Dessy Ekawati 1*, Nurul Azmi Arfan 2, Esti Pratiwi Yosin 2, Endang Yuswatiningsih 3
1 Department of Nursing, Faculty of Health, Institute of Science and Health Technology Insan Cendekia Medika Jombang, Indonesia.
2 Department of Midwifery, Faculty of Health, Institute of Science and Health Technology Insan Cendekia Medika Jombang, Indonesia.
3 Vocational Nursing Study Program, Ngawi District Government Nursing Academy, Indonesia.
* Corresponding Author: Dessy Ekawati, Department of Nursing, Faculty of Health, Institute of Science and Health Technology Insan Cendekia Medika Jombang, Indonesia. E-mail: dessyekawati.s1201@gmail.com, +6289624753811
Cite this article
ABSTRACT
Background: Pregnancy-related stress can affect a child’s development for a long time, increasing the likelihood of teenage anxiety. High levels of stress hormone exposure during pregnancy may interfere with the development of the nervous system and stress reactions, making a person more susceptible to anxiety disorders.
Objective: The purpose of this study is to determine the degree to which prenatal stress leads to teenage anxiety and to examine the association between maternal stress during pregnancy and teenage anxiety levels.
Methods: A cross-sectional design was used, involving 143 mothers with adolescents aged 10–19 years, selected through purposive sampling. The Prenatal Distress Questionnaire (PDQ) was used to measure prenatal stress, while the Generalized Anxiety Disorder-7 (GAD-7) was used to measure anxiety in adolescents. The link between prenatal stress and teenage anxiety was examined using Spearman’s correlation, and the impact of prenatal stress on teenage anxiety was ascertained using ordinal regression.
Results: Prenatal stress and teenage anxiety were significantly positively correlated, according to Spearman’s correlation test (r= 0.51; p < 0.0001). Ordinal regression analysis indicated that prenatal stress significantly influenced adolescent anxiety (Chi-Square = 27.9; p < 0.0001), explaining 45.6% of its variability (Nagelkerke R²= 0.46).
Conclusion: Maternal stress during pregnancy showed a moderate, significant positive correlation with adolescent anxiety (r= 0.51; p < 0.0001), explaining 45.6% of the variance in anxiety levels. Strengthening psychosocial support for pregnant women and implementing early prenatal stress detection programs are essential strategies to reduce the risk of anxiety disorders in their children. These findings highlight the need for psychological support programs for pregnant women to reduce the risk of anxiety disorders in their children.
Keywords: prenatal stress, adolescent anxiety, maternal anxiety, maternal mental health
INTRODUCTION
Pregnant women face various physical and emotional challenges that can affect their psychological well-being. Stress experienced during pregnancy not only impacts the mother but can also influence fetal development and the child’s well-being in the future. Anxiety experienced by adolescents is one of the long-term effects of prenatal stress that is often overlooked [1]. Previous studies have demonstrated that maternal stress during pregnancy is significantly associated with an increased risk of anxiety symptoms in adolescents, suggesting that early life stress exposure may have enduring psychological consequences [2].
Adolescents with a history of mothers experiencing stress during pregnancy are more vulnerable to anxiety disorders compared to their peers. High exposure to stress hormones in the womb has the potential to disrupt the development of the nervous system and the child’s stress response later in life. Specifically, elevated levels of maternal cortisol during critical periods of fetal development may alter the structure and connectivity of brain regions involved in emotional regulation, such as the amygdala, hippocampus, and prefrontal cortex [3]. Van Den Bergh et al. (2005) found that prenatal exposure to maternal anxiety alters amygdala connectivity in the fetus, potentially affecting emotional regulation into adolescence [4]. Anxiety in adolescents can significantly affect their social life, academic performance, and mental health. Anxiety’s long-term consequences include poorer academic performance, trouble interacting with others, and a higher chance of developing other mental health conditions like depression [5].
Pregnancy can be a period of psychological stress, anxiety, and health concerns. Even in uncomplicated pregnancies, around 20% of women experience excessive worry about future events. Studies suggest that 10-16% of pregnant women are diagnosed with major depressive disorder, while up to 70% experience stress and anxiety. Though the overall prevalence of psychosocial stress during pregnancy remains unclear, research indicates that 22-25% of women experience high stress levels in each trimester [6]. A recent meta-analysis involving over 200,000 pregnant women across 102 studies reported that self-reported anxiety symptoms increased from 18.2% in the first trimester to 24.6% in the third trimester. Meanwhile, clinically diagnosed anxiety disorders were found in approximately 18% of women in the first trimester and 15% in the later stages of pregnancy. This discrepancy may be due to the overlap between depression symptoms and normal emotional fluctuations during pregnancy. Additionally, approximately 6.0–16.7% of pregnant women experience severe stress, while 13.6–91.86% experience mild to moderate stress [7].
Stress during pregnancy can be triggered by various factors, such as economic pressure, household conflicts, lack of social support, and maternal health conditions, including sleep disturbances and prenatal depression [8]. Furthermore, maternal age is important, especially for young moms, who frequently endure higher stress levels as a result of social pressure, mental unpreparedness, and restricted access to quality healthcare facilities. This problem is made worse by ignorance about pregnancy and parenting, which eventually affects the growth of the fetus as well as the health of the mother. Long-term stress can raise the risk of pregnancy issues such gestational hypertension, preeclampsia, and preterm birth by interfering with the control of cortisol, which is involved in the body’s stress response [9]. Additionally, high exposure to stress hormones in the womb can affect fetal nervous system development, particularly in brain regions responsible for emotional and stress regulation, such as the amygdala and prefrontal cortex. Therefore, children of high-stress pregnant moms are more likely to have a lower stress threshold, be more susceptible to psychological strain, and develop anxiety problems during adolescence [10]. A systematic review by Tung et al. (2023) concluded that prenatal stress significantly correlates with increased risk of anxiety and behavioral issues in offspring [11].
Given these findings, it is crucial to better understand how maternal stress during pregnancy may contribute to adolescent mental health outcomes. Preventive efforts can be made by enhancing psychosocial support for pregnant women and providing education on stress management during pregnancy. Maternal mental health programs in healthcare facilities should be strengthened to enable early detection of prenatal stress. Family support and psychological counseling services can also help reduce maternal stress levels, thereby minimizing the risk of anxiety disorders in adolescents later in life [12].
Objective
This study aims to
1) examine the connection between teenage anxiety levels and the stress experienced by the mother during pregnancy, as well as;
2) assess the degree of association between prenatal stress and adolescent anxiety, considering possible confounding factors.
MATERIALS AND METHODS
Design
A cross-sectional study.
Sample
This study involved 143 mothers with adolescent children aged 10–19 years as respondents. Based on the Slovin formula with a 5% margin of error, the minimum required sample size for an estimated population of approximately 223 mothers was 143 participants. Participants were recruited from community health centers (Puskesmas) and Community Health Volunteer in Jombang District, East Java Province, Indonesia, through direct invitations and announcements with the assistance of community leaders. Inclusion criteria were:(1) mothers with adolescent children aged 10–19 years; (2) mothers able to recall and describe their experiences during pregnancy; and (3) willingness to participate by signing informed consent. Exclusion criteria included: (1) mothers with a history of severe psychiatric disorders that could affect memory reliability, and (2) mothers whose adolescent children had diagnosed neurodevelopmental disorders to avoid potential confounding factors. To minimize selection bias, recruitment procedures were standardized with uniform information sheets and consent forms provided to all candidates, and data collection was carried out by trained researchers. Nevertheless, the possibility of selection bias inherent to purposive sampling cannot be completely ruled out. Although convenience sampling allowed for timely data collection, it may have introduced selection bias and limited generalizability, compared to randomized sampling methods used in similar studies.
Data Collection
Data collection in this study was conducted in Jombang, a district in East Java Province, Indonesia, located in the eastern part of Java Island. The study took place from January 2025 to March 2025, focusing on maternal stress during pregnancy and its relationship with adolescent anxiety levels. A structured and systematic approach was implemented to ensure valid and reliable results.
Prior to data collection, a preliminary pilot test involving 10 participants was conducted to evaluate the clarity, comprehension, and cultural relevance of the instruments. To further improve data quality, several study team members with relevant expertise were involved in reviewing the research tools. Dessy Ekawati, holding a master’s degree in psychiatric nursing and formal training in Cognitive Behavioral Therapy (CBT) and statistical data processing, assessed the psychological aspects and clarity of emotional stress-related items. Nurul Azmi Arfan and Esti Pratiwi Yosin, both holding master’s degrees in midwifery with a specialization in maternal and adolescent development, evaluated the cultural appropriateness and contextual suitability of the instruments. Their input was utilized to refine item wording, improve sensitivity to the local context, and enhance the comprehensibility of the questionnaires.
The primary data collection was conducted by Dessy Ekawati, with support from Nurul Azmi Arfan and Esti Pratiwi Yosin, to ensure consistency and minimize procedural bias. Endang Yuswatiningsih, a master’s graduate in community nursing with expertise in statistical analysis, was responsible for supervising data management and quality control. Throughout the research process, participant anonymity and confidentiality were strictly maintained to promote honest and accurate responses. This study is part of a broader research initiative investigating the impact of maternal psychological stress during pregnancy on emotional outcomes during adolescence.
Measures
Maternal stress during pregnancy was measured using the Prenatal Distress Questionnaire (PDQ), while adolescent anxiety was assessed via the Generalized Anxiety Disorder-7 (GAD-7). The PDQ contains 12 items across six facets of prenatal stress, rated on a 5-point Likert scale (1 = Never to 5 = Very often): Baby’s Health & Childbirth, Physical Changes & Pregnancy Symptoms, Relationships & Social Support, Mother’s Role & Responsibilities, Financial & Career Concerns, and Mental & Emotional Health. Total scores range from 12 to 60, and were categorized as follows: low (12–27), moderate (28–43), and high (44–60). A validity test using Confirmatory Factor Analysis (CFA) showed that all items had a loading factor greater than 0.40, while the reliability test with Cronbach’s Alpha = 0.85 indicated good internal consistency. To ensure cultural relevance, the PDQ instrument used has been validated in the Indonesian context [13],
Teenagers’ anxiety levels for the previous two weeks were evaluated using the GAD-7. It consists of seven items classified into None/Minimal Anxiety (0–4), Mild Anxiety (5–9), Moderate Anxiety (10–14), and Severe Anxiety (15–21). The items are assessed on a 4-point Likert scale (0 = Never to 3 = Nearly every day), with a total score ranging from 0 to 21. A validity test of GAD-7 using Exploratory Factor Analysis (EFA) showed a loading factor greater than or equal to 0.60, and the reliability test with Cronbach’s Alpha = 0.91 demonstrated excellent internal consistency. To ensure cultural relevance, the GAD – 7 instrument used has been validated in the Indonesian context [14].
The translation and cross-cultural adaptation of both instruments into Bahasa Indonesia were performed by the research team, composed of experts in psychiatric nursing, midwifery, and community nursing, all of whom are fluent in both English and Bahasa Indonesia. The translation followed a forward and backward translation process to ensure linguistic accuracy and cultural relevance. The pre-final versions were tested on 10 participants during a pilot phase to assess clarity, cultural appropriateness, and understanding, followed by minor linguistic adjustments where necessary.
To ensure the clarity and comprehensibility of the final versions, written instructions were provided to participants, and the operator was available to explain any unclear items during administration. This adaptation process ensured that the instruments remained valid and culturally appropriate for use in the Indonesian context.
Data Analysis
This study assessed adolescent anxiety levels using the Generalized Anxiety Disorder-7 (GAD-7) and maternal prenatal stress using the Prenatal Distress Questionnaire (PDQ). Data analysis, performed with SPSS (version 26), included descriptive statistics to characterize respondents and examine mean values, standard deviations, and data distribution. A normality test using Kolmogorov-Smirnov showed
p < 0.0001 (p < 0.05), indicating that the data were not normally distributed. Therefore, the relationship between maternal stress during pregnancy and adolescent anxiety was analyzed using Spearman’s correlation test, which is suitable for ordinal-scaled data that are not normally distributed. Additionally, to determine the influence of prenatal stress on adolescent anxiety levels, ordinal regression analysis was employed, considering that the dependent variable (adolescent anxiety level) was ordinal. Ordinal regression was used to assess the extent to which an increase in maternal prenatal stress levels contributed to a higher likelihood of adolescent anxiety. All analyses were conducted with a significance level of p < 0.05, indicating that the results obtained were statistically meaningful.
Ethical Considerations
This study was approved by the Institutional Review Board (Ref: 2025-014). Participants provided written informed consent, and data confidentiality was ensured. The study adhered to the ethical principles outlined in the Declaration of Helsinki (2013), and data were stored securely with password-protected files.
RESULTS
Sample Characteristics
All mothers were under 20 years old during pregnancy (100%). Most mothers had dropped out of school or did not continue their education beyond elementary or junior high school (74.1%). The majority of mothers were housewives (63.6%) and married (86%), while single mothers were those who had experienced divorce after giving birth. Most mothers were experiencing their first pregnancy (50.3%), while those with a second or subsequent pregnancy had a history of previous miscarriage. The majority of mothers experienced mild pregnancy complications (81.1%), such as mild anemia, excessive nausea and vomiting, or low blood pressure, while the remaining mothers experienced severe complications (18.9%). Most children of mothers who experienced stress during pregnancy have now reached adolescence, with the majority aged 10-13 years (51.0%) and currently attending junior high school (73.4%). The majority of the children were male (52.4%). Most respondent families belonged to the lower socioeconomic status category (51.0%), and the majority of the children lived in urban areas (51.0%).
During pregnancy, the majority of mothers (91.6%) experienced moderate levels of stress, while a small proportion experienced low (2.1%) or high (7.0%) stress levels, as measured by the Prenatal Distress Questionnaire (PDQ). Among adolescents, 2.7% reported mild anxiety, 88.1% moderate anxiety, and 9.8% severe anxiety, as measured by the GAD-7.
A majority of mothers reporting high stress levels also came from lower socioeconomic backgrounds, which may reflect the compounding effect of economic hardship on prenatal stress.
Table 1 presents the demographic data of respondents.
|
Characteristic |
Category |
n (%) |
M (SD) |
Median (IQR) |
|
Sociodemographic of Mother |
||||
|
Age at pregnancy |
13 – 19 |
15.91(2.02) |
15.91 (14.55–17.27) |
|
|
Education |
Elementary / Junior High School |
106 (74.1%) |
||
|
High School / Vocational High School |
37 (25.9%) |
|||
|
Occupation |
Housewife |
91 (63.6%) |
||
|
Fulltime |
28 (19.6%) |
|||
|
Part – time |
11 (7.7%) |
|||
|
Self – employed |
13 (9.1) |
|||
|
Marital Status |
Married |
123 (86%) |
||
|
Single Parent |
20 (14%) |
|||
|
Number of Children |
First child |
72 (50.3%) |
||
|
Second child or more |
67 (46.9%) |
|||
|
Twins |
4 (2.8) |
|||
|
History of pregnancy complication |
Mild |
116 (81.1) |
||
|
Severe |
27 (18.9) |
|||
|
Sociodemographic of Teenage |
||||
|
Adolescent age |
12 – 18 |
14.04 (1.89) |
14.04 (12.77–15.31) |
|
|
Adolescent gender |
Male |
75 (52.4%) |
||
|
Female |
68 (47.6%) |
|||
|
Education Level |
Junior High School |
105 (73.4%) |
||
|
Senior High School |
38 (26.6%) |
|||
|
Family Socioeconomic status |
Low |
73 (51%) |
||
|
Middle |
70 (49%) |
|||
|
Residence Environment |
Urban |
73 (51%) |
||
|
Rural |
70 (49%) |
|||
|
Maternal stress levels during pregnancy |
Low |
2(1.4%) |
||
|
Middle |
131(91.6%) |
|||
|
High |
10(7%) |
|||
|
Anxiety levels in adolescents |
Mild |
3 (2.1%) |
||
|
Moderate |
126 (88.1%) |
|||
|
Severe |
14 (9.8%) |
|||
Table 1. Sociodemographic, maternal stress levels during pregnancy and adolescent anxiety levels (n = 143)
Relationship Between Maternal Stress During Pregnancy and Adolescent Anxiety Levels
The Spearman test results indicate a positive and significant relationship between maternal stress during pregnancy and adolescent anxiety levels, with a correlation coefficient of 0.51 and a significance value of 0.005 (Table 2).
|
Mean (SD) |
Median (IRQ) |
Sig. (2 tailed) Spearman Correlation |
|
|
Maternal stress levels during pregnancy |
35.82 (4.51) |
35.82 (32.76–38.88) |
Correlation coefficient of 0.512 and significance value (p) of 0.005* |
|
Anxiety levels in adolescents |
12.55 (2.43) |
12.55 (10.91–14.19) |
*p < 0.05, SD = standard deviation, IRQ = interquartile range [Q1, Q3]
Table 2. Relationship Between Maternal Stress Levels During Pregnancy and Adolescent Anxiety Levels
Figure 1 presents a scatter plot showing a moderate positive correlation (r = 0.51) between prenatal stress and adolescent anxiety. This correlation suggests that higher maternal stress levels during pregnancy are associated with increased adolescent anxiety levels. The results also indicate that the relationship between these two variables is moderate to strong and remains statistically significant.
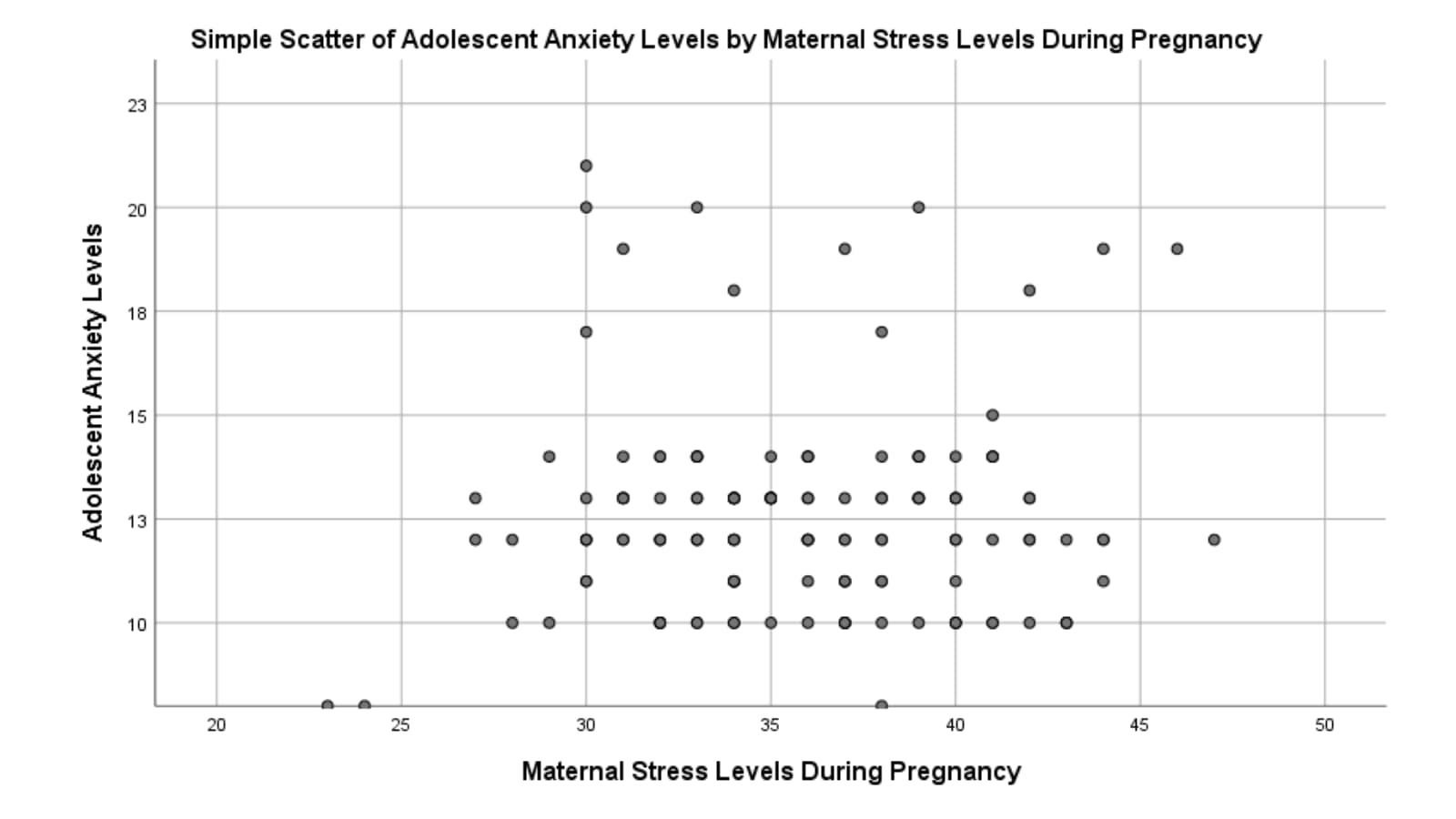
Figure 1 Scatter Plot of Adolescent Anxiety Levels by Maternal Stress Levels During Pregnancy
The crosstabulation table shows the distribution of respondents based on maternal stress levels during pregnancy and adolescent anxiety levels. The majority of adolescents with moderate anxiety levels came from mothers with moderate stress levels (Middle), totaling 118 out of 131 individuals. Among mothers with high stress levels (High), the distribution of adolescent anxiety varied more, with 8 adolescents experiencing moderate anxiety and 2 experiencing severe anxiety (Table 3).
|
Maternal stress levels during pregnancy |
Anxiety levels in adolescents |
Total |
||
|
Mild |
Moderete |
Severe |
||
|
Low |
2 |
0 |
0 |
2 |
|
Middle |
1 |
118 |
12 |
131 |
|
High |
0 |
8 |
2 |
10 |
|
Total |
3 |
126 |
14 |
143 |
Table 3. Crosstabulation of Maternal stress levels during pregnancy and Anxiety levels in adolescents
The Effect of Prenatal Stress on Adolescent Anxiety Levels
The ordinal regression analysis results indicate that the overall model is significant, with a Chi-Square value of 27.894 and p < 0.05, meaning that maternal stress during pregnancy significantly affects adolescent anxiety levels. The Nagelkerke R²value of 0.456 suggests that the model explains 45.6% of the variability in adolescent anxiety levels, indicating a moderate to strong relationship.
The model fit test shows that the Pearson value and Deviance value are both greater than 0.05, indicating a good model fit with the data. The parameter estimation results show that the threshold for category 2 (-3.876, p < 0.0001) is significant, meaning that higher maternal stress during pregnancy increases the likelihood of higher adolescent anxiety levels. Additionally, the variable of maternal stress during pregnancy (1.562, p < 0.0001) is also significant, confirming a direct and significant effect of maternal stress during pregnancy on adolescent anxiety levels.
In Table 4 we reported the results of the Ordinal Regression test.
|
Table 4a. Model Summary for Ordinal Regression |
|||||||||||
|
Model Component |
Value |
df |
Sig. (p-value) |
||||||||
|
Model Fit (Chi-Square) |
27.894 |
2 |
<0.0001 ** |
||||||||
|
Pearson Goodness-of-Fit |
χ² = 4.216 |
– |
0.081 |
||||||||
|
Deviance Goodness-of-Fit |
χ² = 5.678 |
– |
0.067 |
||||||||
|
Nagelkerke R² |
0.456 |
– |
– |
||||||||
|
Table 4b. Parameter Estimates for Predictors of Adolescent Anxiet |
|||||||||||
|
Variable / Threshold |
B |
SE |
Wald χ² |
df |
Sig. |
Exp(B) |
95% CI for Exp(B) |
||||
|
Threshold [Moderate Anxiety] |
–3.876 |
1.102 |
12.39 |
1 |
0.001 ** |
– |
– |
||||
|
Maternal Stress During Pregnancy |
1.562 |
0.496 |
9.91 |
1 |
0.002 ** |
4.77 |
1.60 – 5.05 |
||||
|
Threshold: cutoff value between anxiety categories. ** indicates significant contribution to the model. |
|||||||||||
Table 4. Results of Ordinal Regression Analysis
DISCUSSION
This study demonstrates that prenatal stress has a significant relationship with adolescent anxiety, aligning with the nature vs. nurture debate in child psychological development [15]. The nature factor influences children’s predisposition to anxiety through genetic inheritance from parents, while the nurture factor shapes children’s emotional development through environmental influences during pregnancy, including maternal stress [16]. According to a study by Van Den Bergh et al., (2005), stress experienced by the mother during pregnancy might change the responses of the fetal neurological system, especially in the limbic system, which is essential for controlling emotions [4]. Changes in the limbic system make children exposed to prenatal stress more susceptible to anxiety during adolescence [17]. Our findings are consistent with Rogers et al. (2020), who found a strong association between maternal perinatal mental health and long-term emotional outcomes in children [18].
The sociodemographic characteristics of mothers in this study reinforce the connection between nature and nurture in adolescent anxiety development. Young maternal age, low education levels, and economic pressure increase stress during pregnancy, which subsequently affects child development. Genetic factors may contribute to the inheritance of anxiety tendencies, which are then exacerbated by environmental stress [19]. A study by Sebők-Welker et al., (2024) found that mothers with low education levels have limited stress management skills, worsening the impact of prenatal stress on their children [20]. This further highlights the significant role of the prenatal environment in children’s mental health.
Social and economic support plays a crucial role in clarifying the interaction between nature and nurture in adolescent anxiety development. Some children may have a more sensitive stress response system due to genetic factors, making them more vulnerable to anxiety. A supportive social environment can help mitigate the negative effects of genetic predisposition and prenatal stress [21]. According to a study by Nóblega et al., (2024), mothers from low socioeconomic backgrounds who endure prenatal stress likely to have a greater negative effect on the emotional development of their children [22]. The majority of children in this study lived in urban areas, which, according to Raman et al., (2021), is associated with higher exposure to environmental stressors such as academic and social pressures, further exacerbating their anxiety [23].
The findings of this study support the theory that the interaction between biological (nature) and environmental (nurture) factors significantly determines adolescent anxiety development. A study by Jensen, (2025) found that children whose mothers experienced prenatal stress were more likely to develop anxiety, particularly if they also had a family history of anxiety disorders [24]. Genetic factors provide an initial vulnerability to anxiety, but environmental experiences during pregnancy and childhood determine whether this predisposition develops into a more severe psychological disorder. The findings indicate that maternal stress during pregnancy is not just an individual issue but also contributes to children’s future psychological well-being.
However, this study has several limitations. This study did not control for postnatal maternal anxiety or childhood trauma, which may also influence adolescent outcomes. Additionally, the use of convenience sampling may limit external validity. These limitations should be considered when interpreting the findings. Future research should address these limitations. Longitudinal studies are essential to establish causal links and to examine whether prenatal stress directly leads to persistent anxiety symptoms across developmental stages. Such research could offer deeper insight into the mechanisms linking prenatal conditions to long-term mental health outcomes.
Limitations
This study has several limitations. The use of purposive sampling facilitated the selection of respondents who could recall and describe their pregnancy experiences; however, it limits the generalizability of the findings, as the sample may not represent the broader population of mothers with adolescent children. This method also increases the risk of selection bias, as those who agreed to participate may have had particularly strong emotional experiences, potentially influencing the results. Future studies are recommended to use random or stratified sampling to enhance external validity. Additionally, the data relied on maternal recall of prenatal stress without objective verification such as medical records. This introduces the potential for recall bias, especially considering the time elapsed since pregnancy. Although participants were screened for major psychiatric disorders, no specific assessment of memory reliability was conducted. To address this, future research should consider prospective designs or data triangulation. The study was also limited to a specific geographic and cultural context, which may affect the applicability of the findings to populations with different sociocultural backgrounds. Lastly, the use of self-report measures introduces the possibility of social desirability bias, where participants may adjust their responses to align with perceived expectations.
CONCLUSION
According to this study, teenage anxiety levels are substantially correlated with maternal stress during pregnancy. These findings reinforce previous research suggesting that prenatal stress can influence children’s emotional development through neuroendocrine responses and psychosocial factors. The sociodemographic characteristics of the respondents, such as young maternal age, low education levels, and unfavorable socioeconomic status, contribute to high stress levels during pregnancy, ultimately affecting children’s anxiety in adolescence. The study’s findings highlight the long-term effects of maternal psychological states during pregnancy on the emotional health of offspring. These findings suggest that early interventions aimed at reducing maternal stress during pregnancy may play a key role in preventing anxiety disorders and promoting long-term mental health in children.
Research Ethics and Conflict of Interest
This study was approved by the Institute of Science and Health Technology Insan Cendekia Medika Jombang’s Research Ethics Committee (reference number 2025-014) on January 15, 2025. The authors declare no conflicts of interest.
Funding Sources
We extend our deepest gratitude to the mothers who sincerely recalled their pregnancy experiences and to the adolescents who were willing to share their stories and participate in this research. Without their openness, patience, and participation, this study would not have been possible.
Author Contributions
Concept and study design, manuscript writing and critical manuscript revision: DE, NAA, EPY, EY; data analysis and interpretation: DE, NAA. Final approval before publication: DE, NAA, EPY, EY.
REFERENCES
[1] Chauhan A, Potdar J. Maternal Mental Health During Pregnancy: A Critical Review. Cureus 2022;14. https://doi.org/10.7759/cureus.30656.
[2] Graham AM, Doyle O, Tilden EL, Sullivan EL, Gustafsson HC, Marr M, et al. Effects of maternal psychological stress during pregnancy on offspring brain development: Considering the role of inflammation and potential for preventive intervention. Biol Psychiatry Cogn Neurosci Neuroimaging 2021;7:461. https://doi.org/10.1016/J.BPSC.2021.10.012.
[3] Wu Y, De Asis-Cruz J, Limperopoulos C. Brain structural and functional outcomes in the offspring of women experiencing psychological distress during pregnancy. Mol Psychiatry 2024 297 2024;29:2223–40. https://doi.org/10.1038/s41380-024-02449-0.
[4] Van Den Bergh BRH, Mulder EJH, Mennes M, Glover V. Antenatal maternal anxiety and stress and the neurobehavioural development of the fetus and child: Links and possible mechanisms. A review. Neurosci Biobehav Rev 2005;29:237–58. https://doi.org/10.1016/j.neubiorev.2004.10.007.
[5] Jagtap A, Jagtap B, Jagtap R, Lamture Y, Gomase K. Effects of Prenatal Stress on Behavior, Cognition, and Psychopathology: A Comprehensive Review. Cureus 2023;15. https://doi.org/10.7759/cureus.47044.
[6] Pascal R, Casas I, Genero M, Nakaki A, Youssef L, Larroya M, et al. Maternal Stress, Anxiety, Well-Being, and Sleep Quality in Pregnant Women throughout Gestation. J Clin Med 2023;12:7333. https://doi.org/10.3390/jcm12237333.
[7] Zhang L, Huang R, Lei J, Liu Y, Liu D. Factors associated with stress among pregnant women with a second child in Hunan province under China’s two-child policy: a mixed-method study. BMC Psychiatry 2024;24:1–12. https://doi.org/10.1186/s12888-024-05604-7.
[8] Karnwal R, Sharmila K. Perspective View of Stress, Anxiety, and Depression among Pregnant Women: A Review. J Ecophysiol Occup Heal 2024;24:7–19. https://doi.org/10.18311/jeoh/2024/35771.
[9] Awad-Sirhan N, Simó-Teufel S, Molina-Muñoz Y, Cajiao-Nieto J, Izquierdo-Puchol MT. Factors associated with prenatal stress and anxiety in pregnant women during COVID-19 in Spain. Enferm Clin 2022;32:S5–13. https://doi.org/10.1016/j.enfcli.2021.10.006.
[10] Morales-Munoz I, Ashdown-Doel B, Beazley E, Carr C, Preece C, Marwaha S. Maternal postnatal depression and anxiety and the risk for mental health disorders in adolescent offspring: Findings from the Avon Longitudinal Study of Parents and Children cohort. Aust N Z J Psychiatry 2023;57:82–92. https://doi.org/10.1177/00048674221082519.
[11] Tung I, Hipwell AE, Grosse P, Battaglia L, Cannova E, English G, et al. Prenatal Stress and Externalizing Behaviors in Childhood and Adolescence: A Systematic Review and Meta-Analysis. Psychol Bull 2023;150:107–31. https://doi.org/10.1037/BUL0000407,.
[12] Wardoyo H, Moeloek ND, Basrowi RW, Ekowati M, Samah K, Mustopo WI, et al. Mental Health Awareness and Promotion during the First 1000 Days of Life: An Expert Consensus. Healthc 2024;12. https://doi.org/10.3390/healthcare12010044.
[13] Santoso JB. Pengembangan Skala Revised Prenatala Distress Questionnaire (NuPDQ) Versi Bahasa Indonesia. J Ilm Psikol MANASA 2018;7:62–71.
[14] Budikayanti A, Larasari A, Malik K, Syeban Z, Indrawati LA, Octaviana F. Screening of Generalized Anxiety Disorder in Patients with Epilepsy: Using a Valid and Reliable Indonesian Version of Generalized Anxiety Disorder-7 (GAD-7). Neurol Res Int 2019;2019. https://doi.org/10.1155/2019/5902610,.
[15] Shackman AJ, Gee DG. Maternal Perinatal Stress Associated With Offspring Negative Emotionality, But the Underlying Mechanisms Remain Elusive. Am J Psychiatry 2023;180:708–11. https://doi.org/10.1176/appi.ajp.20230630.
[16] Jami ES, Hammerschlag AR, Bartels M, Middeldorp CM. Parental characteristics and offspring mental health and related outcomes: a systematic review of genetically informative literature. Transl Psychiatry 2021;11. https://doi.org/10.1038/s41398-021-01300-2.
[17] Canini M, Pecco N, Caglioni M, KatušićA, Išasegi IŽ, Oprandi C, et al. Maternal anxiety-driven modulation of fetal limbic connectivity designs a backbone linking neonatal brain functional topology to socio-emotional development in early childhood. J Neurosci Res 2023;101:1484–503. https://doi.org/10.1002/jnr.25207.
[18] Rogers A, Obst S, Teague SJ, Rossen L, Spry EA, MacDonald JA, et al. Association between Maternal Perinatal Depression and Anxiety and Child and Adolescent Development: A Meta-analysis. JAMA Pediatr 2020;174:1082–92. https://doi.org/10.1001/JAMAPEDIATRICS.2020.2910,.
[19] Lopez M, Ruiz MO, Rovnaghi CR, Tam GKY, Hiscox J, Gotlib IH, et al. The social ecology of childhood and early life adversity. Pediatr Res 2021;89:353–67. https://doi.org/10.1038/s41390-020-01264-x.
[20] Sebők-Welker T, Posta E,Ágrez K, Rádosi A, Zubovics EA, Réthelyi MJ, et al. The Association Between Prenatal Maternal Stress and Adolescent Affective Outcomes is Mediated by Childhood Maltreatment and Adolescent Behavioral Inhibition System Sensitivity. Child Psychiatry Hum Dev 2024;55:1–21. https://doi.org/10.1007/s10578-023-01499-9.
[21] Hasriantirisna H, Nanda KR, Munawwarah. M S. Effects of Stress During Pregnancy on Maternal and Fetal Health: A Systematic Review. Adv Healthc Res 2024;2:103–15. https://doi.org/10.60079/ahr.v2i2.339.
[22] Nóblega M, Retiz O, Nuñez del Prado J, Bartra R. Maternal Stress Mediates Association of Infant Socioemotional Development with Perinatal Mental Health in Socioeconomically Vulnerable Peruvian Settings. Int J Environ Res Public Health 2024;21. https://doi.org/10.3390/ijerph21070844.
[23] Raman TL, Aziz NAA, Yaakob SSN. The effects of different natural environment influences on health and psychological well-being of people: A case study in selangor. Sustain 2021;13. https://doi.org/10.3390/su13158597.
[24] Jensen P. From nature to nurture–How genes and environment interact to shape behaviour. Appl Anim Behav Sci 2025;285:106582. https://doi.org/10.1016/j.applanim.2025.106582.