https://doi.org/10.1371/journal.pmed.0040296
- Polit, D. F., & Beck, C. T. (2017). Nursing Research: Generating and Assessing Evidence for Nursing Practice (10th ed.). Wolters Kluwer.
- Comparcini D, Cicolini G, Simonetti V, Mikkonen K, Kääriäinen M, Tomietto M. Developing mentorship in clinical practice: Psychometrics properties of the Mentors' Competence Instrument. Nurse Educ Pract. 2020 Feb;43:102713. https://doi.org/10.1016/j.nepr.2020.102713
- (2023). Microsoft Forms(v. 1.0) [Software]. Microsoft. www.microsoft.com
- IBM Corp. (2020). IBM SPSS Statistics (versione 27)[Software]. https://www.ibm.com/it-it/products/spss-statistics/resources.
- Italian Data Protection Authority (Garante per la protezione dei dati personali). Legislative Decree No. 196 of 30 June 2003 “Italian personal data protection code”. Available at: https://www.privacy.it/archivio/privacycode-en.html; last access: 12/06/2025.
- DECRETO LEGISLATIVO 10 agosto 2018, n. 101. Available at: https://www.gazzettaufficiale.it/eli/id/2018/09/04/18G00129/sg; last access: 12/06/2025.
- European Union General Data Protection Regulation (GDPR) Available at: https://eur-lex.europa.eu/eli/reg/2016/679/oj; last access:12/06/2025.
- Eysenbach G. Improving the quality of Web surveys: the Checklist for Reporting Results of Internet E-Surveys (CHERRIES). J Med Internet Res. 2004 Sep 29;6(3):e34. https://doi.org/10.2196/jmir.6.3.e34
- Sharma A, Minh Duc NT, Luu Lam Thang T, Nam NH, Ng SJ, Abbas KS, et al. A Consensus-Based Checklist for Reporting of Survey Studies (CROSS). J Gen Intern Med. 2021 Oct;36(10):3179-3187. https://doi.org/10.1007/s11606-021-06737-1
- Latour JM, Tume LN. How to do and report survey studies robustly: A helpful mnemonic SURVEY. Nurs Crit Care. 2021 Sep;26(5):313-314. https://doi.org/10.1111/nicc.12669
![]() This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
Exploring the impact of Nurse Manager Leadership Styles on Nurses' Job Performance at Hamad Medical Corporation: A Cross-Sectional Study
Abdelbasset Ghalgaoui 1, 2, *, Mehdi Halleb 1, Maha Mohamed Marzouk Ahmed 1,
Osama Helmi Mohammad Subih 1, Nabil Ajjel 1
- Department of Nursing, Hamad Medical Corporation (HMC), Doha, Qatar.
- Institut Universitaire de Formation des Cadres (INUFOCAD), Port-au-Prince, Haiti.
* Corresponding author: Abdelbasset Ghalgaoui, Graduate Registered Nurse, Department of Nursing, Hamad Medical Corporation (HMC), Doha, Qatar. PhD Student in Education and Governance, Institut Universitaire de Formation des Cadres (INUFOCAD), Port-au-Prince, Haiti. Email: ghalgaouiabdelbasset@gmail.com
Cite this article
ABSTRACT
Introduction: Nurse performance is vital to patient safety and organizational effectiveness. Leadership style is a recognized determinant of performance, influencing consistency, adaptability, and professional growth. Understanding these dynamics is particularly important in multicultural healthcare environments.
Objective: This study explored the impact of nurse manager leadership styles on nurses’ job performance at Hamad Medical Corporation (HMC).
Methods: A cross-sectional survey was conducted with 980 registered nurses recruited through random sampling. Data were collected using a structured questionnaire including socio-demographic characteristics, the Multifactor Leadership Questionnaire (MLQ-5X), and the Nursing Performance Instrument (NPI). Data analysis was performed using SPSS version 26, applying descriptive statistics, and Spearman’s correlation, Mann–Whitney U, and Kruskal–Wallis H tests.
Results: The workforce was predominantly female (72.1%), married (83.7%), and expatriate, with a mean age of 40.4 years. Transactional leadership (2.57 ±085) was the most common style, followed by transformational (2.20±1.05), while passive-avoidant leadership was minimal (1.49±0.97). Transformational leadership demonstrated strong positive associations with consistency of practice and adaptability. Transactional leadership supported compliance but was less effective in stimulating innovation, while passive-avoidant leadership was negatively correlated with performance outcomes.
Conclusion: Transformational leadership emerged as the most effective style for enhancing nurse performance, while transactional leadership sustained compliance without fostering long-term growth. Strengthening transformational leadership among nurse managers at HMC may improve clinical outcomes, adaptability, and organizational performance.
Keywords: Leadership, Nurses, Job Performance, Practice
INTRODUCTION
In the complex and ever-evolving healthcare environment, the performance of nurses is a cornerstone of quality patient care and organizational success [1–4]. Nurses are at the forefront of healthcare delivery, directly influencing patient outcomes, safety, and satisfaction through their clinical skills, critical thinking, and interpersonal interactions [5–7]. The effectiveness with which nurses execute their duties is not solely dependent on their individual competencies but is significantly shaped by the leadership they receive. Nurse managers, in particular, play a crucial role in fostering an environment that optimizes nursing performance, as their leadership styles directly influence the motivation, development, and productivity of their teams [8].
Job performance in nursing encompasses a broad range of behaviors and outcomes, including adherence to protocols, clinical proficiency, teamwork, communication, and adaptability to challenging situations. High-performing nursing teams contribute to reduced medical errors, improved patient recovery rates, and enhanced overall efficiency within healthcare institutions [9–12]. The leadership styles employed by nurse managers have a profound impact on the performance of their nursing staff. Transformational leadership, characterized by its emphasis on inspiring, empowering, and intellectually stimulating nurses, is often associated with higher levels of performance, as it encourages innovation, professional growth, and a strong sense of ownership [13–16]. This style promotes a positive work environment, which is crucial for fostering high performance. In contrast, transactional leadership, which relies on clear directives, rewards, and corrective actions, can ensure compliance with standards but may not always foster the proactive and adaptive behaviors essential for complex clinical environments [17–19]. Passive-avoidant leadership, marked by a lack of engagement and decision-making, typically has detrimental effects on performance, leading to confusion and disorganization[8]. Recent studies continue to highlight the importance of effective nursing leadership in driving performance outcomes [8,14–19].
While existing literature has explored the relationship between nurse manager leadership styles and job performance, there remains a specific research gap concerning the context of Qatar. Studie in Qatar have investigated aspects such as the generational gap between nurses and nurse managers and its potential impact on job performance [20] . However, a comprehensive understanding of how various nurse manager leadership styles directly influence the diverse aspects of nurses' job performance within the unique healthcare landscape of Qatar, considering its multicultural workforce and specific organizational structures, is still limited. There is a particular need to understand which leadership styles are most effective in promoting optimal job performance among nurses in HMC, given the specific cultural and organizational dynamics of the region.
Objective
This study aims to investigate the specific influence of nurse manager leadership styles on nurses’ job performance at HMC. Specifically, it will examine the relationship between transformational, transactional, and laissez-faire leadership styles and various dimensions of nursing performance. The insights gained will be invaluable for developing targeted leadership training programs and organizational policies designed to optimize nursing performance, ultimately contributing to superior patient care and the sustained success of HMC's healthcare mission.
MATERIALS AND METHODS
Type and Classification of Study
This study employed a quantitative, cross-sectional research design to examine the relationship between nurse manager leadership styles and nurses' job satisfaction, work engagement, and job performance at Hamad Medical Corporation (HMC).
Comparisons and Predictors of Interest
The primary focus was on comparing various nurse manager leadership styles and their respective impacts on staff nurses’ job satisfaction, work engagement, and job performance.
Study Duration
The study was conducted over a period of approximately four months, from November 5, 2024, to March 1, 2025.
Sample Size Justification
To ensure reliability and representativeness of the findings, a sample size calculation was conducted based on a population of approximately 12,000 nurses. Using a 95% confidence level and a ±3% margin of error, a sample size of 980 nurses was determined to be appropriate. The sample size was calculated using Cochran’s formula:
where Z = 1.96, p = 0.5, e = 0.03.
The value p=0.5 was selected to provide the most conservative estimate and ensure an adequate sample size in the absence of prior data, while margin of error e = ±3% was chosen to achieve high precision and reliable representativeness of the study results.
Study Population and Setting
The study targeted registered nurses employed across different departments at Hamad Medical Corporation (HMC), Qatar. A simple random sampling procedure was used to select participants. The sampling frame consisted of the complete roster of licensed nurses at HMC, with each nurse assigned a unique identification number. Randomization was performed using Microsoft Excel’s RAND function to generate a randomly ordered list.
To mitigate potential non-response, the initial calculated sample of 980 nurses (based on a 95% confidence level and ±3% margin of error for a population of approximately 12,000 nurses) was increased by 245 nurses, resulting in 1,225 nurses being contacted. The questionnaire was distributed to these nurses via their official HMC email accounts, and 980 responses were received and included in the final study sample. This approach ensured equal probability of selection and broad representation across hospitals and nursing units within HMC.
The study was conducted exclusively within HMC facilities.
Inclusion Criteria
- Registered nurses currently employed at HMC.
- Nurses who voluntarily consented to participate.
- Nurses with a minimum of six months of experience at HMC to ensure familiarity with the organizational culture and leadership practices.
Exclusion Criteria
- Nurses on leave or absent during data collection.
- Nurses in managerial or supervisory roles.
- Contract or temporary nurses.
Data Collection
Data were collected via structured online questionnaires distributed through Google Forms. The survey instruments covered the following areas:
- Socio-demographic Data
- Collected information included age, gender, nationality, years of nursing experience, tenure at HMC, education level, hospital, and department.
- Multifactor Leadership Questionnaire (MLQ-5X)
This 45-item tool assessed leadership styles (transformational, transactional, and laissez-faire) across dimensions such as inspirational motivation, intellectual stimulation, and contingent reward. Responses were recorded on a 5-point Likert scale (0 = "Not at all" to 4 = "Frequently, if not always") [21].
Items were grouped into their respective leadership dimensions using the MLQ scoring key. For each dimension, a mean score was calculated by summing the responses to the items composing that scale and dividing by the number of valid responses. All leadership style subscales consisted of four items each. Blank or missing responses were excluded from the calculations. Higher mean scores indicated more frequent exhibition of the corresponding leadership behaviors. Leadership dimensions were analyzed as continuous variables rather than categorizing leaders into a single leadership style. The tool demonstrated strong reliability, with Cronbach’s alpha ranging from 0.70 to 0.90.
- Nursing Performance Instrument (NPI)
This 20-item instrument assessed nursing performance across clinical and interpersonal dimensions. Responses were rated on a 6-point Likert scale (1 = "Strongly Disagree" to 6 = "Strongly Agree") [22].
NPI scores were calculated by summing the item responses within each domain and dividing by the number of items to obtain mean domain scores. An overall NPI score was computed by averaging all 9 items. Missing responses were excluded from the calculations. Higher scores indicated better perceived nursing performance.
The instrument yielded a Cronbach’s alpha of 0.80, indicating strong reliability.
Statistical Considerations and Data Analysis
Primary and Secondary Outcomes
- Primary Outcomes: Nurses’ job performance.
- Secondary Outcome: The relationship between nurse manager leadership styles and the three primary outcomes.
Data Analysis Plan
1. Descriptive Statistics
Summarized participant characteristics and key variables using means and standard deviations (mean±SD), or medians and interquartile intervals (IQR), for numerical data, while ranges, and percentages for qualitative and categorical data.
2. Inferential Statistics
- Normality of continuous variables was assessed using the Shapiro–Wilk test, which indicated non-normal distribution (p < 0.05).
- Spearman’s Correlation Coefficient: Used to assess associations between leadership styles and outcome variables.
- Mann–Whitney U Test: Applied to compare differences in outcome variables between two independent groups
- Kruskal–Wallis H Test: Used to compare differences across three or more independent groups
- A p-value (p) < 0.05 was considered statistically significant.
Statistical Software
All analyses were performed using SPSS-26 (Statistical Package for the Social Sciences-26).
Ethical Approval and Informed Consent Statement
Informed consent was obtained from all study participants. The purpose, procedures, and voluntary nature of the study were explained through official internal communication channels via HMC e-mail. Participants provided electronic consent after having at least two months to review the study information before deciding to participate. Only registered nurses employed at Hamad Medical Corporation (HMC) who met the inclusion criteria were enrolled. No financial incentives were offered for participation.
The study was approved by the Medical Research Center (MRC) – Local Ethics Committee of Hamad Medical Corporation, Qatar (Protocol No. MRC-01-24-356),with approval granted on 15/08/2024, and was conducted in accordance with the principles of the Declaration of Helsinki and Good Clinical Practice (GCP), as well as the regulations of the Ministry of Public Health (MoPH), Qatar. Participant anonymity and data confidentiality were strictly maintained throughout the study.
RESULTS
Demographic and Professional Characteristics
The study sample (N=980) exhibits a predominant representation of females (72.14%), while males account for 27.86%. The sex ratio of 0.39 males per female (Table 1).
| Characteristics | Categories | Frequency (n) | Percent (%) | Mean± SD | Median (IQR) |
| Gender | Male | 273 | 27.86 | ||
| Female | 707 | 72.14 | |||
| Marital Status | Single | 138 | 14.08 | ||
| Married | 820 | 83.67 | |||
| Widowed | 8 | 0.82 | |||
| Separated / Divorced | 14 | 1.43 | |||
| Nationality | Cuban | 36 | 3.67 | ||
| Egyptian | 16 | 1.63 | |||
| Filipino | 332 | 33.88 | |||
| Indian | 413 | 42.14 | |||
| Iranian | 3 | 0.31 | |||
| Jordanian | 64 | 6.53 | |||
| Lebanese | 5 | 0.51 | |||
| Palestinian | 8 | 0.82 | |||
| Somali | 3 | 0.31 | |||
| Sudanese | 51 | 5.20 | |||
| Tunisian | 49 | 5.00 | |||
| Age (years) | ≤30 years | 64 | 6.53 |
40.40 ± 7.89 |
37 (35-46) |
| ]30-45] | 657 | 67.04 | |||
| > 45 | 259 | 26.43 |
Table 1. Demographic Characteristics (N=980)
The majority of participants are married (83.67%), with a smaller proportion being single (14.08%) or widowed (0.82%). In terms of nationality, the most represented groups are Indian (42.14%) and Filipino (33.88%), collectively comprising over 75% of the total sample, while other nationalities, such as Jordanian (6.53%), Sudanese (5.20%), and Tunisian (5.0%), are present in smaller proportions. Certain nationalities, including Iranian (0.31%) and Somali (0.31%), have minimal representation. The mean age of the participants is 40.40 ±7.89 years, with a minimum age of 26 years and a maximum age of 62 years. The majority belonging to the 30-45 age group (67.04%), followed by those over 45 years (26.43%), and only a small percentage ≤30 years (6.53%).
The professional characteristics of the study sample (N=980) reveal a workforce with diverse experience levels and educational backgrounds (Table 2). The mean years of experience as a nurse is 16.85 ± 7.14 years, ranging from 3 to 39 years. The majority have 5-15 years of experience (54.29%), followed by those with more than 15 years (43.57%), and a small proportion with ≤5 years (2.14%). Experience within Hamad Medical Corporation (HMC) follows a similar trend, with a mean of 9.93 ± 7.54 years, ranging from 1 to 36 years. The distribution shows that 36.73% have ≤5 years, 37.65% have 5-15 years, and 25.61% have over 15 years of experience in HMC.
Regarding education, the majority hold a Bachelor’s degree (76.63%), while 14.18% have a diploma, and 9.18% hold a Master’s degree or higher.
The participants are distributed across various hospitals, with the highest representation from Hamad General Hospital (27.55%), followed by Rumailah Hospital (11.63%), Al Wakra Hospital (11.43%), and Women’s Wellness and Research Center (8.16%). Other facilities, including specialty hospitals like the Communicable Disease Center (1.53%) and The Cuban Hospital (1.73%), have lower representation.
In terms of departmental distribution, the Surgical Department (35.51%) and Medical Department (30.20%) have the highest number of participants, followed by Critical Care/Emergency Services (22.45%) and Outpatient and Ambulatory Services (11.84%).
| Characteristics | Categories | Frequency (n) | Percent (%) | Mean± SD | Median (IQR) |
| Years of experience as a nurse | ≤5 years | 21 | 2.14 |
16.85 ± 7.14 |
15(12-22) |
| ]5-15] | 532 | 54.29 | |||
| > 15 | 427 | 43.57 | |||
| Years of experience in HMC | ≤5 years | 360 | 36.73 |
9.93 ± 7.54 |
7(4-17) |
| ]5-15] | 369 | 37.65 | |||
| > 15 | 251 | 25.61 | |||
| Educational background
|
Diploma | 139 | 14.18 | ||
| Bachelor’s degree | 751 | 76.63 | |||
| Master’s degree | 90 | 9.18 | |||
| Hospital
|
Hamad General Hospital | 270 | 27.55 | ||
| Ambulatory Care Center | 58 | 5.92 | |||
| Qatar Rehabilitation Institute | 17 | 1.73 | |||
| NCCCR | 19 | 1.94 | |||
| Mental Health Service | 48 | 4.90 | |||
| Communicable Disease Center | 15 | 1.53 | |||
| Al Khor Hospital | 72 | 7.35 | |||
| Rumailah Hospital | 114 | 11.63 | |||
| Al Wakra Hospital | 112 | 11.43 | |||
| Hazm Mebaireek General Hospital | 64 | 6.53 | |||
| Aisha Bint Hamad Al Attiyah Hospital | 63 | 6.43 | |||
| The Cuban Hospital | 17 | 1.73 | |||
| Women's Wellness and Research Center | 80 | 8.16 | |||
| Heart Hospital | 31 | 3.16 | |||
| Department
|
Critical Care / Emergency Services | 220 | 22.45 | ||
| Medical Department | 296 | 30.20 | |||
| Surgical Department | 348 | 35.51 | |||
| Outpatient (OPD) and Ambulatory Services | 116 | 11.84 |
Table 2. Professional Characteristics (N=980)
Nurse Manager Leadership Styles
The results indicate that transactional leadership (2.57±0.85) is more dominant than transformational leadership (2.20±1.05), suggesting that leaders in this sample primarily rely on structured management approaches, such as performance-based rewards (contingent reward, 2.56±1.05) and active monitoring (management by exception – active: 2.58±0.98), rather than fostering innovation, motivation, or individualized consideration (Table 3).
| Minimum | Maximum | Mean | S D | Median | Q1 | Q3 | |
| Idealized Attributes or Idealized Influence (Attributes) | 0.00 | 4.00 | 2.19 | 1.14 | 2.25 | 1.50 | 3.00 |
| Idealized Behaviors or Idealized Influence (Behaviors) | 0.00 | 4.00 | 2.35 | 1.15 | 2.50 | 1.75 | 3.25 |
| Inspirational Motivation | 0.00 | 4.00 | 2.34 | 1.22 | 2.50 | 1.50 | 3.25 |
| Intellectual Stimulation | 0.00 | 4.00 | 2.21 | 1.11 | 2.25 | 1.50 | 3.00 |
| Individual Consideration | 0.00 | 4.00 | 1.94 | 0.96 | 2.00 | 1.25 | 2.75 |
| Transformational | 0.00 | 4.00 | 2.20 | 1.05 | 2.35 | 1.55 | 3.00 |
| Contingent Reward | 0.00 | 4.00 | 2.56 | 1.05 | 2.75 | 2.00 | 3.25 |
| Mgmt by Exception (Active) | 0.00 | 4.00 | 2.58 | 0.98 | 2.75 | 2.00 | 3.25 |
| Transactional | 0.25 | 4.00 | 2.57 | 0.85 | 2.62 | 2.00 | 3.12 |
| Mgmt by Exception (Passive) | 0.00 | 4.00 | 1.55 | 1.01 | 1.25 | 0.75 | 2.25 |
| Laissez-Faire | 0.00 | 4.00 | 1.43 | 1.05 | 1.25 | 0.50 | 2.25 |
| Passive Avoidant | 0.00 | 4.00 | 1.49 | 0.97 | 1.37 | 0.75 | 2.12 |
| Extra Effort | 0.00 | 4.00 | 2.17 | 1.20 | 2.33 | 1.00 | 3.00 |
| Effectiveness | 0.00 | 4.00 | 2.25 | 1.22 | 2.50 | 1.00 | 3.00 |
| Satisfaction | 0.00 | 4.00 | 2.28 | 1.31 | 2.50 | 1.00 | 3.00 |
| Outcomes of Leadership | 0.00 | 400 | 2.23 | 1.20 | 2.42 | 1.05 | 3.16 |
Table 3. Nurse Manager Leadership Styles
Within transformational leadership, the highest subscale is idealized influence behaviors (2.35±1.15), indicating that some leaders demonstrate strong role-modeling behaviors. However, individual consideration (1.94±0.96) is the lowest, suggesting that leaders may not provide enough mentorship or personalized support to the nurses.
The passive-avoidant leadership style (1.49±0.97) has the lowest overall scores, particularly laissez-faire leadership (1.43±1.05), indicating that leaders in this sample are generally engaged and do not frequently avoid decision-making. However, the management by exception – passive score (1.55±1.01) suggests that some leaders may still wait until problems arise before taking corrective action.
Regarding leadership outcomes, the scores for effectiveness (2.25±1.22) and satisfaction (2.28±1.31) indicate moderate levels of perceived leader effectiveness and staff satisfaction. Overall outcomes of leadership (2.23±1.20) reflect a tendency towards average performance across the sample, with some variability.
Nurses' Job Performance
The results of the Nursing Performance Instrument (NPI) and its three subscales reveal interesting insights into the nursing workforce’s performance (Table 4).
| Minimum | Maximum | Mean | SD | Median | Q1 | Q3 | |
| Physical / mental decrement | 1.00 | 6.00 | 2.91 | 1.11 | 3.00 | 2.00 | 3.66 |
| Consistent practice | 1.00 | 6.00 | 4.73 | 1.29 | 5.00 | 4.25 | 5.75 |
| Behavioral change | 1.00 | 6.00 | 3.61 | 1.33 | 3.50 | 3.00 | 4.50 |
| Nursing Performance Instrument (NPI) | 1.00 | 5.78 | 3.88 | 0.94 | 3.88 | 3.44 | 4.44 |
Table 4. Nurses' Job Performance
The subscale "Physical/Mental Decrement" had a mean score of 2.91±1.11, suggesting that nurses report a moderate level of physical and mental strain, though it is not perceived as a severe issue overall. The "Consistent Practice" subscale scored the highest, with a mean of 4.73±1.29, indicating that nurses generally perceive themselves as maintaining consistent and stable practices in their roles. The "Behavioral Change" subscale, with a mean of 3.61±1.33, suggests that there is moderate evidence of behavioral changes in nursing practice. Lastly, the overall NPI score of 3.88±0.94 indicates a generally positive view of nursing performance, reflecting a moderate level overall.
Comparison of Socio-demographic Characteristics and Their Association with Nurses' Job Performance
Female nurses had significantly higher job performance than male nurses (mean rank: 536.67 vs. 370.92, p < 0.001) (Table 5).
| Characteristics | Categories | Mean Rank | Test | p-value (test) |
| Gender
|
Male | 370,92 | 63861,5 | < 0.001 (MW)*
|
| Female
|
536,67 | |||
| Marital Status | Single | 551.12 |
9.513
|
0.009 (KW)*
|
| Married | 472.37 | |||
| Widowed | 457.50 | |||
| Nationality | Cuban | 268.22 | 150.584
|
< 0.001 (KW)*
|
| Egyptian | 389.00 | |||
| Filipino | 576.75 | |||
| Indian | 498.81 | |||
| Iranian | 715.83 | |||
| Jordanian | 298.00 | |||
| Lebanese | 717.70 | |||
| Palestinian | 754.00 | |||
| Somali | 649.17 | |||
| Sudanese | 486.15 | |||
| Tunisian | 198.83 | |||
| Age (years) | ≤30 years | 568.97 | 29.617
|
< 0.001 (KW)*
|
| ]30-45] | 456.10 | |||
| > 45 | 558.38 | |||
| Years of experience as a nurse
|
≤5 years | 509.26 | 1.273
|
0.529 (KW)*
|
| ]5-15] | 481.21 | |||
| > 15 | 501.15 | |||
| Years of experience in HMC
|
≤5 years | 472.97 | 0.003 | 11.533 (KW)* |
| ]5-15] | 472.07 | |||
| > 15 | 542.74 | |||
| Educational background | Diploma | 425.49 | 9.391
|
0.009 (KW)*
|
| Bachelor’s degree | 498.19 | |||
| Master’s degree | 526.72 | |||
| Hospital | Hamad General Hospital | 527.88 | 61.003 | < 0.001(KW)* |
| Al Khor Hospital | 375.75 | |||
| Rumailah Hospital | 428.29 | |||
| Al Wakra Hospital | 458.57 | |||
| Hazm Mebaireek General Hospital | 500.56 | |||
| Aisha Bint Hamad Al Attiyah Hospital | 462.40 | |||
| The Cuban Hospital | 263.56 | |||
| Women's Wellness and Research Center | 481.40 | |||
| Heart Hospital | 607.08 | |||
| Ambulatory Care Center | 531.40 | |||
| Qatar Rehabilitation Institute | 583.32 | |||
| NCCCR | 683.03 | |||
| Mental Health Service | 493.17 | |||
| Communicable Disease Center | 703.83 | |||
| Department | Critical Care / Emergency Services | 492.86 | 43.713 | < 0.001(KW)* |
| Medical Department | 488.47 | |||
| Surgical Department | 440.61 | |||
| Outpatient (OPD) and Ambulatory Services | 640.84 |
Note: MW = Mann–Whitney U test; KW = Kruskal–Wallis H test; *p < 0.05 indicates statistical significance.
Table 5. Comparison of Socio-demographic Characteristics and Their Association with Nurses' Job Performance.
Single nurses reported the highest performance, followed by married and widowed nurses (551.12 vs. 472.37 vs. 457.50, p = 0.009). Significant differences were observed across nationalities, with Palestinian nurses showing the highest performance and Tunisian nurses the lowest (754.00 vs. 198.83, p < 0.001).
Regarding age, nurses aged ≤30 years had the highest performance, followed by those >45 years and those aged 30–45 years (568.97 vs. 558.38 vs. 456.10, p < 0.001). Years of experience as a nurse were not significantly associated with performance, although nurses with ≤5 years of experience had higher performance than those with >15 years or 5–15 years (509.26 vs. 501.15 vs. 481.21, p = 0.529).
Years of experience at HMC were significantly associated with performance, with nurses having >15 years of experience showing the highest performance and those with 5–15 years the lowest (542.74 vs. 472.07, p = 0.003). Educational background influenced performance, with nurses holding a Master’s degree reporting the highest and those with a diploma the lowest (526.72 vs. 425.49, p = 0.009).
Job performance differed significantly across hospitals, with the Mental Health Service reporting the highest and ABAH the lowest performance (703.83 vs. 263.56, p < 0.001). Finally, departmental differences were significant, with the Surgical Department showing the highest performance and the Medical Department the lowest (640.84 vs. 440.61, p < 0.001).
Correlation between Nurse Manager Leadership Styles and Nurses’ Performance
Table 6 explores the relationships between leadership styles and various aspects of nursing performance, including physical/mental decrement, consistent practice, behavioral change, and overall performance measured by the Nursing Performance Instrument (NPI).
Transformational leadership shows a moderate positive correlation with consistent practice (rho = 0.323, p <0.001) and a weak positive correlation with nursing performance (rho = 0.146, p < 0.001). However, there are no significant relationships with physical/mental decrement (rho = 0.017, p = 0.597) or behavioral change (rho = 0.022, p = 0.489). These results suggest that transformational leadership encourages consistent practice and slightly enhances overall performance but does not appear to directly influence nurses' physical or mental well-being or their immediate behavioral adjustments.
|
|
Physical/mental decrement | Consistent practice | Behavioral change | Nursing Performance Instrument (NPI) | |
| Transformational
|
Spearman Coefficient | 0.017 | 0.323 | 0.022 | 0.146 |
| p-value | 0.597 | < 0.001 | 0.489 | <0.001 | |
| Transactional
|
Spearman Coefficient | -0.277 | -0.055 | -0.339 | -0.230 |
| p-value | < 0.001 | 0.083 | < 0.001 | < 0.001 | |
| Passive Avoidant
|
Spearman Coefficient | 0.038 | -0.073 | -0.087 | -0.121 |
| p-value | 0.233 | 0.022 | 0.006 | < 0.001 | |
Table 6. Correlation between Nurse Manager Leadership Styles and Nurses’ Performance.
Transactional leadership presents a negative correlation with physical/mental decrement (rho = -0.277, p < 0.001), behavioral change (rho = -0.339, p < 0.001), and nursing performance (rho = -0.230, p < 0.001). The correlation with consistent practice is not significant (rho = -0.055, p = 0.083). These findings imply that transactional leadership may be associated with declines in behavioral adaptability and overall performance, potentially reflecting a rigid, reward-punishment dynamic that does not foster flexibility or proactive nursing behaviors.
Passive-avoidant leadership demonstrates weak negative correlations with consistent practice (rho = -0.073, p = 0.022), behavioral change (rho = -0.087, p = 0.006), and nursing performance (rho = -0.121, p < 0.001), though no significant relationship is found with physical/mental decrement (rho = 0.038, p = 0.233). This suggests that passive-avoidant leadership slightly undermines effective nursing practices and performance, likely due to a lack of guidance and support.
In summary, transformational leadership has the most positive influence, especially on consistent practice and overall nursing performance. In contrast, transactional leadership seems linked to negative outcomes, particularly regarding behavioral flexibility and performance, while passive-avoidant leadership also has small but significant negative effects.
DISCUSSION
Demographic and Professional Characteristics
The demographic characteristics of the sample provide important context for interpreting job performance outcomes. The high representation of women (72.14%) is consistent with the global nursing workforce [23,24], though the smaller proportion of men (27.86%) may affect team diversity and performance styles [25]. The predominance of married nurses (83.67%) suggests stability, yet also underscores the dual stressors of family and professional responsibilities, which can affect concentration and efficiency [26,27]. The reliance on expatriate staff, especially Indian (42.14%) and Filipino (33.88%) nurses, reflects regional workforce trends but introduces cultural adaptation challenges that may shape performance consistency [28]. The average age (40.40 years) and extensive experience (16.85±7.14 years) demonstrate a mature workforce capable of sustaining performance. However, the limited presence of younger nurses (≤5 years’ experience, 2.14%) may hinder succession planning and innovation. The predominance of bachelor’s degrees (76.63%) indicates solid educational preparation, though the limited advanced degrees (9.18%) highlight opportunities to strengthen specialized competencies.
Nurse Manager Leadership Styles
Leadership findings confirmed transactional leadership (2.57±085) as the dominant style, with contingent rewards (2.56±1.05) and active monitoring (2.58±0.98) driving structured compliance. While these strategies ensure adherence to standards, they may not stimulate the innovation and adaptability increasingly demanded in modern healthcare settings [15,18]. The low emphasis on individual consideration (1.94±0.96) suggests a lack of personalized development, limiting opportunities for performance growth [8]. By contrast, transformational leadership has been consistently linked to enhanced job performance across diverse contexts [14,16]. Although passive-avoidant leadership (1.49±0.97) was rare, its occasional presence risks undermining performance through delayed intervention. These results suggest that adopting transformational leadership at HMC could strengthen consistency, adaptability, and clinical performance.
Nurses' Job Performance
The high consistent practice scores (4.73±1.29) highlight nurses’ reliability in adhering to established protocols, a strength in error-prone healthcare settings. However, moderate behavioral change (3.61±1.33) signals resistance to adapting workflows, possibly due to rigid transactional leadership or fear of reprisal for deviations. The overall performance score (NPI = 3.88) suggests competence but not excellence, aligning with environments prioritizing compliance over innovation. Notably, physical/mental decrement (2.91±1.11) indicates that strain, while not severe, may hinder proactive initiatives. In a similar context in Iran, nurse performance was also reported at a moderate level, with the general performance aspect receiving the highest average score and the mental aspect the lowest [29].
Comparison of Socio-demographic Characteristics and Their Association with Nurses' Job Performance
Job performance varied markedly across demographics. Females outperformed males (p < 0.001), aligning with a study conducted in the same context in Jordan, a Middle Eastern country, which linked female nurses to higher job performance [30]. This gender gap may reflect both enduring social norms around caring roles and targeted soft-skills training that disproportionately benefits female practitioners.
Single nurses showed higher performance (mean rank = 551.12) than married or widowed peers, possibly due to fewer familial responsibilities or greater focus on career progression. This contrasts with studies conducted in Jordan and Turkey, which found no significant relationship between marital status and job performance [30,31]. Nationality-based differences were stark: Palestinian nurses (mean rank = 754.00) excelled, while Tunisians (mean rank = 198.83) underperformed. This may reflect disparities in training quality, language proficiency, or workplace integration. Younger nurses (≤30 years) outperformed older colleagues (p < 0.001), suggesting adaptability to new protocols or technologies. Paradoxically, nurses with >15 years of HMC experience also performed well, indicating that institutional knowledge complements innovation. In the same context, a study conducted in Jordan found that age and experience were related to job performance [30].
Master’s-trained nurses (mean rank = 526.72) outperformed diploma holders, underscoring the value of advanced education in clinical decision-making. Hospitals like the Mental Health Service (mean rank = 703.83). Surgical departments (mean rank = 640.84) reported superior performance, likely due to specialized workflows or interdisciplinary collaboration. These findings advocate for competency-based training and equitable recognition of diverse backgrounds.
Correlation between Nurse Manager Leadership Styles and Nurses’ Job Performance
Transformational leadership moderately enhanced consistent practice (rho = 0.323, p < 0.001) but had no impact on behavioral change, suggesting it fosters reliability over innovation. The findings partially align with those reported by Mohammed Qtait on 2023, who conducted a systematic review of 12 quantitative studies investigating the relationship between leadership styles and nurse performance, reports that transformational leadership had the strongest positive correlation enhancing nursing care quality, job satisfaction, motivation, and patient outcomes [8].
Transactional leadership correlated negatively with performance (rho = -0.230, p < 0.001), particularly behavioral change (rho = -0.339, p < 0.001), implying rigid reward-punishment systems hinder adaptability. However, Qtait’s review found a moderate positive correlation between transactional leadership and nurse performance, indicating some benefits under structured systems [8].
Passive-avoidant leadership also undermined performance (rho = -0.121, p < 0.001), in line with Qtait’s conclusion that laissez-faire leadership had weak or no positive impact [8]. This consistent finding emphasizes that ambiguity, lack of guidance, and disengagement by leaders can significantly reduce nurse motivation and clarity in roles.
Recommendations
The findings of this study highlight the critical need to strengthen transformational leadership competencies among nurse managers at Hamad Medical Corporation (HMC). It is recommended that HMC invest in ongoing leadership development programs that emphasize communication, motivation, and professional empowerment to promote inspiring and participative managerial behaviors. Transformational leadership, by encouraging autonomy and creativity, can significantly enhance both individual and collective nursing performance, fostering consistency in clinical practice and adaptability in complex healthcare settings.
Furthermore, leadership competency assessments should be integrated into managerial performance evaluations to ensure that adopted leadership styles align with organizational goals and contribute to nurse productivity and job satisfaction. Organizational culture should also move toward reducing overreliance on transactional leadership, which focuses primarily on control and rewards, and instead foster more collaborative, innovative, and supportive leadership approaches.
Finally, creating a psychologically and physically supportive work environment is essential to reduce stress and fatigue among nurses, both of which can negatively affect long-term job performance
Strengths and limitations of the study
This study possesses several methodological strengths that enhance its scientific credibility. First, the use of a large and randomly selected sample (N = 980) provides strong representativeness and statistical reliability. The application of validated international instruments, namely the Multifactor Leadership Questionnaire (MLQ-5X) for assessing leadership styles and the Nursing Performance Instrument (NPI) for measuring clinical performance, adds to the study’s methodological rigor. Moreover, the use of robust statistical analyses including Spearman’s correlation, Mann–Whitney U, and Kruskal–Wallis H tests enabled comprehensive exploration of relationships between leadership styles and various aspects of job performance, providing a multidimensional understanding of these dynamics. Despite its strengths, the study also presents certain limitations. The most significant is its cross-sectional design, which limits the ability to infer causality between leadership style and nurse performance. It remains unclear whether transformational leadership directly improves performance, or whether nurses who perform better perceive their leaders as more transformational. Additionally, self-reported data may have introduced response bias, as participants could overestimate their performance due to social desirability or professional pride. Studies would provide a broader and more causal understanding of these leadership–performance relationships.
CONCLUSION
This study clearly demonstrates that nurse manager leadership styles have a significant and differentiated impact on nurses’ job performance within Hamad Medical Corporation. The results reveal that transformational leadership exerts the most substantial positive effect, enhancing consistency in clinical practice, adaptability to change, and overall professional performance. Nurses who perceive their leaders as visionary, supportive, and encouraging are more motivated, committed, and productive. These findings align with international literature showing that transformational leaders foster collaboration, reduce clinical errors, and improve both patient outcomes and staff well-being. In contrast, transactional leadership, while effective in maintaining compliance and operational discipline, tends to have limited influence on creativity and long-term professional growth. Its focus on control and reward systems may sustain performance in routine tasks but fails to nurture the initiative and innovation required in dynamic healthcare environments. On the other hand, passive-avoidant leadership emerges as the least effective style, being associated with disorganization, lack of motivation, and decreased performance due to minimal managerial involvement or guidance.
The implications for nursing leadership are profound. Developing a structured and culturally adaptive transformational leadership model should be a strategic priority for HMC. Such an approach can strengthen clinical performance, enhance innovation, reduce turnover, and promote a collaborative culture focused on quality and patient safety. Ultimately, this study underscores that effective leadership in nursing transcends task management it is fundamentally about mobilizing human potential to achieve excellence, empowerment, and resilience within healthcare organizations.
Local Ethics Committee approval
The study was approved by the Medical Research Center (MRC) – Local Ethics Committee of Hamad Medical Corporation, Qatar (Protocol No. MRC-01-24-356) and was conducted in accordance with the principles of the Declaration of Helsinki and Good Clinical Practice (GCP), as well as the regulations of the Ministry of Public Health (MoPH), Qatar. Participant anonymity and data confidentiality were strictly maintained throughout the study.
Conflicts of interest
This study was conducted in accordance with ethical standards. All participants provided informed consent. The authors declare no conflict of interest.
Sources of funding
This research received funding from the Medical Research Center at HMC.The authors thank the
Author contributions
Conception and design: Abdelbasset Ghalgaoui
Data collection: Abdelbasset Ghalgaoui
Data analysis and interpretation: Abdelbasset Ghalgaoui, Osama Helmi Mohammad Subih, Maha Mohamed Marzouk Ahmed, Mehdi Halleb, Nabil Ajjel.
Drafting of the manuscript: all authors.
Critical revision of the manuscript: Abdelbasset Ghalgaoui, Mehdi Halleb
Final approval: all authors
Acknowledgements
The authors thank the staff of Hamad Medical Corporation for their collaboration.
REFERENCES
- DeLucia PR, Ott TE, Palmieri PA. Performance in Nursing. Reviews of Human Factors and Ergonomics. SAGE Publications; 2009;5:1–40. https://doi.org/10.1518/155723409X448008
- El-Gazar HE, Zoromba MA. Nursing Human Resource Practices and Hospitals’ Performance Excellence: The Mediating Role of Nurses’ Performance. Acta Biomed. 2021;92:e2021022. https://doi.org/10.23750/abm.v92iS2.11247
- Gurses AP, Carayon P, Wall M. Impact of Performance Obstacles on Intensive Care Nurses’ Workload, Perceived Quality and Safety of Care, and Quality of Working Life. Health Services Research. 2009;44:422–43. https://doi.org/10.1111/j.1475-6773.2008.00934.x
- Shahnavazi A, Bouraghi H, Eshkiki MF, Shahnavazi H. The Effect of Perceived Organizational Climate on the Performance of Nurses in Private Hospitals [Internet]. Journal of Clinical Research in Paramedical Sciences. Brieflands; 2021 Dec. https://doi.org/10.5812/jcrps.108532
- Bae JY, Bae SH. The Effect of Clinical Nurses’ Critical Thinking Disposition and Communication Ability on Patient Safety Competency. J Korean Acad Fundam Nurs. Korean Academy of Fundamentals of Nursing; 2022;29:159–69. https://doi.org/10.7739/jkafn.2022.29.2.159
- Saputri CA. The Role of Nursing Interventions in Patient Satisfaction and Outcomes. AHR. 2023;1:75–87. https://doi.org/10.60079/ahr.v1i2.359
- Wieke Noviyanti L, Ahsan A, Sudartya TS. Exploring the Relationship between Nurses’ Communication Satisfaction and Patient Safety Culture. Journal of Public Health Research. SAGE Publications; 2021;10:jphr.2021.2225. https://doi.org/10.4081/jphr.2021.2225
- Qtait M. Systematic Review of Head Nurse Leadership Style and Nurse Performance. International Journal of Africa Nursing Sciences. 2023;18:100564. https://doi.org/10.1016/j.ijans.2023.100564
- Alrabadi N, Shawagfeh S, Haddad R, Mukattash T, Abuhammad S, Al-rabadi D, et al. Medication errors: a focus on nursing practice. J Pharm Health Serv Res. 2021;12:78–86. https://doi.org/10.1093/jphsr/rmaa025
- Asante BL, Zúñiga F, Favez L. Quality of care is what we make of it: a qualitative study of managers’ perspectives on quality of care in high-performing nursing homes. BMC Health Serv Res. 2021;21:1090. https://doi.org/10.1186/s12913-021-07113-9
- Christopher-Dwyer K, Scanlon KG, Crimlisk JT. Critical Care Resource Nurse Team: A Patient Safety and Quality Outcomes Model. Dimensions of Critical Care Nursing. 2022;41:46. https://doi.org/10.1097/DCC.0000000000000501
- Howell EA, Sofaer S, Balbierz A, Kheyfets A, Glazer KB, Zeitlin J. Distinguishing High-Performing From Low-Performing Hospitals for Severe Maternal Morbidity: A Focus on Quality and Equity. Obstet Gynecol. 2022;139:1061–9. https://doi.org/10.1097/AOG.0000000000004806
- Bass BM, Riggio RE. Transformational Leadership. Psychology Press; 2006.
- Hasan AA, Ahmad SZ, Osman A. Transformational leadership and work engagement as mediators on nurses’ job performance in healthcare clinics: work environment as a moderator. Leadersh Health Serv (Bradf Engl). 2023;36:537–61. https://doi.org/10.1108/LHS-10-2022-0097
- Wang H-F, Chen Y-C, Yang F-H, Juan C-W. Relationship between transformational leadership and nurses’ job performance: The mediating effect of psychological safety. Social Behavior and Personality: an international journal. 2021;49:1–12. https://doi.org/10.2224/sbp.9712
- Wijayanti K, Aini Q. The Influence of Transformational Leadership Style to Nurse Job Satisfaction and Performance in Hospital. Journal of World Science. 2022;1:485–99. https://doi.org/10.58344/jws.v1i7.69
- Al-Rjoub S, Alsharawneh A, Alhawajreh MJ, Othman EH. Exploring the Impact of Transformational and Transactional Style of Leadership on Nursing Care Performance and Patient Outcomes. Journal of Healthcare Leadership. Dove Medical Press; 2024;16:557–68. https://doi.org/10.2147/JHL.S496266
- Mekonnen M, Bayissa Z. The Effect of Transformational and Transactional Leadership Styles on Organizational Readiness for Change Among Health Professionals. SAGE Open Nursing. SAGE Publications Inc; 2023;9:23779608231185923. https://doi.org/10.1177/23779608231185923
- Suwarno B. Analysis Head Nurses’ Leadership Styles to Staff Inpatient Nurses’ Job Performance in Hospital. International Journal of Science, Technology & Management. 2023;4:317–26. https://doi.org/10.46729/ijstm.v4i2.770
- Abujaber AA, Nashwan AJ, Santos MD, Al-Lobaney NF, Mathew RG, Alikutty JP, et al. Bridging the generational gap between nurses and nurse managers: a qualitative study from Qatar. BMC Nurs. 2024;23:623. https://doi.org/10.1186/s12912-024-02296-y
- Avolio BJ, Bass BM. Multifactor leadership questionnaire: manual and sample set. Third edition. Place of publication not identified: Mind Garden, Inc.; 2004.
- Sagherian K, Steege LM, Geiger-Brown J, Harrington D. The Nursing Performance Instrument: Exploratory and Confirmatory Factor Analyses in Registered Nurses. J Nurs Res. 2018;26:130–7. https://doi.org/10.1097/jnr.0000000000000215
- Kharazmi E, Bordbar N, Bordbar S. Distribution of nursing workforce in the world using Gini coefficient. BMC Nursing. 2023;22:151. https://doi.org/10.1186/s12912-023-01313-w
- State of the world’s nursing report 2025 [Internet]. 2025 [cited 2025 Sept 22]. https://www.who.int/publications/i/item/9789240110236. Accessed 22 Sept 2025
- Shen J, Guo Y, Chen X, Tong L, Lei G, Zhang X. Male nurses’ work performance: A cross sectional study. 2022;101:e29977. https://doi.org/10.1097/MD.0000000000029977
- Al-Hasnawi AA, Aljebory MKA. Relationship between nurses’ performance and their demographic characteristics. Journal Port Science Research. 2023;6:11–5. https://doi.org/10.36371/port.2023.1.3
- Hwang E, Yu Y. Effect of Sleep Quality and Depression on Married Female Nurses’ Work–Family Conflict. International Journal of Environmental Research and Public Health. Multidisciplinary Digital Publishing Institute; 2021;18:7838. https://doi.org/10.3390/ijerph18157838
- Turjuman F, Alilyyani B. Emotional Intelligence among Nurses and Its Relationship with Their Performance and Work Engagement: A Cross-Sectional Study. Alamri M, editor. Journal of Nursing Management. 2023;2023:1–8. https://doi.org/10.1155/2023/5543299
- Niri M al-SM, Khademian Z, Rivaz M. Nurses’ Performance as a Mediator Between Nurses’ Fatigue and Patient Safety Culture: A Structural Equation Model Analysis. Nursing Open. 2025;12:e70168. https://doi.org/10.1002/nop2.70168
- Al-Harazneh R, Abu shosha GM, Al-Oweidat IA, Nashwan AJ. The influence of job security on job performance among Jordanian nurses. International Journal of Africa Nursing Sciences. 2024;20:100681. https://doi.org/10.1016/j.ijans.2024.100681
- Ari HO. Determining the Relationship Between Work Stress and Job Performance: A Cross-Sectional Study Among Healthcare Workers. Journal of Nursing Management. 2025;2025:5051149. https://doi.org/10.1155/jonm/5051149
![]() This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
SELF-CARE KNOWLEDGE, BEHAVIORAL PRACTICES, AND PREVENTIVE STRATEGIES FOR DIABETIC FOOT ULCERS AMONG INDIVIDUALS WITH DIABETES IN TERTIARY HOSPITALS IN NIGERIA: A CROSS-SECTIONAL STUDY
Oseni Rukayat Ejide ¹, Emmanson Emmanson ²*, Kolawole Ifeoluwapo ¹,
Adejumo Prisca1, Obilor Helen3
- Department of Nursing Sciences, University of Ibadan, Nigeria
- Department of Human Anatomy, University of Cross River State, Nigeria
- School of Nursing, Queen’s University, Kingston, Ontario, Canada
* Corresponding Author: Emmanson Emmanson, Department of Human Anatomy, University of Cross River State, Nigeria. Email: emmansonemmanson35@gmail.com. ORCID: https://orcid.org/0009-0006-7285-7574
Cite this article
ABSTRACT
Introduction: The increasing prevalence of diabetes is a global public health concern, with foot ulcer prevention techniques, low self-care knowledge, and a lack of confidence contributing to complications like foot ulcers.
Methods: This cross-sectional study, conducted between January and December 2022, evaluated foot self-care knowledge, self-efficacy, and self-care behaviors among individuals with diabetes attending public tertiary hospitals in Abeokuta, Nigeria. Data from randomly selected 120 out-patients was collected using a multidimensional questionnaire, and multiple regression analysis was used to assess associations between variables.
Results: It was found that participants’ mean age was 44.8±14.65 years. Majority (58.3%) of them did not attend foot self-care education classes and had received a type-2 diabetes diagnosis within the previous 24 months. Many of the patients had low knowledge of foot self-care (55%), low self-care efficacy (55%) and poor self-care behavior (55%). Poor self-care behavior was predicted by low efficaciousness (p<0.0001) and low knowledge of foot self-care (p<0.0001).
Conclusion: The study concluded that the extent of knowledge significantly influenced self-care behaviors and the efficacy of foot self-care in averting diabetic foot ulcers. Improving these behaviors requires teaching appropriate knowledge through hands-on self-care treatments and gaining support from policymakers for its sustainability.
Keywords: Diabetes Foot Ulcer, Self-Care Knowledge, Efficacy, Behavior, Confidence.
INTRODUCTION
With an increasing prevalence, diabetes mellitus has become a global public health concern [1]. It raises mortality, illness, and medical expenses [1,2]. There are 537 million adults (20–79 years old) worldwide with diabetes as reported by International Diabetes Federation (IDF) [1]. Conversely, by 2060, the incidence of diabetes is expected to increase to 700% for type II and 65% for type I, according to the Centers for Disease Control and Prevention [3]. Additionally, diabetes is thought to be the cause of 6.7 million fatalities annually [1], with 1.5 million of those deaths occurring primarily in low- and middle-income nations [4].
According to IDF data from 2021, 1 in 22 adult Africans has diabetes, and 54% of Africans have diabetes but have not been diagnosed [1]. In Nigeria, the prevalence of diabetes rose from 2.2% in 1997 to over 6% in 2015, a more than 100% increase, according to World Health Organization (WHO) [5]. The IDF stated that the sub-Saharan region had the greatest estimated prevalence of diabetes, at 3,623,500 (3.7%). The prevalence rates of diabetic foot ulcers (DFU) in Nigeria vary from 11% to 32%, according to Ugwu et al. [6]. The rising rate of diabetes in Nigeria has been mostly linked to demographic shifts, including urbanization, the adoption of unsafe habits, poor diets that include sugar-sweetened beverages, inactivity, and dangerous alcohol and tobacco use [5,6]. This has also led to complications such as diabetic foot ulcers. This necessitates investigating the level of knowledge of people with diabetes mellitus (PWDM) on foot ulcer preventive self-care activities in selected hospitals in Abeokuta.
Millions of individuals worldwide are impacted by the dangerous side effect of diabetes called diabetic foot ulcers. It is lethal and can cause gangrene, infection, ischemia problems, neuropathy, macrovascular disease, and microvascular damage. According to Robles et al. [7], DFU is a challenging, expensive, and chronic health problem that increases morbidity and death. According to Oliver and Mutlouglu [8], ulcers are typically persistent and can occur in inpatient as well as outpatient environments. An array of variables, such as male gender, diabetes for over a decade, the advanced age of the patients, obesity, dry skin, insufficient circulation, underpinning nerve damage, callus formation, foot defects, improper foot hygiene, and poorly fitting shoes, are linked to the development of DFU, according to Khan, Khan, & Farooqui [9] and Oliver & Mutlouglu, [8]. Despite being controllable through education, it is the most costly and fatal event related with lower extremity amputation (LEA) and frequently associated with high morbidity and death [6]. Families and societies are consequently forced to bear a greater financial burden [10,11]. Other adverse effects include poor quality-of-life [12, 13]. In light of these burdens, it is important to assess how confident PWDM are in their ability to avoid foot ulcers in the selected hospitals. Therefore, this study assumes there is no significant association between efficacy and behavior of PWDM.
According to Sari et al. [14], poor foot self-care is the main factor contributing to DFU, while appropriate foot self-care can cut the risk of DFU, hospital stays, and amputations by 50%. Client-focused education on self-efficacy in FSC practices should be promoted in a time- and cost-effective manner, as continuous physician supervision is not always possible [15]. For this reason, Adeyemi et al. [16] proposed that appropriate foot care methods and patient education can avoid or lower the risk for DFU in the interim. Previous studies [9,14,17,18] revealed low to moderate foot care practice, inadequate understanding of DFU, and attitudes toward foot care prevention. People with diabetes mellitus in Sub-Saharan Africa also showed fair but insufficient awareness of diabetic foot care [19]; this is comparable to what is available in other parts of the world. Research on effective FSC behavior is still limited, and incidence of DFU, limb loss, and DFU-related premature death have increased in Nigeria. Similar to what was found by Ojewale, Okoye, and Ani [20], their study on FSC behavior and self-efficacy among PWDM in the University College Hospital, Nigeria, revealed a scarcity of investigations. Consequently, research on PWDM self-care knowledge, efficacy, and behavior is crucial. It is therefore important to explore the foot self-care behavior of PWDM in selected hospitals. In line with this, the study tested the hypothesis that there is no significant association between age, gender, educational status and behavior of FSC among PWDM, and that there is no significant association between knowledge of FSC and the behavior of PWDM. Thus, with the goal to prevent foot ulcers, this study assessed PWDM's self-care knowledge, efficacy, and behavior.
MATERIALS AND METHODS
Study design
This is a cross-sectional descriptive study which assessed the FSC knowledge, self-care efficacy and behavior of PWDM toward DFU prevention in Federal Medical Hospital (FMC), and State Hospital, Ijaiye, Abeokuta, Nigeria, between January and December 2022.
Target population
This included PWDM (type 1 and 2) in the selected hospitals.
Study population
PWDM who attended outpatient clinics, who were estimated to be 200 monthly in FMC, and 120 monthly in the State Hospital, Ijaiye, Abeokuta, respectively.
Inclusion criteria
Adult PWDM male and female aged 18 years and above managed for at least three months, that attended OPD clinic of FMC and State Hospital, Ijaiye, Abeokuta and gave consent to participate were included in the study.
Exclusion criteria
PWDM with existing DFU, those critically ill, and those on admission were excluded from the study.
Sample size estimation
The minimum sample size was determined using Cochran’s formula for estimating proportions in large populations:
where:
n0 = initial sample size, Z = standard normal deviation at 95% confidence (1.96), p = estimated proportion of the population with the attribute, q = 1 – p, e = desired margin of error.
Since no prior prevalence estimate of foot-care knowledge among individuals with diabetes in Abeokuta was available, the study used p = 50%. This value is conventionally used when there is insufficient prior data, as it maximizes sample size and increases precision. The margin of error was set at e = 10%. Based on previous values the estimated sample size is:

Additionally, a 20% attrition rate (AR) was included:
![]()
Thus, the final sample size used in this study was 120. Particularly, we adopted a relatively large margin of error (e=10%) and an attrition rate of 20%, as this is an explorative study.
Sampling technique
Two out of the three hospitals in Abeokuta; Federal Medical Center, Abeokuta and State Hospital, Ijaiye were selected using random sampling technique. A total of 120 participants were later recruited from the 2 hospitals.
Instrument for data collection
Data was obtained from respondents using structured and validated questionnaires, the questionnaire was in three sections. Section A addressed demographic data and knowledge of FSC. Section B assessed FSC behavior activities using a validated 26-item self-report tool adapted form of Nottingham Assessment of Functional Foot-care (NAFFS) [21]. While section C addressed the question on foot care efficacy using an adapted 12-item Foot Care Confidence Scale (FCCS) by Sloan Helen L. (2002) [22].
Validity of the instrument
The instrument was subjected to face and construct validity by thorough scrutiny by the researcher’s supervisor and expert clinician caring for PWDM and DFU. The multidimensional validated questionnaire containing sections on FCCS and NAFFS was subjected to forward and backward translation to Yoruba and English to ensure their validity. The items in each section of the instrument were further subjected to content validity testing by submitting the instrument to five experts and using Lawshe's formula to ensure the content validity ratio (CVR) for each item in each section of the instrument, resulting in the content validity index (CVI) for each section. According to Ayre and Sally (2013) [23], the CVR (content validity ratio) proposed by Lawshe (1975) [24] is a linear transformation of a proportional level of agreement on how many “experts” within a panel rate an item “essential” calculated in the following way:
CVR is the content validity ratio, ne is the number of panel members indicating an item “essential,” and N is the number of panel members.Just like r, CVR ranges between -1 through 0 to +1.
The closer to +1 is CVR for an item; the more valid is the item in the scale while CVR values closer to 0 imply lack of content validity. However, CVI is computed by dividing sum of CVR values by the total number of items. CVI is interpreted for the scale the same way CVR values are interpreted for the items. Table 1 displayed the CVIs for the relevant sections of the multidimensional instrument:
|
Instrument |
Number of Items |
Content Validity Index (CVI) |
Comment |
|
Foot Self-care Knowledge scale |
7 |
0.84 |
Valid |
|
FCCS |
12 |
0.76 |
Valid |
|
NAFFS |
26 |
0.86 |
Valid |
Table 1. Validity table
Reliability of the instrument
The reliability of the knowledge part of the questionnaire in section A was established using the Kuder Richardson formula- 20, KR20 conducted on SPSS Version 23 because of the dichotomous nature of the items in the section of the multidimensional instrument. Though the other 2 validated instruments, FCCS and NAFFS reportedly had Cronbach’s alpha reliability indices of 0.92 and 0.91 respectively, but all these instruments were revalidated by administering them on a sample of 30 respondents similar to but entirely different from those recruited for the main study. The reliability index obtained for the instruments was > 0.9 (Table 2).
|
Instrument |
Number of items |
Cronbach Alpha/KR20 |
Comment |
|
Foot Self-care Knowledge scale |
7 |
0.972 |
Sufficiently Reliable |
|
FCCS |
12 |
0.996 |
Sufficiently Reliable |
|
NAFFS |
26 |
0.997 |
Sufficiently Reliable |
Table 2. Reliability indices for the variables in the multidimensional instrument
Method of data collection
After gaining approval from the two institutions' ethical committee, the individual's informed consent, and permission from the head of the OPD at both, the instruments for data collection were given to study participants on clinic days over the course of four months (July to October, 2023), two research assistants attended a two-day training session where they learned about the objectives of the study, the content of foot care and DFU prevention guidelines/standards, FSC behavior and self-efficacy tools, and how to distribute the questionnaires. They were selected from among the registered nurses who care for patients with diabetes and DFU at Sacred Heart Hospital, Lantoro. Targeting their clinic hours on Mondays and Wednesdays, the study settings (FMC and State Hospital, Ijaye, respectively) were visited in the morning. As soon as the surveys were completed, they were gathered. People who were illiterate were helped to complete the surveys by having them translated into their native tongue.
Method of data analysis
Descriptive statistics such as means and standard deviations were used for continuous variables, while frequencies and percentages were used for categorical variables.
Responses to attitudinal or perception-based questions were measured using a 5-point Likert scale (1 = Strongly Disagree, 2 = Disagree, 3 = Neutral, 4 = Agree, 5 = Strongly Agree). Where applicable, composite scores were computed, and the scale reliability was assessed using Cronbach’s alpha.
Inferential statistics, including chi-square tests for categorical variables and independent t-tests or ANOVA for comparing group means, were applied where appropriate.
Statistical significance was set at p < 0.05. Data were entered and analyzed using IBM SPSS Statistics version 23.0 (IBM Corp., Armonk, NY, USA).
RESULTS
One hundred and twenty questionnaires were administered to the respondents, same received and used for analysis.
|
Characteristics |
Categories |
n (%) |
Mean |
SD |
|
Age (years) |
21–30 |
28 (23.3) |
||
|
31–40 |
24 (20.0) |
|||
|
41–50 |
21 (17.5) |
|||
|
51–60 |
26 (21.7) |
44.8 |
14.65 |
|
|
61–70 |
17 (14.2) |
|||
|
>70 |
4 (3.3) |
|||
|
Gender ᵃ |
Female |
85 (70.8) |
1.29 |
0.46 |
|
Male |
35 (29.2) |
|||
|
Marital status ᵇ |
Single |
30 (25.0) |
2.13 |
0.90 |
|
Married |
55 (45.8) |
|||
|
Separated/Divorced |
24 (20.0) |
|||
|
Widowed |
11 (9.2) |
|||
|
Educational status ᶜ |
No formal education |
28 (23.3) |
2.55 |
1.13 |
|
Primary |
31 (25.8) |
|||
|
Secondary |
28 (23.3) |
|||
|
Tertiary |
33 (27.5) |
|||
|
Occupation ᵈ |
Unemployed |
28 (23.3) |
2.53 |
1.08 |
|
Farming |
28 (23.3) |
|||
|
Trading |
37 (30.8) |
|||
|
Civil servant |
27 (22.5) |
|||
|
Type of diabetes ᵉ |
Type 1 |
50 (41.7) |
1.58 |
0.50 |
|
Type 2 |
70 (58.3) |
|||
|
Duration since diagnosis ᶠ |
1–24 months |
87 (72.5) |
1.47 |
0.87 |
|
25–48 months |
17 (14.2) |
|||
|
49–72 months |
9 (7.5) |
|||
|
>72 months |
7 (5.8) |
|||
|
Previous foot–care education ᵍ |
Yes |
50 (41.7) |
1.58 |
0.50 |
|
No |
70 (58.3) |
|||
|
Foot-care frequency ʰ |
Once a week |
16 (13.3) |
2.75 |
1.59 |
|
2–6 times/week |
22 (18.3) |
|||
|
Once a day |
8 (6.7) |
|||
|
>1 time/day |
4 (3.3) |
|||
|
Not applicable |
70 (58.3) |
|||
|
Knowledge of foot care ⁱ |
No idea |
72 (60.0) |
0.48 |
0.65 |
|
Moderate idea |
38 (31.7) |
|||
|
Expert idea |
10 (8.3) |
|||
|
Performs foot care independently ʲ |
Yes |
87 (72.5) |
1.28 |
0.45 |
|
No |
33 (27.5) |
|||
|
**If No, who helps? **ᵏ |
Family |
31 (25.8) |
2.02 |
0.98 |
|
Friends |
2 (1.7) |
|||
|
Not applicable |
87 (72.5) |
Table 3. Sociodemographic characteristics of 120 respondents (Source: Field survey, 2023)
Table 3 showed the demographic distribution of the respondents. The majority 28 (23.1%) of them are in the age group of 21-30 years, while the 4 (3.3%) that were above 70 years were the least in the distribution with the mean age of 44.8±14.65 years. About three-quarters 85 (70.8%) are female, while 35 (29.2%) are male. The majority were married, 55 (45.8%), and 30 (25%) are single. Most of the respondents had higher education 33 (27.5%), while both illiterates and secondary school completers were 28 (23.3%), respectively. Traders were more than other categories at 37 (30.8%) followed by civil servants at 27 (22.5%).
As shown further in Table 3, more than half 70 (58.3%) of the respondents had T2DM with majority 87 (72.5%) diagnosed within the past 24 months. Findings also revealed that 50 (41.7%) of the respondents had prior attendance at FSC education while 70 (58.3%) had no such experience. A few, 16 (13.3%), 22 (18.3%), 8 (6.7%) and 4 (3.3%) of the participants attended once a month, every other month, whenever chanced, and when reminded respectively, while this was not applicable to 70 (58.3%) of them. The majority, 72 (60.0%) of the participants had no idea know what foot care is, 38 (31.7%) had moderate idea while 10 (8.3%) claimed to have expertise idea. Finally, 87 (72.5%) performed foot care by themselves while 33 (27.5%) did not.
Respondents’ knowledge of foot self-care
|
Item |
No |
Yes |
|
|
People with diabetes should check their feet at least once a day |
77(64.2%) |
43(35.8%) |
|
|
People with diabetes should inspect their toes, nails, and cut it straight |
77(64.2%) |
43(35.8%) |
|
|
The feet should be washed, and lotion applied to moisturize them |
77(64.2%) |
43(35.8%) |
|
|
People with diabetes should warm their feet with lantern |
66(55%) |
54(45%) |
|
|
Before putting on shoes, people with diabetes should inspect the interior of them |
76(63.3%) |
44(36.7%) |
|
|
Foot corn/callus should be removed with razor blade |
76(63.3%) |
44(36.7%) |
|
|
People with diabetes should wear shoes that are not too tight |
76(63.3%) |
44(36.7%) |
Table 4. Knowledge of 120 respondents on foot self-care (Source: Field survey, 2023)
From table 4 the majority 77 (64.2%) of the participants declined that, PWDM should check their foot once daily, inspect their toes, nails, and cut it straight and the feet should be washed, and lotion applied to moisturize them. A little above half 66 (55.0%) disagreed with the statement that PWDM should warm their feet with lantern. Additionally, 44 (36.7%) of the respondents indicated that PWDM should wear shoes that are not too tight, remove corns and calluses from their feet with a razor blade, and check the inside of their shoes before wearing them.
Summary of respondents’ knowledge about foot self-care
Overall, the mean knowledge score was 9.63+3.08. As shown in Figure 1, 55% of the respondents had low level of knowledge of foot care, 17.5% of them had moderate knowledge while only 27.5% of them had high knowledge of foot self-care.
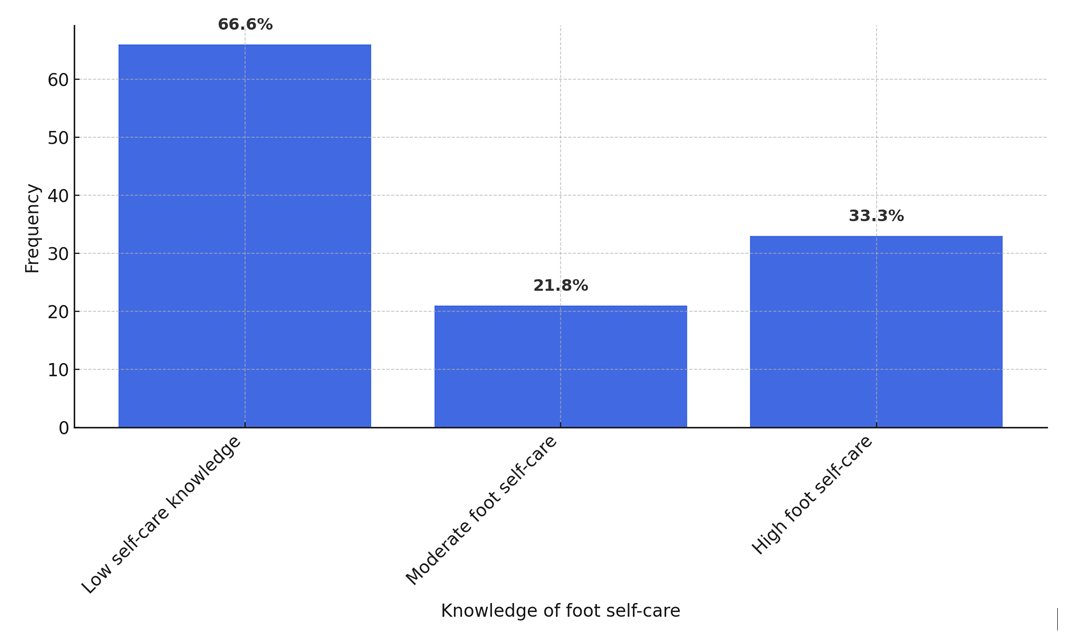
Figure 1. Respondents’ level of knowledge about foot self-care
Self-efficacy to practice foot ulcer preventive activities among patients
|
|
Strongly not confident |
Moderately not confident |
Confident |
Moderately confident |
Strongly confident |
|
f (%) |
f (%) |
f (%) |
f (%) |
f (%) |
|
|
I can protect my feet |
66 (55%) |
0 (0%) |
11 (9.2%) |
32 (26.7%) |
11 (9.2%) |
|
I can examine my feet every day to check for cuts, scratches, blisters, redness, or dryness even if I'm not in pain or uncomfortable. |
66 (55%) |
0 (0%) |
11 (9.2%) |
32 (26.7%) |
11 (9.2%) |
|
I can determine when to use a pumice stone to smooth corns and/or calluses on my feet. I can dry between my toes after washing my feet. I can determine when my toenails need to be clipped by a podiatrist. |
66 (55%) |
0 (0%) |
11 (9.2%) |
32 (26.7%) |
11 (9.2%) |
|
Prior to dipping my feet into the water, I may check the water's temperature. |
66 (55%) |
0 (0%) |
11 (9.2%) |
32 (26.7%) |
11 (9.2%) |
|
Even when I'm not in pain or uncomfortable, I may examine my feet daily to look for cuts, scratches, blisters, redness, or dryness. |
66 (55%) |
0 (0%) |
11 (9.2%) |
32 (26.7%) |
11 (9.2%) |
|
I am able to judge when to use a pumice stone on my foot to remove calluses and/or corns. After washing my feet, I can pat dry between my toes. I am able to tell when a podiatrist is necessary to trim my toenails. |
66 (55%) |
0 (0%) |
0 (0%) |
43 (35.8%) |
11 (9.2%) |
|
I could take a look at the water's temperature before putting my feet in it. |
66 (55%) |
0 (0%) |
0 (0%) |
44 (36.7%) |
10 (8.3%) |
|
If I was told to do so, I can wear shoes and socks every time I walk (includes walking indoors) |
66 (55%) |
0 (0%) |
10 (8.3%) |
44 (36.7%) |
0 (0%) |
|
When I go shopping for new shoes, I can choose shoes that are good for my feet |
66 (55%) |
0 (0%) |
10 (8.3%) |
44 (36.7%) |
0 (0.0%) |
|
I can call my doctor about problems with my feet |
66 (55%) |
0 (0%) |
0 (0%) |
44 (36.7%) |
10 (8.3%) |
|
I can check the insides of my shoes for problems that can harm my feet before putting them on |
55 (45.8%) |
11 (9.2%) |
11 (9.2%) |
33 (27.5%) |
10 (8.3%) |
|
I can routinely apply lotion on my feet if directed to do so |
55 (45.8%) |
11 (9.2%) |
11 (9.2%) |
22 (18.3%) |
21 (17.5%) |
Table 5: Measure of confidence (Self-efficacy), N=120
As shown in Table 5, 66 (55.0%), 0 (0.0%), 11 (9.2%), 32 (26.7%) and 11 (9.2%) of the participants responded that, they were strongly not confident, moderately not confident, confident, moderately confident and strongly confident respectively to each of items ‘I can protect my feet’, ‘even without pain/discomfort, I can look at my feet daily to check for cuts, scratches, blisters, redness or dryness’, ‘After washing my feet, I can dry between my toes’, ‘I can judge when my toenails need to be trimmed by a podiatrist’, ‘I can trim my toenails straight across’, and ‘I can figure out when to use a pumice stone to smooth corns and/or calluses on my feet’. Majority of the participants agreed they were strongly not confident, moderately not confident, confident, moderately confident and strongly confident respectively to item which stated, "I can test the water's temperature before putting my feet into it". Overall, the mean self-efficacy score was 28.47±18.19.
|
Behavior Item |
Response Options |
f (%) |
|
Examination & Hygiene |
||
|
How often do you examine your feet? |
Once a week |
11 (9.2) |
|
2–6 times a week |
55 (45.8) |
|
|
Once a day |
21 (17.5) |
|
|
More than once a day |
33 (27.5) |
|
|
Do you check your shoes before you put them on? |
Once a week |
11 (9.2) |
|
2–6 times a week |
55 (45.8) |
|
|
Once a day |
21 (17.5) |
|
|
More than once a day |
33 (27.5) |
|
|
Do you check your shoes when you take them off? |
Once a week |
33 (27.5) |
|
2–6 times a week |
33 (27.5) |
|
|
Once a day |
21 (17.5) |
|
|
More than once a day |
33 (27.5) |
|
|
Do you wash your feet? |
Once a week |
33 (27.5) |
|
2–6 times a week |
33 (27.5) |
|
|
Once a day |
21 (17.5) |
|
|
More than once a day |
33 (27.5) |
|
|
Do you check feet are dry after washing? |
Once a week |
33 (27.5) |
|
2–6 times a week |
33 (27.5) |
|
|
Once a day |
21 (17.5) |
|
|
More than once a day |
33 (27.5) |
|
|
Do you dry between toes? |
Once a week |
33 (27.5) |
|
2–6 times a week |
33 (27.5) |
|
|
Once a day |
21 (17.5) |
|
|
More than once a day |
33 (27.5) |
|
|
Do you use moisturizing cream on your feet? |
Once a week |
33 (27.5) |
|
2–6 times a week |
33 (27.5) |
|
|
Once a day |
21 (17.5) |
|
|
More than once a day |
33 (27.5) |
|
|
Do you apply cream between toes? |
Once a week |
33 (27.5) |
|
2–6 times a week |
33 (27.5) |
|
|
Once a day |
21 (17.5) |
|
|
More than once a day |
33 (27.5) |
|
|
Are your toenails cut? |
Once a week |
33 (27.5) |
|
2–6 times a week |
33 (27.5) |
|
|
Once a day |
21 (17.5) |
|
|
More than once a day |
33 (27.5) |
|
|
Footwear Habits |
||
|
Do you wear unfastened slippers? |
Most of the time |
33 (27.5) |
|
Sometimes |
33 (27.5) |
|
|
Rarely |
10 (8.3) |
|
|
Never |
44 (36.7) |
|
|
Do you wear sneakers? |
Most of the time |
33 (27.5) |
|
Sometimes |
33 (27.5) |
|
|
Rarely |
10 (8.3) |
|
|
Never |
44 (36.7) |
|
|
Do you wear shoes with straps, Velcro, or lace-up closures? |
Most of the time |
33 (27.5) |
|
Sometimes |
33 (27.5) |
|
|
Rarely |
21 (17.5) |
|
|
Never |
33 (27.5) |
|
|
Do you wear shoes with pointy toes? |
Most of the time |
33 (27.5) |
|
Sometimes |
33 (27.5) |
|
|
Rarely |
21 (17.5) |
|
|
Never |
33 (27.5) |
|
|
Do you dress in mules or flip-flops? |
Most of the time |
33 (27.5) |
|
Sometimes |
33 (27.5) |
|
|
Rarely |
21 (17.5) |
|
|
Never |
33 (27.5) |
|
|
Is it customary to break in new shoes gradually? |
Always |
22 (18.3) |
|
Most of the time |
44 (36.7) |
|
|
Sometimes |
21 (17.5) |
|
|
Rarely/Never |
33 (27.5) |
|
|
Do you wear synthetic socks (e.g., nylon)? |
Most of the time |
22 (18.3) |
|
Sometimes |
44 (36.7) |
|
|
Rarely |
21 (17.5) |
|
|
Never |
33 (27.5) |
|
|
Do you wear shoes without socks/tights? |
Never |
22 (18.3) |
|
Rarely |
44 (36.7) |
|
|
Sometimes |
21 (17.5) |
|
|
Often |
33 (27.5) |
|
|
How often do you replace socks/tights? |
< 4 times/week |
33 (30.3) |
|
4–6 times/week |
21 (19.3) |
|
|
Daily |
33 (30.3) |
|
|
> once/day |
22 (20.2) |
|
|
Barefoot Practices & First Aid |
||
|
Do you go barefoot at home? |
Often |
11 (9.2) |
|
Sometimes |
55 (45.8) |
|
|
Rarely |
21 (17.5) |
|
|
Never |
33 (27.5) |
|
|
Are you barefoot outside? |
Often |
22 (18.3) |
|
Sometimes |
44 (36.7) |
|
|
Rarely |
32 (26.7) |
|
|
Never |
22 (18.3) |
|
|
Do you use a hot water bottle in bed? |
Often |
22 (18.3) |
|
Sometimes |
44 (36.7) |
|
|
Rarely |
32 (26.7) |
|
|
Never |
22 (18.3) |
|
|
For corns, do you use home treatments (e.g., plasters)? |
Never |
22 (18.3) |
|
Rarely |
44 (36.7) |
|
|
Sometimes |
21 (17.5) |
|
|
Often |
33 (27.5) |
|
|
For blisters, do you use a dry dressing? |
Never |
22 (18.3) |
|
Rarely |
44 (36.7) |
|
|
Sometimes |
10 (8.3) |
|
|
Often |
44 (36.7) |
|
|
For cuts/grazes/burns, do you use a dry dressing? |
Never |
22 (18.3) |
|
Rarely |
44 (36.7) |
|
|
Sometimes |
21 (17.5) |
|
|
Often |
33 (27.5) |
Table 6. Respondents’ foot self-care behavior/activities, N=120.
As shown in Table 6, 11 (9.2%), 55 (45.8%), 21 (17.5%) and 33 (27.5%) consented that, they examined their feet and check their shoes before they put them on once a week, 2 – 6 times a week, once a day and more than once a day respectively. Also, 33 (27.5%), 33 (27.5%), 21 (17.5%) and 33 (27.5%) responded once a week, 2 – 6 times a week, once a day and more than once a day respectively to each of items; "Do you wash your feet?" "Do you check that your feet are dry after washing?" "Do you dry between your toes?" "Do you use moisturizing cream on your feet?" "Do you use moisturizing cream between your toes?" and "Are your toenails cut?" - for each item, 33 (27.5%), 33 (27.5%), 10 (8.3%), and 44 (36.7%) of the participants gave their response most of the time, occasionally, seldom, and never, respectively. For questions on "Do you wear trainers?" and "Do you wear slippers without fastenings?" - 33 (27.5%), 21 (17.5%), 33 (27.5%), and 33 (27.5%) of the participants answered each item most of the time, seldom, infrequently, and never, respectively.
For the question, ‘Do you break in new shoes gradually?’, 22 (18.3%), 44 (36.7), 21 (17.5%) and 33 (27.5%) of the subjects responded always, most of the time, sometimes and rarely/never respectively. Similarly, 22 (18.3%), 44 (36.7), 21 (17.5%) and 33 (27.5%) responded most of the time, sometimes, rarely and never respectively to “Do you wear artificial fiber (e.g., nylon) socks. The response pattern was also 22 (18.3%), 44 (36.7), 21 (17.5%) and 33 (27.5%) implying never, rarely, sometimes and often respectively for question ‘Do you wear shoes without socks/stockings/tights?’ ‘Do you change your socks/stockings/tights?’ got the response pattern, 22 (20.2%), 33 (30.3%), 21 (19.3%) and 33 (30.3%) implying more than once a day, daily, 4-6 times a week and less than 4 times a week respectively for a total of 109 responses for the item.
Items ‘Do you walk around the house in bare feet?’ and ‘Do you walk outside in bare feet?’ turned in the response pattern, 11 (9.2%), 55 (45.8), 21 (17.5%) and 33 (27.5%) to denote often, sometime, rarely and never respectively. Also, 22 (18.3%), 44 (36.7%), 32 (26.7%) and 22 (18.3%) gave the responses, often, sometime, rarely and never respectively to item "Do you use a hot water bottle in bed?", item "Do you place your feet close to the flames?" and "Do you place your feet on a radiator?". For item ‘Do you use corn remedies/ corn plasters/paints when you get a corn?’ and item ‘Do you put a dry dressing on a graze, cut or burn when you get one?’, 22 (18.3%), 44 (36.7%), 21 (17.5%) and 33 (27.5%) of the participants responded, never, rarely, sometimes and often respectively to each of the items. On the other hand, the responses to the question, "Do you put a dry dressing on a blister when you get one?" were as follows: 22 (18.3%), 44 (36.7%), 10 (8.3%), and 44 (36.7%). Whereas the mean of 39.34±27.57 was obtained for respondents’ foot self-care behavior.
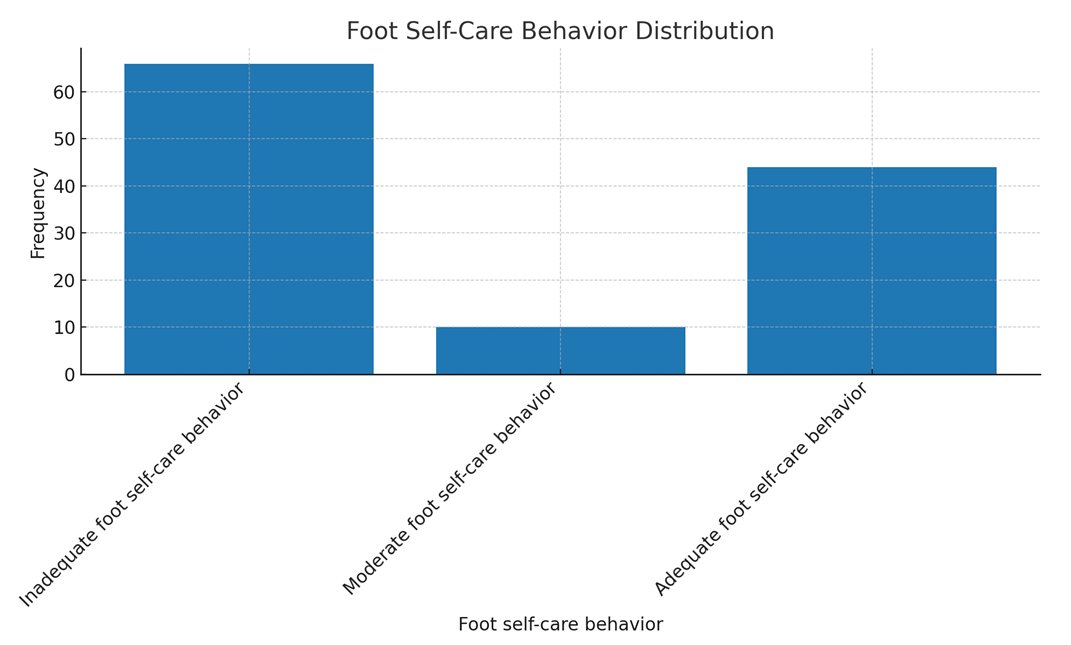
Figure 2. Respondents’ foot self-care behavior
As shown in Figure 2, 66(55%) of them had inadequate foot self-care behavior, only 10 (8.3%) of them had moderate foot self-care behavior, while 44 (36.7%) of the respondents had adequate foot self-care behavior.
Hypotheses testing
Ho: There is no significant individual and composite association between age, gender, educational status and behavior of FSC among PWDM.
|
Model |
Unstandardized Coefficients (B) |
Std. Error |
Standardized Coefficients (Beta) |
t |
Sig. (p-value) |
|
|
(Constant) |
38.543 |
7.692 |
5.011 |
<0.0001 |
||
|
Age |
2.622 |
6.077 |
0.133 |
0.432 |
0.667 |
|
|
Gender |
-1.078 |
9.246 |
-0.018 |
-0.117 |
0.907 |
|
|
Educational Status |
-2.089 |
8.227 |
-0.086 |
-0.254 |
0.800 |
|
|
Note: Dependent Variable = FSC Behavior |
||||||
Table 7. Multivariate analysis between age, gender, educational status and foot self-care behavioramongPWDM
As shown in Table 7, multiple regression analysis was conducted to predict the association between age, gender and educational status and self-care behavior. Particularly, by ANOVA summary for the Regression Model, the resultant model was not significant, F (3, 119) = 0.97, p = 0.962, R2= 0.002. Table 7 revealed that the individual variables also had no significant association of age (t = 0.432, p = 0.667), gender (t = -0.117, p = 0.907) and educational status (t = -0.254, p = 0.800) with FSC behavior.
As shown in Table 8, multiple regression analysis was conducted to test the association between knowledge of FSC, efficacy and self-care behavior of people with diabetes. Particularly, by ANOVA summary for the Regression Model, the resultant model for foot self-care efficacy and FSC knowledge against self-care behavior was significant, F (2, 119) = 589.764, p<0.0001, R2= 0.910.
Table 8 revealed that individual variables had significant association FSC knowledge (t =8.252, p<0.0001) and FSC efficacy (t =3.610, p<0.0001) with FSC behavior.
|
Predictor |
Unstandardized Coefficients (B) |
Std. Error |
Standardized Coefficients (Beta) |
t |
Sig. (p-value) |
|
(Constant) |
-31.312 |
3.983 |
– |
-7.861 |
<0.0001 |
|
Foot Self-Care Knowledge |
6.023 |
0.730 |
0.672 |
8.252 |
<0.0001 |
|
Foot Self-Care Efficacy |
0.446 |
0.123 |
0.294 |
3.610 |
<0.0001 |
|
Note: Dependent Variable = Foot Self-Care Behavior. |
|||||
Table 8. Multivariate analysis between Foot Self-Care Knowledge, Foot Self-Care Efficacy and Foot Self-Care Behavior amongPWDM
DISCUSSION
The current investigation discovered that very few participants were older than 70. This result contradicts the age-based rate reported by Odusan, Amoran, and Salami [25], who observed that the elderly have a higher prevalence of diabetes than youngsters. Nonetheless, the present result is consistent with the CDC's [26] assertion that the number of children, adolescents, and young adults developing DM is rising. The fact that many young people are leading improper lifestyles could help to explain this predicament. Some of these youths, who come from parents who are secure in terms of socioeconomic status yet reside in the city, lead unhealthy lives because they eat junk food and exercise infrequently. This scenario can make a good number of them to be diabetic. The study’s finding in concordance with previous research findings shows more females with diabetes, this agrees with Turan et al. [27] and Wazqar et al. [5] that more females are diagnosed with diabetes more than their male counterparts. Most of the respondents had higher education this is in agreement with Bekele [28] findings that higher educational status is one of the predictors of FSC practices. Majority were T2DM (53.8%) which corresponds with Sen et al. [29] and Wanja et al. [30], of which majority were diagnosed within the last 24 months.
The level of knowledge of PWDM on foot ulcer preventive self-care activities.
One of the main conclusions of this study was that the respondents' level of FSC knowledge was low. Consequently, there is a need for skilled instruction on diabetes FSC and the creation of guidelines for PWDM to carry out FSC. This conclusion runs counter to prior research by Alshammari et al. [31], who discovered that around 282 (76.6%) of the patients in their Riyadh, Saudi Arabia, study had a thorough awareness of foot ulcers and diabetic foot. The literature, however, provides a wealth of evidence to support the reported position of low knowledge of FSC. Goie and Naidoo [12] and Adeyemi et al. [16] for example, agreed with Ogunlana [29] when she stated that individuals with diabetes mellitus in Sub-Saharan Africa have a limited understanding of the complications associated with their disease. As Africans, we rely heavily on the rule of thumb in many situations, particularly in times of emergency when managing diabetes calls for it. Except for the standard, frequently ineffectual recommendations obtained during hospital visits, there are very few proactive steps available for managing the difficulties associated with diabetes in such circumstances. Thus, the creation of an out-of-hospital care regimen becomes necessary.
The self-efficacy of PWDM to practice foot ulcer preventive activities
The discovery that the majority of those who participated had poor FSC Efficacy scores is another indication of the growing mortality and morbidity linked to diabetes and its complications. People lack the abilities, bravery, and self-assurance necessary to combat, control, and overcome DFU, a serious symptom that causes suffering and casualties for diabetics. The findings in this study deviated from the seemingly typical trend, even though Narmawan, Syahrul, and Erika [32] and Sharoni et al. [33] had previously demonstrated that the patients in their studies had high FSC efficacy. Additional published research that supports the inherent deficiencies in FSC efficacy or parallel variables among diabetics include Wazqar et al. [5], Khan et al. [9], Mekonen and Demssie [34], and Turan et al. [27]. These studies were founded on evidentiary viewpoints. It is interesting to know why the present result in this study—which isn't generally praised in the literature—is what it is. However, the majority's low FSC efficacy is not surprising in the slightest because, despite claims to the contrary, a population lacking in knowledge cannot assert that it has high self-efficacy—a concept that is far higher than knowledge and that no conventional education can ensure. In summary, while knowing is crucial for self-care, it might not necessarily translate into self-efficacy. This suggests that educational initiatives that just emphasize knowledge may not result in self-efficacy, and it is unwarranted to assume that a lack of knowledge will lead to a lack of efficacy or self-confidence. This means that, if self-efficacy had been high, the participants in this study would have had low moment foot self-care knowledge.
Foot self-care behavior of people with diabetes
A significant finding of this study indicated that a considerable number of individuals had insufficient foot self-care practices. This leads to the primary rationale of this study. Low levels of self-care behavior are thought to be the underlying cause of DFU. The present finding of low self-care behavior with respect to DFU emphasizes the earlier position of Ammar et al. [35] that foot ulcers and amputations are regrettably prevalent with poverty, improper sanitation and hygiene, and barefoot walking often connecting to worsen the adverse effects of diabetic foot damage. Hirpha, Tatiparthi, and Mulugeta's [13] additional research, which observed that those with diabetes did not sufficiently self-inspect, wash their feet at least once a day, dry after washing, and moisturize the dry skin as they walked barefoot, in sandals or slippers, or in shoes without socks, supports the results under discussion. It is important to stress that the existing practice goes against the advice given by Armstrong et al. [36] and van Netten et al. [37], who provided factual evidence to support their recommendations regarding the importance of routine foot inspections for PWDM. The problem persists when the number of patients in need of health care services is not matched by the number of caregivers and health workers/educators currently in place. This documented anomaly is therefore not unrelated to the culture of unsanitary living, complacency, misinformation, and poor knowledge among some people.
The results demonstrated that foot self-care behavior was not predicted by age, gender, or educational attainment. While earlier research [33,32,20,38] suggested that specific age, gender, and educational level reinforce FSC behavior, the present investigation has documented the opposite for reasons that are closely related to the fact that care behavior is a personal matter, independent of known biases or socioeconomic inclinations.
The findings also highlight the importance of collaboration in attempts to instill the necessary skills and attitude to give the motivation needed for effective self-care behavior. Lastly, the significant individual and joint association of FSC knowledge and foot care self-efficacy with FSC behavior highlights the need for each of these factors to instill self-care behavior. In their research, Wendling and Beadle [39] showed that self-efficacy advancement is a successful nursing intervention for health promotion. Positive outcomes, such as better outcomes for people with diabetes mellitus, fewer admissions, and fewer ER visits, have been linked to this. Additionally, the study offered some limited understanding of the significance of the identified relationships. Support for the necessity of matching knowledge to practical skill training was given in 2016 by Sarkar et al. and Sharoni et al. [33], whose studies, respectively, demonstrated a major beneficial connection between self-efficacy and self-care practices among PWDM and an improvement in FSC behavior, foot care knowledge, foot care outcome expectation, and QoL (physical symptoms) after training.
CONCLUSION
Patients with diabetic foot ulcers (DM) frequently get DFU, and foot self-care (FSC) is a useful strategy to reduce this risk. But self-care is becoming more and more common because paid care services are expensive and there aren't many caregivers accessible. With an emphasis on young individuals aged 21 to 30, the research sought to assess FSC behavior for DM patients. Participants in the study had poor scores on behavior, efficacy, and knowledge assessments. Age, gender, and educational attainment did not significantly correlate with foot self-care behavior.
It is necessary to invest in educational interventions to provide patients with the skills and knowledge necessary for good foot care practices. These initiatives shouldn't, however, necessarily be classified according to factors like age, gender, or educational attainment. The results demonstrated a substantial correlation between efficacy and foot self-care behavior, indicating that increasing efficacy or FSC knowledge on its own might greatly enhance self-care behavior.
According to the study's findings, 91.1% of the variance in foot self-care behavior could be explained by knowledge of FSC and efficacy, which had a substantial composite connection with foot self-care behavior. In order to expedite the practice of foot self-care, educators must impart information of foot self-care (FSC) and its efficacy in addition to the requisite technology, scientific skills, practices, and artistic qualities. For greatest benefit, this will assist DM patients in initiating, managing, and engaging in self-care practices.
Based on the findings and discussions presented in this study, several important recommendations are proposed. Healthcare providers should prioritize expanding and promoting diabetes education programs that not only enhance patients' knowledge of foot self-care (FSC) but also strengthen self-efficacy by teaching practical skills and fostering confidence in patients' ability to carry out these activities. Patients must also be educated on the importance of choosing appropriate footwear, with a strong emphasis on the benefits of well-fitting shoes and the risks of walking barefoot, both indoors and outdoors, as a preventive measure against foot complications. In addition to education, healthcare professionals and educators are encouraged to implement strategies that boost patients' self-efficacy, such as goal-setting, individualized feedback, and supportive reinforcement that affirms their ability to manage self-care effectively.
Developing and distributing clear, concise self-care guidelines or protocols is essential, as is stressing the importance of regular foot examinations. Patients should be empowered to conduct daily foot checks and trained to identify signs such as cuts, blisters, or dryness that may require prompt attention. Furthermore, they should be cautioned against risky practices like using razor blades to remove corns and calluses and instead be encouraged to seek professional care for such concerns. Another important hygiene recommendation is to emphasize the necessity of changing socks regularly to maintain healthy foot conditions and prevent infections. These educational efforts should be institutionalized within healthcare policies at both national and facility levels, and embedded into healthcare training curricula for sustainable impact. Additional studies should be carried out to assess the effectiveness of foot care education, identify barriers to its implementation, and develop strategies to address these challenges.
Limitations and recommendations
The generalizability of the findings may be limited by factors such as sample size and study design, and future research should consider broadening the scope and incorporating multiple methodological approaches to enrich the validity of results. This study contributes to knowledge by showing that while knowledge is important, it alone is insufficient to improve patients’ foot self-care behavior unless it is reinforced by self-efficacy strategies and potentially other factors not examined in this research. It also presents evidence that differentiated learning based on age, gender, or education level may not be necessary for effective foot self-care training among patients. A key outcome of this study is the proposed knowledge-efficacy-behavior framework, which provides a conceptual basis for mastering diabetic foot self-care behavior.
In light of the study’s limitations and findings, further investigations are encouraged. Future researchers may consider integrating more independent variables—such as personal hygiene habits, coexisting health conditions, and access to healthcare services or information—into predictive models for foot self-care behavior. A quasi-experimental study design may also be employed to evaluate the effectiveness of targeted intervention packages on patients’ behavior. Additionally, new tools such as systematic observation instruments can be developed to complement the questionnaire method used in this study, offering a more comprehensive assessment of self-care practices.
Local Ethics Committee approval:
1. The study protocol was approved by the Research and Ethics Committee of Ogun State Hospital Management Board with REF NO: SHA 52/VOL XII/116. Date of approval: August 23, 2023.
2. The study protocol was approved by the Research and Ethics Committee of Federal Medical Center with REF NO: FMCA/470/HREC/01/2023/23NHREC/08/10-2015. Date of approval: June 19, 2023
Competing interests: None to declare.
Funding: This research received no external funding.
Authors’ contribution
Oseni Rukayat: Conceptualized idea and conducted full research.
Emmanson Emmanson: Assisted with the research and manuscript preparation for publication
Kolawole Ifeoluwapo:Assisted with the design of questionnaire and conducting interviews with the selected nurses.
Adejumo Prisca: Was responsible for literature reviews.
Obilor Helen: performed data analysis and edited the manuscript for publication.
REFERENCES
- International Diabetes Federation (2022). Diabetes around the world in 2021. 10th edition. https://diabetesatlas.org/#:~:text=1%20in%208%20adults%20(206,caused%20by%20diabetes%20in%202021. Accessed 24/02/2023.
- Paulsamy, P., Ashraf, R., Alshahrani, S. H. et al. (2021). Social Support, Self-Care Behaviour and Self-Efficacy in Patient with Type 2 Diabetes during the COVID- 19 Pandemic: A Cross-Sectional Study. National Library of Medicine. Healthcare (Basel). 9(11):1607. Doi:10.3390/healthcare9111607. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8622453/. Accessed 02/11/2023.
- Center For Disease Control and Prevention, (2023). Diabetes in Young People Is on the Rise. https://www.cdc.gov/diabetes/resources-publications/research-summaries/diabetes-young-people.html. Accessed 15/11/2023.
- World Health Organization, (2022). Diabetes. https://www.who.int/health-topics/diabetes#tab=tab_1. Accessed 05/06/2022.
- Wazqar AA, Baatya MM, Lodhi FS, Khan AA. Assessment of knowledge and foot self-care practices among diabetes mellitus patients in a tertiary care centre in Makkah, Saudi Arabia: a cross-sectional analytical study. Pan Afr Med J. 2021 Oct 29;40:123. doi: 10.11604/pamj.2021.40.123.30113. PMID: 36118942; PMCID: PMC9463747.
- Ugwu E, Adeleye O, Gezawa I, Okpe I, Enamino M, Ezeani I. Burden of diabetic foot ulcer in Nigeria: Current evidence from the multicenter evaluation of diabetic foot ulcer in Nigeria. World J Diabetes. 2019 Mar 15;10(3):200-211. doi: 10.4239/wjd.v10.i3.200. PMID: 30891155; PMCID: PMC6422858.
- Robles, R. B., Compean Ortiz, L. G., […] and Martinez, S. P. (2017). Knowledge and Practice of Diabetes Foot Care and Risk of Developing Foot Ulcers inMexico May Have Implications for Patients of Mexican Heritage Living in the US. SAGE Journals Vol 43, Issue 3. https://doi.org/10.1177/0145721717706417. Accessed 28/03/2023.
- Oliver, T I. and Mutlouglu, M. (2022). Diabetic Foot Ulcers. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan-. https://www.ncbi.nlm.nih.gov/books/NBK537328/.Accessed 24/07/2022.
- Khan, Y., M. Khan, M., & Raza Farooqui, M. (2017). Diabetic foot ulcers: a review of current management. International Journal of Research in Medical Sciences, 5(11), 4683–4689. https://doi.org/10.18203/2320-6012.ijrms20174916.
- Rahaman HS, Jyotsna VP, Sreenivas V, Krishnan A, Tandon N. Effectiveness of a Patient Education Module on Diabetic Foot Care in Outpatient Setting: An Open-label Randomized Controlled Study. Indian J Endocrinol Metab. 2018 Jan-Feb;22(1):74-78. doi: 10.4103/ijem.IJEM_148_17. PMID: 29535941; PMCID: PMC5838916.
- Boulton, Andrew. (2021). Diabetic Foot Disease during the COVID-19 Pandemic. Medicina. 57. 97. 10.3390/medicina57020097.
- Goie TT, Naidoo M. (2016). Awareness of diabetic foot disease amongst patients with type 2 diabetes mellitus attending the chronic out-patients department at a regional hospital in Durban, South Africa. Afr J Prm Health Care Fam Med. 8(1), a1170. http://dx.doi.org/10.4102/phcfm.v8i1.1170. Accessed 07/07/2022.
- Hirpha, N., Tatiparthi, R., and Mulugeta, T. (2020). Diabetic Foot Self-Care Practices Among Adult Diabetic Patients: A Descriptive Cross-Sectional Study. https://doi.org/10.2147/DMSO.S285929. Accessed 18/01/2023.
- Rural Health Information Hub (2020). Module 1: Health promotion and disease. Available at: https://www.ruralhealthinfo.org/toolkits/health-promotion/1/introduction. Last access: 02/01/2023.
- Mallorquí-Bagué, N., Lozano-Madrid, M., Toledo, E., Corella, D., Salas-Salvadó, J., Cuenca-Royo, A., ... & Fernández-Aranda, F. (2018). Type 2 diabetes and cognitive impairment in an older population with overweight or obesity and metabolic syndrome: baseline cross-sectional analysis of the PREDIMED-plus study. Scientific reports, 8(1), 16128 doi: 10.1038/s41598-018-33843-8.
- Adeyemi TM, Olatunji TL, Adetunji AE, Rehal S. Knowledge, Practice and Attitude towards Foot Ulcers and Foot Care among Adults Living with Diabetes in Tobago: A Qualitative Study. Int J Environ Res Public Health. 2021 Jul 29;18(15):8021. doi: 10.3390/ijerph18158021. PMID: 34360314; PMCID: PMC8345419.
- Mekonen EG, Gebeyehu Demssie T. Preventive foot self-care practice and associated factors among diabetic patients attending the university of Gondar comprehensive specialized referral hospital, Northwest Ethiopia, 2021. BMC Endocr Disord. 2022 May 11;22(1):124. doi: 10.1186/s12902-022-01044-0. PMID: 35546665; PMCID: PMC9097232.
- Tuha A, Getie Faris A, Andualem A, Ahmed Mohammed S. Knowledge and Practice on Diabetic Foot Self-Care and Associated Factors Among Diabetic Patients at Dessie Referral Hospital, Northeast Ethiopia: Mixed Method. Diabetes Metab Syndr Obes. 2021 Mar 17;14:1203-1214. doi: 10.2147/DMSO.S300275. PMID: 33762837; PMCID: PMC7982550.
- Ogunlana MO, Govender P, Oyewole OO, Odole AC, Falola JL, Adesina OF, Akindipe JA. Qualitative exploration into reasons for delay in seeking medical help with diabetic foot problems. Int J Qual Stud Health Well-being. 2021 Dec;16(1):1945206. doi: 10.1080/17482631.2021.1945206. PMID: 34219610; PMCID: PMC8259813.
- Ojewale, L.Y., Okoye, E. A. and Ani, O. B. (2021). Diabetes Self-Efficacy and Associated Factors among People Living with Diabetes in Ibadan, Southwestern Nigeria. European Journal of Medical and Health Sciences. Vol. 3 No. 6. https://doi.org/10.24018/ejmed.2021.3.6.1129.
- Lincoln, N., Jeffcoate, W., Ince, P., Smith, M. and Radford, K. (2007), Validation of a new measure of protective footcare behaviour: the Nottingham Assessment of Functional Footcare (NAFF). Pract Diab Int, 24: 207-211. https://doi.org/10.1002/pdi.1099
- Sloan HL. Developing and testing of the Foot Care Confidence Scale. J Nurs Meas. 2002 Winter;10(3):207-18. doi: 10.1891/jnum.10.3.207.52564. PMID: 12885146
- Ayre, C., & Scally, A. J. (2014). Critical values for Lawshe’s content validity ratio: Revisiting the original methods of calculation. Measurement and Evaluation in Counseling and Development, 47(1), 79–86. https://doi.org/10.1177/0748175613513808
- Lawshe, C. H. (1975). A quantitative approach to content validity. Personnel psychology, 28(4).
- Odusan, O., Amoran, O. E., & Salami, O.E. (2017). Prevalence and pattern of diabetic foot ulcers among adults with diabetes in a secondary health care facility in Lagos, Nigeria. Anals of health research:3(2). https://www.annalsofhealthresearch.com/index.php/ahr/article/view/70. Accessed 28/03/2023
- Center For Disease Control and Prevention, (2023). Diabetes in Young People Is on the Rise.https://www.cdc.gov/diabetes/resources-publications/research-summaries/diabetes-young-people.html. Accessed 15/11/2023
- Turan, E., Onalan, R., Iscimen, N. C., Ozan, Z. T., Yildirim, T., & Aral, Y. (2020). Foot Self-Care Behavior in Patients with Diabetes. J Soc Health Diab:2020;8:13-17 http://doi.org/10.1055/s-0040-1716812
- Bekele, F., Berhanu, D., Sefera, B., & Babu, Y. (2021). Diabetic foot self-care practices and its predictors among chronic diabetic mellitus patients of Southwestern Ethiopia hospitals: a cross-sectional study. https://doi.org/10.1016/j.ijans.2022.100489. Accessed 25/03/2023.
- Şen HM, Şen H, Aşık M, Özkan A, Binnetoglu E, Erbağ G, Karaman HI. The importance of education in diabetic foot care of patients with diabetic neuropathy. Exp Clin Endocrinol Diabetes. 2015 Mar;123(3):178-81. doi: 10.1055/s-0034-1389981. Epub 2014 Oct 14. PMID: 25314654.
- Wanja L, Mwenda C, Mbugua R, Njau S. (2019). Determinants of foot self-care practices among diabetic patients attending diabetic clinic at a referral hospital, Meru County – Kenya. Int J Sci Res Public. 9(10):p9461. Doi:10.29322/ijsrp.9.10.2019.p9461. Accessed 18/01/2023.
- Alshammari ZJ, Alsaid LA, Parameaswari PJ, Alzahrani AA. Attitude and knowledge about foot care among diabetic patients in Riyadh, Saudi Arabia. J Family Med Prim Care. 2019 Jun;8(6):2089-2094. doi: 10.4103/jfmpc.jfmpc_248_19. PMID: 31334185; PMCID: PMC6618215.
- Narmawan, Narmawan & Syahrul, Syahrul & Erika, Kadek Ayu. (2018). THE BEHAVIOR OF FOOT CARE IN PATIENTS WITH TYPE 2 DIABETES MELLITUS: APPLYING THE THEORY OF PLANNED BEHAVIOUR. Public Health of Indonesia. 4. 129-137. 10.36685/phi.v4i3.209.
- Sharoni SKA, Abdul Rahman H, Minhat HS, Shariff Ghazali S, Azman Ong MH. A self-efficacy education programme on foot self-care behaviour among older patients with diabetes in a public long-term care institution, Malaysia: a Quasi-experimental Pilot Study. BMJ Open. 2017 Jun 8;7(6):e014393. doi: 10.1136/bmjopen-2016-014393. PMID: 28600363; PMCID: PMC5623401.
- Mekonen EG, Gebeyehu Demssie T. Preventive foot self-care practice and associated factors among diabetic patients attending the university of Gondar comprehensive specialized referral hospital, Northwest Ethiopia, 2021. BMC Endocr Disord. 2022 May 11;22(1):124. doi: 10.1186/s12902-022-01044-0. PMID: 35546665; PMCID: PMC9097232.
- Ammar I, Jude E, Katia Langton FR, et al. (2017). International Diabetes Federation (IDF): Clinical Practice Recommendation on the Diabetic Foot: A Guide for Healthcare Professionals. Vol. 127; 2017. Doi:10.1016/j.diabres.2017.04.013. Accessed 18/01/2023.
- Armstrong DG, Boulton AJM, Bus SA. Diabetic Foot Ulcers and Their Recurrence. N Engl J Med. 2017 Jun 15;376(24):2367-2375. doi: 10.1056/NEJMra1615439. PMID: 28614678.
- van Netten JJ, Price PE, Lavery LA, Monteiro-Soares M, Rasmussen A, Jubiz Y, Bus SA; International Working Group on the Diabetic Foot. Prevention of foot ulcers in the at-risk patient with diabetes: a systematic review. Diabetes Metab Res Rev. 2016 Jan;32 Suppl 1:84-98. doi: 10.1002/dmrr.2701. PMID: 26340966.
- Ong JJ, Azmil SS, Kang CS, Lim SF, Ooi GC, Patel A, Mawardi M. Foot care knowledge and self-care practices among diabetic patients in Penang: A primary care study. Med J Malaysia. 2022 Mar;77(2):224-231. PMID: 35338631.
- Wendling S, Beadle V. The relationship between self-efficacy and diabetic foot self-care. J Clin Transl Endocrinol. 2015 Jan 27;2(1):37-41. doi: 10.1016/j.jcte.2015.01.001. PMID: 29159107; PMCID: PMC5685009.
![]() This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
The Impact of Nurse Manager Leadership Styles on Nurse Job Satisfaction: A CrossSectional Study at Hamad Medical Corporation, Qatar
Abdelbasset Ghalgaoui 1, 2 *, Nabil Ajjel 1, Maha Mohamed Marzouk Ahmed 1,
Osama Helmi Mohammad Subih 1, Mehdi Halleb 1
1. Department of Nursing, Hamad Medical Corporation (HMC), Doha, Qatar.
2. Institut Universitaire de Formation des Cadres (INUFOCAD), Port-au-Prince, Haiti.
* Corresponding author: Abdelbasset Ghalgaoui, Graduate Registered Nurse, Department of Nursing, Hamad Medical Corporation (HMC), Doha, Qatar. PhD Student in Education and Governance, Institut Universitaire de Formation des Cadres (INUFOCAD), Port-au-Prince, Haiti. Email: ghalgaouiabdelbasset@gmail.com
Cite this article
ABSTRACT
Introduction: Job satisfaction is a key determinant of nurse retention, morale, and quality of care. Leadership styles directly shape satisfaction by influencing recognition, autonomy, and support within clinical environments. In Qatar’s multicultural nursing workforce, understanding these dynamics is critical.
Objective: This study investigated the relationship between nurse manager leadership styles and nurses’ job satisfaction at Hamad Medical Corporation (HMC).
Method: A cross-sectional survey was conducted with 980 registered nurses recruited through simple random sampling. Data were collected using a structured online questionnaire incorporating socio-demographic data, the Multifactor Leadership Questionnaire (MLQ-5X), and the Minnesota Satisfaction Questionnaire – Short Form (MSQ). Descriptive and inferential statistics, including Spearman’s correlation, Mann–Whitney U, and Kruskal–Wallis H tests, were employed.
Results: The sample was predominantly female (72.1%) and expatriate, with Indian (42.1%) and Filipino (33.9%) nurses forming the largest groups. Transactional leadership (mean = 2.57) was more common than transformational leadership (mean = 2.20). Overall satisfaction levels were moderate. Transformational leadership showed a strong positive correlation with both intrinsic satisfaction (rho = 0.66, p < 0.001) and extrinsic satisfaction (rho = 0.79, p < 0.001), yielding an overall significant relationship with total job satisfaction (rho = 0.73, p < 0.001).Transactional leadership demonstrated a weak to moderate positive correlation (rho = 0.30, p < 0.001), while passive-avoidant leadership showed no meaningful association with satisfaction (rho = 0.06, p = 0.041).
Conclusion: Transformational leadership has the strongest influence on job satisfaction, while transactional and passive-avoidant styles limit long-term fulfillment. Enhancing transformational leadership at HMC may improve satisfaction, retention, and workforce stability.
Keywords: Leadership, Nurses, Job Satisfaction, Retention
INTRODUCTION
In the dynamic and demanding field of healthcare, nurses occupy a vital role. They are not merely caregivers but the backbone of healthcare institutions, providing essential treatment, compassion, and expertise to patients in need. The satisfaction of nurses is a crucial element that directly impacts their well-being, retention, and ultimately the quality of care delivered to patients.
Leadership plays a central role in shaping the experiences of nurses within healthcare organizations. Nurse managers, through their leadership styles, have the ability to empower their teams, foster a supportive work culture, and contribute to overall job satisfaction. Effective leadership can inspire motivation, strengthen commitment, and enhance the professional fulfillment of nurses. Conversely, ineffective or unsupportive leadership can create dissatisfaction, burnout, and even intentions to leave the profession, posing challenges for healthcare quality and staff retention[1,2].
Avolio and Bass have identified three primary leadership styles: transformational, transactional, and passive-avoidant (laissez-faire). Transformational leaders inspire and motivate followers toward shared goals, encouraging innovation and personal growth. Transactional leaders emphasize structure, rewards, and performance management. Passive-avoidant leaders, however, tend to disengage, avoiding intervention and decision-making, often resulting in reduced productivity and workplace dissatisfaction[3,4]. Nurse managers often apply one or a combination of these styles, with varying outcomes on nurse satisfaction.
Studies conducted in Qatar and the surrounding region highlight the prevalence and influence of leadership styles in healthcare. For example, transformational leadership has been shown to be the most commonly practiced style among nursing leaders in Qatar[5]. Additionally, research in Saudi Arabia and Bahrain has demonstrated that transformational and transactional leadership approaches are positively linked to nurses’ satisfaction, commitment, and reduced turnover intentions[6,7]. These findings reinforce the importance of leadership style as a determinant of nurse satisfaction in Middle Eastern healthcare settings, including at HMC.
The relevance of this issue at HMC is further underscored by local research showing that a significant proportion of nurses and healthcare workers have reported dissatisfaction, stress, and turnover intentions, particularly during and after the COVID-19 pandemic[8]. Such challenges highlight the pressing need to evaluate how leadership styles adopted by nurse managers influence nurses’ satisfaction within HMC.
Therefore, this study seeks to explore the perceptions of nurses regarding their managers’ leadership styles and to examine the relationship between these leadership approaches and nurses’ job satisfaction. Understanding this relationship is crucial to developing effective leadership strategies that enhance nurse satisfaction, reduce turnover, and improve the overall quality of patient care. Addressing this gap is essential to achieving Qatar’s National Health Strategy goals for workforce sustainability and excellence in healthcare delivery.
Objectives
This study aimed to describe nurses’ perceptions of their managers’ leadership styles, assess their job satisfaction levels, and examine associations between leadership approaches and satisfaction dimensions.
MATERIALS AND METHODS
Type and Classification of Study
This study employed a quantitative, cross-sectional research design to examine the relationship between nurse manager leadership styles and nurses' job satisfaction at HMC, Qatar.
Comparisons and Predictors of Interest
The primary focus was on comparing various nurse manager leadership styles and their respective impacts on staff nurses’ job satisfaction.
Study Duration
The study was conducted over a period of approximately four months, from November 5, 2024, to March 1, 2025.
Sample Size Justification
To ensure reliability and representativeness of the findings, a sample size calculation was conducted based on a population of approximately 12,000 nurses. Using a 95% confidence level and a ±3% margin of error, an estimate minimal sample size of 1067 nurses was determined to be appropriate. The sample size was calculated using Cochran’s formula:
where Z = 1.96, p = 0.5, e = 0.03. Since the estimate minimal sample size is large and >5% compared to the population from which it is obtained (12,000), the sample size can be reduced to 980 nurses.
The value p = 0.5 was chosen to provide the most conservative estimate and ensure adequate sample size in the absence of prior data, while a ±3% margin of error was selected to achieve high precision and reliable representativeness of the study findings.
Study Population and Setting
The study population comprised registered nurses working in various departments across Hamad Medical Corporation (HMC), Qatar. Participants were selected through a simple random sampling method. The sampling frame included the complete list of licensed nurses at HMC, each assigned a unique identification number. Using Microsoft Excel’s RAND function, the list was randomly ordered to facilitate unbiased selection.
To account for an anticipated non-response rate, the initial calculated sample of 980 nurses determined based on a 95% confidence level and a ±3% margin of error for a population of approximately 12,000 nurses was increased by 245, resulting in a total of 1,225 nurses being invited to participate. Questionnaires were distributed via official HMC email accounts, and 980 completed responses were obtained, forming the final study sample. This strategy ensured a representative sample across different hospitals and nursing units within HMC.
The study was carried out exclusively within HMC facilities.
Inclusion Criteria
- Registered nurses currently employed at HMC.
- Nurses who voluntarily consented to participate.
- Nurses with a minimum of six months of experience at HMC to ensure familiarity with the organizational culture and leadership practices.
Exclusion Criteria
- Nurses on leave or absent during data collection.
- Nurses in managerial or supervisory roles.
- Contract or temporary nurses.
Data Collection
Data were collected via structured online questionnaires distributed through Google Forms. The survey instruments covered the following areas:
- Socio-demographic Data
Collected information included age, gender, nationality, years of nursing experience, tenure at HMC, education level, hospital, and department. Age was categorized into three groups (≤30 years, 31–45 years, and >45 years) to reflect early, mid-, and late-career stages. Similarly, years of nursing experience and years of experience within HMC were grouped as ≤5 years, 6–15 years, and >15 years to allow meaningful comparisons between groups and ensure adequate sample sizes for statistical analysis.
- Multifactor Leadership Questionnaire (MLQ-5X)
This 45-item tool assessed leadership styles (transformational, transactional, and laissez-faire) across dimensions such as inspirational motivation, intellectual stimulation, and contingent reward. Responses were recorded on a 5-point Likert scale (0 = "Not at all" to 4 = "Frequently, if not always") [9]. Items were grouped into their respective leadership dimensions using the MLQ scoring key. For each dimension, a mean score was calculated by summing the responses to the items composing that scale and dividing by the number of valid responses. All leadership style subscales consisted of four items each. Blank or missing responses were excluded from the calculations. Higher mean scores indicated more frequent exhibition of the corresponding leadership behaviors. Leadership dimensions were analyzed as continuous variables rather than categorizing leaders into a single leadership style.
The tool demonstrated strong reliability, with Cronbach’s alpha ranging from 0.70 to 0.90.
- Minnesota Satisfaction Questionnaire (Short Form)
This 20-item scale measured job satisfaction across facets such as supervision, pay, promotion, coworkers, and communication. Responses ranged from 1 ("Not Satisfied") to 5 ("Extremely Satisfied")[10]. The instrument showed good internal consistency, with a Cronbach’s alpha range of 0.70 to 0.90.
Primary and Secondary Outcomes
- Primary Outcomes: Nurses’ job satisfaction.
- Secondary Outcome: The relationship between nurse manager leadership styles and the three primary outcomes.
Statistical analysis
Descriptive statistics were used to summarize participant characteristics and key variables such as means, standard deviations, medians, ranges, and percentages. Normality of continuous variables was assessed using the Shapiro–Wilk test, which indicated non-normal distribution (p < 0.05). Therefore, non-parametric statistical tests were applied, including Mann–Whitney U and Kruskal–Wallis H for group comparisons.
Correlation between leadership styles and job satisfaction was analyzed using Spearman’s rank correlation coefficient (ρ) due to non-normal distribution. The statistical tests with p-value < 0.05 were considered significant. All analyses were performed using SPSS-26 software.
Ethical Approval and Informed Consent Statement
Informed consent was obtained from all study participants. The purpose, procedures, and voluntary nature of the study were explained through official internal communication channels via HMC e-mail. Participants provided electronic consent after having at least two months to review the study information before deciding to participate. Only registered nurses employed at HMC who met the inclusion criteria were enrolled. No financial incentives were offered for participation.
The study was approved by the Medical Research Center (MRC) – Local Ethics Committee of Hamad Medical Corporation, Qatar (Protocol No. MRC-01-24-356), with approval granted on 15/08/2024, and was conducted in accordance with the principles of the Declaration of Helsinki and Good Clinical Practice (GCP), as well as the regulations of the Ministry of Public Health (MoPH), Qatar. Participant anonymity and data confidentiality were strictly maintained throughout the study.
RESULTS
Demographic and Professional Characteristics
The study sample of 980 nurses demonstrated a pronounced gender imbalance, with females constituting nearly three-quarters of the workforce (Table 1). Marriage was the predominant status, and Indian and Filipino nationals together comprised more than three-quarters of the participants, highlighting the concentration of the workforce among specific nationalities. Age distribution indicated that the majority of nurses were mid-career professionals aged 30–45 years (67.04%), whereas younger nurses (≤30 years) formed a small minority (6.53%).
|
Characteristics |
Categories |
Frequency (n) |
Percent (%) |
Mean± SD |
|
Gender |
Male |
273 |
27.86 |
|
|
Female |
707 |
72.14 |
||
|
Marital Status |
Single |
138 |
14.08 |
|
|
Married |
820 |
83.67 |
||
|
Widowed |
8 |
0.82 |
||
|
Separated / Divorced |
14 |
1.43 |
||
|
Nationality |
Cuban |
36 |
3.67 |
|
|
Egyptian |
16 |
1.63 |
||
|
Filipino |
332 |
33.88 |
||
|
Indian |
413 |
42.14 |
||
|
Iranian |
3 |
0.31 |
||
|
Jordanian |
64 |
6.53 |
||
|
Lebanese |
5 |
0.51 |
||
|
Palestinian |
8 |
0.82 |
||
|
Somali |
3 |
0.31 |
||
|
Sudanese |
51 |
5.20 |
||
|
Tunisian |
49 |
5.00 |
||
|
Age (years) |
≤30 years |
64 |
6.53 |
40.40 ± 7.89 |
|
]30-45] |
657 |
67.04 |
||
|
> 45 |
259 |
26.43 |
Table 1. Demographic Characteristics (N=980)
Hospital and departmental distribution demonstrated a concentration of staff in a limited number of facilities and clinical areas. Hamad General Hospital employed the largest share (27.55%), followed by Rumailah (11.63%), Al Wakra (11.43%), and the Women’s Wellness & Research Center (8.16%). The Surgical and Medical departments collectively accounted for more than 65% of participants, whereas Critical Care, Emergency, and Outpatient/ Ambulatory units had smaller staff representation.
These demographic patterns suggest that the HMC nursing workforce is highly experienced and predominantly composed of expatriate professionals, highlighting the importance of culturally adaptive leadership strategies.
|
Characteristics |
Categories |
Frequency (n) |
Percent (%) |
Mean± SD |
|
Years of experience as a nurse |
≤5 years |
21 |
2.14 |
16.85 ± 7.14 |
|
]5-15] |
532 |
54.29 |
||
|
> 15 |
427 |
43.57 |
||
|
Years of experience in HMC |
≤5 years |
360 |
36.73 |
9.93 ± 7.54 |
|
]5-15] |
369 |
37.65 |
||
|
> 15 |
251 |
25.61 |
||
|
Educational background |
Diploma |
139 |
14.18 |
|
|
Bachelor’s degree |
751 |
76.63 |
||
|
Master’s degree |
90 |
9.18 |
||
|
Hospital |
Hamad General Hospital |
270 |
27.55 |
|
|
Ambulatory Care Center |
58 |
5.92 |
||
|
Qatar Rehabilitation Institute |
17 |
1.73 |
||
|
NCCCR |
19 |
1.94 |
||
|
Mental Health Service |
48 |
4.90 |
||
|
Communicable Disease Center |
15 |
1.53 |
||
|
Al Khor Hospital |
72 |
7.35 |
||
|
Rumailah Hospital |
114 |
11.63 |
||
|
Al Wakra Hospital |
112 |
11.43 |
||
|
Hazm Mebaireek General Hospital |
64 |
6.53 |
||
|
Aisha Bint Hamad Al Attiyah Hospital |
63 |
6.43 |
||
|
The Cuban Hospital |
17 |
1.73 |
||
|
Women's Wellness and Research Center |
80 |
8.16 |
||
|
Heart Hospital |
31 |
3.16 |
||
|
Department |
Critical Care / Emergency Services |
220 |
22.45 |
|
|
Medical Department |
296 |
30.20 |
||
|
Surgical Department |
348 |
35.51 |
||
|
Outpatient (OPD) and Ambulatory Services |
116 |
11.84 |
Table 2. Professional Characteristics (N=980)
Nurse Manager Leadership Styles
The analysis of nurse manager leadership styles revealed that transactional leadership was more prominent (mean = 2.57, SD = 0.85; Q1 = 2.00, Q3 = 3.12) compared to transformational leadership (mean = 2.20, SD = 1.05; Q1 = 1.55, Q3 = 3.00). This suggests that managers primarily use structured management approaches, emphasizing performance-based rewards and active monitoring (Table 3).
|
|
Minimum |
Maximum |
Mean |
S D |
Median |
Q1 |
Q3 |
|
Idealized Attributes or Idealized Influence (Attributes) |
0.00 |
4.00 |
2.19 |
1.14 |
2.25 |
1.50 |
3.00 |
|
Idealized Behaviors or Idealized Influence (Behaviors) |
0.00 |
4.00 |
2.35 |
1.15 |
2.50 |
1.75 |
3.25 |
|
Inspirational Motivation |
0.00 |
4.00 |
2.34 |
1.22 |
2.50 |
1.50 |
3.25 |
|
Intellectual Stimulation |
0.00 |
4.00 |
2.21 |
1.11 |
2.25 |
1.50 |
3.00 |
|
Individual Consideration |
0.00 |
4.00 |
1.94 |
0.96 |
2.00 |
1.25 |
2.75 |
|
Transformational |
0.00 |
4.00 |
2.20 |
1.05 |
2.35 |
1.55 |
3.00 |
|
Contingent Reward |
0.00 |
4.00 |
2.56 |
1.05 |
2.75 |
2.00 |
3.25 |
|
Mgmt by Exception (Active) |
0.00 |
4.00 |
2.58 |
0.98 |
2.75 |
2.00 |
3.25 |
|
Transactional |
0.25 |
4.00 |
2.57 |
0.85 |
2.62 |
2.00 |
3.12 |
|
Mgmt by Exception (Passive) |
0.00 |
4.00 |
1.55 |
1.01 |
1.25 |
0.75 |
2.25 |
|
Laissez-Faire |
0.00 |
4.00 |
1.43 |
1.05 |
1.25 |
0.50 |
2.25 |
|
Passive Avoidant |
0.00 |
4.00 |
1.49 |
0.97 |
1.37 |
0.75 |
2.12 |
|
Extra Effort |
0.00 |
4.00 |
2.17 |
1.20 |
2.33 |
1.00 |
3.00 |
|
Effectiveness |
0.00 |
4.00 |
2.25 |
1.22 |
2.50 |
1.00 |
3.00 |
|
Satisfaction |
0.00 |
4.00 |
2.28 |
1.31 |
2.50 |
1.00 |
3.00 |
|
Outcomes of Leadership |
0.00 |
400 |
2.23 |
1.20 |
2.42 |
1.05 |
3.16 |
Table 3. Nurse Manager Leadership Styles.
Within the transactional domain, contingent reward (mean = 2.56, SD = 1.05; Q1 = 2.00, Q3 = 3.25) and management by exception active (mean = 2.58, SD = 0.98; Q1 = 2.00, Q3 = 3.25) were the most utilized strategies.
Among transformational leadership subscales, idealized influence behaviors (mean = 2.35, SD = 1.15; Q1 = 1.75, Q3 = 3.25) scored highest, indicating that some leaders act as strong role models. Conversely, individual consideration (mean = 1.94, SD = 0.96; Q1 = 1.25, Q3 = 2.75) was lowest, suggesting limited mentorship or personalized support for staff.
Passive-avoidant leadership had the lowest overall scores (mean = 1.49, SD = 0.97; Q1 = 0.75, Q3 = 2.12), particularly laissez-faire leadership (mean = 1.43, SD = 1.05; Q1 = 0.50, Q3 = 2.25), showing that managers generally remain engaged and avoid ignoring decision-making responsibilities. Management by exception passive (mean = 1.55, SD = 1.01; Q1 = 0.75, Q3 = 2.25) indicated occasional reactive behaviors. Leadership outcomes were moderate, with effectiveness (mean = 2.25, SD = 1.22; Q1 = 1.00, Q3 = 3.00) and satisfaction (mean = 2.28, SD = 1.31; Q1 = 1.00, Q3 = 3.00) reflecting satisfactory performance from the staff perspective.
The dominance of transactional leadership may reflect the organizational focus on compliance and efficiency rather than on empowerment or innovation.
Nurses' Satisfaction
The results indicate that nurses experience moderate job satisfaction across both intrinsic and extrinsic dimensions as well as in the overall satisfaction measured by the Minnesota Satisfaction Questionnaire (MSQ) - Short Form. For intrinsic satisfaction, 57.55% of participants fall into the average category (Table 4), while 20.41% report low satisfaction, with a mean score of 2.93 ± 0.93 (Q1 = 2.00, Q3 = 2.00). The quartile values indicate that most respondents cluster tightly around the lower end of the moderate range, suggesting limited variability in perceived intrinsic motivators. In contrast, extrinsic satisfaction shows that 57.14% of respondents are moderately satisfied, but a slightly higher percentage (22.86%) report low satisfaction, with a mean score of 2.74 ± 1.01 (Q1 = 2.00, Q3 = 2.00). Similar to intrinsic satisfaction, the Q1 and Q3 values suggest that extrinsic satisfaction is concentrated at the lower boundary of moderate satisfaction, reinforcing the need for improvements in external factors such as pay and recognition.
Regarding overall satisfaction (MSQ), 71.84% of respondents are in the average category, 8.57% report low satisfaction, and 19.59% report high satisfaction, with a mean score of 2.87 ± 0.94 (Q1 = 2.00, Q3 = 2.00). The quartile distribution again shows that the majority of nurses fall at the lower end of the moderate satisfaction range. The moderate satisfaction levels indicate room for improvement, particularly in extrinsic factors such as pay and recognition.
|
|
Range |
Frequency |
Percent |
Min |
Max |
Mean±SD |
Median [Q1, Q3] |
|
Intrinsic Satisfaction |
Low Satisfaction |
200 |
20.41 |
1.00 |
5.00 |
2.93 (0.93) |
3.00 [2.41, 3.58] |
|
Average Satisfaction |
564 |
57.55 |
|||||
|
High Satisfaction |
216 |
22.04 |
|||||
|
Extrinsic Satisfaction |
Low Satisfaction |
224 |
22.86 |
1.00 |
5.00 |
2.74 (1.01) |
2.83 [2.00, 3.50] |
|
Average Satisfaction |
560 |
57.14 |
|||||
|
High Satisfaction |
196 |
20.00 |
|||||
|
General Satisfaction of MSQ |
Low level of satisfaction |
84 |
8.57 |
1.00 |
5.00 |
2.87 (0.94) |
2.95 [2.25, 3.55] |
|
Average level of satisfaction |
704 |
71.84 |
|||||
|
High level of satisfaction |
192 |
19.59 |
Table 4. Nurses' Satisfaction
Comparison of Socio-demographic Characteristics and Their Association with Nurses' Satisfaction
In Table 5, female nurses reported significantly higher job satisfaction than male nurses (mean rank: 506.43 vs 449.23, p = 0.005). Single nurses showed the highest satisfaction, followed by married and widowed nurses (550.57 vs. 473.29 vs 373.50, p = 0.006). Significant differences were observed across nationalities, with Somali nurses reporting the highest satisfaction and Cuban nurses the lowest (665.17 vs 254.44, p < 0.001). No significant differences were found by age, although nurses aged ≤30 years had slightly higher satisfaction than those >45 years and those aged 30–45 years (524.38 vs 513.45 vs 478.15, p = 0.144). Similarly, years of nursing experience showed no significant differences, but nurses with ≤5 years of experience reported higher satisfaction than those with >15 years or 5–15 years (589.64 vs 494.45 vs. 483.42, p = 0.224).
Years of experience within HMC was significantly associated with satisfaction, with nurses having >15 years reporting the highest and those with 5–15 years reporting the lowest satisfaction (537.60 vs 422.53, p < 0.001).
|
Characteristics |
Categories |
Mean Rank |
Statistic |
p-value (Test) |
|
Gender |
Male |
449.23 |
85239.5 |
0.005(MW)* |
|
Female |
506.43 |
|||
|
Marital Status |
Single |
550.57 |
10.32 |
0.006(KW)* |
|
Married |
473.29 |
|||
|
Widowed |
373.50 |
|||
|
Nationality |
Cuban |
254.44 |
35.18 |
< 0.001(KW)* |
|
Egyptian |
375.50 |
|||
|
Filipino |
494.46 |
|||
|
Indian |
502.89 |
|||
|
Iranian |
604.50 |
|||
|
Jordanian |
543.19 |
|||
|
Lebanese |
598.90 |
|||
|
Palestinian |
515.75 |
|||
|
Somali |
665.17 |
|||
|
Sudanese |
442.23 |
|||
|
Tunisian |
518.79 |
|||
|
Age (years) |
≤30 years |
524.38 |
3.87 |
0.144(KW) |
|
]30-45] |
478.15 |
|||
|
> 45 |
513.45 |
|||
|
Years of experience as a nurse |
≤5 years |
589.64 |
2.99 |
0.224(KW) |
|
]5-15] |
483.42 |
|||
|
> 15 |
494.45 |
|||
|
Years of experience in HMC
|
≤5 years |
527.33 |
34.35 |
< 0.001(KW)* |
|
]5-15] |
422.53 |
|||
|
> 15 |
537.60 |
|||
|
Educational background |
Diploma |
529.18 |
11.51 |
0.003(KW)* |
|
Bachelor’s degree |
474.27 |
|||
|
Master’s degree |
566.21 |
|||
|
Hospital |
Hamad General Hospital |
515.00 |
52.14 |
< 0.001(KW)* |
|
Al Khor Hospital |
378.97 |
|||
|
Rumailah Hospital |
503.45 |
|||
|
Al Wakra Hospital |
479.68 |
|||
|
Hazm Mebaireek General Hospital |
505.44 |
|||
|
Aisha Bint Hamad Al Attiyah Hospital |
445.29 |
|||
|
The Cuban Hospital |
280.97 |
|||
|
Women's Wellness and Research Center |
536.80 |
|||
|
Heart Hospital |
594.37 |
|||
|
Ambulatory Care Center |
525.71 |
|||
|
Qatar Rehabilitation Institute |
607.68 |
|||
|
NCCCR |
624.71 |
|||
|
Mental Health Service |
343.33 |
|||
|
Communicable Disease Center |
501.30 |
|||
|
Department |
Critical Care / Emergency Services |
529.34 |
35.339 |
< 0.001(KW)* |
|
Medical Department |
430.85 |
|||
|
Surgical Department |
479.99 |
|||
|
Outpatient (OPD) and Ambulatory Services |
600.57 |
Note: MW = Mann–Whitney U test; KW = Kruskal–Wallis H test; *p < 0.05 indicates statistical significance.
Table 5. Comparison of Socio-demographic Characteristics and Their Association with Nurses' Satisfaction.
Educational background also influenced satisfaction, with nurses holding a Master’s degree reporting the highest satisfaction, followed by diploma and Bachelor’s degree holders (566.21 vs 529.18 vs. 474.27, p = 0.003). Job satisfaction differed significantly across hospitals, with QRI reporting the highest and ABAH the lowest (624.71 vs 280.97, p < 0.001). Finally, departmental differences were significant, with Outpatient (OPD) and Ambulatory Services showing the highest satisfaction and the Medical Department the lowest (600.57 vs 430.85, p < 0.001).
Correlation between Nurse Manager Leadership Styles and Nurses’ Satisfaction
The analysis reveals distinct relationships between leadership styles and job satisfaction dimensions (Table 6).
|
Intrinsic Satisfaction |
Extrinsic Satisfaction |
Minnesota Satisfaction Questionnaire (Short Form) |
||
|
Transformational
|
Spearman Coefficient (rho) |
0.66 |
0.79 |
0.73 |
|
p-value |
< 0.001* |
< 0.001* |
< 0.001* |
|
|
Transactional
|
Spearman Coefficient (rho) |
0.27 |
0.33 |
0.30 |
|
p-value |
< 0.001* |
< 0.001* |
< 0.001* |
|
|
Passive Avoidant
|
Spearman Coefficient (rho) |
0.08 |
0.04 |
0.06 |
|
p-value |
0.007* |
0.142 |
0.041* |
|
Note: *p < 0.05 indicates statistical significance.
Table 6. Correlation between Nurse Manager Leadership Styles and Nurses’ Satisfaction.
Transformational leadership shows the strongest positive correlations with all forms of satisfaction: intrinsic satisfaction (rho = 0.66, p < 0.001), extrinsic satisfaction (rho = 0.79, p < 0.001), and overall job satisfaction measured by the Minnesota Satisfaction Questionnaire (MSQ) (rho = 0.73, p < 0.001). This suggests that employees who perceive their leaders as inspiring, supportive, and visionary tend to experience higher satisfaction both from the work itself and from external rewards.
Transactional leadership also shows positive but more moderate correlations: intrinsic satisfaction (rho = 0.27, p < 0.001), extrinsic satisfaction (rho = 0.33, p < 0.001), and overall satisfaction (rho = 0.30, p < 0.001). This implies that while reward-based leadership influences job satisfaction, its impact is less pronounced than that of transformational leadership, particularly affecting extrinsic satisfaction. In contrast, passive-avoidant leadership has minimal associations with job satisfaction. The correlations are very weak for intrinsic satisfaction (rho = 0.08, p = 0.007) and overall satisfaction (rho = 0.065, p = 0.041), and non-significant for extrinsic satisfaction (rho = 0.04, p = 0.142). This indicates that passive leadership, marked by inaction and avoidance of responsibility, has little to no effect on employee satisfaction.
Overall, these findings highlight the significant role of transformational leadership in fostering job satisfaction, while transactional leadership has a moderate influence, and passive-avoidant leadership remains largely ineffective. These results confirm that transformational leadership is the most powerful predictor of nurse satisfaction, emphasizing the need for leadership development programs at HMC
DISCUSSION
Demographic and Professional Characteristics
The study sample predominantly comprised female nurses (72.14%), reflecting global trends in nursing gender distribution. The underrepresentation of males (27.86%) highlights ongoing gender disparities in the profession, which may influence workplace dynamics and care delivery. The high proportion of married participants (83.67%) suggests a stable workforce, though potential stressors related to work-life balance warrant consideration. The dominance of Indian (42.14%) and Filipino (33.88%) nationalities aligns with Qatar’s reliance on expatriate healthcare workers, raising questions about cultural adaptation and retention strategies. The mean age of 40.40 years and extensive experience (16.85 ± 7.14 years), indicate a mature, seasoned workforce. However, the low representation of nurses with ≤5 years of experience (2.14%) may signal challenges in recruiting younger professionals. The predominance of Bachelor’s degrees (76.63%) reflects standardization in nursing education, yet the limited advanced degrees (9.18%) suggests opportunities for career development. The concentration of nurses in surgical and medical departments (65.71%) underscores the demand for acute care expertise, while lower representation in specialized units (e.g., Communicable Disease Center) may reflect niche-staffing needs.
Nurse Manager Leadership Styles
The predominance of transactional leadership (mean = 2.57) over transformational styles (mean = 2.20), while passive-avoidant leadership was minimal overall (mean = 1.49) suggests a managerial focus on structured, compliance-driven approaches in this healthcare setting. The reliance on contingent rewards (mean = 2.56) and active monitoring (mean = 2.58) aligns with environments prioritizing task completion over innovation, which may reflect high-pressure clinical demands requiring strict adherence to protocols. However, the low emphasis on individual consideration (mean = 1.94) a core transformational trait indicates missed opportunities for personalized mentorship and emotional support, factors critical for nurse retention and job satisfaction. The moderate to low use of management by exception passive (mean = 1.55) suggests some leaders delay addressing issues until problems escalate, potentially eroding trust. These findings mirror studies where transactional leadership ensures baseline efficiency but fails to inspire long-term commitment [3]. The moderate effectiveness (mean = 2.25) and satisfaction (mean = 2.28) scores further underscore the limitations of overly transactional approaches in fostering intrinsic motivation.
Similar patterns have been observed in studies conducted across the Middle East. In this study, transactional leadership dominates, while other studies highlight differences between transformational and transactional leadership styles in healthcare settings. Passive-avoidant leadership remains very rare. A study conducted in Jordan found that respondents perceived transactional leadership as the most prevalent style among their nurse managers, followed by transformational leadership, with passive-avoidant leadership being the least common [11]. Conversely, two studies conducted in Saudi Arabia reported that transformational leadership was the most dominant style [12,13].
Nurses' Satisfaction
Moderate intrinsic (mean = 2.93) and extrinsic (mean = 2.74) satisfaction scores reveal unmet needs in both personal fulfillment and external rewards. The 20.41% reporting low intrinsic satisfaction suggests gaps in professional growth opportunities, such as limited access to training or leadership roles. Extrinsic dissatisfaction (22.86% low satisfaction) may stem from inflexible schedules, inadequate compensation, or insufficient recognition issues exacerbated by transactional leadership’s focus on extrinsic rewards.
In the same regional context, a study conducted in Saudi Arabia also found generally low levels of job satisfaction [14]. In contrast, a study in a public hospital in Poland using the same Minnesota Satisfaction Questionnaire (MSQ) reported higher satisfaction scores, ranging from 3.05 to 3.43, indicating a higher overall level of job satisfaction. In that study, dimensions such as recognition, independence, and working conditions were rated more favorably, and overall satisfaction with work and life was significantly higher [15]. These differences may reflect organizational or leadership factors, such as limited development opportunities or reliance on transactional leadership in our context. Enhancing training access, recognition, and flexibility may help improve satisfaction and address these gaps.
Comparison of Socio-demographic Characteristics and Their Association with Nurses' Satisfaction
Job satisfaction disparities highlight systemic inequities. Females reported higher satisfaction than males (p = 0.005), potentially due to alignment with societal caregiving roles or workplace inclusivity efforts. A study conducted in Poland within a similar context also found a relationship between gender and job satisfaction [15]. Single nurses (mean rank = 550.57) were more satisfied than married or widowed peers, possibly due to fewer work-life conflicts. Somali nurses (mean rank = 665.17) reported the highest satisfaction, while Tunisians (mean rank = 49) expressed profound dissatisfaction, underscoring the impact of cultural integration and institutional support. A cross‐sectional survey in Saudi Arabia found significant associations between nationality and lower job satisfaction, particularly when orientation and language support were lacking[16]. Younger nurses (≤30 years) and those with ≤5 years of experience showed higher satisfaction, suggesting optimism or alignment with early-career expectations. Nurses with >15 years at HMC were more satisfied (p < 0.001), likely due to career stability or leadership roles. Master’s-degree or more holders (mean rank = 566.21) reported greater satisfaction than diploma and bachelor nurses, emphasizing the role of education in professional fulfillment. Hospitals like QRI (mean rank = 624.71) and outpatient departments (mean rank = 600.57) scored highly, possibly due to manageable workloads or patient interaction. Addressing these variations requires culturally sensitive policies and career development pathways. A meta‐analysis study reported that the negative impact of nurse burnout on outcomes was not moderated by age, sex, or experience implying demographic factors alone may not drive overall well-being in broader contexts[17].
Correlation between Nurse Manager Leadership Styles and Nurses’ Satisfaction
Transformational leadership’s exceptionally strong correlation with overall satisfaction (rho = 0.73, p < 0.001), and especially extrinsic satisfaction (rho = 0.79, p < 0.001), is consistent with Specchia et al.’s systematic review of 12 studies, which identified 9 out of 9 studies showing a positive relationship between transformational behaviors and nurses’ job satisfaction[18]. Gebreheat et al.’s integrative review similarly found that 17 out of 17 studies reported a positive impact of transformational leadership on nurses’ job satisfaction[19]. That It is likely due to its emphasis on recognition and shared goals.
Conversely, transactional leadership’s moderate correlation with overall satisfaction (rho = 0.30, p < 0.001), intrinsic satisfaction (rho = 0.27, p < 0.001) and extrinsic satisfaction (rho = 0.33, p < 0.001) mirrors Specchia et al.’s finding that four studies observed positive correlations, three found no significant relationship, and one even reported a negative link between transactional behaviors and satisfaction[18]. While contingent rewards can satisfy baseline needs reflected in our moderate extrinsic coefficient, they lack the deeper emotional resonance necessary to engender long-term commitment or intrinsic fulfillment.
Finally, passive-avoidant leadership exhibited negligible associations with all satisfaction metrics (overall rho = 0.06, p = 0.041; intrinsic rho = 0.08, p = 0.007; extrinsic rho = 0.04, p = 0.142), reinforcing Specchia et al.’s observation that three studies documented a negative correlation between passive-avoidant behaviors and nurse satisfaction[18]. When managers abdicate decision-making and fail to provide feedback or recognition, role ambiguity and diminished trust arise, eroding both extrinsic perceptions (no rewards or performance guidance) and intrinsic drivers (no inspiration or support).
Recommendations
The study underscores the critical importance of nurse manager leadership styles in shaping nurses’ job satisfaction at HMC. Based on the findings, several recommendations are proposed to enhance satisfaction and overall workplace well-being.
Firstly, HMC should invest in comprehensive leadership training programs that prioritize transformational leadership development. Such programs should focus on building leaders’ ability to inspire, empower, and communicate effectively with their teams. Emphasizing qualities such as empathy, recognition, and individualized consideration can strengthen nurses’ intrinsic motivation and sense of belonging, which are key determinants of satisfaction.
Secondly, the organization should foster open communication and participatory decision-making. When nurses are given opportunities to contribute to clinical and administrative decisions, their sense of value and autonomy increases two crucial components of job satisfaction. Leadership practices should therefore promote a culture of inclusion, transparency, and trust across all nursing departments.
In addition, regular satisfaction assessments should be integrated into the organization’s quality improvement framework to monitor workforce morale and identify emerging concerns early. Findings from these assessments can inform policy adjustments, recognition systems, and workload management strategies. Finally, HMC should establish mentorship and peer-support programs where experienced leaders and senior nurses can provide guidance and career support, further enhancing job satisfaction and retention among younger or less experienced staff.
Strengths and limitations of the study
This study is characterized by several notable strengths that enhance its credibility and contribution to nursing leadership research. A major strength lies in its large and diverse sample (N = 980), which ensures representativeness across multiple hospitals and departments within HMC. The use of validated instruments, including the Multifactor Leadership Questionnaire (MLQ-5X) for assessing leadership and the Minnesota Satisfaction Questionnaire (MSQ) – Short Form for measuring job satisfaction, ensures psychometric reliability and international comparability.
Furthermore, the study employs rigorous statistical techniques such as Spearman’s correlation, Mann–Whitney U, and Kruskal–Wallis H tests to analyze associations between leadership styles and satisfaction outcomes. This comprehensive analytical framework provides robust evidence of the differential effects of transformational, transactional, and passive-avoidant leadership on satisfaction levels. Finally, by situating the research within Qatar’s multicultural healthcare context, the study contributes original insights into how leadership behaviors influence satisfaction in a diverse, expatriate workforce a perspective that is often underrepresented in global nursing literature.
Despite its valuable findings, several limitations must be acknowledged. The cross-sectional design restricts causal inference, meaning that while correlations between leadership styles and satisfaction are established, it cannot be conclusively stated that leadership style directly causes changes in satisfaction levels. Longitudinal studies would be needed to track the evolution of satisfaction over time in response to leadership interventions. Additionally, the use of self-administered questionnaires introduces potential response bias, as participants may have provided socially desirable answers rather than fully objective reflections of their experiences. Common-method bias may also have occurred because both leadership styles and job satisfaction were measured through self-report instruments administered in the same session. The homogeneity of the sample, composed largely of expatriate nurses, limits the generalizability of results to settings with different cultural or workforce compositions. Furthermore, the linguistic and cultural diversity of participants may have affected interpretation or understanding of questionnaire items. The study was conducted exclusively at HMC, meaning institutional factors such as policies, resources, or management structures may have influenced outcomes. Finally, there was limited control for potential confounders, as unmeasured factors such as workload, unit-specific culture, or individual personality traits may also have impacted job satisfaction.
CONCLUSION
This study provides evidence that nurse manager leadership styles significantly influence nurses’ job satisfaction at Hamad Medical Corporation (HMC). Transformational leadership emerged as the strongest positive predictor of intrinsic, extrinsic, and overall job satisfaction, suggesting that leaders who inspire, support, and engage their staff foster higher levels of professional fulfillment. Transactional leadership was associated with moderate positive effects, primarily on extrinsic satisfaction, while passive-avoidant leadership showed minimal or negligible impact on all satisfaction dimensions.
The study also identified significant variations in job satisfaction across hospitals, departments, nationalities, and educational levels, highlighting the role of organizational context and workforce diversity in shaping nurses’ experiences. These findings suggest that targeted interventions promoting transformational leadership behaviors such as mentorship, recognition, and participatory decision-making may enhance nurse satisfaction, retention, and overall workforce stability at HMC.
However, this study has limitations that should be considered when interpreting the results. The cross-sectional design prevents causal inferences, and reliance on self-reported data introduces the potential for response bias and common-method bias. Additionally, linguistic and cultural differences among participants may have influenced responses. Therefore, while the results provide valuable insights for HMC, their generalizability to other healthcare settings is limited, and further research using longitudinal or multi-site designs is recommended.
Local Ethics Committee approval
The study was approved by the Medical Research Center (MRC) – Local Ethics Committee of Hamad Medical Corporation, Qatar (Protocol No. MRC-01-24-356), with approval granted on 15/08/2024, and was conducted in accordance with the principles of the Declaration of Helsinki and Good Clinical Practice (GCP), as well as the regulations of the Ministry of Public Health (MoPH), Qatar. Participant anonymity and data confidentiality were strictly maintained throughout the study.
Conflicts of interest
This study was conducted in accordance with ethical standards. All participants provided informed consent. The authors declare no conflict of interest.
Sources of funding
This research received funding from the Medical Research Center at HMC.
Author contributions
Conception and design: Abdelbasset Ghalgaoui
Data collection: Abdelbasset Ghalgaoui
Data analysis and interpretation: Abdelbasset Ghalgaoui
Drafting of the manuscript: all authors
Critical revision of the manuscript: Abdelbasset Ghalgaoui, Nabil Ajjel
Final approval: all authors
Acknowledgements
The authors thank the staff of Hamad Medical Corporation for their collaboration.
REFERENCES
- 1. Çamveren H, Arslan Yürümezoğlu H, Kocaman G. Why do young nurses leave their organization? A qualitative descriptive study. International Nursing Review. 2020;67:519–28. https://doi.org/10.1111/inr.12633
- 2. Labrague LJ, Nwafor CE, Tsaras K. Influence of toxic and transformational leadership practices on nurses’ job satisfaction, job stress, absenteeism and turnover intention: A cross-sectional study. Journal of Nursing Management. 2020;28:1104–13. https://doi.org/10.1111/jonm.13053
- 3. Avolio B. Full Range Leadership Development. 2nd edition. Los Angeles, Calif London: SAGE Publications, Inc; 2010.
- 4. Avolio BJ, Bass BM, editors. Developing Potential Across a Full Range of Leadership TM: Cases on Transactional and Transformational Leadership. New York: Psychology Press; 2001. https://doi.org/10.4324/9781410603975
- 5. Al-Thawabiya A, Singh K, Al-Lenjawi BA, Alomari A. Leadership styles and transformational leadership skills among nurse leaders in Qatar, a cross-sectional study. Nursing Open. 2023;10:3440–6. https://doi.org/10.1002/nop2.1636
- 6. AL-Dossary RN. Leadership Style, Work Engagement and Organizational Commitment Among Nurses in Saudi Arabian Hospitals. Journal of Healthcare Leadership. Dove Medical Press; 2022;14:71–81. https://doi.org/10.2147/JHL.S365526
- 7. Pattali S, Sankar JP, Al Qahtani H, Menon N, Faizal S. Effect of leadership styles on turnover intention among staff nurses in private hospitals: the moderating effect of perceived organizational support. BMC Health Serv Res. 2024;24:199. https://doi.org/10.1186/s12913-024-10674-0
- 8. Nashwan AJ, Abujaber AA, Villar RC, Nazarene A, Al-Jabry MM, Fradelos EC. Comparing the Impact of COVID-19 on Nurses’ Turnover Intentions before and during the Pandemic in Qatar. Journal of Personalized Medicine. Multidisciplinary Digital Publishing Institute; 2021;11:456. https://doi.org/10.3390/jpm11060456
- 9. Avolio BJ, Bass BM. Multifactor leadership questionnaire: manual and sample set. Third edition. Place of publication not identified: Mind Garden, Inc.; 2004.
- 10. Weiss DJ, Dawis RV, England GW, Lofquist LH. Minnesota satisfaction questionnaire–short form. Educational and Psychological Measurement [Internet]. 1977 [cited 2025 July 1]; https://psycnet.apa.org/doiLanding?doi=10.1037%2Ft08880-000. Accessed 1 July 2025
- 11. Suliman M, Aljezawi M, Almansi S, Musa A, Alazam M, Ta’an WF. Effect of nurse managers’ leadership styles on predicted nurse turnover. Nurs Manag (Harrow). 2020;27:20–5. https://doi.org/10.7748/nm.2020.e1956
- 12. Areej Mohammed Asiri, Sabah Mahmoud Mahran, Naglaa Abdelaziz Elseesy. A study of staff nurses’ perceptions of nursing leadership styles and work engagement levels in Saudi general hospitals. International Journal of Advanced and Applied Sciences. IASE; 2023;10:55–61. https://doi.org/10.21833/ijaas.2023.01.008
- 13. Alluhaybi A, Usher K, Durkin J, Wilson A. Clinical nurse managers’ leadership styles and staff nurses’ work engagement in Saudi Arabia: A cross-sectional study. PLOS ONE. Public Library of Science; 2024;19:e0296082. https://doi.org/10.1371/journal.pone.0296082
- 14. Al Bazroun MI, Aljarameez F, Alhamza R, Ahmed GY, Alhybah F, Al Mutair A. Factors influencing job satisfaction and anticipated turnover among intensive care nurses in Saudi Arabia. British Journal of Healthcare Management. Mark Allen Group; 2023;29:1–10. https://doi.org/10.12968/bjhc.2021.0146
- 15. Tomaszewska K, Kowalczuk K, Majchrowicz B, Kłos A, Kalita K. Areas of professional life and job satisfaction of nurses. Front Public Health [Internet]. Frontiers; 2024 [cited 2025 May 13];12. https://doi.org/10.3389/fpubh.2024.1370052
- 16. Almansour H, Gobbi M, Prichard J, Ewings S. The association between nationality and nurse job satisfaction in Saudi Arabian hospitals. Int Nurs Rev. 2020;67:420–6. https://doi.org/10.1111/inr.12613
- 17. Li LZ, Yang P, Singer SJ, Pfeffer J, Mathur MB, Shanafelt T. Nurse Burnout and Patient Safety, Satisfaction, and Quality of Care. JAMA Netw Open. 2024;7:e2443059. https://doi.org/10.1001/jamanetworkopen.2024.43059
- 18. Specchia ML, Cozzolino MR, Carini E, Di Pilla A, Galletti C, Ricciardi W, et al. Leadership Styles and Nurses’ Job Satisfaction. Results of a Systematic Review. International Journal of Environmental Research and Public Health. Multidisciplinary Digital Publishing Institute; 2021;18:1552. https://doi.org/10.3390/ijerph18041552
- 19. Gebreheat G, Teame H, Costa EI. The Impact of Transformational Leadership Style on Nurses’ Job Satisfaction: An Integrative Review. SAGE Open Nursing. SAGE Publications Inc; 2023;9:23779608231197428. https://doi.org/10.1177/23779608231197428
Current state of the experience of receiving evidence-based practice education and its relationship with evidence-based practice knowledge and skills among hospital nurses: A cross-sectional questionnaire survey in Western Japan
Hideaki Furuki 1*, Nao Sonoda 1, Akiko Morimoto 1
- Graduate School of Nursing, Osaka Metropolitan University, Osaka, Japan
* Corresponding author: Hideaki Furuki, MSc, RN, PHN, Osaka Metropolitan University, Graduate School of Nursing, 1–4–3 Asahi-machi, Abeno Ward, Osaka City, Osaka 545–8585, Japan. E-mail address: s21262g@omu.ac.jp
Cite this article
ABSTRACT
Introduction: Although evidence-based practice (EBP) is a core nursing competency, little is known about the extent to which nurses are educated on the five steps of EBP, including the specific educational content within each step, in pre-licensure and in-service education, and how these educational experiences relate to their knowledge and skills.
Objectives: To examine the extent of nurses’ experience of receiving specific educational content related to each step of EBP in pre-licensure and in-service education, and to evaluate the associations between these experiences and EBP knowledge and skills.
Methods: This cross-sectional questionnaire survey was conducted between June and September 2022 among 2,672 employed hospital nurses in Japan. EBP knowledge and skills were measured using the Japanese version of the EBP Questionnaire. Experience of receiving EBP education in pre-licensure and in-service education was assessed using items developed from EBP textbooks and core competency literature. Analysis of covariance and relative importance analysis were conducted to evaluate the association between the experience of receiving EBP education and EBP knowledge and skills.
Results: 718 nurses (26.9%) were included in the final analysis. The findings showed that nurses’ experience of receiving EBP education was generally limited, with fewer than 25% having learned any EBP-education item, except literature databases, in pre-licensure education. Similarly, fewer than 25% have learned each EBP-education item in in-service education. The adjusted mean EBP knowledge and skills score increased progressively with the extent of education received across the five steps of EBP (20.6 for no steps to 35.5 for five steps), showing a consistent dose–response relationship (p for trend < 0.001). Relative importance analysis showed that the Step 4 and Step 5 items were placed toward the upper end of the contribution rankings.
Conclusions: To effectively improve nurses’ EBP knowledge and skills, providing a practical, EBP-specific program that comprehensively covers all five EBP steps would be essential. Additionally, developing programs for training educators would also be essential.
Keywords: Education, Evidence-based practice, Nurse, Knowledge, Skills.
INTRODUCTION
Evidence-based practice (EBP) is defined as a problem-solving approach that can be used to deliver health care that integrates the best evidence from research and patient care data with clinician expertise as well as patient preferences and values [1]. The risks of adverse outcomes such as mortality, falls, and ventilator-associated pneumonia are reported to be reduced when EBP is implemented [2-5]. Both the American Nurses Association and the American Association of Colleges of Nursing have identified EBP as a core competency for nurses, reflecting its critical role in improving patient care [6,7]. Therefore, promoting EBP education for nurses is recognized as a global priority in nursing. Previous studies on the experience of receiving EBP education have reported its prevalence, instructional hours, and delivery formats (e.g., integration into research methodology or statistics courses) in pre-licensure education [8-11]. Since EBP implementation requires knowledge and skills related to its five steps (Step 1: ask, Step 2: acquire, Step 3: appraise, Step 4: apply, and Step 5: assess), it is essential to receive education on each of these steps. However, no study has examined the extent to which nurses have received specific educational content related to each step of EBP, such as how to formulate clinical questions using the PICO (Patient, Intervention, Comparison, Outcome) or PECO (Patient, Exposure, Comparison, Outcome) framework, and search using databases for clinical guidelines and systematic reviews [12]. Clarifying which aspects of EBP education have been adequately covered and which have not is essential for developing an effective EBP educational program. Additionally, although previous studies have examined the relationship between whether nurses received EBP education and EBP knowledge and skills, no research has assessed how the extent of education received across the five EBP steps relates to these competencies [13-15]. Furthermore, there has been no evaluation of which EBP-education items have a greater contribution to EBP knowledge and skills. Such evaluations would clarify how the comprehensiveness of EBP education relates to levels of EBP knowledge and skills, and which EBP-education items have a greater contribution to EBP competency. This, in turn, would inform the design and prioritization of more effective educational programs. Previous studies have identified factors associated with nurses’ EBP knowledge and skills, including age, gender, educational level, years of clinical nursing experience, employment position, advanced practice certification, participation in EBP education, experience conducting research, and resources and organizational support for EBP [12]. These factors are potential confounders when examining associations between educational exposure and EBP competency. This study was conceptually guided by Kirkpatrick’s evaluation model [16], which conceptualizes training outcomes across four cumulative levels: Level 1—Reaction (how favorable, engaging, and relevant the training is), Level 2—Learning (the degree to which participants acquire intended including knowledge, skills, and confidence), Level 3—Behavior (the degree to which participants apply what they learned on the job), and Level 4—Results (the degree to which targeted organizational outcomes occur).
In our study, the primary endpoints—EBP knowledge and skills—map to Level 2 (Learning), and the extent of experience of receiving EBP education was treated as the educational input expected to produce a dose–response in Level-2 outcomes.
Objective
This study aimed to examine the extent of hospital nurses’ experience of receiving specific educational content related to each step of EBP in both pre-licensure and in-service education in Japan. We also evaluated the associations between these educational experiences and EBP knowledge and skills, and which EBP-education items have a greater contribution.
MATERIALS AND METHODS
Study design and participants
This cross-sectional questionnaire survey was conducted between June and September 2022 among hospital nurses from six hospitals in Western Japan (three universities: two private and one public). Sites were selected for convenience based on pre-existing collaborations and confirmed site willingness. All registered nurses working at these hospitals who met the eligibility criteria were invited to participate. The inclusion criteria were as follows: 1) currently employed as a nurse at a hospital and 2) directly involved in patient care. Nurses in managerial positions, such as directors of nursing, assistant directors of nursing, and head nurses, were excluded. A structured, self-administered, paper-based questionnaire was distributed to participants, and completed questionnaires were returned in sealed envelopes via mail. The study protocol was prepared in accordance with the Declaration of Helsinki and approved by the institutional review board of Osaka Metropolitan University (approval date: June 24, 2022; approval number: 2022–215). The present study used data from the same project as our prior publication [17], though it addresses different research aims and conducts independent analyses.
Data collection procedures and instruments for data collection
Participants were provided with a written explanation of the study’s purpose, procedures, and measures to ensure confidentiality, and that participation was voluntary. Informed consent, considered “appropriate consent” under relevant ethical guidelines [18], was obtained by having participants check a box in the consent section of the questionnaire to indicate their agreement. Data collection was coordinated through the nursing departments at the participating hospitals. After obtaining site approvals, the research team mailed a paper-based questionnaire to the Director of Nursing at each collaborating hospital. The directors then distributed the questionnaire to unit head nurses, who in turn handed it to the eligible staff nurses. All questionnaires were self-administered in paper format; no electronic survey was used, and no individual email addresses or staff contact lists were provided to the researchers. Completed questionnaires were placed by respondents into sealed envelopes and returned by postal mail directly to the study office, thereby maintaining respondent anonymity and confidentiality.
EBP knowledge and skills
EBP knowledge and skills were measured using the Japanese version of the Evidence-Based Practice Questionnaire (EBPQ-J) [18], a validated translation of the original EBPQ developed by Upton and Upton (2006). Both versions have demonstrated high reliability and validity [19-21]. Total scores for EBP knowledge and skills range from 9 to 63, with higher scores indicating greater knowledge and skills. The original EBPQ comprises three subscales: EBP implementation, attitudes toward EBP, and EBP knowledge and skills. The EBPQ-J reorganizes these into four subscales by dividing the knowledge and skills domain into two components: EBP knowledge and skills related to research (score range: 7–49) and EBP knowledge and skills related to practice (score range: 2–14). EBP knowledge and skills were assessed using the total scores of the two subdomains in accordance with the components of the EBPQ. Questionnaire items on the EBP knowledge and skills related to research subscale include statements such as, “Ability to apply necessary information to hypotheses in research question studies,” “Knowledge of methods to search for and obtain evidence,” and “Ability to determine whether the contents of a study are valid (level of bias).” Questionnaire items on the EBP knowledge and skills related to practice subscale include statements such as “Ability to share ideas and information with colleagues” and “Ability to convey new information regarding care with colleagues.” Cronbach’s alpha for the EBP knowledge and skills subscale in the present study was 0.95.
Based on previous literature on factors associated with EBP knowledge and skills [12], we collected the following factors as potential confounders in evaluating the relationship between the experience of receiving EBP education and EBP knowledge and skills using a self-administered questionnaire. These included: age, gender, educational level (diploma, associate degree, bachelor's degree, or master's degree), years of clinical nursing experience, employment position (staff nurse, charge nurse, or assistant head nurse), advanced practice certification (none, certified nurse, or certified specialist nurse), number of times conducting research, access to a literature database (yes or no), and organizational attitude toward EBP ("Is your workplace a positive attitude toward EBP?" non-positive, neither, moderately positive, or very positive). Regarding advanced practice certification in Japan, certified nurse specialists are required to complete a graduate program, which aligns with the qualifications for advanced practice roles in other countries, such as nurse practitioners or clinical nurse specialists [22]. In contrast, certified nurses are registered nurses who have completed specialized clinical training, although a master’s degree is not required for this certification.
Experience of receiving EBP education
The experience of receiving EBP education was measured for both pre-licensure and in-service education. EBP-education items were developed based on key textbooks on EBP [23-25] and literature on EBP core competencies for healthcare professionals [26]. Items were categorized into knowledge and skills components and aligned with the five steps of EBP. Step 1 (Ask) included knowledge of clinical questions and the PICO or PECO framework, as well as skills in formulating clinical questions using that framework. Step 2 (Acquire) included knowledge of efficient evidence searching, such as searching in the following order: systems, summaries, clinical practice guidelines, systematic reviews, and original articles. It also encompassed knowledge of the characteristics and search methods of literature databases (e.g., PubMed and Ichushi Web, a bibliographic database indexing primarily Japanese-language literature on medicine, nursing, dentistry, and pharmacy) and of databases for clinical practice guidelines and systematic reviews (e.g., Minds Guideline Library, a database for domestic clinical practice guidelines published in Japan, and the Cochrane Library). Furthermore, Step 2 included skills in conducting searches for evidence using an efficient order and relevant databases. Step 3 (Appraise) included knowledge of differences in levels of evidence according to study design, random and systematic error, and descriptive and inferential statistics, along with skills in critically appraising literature based on these domains. Step 4 (Apply) included knowledge of the four components required to apply evidence in practice—patient’s clinical state and circumstances, research evidence, patient’s preferences and actions, and clinical expertise—as well as skills in applying these components in clinical decision-making. Step 5 (Assess) included the skill of evaluating the outcomes of EBP. For each EBP-education item, participants were asked to rate their experience on a five-point Likert scale: “Have not learned at all,” “Have not learned,” “Neither,” “Have learned,” and “Have learned a lot.”
Statistical analyses
First, descriptive statistics were used to summarize participants’ characteristics. Continuous variables, such as age and EBP knowledge and skills scores, are presented as means and standard deviations, and dichotomous and categorical data as frequencies and percentages. Next, the experience of receiving EBP education in both pre-licensure and in-service education was summarized for each EBP-education item using frequencies and percentages across the five response categories. Third, analysis of covariance (ANCOVA) was conducted to examine the association between the extent of education received across the five steps of EBP and EBP knowledge and skills. In this model, the extent of education received across the five steps of EBP was treated as the independent variable, and the EBP knowledge and skills score as the dependent variable. In this study, due to the small number of participants who responded “Have learned a lot,” this response was combined with “Have learned” into a single category labeled “Have learned” to improve interpretability. Consequently, the level to which EBP education has been experienced was categorized into four levels: “Have not learned at all,” “Have not learned,” “Neither,” and “Have learned.” For each EBP-education item, the level of educational experience was determined based on responses for both pre-licensure and in-service education. Specifically, when participants reported different amounts of education received across the two educational settings, the higher of the two responses was retained, based on the following rank order: “Have not learned at all” < “Have not learned” < “Neither” < “Have learned.” For instance, if a participant responded, “Have not learned at all” in pre-licensure education and “Have learned” in in-service education, their overall experience for that item was categorized as “Have learned.” The extent of education received across the five steps of EBP was derived by considering participants to have received education on a given step only if they responded “Have learned” to all items within that step. Based on the number of steps for which this condition was met, participants were categorized into one of six groups: those who had received education on no, one, two, three, four, or all five steps. The model included potential confounding variables, including gender, educational level, years of clinical nursing experience, position, advanced practice certification, number of times of experience conducting research, access to a literature database, and organizational attitude toward EBP. Adjusted means and 95% confidence intervals were determined for each category, and a p-value for linear trend was calculated from the linear component (F test) of a polynomial contrast within the ANCOVA framework. Fourth, ANCOVA was conducted for each EBP-education item to examine the association between item-specific experience of receiving EBP education and EBP knowledge and skills. All models used the same four ordered categories (“Have not learned at all,” “Have not learned,” “Neither,” “Have learned”) and the same set of covariates as above. Adjusted means and 95% confidence intervals were determined for each category of level to which EBP education has been experienced, and p-values for linear trends were calculated analogously from the linear component (F test) of a polynomial contrast. The effect sizes were calculated using partial η². For all ANCOVA models, we assessed residual normality with Q–Q plots and homogeneity of variance with residual-versus-fitted plots.
Finally, relative importance analysis was conducted using the Lindemann–Merenda–Gold (LMG) method with the R package “relaimpo” to quantify the contribution of each EBP-education item to EBP knowledge and skills [27,28]. The LMG method is particularly useful when explanatory variables are correlated, as it quantifies each variable’s relative importance by averaging its incremental contribution to R² across all possible orderings [29,30]. Each EBP-education item was dummy-coded as a four-level factor (“Have not learned at all,” “Have not learned,” “Neither,” or “Have learned”). The model included the same covariates as in the ANCOVA (gender, educational level, years of clinical nursing experience, employment position, advanced practice certification, number of times of experience conducting research, access to a literature database, and organizational attitude toward EBP). Contributions were expressed as the percentage of the EBP-education items-only R² (i.e., the proportion of variance explained by the EBP-education items after adjustment for covariates), and 95% confidence intervals were obtained via bootstrap resampling (B = 1,000). We used complete-case analysis because overall missingness was low and missingness often occurred in blocks across item batteries, limiting cross-variable information for imputation. All analyses were performed using IBM SPSS Statistics for Windows version 29 software (IBM SPSS Japan, Tokyo, Japan) or R version 4.4.2 (R Foundation for Statistical Computing, Vienna, Austria). All reported p-values were two-tailed, and values of <0.05 were considered statistically significant.
RESULTS
In total, 2,672 nurses were invited to participate. Of these, 766 (28.7%) responded to the mail survey. After excluding those with missing data, 718 nurses (26.9%) were included in the final analysis. The characteristics of the participants are presented in Table 1. The mean age (standard deviation) was 36.0 (10.0) years; more than 90% of the participants were female, 40.1% had a bachelor’s degree, and 4.0% had a master’s degree. More than half the participants had more than 10 years of clinical experience, most were employed at hospitals with access to a literature database, and more than 60% reported that their organization had a positive attitude toward EBP. The mean EBP knowledge and skills score (standard deviation) was 22.4 (10.4) points, indicating a relatively low level of EBP-related competency among the participants.
Variables Personal factors Age (years) 36.0 (10.0) Gender Women 663 (92.3) Men 55 (7.7) Educational level Diploma or associate degree 400 (55.7) Bachelor’s degree 287 (40.0) Master’s degree 31 (4.3) Years of clinical nursing experience ≤3 159 (22.1) 4–9 160 (22.3) ≥10 399 (55.6) Employment position Staff nurse 653 (90.9) Charge nurse or assistant head nurse 65 (9.1) Advanced practice certification No 692 (96.4) Certified nurse or certified specialist nurse 26 (3.6) Number of times conducting research 0 322 (44.9) 1 146 (20.3) ≥2 250 (34.8) Work-environment factors Literature database No 29 (4.0) Yes 689 (96.0) Organizational attitude toward EBP Nonpositive 82 (11.4) Neither 186 (25.9) Moderately positive 281 (39.2) Very positive 169 (23.5) Outcome EBP knowledge and skills score (points) 22.4 (10.4) Note: Age and EBP knowledge and skills score are presented as mean (standard deviation). Dichotomous data and categorical data are presented as n (%). EBP, evidence-based practice.
Table 1. Participants’ characteristics (n=718).
Experience of receiving EBP education in pre-licensure education
Figure 1 illustrates the experience of receiving EBP education in pre-licensure education among Japanese hospital nurses.
Figure 1. Experience of receiving EBP education in pre-licensure education among Japanese hospital nurses
Note on Figure 1
Proportions represent the distribution of responses to each EBP-education item. Items were categorized into knowledge and skills components and aligned with the five steps of EBP.
a Literature databases refer to resources such as PubMed and Ichushi Web, a bibliographic database indexing primarily Japanese-language literature on medicine, nursing, dentistry, and pharmacy.
b Databases for clinical practice guidelines and systematic reviews refer to resources such as the Minds Guideline Library, a database for domestic clinical practice guidelines published in Japan, and the Cochrane Library.
c The four components are as follows: (1) the patient’s clinical state and circumstances, (2) research evidence, (3) the patient’s preferences and actions, and (4) clinical expertise.
EBP: evidence-based practice; PECO: Patient, Exposure, Comparison, Outcome; PICO: Patient, Intervention, Comparison, Outcome.
Overall, participants’ experience of receiving pre-licensure EBP education was limited. The proportion of nurses who reported that they had learned about skills-related items was lower than the proportion who reported that they had learned about knowledge-related items. Approximately 40% of the nurses reported having learned about characteristics and search methods of literature databases, though fewer than 25% reported having learned about any of the other EBP-education items. Fewer than 10% of nurses reported that they had learned how to formulate clinical questions using the PICO/PECO framework regarding characteristics and search methods of databases for clinical practice guidelines and systematic reviews, how to conduct a search using databases for clinical practice guidelines and systematic reviews, and how to evaluate the outcomes of EBP. Table 2 provides detailed results for each EBP-education item.
Have not learned at all Have not learned Neither Have learned Have learned a lot
EBP – Step 1 (Ask) Knowledge Clinical Questions 253 (35.2) 207 (28.8) 109 (15.2) 132 (18.4) 17 (2.4) The PICO/PECO framework 341 (47.5) 202 (28.1) 92 (12.8) 70 (9.7) 13 (1.8) Skills How to formulate clinical questions using the PICO/PECO framework 378 (52.6) 207 (28.8) 86 (12.0) 42 (5.8) 5 (0.7) EBP – Step 2 (Acquire) Knowledge Efficient order of evidence searching 250 (34.8) 215 (29.9) 109 (15.2) 128 (17.8) 16 (2.2) Characteristics and search methods of literature databases a 181 (25.2) 157 (21.9) 81 (11.3) 237 (33.0) 62 (8.6) Characteristics and search methods of databases for clinical practice guidelines and systematic reviews b 365 (50.8) 199 (27.7) 106 (14.8) 42 (5.8) 6 (0.8) Skills How to search for evidence in an efficient order 314 (43.7) 198 (27.6) 113 (15.7) 81 (11.3) 12 (1.7) How to search using literature databasesa 217 (30.2) 138 (19.2) 84 (11.7) 215 (29.9) 64 (8.9) How to search using databases for clinical practice guidelines and systematic reviews b 350 (48.7) 204 (28.4) 114 (15.9) 43 (6.0) 7 (1.0) EBP – Step 3 (Appraise) Knowledge Differences in levels of evidence according to research design 266 (37.0) 165 (23.0) 99 (13.8) 156 (21.7) 32 (4.5) Random and systematic error 285 (39.7) 162 (22.6) 99 (13.8) 143 (19.9) 29 (4.0) Descriptive and inferential statistics 266 (37.0) 155 (21.6) 112 (15.6) 162 (22.6) 23 (3.2) Skills How to critically appraise literature based on knowledge of research designs and levels of evidence 275 (38.3) 164 (22.8) 127 (17.7) 136 (18.9) 16 (2.2) How to critically appraise literature based on knowledge of random and systematic error 297 (41.4) 184 (25.6) 137 (19.1) 92 (12.8) 8 (1.1) How to critically appraise literature based on knowledge of descriptive and inferential statistics 292 (40.7) 186 (25.9) 140 (19.5) 92 (12.8) 8 (1.1) EBP – Step 4 (Apply) Knowledge The four components of Step 4c 270 (37.6) 202 (28.1) 152 (21.2) 88 (12.3) 6 (0.8) Skills How to apply the four components of Step 4 in nursing practice c 274 (38.2) 201 (28.0) 150 (20.9) 87 (12.1) 6 (0.8) EBP – Step 5 (Assess) Skills How to evaluate the outcomes of EBP 333 (46.4) 199 (27.7) 132 (18.4) 51 (7.1) 3 (0.4) Note: Experience of receiving EBP education is presented as the number of participants (%).
a Literature databases refer to resources such as PubMed and Ichushi Web, a bibliographic database indexing primarily Japanese-language literature on medicine, nursing, dentistry, and pharmacy.
b Databases for clinical practice guidelines and systematic reviews refer to resources such as the Minds Guideline Library, a database for domestic clinical practice guidelines published in Japan, and the Cochrane Library.
c The four components are as follows: (1) the patient’s clinical state and circumstances, (2) research evidence, (3) the patient’s preferences and actions, and (4) clinical expertise.
EBP: evidence-based practice: PECO: Patient, Exposure, Comparison, Outcome; PICO: Patient, Intervention, Comparison, Outcome.
Table 2. Experience of receiving EBP education in pre-licensure education among Japanese hospital nurses (n=718)
Experience of receiving EBP education in in-service education
Figure 2 illustrates the experience of receiving EBP education in in-service education among Japanese hospital nurses.
Note on Figure 2
Proportions represent the distribution of responses to each EBP-education item. Items were categorized into knowledge and skills components and aligned with the five steps of EBP.
a Literature databases refer to resources such as PubMed and Ichushi Web, a bibliographic database indexing primarily Japanese-language literature on medicine, nursing, dentistry, and pharmacy.
b Databases for clinical practice guidelines and systematic reviews refer to resources such as the Minds Guideline Library, a database for domestic clinical practice guidelines published in Japan, and the Cochrane Library.
c The four components are as follows: (1) the patient’s clinical state and circumstances, (2) research evidence, (3) the patient’s preferences and actions, and (4) clinical expertise.
EBP, evidence-based practice, PECO, Patient, Exposure, Comparison, Outcome; PICO, Patient, Intervention, Comparison, Outcome.
Figure 2. Experience of receiving EBP education in in-service education among Japanese hospital nurses.
Overall, participants’ experience of receiving EBP education was limited. For all EBP-education items, fewer than 25% of nurses reported that they had learned about the content, with the percentage of respondents who reported learning about skills-related items being even lower than the percentage of those who reported learning about knowledge-related items. Fewer than 10% of nurses reported that they learned how to formulate clinical questions using the PICO/PECO framework, characteristics and search methods of databases for clinical practice guidelines and systematic reviews, how to conduct a search using databases for clinical practice guidelines and systematic reviews, how to critically appraise literature based on knowledge of random and systematic error, how to critically appraise literature based on knowledge of descriptive and inferential statistics, and how to evaluate the outcomes of EBP. Table 3 provides detailed results for each EBP-education item.
Have not learned at all Have not learned Neither Have learned Have learned a lot EBP – Step 1 (Ask) Knowledge Clinical Questions 276 (38.4) 192 (26.7) 114 (15.9) 126 (17.5) 10 (1.4) The PICO/PECO framework 322 (44.8) 197 (27.4) 98 (13.6) 95 (13.2) 6 (0.8) Skills How to formulate clinical questions using the PICO/PECO framework 340 (47.4) 203 (28.3) 105 (14.6) 66 (9.2) 4 (0.6) EBP – Step 2 (Acquire) Knowledge Efficient order of evidence searching 296 (41.2) 190 (26.5) 118 (16.4) 103 (14.3) 11 (1.5) Characteristics and search methods of literature databases a 250 (34.8) 188 (26.2) 107 (14.9) 154 (21.4) 19 (2.6) Characteristics and search methods of databases for clinical practice guidelines and systematic reviews b 355 (49.4) 194 (27.0) 114 (15.9) 50 (7.0) 5 (0.7) Skills How to search for evidence in an efficient order 332 (46.2) 200 (27.9) 111 (15.5) 69 (9.6) 6 (0.8) How to search using literature databasesa 272 (37.9) 184 (25.6) 100 (13.9) 146 (20.3) 16 (2.2) How to search using databases for clinical practice guidelines and systematic reviews b 353 (49.2) 195 (27.2) 109 (15.2) 57 (7.9) 4 (0.6) EBP – Step 3 (Appraise) Knowledge Differences in levels of evidence according to research design 326 (45.4) 187 (26.0) 110 (15.3) 88 (12.3) 7 (1.0) Random and systematic error 344 (47.9) 199 (27.7) 101 (14.1) 69 (9.6) 5 (0.7) Descriptive and inferential statistics 339 (47.2) 196 (27.3) 104 (14.5) 73 (10.2) 6 (0.8) Skills How to critically appraise literature based on knowledge of research designs and levels of evidence 335 (46.7) 190 (26.5) 112 (15.6) 75 (10.4) 6 (0.8) How to critically appraise literature based on knowledge of random and systematic error 349 (48.6) 203 (28.3) 106 (14.8) 55 (7.7) 5 (0.7) How to critically appraise literature based on knowledge of descriptive and inferential statistics 350 (48.7) 198 (27.6) 104 (14.5) 61 (8.5) 5 (0.7) EBP – Step 4 (Apply) Knowledge The four components of Step 4 c 309 (43.0) 197 (27.4) 119 (16.6) 84 (11.7) 9 (1.3) Skills How to apply the four components of Step 4 in nursing practice c 311 (43.3) 197 (27.4) 120 (16.7) 81 (11.3) 9 (1.3) EBP – Step 5 (Assess) Skills How to evaluate the outcomes of EBP 347 (48.3) 192 (26.7) 116 (16.2) 58 (8.1) 5 (0.7) Note: Experience of receiving EBP education is shown as the number of participants (%).
a Literature databases refer to resources such as PubMed and Ichushi Web, a bibliographic database indexing primarily Japanese-language literature on medicine, nursing, dentistry, and pharmacy.
b Databases for clinical practice guidelines and systematic reviews refer to resources such as the Minds Guideline Library, a database for domestic clinical practice guidelines published in Japan, and the Cochrane Library.
c The four components are as follows: (1) the patient’s clinical state and circumstances, (2) research evidence, (3) the patient’s preferences and actions, and (4) clinical expertise.
EBP: evidence-based practice; PECO: Patient, Exposure, Comparison, Outcome; PICO: Patient, Intervention, Comparison, Outcome.
Table 3. Experience of receiving EBP education in in-service education among Japanese hospital nurses (n=718)
Q–Q plots (quantile–quantile plot)
The Q–Q plots (Figure 3, 4 and 5) indicated approximately normal residuals, and the residual-versus-fitted plots showed no funneling, suggesting no material heteroscedasticity.
Figure 3. Normal Q–Q plots of residuals for ANCOVA models (Panels A–H).
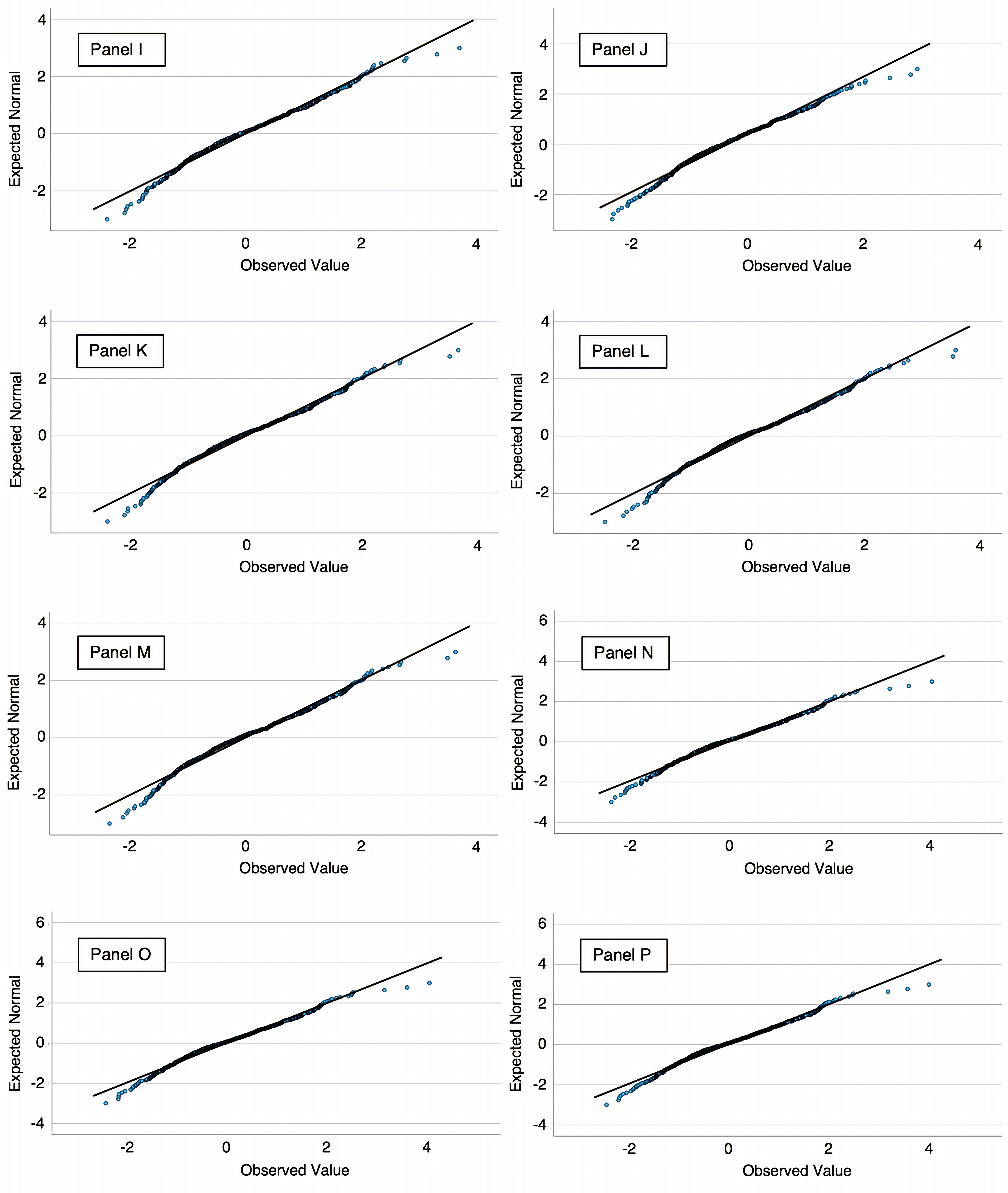
Figure 4. Normal Q–Q plots of residuals for ANCOVA models (Panels I–P).
Figure 5. Normal Q–Q plots of residuals for ANCOVA models (Panels Q–S).
Note on Figures 3-5
Panels: A, six-category model—those who had received education on no, one, two, three, four, or all five steps; B, Step 1—Knowledge: Clinical Questions; C, Step 1—Knowledge: The PICO/PECO Framework; D, Step 1—Skills: How to formulate clinical questions using the PICO/PECO Framework; E, Step 2—Knowledge: Efficient order of evidence searching; F, Step 2—Knowledge: Characteristics and search methods of literature databases; G, Step 2—Knowledge: Characteristics and search methods of databases for clinical practice guidelines and systematic reviews; H, Step 2—Skills: How to search for evidence in an efficient order; I, Step 2—Skills: How to search using literature databases; J, Step 2—Skills: How to search using databases of clinical practice guidelines and systematic review; K, Step 3—Knowledge: Differences in levels of evidence according to research design; L, Step 3—Knowledge: Random and systematic error; M, Step 3—Knowledge: Descriptive and inferential statistics; N, Step 3—Skills: How to critically appraise literature based on knowledge of research designs and levels of evidence; O, Step 3—Skills: How to critically appraise literature based on knowledge of random and systematic error; P, Step 3—Skills: How to critically appraise literature based on knowledge of descriptive and inferential statistics; Q, Step 4—Knowledge: The four components of Step 4; R, Step 4—Skills: How to apply the four components of Step 4 in nursing practice; S, Step 5—Skills: How to evaluate the outcomes of EBP.
Association between the extent of education received across the five steps of EBP and EBP knowledge and skills
Figure 6 illustrates the association between the extent of received education across the five steps of EBP and EBP knowledge and skills scores.
Figure 6. Association between the extent of received education across the five steps of EBP and EBP knowledge and skills
Note on Figure 6
Adjusted mean scores were estimated using analysis of covariance. Scores were adjusted for gender, educational level, years of clinical nursing experience, employment position, advanced practice certification, number of times conducting research, access to a literature database, and organizational attitude toward EBP. Error bars represent 95% confidence intervals.
EBP, evidence-based practice.
The figure shows the mean score for EBP knowledge and skills increased progressively as the number of EBP steps for which education had been received increased. The lowest scores were observed among nurses who had not received education on any of the steps, whereas the highest scores were observed among those who had received education on all five steps. This trend was statistically significant, indicating a dose–response relationship (p for trend<0.001).
Associations between item-specific experience of receiving EBP education and EBP knowledge and skills
Table 4 shows the associations between item-specific experience of receiving EBP education and EBP knowledge and skills scores. For all EBP-education items, participants who reported receiving more EBP education had significantly higher adjusted mean scores for EBP knowledge and skills. The scores showed a consistent increasing trend across the four response categories, and the linear trend was statistically significant for all EBP-education items (p for trend<0.001).
Adjusted meana (95% CI)
p for trend Effect size: partial η² EBP – Step 1 (Ask) Knowledge: Clinical Questions <0.001 0.09 Have not learned at all 18.5 (17.1–20.0) Have not learned 20.5 (19.1–21.8) Neither 25.3 (23.6–26.9) Have learned b 25.7 (24.3–27.0) Knowledge: The PICO/PECO Framework <0.001 0.12 Have not learned at all 19.1 (17.9–20.3) Have not learned 20.8 (19.6–22.1) Neither 25.6 (23.9–27.4) Have learned b 27.8 (26.3–29.3) Skills: How to formulate clinical questions using the PICO/PECO Framework <0.001 0.12 Have not learned at all 19.2 (18.1–20.3) Have not learned 21.7 (20.5–22.9) Neither 25.5 (23.8–27.2) Have learned b 29.4 (27.5–31.3) EBP – Step 2 (Acquire) Knowledge: Efficient order of evidence searching <0.001 0.10 Have not learned at all 18.6 (17.3–20.0) Have not learned 20.5 (19.2–21.8) Neither 24.7 (23.0–26.3) Have learned b 26.4 (25.1–27.7) Knowledge: Characteristics and search methods of literature databases c <0.001 0.07 Have not learned at all 16.5 (14.7–18.4) Have not learned 20.4 (18.7–22.0) Neither 24.5 (22.5–26.4) Have learned b 24.4 (23.3–25.4) Knowledge: Characteristics and search methods of databases for clinical practice guidelines and systematic reviewsd <0.001 0.14 Have not learned at all 19.1 (18.0–20.2) Have not learned 21.9 (20.6–23.2) Neither 24.8 (23.3–26.3) Have learned b 31.1 (29.1–33.1) Skills: How to search for evidence in an efficient order <0.001 0.10 Have not learned at all 19.1 (17.9–20.3) Have not learned 21.3 (20.0–22.6) Neither 24.5 (22.9–26.0) Have learned b 27.9 (26.3–29.5) Skills: How to search using literature databasesc <0.001 0.08 Have not learned at all 17.1 (15.4–18.7) Have not learned 20.3 (18.6–22.1) Neither 23.1 (21.2–25.0) Have learned b 25.0 (24.0–26.0) Skills: How to search using databases for clinical practice guidelines and systematic reviewsd <0.001 0.11 Have not learned at all 19.2 (18.1–20.3) Have not learned 22.1 (20.8–23.4) Neither 25.0 (23.5–26.6) Have learned b 29.1 (27.1–31.0) EBP – Step 3 (Appraise) Knowledge: Differences in levels of evidence according to research design <0.001 0.07 Have not learned at all 18.5 (17.1–19.9) Have not learned 21.1 (19.6–22.6) Neither 24.3 (22.7–26.0) Have learned b 25.5 (24.2–26.8) Knowledge: Random and systematic error <0.001 0.07 Have not learned at all 18.5 (17.2–19.9) Have not learned 22.2 (20.7–23.6) Neither 24.9 (23.2–26.6) Have learned b 25.3 (23.9–26.7) Knowledge: Descriptive and inferential statistics <0.001 0.06 Have not learned at all 18.7 (17.3–20.1) Have not learned 21.5 (20.0–23.0) Neither 24.4 (22.8–26.0) Have learned b 25.3 (24.0–26.7) Skills: How to critically appraise literature based on knowledge of research designs and levels of evidence <0.001 0.09 Have not learned at all 18.3 (17.0–19.7) Have not learned 21.0 (19.5–22.5) Neither 23.9 (22.4–25.4) Have learned b 26.9 (25.4–28.3) Skills: How to critically appraise literature based on knowledge of random and systematic error <0.001 0.10 Have not learned at all 18.6 (17.3–19.8) Have not learned 21.8 (20.5–23.1) Neither 24.2 (22.7–25.7) Have learned b 28.0 (26.3–29.7) Skills: How to critically appraise literature based on knowledge of descriptive and inferential statistics <0.001 0.10 Have not learned at all 18.8 (17.5–20.1) Have not learned 21.2 (19.9–22.6) Neither 24.2 (22.7–25.6) Have learned b 28.1 (26.4–29.7) EBP – Step 4 (Apply) Knowledge: The four components of Step 4e <0.001 0.12 Have not learned at all 18.5 (17.2–19.8) Have not learned 20.7 (19.4–22.0) Neither 24.6 (23.1–26.0) Have learned b 28.2 (26.6–29.7) Skills: How to apply the four components of Step 4 in nursing practicee <0.001 0.12 Have not learned at all 18.4 (17.2–19.7) Have not learned 21.1 (19.8–22.4) Neither 24.6 (23.2–26.1) Have learned b 27.9 (26.3–29.5) EBP – Step 5 (Assess) Skills: How to evaluate the outcomes of EBP <0.001 0.15 Have not learned at all 18.5 (17.3–19.6) Have not learned 21.8 (20.5–23.1) Neither 24.9 (23.5–26.4) Have learned b 30.4 (28.6–32.3) Note: a Adjusted mean scores were estimated using analysis of covariance. Scores were adjusted for gender, educational level, years of clinical nursing experience, employment position, advanced practice certification, number of times conducting research, access to a literature database, and organizational attitude toward EBP.
b The responses “Have learned” and “Have learned a lot” were combined into a single category labeled “Have learned.” For each EBP-education item, the level of educational experience was determined based on responses for both pre-licensure and in-service education. When participants reported different levels of experience across the two educational settings, the higher of the two was retained, following the rank order: “Have not learned at all” < “Have not learned” < “Neither” < “Have learned.”
c Literature databases refer to resources such as PubMed and Ichushi Web, a bibliographic database indexing primarily Japanese-language literature on medicine, nursing, dentistry, and pharmacy.
d Databases for clinical practice guidelines and systematic reviews refer to resources such as the Minds Guideline Library, a database for domestic clinical practice guidelines published in Japan, and the Cochrane Library.
e The four components are as follows: (1) the patient’s clinical state and circumstances, (2) research evidence, (3) the patient’s preferences and actions, and (4) clinical expertise.
CI: confidence interval; EBP: evidence-based practice; PECO: Patient, Exposure, Comparison, Outcome; PICO: Patient, Intervention, Comparison, Outcome.
Table 4. Associations between item-specific experience of receiving EBP education and EBP knowledge and skills (n=718).
Relative importance of EBP-education items for the EBP knowledge and skills
Figure 7 illustrates the relative importance of EBP-education items for the EBP knowledge and skills score.
Figure 7. Relative importance of EBP-education items for the EBP knowledge and skills score.
Note on Figure 7
Bars show the % of EBP education items-only R² contributed by each item, computed using the Lindeman–Merenda–Gold method; error bars are bootstrapped 95% confidence intervals. R²=0.338; adjusted R²=0.270; EBP education items-only R²=0.217. The model included EBP-education items, gender, educational level, years of experience as a clinical nurse, employment position, advanced practice certification, number of experiences conducting research, literature database, and organizational attitude toward EBP.
a Literature databases refer to resources such as PubMed and Ichushi Web, a bibliographic database indexing primarily Japanese-language literature on medicine, nursing, dentistry, and pharmacy.
b Databases for clinical practice guidelines and systematic reviews refer to resources such as the Minds Guideline Library, a database for domestic clinical practice guidelines published in Japan, and the Cochrane Library.
c The four components are as follows: (1) the patient’s clinical state and circumstances, (2) research evidence, (3) the patient’s preferences and actions, and (4) clinical expertise.
EBP, evidence-based practice, PECO, Patient, Exposure, Comparison, Outcome; PICO, Patient, Intervention, Comparison, Outcome.
Ranked by relative importance, the three items accounting for the largest proportion of explained variance were Step 5—Skills (evaluating EBP outcomes), Step 2—Knowledge (characteristics and search methods of databases for clinical practice guidelines and systematic reviews), and Step 4—Knowledge (the four components of Step 4).
Table 5 shows detailed results for the same linear regression model, including unstandardized coefficients, standard errors, p-values, and the change-in-R² (ΔR²) and partial F (ΔF) statistics for all variables.
Factors Reference B (SE) p-value for B ΔR² ΔF p-value for ΔF Experience of receiving EBP education Step 1 (Ask) Knowledge: Clinical Questions 0.002 0.788 0.501 Have not learned vs have not learned at all 0.134 (1.388) 0.923 Neither vs have not learned at all 1.537 (1.698) 0.366 Have learned b vs have not learned at all −0.550 (1.580) 0.728 Knowledge: The PICO/PECO Framework 0.001 0.434 0.729 Have not learned vs have not learned at all −0.868 (2.001) 0.665 Neither vs have not learned at all 1.066 (2.569) 0.678 Have learned b vs have not learned at all 0.981 (2.541) 0.700 Skills: How to formulate clinical questions using the PICO/PECO Framework 0.001 0.316 0.814 Have not learned vs have not learned at all 0.869 (1.991) 0.663 Neither vs have not learned at all −0.061 (2.572) 0.981 Have learned b vs have not learned at all 1.561 (2.668) 0.559 Step 2 (Acquire) Knowledge: Efficient order of evidence searching 0.001 0.457 0.712 Have not learned vs have not learned at all −0.983 (1.418) 0.489 Neither vs have not learned at all 0.700 (1.742) 0.688 Have learned b vs have not learned at all −0.285 (1.630) 0.861 Knowledge: Characteristics and search methods of literature databases c 0.006 1.806 0.145 Have not learned vs have not learned at all 2.983 (1.721) 0.084 Neither vs have not learned at all 3.361 (2.181) 0.124 Have learned b vs have not learned at all 1.291 (1.862) 0.488 Knowledge: Characteristics and search methods of databases for clinical practice guidelines and systematic reviews d 0.007 2.450 0.063 Have not learned vs have not learned at all 0.126 (1.712) 0.941 Neither vs have not learned at all 0.161 (2.044) 0.937 Have learnedb vs have not learned at all 5.267 (2.362) 0.026 Skills: How to search for evidence in an efficient order 0.002 0.622 0.601 Have not learned vs have not learned at all −1.987 (1.546) 0.199 Neither vs have not learned at all −2.202 (1.974) 0.265 Have learned b vs have not learned at all −1.849 (1.936) 0.340 Skills: How to search using literature databases c 0.005 1.553 0.200 Have not learned vs have not learned at all 0.170 (1.801) 0.925 Neither vs have not learned at all 0.507 (2.071) 0.807 Have learned b vs have not learned at all 2.977 (1.820) 0.102 Skills: How to search using databases for clinical practice guidelines and systematic reviews d 0.003 0.920 0.431 Have not learned vs have not learned at all 2.449 (1.877) 0.192 Neither vs have not learned at all 2.042 (2.235) 0.361 Have learned b vs have not learned at all −0.141 (2.382) 0.953 Step 3 (Appraise) Knowledge: Differences in levels of evidence according to research design 0.002 0.687 0.560 Have not learned vs have not learned at all −1.849 (1.875) 0.324 Neither vs have not learned at all −2.001 (2.234) 0.371 Have learned b vs have not learned at all −0.229 (1.980) 0.908 Knowledge: Random and systematic error 0.003 1.088 0.354 Have not learned vs have not learned at all 2.687 (2.142) 0.210 Neither vs have not learned at all 2.707 (2.698) 0.316 Have learned b vs have not learned at all 0.051 (2.387) 0.983 Knowledge: Descriptive and inferential statistics 0.0003 0.110 0.954 Have not learned vs have not learned at all −1.099 (2.165) 0.612 Neither vs have not learned at all −0.453 (2.457) 0.854 Have learned b vs have not learned at all −0.272 (2.189) 0.901 Skills: How to critically appraise literature based on knowledge of research designs and levels of evidence 0.002 0.609 0.609 Have not learned vs have not learned at all 0.132 (2.120) 0.950 Neither vs have not learned at all 1.613 (2.322) 0.487 Have learned b vs have not learned at all 2.325 (2.262) 0.304 Skills: How to critically appraise literature based on knowledge of random and systematic error 0.008 2.664 0.047 Have not learned vs have not learned at all 8.249 (3.581) 0.022 Neither vs have not learned at all −2.465 (4.695) 0.600 Have learned b vs have not learned at all 2.502 (4.050) 0.537 Skills: How to critically appraise literature based on knowledge of descriptive and inferential statistics 0.007 2.342 0.072 Have not learned vs have not learned at all −8.528 (3.629) 0.019 Neither vs have not learned at all 0.019 (4.635) 0.997 Have learned b vs have not learned at all −2.651 (3.863) 0.493 Step 4 (Apply) Knowledge: The four components of Step 4 e 0.002 0.532 0.660 Have not learned vs have not learned at all −0.384 (2.540) 0.880 Neither vs have not learned at all 1.302 (3.083) 0.673 Have learned b vs have not learned at all 2.645 (3.052) 0.387 Skills: How to apply the four components of Step 4 in nursing practicee 0.0005 0.162 0.922 Have not learned vs have not learned at all −0.611 (2.588) 0.814 Neither vs have not learned at all −0.356 (3.182) 0.911 Have learnedb vs have not learned at all −1.695 (3.115) 0.587 Step 5 (Assess) Skills: How to evaluate the outcomes of EBP 0.009 2.948 0.032 Have not learned vs have not learned at all 2.054 (1.560) 0.188 Neither vs have not learned at all 2.006 (1.771) 0.258 Have learned b vs have not learned at all 5.608 (1.960) 0.004 Potential confounding factors Gender 0.001 1.448 0.229 Men vs women 1.584 (1.316) 0.229 Educational level 0.016 8.043 <0.001 Bachelor’s degree vs diploma or associate degree −0.158 (0.932) 0.865 Master's degree vs diploma or associate degree 7.161 (1.869) <0.001 Years of clinical nursing experience 0.001 0.266 0.766 4–9 vs ≤3 −0.16 (1.079) 0.882 ≥10 vs ≤3 −0.757 (1.129) 0.503 Employment position 0.001 0.607 0.436 Charge nurse or assistant head nurse vs staff nurse 1.006 (1.292) 0.436 Advanced practice certification 0.003 2.475 0.116 Certified nurse or certified specialist nurse vs no 3.073 (1.953) 0.116 Number of times conducting research 0.013 6.433 0.002 1 vs 0 1.893 (1.001) 0.059 ≥2 vs 0 3.698 (1.032) <0.001 Literature database 0.001 0.628 0.428 Yes vs no 1.405 (1.773) 0.428 Organizational attitude toward EBP 0.002 0.581 0.628 Neither vs non-positive −0.921 (1.232) 0.455 Moderately positive vs non-positive −0.305 (1.179) 0.796 Very positive vs non-positive 0.388 (1.280) 0.762 Note: These results are from the same model used for the relative-importance analysis in Figure 7.
Dummy variables coded 0 for “have not learned at all”/ 1 for “have not learned”/ 2 for “neither”/ 3 for “have learned” (EBP education items); 0 for women/1 for men (gender); 0 for diploma or associate degree/1 for bachelor's degree/2 for master’s degree (educational level); 0 for “≤3”/1 for “4–9”/2 for “≥10” (years of clinical nursing experience); 0 for staff nurse/1 for charge nurse and assistant head nurse (employment position); 0 for “no”/1 for certified nurse or certified specialist nurse (advanced practice certification); 0 for “0”/1 for “1”/2 for “≥2” (number of times conducting research); 0 for “no”/1 for “yes” (literature database); and 0 for non-positive/1 for neither /2 for moderately positive /3 for very positive (organizational attitude toward EBP).
R²=0.338; adjusted R²=0.270; EBP education items-only R²=0.217.
a EBP knowledge and skills measured by the Evidence-Based Practice Questionnaire Japanese version. EBP knowledge and skills score ranges from 9 to 63, with higher scores indicating more EBP knowledge and skills.
b The responses “Have learned” and “Have learned a lot” were combined into a single category labeled “Have learned.” For each EBP-education item, the level of educational experience was determined based on responses for both pre-licensure and in-service education. When participants reported different levels of experience across the two educational settings, the higher of the two was retained, following the rank order: “Have not learned at all” < “Have not learned” < “Neither” < “Have learned.”
c Literature databases refer to resources such as PubMed and Ichushi Web, a bibliographic database indexing primarily Japanese-language literature on medicine, nursing, dentistry, and pharmacy.
d Databases for clinical practice guidelines and systematic reviews refer to resources such as the Minds Guideline Library, a database for domestic clinical practice guidelines published in Japan, and the Cochrane Library.
e The four components are as follows: (1) the patient’s clinical state and circumstances, (2) research evidence, (3) the patient’s preferences and actions, and (4) clinical expertise.
B: unstandardized coefficients; CI: confidence interval; EBP: evidence-based practice; PECO: Patient, Exposure, Comparison, Outcome; PICO: Patient, Intervention, Comparison, Outcome; SE: standard error; ΔR²: increase in R-squared attributable to adding the variable to a model that already contains all other variables; i.e., the variable’s semi-partial R² (unique contribution); ΔF: partial F statistic for adding the variable to the model.
Table 5. Regression results for the EBP knowledge and skills score a, including all variables.
DISCUSSION
This study investigated the extent of Japanese hospital nurses’ experience of receiving specific educational content related to each step of EBP in both pre-licensure and in-service education and examined its association with EBP knowledge and skills. The findings showed that the experience of receiving EBP education was limited overall, with even lower levels observed for skills-related items. In both pre-licensure and in-service education, fewer than 10% of nurses reported having learned how to formulate clinical questions using the PICO/PECO framework, characteristics and search methods of databases for clinical practice guidelines and systematic reviews, how to search using databases for clinical practice guidelines and systematic reviews, and how to evaluate the outcomes of EBP. Additionally, a statistically significant dose-response relationship was observed between the extent of education received across the five EBP steps and the level of EBP knowledge and skills. Furthermore, in all EBP-education items, higher item-specific experience of receiving EBP education was significantly associated with greater EBP knowledge and skills scores. Furthermore, relative importance analysis showed three leading contributors. These were Step 5—Skills (evaluating EBP outcomes), Step 2—Knowledge (characteristics and search methods of databases for clinical practice guidelines and systematic reviews), and Step 4—Knowledge (the four components of Step 4). These findings suggest that comprehensive exposure to EBP education may play a critical role in developing EBP competencies. Additionally, the observed dose–response between the extent of experience of EBP education and knowledge/skills aligns with Kirkpatrick Level 2 (Learning)—i.e., greater educational coverage is associated with stronger learning outcomes [16]. While our endpoints were confined to Level 2, the model indicates that strengthened learning can support subsequent behavior (Level 3) and results (Level 4). Thus, future studies should extend the evaluation to Levels 3 and 4.
Our findings indicated that nurses’ experience of receiving EBP education was generally limited. Except for items related to literature databases, fewer than 25% of nurses reported having learned about any of the EBP-education items in pre-licensure education. The percentage of nurses who had learned about each EBP-education item in in-service education was consistently below 25%. Although EBP education has been insufficiently embedded in both pre-licensure and in-service curricula in Japan [31,32], such limited exposure is not unique to Japan. Recent reviews have reported that, worldwide, many nurses have never received EBP education [12] and that the overall level of EBP knowledge and skills among nurses remains low [33]. These findings highlight the urgent global need to improve EBP education. However, both pre-licensure and in-service education settings lack sufficient educators capable of providing EBP education [8, 34]. This shortage is likely a major contributor to nurses having limited experience in receiving EBP education. Therefore, developing and implementing training programs to equip educators with the competencies needed to provide EBP education is important. In so doing, the infrastructure for teaching EBP could be strengthened, and EBP implementation in nursing practice can be promoted.
In the present study, a stepwise increase in EBP knowledge and skills scores was observed as the number of EBP steps for which education had been received increased, indicating an association between the comprehensiveness of the EBP education and competency level. Additionally, the item-specific experience of receiving EBP education was positively associated with EBP knowledge and skills scores across all EBP-education items, and a relative importance analysis indicated that the Step 4 and Step 5 items were placed toward the upper end of the contribution rankings. These findings provide quantitative evidence that supports the argument that education encompassing all five steps of EBP is important to improve EBP knowledge and skills [35]. One systematic review has indicated that EBP educational programs tend to focus solely on Steps 1 to 3 of the five steps of EBP [36]. Therefore, future EBP education programs must comprehensively incorporate all five steps rather than only focus on specific ones. At the same time, in the present study, even among nurses who had received education on all five steps, the mean EBP knowledge and skills score was 35.5 on a scale ranging from 9 to 63, indicating that their competency levels remained insufficient. This suggests that to develop EBP competencies, both an adequate extent of educational content and appropriate educational delivery methods are required. In other words, providing practical education programs focused on EBP could be necessary to improve EBP competency levels among nurses effectively. However, EBP education is often integrated into broader courses, such as nursing research or statistics, and is rarely offered as a stand-alone program [8, 9, 10, 11]. Therefore, developing practical, EBP-specific educational programs would be essential to improve nurses' EBP knowledge and skills effectively.
Limitations
This study had several limitations. First, because of the cross-sectional design, a causal association between the experience of receiving EBP education and EBP knowledge and skills cannot be established; however, a statistically significant trend was observed in which EBP knowledge and skills scores increased with the amount of EBP education received, as indicated by the p for trend. This finding serves as additional evidence supporting a dose-response relationship between the two. Second, because the response rate was 28.7%, we must include the possibility of selection bias in which people with relatively more interest in EBP were selected. Third, the study relied on self-reported participant experience with EBP education, which may have introduced recall bias. To obtain a more objective understanding of EBP education's current status, future research should directly investigate institutions such as universities, vocational schools, and healthcare facilities by examining their course offerings, content, and number of instructional hours. Fourth, because our survey data were collected in 2022 (June–September), the findings may not fully reflect the current landscape of EBP education. However, the first explicit mention of EBP in Japan’s pre-licensure education was included in the Model Core Curriculum for Nursing Education (2024 revision) in March 2025 [37]; as this reform will chiefly affect future cohorts, any immediate influence on the educational exposure of the current hospital nursing workforce is likely modest. Finally, this study was conducted in Japan, where EBP education has not been fully promoted. This geographic specificity means that comparisons with findings from countries having more advanced EBP education should be made with caution. Despite this, the results may offer valuable insights, particularly for countries where EBP education is still in its early stages of promotion.
CONCLUSION
We investigated the extent to which hospital nurses in Japan had experienced receiving specific educational content related to each step of EBP in both pre-licensure and in-service education; we also examined its association with EBP knowledge and skills. Fewer than 25% of nurses reported having learned about any of the EBP-education items except for characteristics and search methods of literature databases in pre-licensure education, and fewer than 25% reported having learned about each EBP-education item in in-service education. A dose–response relationship was observed between the number of EBP steps for which education was received and the level of EBP competency. Additionally, the item-specific experience of receiving EBP education was positively associated with EBP knowledge and skills scores across all EBP-education items, and a relative importance analysis indicated that the Step 4 and Step 5 items were placed toward the upper end of the contribution rankings. In the future, to effectively improve the EBP knowledge and skills of nurses, it would be essential to: (1) design educational programs that comprehensively cover all five steps rather than only placing focus on specific steps; (2) develop practical, EBP-specific educational programs; and (3) develop educational programs that enable EBP educators to cultivate professionals capable of delivering such education.
List of abbreviations
EBP: evidence-based practice
PICO: Patient, Intervention, Comparison, Outcome
PECO: Patient, Exposure, Comparison, Outcome
Competing interest
The authors declare that they have no competing financial interests or personal relationships that may have influenced the work reported in this study.
Funding sources
No external funding.
Author contributions
All authors listed meet the authorship criteria according to the guidelines of the International Committee of Medical Journal Editors and agree with the manuscript. Hideaki Furuki: Conceptualization, Methodology, Formal analysis, Investigation, Data curation, Visualization, writing – original draft, writing – review, and editing, and project administration. Nao Sonoda: Conceptualization, Methodology, Formal analysis, Investigation, Data curation, Visualization, writing-review and editing, and project administration. Akiko Morimoto: Conceptualization, Methodology, Formal analysis, Investigation, Data curation, Visualization, writing – review and editing, project administration.
Acknowledgments
We are grateful to all the participants who participated in this study. We thank Miwa Fukumitsu, Haruna Sakamoto, and Risa Koike for their contributions to this study.
REFERENCES
- Melnyk BM, Fineout-Overholt E, Stillwell SB, Williamson KM. Evidence-based practice: Step by step: The seven steps of evidence-based practice. Am J Nurs. 2010;110(1):51–53. doi:10.1097/01.NAJ.0000366056.06605.d2
- Connor L, Dean J, McNett M, Tydings DM, Shrout A, Gorsuch PF, et al. Evidence-based practice improves patient outcomes and healthcare system return on investment: Findings from a scoping review. Worldviews Evid Based Nurs. 2023;20:6–15. doi:10.1111/wvn.12621
- Melnyk BM, Fineout-Overholt E, Giggleman M, Choy K. A test of the ARCC model improves implementation of evidence-based practice, healthcare culture, and patient outcomes. Worldviews Evid Based Nurs. 2017;14(1):5–9. doi:10.1111/wvn.12188
- Wu Y, Brettle A, Zhou C, Ou J, Wang Y, Wang S. Do educational interventions aimed at nurses to support the implementation of evidence-based practice improve patient outcomes? A systematic review. Nurse Educ Today. 2018;70:109–114. doi:10.1016/j.nedt.2018.08.026
- Knežević D, Jović D, Petković M. The impact of introducing a nursing education protocol on the incidence of Clostridium difficile infections in the hospital environment: A quasi-experimental study. NSC Nursing. 2023;2(4):62–84. doi:10.32549/OPI-NSC-89.
- American Association of Colleges of Nursing. The Essentials: Core Competencies for Professional Nursing Education. Washington (DC): AACN; 2021. [Internet]. Available from: https://www.aacnnursing.org/Portals/0/PDFs/Publications/Essentials-2021.pdf (Accessed: September 6, 2025).
- American Nurses Association. Nursing: Scope and Standards of Practice. 4th ed. Silver Spring (MD): American Nurses Association; 2021.
- Hung HY, Huang YF, Tsai JJ, Chang YJ. Current state of evidence-based practice education for undergraduate nursing students in Taiwan: A questionnaire study. Nurse Educ Today. 2015;35:1262–1267. doi:10.1016/j.nedt.2015.05.001
- Malik G, McKenna L, Griffiths D. An analysis of evidence-based practice curriculum integration in Australian undergraduate nursing programs. GSTF J Nurs Health Care. 2015;3(1):158–164. doi:10.7603/s40743-015-0029-z
- Skela-Savič B, Gotlib J, Panczyk M, Patelarou AE, Bole U, Ramos-Morcillo AJ, et al. Teaching evidence-based practice (EBP) in nursing curricula in six European countries – A descriptive study. Nurse Educ Today. 2020;94:104561. doi:10.1016/j.nedt.2020.104561
- Song CE, Kim WG, Lim YJ. An analysis of evidence-based practice courses in Korean nursing education systems. 2019;5(10):e02650. doi:10.1016/j.heliyon.2019.e02650
- Furuki H, Sonoda N, Morimoto A. Factors related to the knowledge and skills of evidence-based practice among nurses worldwide: A scoping review. Worldviews Evid Based Nurs. 2023;20:16–26. doi:10.1111/wvn.12623
- Alqahtani N, Oh KM, Kitsantas P, Rodan M. Nurses’ evidence-based practice knowledge, attitudes and implementation: A cross-sectional study. J Clin Nurs. 2020;29(1–2):274–283. doi:10.1111/jocn.15097
- Filippini A, Sessa A, Di Giuseppe G, Angelillo IF. Evidence-based practice among nurses in Italy. Eval Health Prof. 2011;34(3):371–382. doi:10.1177/0163278710387924
- Tomotaki A, Fukahori H, Sakai I. Exploring sociodemographic factors related to practice, attitude, knowledge, and skills concerning evidence-based practice in clinical nursing. Jpn J Nurs Sci. 2020;17(1):e12260. doi:10.1111/jjns.12260
- Kirkpatrick JD, & Kirkpatrick WK. Kirkpatrick’s four levels of training evaluation. Alexandria: ATD Press; 2016.
- Ministry of Education, Culture, Sports, Science and Technology; Ministry of Health, Labour and Welfare; Ministry of Economy, Trade and Industry. Ethical guidelines for medical and biological research involving human subjects. 2024. Japanese. [Internet]. Available from: https://www.lifescience.mext.go.jp/files/pdf/n2181_01.pdf (Accessed: September 6, 2025).
- Furuki H, Sonoda N, Morimoto A. Relationship between evidence-based practice knowledge and skills and evidence-based practice implementation in subgroups of professional and work environment factors among hospital nurses: A cross-sectional study. Jpn J Nurs Sci. 2025;22(4):e70018. doi:10.1111/jjns.70018
- Tomotaki A, Fukahori H, Sakai I, Kurokohchi K. The development and validation of the Evidence-Based Practice Questionnaire: Japanese version. Int J Nurs Pract. 2018;24(2):e12617. doi:10.1111/ijn.12617
- Leung K, Trevena L, Waters D. Systematic review of instruments for measuring nurses’ knowledge, skills and attitudes for evidence-based practice. J Adv Nurs. 2014;70:2181–2195. doi:10.1111/jan.12454
- Upton D, Upton P. Development of an evidence-based practice questionnaire for nurses. J Adv Nurs. 2006;53(4):454–458. doi:10.1111/j.1365-2648.2006.03739.x
- International Council of Nurses. Guidelines on Advanced Practice Nursing 2020. Geneva: International Council of Nurses; 2020. Available from: https://www.icn.ch/resources/publications-and-reports/guidelines-advanced-practice-nursing-2020 (Accessed: September 6, 2025).
- Guyatt G, Rennie D, Meade MO, Cook DJ, editors. Users’ Guides to the Medical Literature: A Manual for Evidence-Based Clinical Practice. 3rd ed. New York: McGraw-Hill Education; 2015.
- Melnyk BM, Fineout-Overholt E. Evidence-based Practice in Nursing & Healthcare: A Guide to Best Practice. 5th ed. Philadelphia: Wolters Kluwer; 2023.
- Straus SE, Glasziou P, Richardson WS, Haynes RB. Evidence-Based Medicine: How to Practice and Teach EBM. 5th ed. Edinburgh: Elsevier; 2018.
- Albarqouni L, Hoffmann T, Straus S, Olsen NR, Young T, Ilic D, et al. Core competencies in evidence-based practice for health professionals: Consensus statement based on a systematic review and Delphi survey. JAMA Netw Open. 2018;1:e180281. doi:10.1001/jamanetworkopen.2018.0281
- Groemping U. Relative importance for linear regression in R: The package relaimpo. J Stat Softw. 2006;17(1):1–27. doi:10.18637/jss.v017.i01
- Groemping U. relimpo: Relative Importance of Regressors in Linear Models. Version 2.2-7; 2023. [Internet]. Available from: https://cran.r-project.org/web/packages/relaimpo/relaimpo.pdf (Accessed: September 6, 2025).
- Bi J. A review of statistical methods for determination of relative importance of correlated predictors and identification of drivers of consumer liking. J Sens Stud. 2012;27(2):87–101. doi:10.1111/j.1745-459X.2012.00370.x
- Tonidandel S, LeBreton JM. Relative importance analysis: A useful supplement to regression analysis. J Bus Psychol. 2011;26(1):1–9. doi:10.1007/s10869-010-9204-3
- Ministry of Education, Culture, Sports, Science and Technology. Model Core Curriculum for Nursing Education (2024 Revised Edition). 2025. Japanese. [Internet]. Available from: https://www.mext.go.jp/a_menu/koutou/iryou/mext_00021.html (Accessed: October 22, 2025).
- Tomotaki A, Sakai I, Fukahori H, Tsuda Y, Okumura-Hiroshige A. Factors affecting the critical appraisal of research articles in Evidence-Based practices by advanced practice nurses: A descriptive qualitative study. Nurs Open. 2023;10(6):3719-3727. doi:10.1002/nop2.1628
- Li H, Xu R, Gao D, Fu H, Yang Q, Chen X, et al. Evidence-based practice attitudes, knowledge and skills of nursing students and nurses: A systematic review and meta-analysis. Nurse Educ Pract. 2024;78:104024. doi:10.1016/j.nepr.2024.104024
- Abu-Odah H, Said NB, Nair SC, Allsop MJ, Currow DC, Salah MS, et al. Identifying barriers and facilitators of translating research evidence into clinical practice: A systematic review of reviews. Health Soc Care Community. 2022;30:e3265–e3276. doi:10.1111/hsc.13898
- Stevens KR. The impact of evidence-based practice in nursing and the next big ideas. Online J Issues Nurs. 2013;18(2):4.
- Albarqouni L, Hoffmann T, Glasziou P. Evidence-based practice educational intervention studies: A systematic review of what is taught and how it is measured. BMC Med Educ. 2018;18(1):177. doi:10.1186/s12909-018-1284-1
- Ministry of Education, Culture, Sports, Science and Technology. Model Core Curriculum for Nursing Education (2024 Revised Edition). 2025. Japanese. [Internet]. Available from: https://www.mext.go.jp/a_menu/koutou/iryou/mext_00021.html (Accessed: October 12, 2025).
This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
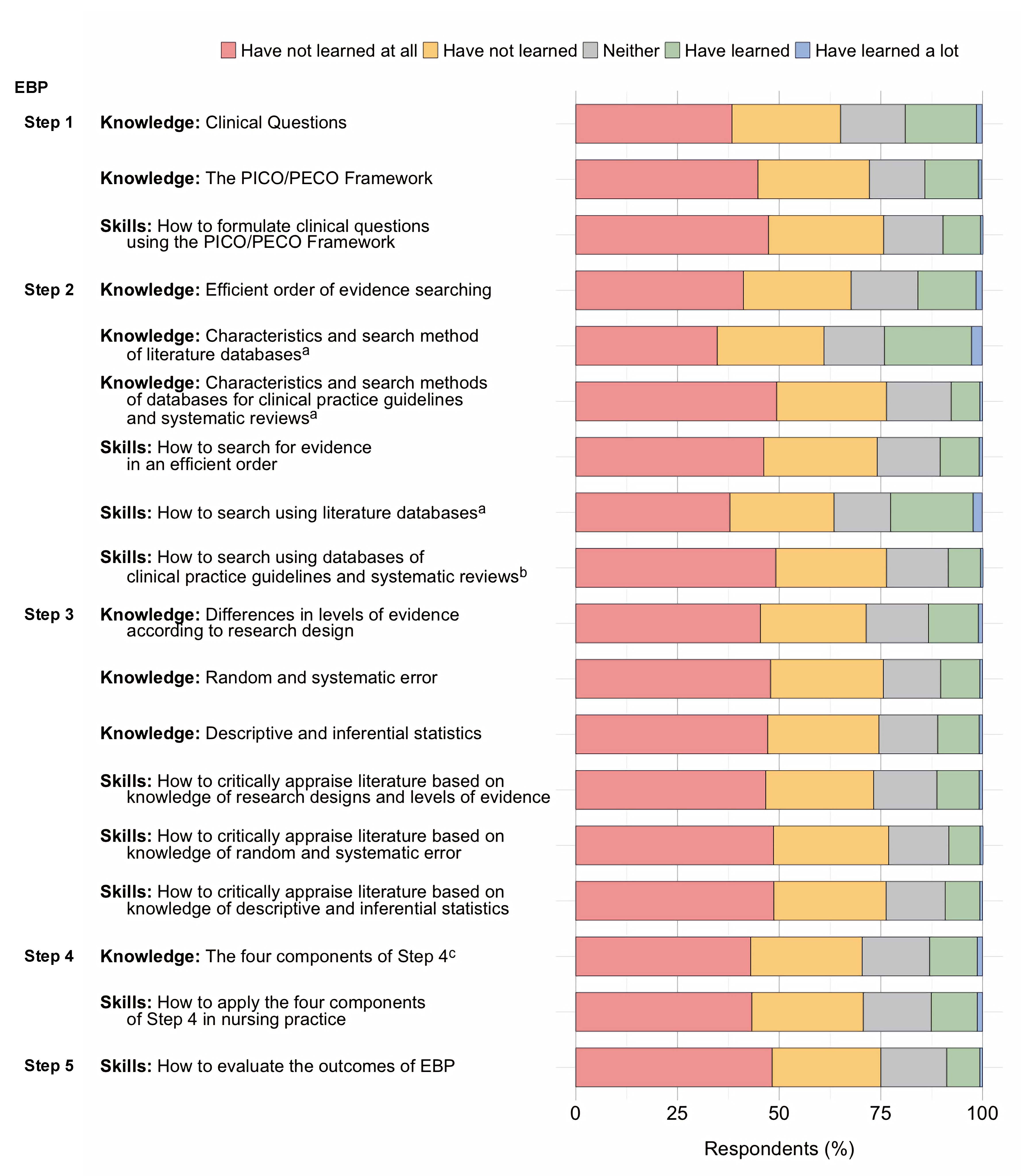
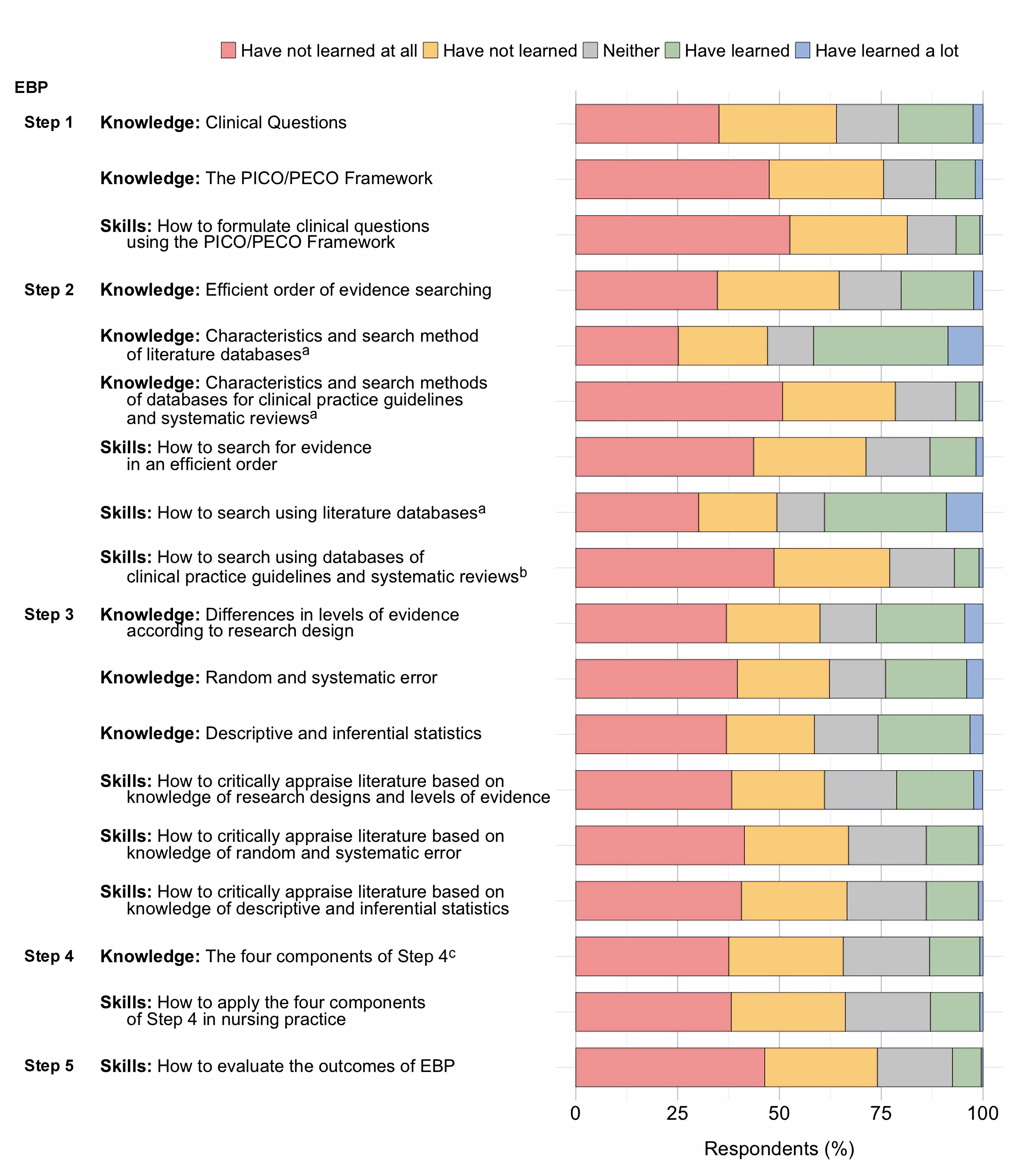
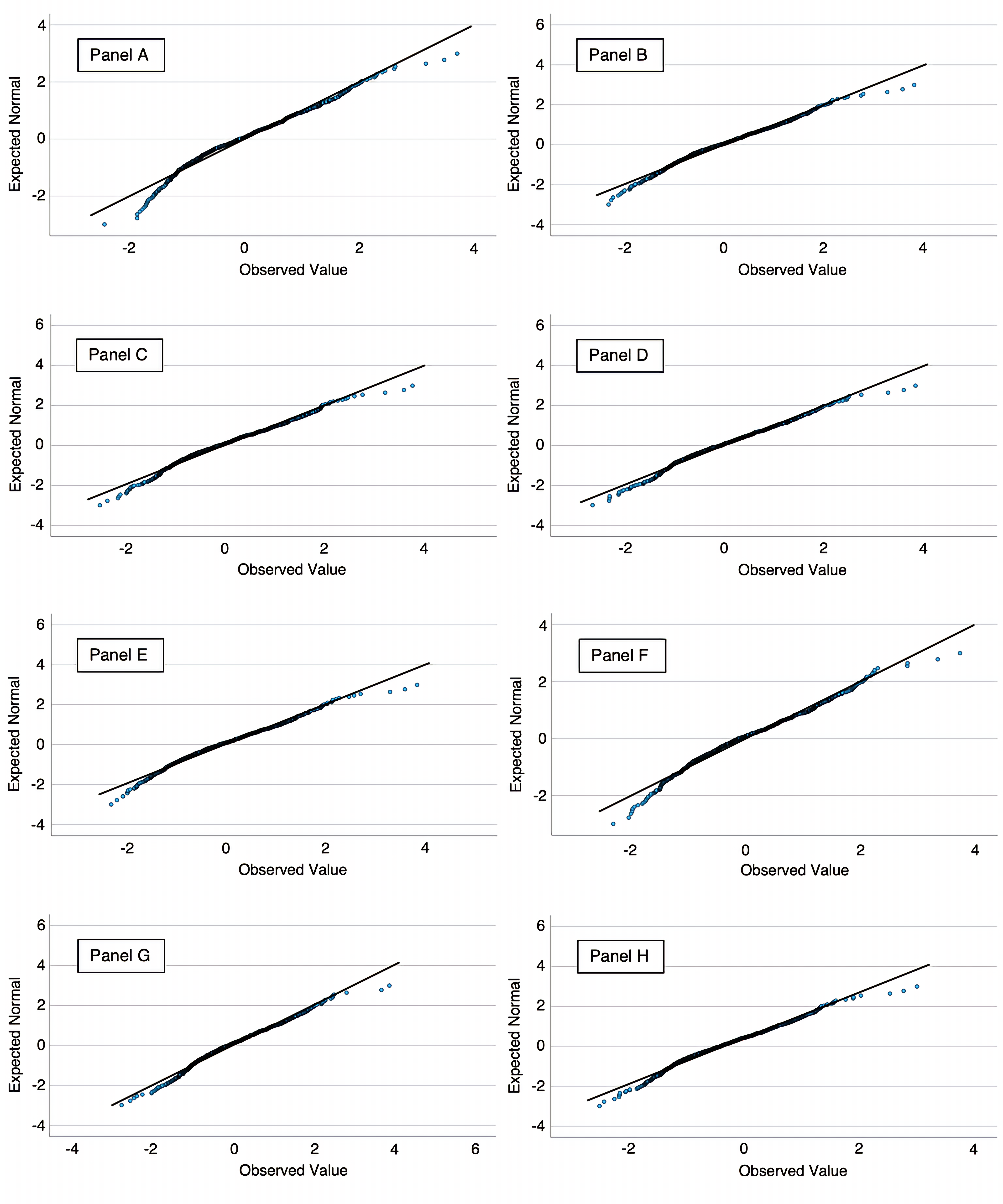
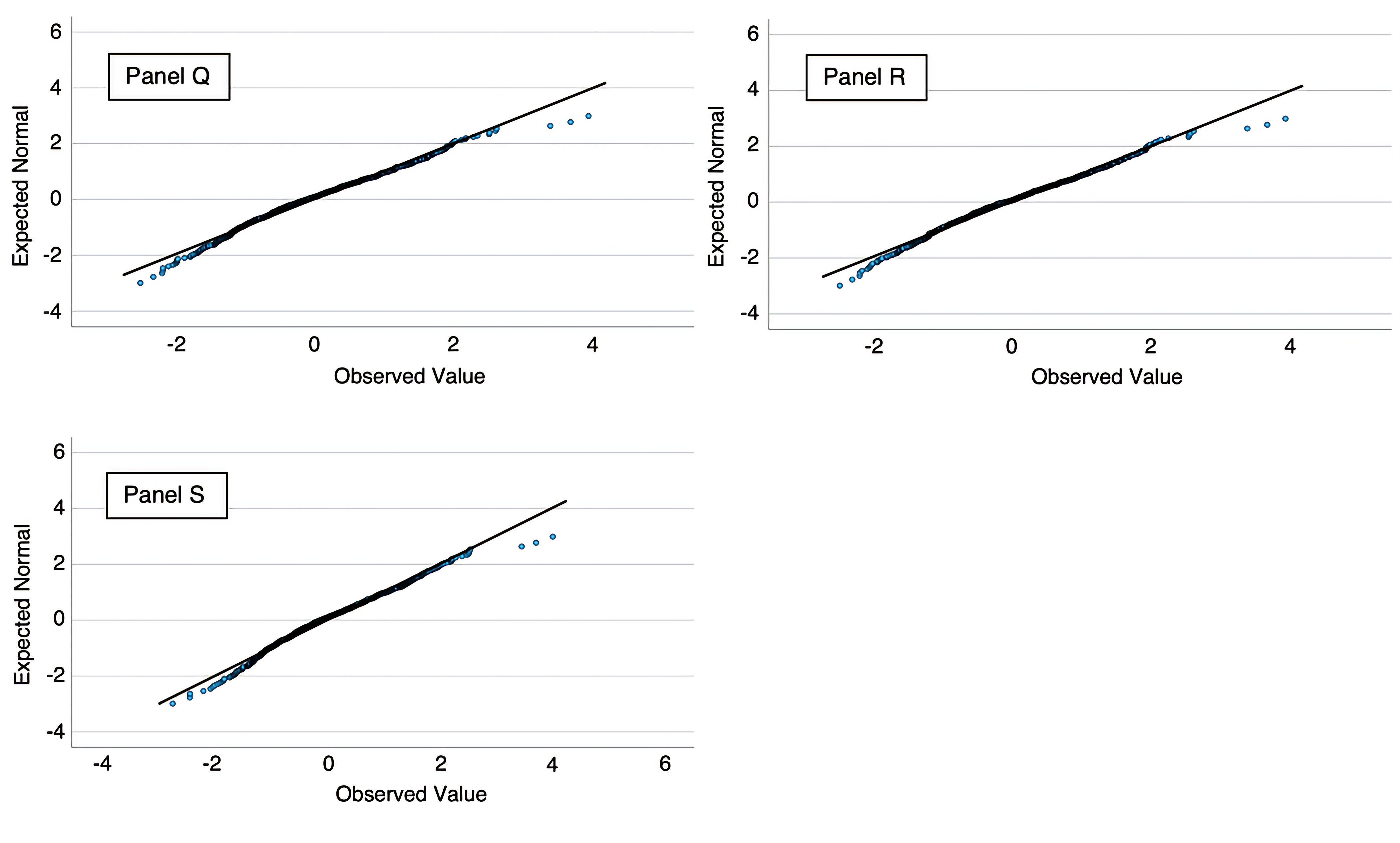
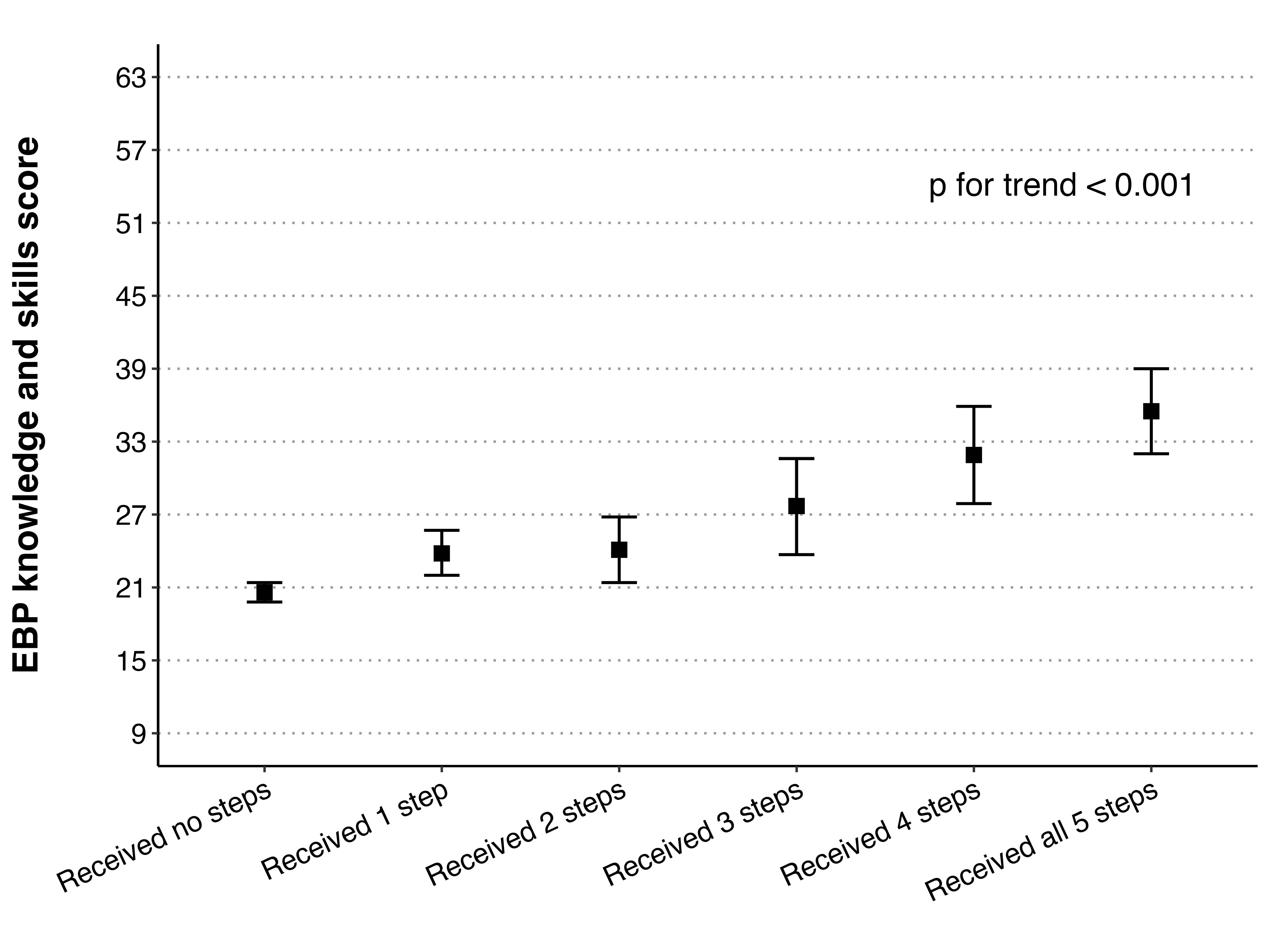
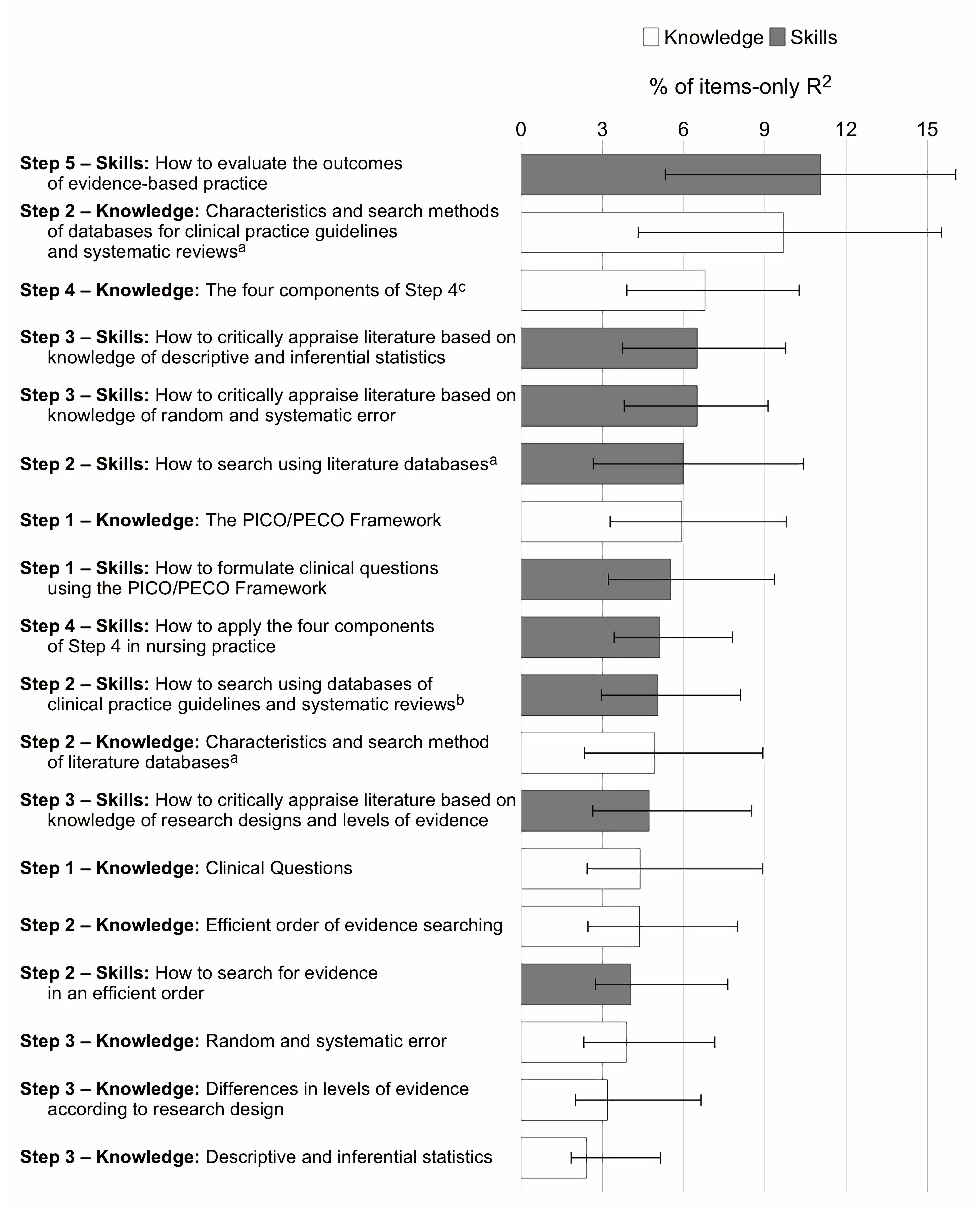
AUTISM SPECTRUM DISORDERS KNOWLEDGE: RESULTS FROM AN ITALIAN NURSING STUDENTS MULTICENTER CROSS-SECTIONAL STUDY
Martina Cotugno 1*, Flavio Prezzolini 2, Stefania Catanzaro 3, Emanuele Di Simone 4,
Marco Di Muzio 5, Alessio Mazzotta 3
- Department of Public Health and Infectious Diseases, Sapienza University of Rome, Rome, Italy.
- Department of Emergency Acceptance, Critical Areas and Trauma, University Hospital “Policlinico Umberto I”, Rome, Italy.
- Teaching Center for Healthcare Professions University Hospital “Policlinico Umberto I”, Rome, Italy.
- Department of Medical, Movement and Wellbeing Sciences, Parthenope University of Naples, Naples, Italy.
- Department of Clinical and Molecular Medicine, Sapienza University of Rome, Rome, Italy.
* Corresponding author: Martina Cotugno, master’s degree student in Nursing Sciences, Department of Public Health and Infectious Diseases, Sapienza University of Rome, (Rome), Italy. E-mail: martinacotugno72@gmail.com
Cite this article
ABSTRACT
Introduction: Autism spectrum disorders (ASD) represent a constantly evolving neurodevelopmental condition that requires specific preparation by the entire multidisciplinary team. However, multiple scientific evidences report little training on ASD in nursing degree courses. The study above aims to assess the level of theoretical knowledge of Italian students regarding autism in pediatric age.
Materials and Methods: A multicenter cross-sectional study was conducted on 104 students enrolled in the Nursing degree programme, regularly enrolled in the 2nd and 3rd years of the course at different Italian universities, with or without previous experience in pediatric or mental health services. Knowledge was assessed by administering a validated questionnaire, the Knowledge About Childhood Autism Among Healthcare Workers (KCAHW). Sociodemographic variables and information on training and placement experience with children with ASD were collected. Data were analysed using descriptive and inferential statistics.
Results: The average score obtained on the KCAHW was 9.5 out of 19 (SD = 2.78), indicating an insufficient level of knowledge. Scores were significantly higher among students with direct experience with children with ASD (median: 11.0 vs. 9.3; p=0.015) and among female students than male students (mean: 9.9 vs. 8.7; p=0.016). Theoretical training and age were not significantly different.
Discussion: The results indicate the existence of a vital training gap. Direct clinical experience proves to be decisive in the improvement of theoretical knowledge. Integrating compulsory modules and structured ASD training in nursing education is recommended to ensure competent, small patient-centred care.
Keywords: Autism Spectrum Disorder (ASD); nursing education; undergraduate nursing students; theoretical knowledge; KCAHW questionnaire.
INTRODUCTION
Autism spectrum disorders (ASD) are a neurodevelopmental disorder that is steadily evolving worldwide. According to the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) [1], ASD symptoms are defined “persistent deficits in social communication and social interaction across multiple contexts […] restricted, repetitive patterns of behaviour, interests, or activities”, moreover, the DSM-5 frames ASD as a single spectrum condition, replacing previous categorical subtypes and recognizing both the clinical variability and the differing levels of support individuals may need. In 2022, the World Health Organisation (WHO)’s International Classification of Diseases, 11th Revision (ICD-11) provided a similar definition, highlighting the symptoms' pervasive nature and clinical variability [2]. The global prevalence is estimated at around 0,6%. A recent meta-analysis estimated the global prevalence of ASD to be around 1% [3]. Data from the Global Burden of Disease Study estimates that approximately 1 in 127 individuals is affected by an autism spectrum disorder, corresponding to approximately 61.8 million people [4]. In Italy, a national study on children between 7 and 9 years old has identified a prevalence between male and female genders of 4.4:1 [5,6]. These data, gathered from surveys conducted across the entire school-age population in three Italian regions, confirm trends consistent with global trends [5]. The early increase in diagnosis has been attributed to improved screening procedures and greater social awareness. Despite the high prevalence of autism spectrum disorders and the complexity of care they entail, numerous studies show a significant lack of specific training among nurses and, more generally, among healthcare professionals. According to a systematic review, most healthcare professionals report low self-efficacy, a low level of theoretical knowledge and relational difficulties when interacting with patients with ASDs [7]. The results indicate that both undergraduate education on autism is highly heterogeneous and often not mandatory, leading to educational gaps that translate into suboptimal quality of care. An Italian study revealed that more than 60% of pediatric nurses did not receive any specific training on autism spectrum disorders during their academic career [8]. Furthermore, less than 40% consider themselves prepared to manage the nursing care of a child with ASD in both hospital and community settings [8]. Critical issues include lacking communication skills, difficulty using specific behavioural strategies, and limited knowledge of augmentative alternative communication (AAC) tools. This situation is also confirmed internationally. A pilot study on educational programs in the USA has shown that only 10-15% of nursing degree courses include compulsory modules on ASD [9]. A survey of nursing professors pointed out that in most nursing schools, there are no structured courses on autism and, when they are present, they are often limited to short theoretical references [10]. However, more recent studies have confirmed these critical issues internationally. Various studies have shown that, in clinical simulation settings, students show difficulties in emotional and communicative management with patients with ASD [11]. In addition, further studies report that both nurses and students are still partially prepared, underlining the need for specific and standardised training programmes between universities [12-14]. Further studies have confirmed that barriers to caring for patients with ASD are amplified by poorly structured training and poor communication skills among health professionals [7,15]. A systematic review has also highlighted critical issues in health services and communication between professionals, patients and caregivers [16]; in addition, the Italian Ministry of Health provides official information and materials aimed at families and professionals [17]. The guidelines issued by the Italian National Institute of Health (ISS) are now a key reference point for diagnosing and managing autism in Italy. On World Autism Awareness Day, the ISS released data and promoted awareness initiatives. The study highlights the urgent need to include specific content on autism in university programmes, combining a theoretical approach with practical experience in specialist contexts, to ensure safe, competent and truly person-centred care. Despite the obvious clinical and care relevance of autism in Italy, studies assessing nursing students' knowledge of ASD are still lacking. Most research focuses on pediatric nurses already in the working context, while there is little evidence analysing basic training during the university course. This study was conceived to respond to this deficiency to assess Italian nursing students' knowledge of pediatric autism, using a validated instrument, the KCAHW, and involving several university venues throughout Italy. The study intends to offer an up-to-date overview of students' awareness and preparation by highlighting educational inhomogeneities among the various universities and verifying the consistency between internship experiences and the competence acquired on the topic. In summary, this study contributes to the scientific and academic debate on integrating autism training into nursing curricula, with potential implications for the practical training of healthcare professionals and, indirectly, the quality of care provided to pediatric patients with autism.
MATERIALS AND METHODS
Study Designed
A cross-sectional study was conducted to assess the level of knowledge among nursing students about autism spectrum disorders. The aforementioned study design involved the administration of a validated questionnaire, the Knowledge About Childhood Autism Among Healthcare Workers (KCAHW), to a heterogeneous sample of undergraduate students in a single period to replicate the students' theoretical background acquired during their education. Using a validated tool such as the KCAHW aligns with recent methodological approaches that use paediatric simulations or standardised patients with ASD to evaluate training effectiveness [11,20,21]. The KCAHW contains 19 questions divided into four domains:
- Domain 1: 8 questions on inappropriate social interactions in children with ASD;
- Domain 2: 1 question on impaired communication and language development;
- Domain 3: 4 questions on obsessive-compulsive, repetitive and stereotypical behaviours;
- Domain 4: 6 questions on comorbidity and age of onset of the disorder.
Each item has three answer options, only one of which is correct. Correct answers are worth 1 point, while incorrect answers or “don't know” answers are worth 0 points. The total score ranges from 0 to 19, with higher scores indicating greater knowledge. In the literature, a cut-off of 60% correct answers has been proposed to identify a minimum basic level of knowledge. Previous studies have reported satisfactory internal consistency (Cronbach's α =0.97) and adequate content validity for the KCAHW [22].
Study site
The survey was administered online using Google Forms in July 2024. Students who were enrolled in ten nursing degree courses throughout Italy were involved. The universities involved were: Sapienza University of Rome, “Aldo Moro” of Bari, University “del Salento” of Lecce, “Federico II” of Naples, University of Palermo, “Gabriele D'Annunzio” of Chieti-Pescara, "Bicocca" of Milan, and the Universities of Bologna, Firenze and Trieste.
Participants
The sample was composed using a combination of convenience and snowball sampling strategies. Participants were first recruited through convenience sampling, as this approach allowed us access to readily available individuals willing to participate. Then, a snowball sampling strategy was applied to expand the sample and include participants who might otherwise have been difficult to reach, whereby early respondents enrolled additional eligible participants through diffusion of the survey link (direct access to the Google Form platform). The final sample consisted of 104 students enrolled in the nursing degree programme, chosen according to the following inclusion criteria: Enshrined in the second or third year of the degree programme. Previous experience in paediatric or child mental health services was not considered an inclusion criterion but was recorded as a descriptive variable.
For analytical purposes, age was categorized into three groups (18-20, 20-22, ≥23 years). This classification was not intended to represent clinical thresholds but was based on the distribution of the sample and on the typical progression within the nursing degree programme (early years, middle years and delayed or outside prescribed time students).
Ethical considerations
This study adhered to the ethical standards outlined in the Helsinki Declaration and complied with General Data Protection Regulation-EU Regulation 679/2016 (GDPR). According to the Regulation for the functioning of the “Comitato Etico per la Ricerca Transdisciplinare (CERT)” of Sapienza University (Protocol 103110, 31 May 2024), anonymous, non-interventional studies that do not involve the collection of sensitive personal data are exempt from formal ethical approval. As our study fulfilled these criteria, no ethical review was required. Indeed, no sensitive personal data was collected; the questionnaire was designed to gather only general, non-identifiable information. The Google Forms platform, as set by the authors, did not collect any e-mail addresses and automatically anonymised responses with progressive numeric codes, so no personal identification was possible. The participation in the study through questionnaire response implied the acceptance of informed consent to participate, where characteristics and all data collection modalities were reported. Moreover, responders could abandon the survey at any time if the questions were deemed too personal or inappropriate, without any partial responses being collected. The authorisation of the survey administration to students was obtained from the Director of the nursing degree programme, following a previous evaluation of the survey items, structure, and questions.
Statistical analysis
Quantitative variables were described as mean ± standard deviation (SD) if normally distributed, or as median and interquartile range (IQR) if not. Categorical variables were presented as absolute frequencies and percentages. The normality of distributions was verified using the Shapiro-Wilk test, while the homogeneity of variances was verified using Levene's test. Comparisons between two independent groups were performed using the t-test for independent samples when the assumptions of normality and homoscedasticity were met; otherwise, the non-parametric Mann-Whitney U test was applied. Comparisons between more than two groups were performed using one-way ANOVA only in the presence of normal distribution and homoscedasticity; otherwise, the Kruskal-Wallis test was used. Box plots were used for the graphical representation of scores: the horizontal line inside the box represents the median, the box limits correspond to the 25th and 75th percentiles (IQR), and the whiskers indicate the minimum and maximum values. All tests with p-values < 0.05 were considered significant. The internal consistency of the KCAHW was assessed using Cronbach’s α coefficient, calculated on the overall sample. To conclude descriptive statistics were used to summarise the socio-demographic characteristics of the sample. All analyses were performed using IBM SPSS Statistics, version 27.0.
RESULTS
The study included 104 nursing students. The highest response rate was found among the Sapienza University students of Rome, representing approximately 71% of the total participants. The majority were female (71%), with a relatively even age distribution between the groups, 20-22 years (48%) and over 22 (48%). Only 21.1% reported that they had received specific training on ASD during their training, while 14.4% stated that they had cared for children with autism during their internship experience. The average score on the questionnaire was 9.5 out of 19 (SD=2.78), with values ranging from 1 to 15 (Table 1).
Mean Standard deviation (SD) Minimum value Maximum value Median 9.5 2.78 1.0 15.0 10.0 Table 1. KCAHW descriptive statistics
The distribution of the score suggests an insufficient general level of knowledge on the subject of autism in paediatric age. Table 2 shows the distribution of KCAHW scores across the four domains and the total score. Students scored highest in domain 1 (social interaction; mean=4.63, median=5) and domain 3 (repetitive behaviours; mean=2.45, median=3). The lowest performance was observed in domain 2 (communication; mean=0.40, median=0). Domain 4 (comorbidity and age of onset) showed a mean of 2.86 (median=3). The mean total score was 10.35 (SD=3.08, median=10; range 1-17), indicating overall insufficient knowledge.
Domain Items (n)
Standard deviation (SD) Mean Minimum value
Maximum value
Median Domain 1 social interaction
8 1.80 4.63 0 8 5 Domain 2 communication 1 0.49 0.40 0 1 0 Domain 3 Repetitive behaviours 4 1.10 2.45 0 4 3 Domain 4 Comorbidity and onset
6 1.24 2.86 0 5 3 Total score 19 3.08 10.35 1 17 10 Table 2. Distribution of scores across the four domains and total score KCAHW
Statistical tests were then conducted to assess the association between socio-demographic variables and the score obtained (Table 3).
Comparison Statistical test Statistical value p-value ASD training (yes or no) Mann-Whitney U U=1245.0 0.261 Internship experiences with children affected by ASD (yes or no) Mann-Whitney U
U=1080.0
0.015
Sex (female-male) t-test t=2.47 0.016 Age groups (18-20/20-22/≥23) Kruskal-Wallis H=0.49 0.612 Note: Parametric tests (t-test, one-way ANOVA) were applied only when assumptions of normality and homoscedasticity were met; otherwise, non-parametric alternatives (Mann–Whitney U, Kruskal–Wallis) were used. Table 3. Statistical test results
Students who had previously had placement experience with children with ASD scored significantly higher (median: 11.0 vs. 9.3; Mann-Whitney U=1080.0; p=0.015). Similarly, a difference in performance between students with and without clinical experience was also found in a study conducted in 2024, confirming the formative impact of internship activities [13].
Female gender was associated with a significantly higher score (mean: 9.9 vs. 8.7; t=2.47; p=0.016). There was no significant difference between those who had received specific training on autism spectrum disorders and those who had no organised courses on this topic in their curricula (Mann-Whitney U=1245.0; p=0.216). Age did not significantly impact the overall score statistically (Kruskal-Wallis H=0.49; p=0.612).
The scores obtained from the questionnaire were represented graphically as a function of training and clinical-practical internship experience. The box plots show greater variability and a higher median in the groups who have had training placement experience with children with autism spectrum disorders than in those who have not had clinical practice experience in this area. The internal consistency of the KCAHW, assessed through Cronbach’s α, was 0.54 in this sample, in line with other studies on student populations and confirming the multidimensional nature of the tool.
The box plot (Figure 1 and 2) represents the median (horizontal line inside the box), the interquartile range (IQR) (25th-75th percentile; extremes of the box), and the minimum and maximum values (whiskers).
In Figure 1, students who had received specific training on ASD reported higher median scores and less variability than those without training.
In Figure 2, students with internship experience with children with ASD obtained higher scores and a more compact distribution, indicating a generally higher and more homogeneous level of knowledge than the group without direct experience.
Figure 1. Distribution of KCAHW scores based on ASD training
Figure 2. Distribution of KCAHW scores based on internship experience
DISCUSSION
The study analysed the level of theoretical knowledge about autism in developmental age among students in a nursing degree program using a validated instrument, the KCAHW. The results show insufficient knowledge, with an average of less than half of the maximum achievable score. The domain analysis also showed that the lowest scores were obtained in the area of communication (domain 2), while relatively higher scores were found in social interaction (domain 1) and repetitive behaviours (domain 3). These results suggest that the communicative aspects of autism remain particularly underestimated among nursing students, highlighting a specific gap that training curricula should address. This finding is in line with what is reported in the international literature, where a general inadequacy of basic nursing education concerning neurodevelopmental disorders, particularly those of the autistic spectrum, is emphasised [7,10]. One of the most significant pieces of evidence that emerged concerns the positive association between internship experience with children with ASD and a higher score on the questionnaire. This result confirms the effectiveness of clinical-practical learning as a fundamental tool for consolidating theoretical knowledge and developing specific communication and relational skills [9]. In line with these findings, several studies have highlighted how direct field experience is associated with improved professional preparedness and safety [10,12,13]. Realistic simulation is also an effective educational strategy, as some studies have observed improvements in post-simulation communication skills [11,21]. The presence of field experience allows students to consciously confront the complexity of care related to autism spectrum disorders, favouring a less stereotypical approach. This finding aligns with numerous results that show that the perception of nurses' competencies is mainly linked to clinical experience and not only to theoretical training [14,26]. Also of great importance is the significant difference found in gender, with female students reporting higher average results than male students. This datum, already highlighted in other training contexts, could be linked to psycho-social variables such as a greater predisposition to helping relationships or a different motivation in the in-depth study of themes related to the behavioural and relational sphere. Contrary to expectations, the presence or absence of basic theoretical training on ASD did not show statistically significant differences in the scores obtained. This may reflect the poor systematisation and heterogeneity of the content available in the various courses of study and the predominantly theoretical nature of these training modules, which are not supplemented with practical experience. Similarly, the age of the students was not found to be predictive of the level of knowledge, suggesting that the accumulation of academic years does not necessarily guarantee greater competence on the subject. Some researchers propose the integration of new technologies in nursing education. Numerous studies highlight the effectiveness of virtual reality in training students in interactions with patients with autism spectrum disorders [27]. In contrast, others focus on using artificial intelligence to support healthcare professionals in managing ASDs [28]. Several qualitative studies based on clinical simulation have also highlighted areas for improvement in nursing education on autism spectrum disorders [29]. These new perspectives open up different scenarios for the training of healthcare professionals and deserve further investigation. The collected data show a substantial training gap within the Italian nursing curricula. A recent observational study found limited knowledge of nurses regarding autism spectrum disorders [30]. In light of the increasing prevalence of ASD and the growing need for healthcare professionals competent in the management of this population [31], there is an urgent need for the integration of structural, multidisciplinary and experience-based education. Some recent experiments suggest the integration of immersive technologies and intelligent tools to enhance the effectiveness of teaching. Virtual reality, in particular, has proven helpful in improving students' social and relational skills in simulated settings with patients with ASD [27]. Furthermore, the use of artificial intelligence to support early diagnosis and care planning is growing [28], with good results also in training healthcare professionals [32]. Finally, a following step forward is the specific training of pediatric nursing staff on common aggressive behaviours in children with ASD, as reported by several researchers who conducted a pilot RCT showing how simulation increases staff safety and operational skills [33].
Limitations
The study’s main limitations include the small sample size (n=104), the relatively low response rate across the ten university courses involved, and the non-probabilistic nature of the sampling, which limits the generalizability of the results to the entire Italian nursing student population. The low response rate may reflect the voluntary and self-administered nature of the survey, as well as the variability in students' availability and motivation to participate. This aspect could have introduced a further selection bias, as the students who responded may have been more interested or sensitised to the topic compared to those who did not. The choice of the sample was based on the availability and accessibility of students at specific university sites, introducing a possible selection bias. Secondly, a self-administered questionnaire may have exposed the results to social desirability bias or subjective interpretations of the questions, even though the KCAHW is internationally validated. Another limitation is the purely theoretical assessment of knowledge without in-depth exploration of practical or attitudinal expertise or the ability to apply the acquired knowledge in real clinical contexts. Furthermore, the training received was investigated with a single closed question without a qualitative-quantitative assessment of the training content addressed. Finally, as this is a cross-sectional study, it is impossible to establish causal relationships between the analysed variables, but only statistical associations. Forward-looking longitudinal studies could help us understand how knowledge evolves and the real impact of training programmes on acquiring specific competencies. Overall, the findings suggest that nursing students show insufficient knowledge of autism and limited attitudinal preparedness for managing children with ASD. This highlights the need for nursing curricula to include not only theoretical content, but also experiential and practical training aimed at improving students’ attitudes, confidence, and readiness to interact with autistic patients and their families
CONCLUSION
In conclusion, the study highlights the need for a more comprehensive theoretical education in ASD for nursing students, focusing on developing skills in the clinical setting. Educational strategies should therefore address both theoretical knowledge and students’ attitudes toward autism, fostering more adequate preparedness for clinical practice. The absence of statistical significance for the theoretical training received suggests a potential fragmentation and inhomogeneity of the content delivered in degree courses that would merit systemic reflection at an academic and institutional level. In light of the increase in the prevalence of ASD and the growing complexity of care that this condition entails, there emerges an urgent need to integrate specific, up-to-date content applicable in clinical practice into nursing education courses. In particular, it would be better if supervised internship experiences in specialist settings accompany the adoption of mandatory modules on autism within academic programmes. Further multicentre research and larger samples will be necessary to validate these results and further investigate the effectiveness of training interventions in terms of their practical-assistance spin-offs, with a view to continually improving the quality of care for the paediatric population with autism spectrum disorders. Finally, as highlighted in the international literature, an up-to-date and multidisciplinary understanding of autism spectrum disorders is fundamental to improving the quality of care and reducing inequalities in access to care [34]. However, in light of the sustainability of training programmes, it does not seem realistic to envisage the introduction of specific modules for each individual clinical condition. Rather, it would be appropriate to promote cross-cutting strategies aimed at enhancing students' preparation, motivation and attitude before each internship experience, so as to strengthen the link between theory and practice and promote more effective learning in different clinical contexts.
Conflicts of interest and sources of funding
The authors declare that they have no conflicts of interest. This research did not receive any external funding.
Author contributions
MC designed the study, collected the data, and wrote the first draft of the manuscript. FP and SC collected and analysed the data and critically reviewed the paper. MDM and EDS co-supervised the work, contributed to data analysis, and critically reviewed the content. AM supervised the study, and critically reviewed the manuscript. All authors participated in the final revision of the manuscript and approved the submitted version.
REFERENCES
- American Psychiatric Association. Diagnostic and statistical manual of mental disorders: DSM-5. 5a ed. Arlington, VA: American Psychiatric Association; 2013. doi: 10.1176/appi.books.978089042559
- World Health Organisation. International classification of diseases for mortality and morbidity statistics (11th revision). Available at: https://icd.who.int. Last access: July 09, 2025
- Salari N, Rasoulpoor S, Rasoulpoor S, Shohaimi S, Jafarpour S, Abdoli N, et al. The global prevalence of autism spectrum disorder: A comprehensive systematic review and meta-analysis. Ital J of Pediatr. 2022;48(1):112. doi: 10.1186/s13052-022-01310-w
- Global Burden of Disease Study 2021 Autism Spectrum Collaborators. The global epidemiology and health burden of the autism spectrum: Findings from the Global Burden of Disease Study 2021. Lancet Psychiatry. 2025;12(2):111–21. doi: 10.1016/S2215-0366(24)00363-8
- Scattoni ML, Fatta LM, Micai M, Sali ME, Bellomo M, Salvitti T, et al. Autism spectrum disorder prevalence in Italy: A nationwide study promoted by the Ministry of Health. Child Adolesc Psychiatry Ment Health. 2023; 17:73. doi: 10.1186/s13034-023-00673-0
- Istituto Superiore di Sanità. Autismo: Prevalenza stimata nella fascia d’età 7–9 anni in Italia – Rapporto Osservatorio Nazionale Autismo. Available from: https://www.iss.it/autismo. Last access: July 09, 2025.
- Corden K, Brewer R, Cage E. A systematic review of healthcare professionals’ knowledge, self-efficacy and attitudes towards working with autistic people. Rev J Autism Dev Disord. 2022; 9:386–99. doi: 10.1007/s40489-021-00263-w
- Corsano P, Cinotti M, Guidotti L. Paediatric nurses’ knowledge and experience of autism spectrum disorders: An Italian survey. J Child Health Care. 2020;24(3):486–95. doi: 10.1177/1367493519875339
- Giarelli E, Ruttenberg J, Segal A. Continuing education for nurses in the clinical management of autism spectrum disorders: Results of a pilot evaluation. J Contin Educ Nurs. 2012;43(4):169–76. doi: 10.3928/00220124-20111101-01
- Gardner MR, Suplee P D, Jerome-D’Emilia B. Survey of nursing faculty preparation for teaching about autism spectrum disorders. Nurse Educ. 2016;41(4):212–6. doi: 10.1097/NNE.0000000000000237
- Jiménez-Ruiz I, Pérez-Cabezas V, Carrillo de la Peña MT, Pozo Rodríguez F. Training nursing students with simulated patients with autism: Communicative and emotional skills development. Clin Simul Nurs. 2022; 66:1–10. doi: 10.1016/j.nepr.2022.103488
- Gercek Ö, Arslan S, Sobcali S. Healthcare students’ perceptions and attitudes towards peers with autism spectrum disorders. J Autism Dev Disord. 2024; doi: 10.1007/s10803-024-06368-5
- Gercek E, Celikkol Sadic Ç, Kocoglu G. The level of knowledge about autism spectrum disorders among healthcare professionals in a Turkish university hospital: A cross-sectional study. Turk J Clin Psychiatry. 2024;27(1):12–20. doi: 10.5505/tjcp.2023.375056
- Cashin A, Watson N, Newman C. Nurses’ knowledge and attitudes towards people with autism spectrum disorder: An international survey. Nurse Educ Today. 2021; 103:104937. doi: 10.1016/j.nedt.2021.104937
- Miri J, Colleague. An assessment of pediatric nurses’ awareness and perceived competence regarding autism spectrum disorder. J Autism Dev Pract. 2023. doi: 10.1155/2023/4815914
- Đorđević M, Glumbić N, Troshanska J. A systematic review of individuals with autism in the healthcare system: Experiences of healthcare workers, individuals with autism and their parents. Hrv Rev Rehabil Istraz. 2025; 61(1):131–43. doi: 10.31299/hrri.61.1.8
- Ministero della Salute. Disturbi dello spettro autistico – Informazioni ufficiali e materiali informativi. Available from: https://www.salute.gov.it/portale/autismo/. Last access: July 09, 2025
- Istituto Superiore di Sanità (ISS). Giornata mondiale della Consapevolezza dell’Autismo: in Italia un bimbo ogni 77. Available from: https://www.iss.it/?p=3421. Last access: July 09, 2025
- Istituto Superiore di Sanità (ISS). Introduction and methods of the evidence-based guidelines for the diagnosis and management of autism spectrum disorder by the Italian National Institute of Health. Health Qual Life Outcomes. 2020; 18:81. doi: 10.1186/s12955-020-01320-4
- Kim E, Song S, Kim S. Development of pediatric simulation-based education: A systematic review. 2023; 22:291. doi: 10.1186/s12912-023-01458-8
- Jiménez‐Ruiz I, Pérez‐Cabezas V, Carrillo‐de‐la‐Peña MT, Pozo‐Rodríguez F. What can be improved in learning to care for people with autism? A qualitative study based on clinical nursing simulation. 66:103488. doi: 10.1016/j.nepr.2022.103488
- Bakare M, Ebigbo P, Agomoh A, Menkiti N. Knowledge about childhood autism among health workers (KCAHW) questionnaire: description, reliability and internal consistency. Clin Pract Epidemiol Ment Health. 2008;4(17). doi: 1186/1745-0179-4-17
- World Medical Association. World Medical Association Declaration of Helsinki: Ethical principles for medical research involving human subjects. JAMA. 2013;310(20):2191–2194. doi: 10.1001/jama.2013.281053
- European Parliament and Council. Regulation (EU) 2016/679 of the European Parliament and of the Council of 27 April 2016 on the protection of natural persons with regard to the processing of personal data and on the free movement of such data, and repealing Directive 95/46/EC (General Data Protection Regulation). Available at: https://eur-lex.europa.eu/eli/reg/2016/679/oj. Last access: August 27, 2025
- Sapienza Università di Roma. Comitato Etico per la Ricerca Transdisciplinare (CERT). Available at: https://www.uniroma1.it/it/pagina/cert-comitato-etico-per-la-ricerca-transdisciplinare. Last access: August 27, 2025
- Cashin A, Watson N, Newman C. A survey of registered nurses’ educational experiences and self perceived capability to care for people with intellectual disability and/or autism spectrum disorder. J Intellect Dev Disabil. 2021; doi: 10.3109/13668250.2021.1967897
- Kourtesis P, Kouklari EC, Roussos P, Mantas V, Papanikolaou K, Skaloumbakas C, et al. Virtual reality training of social skills in autism spectrum disorder: an examination of acceptability, usability, user experience, social skills, and executive functions. arXiv; 2023. doi: 10.48550/arXiv.2304.07498
- Mohammadi Rouzbahani M, Karimipour H. Using artificial intelligence to support diagnosis and care in autism spectrum disorder: A review. arXiv; 2024. doi: 10.48550/arXiv.2407.08902
- Díaz Agea JL, Macías Martínez N, Leal Costa C, Girón Poves G, García Méndez JA, Jiménez Ruiz I. What can be improved in learning to care for people with autism? A qualitative study based on clinical nursing simulation. Nurse Educ Pract. 2022; 66:103488. doi: 10.1016/j.nepr.2022.103488
- Ferrara R, Campagna G, Ricci P, Damato F, Ricci L, Iovino L, et al. Developmental Psychology and Healthcare Professions: Autism Knowledge Among Nurses: An Observational Study. Clin Pract. 2024;14(6):2693–2704. doi: 10.3390/clinpract14060212
- Erdoğan Ç, Turan T. Determination of pediatric nurses’ knowledge of and attitudes towards childhood autism and CT recommendations. Trends Pediatr. 4(2):89–95. doi: 10.59213/TP.2023.84856
- Sandanasamy S, McFarlane P, Okamoto Y, Couper AL. Leveraging machine learning to enhance nurses’ practice for autism spectrum disorder care: A narrative review. J Nurs Res Clin Pract. 2024. doi: 10.32598/JNRCP.2408.1169
- Mitchell ML, Newall FH, Heywood MG, Sokol J, Williamss KJ. Simulation-based education for staff managing aggression and high risk behaviors in children with autism spectrum disorder in the hospital setting: A pilot and feasibility cluster randomized controlled trial. J Nurs Educ Pract. 2021;11(11):48. doi: 10.5430/jnep.v11n11p48
- Lord C, Elsabbagh M, Baird G, Veenstra-Vanderweele J. Autism spectrum disorder. Lancet. 392(10146):508–80. doi: 10.1016/S0140-6736(18)31129-2
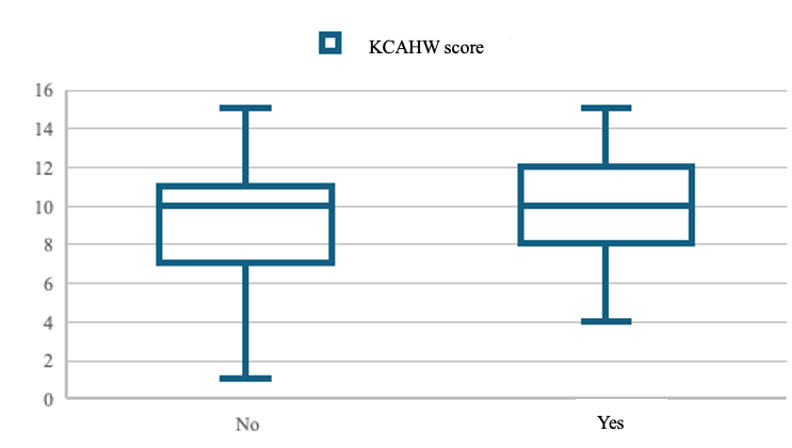
EXPLORING SELF-EFFICACY, FAMILY SUPPORT, AND POSTPARTUM DEPRESSION IN MOTHERS AFTER CRYPTIC PREGNANCY: A CROSS-SECTIONAL STUDY
Ifa Nofalia 1, Dwi Prasetianingati 1, Dessy Ekawati 1*
- Department of Nursing, Faculty of Health, Institute of Science and Health Technology Insan Cendekia Medika Jombang
* Corresponding author: Dessy Ekawati., Department of Nursing, Faculty of Health, Institute of Science and Health Technology Insan Cendekia Medika Jombang. E-mail: dessyekawati.s1201@gmail.com
Cite this article
ABSTRACT
Introduction: Cryptic pregnancy, or the delayed recognition of pregnancy until late gestation, poses unique psychological challenges for mothers due to the lack of prenatal preparation and sudden transition to motherhood. These circumstances may increase the risk of postpartum depression. Protective factors such as maternal self-efficacy and family support are believed to play an important role in reducing depressive symptoms after childbirth.
Objective: The purpose of this study is (1) to analyze the relationship between maternal self-efficacy and postpartum depression among mothers with a history of cryptic pregnancy, (2) to analyze the relationship between family support and postpartum depression, and (3) to assess the extent to which maternal self-efficacy and family support predict postpartum depression levels.
Materials and Methods: A cross-sectional study was conducted in Jombang Regency, East Java, Indonesia, from May to August 2025, involving 104 mothers with a history of cryptic pregnancy recruited by non-probability snowball sampling. Maternal self-efficacy was assessed using the 15-item questionnaire developed by Witungga et al. (2024; α = 0.916), family support with the 14-item questionnaire by the same authors (α = 0.836), and postpartum depression with the Edinburgh Postnatal Depression Scale (EPDS; Adli, 2022). Data were analyzed using Spearman’s rank correlation and ordinal logistic regression.
Results: Most respondents had moderate self-efficacy (72.1%), fair family support (65.4%), and no signs of postpartum depression (68.3%). Spearman’s correlation showed significant negative associations between self-efficacy (ρ = –0.426, p = 0.001) and family support (ρ = –0.398, p = 0.002) with postpartum depression. Multivariate ordinal logistic regression indicated that both self-efficacy (B = –0.462, p = 0.014, OR = 0.63, 95% CI = 0.44–0.91) and family support (B = –0.518, p = 0.012, OR = 0.60, 95% CI = 0.40–0.89) were significant protective factors, jointly explaining 28.9% of variance in postpartum depression (Nagelkerke R² = 0.289).
Conclusion: Maternal self-efficacy and family support are significant protective factors against postpartum depression in mothers with cryptic pregnancy. Strengthening maternal confidence and empowering family support systems are essential strategies to mitigate depressive symptoms in this vulnerable group.
Keywords: cryptic pregnancy, family support, maternal self-efficacy, postpartum depression
INTRODUCTION
Postpartum depression (PPD) is a major public health concern, affecting approximately 10–20% of mothers worldwide, with higher prevalence reported in low- and middle-income countries (LMICs) compared to high-income settings [1,2]. In Indonesia, national surveys have shown increasing rates of postpartum depressive symptoms, with prevalence reaching 11.2% in East Java in 2023, indicating a substantial and growing burden [3]. Despite these numbers, many cases remain undetected due to limited screening and strong sociocultural norms that discourage disclosure of psychological distress.
One critical factor influencing maternal adaptation is the level of social and family support. Numerous studies demonstrate that family support functions as a protective buffer against PPD, with inadequate support consistently linked to more severe depressive symptoms [4]. In particular, emotional responsiveness from partners and close relatives helps reduce maternal stress, facilitates the adjustment process to motherhood, and strengthens the bond between mother and infant. On the other hand, rejection, blame, or neglect from family members can worsen emotional instability and increase the risk of depressive outcomes.
Another important determinant of maternal well-being is maternal self-efficacy, defined as a mother’s belief in her ability to successfully care for her infant. Evidence indicates that higher maternal self-efficacy is associated with reduced depressive symptoms, more effective coping strategies, and better overall postpartum adjustment [5,6]. Mothers with low self-efficacy often report feelings of helplessness, decreased motivation to provide infant care, and heightened vulnerability to depression. Strengthening maternal confidence is therefore essential to preventive and therapeutic interventions in postpartum mental health.
Cryptic or denied pregnancy represents a unique context that has received little empirical attention. In this condition, pregnancy remains unrecognized until late gestation or even the onset of labor. Although traditionally considered rare, recent reviews suggest cryptic pregnancies may occur more frequently than previously assumed, and they present distinct psychosocial challenges for both mothers and families [7]. The lack of preparedness, combined with social stigma and disrupted family dynamics, places these mothers at particular risk of postpartum psychological distress. Yet, systematic research on PPD in women with cryptic pregnancies remains extremely limited.
Nurses play a central role in maternal and child health by conducting early screening, providing psychosocial education, and strengthening family-centered care systems. Understanding how maternal self-efficacy and family support influence postpartum depressive symptoms among mothers with cryptic pregnancies is therefore critical for nursing practice and policy.
Objective: This study aims to (1) analyze the relationship between maternal self-efficacy and postpartum depression among mothers with a history of cryptic pregnancy, (2) to analyze the relationship between family support and postpartum depression among mothers with a history of cryptic pregnancy, and (3) to assess the extent to which maternal self-efficacy and family support predict postpartum depression levels among mothers with a history of cryptic pregnancy.
MATERIALS AND METHODS
Study Population
This study was conducted in Jombang Regency, East Java, Indonesia, from April to July 2025. The target population included women who had experienced a cryptic pregnancy within the last one to two years. Due to the rarity and sensitive nature of cryptic pregnancy, a non-probability snowball sampling technique was employed. An initial group of participants (seed respondents) identified through community health centers and local networks served as starting points, and they referred other eligible women who had undergone similar experiences. A total of 104 respondents were successfully recruited.
The study protocol adhered to the ethical principles outlined in the Declaration of Helsinki and was approved by the Scientific and Ethics Committee of the Institute for Learning Development and Quality Assurance, Institute of Science and Health Technology Insan Cendekia Medika Jombang (Ref: LP3M/ICME/ETIK/0425/2025). All participants were fully informed about the study’s objectives and procedures and provided written informed consent prior to participation.
Inclusion Criteria
Participants were eligible for inclusion if they were women aged 18–40 years who had experienced a cryptic pregnancy that resulted in a live birth within the previous 12 months. They were required to be able to read and write in Indonesian, possess adequate cognitive capacity to complete the questionnaire independently, and provide informed consent voluntarily. These criteria were established to ensure that participants could fully understand and respond to the study instruments with accuracy and autonomy.
Exclusion Criteria
Women were excluded from the study if they had a current diagnosis or documented history of major psychiatric disorders such as schizophrenia, bipolar disorder, or major depressive disorder prior to the pregnancy. Additionally, individuals who had experienced fetal loss (miscarriage or stillbirth), or who were undergoing psychiatric treatment unrelated to postpartum depression at the time of data collection, were also excluded. These exclusion criteria aimed to minimize potential confounding effects on the assessment of postpartum depression symptoms.
Instruments
Three validated instruments were used in this study. Maternal self-efficacy was measured using a 15-item Likert-scale questionnaire developed by Witungga et al. (2024), with a Cronbach’s alpha of 0.916; responses ranged from 1 (strongly disagree) to 4 (strongly agree), and scores were categorized as low, moderate, or high. Family support was assessed using a 14-item questionnaire also developed by Witungga et al. (2024), with a Cronbach’s alpha of 0.836; each item was scored dichotomously (yes = 2, no = 1), and total scores were classified into poor, sufficient, or good support [8]. Postpartum depression was evaluated using the Edinburgh Postnatal Depression Scale (EPDS), originally developed by Cox, Holden, and Sagovsky (1987) and adapted into Indonesian by Adli (2022); this 10-item scale assesses maternal mood in the past week, with each item scored from 0 to 3 for a total range of 0–30, where higher scores indicate greater depressive severity. The EPDS has consistently demonstrated robust psychometric properties across international studies, with Cronbach’s alpha values ranging from 0.80 to 0.88 and sensitivity above 85% in detecting postpartum depression [9].
Variables
The independent variables in this study were maternal self-efficacy (categorized into low, moderate, and high) and family support (categorized into poor, fair, and good). The dependent variable was postpartum depression, measured by the Edinburgh Postnatal Depression Scale (EPDS) and categorized into three levels: no signs of depression, depression may be present, and clear signs of depression. Sociodemographic characteristics were included as control variables, consisting of age, last educational attainment, marital status, occupation, family income, place of residence, number of children (including the child from the cryptic pregnancy), gestational age at the time the pregnancy was discovered, previous pregnancy history, access to healthcare, mode of delivery, presence of a birth companion, complications during pregnancy or delivery, and history of mental health problems. Household income was recorded in Indonesian Rupiah (IDR) and converted to United States Dollars (USD) using the 2025 average exchange rate (1 USD ≈ 15,500 IDR) to enhance international readability.
Statistical Analysis
All data were analyzed using SPSS software version 26 for Windows. Descriptive statistics were employed to summarize the sociodemographic characteristics of the participants. The Kolmogorov–Smirnov test was used to assess data normality and indicated that the data were not normally distributed (p < 0.05). Spearman’s rank correlation test was used to evaluate the relationships between maternal self-efficacy, family support, and postpartum depression. To further identify the strength and direction of predictors on postpartum depression levels, ordinal logistic regression analysis was conducted. This method is appropriate given the ordinal nature of the dependent variable and non-normal data distribution. Statistical significance was defined as a p-value less than 0.05.
RESULTS
Sample Characteristics
The mean age of respondents was 28.45 years (SD = 6.14), with the largest proportion aged 25–29 years (32.7%). More than half had completed secondary education (55.8%), were married (89.4%), and worked as housewives (68.3%). More than half of the participants reported a monthly family income between 152 and less than 304 USD (55.8%), with a mean income of 139.78 USD (SD = 88.55) and a median of 187.46 USD (IQR = 44.87–210.26), and the majority resided in urban areas (60.6%). Nearly half had two children, including the child from the cryptic pregnancy (44.2%), and most discovered their pregnancy in the third trimester (≥ 28 weeks) (61.5%); a considerable proportion reported previous pregnancies, including unplanned pregnancy or miscarriage (44.2%). Access to healthcare was most frequently moderate, requiring 30–60 minutes with limited transportation (50%). The most common mode of delivery was spontaneous vaginal delivery at a healthcare facility (48.1%), with most accompanied by a husband or family member during childbirth (67.3%). The majority experienced no pregnancy or delivery complications (72.1%) and none reported a history of mental health disorders (100%). Self-efficacy assessments indicated that self-efficacy was predominantly moderate (72.1%), while family support was most often fair (65.4%). Regarding postpartum depression, most mothers exhibited no signs of depression (68.3%), while nearly one-third showed possible symptoms (31.7%). Table 1 shows the demographic data of respondents.
Characteristic Category n (%) M (SD) Median (IQR) Sociodemographic of Respondent
Age < 20 9 (8.7%) 28.45 (6.137) 28 (24 – 33) 20–24 20 (19.2%) 25–29 34 (32.7%) 30–34 21 (20.2%) ≥ 35 20 (19.2%) Last educational attainment Basic education (Elementary School or equivalent) 46 (44.2%) Secondary education (Junior/Senior High School or equivalent) 58 (55.8%) Higher education (Diploma, Bachelor’s, or Postgraduate) 0 (0%) Marital Status Married 93 (89.4%) Unmarried 3 (2.9%) Divorced/Widowed 8 (7.7%) Occupation Housewife 71 (68.3%) Employed 22 (21.2%) Unemployed 4 (3.8%) Others 7 (6.7%) Family income < USD 60,79 45 (43.3%) USD 139.78 (88.55) USD 187.46 (44.87 – 210.26) USD 152 ≤ 304 58 (55.8%) ≥ USD 303,93 1 (1.0 %) Place of residence Urban 63 (60.6%) Rural 41 (39.4 %) Number of children (including children during cryptic pregnancy) 1 child 42 (40.4 %) 2 children 46 (44.2%) ≥ 3 children 16 (15.4%) Gestational age at the time the pregnancy was discovered < 12 weeks (1st trimester) 19 (18.3%) 12–27 weeks (2nd trimester) 21(20.2%) ≥ 28 weeks (3rd trimester) 64 (61.5%) Previous Pregnancy History No previous pregnancy 27 (26.0%) Yes, all planned pregnancies 31 (29.8%) Yes, including unplanned pregnancy/miscarriage 46 (44.2%) Access to healthcare Easy (≤ 30 minutes, transportation available) 32 (30.8%) Moderate (30–60 minutes, limited transportation) 52 (50%) Difficult (> 60 minutes, poor transportation access) 20 (19.2%) Mode of delivery Spontaneous/vaginal at a healthcare facility 50 (48.1%) Spontaneous/vaginal at home 20 (19.2%) Cesarean section (C-section) at a healthcare facility 24 (23.1%) Others (e.g., without medical assistance) 10 (9.6%) Presence of a birth companion Husband/Family 70 (67.3%) Healthcare provider 32 (30.8%) Alone/No attendant 2 (1.9%) Complications during Pregnancy or delivery None 75 (72.1%) Present 29 (27.9%) Mental health history None 104 (100%) Self - Efficacy Low 0 (0%) 32.45 (5.812) 32 (28 – 37) Moderate 75 (72.1%) High 29 (27.9%) Family Support Poor 0 (0%) 28.63 (4.925) 29 (25–32) Fair 68 (65.4%) Good 36 (34.6%) Postpartum Depression No signs of depression 71 (68.3%) 10.82 (3.214) 11 (9 – 13) Depression may be present 33 (31.7%) Clear signs of depression 0 (0%) Abbreviations: n = number; % = percentage; M = mean; SD = standard deviation; IQR = interquartile range; USD = United States Dollar. All variables had complete data (n = 104).
Table 1. Sociodemographic, Self – Efficacy, Family Support and Postpartum Depression.
Relationship Between Self-Efficacy and Postpartum Depression
The Spearman correlation test results indicate a negative and significant relationship between self-efficacy and postpartum depression, with a correlation coefficient of ρ = –0.426 and a significance value of p value = 0.001 (Table 2). This finding suggests that higher levels of self-efficacy are associated with lower levels of postpartum depression. The strength of the relationship is moderate and remains statistically significant.
Variable M (SD) Median (IQR) Sig. (2-tailed) Spearman Correlation Self-efficacy 32.45 (5.812) 32 (28 – 37) Correlation coefficient ρ = –0.426, p value = 0.001**
Postpartum depression 10.82 (3.214) 11 (9 – 13) *p < 0.05, **p < 0.01, SD = standard deviation, IRQ = interquartile range [Q1, Q3]; M = mean.
Table 2. Relationship Between Self-Efficacy and Postpartum Depression (N = 104).
Figure 1 presents a scatter plot showing a moderate negative correlation (ρ = –0.426, p value = 0.001) between self-efficacy and postpartum depression. This correlation suggests that higher levels of maternal self-efficacy are associated with lower levels of postpartum depression. The results also indicate that the relationship between these two variables is moderate and statistically significant.
Figure 1. Scatter Plot of Postpartum Depression Levels by Self-Efficacy Levels. The trend line is in red.
The crosstabulation analysis further shows the distribution of respondents based on self-efficacy levels and postpartum depression symptoms (Table 3).
Self-Efficacy Postpartum Depression Total No signs of depression Depression may be present Moderate 55 20 75 High 16 13 29 Total 71 33 104 Table 3. Crosstabulation of Self-Efficacy and Postpartum Depression.
Among those with moderate self-efficacy, 55 mothers reported no signs of depression, while 20 mothers showed possible signs of depression, totaling 75 individuals. In contrast, among those with high self-efficacy, 16 mothers reported no signs of depression and 13 mothers experienced possible depression, totaling 29 individuals.\
Relationship Between Family Support and Postpartum Depression
Correlation analysis using Spearman's correlation coefficient indicates a negative and significant relationship between family support and postpartum depression, with a correlation coefficient of ρ = –0.398 and a significance value of p value = 0.002 (Table 4). This suggests that higher levels of family support are associated with lower levels of postpartum depression, and the strength of this relationship is moderate and statistically significant.
Variable M (SD) Median (IQR) Sig. (2-tailed) Spearman Correlation Family support 28.63 (4.925) 29 (25–32) Correlation coefficient ρ = –0.398, p value = 0.002**
Postpartum depression 10.82 (3.214) 11 (9–13) *p < 0.05, **p < 0.01, SD = standard deviation, IRQ = interquartile range [Q1, Q3]; M = mean.
Table 4. Relationship Between Family Support and Postpartum Depression (N = 104)
Figure 2 presents a scatter plot to visualize the joint values for the family support and postpartum depression variables, and to observe possible relationships, trends, between the variables. We observed from Figure 2 a moderate negative correlation (ρ = –0.398, p value = 0.002) between family support and postpartum depression. This correlation suggests that higher levels of family support are associated with lower levels of postpartum depression. The results also indicate that the relationship between these two variables is moderate and remains statistically significant.
Figure 2. Scatter Plot of Postpartum Depression Levels by Family Support Levels. The trend line is in red.
The crosstabulation analysis further shows the distribution of respondents based on family support and postpartum depression symptoms (Table 5).
Family Support Postpartum Depression Total No signs of depression Depression may be present Fair 44 24 68 Good 27 9 36 Total 71 33 104 Table 5. Crosstabulation of Family Support and Postpartum Depression
Among mothers with fair family support, 44 reported no signs of depression while 24 experienced possible signs of depression, totaling 68 individuals. Conversely, among those with good family support, 27 mothers reported no depression and 9 mothers experienced possible depression, totaling 36 individuals.
The Combined Effect of Maternal Self-Efficacy and Family Support on Postpartum Depression
The results of the multivariate ordinal logistic regression analysis showed that both maternal self-efficacy and family support have significant effects on postpartum depression. The overall model shows a Nagelkerke R² value of 0.289, indicating that the combination of maternal self-efficacy and family support explains 28.9% of the variability in postpartum depression levels.
In Table 6, we reported the results of the multivariate ordinal logistic regression analysis of maternal self-efficacy and family support on postpartum depression.
Predictor B SE Wald OR (Exp(B)) 95% CI for OR p value Maternal self-efficacy -0.462 0.188 6.030 0.63 0.44 – 0.91 0.014 * Family support -0.518 0.205 6.367 0.60 0.40 – 0.89 0.012 * -2 Log Likelihood 178.21 Nagelkerke R² 0.289 *Significant at p < 0.05
Table 6. Multivariate Ordinal Logistic Regression of Maternal Self-Efficacy and Family Support on Postpartum Depression (n = 104).
The parameter estimates indicate that maternal self-efficacy has a significant negative association with postpartum depression (B = –0.462, Wald = 6.018, p value = 0.014, OR = 0.63, 95% CI = 0.44–0.91). This means that mothers with higher self-efficacy are less likely to experience postpartum depression. Similarly, family support also shows a significant negative association with postpartum depression (B = –0.518, Wald = 6.367, p value = 0.012, OR = 0.60, 95% CI = 0.40–0.89), indicating that greater family support reduces the risk of postpartum depression. These findings suggest that maternal self-efficacy and family support are both protective factors against postpartum depression, and their combined contribution highlights the importance of strengthening personal and social resources for mothers during the postpartum period.
DISCUSSION
This study demonstrates that maternal self-efficacy has a significant negative relationship with postpartum depression among mothers with a history of cryptic pregnancy. This aligns with the first objective of the study, which was to examine the association between self-efficacy and depressive symptoms. The finding supports Bandura’s theory of self-efficacy, which emphasizes the individual’s belief in their ability to organize and carry out tasks as a key factor in managing stress and emotional well-being [9]. Mothers with higher self-efficacy are able to adapt more effectively to the demands of motherhood, thereby lowering their vulnerability to depression. In the context of cryptic pregnancy, where mothers experience limited prenatal preparation, reduced medical supervision, and a sudden transition to motherhood, self-efficacy becomes an essential psychological resource [10]. Similar results have been reported in other countries. For instance, Chase et al. (2021) found that low maternal self-efficacy was strongly associated with higher levels of postpartum depression, suggesting that interventions aimed at improving confidence can be applied across different cultural settings [11].
The second objective of the study was to examine the role of family support in maternal mental health. Family support also showed a significant negative association with postpartum depression, reinforcing the importance of social and cultural contexts. Support from close relatives, especially spouses, provides emotional reassurance, practical help, and a sense of security, all of which buffer against the stress of childbirth and early parenting [12]. This result echoes findings from Delong et al. (2022), who demonstrated that social support plays a protective role in maternal well-being and strengthens maternal–infant interactions [13]. In Indonesia, where collectivist culture and family involvement in childcare are deeply rooted, family support becomes even more crucial. Mothers who experience cryptic pregnancy may feel shocked, unprepared, or even stigmatized due to the late discovery of their condition. In such situations, family members, particularly nurses within the community or family health settings, play a vital role in reducing stigma and supporting maternal adjustment [14].
The third objective of the study was to explore the combined effects of maternal self-efficacy and family support. The multivariate regression analysis confirmed that these two factors jointly predict postpartum depression, explaining nearly one-third of the variance. This suggests that personal psychological resources and external social support interact to shape maternal mental health outcomes. Comparable results have been found in other regions, where interventions that simultaneously enhance coping skills and involve family members proved more effective in reducing postpartum depression than those focusing on a single factor [15]. From a nursing perspective, this highlights the need for nurses to not only build mothers’ confidence through education and counseling but also to engage families in the care process [16]. The clinical implication is that nursing practice in both community and hospital settings should adopt a family-centered approach to maternal mental health. Furthermore, for future research, cross-cultural studies could provide valuable insights into how these factors operate in different healthcare systems and societies, and how nurses can tailor interventions to local needs.
Limitations
This study has several limitations. First, the use of a snowball sampling technique limits the representativeness of the sample and increases the risk of selection bias, as respondents were recruited through networks and may not reflect the broader population of mothers with cryptic pregnancy. Second, the reliance on self-reported questionnaires raises the possibility of recall bias and social desirability bias, where participants may underreport depressive symptoms or overstate family support. Third, this study did not control for other important psychosocial or environmental variables, such as marital conflict, domestic violence, or financial instability, which may independently contribute to postpartum depression. Fourth, the research was conducted in a single geographic area (Jombang Regency, East Java), and thus the findings may be influenced by local cultural norms and may not be generalizable to other populations with different sociocultural backgrounds. Finally, the cross-sectional design of this study prevents causal inferences, as it only identifies associations rather than longitudinal patterns. Future studies should adopt prospective or longitudinal designs with random sampling to establish causal pathways and improve external validity.
CONCLUSION
According to this study, maternal self-efficacy and family support are significant protective factors against postpartum depression among mothers with a history of cryptic pregnancy. Mothers with higher self-efficacy and stronger family support are less likely to experience depressive symptoms after childbirth. These findings reinforce previous evidence that both personal psychological resources and social environments are central in determining maternal mental health outcomes. The study highlights the urgent need for interventions that not only enhance maternal self-efficacy through counseling, psychoeducation, and peer support but also strengthen family involvement in postpartum care. Given that cryptic pregnancy presents unique psychological challenges due to the sudden recognition of pregnancy, integrated strategies focusing on both individual empowerment and family support systems may serve as effective preventive measures for postpartum depression.
Author Contributions
Study conceptualization and design (I.N., D.P., D.E.), data collection and analysis (I.N., D.E.), interpretation and manuscript drafting (I.N., D.P., D.E.), critical manuscript revision (D.E., D.P.). All authors have read and approval the final version of the manuscript.
Local Ethics Committee approval
This study was approved by the Research Ethics Committee of the Institute of Science and Health Technology Insan Cendekia Medika Jombang (reference number LP3M/ICME/ETIK/0425/2025 on February 10, 2025.
Conflict of Interest
The authors declare no conflicts of interest.
Funding Sources
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Acknowledgements
We extend our deepest gratitude to the mothers who shared their experiences of cryptic pregnancy and postpartum adjustment, as well as their families who supported this study by participating in interviews and completing the questionnaires. Without their openness, trust, and participation, this research would not have been possible.
REFERENCES
- Roddy Mitchell A, Gordon H, Lindquist A, Walker SP, Homer CSE, Middleton A, et al. Prevalence of Perinatal Depression in Low- and Middle-Income Countries: A Systematic Review and Meta-analysis. JAMA Psychiatry 2023;80:425–31. https://doi.org/10.1001/jamapsychiatry.2023.0069.
- Shorey S, Chee CYI, Ng ED, Chan YH, Tam WWS, Chong YS. Prevalence and incidence of postpartum depression among healthy mothers: A systematic review and meta-analysis. J Psychiatr Res 2018;104:235–48. https://doi.org/10.1016/j.jpsychires.2018.08.001.
- Bestari, A. D., Westriningrum, L., Didah, D., Gumilang, L., & Mandiri,
(2025). Faktor-Faktor yang Berhubungan dengan Resiko Depresi
Postpartum pada Ibu Nifas di Kota Bandung. Malahayati Nursing Journal,
7(2), 658-674. https://doi.org/10.33024/mnj.v7i2.17747- Cho H, Lee K, Choi E, Cho HN, Park B, Suh M, et al. Association between social support and postpartum depression. Sci Rep 2022;12. https://doi.org/10.1038/S41598-022-07248-7,.
- Han L, Zhang J, Yang J, Yang X, Bai H. Between Personality Traits and Postpartum Depression: The Mediated Role of Maternal Self-Efficacy. Neuropsychiatr Dis Treat 2022;18:597. https://doi.org/10.2147/NDT.S346327.
- Zarroug M, Altaf MF, Shaikh S, Tidjani A, Bashir O, Ayash MI, et al. The Prevalence and Risk Factors of Postpartum Depression Among Saudi Arabian Women—A Systematic Review and Meta-Analysis. Healthc 2025;13:2040. https://doi.org/10.3390/HEALTHCARE13162040/S1.
- Duckitt K. Cryptic pregnancy. Case Reports Women’s Heal 2023;38:e00503. https://doi.org/10.1016/J.CRWH.2023.E00503.
- Witungga RAA, Purwatiningrum DA, Gumanti KA, Sariati Y. The Relationship Of Maternal Self-Efficacy And Family Social Support To The Achivement Of Maternal Identity In Postpartum Women With A History Of Early Marriage. JKM (Jurnal Kebidanan Malahayati) 2024;10:1349–58. https://doi.org/10.33024/jkm.v10i12.17682.
- Adli FK. Edinburgh Post-natal Depression Scale (EPDS): Deteksi Dini dan Skrining Depresi Post-partum. J Kesehat 2022;13:430–6. https://doi.org/10.26630/JK.V13I2.2741.
- Shuriah NN, McFarland E, Spenn B, Butz McManus K, McManus B. Denial of Pregnancy or Cryptic Pregnancy. BIO4960 Pract Biol I 2024.
- Chase T, Shah A, Maines J, Fusick A. Psychotic pregnancy denial: a review of the literature and its clinical considerations. J Psychosom Obstet Gynecol 2021;42:253–7. https://doi.org/10.1080/0167482X.2020.1789584,.
- Chechko N, Losse E, Stickel S. A case report involving the experience of pervasive pregnancy denial: detailed observation of the first 12 postpartum weeks. BMC Psychiatry 2022;22. https://doi.org/10.1186/s12888-022-04377-1.
- Delong H, Eutrope J, Thierry A, Sutter-Dallay AL, Vulliez L, Gubler V, et al. Pregnancy denial: a complex symptom with life context as a trigger? A prospective case–control study*. BJOG An Int J Obstet Gynaecol 2022;129:485–92. https://doi.org/10.1111/1471-0528.16853,.
- Dlamini LP, Hsu YY, Shongwe MC, Wang ST, Gau ML. Maternal Self-Efficacy as a Mediator in the Relationship Between Postpartum Depression and Maternal Role Competence: A Cross-Sectional Survey. J Midwifery Women’s Heal 2023;68:499–506. https://doi.org/10.1111/JMWH.13478;JOURNAL:JOURNAL:18791565B;WGROUP:STRING:PUBLICATION.
- Mercan Y, Selcuk KT. Association between postpartum depression level, social support level and breastfeeding attitude and breastfeeding self-efficacy in early postpartum women. PLoS One 2021;16:e0249538. https://doi.org/10.1371/JOURNAL.PONE.0249538.
- César-Santos B, Bastos F, Dias A, Campos MJ. Family Nursing Care during the Transition to Parenthood: A Scoping Review. Healthcare 2024;12:515. https://doi.org/10.3390/HEALTHCARE12050515.
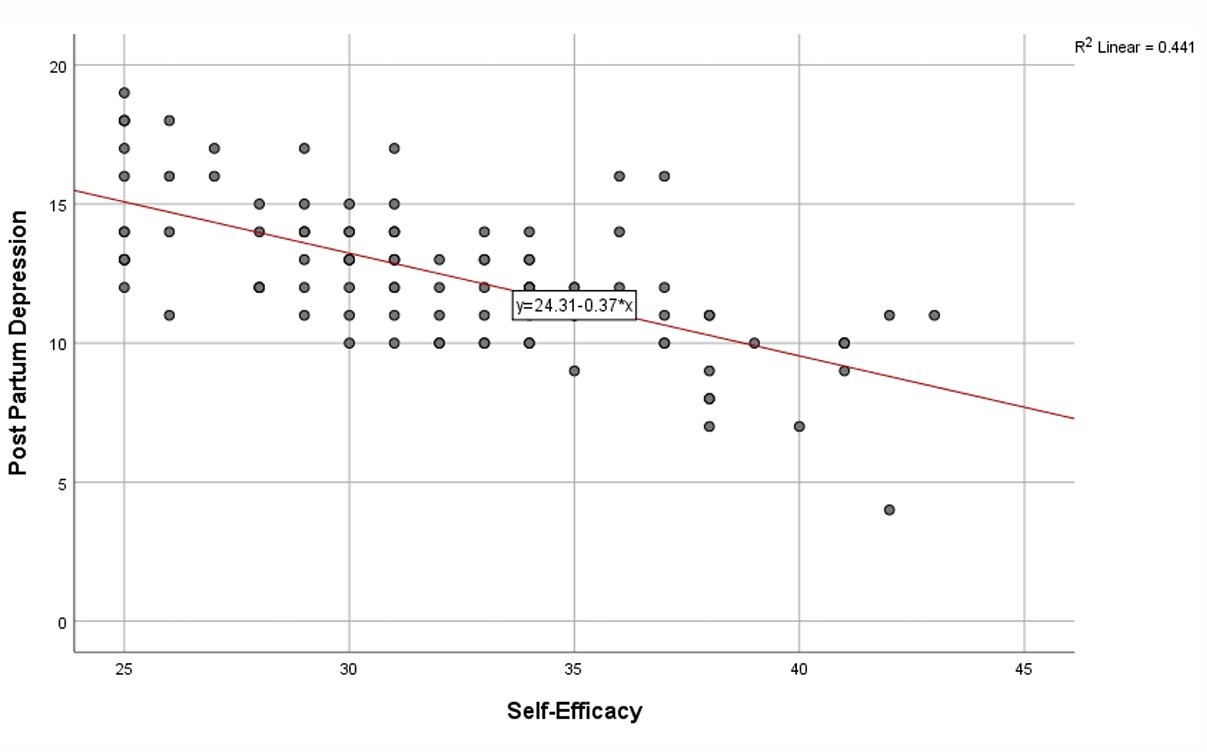
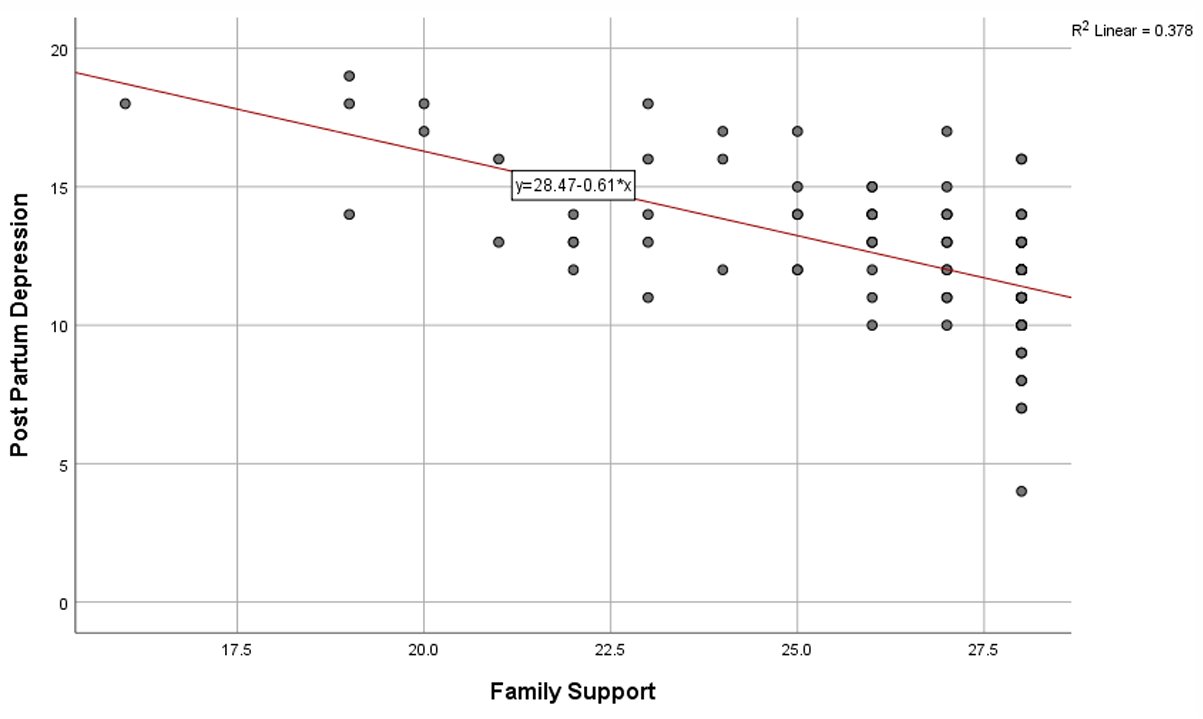
EFFECTIVENESS OF TAPPING AND MASSAGE TECHNIQUE IN PROMOTING VENOUS DILATION FOR PERIPHERAL INTRAVENOUS CATHETER INSERTION: A SYSTEMATIC REVIEW
Rita Citarella 1*, Aniello Lanzuise 2, Vittoria Masullo 3 Marco Abagnale 4
- Department of Surgery and Anesthesia, “Umberto I” Hospital of Nocera Inferiore”, 84014, Salerno, Italy.
- Corporate Health Management, "Ospedale dei Colli",80131, Napoli, Italy.
- University surgical clinic, “San Giovanni di Dio e Ruggi d’Aragona”,84131, Salerno, Italy.
- Department of Critical Care, M. Scarlato Hospital, 84018, Scafati, Salerno, Italy.
* Corresponding author: Rita Citarella, Department of Surgery and Anesthesia at Umberto I Hospital of Nocera Inferiore, 84014 Salerno, Italy. E-mail: rita.citarella.91@gmail.com
Cite this article
ABSTRACT
Introduction: Peripheral intravenous catheter (PIVC) insertion is a common clinical procedure, yet achieving successful venous access, particularly at the first attempt, remains a significant challenge. Techniques such as tapping and massage have been proposed to enhance venous dilation and facilitate cannulation.
Objective: This study aims to evaluate and compare the effectiveness of tapping and massage each compared to tourniquet-only application, in promoting peripheral venous dilation.
Materials and Methods: This study is a systematic review conducted following the PRISMA 2020 guidelines. A systematic search was conducted in PubMed, Scopus, MEDLINE, and CINAHL. All databases were accessed in April 2025 to retrieve studies published between January 2015 and April 2025. Studies were eligible if they involved adult participants, compared tapping and/or massage with standard tourniquet application or control, and reported outcomes related to vein diameter, cross-sectional area, or palpability. Quality assessment was performed using the NIH Quality Assessment Tool and for the risk of bias was used the ROBINS-I.
Results: Tapping was associated with modest improvements in vein diameter and palpability in some studies, but not in others. Massage showed improvements in palpability, yet no clear advantage over tapping was consistently demonstrated. No clear clinical advantage of one technique over the other was consistently demonstrated, and no study assessed outcomes such as first-attempt success rate. Methodological limitations included small sample sizes, and lack of randomization.
Conclusions: Both tapping and massage may promote venous dilation in young, healthy adults, but the evidence is limited. The generalizability of these findings to broader clinical populations, including elderly patients and those with difficult venous access, is uncertain. High-quality studies involving diverse populations and standardized outcome measures are needed to establish the effectiveness of these techniques in routine clinical practice.
Keywords: tapping technique, massage technique, venous dilation, peripheral intravenous catheter, phlebotomy, venipuncture.
INTRODUCTION
Peripheral intravenous catheter (PIVC) placement is a common procedure performed in approximately 80% of hospitalized patients to administer infusion solutions and antibiotics [1]. It is one of the most commonly recommended vascular access methods for short-term infusion therapy (≤7 days) and administration of low-osmolarity or low-irritation drugs [2,3]. It is also approved for emergency situations, regardless of the drugs administered [4]. The demand for PIVC in older adults is increase due to the rapid growth of the aging population [5]. However, several studies have reported higher initial failure rates of PIVC insertion in older adults up to 39% compared to younger adults, where rates range from 12% to 30% [6]. PIVC failure not only leads to complications and delayed treatments but also affects patient’s quality of life and increases healthcare costs [7].
For safe and successful PIVC insertion, it is crucial to select an appropriate vein. Traditionally, vein selection is based on visual inspection, palpation, or imaging techniques such as infrared or ultrasound devices. Larger veins are generally recommended for easier cannulation [8], and achieving adequate venous dilation is essential for the procedure’s success. Current guidelines recommend inserting the PIVC into the forearm cutaneous veins rather than the median cubital vein, due to considerations of daily activities and lower complication risks [9,10]. However, the forearm veins are thinner, branch more peripherally, and are often more difficult to access compared to the median cubital vein [11]. As a result, between 12% and 26% of patients require multiple attempts for successful PIVC insertion following an initial failure [12]. Repeated PIVC punctures increase the risk of complications such as pain, nerve damage, and accidental arterial puncture [13]. Furthermore, these multiple attempts result in additional time and staffing costs associated with the procedure [14]. Difficulty in establishing peripheral intravenous access is a common clinical challenge, particularly in patients with fragile veins, obesity, dehydration, or chronic illnesses [15]. Failed first-attempt cannulation can delay treatment, increase patient discomfort, and raise healthcare costs. Nurses are primarily responsible for PIVC placement in most clinical settings [16]. Therefore, identifying and applying effective, evidence-based techniques to facilitate venous dilation is a key component of nursing practice, with direct implications for patient safety and quality of care [17]. Understanding which technique whether tapping, massaging, or other methods is the most effective in promoting venous dilation is essential for optimizing clinical practice. Evidence-based recommendations are needed to guide nurses in selecting the best approach, ensuring both procedural success and patient comfort [18]. PIVC insertion relies on palpation to identify a vein's Therefore, it is essential to ensure adequate venous dilation and to carefully select an appropriate vein for PIVC insertion through palpation. The most commonly used technique for promoting venous dilation involves applying a tourniquet to induce venous stasis [19]. However, relying solely on a tourniquet may not always provide sufficient dilation. To enhance the effect of the tourniquet, nurses often instruct patients to open and close their fist or maintain a clenched fist. Additionally, they may massage the forearm, tap over the vein [20], or apply warmth to the forearm [21].
Among these methods, tapping and massaging are proactive techniques in which the nurse provides direct stimulation to the vein. These techniques do not require the patient's active participation or the use of additional equipment, and they can be implemented quickly and easily in various clinical situations [22]. Tapping is recommended when the target vein is not prominent and/or needs to be made more prominent for venipuncture [23] and is an effective method of vasodilation [24]. The following factors are reported to be involved in vasodilation mechanisms by tapping: the production of nitric oxide (NO) and other vasoactive substances from the endothelium by mechanical stress, such as shear stress, and the axon reflex associated with pain stimulation [25]. Despite the widespread use of techniques such as tapping and massaging in clinical practice, current international guidelines lack specific recommendations regarding their effectiveness in promoting venous dilation [26]. Limited studies have investigated the physiological mechanisms and clinical efficacy of these manual stimulation techniques, highlighting the need for further research to establish evidence-based best practices.
Purpose
This systematic review aims to evaluate and compare the effectiveness of tapping and massage each compared to tourniquet-only application, in promoting peripheral venous dilation.
MATERIALS AND METHODS
We conducted a systematic review following the preferred reporting items for systematic reviews and meta-analyses, the PRISMA statement version 2020 [26]. We used the PICO (Table 1) framework.
|
POPOLATION |
Patients undergoing peripheral intravenous catheter (PIVC) insertion |
|
INTERVENTION |
Tapping or massage as techniques for venous dilation |
|
COMPARISON |
Tourniquet |
|
OUTCOME |
Efficacy of techniques in promoting venous dilation, measured by changes in vein diameter, cross-sectional area and vein palpability. |
Table 1. PICO framework
Eligibility Criteria
We included both observational and experimental studies that: involved patients undergoing peripheral intravenous catheter (PIVC) insertion; compared tapping and/or massage with tourniquet-only or control techniques; reported outcomes related to venous dilation, such as vein diameter, cross-sectional area, or palpability; were published in English in peer-reviewed journals from January 2015 to April 2025. We excluded: studies on pediatric or animal populations; systematic reviews, commentaries, letters, and abstracts; studies involving non-manual techniques (ultrasound-guided cannulation or pharmacologic interventions). We excluded pediatric patients, elderly individuals, and those with chronic conditions because the available literature on this topic primarily involved healthy adult participants. This choice reflects the current scope of published evidence rather than a methodological preference.
Search Strategy
We performed a comprehensive literature search in PubMed, Scopus, MEDLINE (via EBSCOhost), and CINAHL. The literature search covered the period from January to April 2025. All databases were accessed in April 2025. We used relevant MeSH terms and Boolean operators. A full list of search strings is reported in Table 2.
|
DATABASE |
SEARCH STRING |
|
PubMed |
("phlebotomy"[MeSH Terms] OR "phlebotomy"[All Fields] OR "venipuncture"[All Fields] OR "venipunctures"[All Fields] OR ("phlebotomy"[MeSH Terms] OR "phlebotomy"[All Fields] OR "phlebotomies"[All Fields]) OR (("cutaneous"[All Fields] OR "cutaneously"[All Fields] OR "cutanous"[All Fields]) AND ("vein s"[All Fields] OR "veins"[MeSH Terms] OR "veins"[All Fields]))) AND ("mechanical"[All Fields] OR "mechanically"[All Fields] OR "mechanicals"[All Fields] OR "mechanics"[MeSH Terms] OR "mechanics"[All Fields] OR "mechanic"[All Fields] OR ("tapped"[All Fields] OR "tapping"[All Fields] OR "tappings"[All Fields]) OR ("massage"[MeSH Terms] OR "massage"[All Fields] OR "massages"[All Fields] OR "massaged"[All Fields] OR "massager"[All Fields] OR "massagers"[All Fields] OR "massaging"[All Fields]) OR ("palpate"[All Fields] OR "palpated"[All Fields] 24/04/2025 120 9 OR "palpates"[All Fields] OR "palpating"[All Fields] OR "palpation"[MeSH Terms] OR "palpation"[All Fields] OR "palpations"[All Fields] OR "palpator"[All Fields] OR "palpators"[All Fields])) AND ((("veins"[MeSH Terms] OR "veins"[All Fields] OR "vein"[All Fields]) AND ("visibilities"[All Fields] OR "visibility"[All Fields] OR "visible"[All Fields] OR "visibles"[All Fields])) OR ("veins"[MeSH Terms] OR "veins"[All Fields] OR "venous"[All Fields]) OR ("venodilating"[All Fields] OR "venodilation"[All Fields] OR "venodilator"[All Fields] OR "venodilators"[All Fields]) OR ("vasodilate"[All Fields] OR "vasodilated"[All Fields] OR "vasodilates"[All Fields] OR "vasodilating"[All Fields] OR "vasodilation"[MeSH Terms] OR "vasodilation"[All Fields] OR "vasodilations"[All Fields] OR "vasodilative"[All Fields] OR "vasodilator agents"[Pharmacological Action] OR "vasodilator agents"[Supplementary Concept] OR "vasodilator agents"[All Fields] OR "vasodilator"[All Fields] OR "vasodilator agents"[MeSH Terms] OR ("vasodilator"[All Fields] AND "agents"[All Fields]) OR "vasodilators"[All Fields])) |
|
SCOPUS |
( INDEXTERMS ( phlebotomy ) OR ALL ( phlebotomy ) OR ALL ( venipuncture ) OR ALL ( venipunctures ) OR ( INDEXTERMS ( phlebotomy ) OR ALL ( phlebotomy ) OR ALL ( phlebotomies ) ) OR ( ( ALL ( cutaneous ) OR ALL ( cutaneously ) OR ALL ( cutanous ) ) AND ( ALL ( "vein s" ) OR INDEXTERMS ( veins ) OR ALL ( veins ) ) ) ) AND ( ALL ( mechanical ) OR ALL ( mechanically ) OR ALL ( mechanicals ) OR INDEXTERMS ( mechanics ) OR ALL ( mechanics ) OR ALL ( mechanic ) OR ( ALL ( tapped ) OR ALL ( tapping ) OR ALL ( tappings ) ) OR ( INDEXTERMS ( massage ) OR ALL ( massage ) OR ALL ( massages ) OR ALL ( massaged ) OR ALL ( massager ) OR ALL ( massagers ) OR ALL ( massaging ) ) OR ( ALL ( palpate ) OR ALL ( palpated ) OR ALL ( palpates ) OR ALL ( palpating ) OR INDEXTERMS ( palpation ) OR ALL ( palpation ) OR ALL ( palpations ) OR ALL ( palpator ) OR ALL ( palpators ) ) ) AND ( ( ( INDEXTERMS ( veins ) OR ALL ( veins ) OR ALL ( vein ) ) AND ( ALL ( visibilities ) 24/04/2025 282 52 OR ALL ( visibility ) OR ALL ( visible ) OR ALL ( visibles ) ) ) OR ( INDEXTERMS ( veins ) OR ALL ( veins ) OR ALL ( venous ) ) OR ( ALL ( venodilating ) OR ALL ( venodilation ) OR ALL ( venodilator ) OR ALL ( venodilators ) ) OR ( ALL ( vasodilate ) OR ALL ( vasodilated ) OR ALL ( vasodilates ) OR ALL ( vasodilating ) OR INDEXTERMS ( vasodilation ) OR ALL ( vasodilation ) OR ALL ( vasodilations ) OR ALL ( vasodilative ) OR ALL ( "vasodilator agents" ) OR CHEM ( term ) OR ALL ( "vasodilator agents" ) OR ALL ( vasodilator ) OR INDEXTERMS ( "vasodilator agents" ) OR ( ALL ( vasodilator ) AND ALL ( agents ) ) OR ALL ( vasodilators ) ) ) AND ( LIMIT-TO ( SUBJAREA , "NURS" ) ) |
|
MEDLINE |
((MH phlebotomy+) OR phlebotomy OR venipuncture OR venipunctures OR ((MH phlebotomy+) OR phlebotomy OR phlebotomies) OR ((cutaneous OR cutaneously OR cutanous) AND ("vein s" OR (MH veins+) OR veins))) AND (mechanical OR mechanically OR mechanicals OR (MH mechanics+) OR mechanics OR mechanic OR (tapped 24/04/2025 143 OR tapping OR tappings) OR ((MH massage+) OR massage OR massages OR massaged OR massager OR massagers OR massaging) OR (palpate OR palpated OR palpates OR palpating OR (MH palpation+) OR palpation OR palpations OR palpator OR palpators)) AND ((((MH veins+) OR veins OR vein) AND (visibilities OR visibility OR visible OR visibles)) OR ((MH veins+) OR veins OR venous) OR (venodilating OR venodilation OR venodilator OR venodilators) OR (vasodilate OR vasodilated OR vasodilates OR vasodilating OR (MH vasodilation+) OR vasodilation OR vasodilations OR vasodilative OR "vasodilator agents" OR (MW "vasodilator agents") OR "vasodilator agents" OR vasodilator OR (MH "vasodilator agents+") OR (vasodilator AND agents) OR vasodilators)) |
|
CINAHL |
((MH phlebotomy+) OR phlebotomy OR venipuncture OR venipunctures OR ((MH phlebotomy+) OR phlebotomy OR phlebotomies) OR ((cutaneous OR cutaneously OR cutanous) AND ("vein s" OR (MH veins+) OR 24/04/2025 40 veins))) AND (mechanical OR mechanically OR mechanicals OR (MH mechanics+) OR mechanics OR mechanic OR (tapped OR tapping OR tappings) OR ((MH massage+) OR massage OR massages OR massaged OR massager OR massagers OR massaging) OR (palpate OR palpated OR palpates OR palpating OR (MH palpation+) OR palpation OR palpations OR palpator OR palpators)) AND ((((MH veins+) OR veins OR vein) AND (visibilities OR visibility OR visible OR visibles)) OR ((MH veins+) OR veins OR venous) OR (venodilating OR venodilation OR venodilator OR venodilators) OR (vasodilate OR vasodilated OR vasodilates OR vasodilating OR (MH vasodilation+) OR vasodilation OR vasodilations OR vasodilative OR "vasodilator agents" OR (MW "vasodilator agents") OR "vasodilator agents" OR vasodilator OR (MH "vasodilator agents+") OR (vasodilator AND agents) OR vasodilators)) |
Table 2. Search String
Study Selection
After removing duplicates, two authors (RC and MA) independently screened titles and abstracts. Full texts were retrieved when eligibility was unclear. Discrepancies were resolved through discussion. The selection process followed PRISMA 2020 recommendations and was supported by Rayyan software [27], while to organize and manage the references we used Zootero.
Data Extraction
Two authors independently extracted data using a predefined form. Extracted information included author, year, country, study design, sample size, participant characteristics, intervention, and main outcomes. Final verification was conducted by RC and MA.
Quality Assessment and Risk of Bias
Methodologically, two authors (RC, MA) independently assessed the quality of the included articles using tools from the National Institutes of Health (NIH) [28] for observational and controlled intervention studies. The first author (RC) was the final decider of the overall quality assessment. The quality assessment criteria included the following items:
Q1. Clear statement of objectives
Q2. Adequacy of sample size
Q3. Clear description of participant characteristics
Q4. Description of intervention techniques (tapping, massage, or control)
Q5. Description of outcome measures (venous diameter, cross-sectional area, palpability)
Q6. Appropriateness of data analysis methods
Q7. Use of validated outcome measures
Q8. Blinding of outcome assessors
Q9. Randomization process described
Q10. Allocation concealment
Q11. Reporting of dropout, or missing data
Q12. Reporting of study limitations
Q13. Ethical approval and consent
The summary of the study quality assessment is shown in Table 3.
|
Authors |
Q1 |
Q2 |
Q3 |
Q4 |
Q5 |
Q6 |
Q7 |
Q8 |
Q9 |
Q10 |
Q11 |
Q12 |
Q13 |
|
Ichimura et al., 2015 [30] |
Y |
N |
Y |
Y |
Y |
Y |
Y |
N |
N |
N |
Y |
Y |
Y |
|
Yasuda et al., 2019 [31] |
Y |
N |
Y |
Y |
Y |
Y |
Y |
N |
N |
N |
Y |
Y |
Y |
|
Yasuda et al., 2020 [32] |
Y |
N |
Y |
Y |
Y |
Y |
Y |
N |
N |
N |
Y |
Y |
Y |
|
Yasuda et al., 2023 [33] |
Y |
N |
Y |
Y |
Y |
Y |
Y |
N |
N |
N |
Y |
Y |
Y |
Legend: Y: YES (the study met the criterion); N: NO (the study did not meet the criterion).
Table 3. Quality assessment table Summary of studies quality assessment based on NIH
From the table, we can deduce that all studies responded positively (Y) to most of the criteria related to the description of interventions, outcomes, statistical analyses, participants, and ethical approval (Q1, Q3–Q7, Q11–Q13). However, common limitations were identified in the criteria related to randomization procedures (Q2, Q9), blinding of outcome assessors (Q8), and allocation concealment (Q10), where all studies showed an “N”. This indicates that, while the studies provided a clear description of interventions and outcomes, they lacked critical information about how participants were allocated to groups (randomization), how blinding was implemented, and how selection bias was avoided (allocation concealment). Furthermore, all included studies were conducted exclusively on young and healthy adult populations (ages 20–29 years), limiting the generalizability of findings to broader clinical contexts.
The risk of bias in the included studies was assessed using the ROBINS-I (Risk Of Bias In Non-randomized Studies - of Interventions) tool [29]. This tool evaluates the risk of bias across seven domains using three judgements (serious, moderate and low): confounding (D1), selection of participants (D2), classification of interventions (D3), deviations from intended interventions(D4), missing data (D5), measurement of outcomes (D6), and selection of reported results. This system allowed a clear visualization of potential sources of bias across the studies.
The final judgment was based on a consensus between two independent authors, with the first two authors (RC, MA) acting as the final decision-maker in case of disagreements. Given the quasi-experimental nature of the included studies, ROBINS-I [29] was considered the most appropriate method for evaluating bias in this systematic review. (Figure 1)

Figure 1. Risk of bias assessment in the selected articles according to ROBINS-I tool.
In summary, all four studies showed moderate to serious concerns across several domains, particularly due to lack of randomization details, blinding, potential confounding factors, and small sample sizes. These methodological limitations, combined with the exclusive inclusion of young healthy adult participants, should be taken into account when interpreting the findings.
RESULTS
A total of 585 records were identified through database searches (PubMed: 120; Scopus: 282; MEDLINE: 143; CINAHL: 40). After removing 120 duplicates, 465 records remained for title and abstract screening. Of these, 442 were excluded based on inclusion criteria. Twenty-three full-text articles were assessed, and 4 studies met all eligibility criteria and were included in the final synthesis (see PRISMA flow diagram, Figure 2).
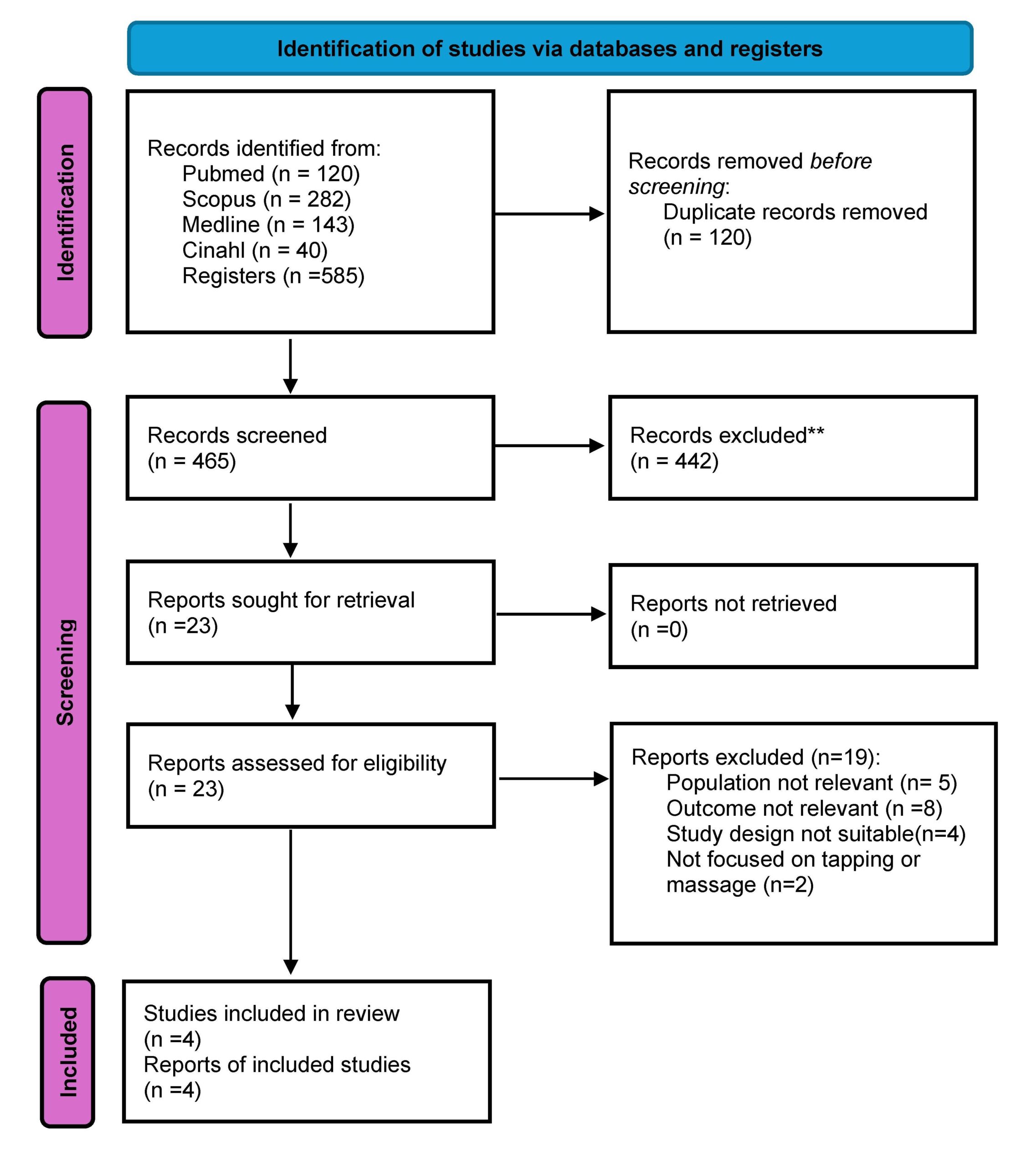
Figure 2. Prisma flowchart for literature search
All included studies were conducted in Japan between 2015 and 2023 and involved a total of 120 healthy adult participants, mostly nursing students with a mean age between 20 and 29 years. The designs were either quasi-experimental or observational. The interventions evaluated included tapping, massage, and tourniquet-only techniques, aimed at enhancing venous dilation prior to PIVC insertion. A total of four studies met the inclusion criteria. This limited number reflects the current scarcity of primary research focused on the use of tapping and massage techniques for peripheral venous access.
The primary outcomes of interest were vein diameter (mm), vein cross-sectional area (mm²), and vein palpability (score). The vein diameter and cross-sectional area were measured using ultrasound in experimental designs, while the vein palpability were assessed through palpation scores in quasi-experimental or observational studies. For quantitative studies that reported statistical comparisons, we collected available data such as means, standard deviations, and, where applicable, p-values, odds ratios (OR), and 95% confidence intervals (CI) (Table 4). No studies reported clinical endpoints such as first-attempt success rate.
|
Study |
Intervention |
Outcome measure |
Tapping (mean ± SD) |
Massage (mean ± SD) |
Control (mean ±SD) |
p-value |
OR |
95% CI |
|
Ichimura et al., 2015 [30] |
Tapping, Control |
Vein diameter (mm) |
2.98± 0.45 |
- |
2.51±0.38 |
<0.01 |
1.75 |
1.15-2.35 |
|
Yasuda et al., 2019 [31] |
Tapping, Massage |
Vein palpability (score) |
4.5±0.6 |
3.8±0.7 |
3.2±0.5 |
<0.01 |
2.1 |
1.40-2.80 |
|
Ichimuda et al., 2020 [32] |
Tapping, Massage |
Cross-sectional area (mm²) |
6.45±1.32 |
5.87±1.20 |
5.32±1.15 |
<0.05 |
1.65 |
1.05-2.25 |
|
Yasuda et al., 2023 [33] |
Tapping, Massage |
Vein diameter (mm) |
3.12 ± 0.54 |
2.85±0.49 |
2.72±0.44 |
<0.01 |
1.85 |
1.20-2.50 |
SD: standard deviation
Table 4. Interventions, outcomes and available data of the selected studies
General Characteristics
The studies were conducted in laboratory settings, maintaining a controlled environment similar to clinical conditions (temperature 22-24 ̊C, humidity 45-65%) consistent with summer hospital standards. Participants were seated with their arms on a shape [30-32] or supine keeping their forearms on the bed during the intervention [33]. The populations studied were exclusively composed of healthy young adults aged approximately 20-29 years, without clinical comorbidities or indications of difficult venous access (DVA). It is important to note that the inclusion of young, healthy volunteers was a limitation dictated by the available literature, as no studies involving older adults, hospitalized patients, or individuals with comorbidities were found in the literature search. Therefore, the generalizability of the findings to broader patient populations remains limited. All studies compared tapping (a light, repetitive mechanical stimulation applied to the skin) and/or massage (manual pressure and friction techniques) with a control group where only a tourniquet was used. The primary outcomes measured were:
- Venous diameter (mm): assessed using ultrasound, representing the width of the vein (n=4; 100%)
- Cross-sectional area (mm²): a two-dimensional measure of the vein’s size, assessed using ultrasound (n=3; 75%)
- Vein palpability (score): a qualitative measure of how easily the vein could be felt during palpation (n=3; 75%)
No studies assessed the first-attempt success rate of peripheral intravenous catheter (PIVC) insertion or reported clinical outcomes related to successful cannulation. (Table 5).
|
Author(s) (year) |
Aim |
Study design |
Participants |
Evaluation methods |
Effect of tapping |
Effect of massage |
|
Ichimira et al., 2015 [30] |
To compare tapping and control groups for vein diameter |
Experimental study |
40 ha (20 yrs) |
Ultrasound |
Increased diameter |
Not assessed |
|
Yasuda et al.,2019 [31] |
To assess vein palpability under different stimulation techniques |
Quasi Experimental study |
30 ha (20-29 yrs) |
Palpation score |
Higher palpability |
Moderate palpability) |
|
Ichimura et al., 2020 [32] |
To evaluate cross-sectional area increase through tap |
Experimental study |
20 ha (19-22 yrs) |
Ultrasound |
Higher increase |
Moderate increase |
|
Yasuda et al., 2023 [33] |
To evaluate the effect of tap and mas on -vein diameter |
Quasi Experimental study |
40 ha (20-29 yrs) |
Ultrasound |
Greater increase in vein diameter |
Moderate increase in vein diameter |
Tap= tapping; Mas= massage; healthy adult= ha; yrs= years. Tapping showed higher numerical values compared to massage, but differences were not consistently statistically significant across all studies.
Table 5. Characteristics of studies included.
DISCUSSION
This systematic review aimed to evaluate the effects of tapping and massage techniques on venous dilation during peripheral intravenous catheter (PIVC) placement, compared to the standard use of a tourniquet alone. The findings suggest that both interventions may help improve vein visibility and diameter, offering a potential advantage in clinical practice, especially in settings where vascular access is challenging. Physiologically, gentle cutaneous stimulation is believed to enhance local blood flow through neurovascular mechanisms, including sympathetic reflexes and activation of mechanoreceptors [24,25]. While the included studies employed different approaches to measurement such as ultrasound imaging [30,32,33] and palpation [31,33], they all reported improvements in vein dilation following tapping or massage, supporting the hypothesis that these techniques promote local vasodilation. Although all included studies reported positive effects of tapping or massage on vein dilation, the magnitude and consistency of these effects varied. Two studies [30,32] measured outcomes using ultrasound, reporting significant increases in vein diameter and cross-sectional area following intervention. One study [31] assessed palpability scores through subjective evaluation, while another [33] used a combination of both methods. These methodological differences likely contributed to the variation in outcomes observed.
Importantly, the effectiveness of tapping and massage techniques may vary based on patient characteristics. All included studies were conducted on healthy young adults aged between 20 to 29 years. This homogeneous population limits the generalizability of findings to broader clinical contexts, such as elderly patients or those with chronic conditions (e.g., diabetes, obesity), who may present different venous characteristics or an increased risk of difficult venous access (DVA). None of the studies stratified results by specific comorbidities or clinical variables, making it difficult to assess the potential differential effects of the interventions in diverse patient populations. The modifiable factors analyzed in the included studies were related to the application of tapping or massage techniques before peripheral intravenous catheter (PIVC) insertion. [Table 4] Tapping showed a greater impact on vein diameter (OR range 1.75 – 2.10), vein cross-sectional area (OR range 1.65 – 1.85), and vein palpability (OR range 1.85 – 2.10) compared to control conditions. However, the differences between tapping and massage were not statistically significant, suggesting that both techniques may have comparable effects. The studies consistently demonstrated that both tapping and massage significantly increase venous dilation compared to control, likely due to the mechanical stimulation triggering the release of nitric oxide and other vasodilators. Massage was also associated with improved vein diameter and palpability, although the effects were generally less pronounced than tapping. No studies reported adverse events associated with either tapping or massage. Regarding non-modifiable factors, none of the studies explicitly analyzed demographic variables such as age or gender in relation to venous dilation outcomes. These findings suggest that both tapping and massage are simple, effective, and low-cost interventions for improving venous dilation prior to PIVC insertion, particularly in patients with difficult venous access. Most existing guidelines continue to focus primarily on tourniquet use and warming techniques, while both tapping and massage remain underutilized in clinical practice. This review highlights the need to consider incorporating tapping and massage into standard protocols, as these techniques have shown comparable efficacy in promoting venous dilation. Although none of the included studies specifically investigated patients with difficult venous access (DIVA), it is reasonable to hypothesize that such techniques could offer clinical benefits in this population, where failed attempts can lead to delays, discomfort, and increased resource utilization. However, further research is required to confirm their effectiveness in more complex clinical scenarios. Comparison with existing literature, also, highlights an underutilization of these techniques in clinical guidelines. Most vascular access protocols continue to emphasize traditional methods such as tourniquet application, fist clenching, or local warming [2,21,26], while manual techniques like tapping and massage are seldom formally recommended despite their frequent use in practice [20,22]. This disconnect may stem from the lack of high-quality studies evaluating these methods. However, tapping has shown a clear physiological rationale through its stimulation of nitric oxide release and vasodilatory reflexes [24,25,32], reinforcing its potential value in pre-cannulation practice. Importantly, none of the reviewed studies reported adverse effects associated with these interventions [30-33]. Despite their promise, the current evidence base is limited by several methodological shortcomings. This review has several limitations. First, all included studies were conducted on small, homogeneous samples of young, healthy adults, and were conducted in Japan which limits the external validity of the findings. None of the studies used randomization or blinding, increasing the risk of selection and performance bias. Sample sizes were generally small, and no power analyses were reported. Additionally, outcome assessment methods varied widely (e.g., ultrasound vs. subjective palpation), which hindered direct comparison across studies. The studies included standardized outcome measures (vein diameter, cross-sectional area, palpability), ensuring comparability of results. However, limitations include the small number of studies (n = 4), limited geographical representation, and the absence of data on pediatric, oncology, or chronic disease populations. These factors limit the ability to draw broad clinical recommendations. Finally, the overall methodological quality of the included studies was moderate, and the risk of bias was found to be moderate to serious, particularly in relation to confounding variables and outcome measurement. Despite these limitations, the results are promising. The consistency of findings suggests a potential benefit that warrants further investigation in patients with greater vascular access difficulty. Tapping and massage are simple, non-invasive, and cost-effective techniques that could be integrated into standard practice to facilitate vascular access, particularly in emergency departments, outpatient clinics, or in cases where veins are difficult to locate. These findings provide a preliminary but meaningful foundation for future clinical trials with more rigorous design, broader populations, and standardized outcome measures. Rather than representing a limitation of our review process, the small number of eligible studies highlights a significant gap in literature.
This review contributes to mapping and critically analyzing the available evidence on this underexplored topic.
Strengths
A key strength of this review is the focused synthesis of experimental [28, 30] o quasi experimental [29,31] evidence on a specific intervention (tapping and massage) for a well-defined outcome (venous dilation prior to PIVC). By focusing on a specific, yet clinically relevant topic, this review addresses a clear gap in the literature and offers practical insights for improving pre-cannulation practices. The methodology followed PRISMA 2020 guidelines, with a robust search strategy across multiple databases and a transparent risk of bias assessment using the ROBINS-I tool [29], ensuring a rigorous and reproducible approach. The inclusion of objective outcome measures such as vein diameter, cross-sectional area, and palpability adds further strength to the review. The review aims to spark interest in future research and contribute to the development of evidence-based guidelines for vascular access optimization. Furthermore, this review highlights the need for a paradigm shift in vascular access practices. While guidelines traditionally emphasize tourniquet application and warming techniques, simple, hands-on interventions like tapping and massage remain largely overlooked in clinical protocols. By shedding light on these low-cost, non-invasive strategies, this review advocates for their potential role in standard vascular access preparation, especially in resource-limited settings where advanced technologies may not be readily available.
CONCLUSIONS
This review suggests that tapping and massage techniques, when used in conjunction with a tourniquet, may improve peripheral vein dilation and palpability in healthy adults. Although the evidence is preliminary and limited by the methodological quality of the studies, the results point to simple, low-cost strategies that could support more effective intravenous access—particularly in clinical situations where veins are difficult to locate. From a practical perspective, these interventions may offer nurses a non-invasive tool to enhance vascular access success, potentially reducing patient discomfort and the need for repeated attempts. Future research should aim to confirm these effects through randomized controlled trials involving larger and more diverse populations. Standardized outcome measures and long-term follow-up will be essential to validate the efficacy and safety of these techniques in real-world clinical settings. Further high-quality primary research is urgently needed to strengthen the evidence base and support future systematic reviews with greater methodological robustness.
Registration
This work has been archived in Prospero with ID CRD420251066139.
Funding statement
This research did not receive any specific grant from funding agencies in public, commercial or not for profit sectors.
Conflict of interest
The authors report no conflict of interest.
Authors’ contributions
RC and MA were the major contributors in writing the manuscript. VM, and AL performed the data collection and interpreted the patient data. All authors read and approved the final manuscript.
REFERENCES
- Alexandrou E, Ray-Barruel G, Carr PJ, Frost SA, Inwood S, Higgins N, Lin F, Alberto L, Mermel ùL, Rickard CM; OMG Study Group. Use of Short Peripheral Intravenous Catheters: Characteristics, Management, and Outcomes Worldwide. J Hosp Med. 2018 May 30;13(5). doi: 10.12788/jhm.3039. PMID: 29813140.
- Zingg W, Barton A, Bitmead J, Eggimann P, Pujol M, Simon A, Tatzel J. Best practice in the use of peripheral venous catheters: A scoping review and expert consensus. Infect Prev Pract. 2023 Feb 3;5(2):100271. doi: 10.1016/j.infpip.2023.100271. PMID: 36910422; PMCID: PMC9995289.
- Moureau NL, Alexandrou E. Vessel Health and Preservation: The Right Approach for Vascular Access. Springer International Publishing. doi:10.1007/978-3-030-03149-7_3
- Pittiruti M, Van Boxtel T, Scoppettuolo G, Carr P, Konstantinou E, Ortiz Miluy G, Lamperti M, Goossens GA, Simcock L, Dupont C, Inwood S, Bertoglio S, Nicholson J, Pinelli F, Pepe G. European recommendations on the proper indication and use of peripheral venous access devices (the ERPIUP consensus): A WoCoVA project. J Vasc Access. 2023 Jan;24(1):165-182. doi: 10.1177/11297298211023274. Epub 2021 Jun 4. PMID: 34088239.
- Carr PJ, Rippey JCR, Cooke ML, Trevenen ML, Higgins NS, Foale AS, Rickard CM. Factors associated with peripheral intravenous cannulation first-time insertion success in the emergency department. A multicentre prospective cohort analysis of patient, clinician and product characteristics. BMJ Open. 2019 Apr 2;9(4):e022278. doi: 10.1136/bmjopen-2018-022278. PMID: 30944127; PMCID: PMC6500093.
- Keogh S, Shelverton C, Flynn J, Mihala G, Mathew S, Davies KM, Marsh N, Rickard CM. Implementation and evaluation of short peripheral intravenous catheter flushing guidelines: a stepped wedge cluster randomised trial. BMC Med. 2020 Sep 30;18(1):252. doi: 10.1186/s12916-020-01728-1. PMID: 32993628; PMCID: PMC7526260.
- Gala S, Alsbrooks K, Bahl A, Wimmer M. The economic burden of difficult intravenous access in the emergency department from a United States' provider perspective. J Res Nurs. 2024 Feb;29(1):6-18. doi: 10.1177/17449871231213025. Epub 2024 Jan 16. PMID: 38495321; PMCID: PMC10939017.
- Blanco P. Ultrasound-guided peripheral venous cannulation in critically ill patients: a practical guideline. Ultrasound J. 2019 Oct 17;11(1):27. doi: 10.1186/s13089-019-0144-5. PMID: 31624927; PMCID: PMC6797689.
- Hadaway L.C., Millam D.A. On the road to successful I.V. starts. Nursing. 2005;35:1–14. doi: 10.1097/00152193-200505001-00001. PMID: 15855836.
- Ingram P, Lavery I. Peripheral intravenous cannulation: safe insertion and removal technique. Nurs Stand. 2007; 22(1):44-47. PMID: 17941430. doi: 10.7748/ns2007.09.22.1.44.c4613
- Gagne P, Sharma K. Relationship of Common Vascular Anatomy to Cannulated Catheters. Int J Vasc Med. 2017;2017:5157914. doi: 10.1155/2017/5157914. PMID: 29410917; PMCID: PMC5749287.
- Lapostolle F, Catineau J, Garrigue B, Monmarteau V, Houssaye T, Vecci I, Tréoux V, Hospital B, Crocheton N, Adnet F. Prospective evaluation of peripheral venous access difficulty in emergency care. Intensive Care Med. 2007 Aug;33(8):1452-7. doi: 10.1007/s00134-007-0634-y. PMID: 17554524.
- Nickel B, Gorski L, Kleidon T, Kyes A, DeVries M, Keogh S, Meyer B, Sarver MJ, Crickman R, Ong J, Clare S, Hagle ME. Infusion Therapy Standards of Practice, 9th Edition. J Infus Nurs. 2024 Jan-Feb 01;47(1S Suppl 1):S1-S285. doi: 10.1097/NAN.0000000000000532. PMID: 38211609.
- Dougherty L. Peripheral cannulation. Nurs Stand. 2008 Sep 3-9;22(52):49-56; quiz 58. doi: 10.7748/ns2009.04.23.33.59.c7187. PMID: 18792744.
- Sabri A, Szalas J, Holmes KS, Labib L, Mussivand T. Failed attempts and improvement strategies in peripheral intravenous catheterization. Biomed Mater Eng. 2013;23(1-2):93-108. doi: 10.3233/BME-120735. PMID: 23442240.
- Carr PJ, Rippey JCR, Cooke ML, Trevenen ML, Higgins NS, Foale AS, Rickard CM. Factors associated with peripheral intravenous cannulation first-time insertion success in the emergency department. A multicentre prospective cohort analysis of patient, clinician and product characteristics. BMJ Open. 2019 Apr 2;9(4):e022278. doi: 10.1136/bmjopen-2018-022278. PMID: 30944127; PMCID: PMC6500093.
- Masamoto T, Yano R. Characteristics of expert nurses' assessment of insertion sites for peripheral venous catheters in elderly adults with hard-to-find veins. Jpn J Nurs Sci. 2021 Jan;18(1):e12379. doi: 10.1111/jjns.12379. PMID: 33025696.
- Marsh N, Larsen EN, Takashima M, Kleidon T, Keogh S, Ullman AJ, Mihala G, Chopra V, Rickard CM. Peripheral intravenous catheter failure: A secondary analysis of risks from 11,830 catheters. Int J Nurs Stud. 2021 Dec;124:104095. doi: 10.1016/j.ijnurstu.2021.104095. PMID: 34689013.
- Potter, P.; Perry, A.; Stockert, P.; Hall, A. Fundamentals of Nursing: Concepts, Process, and Practice, 9th ed.; Elsevier Mosby: St. Louis, MI, USA, 2017.
- Santos-Costa P, Paiva-Santos F, Sousa LB, Bernardes RA, Ventura F, Salgueiro-Oliveira A, Parreira P, Vieira M, Graveto J. Evidence-Informed Development of a Bundle for Peripheral Intravenous Catheterization in Portugal: A Delphi Consensus Study. Nurs Rep. 2022 Jul 7;12(3):498-509. doi: 10.3390/nursrep12030047. PMID: 35894037; PMCID: PMC9326523.
- Lenhardt R, Seybold T, Kimberger O, Stoiser B, Sessler DI. Local warming and insertion of peripheral venous cannulas: single blinded prospective randomised controlled trial and single blinded randomised crossover trial. BMJ. 2002 Aug 24;325(7361):409-10. doi: 10.1136/bmj.325.7361.409. PMID: 12193353; PMCID: PMC119431.
- Biyik Bayram S, Caliskan N. Effects of local heat application before intravenous catheter insertion in chemotherapy patients. J Clin Nurs. 2016 Jun;25(11-12):1740-7. doi: 10.1111/jocn.13193. PMID: 27028834.
- Sasaki S, Murakami N, Matsumura Y, Ichimura M, Mori M. Relationship between tourniquet pressure and a cross-section area of superficial vein of forearm. Acta Med Okayama. 2012;66(1):67-71. doi: 10.18926/AMO/48083. PMID: 22358141.
- Simón-López LC, Luquero-Bueno S, Ovejero-Benito MC, Cuesta-Lozano D, Goodman-Casanova JM, Vargas-Castrillón E, Mazarro DO, De Miguel-Cáceres A, Posada-Moreno P, Zaragoza-García I, Ortuño-Soriano I. Benefits of the application of heat and pressure on peripheral venous cannulation in adults: A randomized controlled trial. J Adv Nurs. 2021 Mar;77(3):1533-1545. doi: 10.1111/jan.14655. PMID: 33219590.
- van Loon FHJ, van Hooff LWE, de Boer HD, Koopman SSHA, Buise MP, Korsten HHM, Dierick-van Daele ATM, Bouwman ARA. The Modified A-DIVA Scale as a Predictive Tool for Prospective Identification of Adult Patients at Risk of a Difficult Intravenous Access: A Multicenter Validation Study. J Clin Med. 2019 Jan 26;8(2):144. doi: 10.3390/jcm8020144. PMID: 30691137; PMCID: PMC6406455.
- Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, Shamseer L, Tetzlaff JM, Akl EA, Brennan SE, Chou R, Glanville J, Grimshaw JM, Hróbjartsson A, Lalu MM, Li T, Loder EW, Mayo-Wilson E, McDonald S, McGuinness LA, Stewart LA, Thomas J, Tricco AC, Welch VA, Whiting P, Moher D. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Syst Rev. 2021 Mar 29;10(1):89. doi: 10.1186/s13643-021-01626-4. PMID: 33781348; PMCID: PMC8008539.
- Ouzzani M, Hammady H, Fedorowicz Z, Elmagarmid A. Rayyan-a web and mobile app for systematic reviews. Syst Rev. 2016 Dec 5;5(1):210. doi: 10.1186/s13643-016-0384-4.
- National Institutes of Health (2014). Quality Assessment Tool for Observational Cohort and Cross-Sectional Studies. Available online at: https://www.nhlbi.nih.gov/health-pro/guidelines/in-develop/cardiovascular-risk-reduction/tools/cohort (last access 24/05/2025)
- J.A. Sterne, M.A. Hernán, B.C. Reeves, et al. ROBINS-I: A tool for assessing risk of bias in non-randomised studies of interventions BMJ 2016;355:i4919. doi: 10.1136/bmj.i4919.
- Ichimura M, Sasaki S, Mori M, Ogino T. Tapping but not massage enhances vasodilation and improves venous palpation of cutaneous veins. Acta Med Okayama. 2015;69(2):79-85. doi: 10.18926/AMO/53336. PMID: 25899629.
- Yasuda K, Sato S, Okada K, Yano R. The venodilation effects of tapping versus massaging for venipuncture. Jpn J Nurs Sci. 2019 Oct;16(4):491-499. doi: 10.1111/jjns.12261. PMID: 31222981.
- Ichimura M, Sasaki S, Ogino T. Tapping enhances vasodilation for venipuncture even in individuals with veins that are relatively difficult to palpate. Clin Anat. 2020 Apr;33(3):440-445. doi: 10.1002/ca.23559. PMID: 31908028.
- Yasuda K, Okada K, Sugimura N, Yano R. Do Tapping and Massaging during Tourniquet Application Promote Dilation of Forearm Cutaneous Veins? A Pilot Quasi-Experimental Study. Healthcare (Basel). 2023 Feb 10;11(4):522. doi: 10.3390/healthcare11040522. PMID: 36833056; PMCID: PMC9956355.
![]() This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.