Presenting Cues to Promote Clinical Reasoning in Physical Assessment for Undergraduate Nursing Students: A Randomized Controlled Study
Akifumi Maeda 1*, Akemi Hirao 1, Akiko Sugimoto 1, Motoko Hori 2
- Department of Critical Care and Emergency Nursing, Faculty of Nursing, Senri Kinran University, Osaka, Japan
- Department of Chronic Care Nursing, Faculty of Nursing, Senri Kinran University, Suita, Osaka, Japan
* Corresponding author: Akifumi Maeda, Department of Critical Care and Emergency Nursing, Faculty of Nursing, Senri Kinran University, 5-25-1 Fujishirodai, Suita, Osaka, Japan. ORCID: http://orcid.org/0000-0002-2628-2224. E-mail: ak-maeda@cs.kinran.ac.jp
Cite this article
ABSTRACT
Introduction: Physical assessment is a fundamental clinical skill in nursing practice and crucial to developing effective nursing care plans. Thus, acquiring knowledge and skills in physical assessment is an essential competence for undergraduate nursing students.
Objective: This study aimed to investigate the effect of utilizing pre-assignment work and presenting specific cues about a case on the clinical reasoning skills of undergraduate nursing students by comparing an intervention group that received specific cues with a control group that did not.
Materials: This randomized controlled trial involved second-year undergraduate nursing students. Participants were randomly assigned to an intervention or control group. Both groups completed a pre-assignment related to heart failure and participated in a 60-minute group case study session. The intervention group received specific cues related to the case during the session, guiding their assessment and care planning. Clinical reasoning skills were evaluated subjectively using the Clinical Reasoning Skills Self-Assessment Scale (CRSS) and objectively by analyzing the students’ responses to the group task.
Results: A total of 94 participants were randomly assigned to either the intervention group (n= 47) or the control group (n= 47). While the pre-session CRSS scores were similar between groups, the post-session scores on several items related to information gathering, interpretation, problem identification, and goal setting were significantly higher in the intervention group. Qualitative analysis of narrative responses revealed that the intervention group provided more specific and patient-centered nursing care plans based on the patient's symptoms, whereas the control group offered more generalized interventions.
Conclusion: The use of pre-assignment and specific cues enhanced students’ ability to interpret patient information and formulate individualized nursing care plans. This approach effectively improved clinical reasoning skills in physical assessment and may serve as a practical alternative in educational settings lacking simulation-based resources.
Keywords: Clinical Reasoning, Physical Assessment, Undergraduate Nursing Student, Cues.
INTRODUCTION
Physical assessment refers to the process of collecting and evaluating information about a patient's physical condition through interviews and physical examination techniques, including inspection, palpation, percussion, and auscultation [1]. It is a core clinical competency in nursing practice [2] and is essential for developing effective nursing care plans [3]. Because accurately collecting both subjective and objective patient data enables nurses to appropriately assess a patient's condition [4], acquiring physical assessment skills is critically important for undergraduate nursing students [5].
In recent years, simulation-based education has attracted attention as an effective method for undergraduate nursing students to acquire physical assessment skills and become clinically competent upon graduation [6,7]. However, implementing simulation-based education requires considerable time and effort, as well as dedicated facilities, expensive manikins, and trained instructors, thereby imposing significant material and human resource burdens [8]. Moreover, the number of students who can participate in a simulation session simultaneously is limited [6], and institutions with large class sizes face challenges in widely implementing this approach. Therefore, there is a need to explore alternative and efficient methods for teaching physical assessment.
The information obtained through physical examination provides specific cues that serve as the starting point for clinical reasoning [9]. Rather than separating physical assessment from clinical reasoning, integrating these two areas in the learning process is expected to enhance students’ practical judgment skills. Clinical reasoning in nursing is defined as the process through which nurses collect and interpret information based on cues, understand patients’ conditions and problems, plan and implement nursing interventions, and evaluate and reflect on outcomes [9]. Physical assessment and clinical reasoning share many commonalities: both involve collecting and interpreting information about a patient’s condition and making decisions regarding nursing care, which require observation, interpretation, and judgment skills [1,9]. By learning these processes in an integrated manner, students can move beyond mere observation of physical findings to logical analysis of the information, identification of patient problems, and development of appropriate nursing care plans.
A "cue" refers to an identifiable physiological or psychosocial change experienced by a patient and includes patient information and recalled knowledge obtained through history-taking and assessment [10]. Tanner positioned these cues, referred to as “noticing,” as the foundation of clinical reasoning [11]. New graduate nurses often collect excessive amounts of information due to underdeveloped skills in distinguishing relevant from irrelevant data when attempting to accurately assess patient conditions and situations [12]. This tendency is also seen in undergraduate nursing students, who frequently struggle to identify key information among a large volume of data, leading to unfocused assessments and disruption of the clinical reasoning process. Although simulation-based education has been explored to improve students’ clinical reasoning, there is limited evidence regarding alternative, low-cost instructional methods that integrate cue recognition with physical assessment in case-based learning [13]. In particular, few studies have rigorously examined whether providing targeted cues during group discussions can enhance the clinical reasoning process in undergraduate nursing education [14].
As one approach to addressing this issue, the present study aimed to examine the effect of using pre-assignment work to help undergraduate nursing students obtain cues during a case-based physical assessment on their clinical reasoning ability.
Objective
This study aimed to examine the effects of using pre-assignment work and presenting specific cues in a case on the clinical reasoning skills of second-year undergraduate nursing students during physical assessment by comparing an intervention group that received specific cues with a control group that did not.
MATERIALS AND METHODS
Study Design
This study employed a parallel-group, two-arm, randomized controlled trial (RCT) design conducted to evaluate the effectiveness of a cue-based educational intervention on clinical reasoning skills in physical assessment. The study was implemented as part of an existing physical assessment course at a private women's university in western Japan.
The design and reporting followed the CONSORT 2025 guidelines for randomized trials [15] in educational research. Intervention and control groups received structured group learning sessions, with only the intervention group being exposed to specific case-related cues. Outcome assessments included both subjective (self-assessment scale) and objective (task-based) measures.
Conceptual Framework
Figure1 presents a conceptual diagram illustrating the process of clinical reasoning and the intervention applied during physical assessment. In this study, the process of clinical reasoning was defined as "the sequence from information collection regarding a case to the planning of interventions (nursing care)."
Participants in the intervention group progressed through the assignments by selecting and recording the information they deemed necessary, based on the "cues" presented by the researcher and the content of their pre-assignment work. This study aimed to examine how the provision of "cues" influenced the subsequent quality of information interpretation, patient understanding, and intervention planning.
The evaluation was structured to verify the effect of the intervention through both subjective and objective assessments, including scores from the Clinical Reasoning Skills Self-Assessment Scale (CRSS), and the content of students' interviews, physical examinations, and nursing care descriptions related to the case.
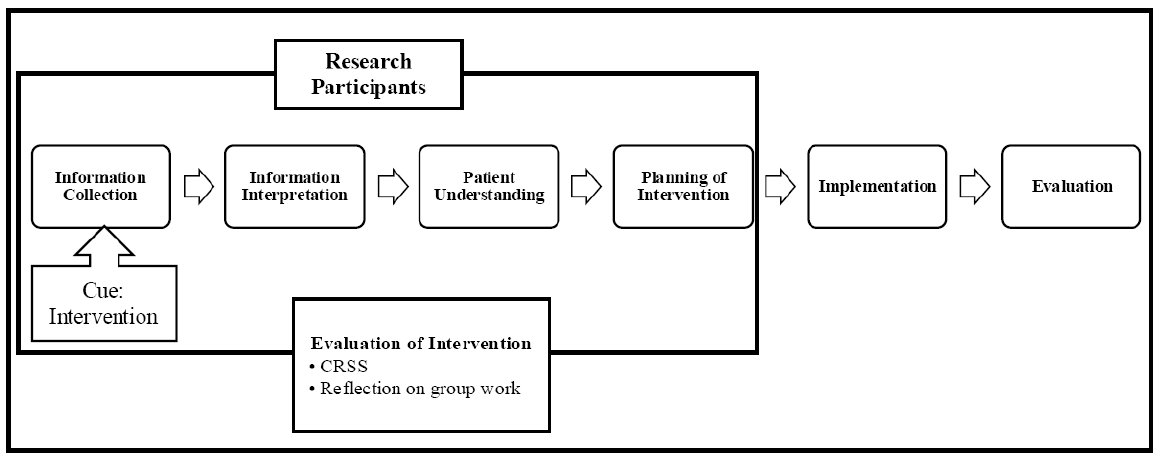
This diagram outlines the clinical reasoning process from information collection to evaluation.
The intervention group received cues to support reasoning during physical assessment, and outcomes were evaluated using CRSS and reflection.
CRSS = Clinical Reasoning Skills Self-Assessment Scale.
Figure 1. Conceptual Framework
Operational Definition
Cue: A cue refers to an identifiable physiological or psychosocial change experienced by a patient and includes patient information, and the recall of related knowledge obtained through history-taking and assessment [10]. In this study, a cue is operationally defined as the judgment material obtained by students through the use of pre-work and thinking based on mechanisms and rationales, enabling them to appropriately assess the condition of the case.
Sample Size
The sample size was calculated to compare the CRSS scores between the intervention and control groups at the end of the study. Based on an alpha level (α) of 0.05, a power (1-β) of 0.80, and a medium effect size of 0.7 (Cohen’s d), a minimum of 35 participants per group was required. Therefore, the minimum total sample size needed was 70 participants. The effect size was estimated based on results from previous similar educational intervention studies in nursing. Particularly, the total sample was expanded to 94 patients to reduce the possible bias due to missing information or data loss. In this way, 47 patients were assigned to each group. The sample size calculation was conducted using G*Power [16].
Study Population
The study was conducted at a private women’s university located in western Japan. The participants were second-year undergraduate students enrolled in the university’s Department of Nursing. All students were female by institutional policy.
Recruitment and Consent Procedure
Seven days prior to the study session, the researchers distributed an informed consent form and provided both verbal and written explanations of the study's objectives and procedures. Students were instructed to submit the completed consent form into a designated collection box at the university by the day before the session. Submission of the form was considered as consent to participate in the study.
Exclusion Criteria
Students were excluded if they (1) were absent, arrived late, or left early on the day of the session; (2) failed to complete the required pre-assignment; or (3) submitted incomplete responses on the CRSS.
Group Allocation
The randomization sequence was generated by the researcher using a computer-generated random number table with a 1:1 allocation ratio. To ensure allocation concealment, group assignments were placed in opaque, sealed envelopes and numbered sequentially. After each participant submitted their informed consent form, a separate coordinator-who was not involved in enrollment, intervention delivery, or outcome assessment-opened the envelope corresponding to the participant. This procedure ensured that neither the personnel responsible for enrollment nor the participants had prior knowledge of group assignments. Participants were blinded to their assigned group throughout the study period. However, due to the nature of the intervention, researchers were not blinded.
This study was not registered in a clinical trial registry, as it involved an educational intervention implemented within an existing university course and did not fall under ICMJE [17] or CONSORT [15] requirements for mandatory trial registration. No changes were made to the original study protocol during the course of the study.
Pre-assignment
To prepare students for the group case study session, a pre-assignment related to heart failure was distributed 14 days in advance. The assignment consisted of six questions focusing on the pathophysiology, assessment, and nursing care of a patient suspected of heart failure (see Appendix Table A1). Students were instructed to complete the assignment individually at home and bring it with them on the day of the session. This pre-assignment was designed to encourage students to review fundamental knowledge about heart failure and to consider appropriate examination methods and nursing interventions. Given the increasing global prevalence of heart failure, particularly in aging populations [18-20], emphasis was placed on recognizing symptoms and planning care based on clinical reasoning.
Study Procedures
The study was conducted on July 11, 2024, during scheduled lectures on physical assessment. Prior to participation, all students had completed 540 minutes of practical training in interview techniques and physical assessments of the respiratory, cardiovascular, gastrointestinal, musculoskeletal, and neurological systems.
Intervention
The intervention and control groups conducted the group case study sessions at separate times and in different classrooms to avoid contamination. Each session was facilitated by four researchers, all of whom were experienced nursing educators with training in physical assessment and case-based learning. To ensure consistency across sessions, all researchers referred to a common set of verbal cues prepared in advance (see Appendix Table A2), which guided the timing and content of each task. Additionally, a pre-session briefing was conducted among all researchers to align their understanding of the procedures, clarify roles, and ensure a uniform approach to facilitation. Both groups received a pre-assignment related to heart failure and completed it individually before the session. Based on previous findings suggesting that collaborative learning enhances clinical reasoning skills among nursing students [21], students worked in teams of 5-6 during the 60-minute sessions and completed six tasks sequentially using written case materials (see Appendix Table A3). Each group’s responses were recorded on standardized answer sheets. In the intervention group, specific cues were presented by the researcher prior to each task to support students’ clinical reasoning. These cues guided students to apply their pre-assignment knowledge and consider pathophysiological mechanisms. For example, prior to the Inspection task, students were asked: “Think about the visible changes or symptoms caused by heart failure.” A complete list of the cues provided is shown in Appendix Table A2.
Outcome Measures
The outcomes were evaluated using both subjective and objective measures.
CRSS Scores
Subjective evaluation of clinical reasoning skills was conducted using the Japanese version of the CRSS [22]. The original CRSS is a 26-item, five-point Likert scale developed to assess clinical reasoning processes in nursing [23]. The Japanese version has demonstrated high reliability (Cronbach’s alpha = 0.95) and acceptable content validity (CVI = 0.78) among nurses and undergraduate nursing students [22]. In the present study, 12 items specifically related to behaviors in direct clinical practice-such as implementing patient care, selecting appropriate interventions, and evaluating care outcomes-were excluded based on the consensus of the research team, as the intervention did not involve actual patient care or clinical settings. Consequently, 14 items that assessed cognitive and judgmental aspects of reasoning, including data gathering, interpretation, and planning, were retained for analysis. Although the original CRSS is multidimensional in design, the retained items in this study primarily reflect the cognitive components of clinical reasoning. The original Japanese version demonstrated acceptable content validity (CVI= 0.78); however, the modified 14-item version used in this study has not undergone a separate content validity evaluation. A total score was calculated by summing the responses to the 14 selected items (score range: 14-70), with higher scores indicating greater perceived clinical reasoning ability. The internal consistency of the modified scale was confirmed in this study, yielding a Cronbach’s alpha of 0.94. The use of the Japanese version of the CRSS was approved by the original developers.
Task Responses
Objective evaluation was conducted based on the written responses of each group to the six case-based tasks. Two evaluators-members of the research team with expertise in nursing education-assessed the specificity and appropriateness of the proposed nursing care using a predefined rubric developed for this study. The rubric included criteria such as: Alignment with the patient’s symptoms and condition, Clarity and feasibility of the proposed care, and Use of patient-specific data rather than generalized interventions. Prior to analysis, the evaluators reviewed several sample responses and calibrated their judgments through discussion to ensure consistency. Although the evaluators were members of the research team, the group allocation of each response was blinded during the assessment process to minimize potential bias.
Statistical Analysis
The CRSS scores for the intervention and control groups were confirmed to be non-normally distributed using the Shapiro-Wilk test. Therefore, the 15-item scores were summarized using the median and interquartile range. The Mann-Whitney U test was used to compare the CRSS scores between the intervention and control groups, and the Wilcoxon signed-rank test was used to compare pre-and post-session scores within each group. For the Mann-Whitney U test, mean rank values were reported in addition to p-values, particularly for items where the medians were equal between groups. For the Wilcoxon signed-rank test, we reported both the test statistic (W) and standardized Z values alongside p-values to enhance the clarity and rigor of the within-group comparisons. A two-tailed p-value less than the 5% significance level was considered statistically significant. All statistical analyses were performed using SPSS, Version 26.0 (IBM Corp, Armonk, NY, USA). Although students worked in small groups of 5-6 during the sessions, the statistical analysis did not account for potential cluster effects. This was because the CRSS was completed independently by each participant, and all instructional materials and procedures were standardized across groups to minimize variability related to group dynamics. Missing data were handled by complete case analysis; participants with incomplete CRSS responses were excluded from the final analysis.
Narrative Responses
Statistical analysis was not performed on the narrative responses. Instead, the responses were analyzed qualitatively using a basic content comparison approach. Two researchers independently reviewed the written narratives from each group and compared the content in terms of specificity and appropriateness of the proposed nursing care interventions. Discrepancies in interpretation were discussed and resolved through consensus to enhance the credibility of the analysis. While a formal thematic analysis was not conducted, this comparative review provided insights into differences in the depth and relevance of reasoning between groups. The lack of a formal qualitative methodology is acknowledged as a limitation of this study and is addressed in the limitations section.
Ethical Considerations
This study was approved by the Senri Kinran University Institutional Review Board (IRB; Approval Number: K24-007 dated May 27, 2024). Participants were informed that their participation and cooperation in the study were entirely voluntary and that non-participation would not result in any disadvantage. They were also informed, both in writing and verbally, that the study would be conducted during the lecture of the Physical Assessment course, and that their participation or non-participation would have no impact on their course grades. In addition, participants were advised that if they felt that their participation influenced their grades or if they perceived any misconduct or harassment related to the study, they could consult with the Harassment Advisory Committee established within the university.
For students who chose not to participate in the study, it was explained that while they would attend the lecture together with other students, they were not required to complete the CRSS and their data would not be included in the study analysis. Due to group assignment logistics, some students who declined to participate were included in the same groups as control group participants. These students were also given the supplementary exercise conducted for the intervention group after the completion of the study to ensure that no disadvantage would arise from their non-participation. Similarly, to prevent any disadvantage, participants assigned to the control group were provided with the same instructional content used for the intervention group after the study was completed.
RESULTS
Participant Flow
A total of 107 second-year undergraduate nursing students were eligible to participate. Of these, 94 students (87.8%) consented to take part in the study. Among those who consented, 93 were 20 years old and one was 22 years old. Participants were randomly assigned to either the intervention group (n = 47) or the control group (n = 47). However, one student in the control group was excluded due to late arrival, resulting in 93 students (86.9%) who completed the intervention as planned-47 in the intervention group and 46 in the control group. Each group was further subdivided into teams of five to six students, resulting in nine subgroups per condition. Due to missing responses on the post-session CRSS, three participants in the intervention group and four in the control group were excluded from the final analysis. Therefore, CRSS data from 44 participants in the intervention group and 42 in the control group were included in the analysis. The flow of participant enrollment, exclusion, allocation, and final inclusion for analysis is illustrated in Figure 2.
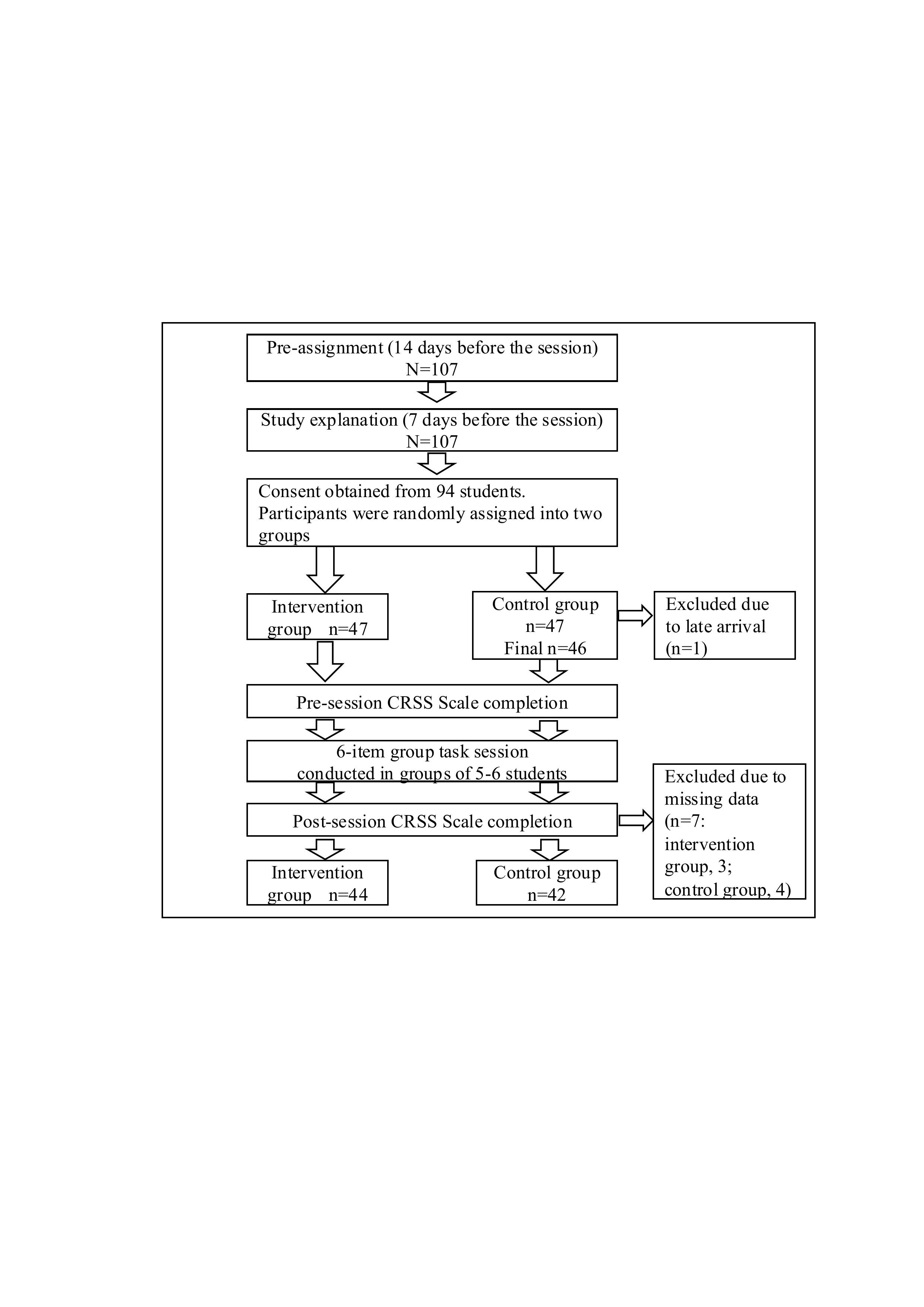
107 students were recruited; 94 consented and were assigned to two groups. After exclusions, CRSS data from 86 participants were analyzed (intervention: 44, control: 42).
CRSS = Clinical Reasoning Skills Self-Assessment Scale.
Figure 2. Study Flow and the Number of Study Participants.
Comparison of the CRSS Scores
The pre-session scores of the CRSS Scale showed no significant differences between the intervention and control groups on all 15 items. However, the post-session scores of the intervention group were significantly higher than those of the control group on ten items (Table 1, 2)
|
No. |
Question items |
Intervention group (n = 44) |
Control group (n = 42) |
Mean Rank (Intervention) |
Mean Rank (Control) |
P value |
|
1 |
I can apply the interview and physical examination to assess the patient’s condition. |
3.00 (2.25-4.00) |
3.00 (3.00-4.00) |
43.60 |
43.39 |
0.96 |
|
2 |
I can interpret the information collected. |
4.00 (3.00-4.00) |
3.50 (3.00-4.00) |
44.51 |
42.44 |
0.67 |
|
3 |
I can recognize the need for more information. |
3.00 (3.00-4.00) |
3.00 (2.75-4.00) |
46.86 |
39.98 |
0.16 |
|
4 |
I can distinguish between necessary and unnecessary information. |
3.00 (3.00-4.00) |
3.00 (2.00-4.00) |
44.50 |
42.45 |
0.68 |
|
5 |
I can anticipate how my decisions will affect the patient's condition. |
4.00 (3.00-4.00) |
3.00 (2.00-4.00) |
47.65 |
39.15 |
0.09 |
|
6 |
I can assess the cause and effect relationships in the patient’s condition. |
3.00 (2.25-4.00) |
3.00 (3.00-3.00) |
45.64 |
41.26 |
0.38 |
|
7 |
I can recognize the need for patient care. |
4.00 (4.00-4.00) |
4.00 (3.75-4.00) |
43.98 |
43.00 |
0.82 |
|
8 |
I can identify nursing problems. |
3.00 (3.00-4.00) |
3.00 (3.00-4.00) |
42.78 |
44.25 |
0.76 |
|
9 |
I can notice changes in the patient's condition. |
4.00 (4.00-4.00) |
4.00 (3.00-4.00) |
46.74 |
40.11 |
0.14 |
|
10 |
I can prioritize the patient’s needs. |
3.00 (3.00-4.00) |
3.00 (3.00-4.00) |
40.93 |
46.19 |
0.28 |
|
11 |
I can establish nursing plans. |
3.00 (2.00-4.00) |
3.00 (3.00-3.00) |
42.95 |
44.05 |
0.83 |
|
12 |
I can plan the necessary care. |
3.50 (3.00-4.00) |
3.00 (3.00-4.00) |
44.55 |
42.40 |
0.67 |
|
13 |
I can determine patient care. |
3.00 (2.25-4.00) |
3.00 (3.00-4.00) |
44.17 |
42.80 |
0.78 |
|
14 |
I can determine patient care quickly. |
3.00 (2.00-4.00) |
3.00 (2.00-3.00) |
45.16 |
41.76 |
0.50 |
|
15 |
Total |
49.00 (40.00-51.00) |
46.00 (41.0-50.25) |
45.50 |
41.40 |
0.44 |
Note 1: The scores for the question items and the total score are presented as medians (interquartile range).
Note 2: The data were analyzed using the Mann-Whitney U test.
Table 1. Comparison of the Pre-session Scores of the CRSS Between the Intervention and Control Groups.
|
No. |
Question items |
Intervention group (n = 44) |
Control group (n = 42) |
Mean Rank (Intervention) |
Mean Rank (Control) |
P value |
|
1 |
I can apply the interview and physical examination to assess the patient’s condition. |
4.00 (4.00-5.00) |
4.00 (4.00-4.00) |
48.17 |
38.61 |
0.039* |
|
2 |
I can interpret the information collected. |
4.00 (4.00-5.00) |
4.00 (4.00-4.00) |
49.07 |
37.67 |
0.014* |
|
3 |
I can recognize the need for more information. |
4.00 (4.00-5.00) |
4.00 (3.00-4.00) |
50.90 |
35.75 |
0.002* |
|
4 |
I can distinguish between necessary and unnecessary information. |
4.00 (4.00-4.00) |
4.00 (3.00-4.00) |
49.20 |
37.52 |
0.015* |
|
5 |
I can anticipate how my decisions will affect the patient's condition. |
4.00 (4.00-5.00) |
4.00 (3.00-4.00) |
49.09 |
37.64 |
0.019* |
|
6 |
I can assess the cause and effect relationships in the patient’s condition. |
4.00 (4.00-5.00) |
4.00 (3.00-4.00) |
49.32 |
37.40 |
0.016* |
|
7 |
I can recognize the need for patient care. |
4.00 (4.00-5.00) |
4.00 (4.00-5.00) |
47.72 |
39.08 |
0.076 |
|
8 |
I can identify nursing problems. |
4.00 (3.00-5.00) |
4.00 (3.00-4.00) |
47.51 |
39.30 |
0.103 |
|
9 |
I can notice changes in the patient's condition. |
4.00 (4.00-5.00) |
4.00 (3.00-4.00) |
50.27 |
36.40 |
0.005* |
|
10 |
I can prioritize the patient’s needs. |
4.00 (4.00-5.00) |
3.00 (3.00-4.00) |
47.36 |
39.45 |
0.111 |
|
11 |
I can establish nursing plans. |
4.00 (4.00-4.75) |
4.00 (3.00-4.00) |
48.42 |
38.35 |
0.040* |
|
12 |
I can plan the necessary care. |
4.00 (4.00-5.00) |
4.00 (3.00-4.00) |
48.07 |
38.71 |
0.062 |
|
13 |
I can determine patient care. |
4.00 (3.00-4.00) |
4.00 (3.00-4.00) |
47.75 |
39.05 |
0.076 |
|
14 |
I can determine patient care quickly. |
4.00 (4.00-4.00) |
3.00 (3.00-4.00) |
48.72 |
38.04 |
0.03* |
|
15 |
Total |
60.00 (53.50.-63.00) |
52.00 (48.00-59.00) |
51.84 |
34.76 |
0.002* |
Note 1: The scores for the question items and the total score are presented as medians (interquartile range).
Note 2: The data were analyzed using the Mann-Whitney U test. Significant differences are indicated by P < 0.05*.
Table 2. Comparison of the Post-session Scores of the CRSS Between the Intervention and Control Groups.
In the between-group comparisons, no significant differences were found between the intervention and control groups in any of the 15 items before the session (Table 3).
However, after the session, the intervention group scored significantly higher than the control group on 10 out of the 15 items (Table 4).
|
No. |
Question items |
Pre-session |
Post-session |
Test Statistic (W) |
Z value |
P value |
|
1 |
I can apply the interview and physical examination to assess the patient’s condition. |
3.00 (2.25-4.00) |
4.00 (4.00-5.00) |
498.00 |
-4.50 |
< 0.001* |
|
2 |
I can interpret the information collected. |
4.00 (3.00-4.00) |
4.00 (4.00-5.00) |
221.00 |
-3.15 |
0.002* |
|
3 |
I can recognize the need for more information. |
3.00 (3.00-4.00) |
4.00 (4.00-5.00) |
549.00 |
-5.01 |
< 0.001* |
|
4 |
I can distinguish between necessary and unnecessary information. |
3.00 (3.00-4.00) |
4.00 (4.00-4.00) |
423.00 |
-4.73 |
< 0.001* |
|
5 |
I can anticipate how my decisions will affect the patient's condition. |
4.00 (3.00-4.00) |
4.00 (4.00-5.00) |
232.50 |
-2.96 |
0.003* |
|
6 |
I can assess the cause and effect relationships in the patient’s condition. |
3.00 (2.25-4.00) |
4.00 (4.00-5.00) |
506.00 |
-4.70 |
< 0.001* |
|
7 |
I can recognize the need for patient care. |
4.00 (4.00-4.00) |
4.00 (4.00-5.00) |
293.50 |
-3.76 |
< 0.001* |
|
8 |
I can identify nursing problems. |
3.00 (3.00-4.00) |
4.00 (3.00-5.00) |
425.00 |
-4.22 |
< 0.001* |
|
9 |
I can notice changes in the patient's condition. |
4.00 (4.00-4.00) |
4.00 (4.00-5.00) |
277.00 |
-4.00 |
< 0.001* |
|
10 |
I can prioritize the patient’s needs. |
3.00 (3.00-4.00) |
4.00 (4.00-5.00) |
441.00 |
-4.54 |
< 0.001* |
|
11 |
I can establish nursing plans. |
3.00 (2.00-4.00) |
4.00 (4.00-4.75) |
528.00 |
-5.13 |
< 0.001* |
|
12 |
I can plan the necessary care. |
3.50 (3.00-4.00) |
4.00 (4.00-5.00) |
456.00 |
-4.21 |
< 0.001* |
|
13 |
I can determine patient care. |
3.00 (2.25-4.00) |
4.00 (3.00-4.00) |
419.00 |
-3.99 |
< 0.001* |
|
14 |
I can determine patient care quickly. |
3.00 (2.00-4.00) |
4.00 (4.00-4.00) |
496.00 |
-5.15 |
< 0.001* |
|
15 |
Total |
49.00 (40.00-51.00) |
60.00 (53.50.-63.00) |
939.00 |
-5.63 |
< 0.001* |
Note 1: The scores for the question items and the total score are presented as medians (interquartile range).
Note 2: The data were analyzed using the Wilcoxon signed-rank sum test. Significant differences are indicated by P < 0.05*.
Table 3. Comparison of the Pre-and Post-session Scores of the CRSS of the Intervention Group.
|
No. |
Question items |
Pre-session |
Post-session |
Test Statistic (W) |
Z value |
P value |
|
1 |
I can apply the interview and physical examination to assess the patient’s condition. |
3.00 (3.00-4.00) |
4.00 (4.00-4.00) |
345.00 |
-3.97 |
< 0.001* |
|
2 |
I can interpret the information collected. |
3.50 (3.00-4.00) |
4.00 (4.00-4.00) |
207.00 |
-2.24 |
0.02* |
|
3 |
I can recognize the need for more information. |
3.00 (2.75-4.00) |
4.00 (3.00-4.00) |
381.00 |
-4.28 |
< 0.001* |
|
4 |
I can distinguish between necessary and unnecessary information. |
3.00 (2.00-4.00) |
4.00 (3.00-4.00) |
234.00 |
-3.17 |
0.001* |
|
5 |
I can anticipate how my decisions will affect the patient's condition. |
3.00 (2.00-4.00) |
4.00 (3.00-4.00) |
264.00 |
-2.84 |
0.004* |
|
6 |
I can assess the cause and effect relationships in the patient’s condition. |
3.00 (3.00-3.00) |
4.00 (3.00-4.00) |
391.50 |
-3.40 |
0.001* |
|
7 |
I can recognize the need for patient care. |
4.00 (3.75-4.00) |
4.00 (4.00-5.00) |
117.00 |
-2.02 |
0.04* |
|
8 |
I can identify nursing problems. |
3.00 (3.00-4.00) |
4.00 (3.00-4.00) |
253.00 |
-2.69 |
0.007* |
|
9 |
I can notice changes in the patient's condition. |
4.00 (3.00-4.00) |
4.00 (3.00-4.00) |
109.00 |
-2.23 |
0.02* |
|
10 |
I can prioritize the patient’s needs. |
3.00 (3.00-4.00) |
3.00 (3.00-4.00) |
149.00 |
-2.30 |
0.02* |
|
11 |
I can establish nursing plans. |
3.00 (3.00-3.00) |
4.00 (3.00-4.00) |
318.50 |
-3.81 |
< 0.001* |
|
12 |
I can plan the necessary care. |
3.00 (3.00-4.00) |
4.00 (3.00-4.00) |
348.50 |
-3.49 |
< 0.001* |
|
13 |
I can determine patient care. |
3.00 (3.00-4.00) |
4.00 (3.00-4.00) |
288.00 |
-2.98 |
0.003* |
|
14 |
I can determine patient care quickly. |
3.00 (2.00-3.00) |
3.00 (3.00-4.00) |
295.00 |
-3.71 |
< 0.001* |
|
15 |
Total |
46.00 (41.0-050.25) |
52.00 (48.00-59.00) |
826.5 |
-4.69 |
< 0.001* |
Note 1: The scores for the question items and the total score are presented as medians (interquartile range).
Note 2: The data were analyzed using the Wilcoxon signed-rank sum test. Significant differences are indicated by P < 0.05*.
Table 4. Comparison of the Pre-and Post-session Scores of the CRSS of the Control Group.
Narrative Responses
During the session, participants in both the intervention and control groups provided narrative responses to a six-task group assignment.
For five of the tasks-Interview, Inspection, Palpation, Percussion, and Auscultation-no notable differences were observed between the two groups. Therefore, the common themes identified from both groups are summarized in Appendix Tables A4-A8. Appendix Tables A4-A8 present representative excerpts of the written narrative responses from both the intervention and control groups for the five physical assessment tasks. These tables illustrate how students applied clinical reasoning to assess physical signs and symptoms through written responses.
However, clear differences emerged between the intervention and control groups in the sixth task, which required students to propose nursing care plans for the simulated patient. Table 5 summarizes these responses, categorized into common responses and those unique to each group.
The intervention group provided more specific nursing care plans based on the patient's symptoms. Example responses included: "Have a lap blanket available for the patient during wheelchair transfer to address cold extremities." "Accompany the patient to the tests/examinations, considering palpitations and shortness of breath."
In contrast, the control group tended to offer general nursing care responses commonly associated with heart failure rather than case-specific interventions. Example responses included: "Provide guidance and management regarding restrictions on salt and water intake."
|
Responses |
|
Common responses from the intervention and control groups |
|
Measure vital signs (respiration, percutaneous oxygen saturation, pulse, blood pressure, respiratory rate and body temperature). |
|
Ensure comfortable positions (Fowler's position or the orthopneic position). |
|
Transfer the patient in a wheelchair due to shortness of breath and edema. |
|
Prepare and administer oxygen therapy. |
|
Explain what to expect before and after the tests/examinations and provide psychological care to reduce the patient's anxiety. |
|
Provide care for edema. |
|
Responses unique to the intervention group |
|
Accompany the patient to the tests/examinations, considering palpitations and shortness of breath. |
|
As emotional support, ask the patient if they are cold or how they are feeling. |
|
Prepare a vomit disposal bag. |
|
Check for changes in the patient's physical condition, facial color, and overall appearance during the examination. |
|
Used closed questions to make it easier for the patient to respond. |
|
Have a lap blanket available for the patient during transfer in a wheelchair to help with cold extremities. |
|
Responses unique to the control group |
|
Provide guidance and management regarding restrictions on salt and fluid intake. |
|
Provide nutritional guidance, including limiting indulgences and alcohol consumption. |
|
Provide bathing assistance. |
|
Perform measures to prevent pressure ulcers. |
|
Explain appropriate actions when symptoms worsen. |
|
Provide care for delirium. |
|
Provide rehabilitation exercise for range of motion. |
|
Provide guidance on lifestyle after discharge and outpatient follow-ups. |
|
Mange fluid balance by monitoring the body weight and urine output. |
|
Perform medication management and administration, including monitoring the effects and side effects. |
Table 5. Narrative Responses Provided by the Intervention and Control Groups: Nursing Care
DISCUSSION
This study aimed to examine the effectiveness of using pre-assignment work and specific cues in a case-based group learning session to enhance the clinical reasoning skills of undergraduate nursing students in physical assessment. The findings revealed two key outcomes that support the value of this educational approach.
First, although the pre-session scores of the CRSS Scale between the intervention and control groups showed no significant difference, the post-session scores of the intervention group were significantly higher on 10 items compared to the control group. The lack of significant differences in pre-session CRSS scores between groups supports the internal validity of the findings by indicating comparable baseline levels of clinical reasoning skills. The intervention group scored significantly higher on items related to information collection (No. 1) and interpretation (Nos. 2 and 6), problem identification (No. 9), and goal setting (Nos. 11 and 14).
Effective clinical reasoning requires nurses to accurately collect relevant cues and take appropriate action for the right patient, at the right time, and for the right reason [24]. Our findings suggest that the participants in the intervention group self-assessed improvements in their ability to collect and interpret information by utilizing the pre-assignment and interpreting the specific cues provided by the researcher as prompts for clinical reasoning. Furthermore, the significantly higher post-session scores in the intervention group indicate that the participants were able to recognize improvements not only in information collection and interpretation but also in planning appropriate nursing care interventions tailored to the patient's needs. These results imply that the intervention strengthened their ability to link patient information to problem identification and appropriate decision-making.
These findings are consistent with previous research indicating that collaborative and cue-based learning strategies can enhance clinical reasoning skills among nursing students. For example, Levett-Jones et al. [10] found that structured case-based learning promoted deeper analysis and more accurate clinical judgments. However, whereas many previous studies focused primarily on simulation-based or full-scale clinical scenarios, the present study demonstrates that similar improvements in clinical reasoning can be achieved through brief, structured interventions embedded in routine coursework. This suggests that even short, well-designed activities can meaningfully contribute to students’ development of clinical reasoning competencies.
Second, regarding the task responses, there were no notable differences between the intervention and control groups in the Interview, Inspection, Palpation, Percussion, and Auscultation tasks. This result is likely because physical assessment skills are generally acquired through repeated practice [3], and both groups had already completed basic training in these skills before participating in the study. However, significant differences emerged in the Nursing Care task.
Participants in the intervention group provided more specific and patient-centered nursing care plans based on the symptoms presented in the case. For example, their responses included: "Have a lap blanket available for the patient during wheelchair transfer to address cold extremities." "Accompany the patient to the tests/ examinations, considering palpitations and shortness of breath."
In contrast, the control group tended to offer generalized nursing interventions typical for heart failure patients, without tailoring their care to the specific symptoms of the case. Example responses included: "Provide guidance and management regarding restrictions on salt and water intake."
This difference suggests that participants in the control group lacked the ability to accurately identify and prioritize patient-specific cues, which was also reflected in their CRSS scores after the session. Supporting nursing students to focus on relevant cues, understand patient conditions and problems, and appreciate how these cues influence clinical judgments and patient outcomes is essential for the development of clinical reasoning skills [25]. In this study, specific cues provided by the researcher helped guide the intervention group participants to focus on the most relevant signs and symptoms, interpret them logically, and develop more targeted and appropriate nursing care interventions. The success of this intervention highlights the importance of structured support strategies in nursing education to bridge the gap between physical assessment findings and effective clinical decision-making. While this study demonstrated immediate improvements in clinical reasoning skills and nursing care specificity following the intervention, it did not assess long-term retention or the transfer of these skills to clinical practice. The sustainability of the observed learning gains and their impact on real-world nursing settings remain unknown. Future studies should incorporate follow-up assessments to evaluate whether these improvements are maintained over time and translated into clinical competence.
Implications for Practice and Future Research
The intervention used in this study, which encouraged undergraduate nursing students to utilize pre-assignment work and obtain specific cues during physical assessment, demonstrated potential for effectively fostering clinical reasoning skills even in settings with limited facilities and time.
This approach could be feasibly integrated into existing lecture-based curricula without the need for high-cost simulation equipment, making it particularly suitable for institutions with limited resources. For example, instructors can implement similar cue-enhanced case discussions in small group settings using printed case materials and structured prompts to guide clinical reasoning.
Future research should examine the long-term impact of this approach on knowledge retention and clinical performance. Additionally, comparative studies across multiple institutions and varying educational contexts are needed to assess the generalizability and scalability of the intervention. Investigating the effectiveness of this method in combination with simulation-based or OSCE-style assessments may also provide insights into optimizing nursing education strategies.
CONCLUSION
This study investigated the effectiveness of combining pre-assignment work with the provision of specific cues during a case-based group learning session to enhance clinical reasoning skills in undergraduate nursing students.
The findings indicate that the intervention group demonstrated significantly greater improvements in clinical reasoning ability compared to the control group, as evidenced by higher post-session scores on 10 items of the CRSS Scale. While no notable differences were observed in task responses related to Interview, Inspection, Palpation, Percussion, and Auscultation, the Nursing Care task revealed important distinctions. Students in the intervention group were more likely to identify relevant information and formulate specific, patient-centered care plans, suggesting a deeper understanding of the case context.
Overall, the results suggest that integrating structured pre-assignment learning with cue-based support can effectively foster clinical reasoning skills. This approach may be particularly beneficial in educational environments where access to simulation-based instruction is limited, offering a practical and scalable strategy to strengthen students’ reasoning capabilities in physical assessment.
Limitations
This study has several limitations. First, it was conducted at a single private women's university, potentially limiting generalizability due to contextual factors such as instructional style. Additionally, gender-related differences in clinical reasoning ability and learning preferences were not examined. These differences may influence how students engage with cue-based learning strategies, and therefore, the applicability of the results to mixed-gender or male student populations remains uncertain.
Second, the study assessed only immediate post-session outcomes; thus, the long-term retention and transfer to clinical practice remain unknown.
Third, while narrative responses were qualitatively reviewed, the absence of a formal thematic or content analysis may have limited the depth of qualitative insights.
Fourth, the sample size calculation followed a parametric approach based on an independent samples t-test using Cohen’s d index, which is commonly employed in educational intervention research.
We acknowledge that Cohen’s d is not the standard effect size for non-parametric tests like the Mann-Whitney U test used in this study. However, due to the lack of established tools supporting a priori power analysis for non-parametric effect sizes such as η² or rank-biserial correlation, we used Cohen’s d as a practical approximation.
Finally, the analysis did not account for potential clustering effects or use an intention-to-treat approach, which may introduce bias and affect the robustness of the findings.
Conflict of interest
The authors declare that they have no conflicts of interest.
Funding
This study was funded by a 2024 Cardiovascular Disease Nursing Research Grant (No. 12) from the Japan Cardiovascular Research Foundation.
Authors contribution
Author 1: Akifumi Maeda, MNS, RN, Lecturer, Faculty of Nursing, Senri Kinran University, Osaka, Japan, Contribution: Conception, design, supervision, funding, materials, data collection and processing, analysis and interpretation, literature review, writing, and critical review. E-mail: ak-maeda@cs.kinran.ac.jp; ORCID; http://orcid.org/0000-0002-2628-2224
Author 2: Akemi Hirao, PhD, RN, Professor, Faculty of Nursing, Senri Kinran University, Osaka, Japan, Contribution: Analysis and interpretation, literature review, writing, and critical review. E-mail: a-hirao@cs.kinran.ac.jp; ORCID: http://orcid.org/0009-0004-2902-5372
Author 3: Akiko Sugimoto, MNS, RN, Assistant Professor, Faculty of Nursing, Senri Kinran University, Osaka, Japan, Contribution: Conception, design, supervision, literature review, and writing. E-mail: a-sugimoto@cs.kinran.ac.jp; ORCID: http://orcid.org/0009-0003-0506-8370
Author 4: Motoko Hori, MNS, RN, Assistant Professor, Faculty of Nursing, Senri Kinran University, Osaka, Japan, Contribution: Conception, design, supervision, literature review, and writing. E-mail: m-hori@cs.kinran.ac.jp; ORCID; http://orcid.org/0000-0003-0864-2473
Acknowledgment
The authors wish to thank Nakaba Cosley for reviewing and providing English language editing on an earlier draft of the manuscript. We also express our sincere gratitude to the developers of the Japanese version of the CRSS for granting us permission to adapt and use the instrument in this study.
AI tools Usage
During the preparation of this manuscript, ChatGPT (OpenAI, https://openai.com/chatgpt) was utilized to assist with the initial English translation of the Japanese manuscript into English. The authors critically reviewed, edited, and validated all AI-generated outputs to ensure their accuracy, clarity, and appropriateness for scholarly publication. Additionally, professional English language editing was performed by Nakaba Cosley to finalize the manuscript. Importantly, no parts of the research data, study results, analysis, or scientific content were generated or altered using AI tools.
Appendix
|
No. |
Pre-assignment |
|
1 2 3 4 5 6 |
What diseases can cause heart failure? What symptoms are associated with failure of the right and left heart? What mechanisms cause those symptoms? What types of physical examinations are performed to address these symptoms? What nursing care can be provided to patients with heart failure? What tests are needed to diagnose and determine the treatment of heart failure? |
Table A1. Pre-assignment
|
The instructor asked participants to refer to their pre-assignment responses and provided the following verbal cues before they began working on each item as a group. |
|
|
Interview |
Think about the mechanism of heart failure that causes the patient's symptoms (dyspnea and edema) and interview the patient, including any associated symptoms. |
|
Inspection |
Think about the visible changes or symptoms caused by heart failure. |
|
Palpation |
Think about the palpable changes or symptoms caused by heart failure. |
|
Percussion |
Think about the symptoms or changes caused by heart failure that can be identified by percussing the body. |
|
Auscultation |
Think about auscultatory changes, such as heart or lung sounds, or symptoms caused by heart failure. |
|
Nursing care |
Think about the nursing care needed based on the patient's current condition and situation. |
Table A2. Verbal Cues Presented to the Intervention Group
|
Case scenario |
|
78-year-old female. The patient has been followed up on an outpatient basis after valve replacement surgery for mitral regurgitation. During her outpatient visit, she says, “I get short of breath when I walk a little, and the legs are swollen.” You’re an outpatient clinic nurse and suspect the patient may be suffering from heart failure. |
|
Group task |
|
Think about the interview and physical examination, using the answers in the pre-assignment to gather information that will provide evidence of heart failure. Also think about the specific nursing care based on the patient's current condition. Describe the contents of the interview, physical examination, and nursing care on the answer sheet. |
Table A3. Case scenario and Group task
|
Responses |
|
Symptom location |
|
Interview the patient about edema of the legs (left-right differences, one leg or both legs). |
|
Symptom history |
|
Interview the patient about when edema of the legs and shortness of breath started and any subsequent changes. |
|
Symptom severity |
|
Interview the patient about the severity of shortness of breath (on a scale of 1 to 10) and the severity of edema (whether socks leave marks or shoes can be worn). |
|
Associated symptoms |
|
Interview the patient if any associated symptoms are present, including loss of appetite, nausea, weight changes, fatigue, and sensation of coldness. |
|
Contributing factors |
|
Interview the patient about situations in which shortness of breath occurs (when walking or at rest). |
|
Interview the patient about lifestyle (physical activity and salt and fluid intake). |
|
Medication |
|
Interview the patient about whether or not the patient is taking any medication, the type of medication, and the medication status. |
Table A4. Narrative Responses Provided by the Intervention and Control Groups: Interview
|
Responses |
|
Respiration |
|
Observe respiratory rate, rhythm, depth, and the presence of orthopnea. |
|
Cyanosis |
|
Observe changes in the color of the skin, nails, and lips. |
|
Distension of the jugular veins |
|
Observe for distension and pulsation of the jugular veins. |
|
Facial color and complexion |
|
Observe for pallor, jaundice, and fatigue in facial complexion. |
|
Edema |
|
Observe for edema, left-right differences, the degree of swelling, and its location (legs and face). |
|
Sweating |
|
Observe for cold sweats and sweating. |
|
Somatotype and abdominal distention |
|
Observe for obesity and abdominal distention. |
Table A5. Narrative Responses Provided by the Intervention and Control Groups: Inspection
|
Responses |
|
Vocal fremitus |
|
Check for decreased or absent vibration of the thorax. |
|
Pulse |
|
Check the pulse rate, rhythm, presence of arrhythmia, left-right differences, and strength. |
|
Coldness of limbs |
|
Check the temperature and presence of coldness in the limbs. |
|
Edema |
|
Press the shin or ankle with a finger to check for indentation, depth, and the time to return. |
|
Liver |
|
Check the size, shape, and tenderness of the liver. |
Table A6. Narrative Responses Provided by the Intervention and Control Groups: Palpation
|
Responses |
|
Pleural effusion |
|
Check for pleural effusion. |
|
Ascites |
|
Check for ascites. |
|
Liver |
|
Check the size of the liver. |
Table A7. Narrative Responses Provided by the Intervention and Control Groups: Percussion
|
Responses |
|
Breath sounds |
|
Check for left-right differences, moist rales, dry rales, and adventitious sounds. |
|
Heart sounds |
|
Check for an accentuated or diminished first heart sound, a loud second heart sound, a third heart sound, and a fourth heart sound. |
|
Vascular murmurs |
|
Check for murmurs in the carotid artery, abdominal aorta, renal artery, and arteries of the lower extremities. |
|
Abdomen |
|
Check for bowel sounds. |
Table A8. Narrative Responses Provided by the Intervention and Control Groups: Auscultation
REFERENCES
- Alfaro-LeFevre R. Nursing process and clinical reasoning. Nurs Educ Perspect. 2012; 33(1): 7, doi: 10.5480/1536-5026-33.1.7.
- Chua WL, Legido-Quigley H, Ng PY, Ali S, Arora S, Liaw SY, et al. Seeing the whole picture in enrolled and registered nurses’ experiences in recognizing clinical deterioration in general ward patients: a qualitative study. Int J Nurs Stud. 2019; 95: 56-64. doi: 10.1016/j.ijnurstu.2019.04.012.
- Goto H, Yamauchi T. Nurse perceptions of physical assessment skills for detecting acute progression of heart failure. Jpn J Nurs Sci. 2020; 18(1): e12368. doi:10.1111/jjns.12368.
- Zambas S, Smythe E A, Koziol-Mclaine J. The consequences of using advanced physical assessment skills in medical and surgical nursing: A hermeneutic pragmatic study. Int J Qual Stud Health Well-being. 2016; 11: 32090. doi: 10.3402/qhw.v11.32090.
- Morrell S, Giannotti N, Pittman G, Roche M, McKinlay L, et al. Physical assessment skills taught in nursing curricula: a scoping review. JBI Evid Synth. 2021; 19(11): 2929-2957. doi: 10.11124/JBIES-20-00086.
- Cant R. P, Cooper, S J. Simulation-based learning in nurse education: systematic review. J Adv Nurs. 2010; 66(1): 3-15. doi:10.1111/j.1365-2648.2009.05240.x.
- Tawalbeh L. Effect of simulation on the confidence of university nursing students in applying cardiopulmonary assessment skills: A randomized controlled trial. J Nurs Res. 2017; 25(4): 289-295. doi: 10.1097/JNR.0000000000000170.
- Ferrari A, Maglio S, Tamirat S, Tesfaye M, Wolde M, Manenti F, et al. Nursing and midwifery simulation training with a newly developed low-cost high-fidelity placenta simulator: a collaboration between Italy and Ethiopia. BMC Med Educ. 2024; 24(1): 42. doi: 10.1186/s12909-024-06152-0.
- Hoffman K. A Comparison of decision-making by expert and novice nurses in the clinical setting, monitoring patient haemodynamic status post abdominal aortic aneurysm surgery. PhD Thesis. University of Technology, Sydney; 2007 [cited 2025 May 2]. Available from: http://hdl.handle.net/10453/21800.
- 10.Levett-Jones T, Hoffman K, Dempsey J, Jeong SY, Noble D, Norton C, et al. The 'five rights' of clinical reasoning: an educational model to enhance nursing students' ability to identify and manage clinically 'at risk' patients. Nurse Educ Today. 2010; 30(6): 515-520. doi: 10.1016/j.nedt.2009.10.020.
- Tanner CA. Thinking like a nurse: a research based model of clinical judgment. J Nurs Educ. 2006; 45(6): 204-211. doi: 10.3928/01484834-20060601-04.
- Hoffman A K, Aitken L M, Duffield C. A comparison of novice and expert nurses’ cue collection during clinical decision-making: Verbal protocol analysis. Nurse Educ Today. 2016; 46:1335-1344. doi: 10.1016/j.nedt.2016.04.001.
- Shin S, Park J H, Kim J H. Effectiveness of patient simulation in nursing education: Meta-analysis. Nurse Educ Today. 2015;35(1):176–182. doi:10.1016/j.nedt.2014.09.009.
- Bahramnezha F, Shakour M, Ravanipour M, Moattari M. Clinical reasoning education: Evaluating the effect of script strategy and reflective practice on nursing students’ reasoning development. BMC Res Notes. 2024;17:240. doi:10.1186/s13104-025-07338-5.
- Hopewell S, Chan AW, Collins GS, Hróbjartsson A, Moher D, Schulz KF, et al. CONSORT 2025 Statement: updated guideline for reporting randomised trials. BMJ. 2025; 388: e081123. doi: 10.1136/bmj-2024-081123.
- Faul F, Erdfelder E, Lang AG, Buchner A. GPower 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behavior Research Methods. 2007; 39(2):175–191. doi:10.3758/BF03193146.
- International Committee of Medical Journal Editors. Clinical Trials Registration. ICMJE. 2022 [cited 2025 Jun 2]. Available from: http://www.icmje.org/recommendations/browse/publishing-and-editorial-issues/clinical-trial-registration.html
- Ponikowski P, Anker SD, AlHabib KF, Cowie MR, Force TL, Hu S, et al. Heart failure: preventing disease and death worldwide. ESC Heart Failure. 2014; 1(1): 4–25. doi: 10.1002/ehf2.12005.
- Okura Y, Ramadan MM, Ohno Y, Suzuki K, Tanaka F, Matsumoto Y, et al. Impending epidemic: future projection of heart failure in Japan to the year 2055. Circ J. 2008; 72(3): 489-491.
- Conrad N, Judge A, Tran J, Mohseni H, Hedgecott D, Crespillo AP, et al. Temporal trends and patterns in heart failure incidence: a population-based study of 4 million individuals. The Lancet. 2018; 391(10120): 572-580. doi: 10.1016/S0140-6736(17)32520-5.
- Harmon MM, Thompson C. Clinical reasoning in pre-licensure nursing students. Teach Learn Nurs. 2015; 10(2): 63-70. doi: 10.1016/j.teln.2014.12.001.
- Naya K, Sakuramoto H, Nojima K, Ohkawa M, Tanaka Y, et al. Translation, reliability, and validity of the Japanese clinical reasoning skills self-evaluation scale: An instrument design study. Cureus. 2024; 16(1): e53177. doi: 10.7759/cureus.53177.
- Havola S, Haavisto E, Mäkinen H, Jalonen P, Koivisto J. The effects of computer-based simulation game and virtual reality simulation in nursing students' self-evaluated clinical reasoning skills. Comput Inform Nurs. 2021; 39(11): 725-735. doi: 10.1097/CIN.0000000000000748.
- Andersen B. Mapping the terrain of the discipline. In: Gray G, Pratt R, editors. Towards a Discipline of Nursing. Melbourne: Churchill Livingstone; 1991. p. 95-124.
- Benner P. From novice to expert: Excellence and power in clinical nursing practice. 2nd ed. Upper Saddle River (NJ): Prentice Hall; 2001.
![]() This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
EFFICACY OF NEGATIVE PRESSURE WOUND THERAPY IN LAPAROTOMY WOUNDS: PROTOCOL FOR A SYSTEMATIC REVIEW AND META-ANALYSIS
Melania De Filippo 1, Marco Abagnale 2*, Anella Di Costanzo 3, Valeria Visconti 4,
Fabio Gennaro Abagnale 2, Rita Citarella 5
1 Department of Abdominal Oncology, Colorectal Surgical Oncology, Istituto Nazionale Tumori – IRCCS "Fondazione G.Pascale”, Napoli, 80131, Napoli, Italy.
2 Department of Critical Care, Unit of Anesthesiology and Intensive Care, M. Scarlato Hospital, Scafati (SA), 84018, Local Healt of Salerno, Salerno, Italy.
3 Department of Cardiac Thoracic Vascular Surgery, Cardiac Thoracic Vascular Surgery, Pineta Grande Hospital, Castel Volturno, Caserta, 81030, Italy.
4 Department of Medicine, Rheumatology Unit, M. Scarlato Hospital, Scafati (SA), 84018, Local Healt of Salerno, Salerno, Italy.
5 Department of Surgery and Anaesthesia, "Umberto I" Hospital of Nocera Inferiore", 84014, Salerno, Italy.
* Corresponding author: Marco Abagnale, e-mail: abagnale.marco@gmail.com
Cite this article
ABSTRACT
Introduction: A laparotomy is a surgical procedure involving an abdominal incision to access the peritoneal cavity, commonly performed for diagnostic and therapeutic purposes, including trauma management and the treatment of gynecological, pelvic, and abdominal conditions. In this context, negative pressure wound therapy (NPWT) serves as an effective adjunct to wound management by applying subatmospheric pressure to the wound bed, thereby promoting granulation tissue formation and reducing local inflammation.
Objective: This systematic review will aim to evaluate the efficacy of NPWT compared to standard wound care in adult patients undergoing laparotomy, with specific attention to key clinical outcomes such as wound healing time, surgical site infection rates, wound dehiscence, and overall complication rates.
Materials and methods: The systematic review follows the PRISMA guidelines and uses the PICO framework for search terms. The studies will be identified through important databases (PubMed, Scopus, CINAHL and Web of Science). Methodological quality and risk of bias will be assessed with JBI critical assessment tools. This protocol for a systematic review has been registered on PROSPERO (N. CRD420251058825).
Results: The results of the systematic search and selection process will be reported using a PRISMA flowchart. The extracted data will include wound healing time, granulation tissue development, infection rates, and adverse events. The quantitative synthesis will be conducted if the homogeneity of the data allows it.
Conclusions: This systematic review will synthesize the available evidence on the efficacy of NPWT in the management of laparotomy wounds. The findings will have implications for clinical practice in surgical wound care and may contribute to the development of standardized wound management protocols.
Keywords: Laparotomy, negative pressure wound therapy, bandages, wound healing, granulation tissue, systematic review.
INTRODUCTION
A laparotomy involves a surgical incision through the abdominal wall to access the peritoneal cavity during a laparotomy procedure [1-5]. This incision is typically a large vertical cut that allows surgeons to examine and treat conditions within the abdominal organs. The term "laparotomy" itself denotes this surgical approach, which is often employed in both emergency and planned surgical settings [6]. Laparotomy remains a common surgical procedure worldwide, particularly in the treatment of abdominal trauma, intestinal obstruction, perforated bowel, and malignancies [3]. Despite its widespread use, laparotomy is associated with a high incidence of postoperative wound complications. Recent data indicate that surgical site infections (SSIs) occur in approximately 20–30% of laparotomy cases, especially in high-risk settings such as emergency surgeries or in patients with comorbidities. According to a multicenter cohort study published in 2022, SSI rates after emergency abdominal surgery reached up to 33%, with wound dehiscence observed in 4–6% of cases [7,8]. Wound dehiscence, defined as the partial or complete separation of a surgically closed wound, is strongly associated with increased morbidity, delayed recovery, and higher mortality. In a recent analysis conducted in the United States, SSIs following laparotomy were found to contribute to an average extended hospital stay of 9.7 days and increased treatment costs by over $20,000 per patient [9]. Surgical wound dehiscence (SWD) occurs in approximately 1% of patients within 30 days following laparotomy, with a prevalence of up to 3% in hepatobiliary surgery [8]. Among older patients, the incidence may reach 10%, with an associated mortality rate of up to 45% [9]. A study involving 674 patients undergoing emergency laparotomy documented a 31.9% rate of surgical complications, including 16.3% SSIs and 5% wound dehiscence. Furthermore, 19.1% of patients required surgical reintervention, while 53.6% experienced additional medical complications such as respiratory failure or sepsis [10].
These complications place a significant burden on healthcare systems. For example, a 2023 analysis estimated that surgical site infections alone contribute to over USD 3.3 billion in annual costs in the United States, primarily due to extended hospital stays, additional interventions, and increased resource utilization [6,7]. In addition, wound complications often require additional interventions, such as reoperations, prolonged antibiotic therapy, or advanced wound care support, thus placing a considerable burden on both healthcare systems and patients. Effective postoperative wound management is therefore essential to reduce these risks and promote optimal recovery. Conventional dressing techniques may be insufficient in high-risk patients or in complex surgical settings. In recent years, NPWT has emerged as an innovative approach to improving surgical wound healing. By applying controlled subatmospheric pressure through a sealed dressing system, NPWT improves tissue perfusion, reduces local edema, and facilitates the removal of exudates and contaminants [11,12]. It also promotes the formation of granulation tissue and can promote faster and longer-lasting wound closure.
Although NPWT is increasingly utilized across various surgical disciplines, no systematic review focused exclusively on its effectiveness in laparotomy wounds exists to date, there is still limited consensus regarding its efficacy specifically in laparotomy wounds. Available studies show heterogeneous results, often influenced by variability in patient populations, the type of procedure (elective vs. emergency laparotomy), surgical techniques, and NPWT protocols (e.g., pressure settings, duration, frequency of dressing changes). Furthermore, many investigations suffer from methodological limitations, small sample sizes, or a lack of attention to patient-reported outcomes such as pain, quality of life, and satisfaction with care. While some reviews in other surgical contexts have reported potential benefits of NPWT, there is currently no systematic synthesis specifically focused on laparotomy wounds. In light of these gaps, the present protocol for a systematic review aims to guide a rigorous systematic review designed to comprehensively assess the clinical efficacy of NPWT in this specific surgical population.
The use of negative pressure wound therapy (NPWT) in laparotomy wounds may offer substantial clinical advantages over conventional wound care approaches. By promoting faster wound healing, reducing the incidence of surgical site infections, and decreasing the risk of wound dehiscence, NPWT has the potential to improve surgical outcomes, particularly in high-risk patients. Its application may also reduce the need for reoperations and prolonged antibiotic therapy, thereby shortening hospital stays and facilitating earlier discharge. From a patient-centered perspective, NPWT may lead to improved pain control, better quality of life, and enhanced satisfaction with care. Integrating NPWT into postoperative care pathways could thus contribute to more efficient resource use and support the development of evidence-based protocols aimed at optimizing recovery following major abdominal surgery.
This systematic review aims to evaluate the efficacy of NPWT in laparotomy wounds by analyzing key clinical outcomes, including wound healing time, incidence of surgical site infection, wound dehiscence, and complication rates. The systematic review will also plan to consider patient-centered outcomes such as pain, quality of life, and satisfaction with care, supporting evidence-based decision-making in postoperative wound treatment.
OUTCOMES
Primary Outcomes
- Incidence of surgical site infection (SSI)
- Wound healing time (days from surgery to complete epithelialization or closure)
- Rate of wound dehiscence (partial or complete separation of the wound)
Secondary Outcomes
- Postoperative pain scores (as measured by validated pain scales, e.g., VAS or NRS)
- Quality of life (measured by validated tools such as EQ-5D, SF-36)
- Patient satisfaction with wound care
- Length of hospital stay
- Rate of reoperation related to wound complications
- Incidence of wound-related hospital readmissions
This systematic review will focus exclusively on adult patients (≥18 years) undergoing laparotomy procedures in either elective or emergency surgical settings.
Where sufficient data homogeneity is identified across studies in terms of populations, interventions, and outcome measures, a meta-analysis will be conducted. Statistical heterogeneity will be assessed using the I² statistic, with a threshold of I² > 50% indicating substantial heterogeneity. In such cases, a random-effects model will be applied. If heterogeneity is too high or data are insufficiently comparable, results will be synthesized using a narrative approach, supported by structured tables and descriptive analysis. Subgroup analyses (e.g., by type of laparotomy or patient risk profile) will be considered where appropriate and data permit.
MATERIALS AND METHODS
Study Protocol
This preliminary protocol for a systematic review is designed to ensure methodological consistency and alignment of the selected studies with the overall objectives of the systematic review. The final synthesis will aim to provide a clear and evidence-based contribution to the scientific discourse on the topic.
The protocol for a systematic review will be conducted in accordance with PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analysis) guidelines. In particular, the PRISMA-P (Preferred Reporting Items for Systematic Review and Meta-Analysis Protocols) checklist [13,14] was used to structure this protocol for a systematic review [refer to supplemental files for the complete checklist], while the full PRISMA 2020 guidelines will be used in the reporting of the final manuscript of the systematic review.
Eligibility criteria
The systematic research was developed following the PICO framework described in Table 1.
| Popolation | Patients undergoing laparotomy and with laparotomy surgical wound |
| Intervention | Negative pressure wound therapy |
| Confront | Standard Care |
| Outcome | Granulation Tissue / Wound Healing |
Table 1. PICO Framework
Eligibility criteria will include peer-reviewed primary research studies investigating the efficacy of negative pressure wound therapy in the management of laparotomy wounds. Eligible study designs will include observational studies (cohort, cross-sectional), quasi-experimental studies, randomized controlled trials (RCTs), non-randomized controlled trials, and interventional studies. The exclusion criteria will outline parameters to maintain the focus and integrity of the systematic review. Studies investigating non-laparotomies wounds, the use of other devices such as Prevena or PICO or conventional dressings, secondary studies, outcomes not related to healing will also be excluded. Similarly, editorials and opinion articles lacking primary data, animal studies, and experimental or laboratory models will be excluded from the scope of this systematic review. In addition, studies focused exclusively on pediatric populations (<18 years) will not be considered. Unpublished studies and academic theses typically lack the rigorous peer review process necessary to ensure methodological soundness, thus raising questions about their reliability and scientific validity. Similarly, while conference abstracts can offer preliminary insights into ongoing research, they are often concise and not sufficiently detailed, lacking the comprehensive data and analytical depth needed to support solid conclusions. The experimental protocols, although valuable for the understanding of the proposed methodologies, do not present empirical results and therefore offer limited utility in evidence-based evaluations. No language restrictions will be applied during the literature search to ensure comprehensive coverage of the available evidence. To mitigate the risk of excluding relevant non-English studies, the systematic review team will use professional translation tools and, when necessary, involve collaborators or native speakers for accurate interpretation of full texts. Articles in languages unfamiliar to the systematic review team will be assessed for eligibility through translated abstracts or consulted with multilingual experts when available.
Sources of information
This systematic review will include primary research studies that directly address the research question, including randomized controlled trials (RCTs), cohort studies, cross-sectional studies, case-control studies, and qualitative investigations.
The protocol for a systematic review was developed using the PICO (Population–Intervention–Comparison–Outcome) framework to ensure a methodologically sound and targeted approach to the synthesis of evidence. To ensure the completeness of the review, a structured and systematic research strategy will be employed. Carefully selected search terms will be applied to multiple electronic databases, including MEDLINE (via PubMed), CINAHL (via EBSCO), Web of Science (WOS), and SCOPUS. All eligible studies published up to the date of data extraction will be considered. Given the specific objective of the research question, the PICO framework will facilitate the precise delineation of the scope of the systematic review (Table 1).
Two independent reviewers will conduct the first screening of the titles and abstracts. In the event of disagreement, a fourth reviewer will be consulted to reach consensus. Full-text articles will be evaluated to determine final eligibility for inclusion in the systematic review.
Research strategy
We used keywords and search terms as shown in the Table 2 Duplicate records will be identified and removed using Rayyan software (Rayyan Enterprise, Cambridge, MA, USA, , accessed on 29.4.2025 [15].
| #1 Laparotomy"[MeSH Terms] |
| #2 Negative Pressure Wound Therapy"[MeSH Terms] |
| #3 negative pressure wound therapy"[MeSH Terms] OR ("negative pressure"[All fields] AND "wound"[All fields] AND "therapy"[All fields]) OR "negative pressure wound therapy"[All fields] OR ("empty"[All fields] AND "assisted"[All fields] AND "closure"[All fields]) OR "void-assisted closure"[All fields] |
| #4 Bandages"[MeSH Terms] Or "Bandages, Hydrocolloids"[MeSH Terms] Or "Occlusive Dressings"[MeSH Terms] |
| #5 Wound healing"[MeSH terms] OR "Granulation tissue"[MeSH terms] |
Table 2. Key terms and search strategy.
The defined keywords adhere to the Mesh term for health research. The keywords being used are varied because they are tailored to the search engine. The keywords are combined with Boolean operators such as “OR” and “AND” (Table 3)
| Database | Research | Results | Date |
| PubMed | ("Laparotomy"[MeSH Terms] AND "Negative Pressure Wound Therapy"[MeSH Terms]) OR ("Negative Pressure Wound Therapy"[MeSH Terms] OR ("Negative Pressure"[All Fields] AND "Wound"[All Fields] AND "Therapy"[All Fields]) OR "Negative Pressure Wound Therapy"[All Fields] OR ("Blank"[All Fields] AND "Assisted"[All Fields] AND "Closure"[All Fields]) OR "Vacuum Assisted Closure"[All Fields])) AND ("Bandages"[MeSH Terms] OR "Bandages, hydrocolloids"[MeSH terms] or "occlusive dressings"[MeSH terms]) and ("Wound healing"[MeSH terms] or "granulation tissue"[MeSH terms]) | 703 | 29/04/2025 |
| Scopus | (INDEXTERMS(Laparotomy) AND INDEXTERMS("Negative Pressure Wound Therapy")) OR (INDEXTERMS("Negative Pressure Wound Therapy") OR (ALL("negative pressure") AND ALL(wound) AND ALL(therapy)) OR ALL("Negative Pressure Wound Therapy") OR (ALL(vacuum) AND ALL(assisted) AND ALL(closure)) OR ALL("vacuum-assisted closure"))AND (INDEXTERMS(BANDAGES) OR INDEXTERMS("Bandages, Hydrocolloid") OR INDEXTERMS("Occlusive Dressings")) AND (INDEXTERMS("Wound Healing") OR INDEXTERMS("Granulation Tissue")) | 1176 | 29/04/2025 |
| CINAHL | ((HD Laparotomy+) AND (HD "Negative Pressure Wound Therapy+")) OR ((MH "Negative Pressure Wound Therapy+") OR ("Negative Pressure" AND Wound And Therapy) OR "Negative Pressure Wound Therapy" OR (Vacuum AND Assisted Closure AND) OR "Vacuum Assisted Closure")AND ((MH Bandages+) OR (MH "Bandages, Hydrocolloid+") OR (MH "Occlusive Dressings+")) AND ((MH "Wound Healing+") OR (MH "Granulation Tissue+")) | 921 | 29/04/2025 |
| WOS | (ALL=Laparotomy AND ALL="Negative Pressure Wound Therapy") OR (ALL="Negative Pressure Wound Therapy" OR (ALL="negative pressure" AND ALL=wound AND ALL=therapy) OR ALL="Negative Pressure Wound Therapy" OR (ALL=vacuum AND ALL=assisted AND ALL=closure) OR ALL="Vacuum-Assisted Closure")AND (ALL=Bandages OR ALL="Bandages, Hydrocolloid" OR ALL="Occlusive Dressings") AND (ALL="Wound Healing" OR ALL="Granulation Tissue") | 230 | 01/05/2025 |
Table 3. The search string
Selection process
The methodological quality of the included studies will be assessed using the Joanna Briggs Institute (JBI) critical evaluation tools, selecting the appropriate checklist based on the study design (e.g., case-control studies, case reports, cohort studies, case series, quasi-experimental studies, and randomized controlled trials) [16]. Each tool includes multiple elements, with response options limited to: Yes, No, ambiguous not applicable. This systematic review protocol will follow the Preferred Reporting Items for Systematic Reviews and Meta-Analyses Protocols (PRISMA-P) guidelines [14,17]. The process of selecting and extracting data will take place in two distinct phases. Initially, two reviewers will independently review the titles and abstracts of all records retrieved using Rayyan software [15] to identify potentially suitable studies. Any disagreements will be resolved by consensus; If necessary, a third reviewer will be consulted to reach the resolution. In the second phase, three reviewers will independently evaluate the full texts of the selected studies and proceed with data extraction. To ensure methodological rigor and consistency throughout the review process, each included study will be critically evaluated for both internal validity and relevance.
The following data will be extracted independently by two reviewers:
- Author(s)
- Year and country of publication
- Study design
- Study population
- Clinical or care context
- Speech(s)
- Primary and secondary outcomes
- Main Findings/Achievements
Data collection process
A PRISMA flowchart will be included to provide a visual representation of the study selection process, detailing the number of records identified, reviewed, evaluated for eligibility, and excluded, along with justifications for exclusion. This revision will follow a systematic and standardized data collection procedure, using a predefined data extraction module to ensure consistency and reproducibility. Key data elements to be extracted from each included study will include: study design, participant characteristics, intervention details, outcome measures, and key outcomes. Quantitative data will be synthesized through narrative synthesis, allowing for a descriptive comparison between studies. Instead, qualitative results will be analyzed using thematic synthesis, aimed at identifying themes, insights, and patterns through the evidence base. Each study will be ranked according to its level of evidence, thus allowing for a comparative assessment of the robustness and reliability of the results. This integrative synthesis of mixed methods will combine qualitative and quantitative evidence to develop a comprehensive understanding of the efficacy of NPWT in laparotomy wound management.
Scan risk assessment study
The risk of bias in included studies will be systematically assessed by two or more independent reviewers using the ROBINS-E (Risk Of Bias In Non-Randomized Studies of Exposures) tool, which is specifically designed to assess bias in observational studies [14].
In the event of disagreement, discrepancies will first be discussed between two reviewers. If consensus cannot be reached, a third reviewer will be consulted to resolve the issue. To evaluate inter-rater reliability during the selection process, the level of agreement between reviewers will be quantitatively assessed using Cohen’s Kappa coefficient.
The ROBINS-E tool assesses the risk of bias in seven areas:
- Confusion bias
- Bias in the selection of participants
- Bias in exposure classification
- Bias due to deviations from planned interventions (post-exposure)
- Bias due to missing data
- Bias on the measurement of results
- Bias on the selection of the reported results.
Each domain will be assessed individually, and domain-level judgments will inform the overall assessment of bias risk for each study. Overall judgment will be classified as low risk, some concerns, high risk or critical risk of bias, in accordance with the ROBINS-E guidelines.
To assess the methodological quality of non-randomised studies, the ROBINS-E tool will be used. This tool was selected because it is specifically designed to evaluate bias in studies assessing the effects of exposures, which is appropriate given the observational nature of many studies expected in this systematic review (e.g., cohort studies comparing NPWT with conventional wound care). ROBINS-E includes domains such as confounding, selection of participants, measurement of exposure and outcomes, and selection of reported results—providing a comprehensive framework for appraising the internal validity of non-randomised designs. Compared to ROBINS-I, which is tailored more closely to interventions and clinical trials, ROBINS-E better aligns with the anticipated heterogeneity in clinical exposure settings observed in surgical wound management research.
Synthesis methods
In accordance with the Joanna Briggs Institute (JBI) data extraction framework, two or more independent reviewers will perform data extraction from full-text articles included in the systematic review to ensure completeness and accuracy. The information collected will include the key characteristics of the study, such as the author and year of publication, country of origin, study objectives, sample demographics, methodology and design, type of intervention, reported outcomes, and key findings. All data will be entered into a Microsoft Excel® spreadsheet to facilitate the construction of structured summary tables and comparative analysis. The synthesis of the results will be mainly narrative in nature, with the aim of identifying and describing recurring patterns and thematic elements in studies. This approach will allow reviewers to highlight conceptual consistencies, methodological trends, and gaps in the literature that could inform future research. Quantitative data, when available, will be presented descriptively, while qualitative data will be analyzed thematically to derive common insights and meaningful interpretations. The synthesis will be guided by a structured framework that explores relationships both within individual studies and across the broader evidence base, in order to map key themes and areas of convergence. In case the included studies demonstrate sufficient methodological and statistical homogeneity, a meta-analysis will be conducted using RevMan 5.3 software. A randomized effects model will be applied to account for variability expected in study design, intervention types, and population characteristics.
Where appropriate, data from included studies will be pooled in a meta-analysis. Heterogeneity will be assessed using the I² statistic and Chi-square test. If substantial heterogeneity is detected (I² > 50%), a random-effects model will be used; otherwise, a fixed-effect model will be applied. To explore sources of heterogeneity, subgroup analyses will be conducted based on predefined variables such as type of laparotomy (elective vs. emergency), NPWT protocol (duration, pressure setting), and patient risk profile (e.g., age, comorbidities). Sensitivity analyses will also be performed by excluding studies at high risk of bias or with small sample sizes to test the robustness of the findings.
Meta-Analysis Criteria
Where appropriate, data from included studies will be pooled in a meta-analysis. Heterogeneity will be assessed using the I² statistic and Chi-square test. If substantial heterogeneity is detected (I² > 50%), a random-effects model will be used; otherwise, a fixed-effect model will be applied. To explore sources of heterogeneity, subgroup analyses will be conducted based on predefined variables such as type of laparotomy (elective vs. emergency), NPWT protocol (duration, pressure setting), and patient risk profile (e.g., age, comorbidities). Sensitivity analyses will also be performed by excluding studies at high risk of bias or with small sample sizes to test the robustness of the findings.
Measurements and results
To ensure a comprehensive evaluation of the efficacy of NPWT in the management of laparotomy wounds, this systematic review will focus on both clinical and patient-centered outcomes. Primary outcomes of interest will include wound healing indicators such as time to complete wound closure, wound infection rates, incidence of wound dehiscence, and length of hospital stay. These measures are considered essential for evaluating the clinical efficacy and safety of NPWT compared to conventional wound care methods. Secondary outcomes will encompass broader dimensions of efficacy, including patient-reported outcomes such as pain reduction, quality of life, and satisfaction with care, when available. Additional findings may include the need for resurgery or revision, antibiotic use, and healthcare resource utilization, providing a more holistic understanding of the impact of NPWT in both acute and post-operative phases. Data related to these outcomes will be extracted and analyzed in relation to study design, population characteristics, intervention protocols, and duration of follow-up. The heterogeneity of result definitions and measurement tools will be taken into account in the summary to ensure the validity and applicability of the results. Through this multidimensional outcome framework, the systematic review aims to generate robust evidence on the clinical efficacy, patient benefit, and potential health system implications of NPWT in the context of laparotomy wound management.
Impact of the review
This systematic review will synthesize original research studies evaluating the efficacy of NPWT in adult patients (≥18 years old) undergoing laparotomy. By systematically analyzing outcomes such as wound healing time, infection rates, and surgical site complications, the systematic review aims to clarify the clinical value of NPWT in laparotomy wound management compared to standard wound care approaches. The systematic review will adopt a structured and transparent methodology to ensure the robustness and reproducibility of the results. Emphasis will be placed on identifying which patient populations and clinical conditions benefit most from NPWT, as well as examining intervention protocols, duration, and care settings. This evidence-based approach will facilitate the integration of best practices into perioperative wound management and postoperative care pathways. If NPWT has been shown to significantly improve clinical outcomes, it can offer a cost-effective and scalable intervention to improve surgical recovery, reduce complications, and optimize hospital resource utilization. In addition, the findings of this systematic review can help healthcare professionals develop targeted postoperative protocols and inform clinical decision-making, ultimately helping to improve patient safety and the quality of surgical care.
DISCUSSION
This systematic review protocol aims to evaluate the efficacy of negative pressure wound therapy (NPWT) in the management of laparotomy wounds, with a primary focus on clinical outcomes such as wound healing time, surgical site infection (SSI) rates, wound dehiscence, and postoperative complications. These outcomes are critical indicators of recovery quality and patient safety following major abdominal surgery [18,19]. NPWT has been shown to promote wound healing through mechanisms such as edema reduction, enhanced local perfusion, and stimulation of granulation tissue formation [11]. Furthermore, it may contribute to a lower incidence of SSIs, particularly in high-risk patients or contaminated surgical fields [12]. Evaluating its clinical efficacy relative to conventional wound care is therefore essential to inform evidence-based surgical practice.
Secondary outcomes will include patient-reported pain scores, quality of life measures, length of hospital stay, readmission rates, and healthcare resource utilization. These broader metrics are fundamental for understanding not only the clinical effectiveness of NPWT, but also its impact on patient experience and economic sustainability [20]. Improved wound outcomes may facilitate earlier discharge, reduce the need for reoperation or prolonged antibiotic therapy, and ultimately lower the overall burden on healthcare systems. Given the significant clinical and financial consequences associated with postoperative complications, the systematic use of NPWT may yield substantial cost savings by decreasing resource consumption and improving care efficiency, particularly in high-risk surgical populations.
This systematic review aims to assess whether the clinical benefits of NPWT are accompanied by tangible economic advantages, thereby providing a robust evidence base to support more informed clinical decision-making and health policy development. By synthesizing current evidence, the systematic review will offer guidance for surgeons, wound care specialists, and nursing professionals, particularly in identifying patient populations and surgical contexts in which NPWT provides the greatest benefit—such as obese individuals, contaminated wounds, or high-tension closures [21]. Ultimately, the findings may contribute to the development of standardized, cost-effective postoperative wound management protocols and promote the integration of advanced wound care technologies into routine surgical practice [22].
Implications for clinical practice
The findings generated by this systematic review may provide a foundation for informing future clinical guidelines on postoperative wound care in laparotomy patients. Should NPWT demonstrate significant clinical benefits, such evidence could support its broader adoption in both public and private healthcare settings. In public systems, this may contribute to more efficient resource allocation by reducing complication rates and hospital stay durations. In private care contexts, it could offer cost-effective strategies that enhance patient satisfaction and surgical outcomes. By synthesising available data across various healthcare environments, the systematic review aims to produce insights that are broadly applicable and relevant to multidisciplinary clinical decision-making. Overall, this systematic review aims to generate evidence that is generalisable across diverse healthcare systems, promoting evidence-based, patient-centered surgical care.. Integrating NPWT as a standard wound care strategy could significantly contribute to improving surgical outcomes by accelerating wound healing, reducing the incidence of surgical site infections, and minimizing wound-related complications. These benefits are particularly relevant in high-risk surgical populations, such as those with obesity, diabetes, or immunosuppression, where wound healing is often impaired. Educating healthcare professionals, especially nurses and surgical staff, on the appropriate indications, application techniques, and monitoring of NPWT is essential to ensure its effective implementation. A structured training approach can help improve adherence to evidence-based wound care protocols and promote consistency in clinical practice. In addition, standardized NPWT protocols can support early mobilization, reduce the need for reoperation, and help reduce hospital stays, ultimately decreasing the burden on healthcare systems. From a patient-centered perspective, the use of NPWT can also improve postoperative experience by reducing pain, improving comfort, and promoting a faster return to daily activities. Effective laparotomy wound management through advanced wound care technologies such as NPWT not only promotes physical recovery but can also positively impact psychological well-being and patient satisfaction. Integrating NPWT into routine postoperative care pathways has the potential to optimize resource utilization, improve clinical efficiency, and align surgical wound management with modern quality and safety standards in healthcare delivery. Therefore, this systematic review aims to support evidence-based decision-making and inform the development of targeted guidelines for the management of laparotomy wounds using NPWT. From an economic point of view, NPWT implementation can offer significant cost savings potential despite the initial expense of the device and consumables. Studies have shown that the use of NPWT can lead to a reduction in overall treatment costs by decreasing the incidence of postoperative wound complications, shortening the length of hospital stay, and minimizing the need for additional surgery or prolonged antibiotic therapy. These factors collectively contribute to lower resource utilization, particularly in high-risk surgical populations where complications are more frequent and costly to manage. In addition, by accelerating wound healing and facilitating early discharge, NPWT can help increase bed turnover and improve hospital efficiency, which is especially relevant in resource-constrained healthcare facilities. While the upfront costs of NPWT systems may seem prohibitive, health economics has shown that these are often offset by downstream savings associated with avoided complications and reduced readmission rates. Therefore, integrating NPWT into standard postoperative care protocols can not only improve patient outcomes, but also represent a cost-effective strategy for surgical services that aims to optimize quality while maintaining financial sustainability.
Limitations
This systematic review may encounter several methodological limitations. While no language restrictions are applied during the selection process, allowing for the inclusion of studies published in any language, a potential risk of bias in selection remains if relevant non-English studies are lost due to translation constraints or limited access to full texts. To mitigate this, translation tools and, when necessary, native speakers will be used to ensure accurate interpretation and data extraction. Another limitation concerns the heterogeneity of the studies included. Differences in surgical indications, patient populations, wound classifications, NPWT protocols (e.g., pressure levels, frequency of dressing changes), and control interventions may call into question the feasibility of conducting a meta-analysis and may limit the comparability of results between studies. In addition, variations in reporting and outcome measurement, such as wound healing time, infection rates, or quality of life indicators, could affect the consistency of outcomes. These discrepancies can introduce a degree of variability that complicates the interpretation of the aggregated results. The risk of bias in primary studies is also a potential limitation. While validated critical evaluation tools will be used to assess methodological quality, the inclusion of observational studies, in particular, may lead to evidence that is more susceptible to confusion and bias due to lack of randomization and blinding. Finally, while the systematic review focuses on adult patients undergoing laparotomy, the diversity of surgical and clinical settings may limit the generalizability of findings to other surgical populations or wound types. However, this systematic review aims to provide a rigorous and comprehensive summary of the available evidence on the efficacy of NPWT in the management of laparotomy wounds.
Meta-bias
Potential meta-biases, including publication bias and selective reporting, will be assessed using funnel charts and the Egger test when at least 10 studies are available for a given outcome. To detect selective reporting of results, study protocols or study registries will be compared with published reports, where accessible.
All studies will be evaluated using the ROBINS-E tool, which includes domains that assess deviations from intended interventions and selective reporting, allowing for a structured assessment of reporting bias and its potential impact on systematic review conclusions.
In addition to assessing publication bias through funnel plots and Egger’s test (where applicable), this protocol for a systematic review acknowledges the inherent limitations associated with relying on published literature. Studies with statistically significant or positive findings are more likely to be published, potentially leading to overestimation of effect sizes. To mitigate this, the search strategy includes grey literature sources and trial registries when available. Furthermore, the systematic review team will consider the impact of language and database indexing bias and transparently report any imbalances in study availability across outcomes or settings. These considerations will help contextualize the findings and strengthen the interpretation of the synthesized evidence.
Funding statement
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
The authors report no conflict of interest.
Authors’ contribution
AM, DFM and CR were the major contributors in writing the manuscript. DCA, VV and AFG performed the data collection and interpreted the patient data. All authors read and approved the final manuscript.
REFERENCES
1. Rajaretnam N, Okoye E, Burns B. Laparotomy. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 [cited 2025 May 22]. Available from: http://www.ncbi.nlm.nih.gov/books/NBK525961/
2. Cleveland Clinic [Internet]. [cited 2025 May 22]. Laparotomy. Available from: https://my.clevelandclinic.org/health/treatments/24767-laparotomy
3. Badia JM, Casey AL, Petrosillo N, Hudson PM, Mitchell SA, Crosby C. Impact of surgical site infection on healthcare costs and patient outcomes: a systematic review in six European countries. J Hosp Infect. 2017 May;96(1):1–15.
4. Anderson DJ, Podgorny K, Berríos-Torres SI, Bratzler DW, Dellinger EP, Greene L, et al. Strategies to prevent surgical site infections in acute care hospitals: 2014 update. Infect Control Hosp Epidemiol. 2014 Jun;35(6):605–27.
5. van Ramshorst GH, Nieuwenhuizen J, Hop WCJ, Arends P, Boom J, Jeekel J, et al. Abdominal wound dehiscence in adults: development and validation of a risk model. World J Surg. 2010 Jan;34(1):20–7.
6. de Lissovoy G, Fraeman K, Hutchins V, Murphy D, Song D, Vaughn BB. Surgical site infection: incidence and impact on hospital utilization and treatment costs. Am J Infect Control. 2009 Jun;37(5):387–97.
7. Argenta LC, Morykwas MJ. Vacuum-assisted closure: a new method for wound control and treatment: clinical experience. Ann Plast Surg. 1997 Jun;38(6):563–76; discussion 577.
8. Wilkes RP, Kilpad DV, Zhao Y, Kazala R, McNulty A. Closed incision management with negative pressure wound therapy (CIM): biomechanics. Surg Innov. 2012 Mar;19(1):67–75.
9. Moher D, Shamseer L, Clarke M, Ghersi D, Liberati A, Petticrew M, et al. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst Rev. 2015 Jan 1;4(1):1.
10. Shamseer L, Moher D, Clarke M, Ghersi D, Liberati A, Petticrew M, et al. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015: elaboration and explanation. 2015 Jan 2 [cited 2025 Feb 8]; Available from: https://www.bmj.com/content/349/bmj.g7647
11. Ouzzani M, Hammady H, Fedorowicz Z, Elmagarmid A. Rayyan-a web and mobile app for systematic reviews. Syst Rev. 2016 Dec 5;5(1):210.
12. Mengesha MB, Chekole TT, Abraha HE, Tsegay EW, Atsbaha AH, Gebreslassie M, et al. Feasibility, acceptability, and effectiveness of group antenatal care on the continuum of care and perinatal outcomes in Sub-Saharan Africa: A systematic review and meta-analysis protocol. PLoS One. 2025 Apr 22;20(4):e0311473.
13. Moher D, Shamseer L, Clarke M, Ghersi D, Liberati A, Petticrew M, et al. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst Rev. 2015 Jan 1;4(1):1.
14. Higgins JPT, Morgan RL, Rooney AA, Taylor KW, Thayer KA, Silva RA, et al. A tool to assess risk of bias in non-randomized follow-up studies of exposure effects (ROBINS-E). Environ Int. 2024 Apr;186:108602.
15. Norman G, Shi C, Goh EL, Murphy EM, Reid A, Chiverton L, et al. Negative pressure wound therapy for surgical wounds healing by primary closure. Cochrane Database Syst Rev. 2022 Apr 26;4(4):CD009261.
16. Banwell PE, Téot L. Topical negative pressure (TNP): the evolution of a novel wound therapy. J Wound Care. 2003 Jan;12(1):22–8.
17. Hyldig N, Vinter CA, Kruse M, Mogensen O, Bille C, Sorensen JA, et al. Prophylactic incisional negative pressure wound therapy reduces the risk of surgical site infection after caesarean section in obese women: a pragmatic randomised clinical trial. BJOG. 2019 Apr;126(5):628–35.
18. Sahebally SM, McKevitt K, Stephens I, Fitzpatrick F, Deasy J, Burke JP, et al. Negative Pressure Wound Therapy for Closed Laparotomy Incisions in General and Colorectal Surgery: A Systematic Review and Meta-analysis. JAMA Surg. 2018 Nov 1;153(11):e183467.
19. Mouës CM, Heule F, Hovius SER. A review of topical negative pressure therapy in wound healing: sufficient evidence? Am J Surg. 2011 Apr;201(4):544–56.
![]() This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
PERCEIVED CAUSES OF CONFLICT AND METHODS OF CONFLICT RESOLUTION AMONG NURSES IN NIGERIAN HOSPITALS
Oseni Rukayat1, Ekpoanwan Esienumoh2, Fakeye Grace 3, Emmanson Emmanson 3*
- Sacred Heart College of Nursing Sciences - Lantoro Abeokuta, Ogun State, Nigeria
- Department of Nursing Sciences, University of Uyo, Akwa Ibom State, Nigeria
- Department of Human Anatomy, University of Cross River State, Nigeria
* Corresponding Author: Emmanson Emmanson, Department of Human Anatomy, University of Cross River University State, Nigeria. E-mail: emmansonemmanson35@gmail.com
Cite this article
ABSTRACT
Introduction: Inherent in every relationship irrespective of number of people involved is the tendency for conflict to occur, either at the intrapersonal, interpersonal, intra-professional or inter-professional level with positive or negative outcome depending on effective resolution of the conflict and the time of resolving it. Conflict has been known to bring about improved relationship, increased cohesiveness, improved communication and productivity when handled and resolved timely. The aims of the study are to identify perceived causes of workplace conflict among nurses and the resolution methods they employ.
Materials and Methods: A cross-sectional research design was used for the study. The sample was 90 nurses on permanent appointment with the hospital drawn using convenient sampling technique. Instruments were validated Rahim Organizational Conflict Inventory (ROCI II) and structured questionnaire on causes of conflicts adapted from Mukeshimana and Asingzwe (2016). Data were analyzed using descriptive statistics of frequencies and percentages and chi-square inferential statistics for causes and resolution methods for conflict at 0.05 level of significance.
Results: The outcome of the study revealed that majority of the respondents are registered nurses and registered midwives only 64 (71.1%), 66 (73.3%) were NO I or NO II; only 8 (8.9%) had Masters or higher education. Injustice (95.6%), unreasonable patient and relative expectation (93.3%), and lack of respect from other health professionals and unequal workload and work schedule (91.1% each) were identified as major causes of workplace conflict. Most prominent method of conflict resolution identified was collaboration (x = 69).
Conclusion: In conclusion, institution should organize training and retraining of nurses regularly, employ more nurses to prevent burnout and job dissatisfaction that can lead to conflict.
Keywords: Collaboration, Workplace conflict, Conflict resolution, Injustice, Nurses
INTRODUCTION
Conflict according to Ronquillo et al. (2023) [11], is the disagreement or difference of opinions between or among individuals which could involve conflicting group or team goals versus individual member’s agendas, insights, or goals which could be potentially harmful to the organization, however, conflict could be positive, promote team-building skills, critical thinking, and bring up new ideas when effectively managed by a competent leader.
Organizational conflict has been known to be an actual or perceived divergent opinion by opposing members of the organization which could involve values, interests, and needs. Opposing members could be individuals on horizontal line of management, or vertical line of management; irrespective of the cause the consequence is usually the same – reduced productivity if the conflict is not resolved early and appropriately (Awan & Saeed, 2015) [3].
Conflict is a part of interpersonal relations and is unfortunately unavoidable and a part of our daily life. For most people, conflict is often threatening and stressful, however conflict can result in the individual or organization discussion of differences that lead to creative solutions, accelerates change in an organization, especially in small businesses, where it is easy to formulate and implement new policies (Ronquillo et al. 2025) [12]. Ronquillo et al. 2025, continued that conflict prompts modification of policies and operation procedures in the organization. In cases of extreme conflict, the organization may conduct a complete overhaul of its leadership, bringing in managers with fresh ideas. According to Awan & Saeed (2015) [3], any threat to the harmony of the organization resulting in conflict sometimes may ultimately impacts negatively on the organization efficiency. Furthermore, where individual and organizational interest conflicts; when people working in an organization cannot maintain a work environment of harmony especially between the manager and subordinate then organizational efficiency, organizational progress cannot be achieved.
According to Oresanjo (2015) [8], conflict is widespread in human societies, meaning that it cannot be ruled out in any human organization, be it schools and colleges, business firms or even social clubs etc. He stated further that conflict is bound to occur because every individual is dependent on other individuals in the organization and once there is interaction, therefore, conflict cannot be ruled out. He maintained that conflict is seen as both disruptive force within an organization and primary source of individual stress. However, it is not entirely destructive. The goal of an organization should be how to control conflict in order not to degenerate into crisis rather than eliminating it.
Every organization is faced with one conflict or the other at a point in the organizational cycle especially when members of the organization perceived or believed that their interest or goal may be jeopardized and not achieved as the organization is progressing. According to Smiley (2010) [13]; Adeyemi and Aigbavboa (2022) [1], managing conflict or conflict resolution is one of the paramount skills that managers must be trained on and must be maintained to ensure organizational efficiency.
Most of the time organizational conflict occur as a result of unhealthy working environment, poor management with some staff being overloaded with work and some other staff are viewed as being redundant this may be consequent to poor organization structure or restructuring; unfair treatment which may be perceived or actual; there may be no clear-cut definition of job roles or job specification. The major causes being poor communication among members of the organization; favouritism with some being promoted while others are not promoted, jealousy and struggle for power have also been identified by different researchers as causes of conflict.
Workplace violence experienced by healthcare teams especially nurse seems to be due to lack of satisfying conflict resolution or when patient and their relations feel their needs are not being met. This problem has been reported repeatedly in most hospitals in Nigeria (Ogbonnaya et al., 2023) [6] same was experienced recently in Sacred Heart Hospital, Lantoro. The need for effective conflict resolution by nurses to prevent escalation of conflict prompted the interest for this study. From literature reviewed by the researcher it was discovered that there is paucity of research work conducted on causes of conflict and the methods of conflict resolution among nurses, between the nurse and other health care professionals; nurses and patient and/or patient’s relations.
This research assessed the causes of workplace conflict among nurses in Sacred Heart Hospital, Lantoro, Abeokuta, Ogun state and methods of conflict resolutions utilized by them.
MATERIALS AND METHODS
Study Population
This was a descriptive cross-sectional study conducted among clinical nurses at Sacred Heart Hospital, Lantoro, Nigeria, between September 2021 and August 2022, with final data analysis completed by December 2022.
The study targeted registered nurses currently working in the hospital across different clinical departments and nursing cadres. Nurses were selected from inpatient and outpatient units based on their availability and consent to participate.
The study protocol matched the Declaration of Helsinki ethical guidelines for clinical studies, and it was approved by the Technical Scientific Committee of Sacred Heart Hospital, Lantoro, with approval letter dated September 15, 2021, ref: SHH/EC/EA/05/09/21. All participants were informed and signed their informed consent.
Inclusion criteria
- Registered nurses licensed by the Nursing and Midwifery Council of Nigeria
- Minimum of 2 years of clinical experience
- Willingness to give informed consent and participate voluntarily
Exclusion criteria
- Nurses on annual leave, sick leave, or study leave during the study period
- Nurses who declined to provide informed consent.
Instrument
This study utilized a common instrument—the Rahim Organizational Conflict Inventory–II (ROCI–II) created by Rahim (1983)—to assess conflict management styles among nurses. Specifically, Forms A, B, and C of the ROCI-II with 28 items each were used to assess conflict resolution styles when dealing with supervisors (Form A), subordinates (Form B), and peers (Form C). The instrument assesses five conflict management styles: Integrating (Collaborating), Obliging (Accommodating), Dominating (Competing), Avoiding, and Compromising.
All of the items on the ROCI-II are measured on a 5-point Likert scale, from 1 = Strongly Disagree to 5 = Strongly Agree. The 28 items on each of the two forms are arrayed into five subscales that correspond to the five conflict resolution styles. The item classification into each style is as follows:
1) Integrating (Collaborating) – 7 items, 2) Obliging (Accommodating) – 6 items, 3) Dominating (Competing) – 5 items, 4) Avoiding – 6 items, 5) Compromising – 4 items.
In addition, an adapted version of the Causes of Conflict Questionnaire by Mukeshimana and Asingzwe (2016) [5] was employed to assess potential causes of conflict in the workplace. The adapted instrument included structured items designed to bring out nurses' views of interpersonal, organizational, and communication-related causes of conflict. The items also received scores on a 5-point Likert scale ranging from 1 = Strongly Disagree to 5 = Strongly Agree. To ensure content validity, the instruments were reviewed by nursing science and educational measurement and evaluation specialists. They checked the items for consistency, relevance, and clarity with the initial instruments. Minor modifications were effected to improve the appropriateness and readability of the questionnaire items to the study environment from their inputs. The final instrument retained the fundamental constructs and design of the initial instruments.
Statistical Analysis
Data obtained were analyzed based on objectives and hypotheses. Socio-demographic data was analyzed using descriptive statistics and presented on a percentage and frequency table.
The non-parametric Friedman test was used for testing the differences between three or more dependent variables. If the Friedman test was positive (P<0.05), the post hoc Wilcoxon signed-rank test was used for pairwise comparison. The chi-square test or Fisher's exact test were performed to assess significant differences in proportions or percentages between two independent variables. Fisher's exact test was used when the chi-square test was found to be inappropriate. Causes and Methods of conflict were analyzed using SPSS version 20 and presented with tables. All the hypotheses were tested with a significance level of 0.05.
RESULTS
Ninety-six copies of the questionnaire were distributed to sample selected for the study but only 90 copies (93.8%) of returned questionnaire were completely filled and met the criteria for analysis. Therefore, 90 copies of the questionnaire were analyzed.
| Characteristics | % (n) |
| Gender | |
| Female | 95.6% (86) |
| Male | 4.4% (4) |
| Religion | |
| Christian | 93.3% (84) |
| Islam | 6.7% (6) |
| Marital status | |
| Single | 51.1% (46) |
| Married | 42.2% (38) |
| Divorced | 4.4% (4) |
| Widow | 2.2% (2) |
| Level of education | |
| RN/RM | 71.1% (64) |
| BNSc | 20.0% (18) |
| ≥MSc | 8.9% (8) |
| Cadre | |
| NO I – NO II | 73.3% (66) |
| SNO - PNO | 11.1% (10) |
| ACNO - ADN | 15.6% (14) |
| Grade level | |
| Below 13 | 73.3% (66) |
| 13 - 15 | 22.2% (20) |
| 16 and above | 4.4% (4) |
Table 1. General characteristics of the sample.
Table 1 shows that more female nurses 86 (95.6%) than male nurses 4 (4.4%) participated in the study. A majority of the respondents are Christians 84 (93.3%). About half of the respondents are single 46 (51.1%), while widows are 2 (2.2%). A majority of the respondents are RN/RM only 64 (71.1%); only 8 (8.9%) had Master’s or higher education. For the cadre, more than half 66 (73.3%) are NO I or NO II. Similarly, 66 (73.3%) are below grade level 13, followed by those on grade level 13 – 15 with 20 (22.2%).
| Causes | Agree % (n) | Disagree % (n) |
| Distrust | 88.9% (80) | 11.1% (10) |
| Refusal to take orders from doctor | 64.4% (58) | 35.6% (32) |
| Doctors consider themselves as superior | 80.0% (72) | 20.0% (18) |
| Lack of respect from other health professionals | 91.1% (82) | 8.9% (8) |
| Different level of education | 77.8% (70) | 22.2% (20) |
| Conflict of interest and absence of procedure and strategies | 80.0% (72) | 20.0% (18) |
| Lack of respect and lack of attention to patient | 71.1% (64) | 28.9% (26) |
| Being insulted by the doctor before patient | 82.2% (74) | 17.8% (16) |
| Order from a doctor which is out of the scope of my practice | 75.6% (68) | 24.4% (22) |
| Delay of the doctor to answer my call in emergency case | 88.9% (80) | 11.1% (10) |
| Injustice from some nurse managers | 95.6% (86) | 4.4% (4) |
| Favouritism | 86.7% (78) | 13.3% (12) |
| Unequal workload and work schedule | 91.1% (82) | 8.9% (8) |
| Unreasonable patient and relative expectation | 93.3% (84) | 6.7% (6) |
| Imbalance nurse-patient ratio | 88.9% (80) | 11.1% (10) |
Table 2. Distribution of Respondent on Causes of Conflict (N = 90)
Table 2 shows that all the items identified constitute strong causes of conflict ranging between 58 (64.0%) and 86 (95.6%) out of 90, with refusal to take orders from doctors being the least count 58 (64.0%) while 86 (95.6%) of the respondents supported injustice from some nurse managers as the major cause of conflict in the hospital, followed by unreasonable patient and relative expectation (93.3%), unequal workload and lack of respect from other health professionals (91.1% each). Delay of the doctor to calls in emergency cases, imbalance nurse-patient ratio, and distrust were also significant causes of conflict with 88.9% respectively.
Figure 1: Percentage distribution of responses to method of conflict resolution utilized by nurses (N = 90). The figure shows the mean percentage values and the standard deviations in brackets.
The figure above shows positive response to various methods of conflict resolution in the hospital. Form A depicts conflict resolution with subordinates, Form B depicts conflict resolution among colleagues, Form C depicts method of conflict resolution among superior. Average of the responses shows the overall average performance across board or of the three forms. It can be observed that most of the respondents discouraged the use of competing resolution with an average score of 38% while they supported the use of collaboration with an average score 69%. Accommodating, compromising and avoiding have equal percentages (average 52.0% each). Therefore, it can be deduced that majority of nurses utilize collaboration in conflict resolution (69.0%) while few nurses use competing (38.0%) in resolving conflict in Sacred Heart Hospital, Lantoro, Abeokuta.
Statistical analysis using the Friedman test (χ² = 92.15, df = 4, p < 0.001) confirmed a significant difference in method preference. Post hoc Wilcoxon signed-rank tests (Holm-corrected) showed that collaboration (median: 69.0) was significantly more used than competing (median: 38.0, p < 0.001), accommodating (median: 52.0, p = 0.003), and avoiding (median: 52.0, p = 0.005). Competing was also significantly less used than accommodating (median: 52.0, p = 0.007).
Table 3 presents a cross-tabulation of the respondents’ preferred methods for conflict resolution in relation to their demographic and professional characteristics, including gender, cadre, and level of education. This descriptive overview highlights distribution patterns across the five conflict resolution styles.
| Characteristics | Accommodating | Avoiding | Collaborating | Competing | Compromising | Total |
| Gender | ||||||
| Male (n=4) | – | – | 4 (100.0%) | – | – | 100.0% |
| Female (n=86) | 6 (7.1%) | 20 (23.8%) | 37 (42.9%) | 4 (4.8%) | 18 (21.4%) | 100.0% |
| Cadre | ||||||
| NO II (n=24) | 1 (4.2%) | 4 (16.7%) | 13 (54.2%) | 1 (4.2%) | 5 (20.8%) | 100.0% |
| NO I (n=9) | 1 (11.1%) | 2 (22.2%) | 3 (33.3%) | – | 3 (33.3%) | 100.0% |
| SNO (n=2) | – | 1 (50.0%) | 1 (50.0%) | – | – | 100.0% |
| PNO (n=1) | – | – | 1 (100.0%) | – | – | 100.0% |
| ACNO (n=1) | – | – | – | 1 (100.0%) | – | 100.0% |
| CNO (n=1) | – | – | 1 (100.0%) | – | – | 100.0% |
| ADN (n=5) | – | 3 (60.0%) | 1 (20.0%) | – | 1 (20.0%) | 100.0% |
| Level of Education | ||||||
| Diploma (n=54) | 2 (3.7%) | 8 (14.8%) | 32 (59.3%) | 2 (3.7%) | 10 (18.5%) | 100.0% |
| B.Sc. (n=12) | 2 (16.7%) | 3 (25.0%) | 3 (25.0%) | 1 (8.3%) | 3 (25.0%) | 100.0% |
| M.Sc. (n=8) | – | 8 (100.0%) | – | – | – | 100.0% |
| Others (n=4) | – | 1 (25.0%) | 2 (50.0%) | – | 1 (25.0%) | 100.0% |
Table 3. Cross tabulation of association of respondent’s characteristics and their method of conflict resolution (N = 90).
Table 4 summarizes the results of statistical analyses used to examine the association between respondents’ characteristics and their chosen method for conflict resolution. Chi-square tests, likelihood ratios, and Fisher-Freeman-Halton exact tests were applied to assess significance.
The analysis showed that there is no significant association between gender and method of conflict resolution used by nurses. The Fisher’s exact test was also carried out because 60% of the expected cell frequencies were below 5, with a minimum expected count of 0.18 which violates the chi square assumption. The p-value (0.453) was greater than the significant level (0.05). Hence, there is no evidence to reject the null hypothesis.
| Gender | Value | df | Asymptotic Sig. (2-sided) | Exact Sig. (2-sided) |
| Pearson Chi-Square | 5.029a | 4 | 0.284 | 0.310 |
| Likelihood Ratio | 6.537 | 4 | 0.162 | 0.176 |
| Fisher-Freeman-Halton Exact Test | 3.402 | 0.453 | ||
| N of Valid Cases | 88 | |||
| Cadre | ||||
| Pearson Chi-Square | 62.306a | 24 | 0.0 | |
| Likelihood Ratio | 35.889 | 24 | 0.056 | 0.02* |
| Fisher-Freeman-Halton Exact Test | 31.533 | 0.049* | ||
| N of Valid Cases | 86 | |||
| Education | ||||
| Pearson Chi-Square | 19.407a | 12 | 0.079 | 0.090 |
| Likelihood Ratio | 18.398 | 12 | 0.104 | 0.097 |
| Fisher-Freeman-Halton Exact Test | 17.089 | 0.073 | ||
| N of Valid Cases | 88 | |||
| * = significant test | * = significant test | * = significant test | * = significant test | * = significant test |
Table 4. Analysis of the association between several variables and method of conflict resolution.
The analysis also showed that there is a significant association between cadre and method of conflict resolution used by nurses. The Fisher’s exact test was carried out because 88.6% of the expected cell frequencies were below 5, with a minimum expected count of 0.09 which violates the chi square assumption. The p-value (0.049) was lower than the significant level (0.05). Hence, the null hypothesis is rejected, and the conclusion is that there is an association between cadre and the conflict resolution.
The level of education was also tested with the style of conflict resolution used by nurses. The Fisher’s exact test was used instead of the chi-square test because 80% of the expected cell frequencies were below 5, with a minimum expected frequency of 0.09 which violates the chi-square assumption. The p-value (0.073) was greater than the significant level (0.05). Hence, there is no evidence to reject the null hypothesis.
DISCUSSION
The perceived factors causing conflict experienced by nurses include injustice from some nurse managers (95.6%) being the major cause of conflict, unreasonable patient and relative expectation (93.3%), unequal workload and lack of respect from other health professionals (91.1% each). Delay of the doctor to calls in emergency cases, imbalance nurse-patient ratio, and distrust (88.9% each), this was supported by Pitsillidou, et al. (2018) [9] findings among health professionals in hospitals of Cyprus to record the types of conflict management that health professionals in Cyprus hospitals encounter in their daily work and to explore the conflicts, their parameters and causes, and the role ambiguity faced by hospital employees. It was discovered that health professionals identified heavy workload, low pay, and varying instructions from different leaders as causes of conflict. In addition, the findings of a study by Olajide et al. (2015) [7] on conflict among nurses and doctors in 2 tertiary hospitals in Ekiti State indicated that odds of conflicts were significantly higher with limited opportunities for staff interaction (OR=1.8, CI=1.1-2.9); desire for power (autonomy) by doctors (OR=3.2, CI=1.9-5.2) and desire for more influence by nurses (OR=12.5, CI=4.8-41.3). Chances of expressing conflicts were significantly higher as strikes (OR=2.1; 1.3-3.5) but less with physical assaults (OR=0.1, CI=0.03-0.41). This is also, supported by Akpabio et al. (2015) [2] research finding which showed that un-resolved conflicts may be linked to poor communication resulting from refusal to cooperate, poor team collaboration and problem-solving, decreased clients’ satisfaction, distrust, split camps, gossips and disruption of work-flow, overwork and poor rewarding system each with frequency of 222 (92.0%); patients-related conflict and leadership conflicts each with frequency of 218 (90.0%); misunderstanding involving nursing colleagues with a frequency of 194 (81.0%); poor work environment 192 (80.0%); conflicts with other health professionals with 189 (78.0%) frequency and discrimination issues with 180 (61.0%) frequency.
Methods of conflict resolution include collaboration, accommodation, and compromising. The study revealed that more than half of the nurses utilized collaboration (69.0%), accommodating, compromising and avoiding (52.0% respectively) and only a few used competitions as a method of conflict resolution. A Friedman test revealed a significant difference in utilizing these conflict resolution methods (χ² = 92.15, df = 4, p < 0.001). Post hoc Wilcoxon signed-rank tests with Holm-Bonferroni correction showed that collaboration was significantly more utilized than competing (p < 0.001), meaning that nurses certainly utilize collaborative styles more than confrontational styles. This is in contrast with the results of Pitsillidou, et al. (2018) [9], that respondents utilized avoidance (73.2%) over negotiation for mutual benefit (54.2%), and compromise (40.5%) as conflict management mechanisms, as compared with the results of Adeyemi and Aigbavboa (2022) [1], that collaboration, accommodating, negotiating, compromising, and mediating were the most common conflict resolution styles utilized by Southwest Nigerian construction professionals. In addition, collaboration was employed significantly more than accommodating (p = 0.003) and avoiding (p = 0.005). These findings validate the perspective that nurses regard collaborative approaches as not only professionally appropriate but also more effective in resolving intricate interpersonal and hierarchical disputes within the clinical setting. Collaboration enhances mutual respect and problem-solving, which are essential values in nursing practice. The findings mirror Adeyemi and Aigbavboa's (2022) [1] results, which also indicated extremely high reliance on cooperation as a conflict resolution style.
Competing was utilized significantly less than accommodating (p = 0.007), demonstrating that aggressive or assertive styles are actively avoided or rejected by nurses. This aligns with the philosophy of caregiving in nursing, which promotes empathy and de-escalation. While some degree of assertiveness may be required in critical care practice, the overall avoidance of competitive conflict resolution suggests a strong professional culture that prioritizes harmony over hierarchy.
Surprisingly, no difference was detected in the use of accommodating, compromising, and avoiding styles (p > 0.05). This can reflect the pragmatic interchangeability of these styles on a day-to-day basis, especially if nurses attempt to minimize friction but not necessarily the source. This passivity or neutrality can be a coping strategy in environments where power imbalances are prevalent, or where organizational constraints reduce formal conflict resolution mechanisms.
There is no relationship between gender and level of education, and conflict resolution style used by nurses, except cadre which influenced conflict resolution approach. This suggests that positional status in an organization plays a role in managing conflict, perhaps due to variations in authority, confidence, and experience. This finding is against Birkhoff's (2015) [4] that gender significantly influences conflict dynamics at the individual and societal levels. In order to understand the role of gender in conflict comprehensively, it is important to examine it through individual, interpersonal, and societal levels. Gender may manifest itself in conflicts through how parties interpret and make sense of the conflict. Birkhoff also presented the findings of Gwartney-Gibbs to support his findings that gender also had an effect on dispute handling mechanisms. Conflict resolution processes for women were not as effective as those of men. For example, women would avoid more than resolving the conflict. However, the current findings show that within professional clinical environments such as Sacred Heart Hospital, formalized positions and codes of conduct can counteract the influences of gender and educational level and bring about similar conflict resolution styles across demographic groups. This highlights the importance of looking more closely at contextual and institutional determinants of conflict behaviour in healthcare organizations, particularly the influence of leadership structure and support systems on employee behaviour.
Implications for practice and future research
The findings have practical implications for policymakers and healthcare administrators. Since the most common approach to resolving conflict was collaboration, institutions should promote team-based training and workshops on collaborative communication improvement, leadership, and emotional intelligence among nurses. Resolving the main causes of conflict e.g., injustice by nurse managers, expectations of patients, and workload disparities can increase job satisfaction, collaboration, and overall patient care quality.
Future studies should seek to conduct multi-centre studies with larger populations of studies in different geopolitical settings of Nigeria for maximum generalizability. Longitudinal studies may also be helpful in identifying changes in conflict resolution patterns over time. Qualitative studies exploring nurses' lived experiences of workplace conflict can also help in understanding factors involved and aid in devising context-specific interventions.
CONCLUSION
The study concludes that the major factors causing conflict among nurses are injustice from some nurse managers, unreasonable patient and relative expectation, unequal workload and lack of respect from other health professionals, delay of the doctor to calls in emergency cases, imbalance nurse-patient ratio, and distrust. Collaboration was discovered to be the main method of conflict resolution utilized by nurses in Sacred Heart Hospital, Lantoro, irrespective of their socio-demographic status of gender and level of education. However, cadre of the nurses influenced method of conflict resolution used.
Limitations
This study was limited to a single hospital, which may affect the generalizability of the findings. The sample size was relatively small, and data collection relied on self-reported responses, which may introduce bias. Future studies should include larger, multi-centre samples for broader applicability.
Funding statement
This research did not receive any specific grant from funding agencies in the public, commercial, or not for profit sectors.
Conflict of interest
The authors report no conflict of interest.
Authors’ contribution
- Oseni Rukayat: Conceptualized idea and conducted full research.
- Ekpoanwan Esienumoh: assisted with the design of questionnaire and conducting interviews with the selected nurses.
- Fakeye Grace: Was responsible for literature reviews
- Emmanson Emmanson: performed data analysis and edited the manuscript for publication.
Acknowledgements
We sincerely appreciate the management and nursing staff of Sacred Heart Hospital, Lantoro, for their support. Special thanks to our academic institutions, mentors, and colleagues for their guidance. We also acknowledge our families and friends for their unwavering encouragement throughout this research. Thank youall.
REFERENCES
- Adeyemi, B. S. and Aigbavboa, C. O. (2022). An Exploratory Factor Analysis for Conflict Resolution Methods among Construction Professionals. MDPI. Vol. 12(6). .
- Akpabio I. I., John M. E., Akpan M. I., Akpabio F. A. and Uyanah D. A. (2015). Work-related Conflict and Nurses’ role performance in a tertiary hospital in South-south Nigeria. Journal of Nursing Education and Practice, 6(2). . Accessed 27/10/2022.
- Awan, A. R. and Saeed S. (2015). Conflict Management and Organizational Performance: A case Study of Askari Bank Ltd. Research Journal of Finance and Accounting, 6(11), . Accessed 24/04/2022.
- Birkhoff J. (2015). Gender, Conflict and Conflict Resolution. . Accessed 17/10/2022
- Mukeshimana M. and Asingzwe D. (2016). Nurse-Doctor Relationship in Rwanda: A Questionnaire Survey. IOSR Journal of Nursing and Health Science.. Accessed 12/09/2022.
- Ogbonnaya, G. U., Ukaegbu, A. U., Aguwa, E., and Emma-Ukaegbu, U. A study on workplace violence against health workers in a Nigerian tertiary hospital. . Accessed 22/01/2023.
- Olajide, A. T., Asuzu M.C, and Obembe T.A. (2015). Doctor-Nurse Conflict in Njgerian Hospitals: Causes and Modes of expression. Journal of Advances in Medicine and Medical Research. VOL. 9(10). . Accessed 04/06/2021.
- Oresanjo, N. O. (2015). Conflict Management in School Organization in Nigeria. International Journal of Development and Management Review. V10(1). https://www.ajol.info>ijdmr>article>view.pdf. Accessed 17/10/2021.
- Pitsillidou, M. , Farmakas, A., Noula, M., and Roupa, Z. (2018). Conflict Management among health Professionals in hospitals in Cyprus. Journal of Nursing Management, 26(3-4). . Accessed on 24/04/2022.
- Rahim, M. A. (1983). Measurement of Organizational Conflict. The Journal of General Psychology, 109(2), 189-199.
- Ronquillo, Y. , Ellis, V. L, &Toney-Butler, T. J. (2023). Conflict Management. National Library of Medicine. ncbi.nlm.nih.gov/books/NBK4704321/
- Ronquillo, Y. , Ellis, V. L., &Toney-Butler, T. J. (2025). Conflict Management. In StatPearls. StatPearls Publishing. Retrieved from https://www.ncbi.nlm.nih.gov/books/NBK470432/
- Smiley, F. (2010). Leadership Guide to Conflict and Conflict Management. . Accessed 24/04/2022.
![]() This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
Biocontainment Transfer: A structured nursing model for enhancing patient care
Federico D’Urso 1*, Salvatore Trifiletti 2, Edoardo Falcone 1, Mara Gracy Basile 1, Ulrico Angeloni 1
1. Public Health Unit, Italian Red Cross – National Headquarters, 00151, Rome, Italy
2. Department of Medical, Surgical Sciences and Advanced Technologies “G. F. Ingrassia”, University of Catania, 95125, Catania, Italy.
* Corresponding author: Federico D’Urso, Public Health Unit, Italian Red Cross – National Headquarters, 00151, Rome, Italy. E-mail: federico.durso@gmail.com
Cite this article
ABSTRACT
Introduction: Biocontainment transfer represents a complex and delicate phase of care, especially in light of the increased demand for safe handling of patients affected by highly transmissible diseases. The COVID-19 pandemic has highlighted the critical need for structured approaches to ensure quality care and safety during these transfers.
Objective: To propose a structured nursing model for managing the care of conscious and communicative patients undergoing biocontainment transport, based on nursing diagnoses and standardized interventions.
Methods: A theoretical-conceptual model was developed based on the NANDA-I 2024–2026 taxonomy to identify nursing diagnoses related to perception, cognition, and stress tolerance. These were systematically combined with appropriate interventions from the Nursing Interventions Classification (NIC) and expected outcomes from the Nursing Outcomes Classification (NOC). The model addresses the clinical and psychological needs of patient across the three phases of transport: pre-transport, transport, and post-transport, with particular focus on anxiety management, communication, and adaptation to isolation.
Results: In the pre-transport phase, the diagnosis of Excessive Anxiety was addressed with interventions to reduce emotional distress and improve patient cooperation through clear, empathetic communication. During transport, the impairment of verbal communication caused by protective equipment and isolation barriers was mitigated through simplified language, visual aids, and strategies to ensure mutual understanding. In the post-transport phase, the model focused on enhancing the patient's coping capacity and resilience, offering emotional support and structured interventions to manage stress and process the experience.
Conclusions: The proposed model provides a comprehensive and systematic framework for nursing care during biocontainment transfers, integrating both clinical and emotional aspects to reduce patient vulnerability and improve the quality of care. As a theoretical model built upon standardized nursing taxonomies, it lays the groundwork for future clinical applications. Prospective and pilot studies will be essential to validate its effectiveness and feasibility in real-world healthcare settings.
Keywords: Biocontainment, Biocontainment patient transport, Nursing process, Clinical complexity, Advanced nursing practice.
INTRODUCTION
The current healthcare landscape has changed radically compared to a few years ago; the COVID-19 pandemic has highlighted structural and staffing shortages on a global scale [1,2]. The increase in the number of patients affected by highly transmissible diseases requiring high-intensity care has led to the widespread introduction of isolation devices that were once reserved for extremely rare situations. Biocontainment isolators have proven to be essential in the transport of these patients and typically include a protective plastic enclosure, a High Efficiency Particulate Air (HEPA) filter that removes harmful airborne particles, and a ventilation system that maintains a clean airflow at controlled pressure, preventing the escape of pathogens [2].
In the presence of diseases characterized by a high risk of mortality or a lack of appropriate preventive measures and effective treatments, the use of isolators becomes essential to ensure maximum safety for both the patient and healthcare personnel [1,3,4].
Preparing and managing the patient for a biocontainment transfer represents one of the most complex challenges for healthcare personnel, requiring protocols and technologies to guarantee both staff protection and the quality of patient care [2].
The use of biocontainment isolators can be compared to a form of physical restraint, as they impose an isolation measure that limits the patient's interaction with the external environment [5].
Although biocontainment isolators are essential for the safe transport of patients, their implementation presents significant logistical and organizational challenges that must be addressed [1,2].
Several studies have addressed the logistical and clinical challenges associated with the transport of patients in high-level containment. Gibbs et al. (2019) provide a comprehensive review of air medical evacuation protocols for biocontainment transport, focusing on technical and operational safety measures [1]. Similarly, Corradi et al. (2021) assess the public health implications of biocontainment systems used in ambulances, while D’Urso et al. (2024) describe possible care protocols for patients transferred using a biocontainment stretcher [2,6]. However, these contributions primarily emphasize technical configurations and infection control, without proposing a structured model of nursing care.
Studies investigating patient management within dedicated biocontainment units (e.g., Flinn et al., 2021) and during pandemic conditions Rehn et al., 2023 have highlighted the complexity of delivering safe care in isolation, yet they stop short of defining a standardized nursing process [3,7]. Other investigations have explored the communicative and emotional needs of patients in constrained settings. For example, the impact of personal protective equipment (PPE) on communication is well documented (Aengst et al., 2022; Saunders et al., 2021), and the relevance of augmentative and alternative communication (AAC) strategies in ICUs has been addressed by Costello (2000) and Zaylskie et al. (2024) [5,8-10]. Ten Hoorn et al. (2016) offer a systematic review on communication with mechanically ventilated patients, further supporting the need for dedicated relational strategies in high-complexity care [11].
While these studies help define the relational and contextual challenges of care in isolation, they do not translate into a structured, taxonomy-based model. Beam et al. (2010) and Swickard et al. (2014), for example, offer insights into the organization of biocontainment units and interfacility critical care transport, but without applying NANDA-I, NIC, or NOC frameworks [12,13].
This overview of the current literature confirms the absence of validated nursing care models specifically designed for conscious and communicative patients undergoing biocontainment transfers, thereby justifying the development of a structured approach grounded in standardized nursing taxonomies.
To fill this gap and address these challenges, the development of a structured nursing care model, based on targeted nursing diagnoses, is essential to guide clinical practice. Such a model can improve patient safety, enhance the quality of communication, and ensure continuity of care throughout the different phases biocontainment transfer process [6,7].
Objective and purpose
The aim of this study is to develop and propose an innovative structured nursing model designed to address both the clinical and psychological needs of conscious and communicative patients undergoing biocontainment transport. The model integrates standardized nursing diagnoses, interventions, and outcomes to enhance communication, reduce anxiety, and improve overall patient care across all phases of transport, laying the foundation for future clinical validation.
DEVELOPMENT OF THE CARE MODEL
Sampling and Eligibility
This study consists of a theoretical and methodological proposal for a structured care model for conscious and communicative patients without the actual collection of clinical data.
The model is designed for future applications in clinical practice and is intended to be validated in prospective studies involving real patients and healthcare teams.
Instruments
The care model is based on the integration of nursing diagnoses (NDs) from the NANDA-I 2024–2026 taxonomy and integrates elements from the NIC (Nursing Interventions Classification) and NOC (Nursing Outcomes Classification) systems. The selection of nursing diagnoses, interventions, and outcomes was informed by a narrative review of literature related to care in isolation, high-risk transport, and psychological support in confined environments. Due to the absence of specific scientific studies on biocontainment transfers, references from similar contexts were used. The process was further refined through structured consensus among the authors, all of whom have experience in emergency nursing and biocontainment patient management. To correctly select the appropriate NDs, an in-depth analysis was conducted of all thirteen domains included in the NANDA-I 2024–2026 classification. Some domains were excluded from consideration for the biocontainment transfer of conscious and communicative patients, as they were not relevant to the specific context. Domain 1 (Health Promotion) was excluded due to its focus on long-term behavioral patterns, domains 2 (Nutrition) and 3 (Elimination and Exchange) were not considered since they are not typically involved in short-term transfers and are managed in longer-duration ones. Domain 4 (Activity/Rest) was excluded because of its limited relevance during transport. Domains 6 (Self-Perception), 7 (Role Relationships), 8 (Sexuality) and 10 (Life Principles) were deemed not pertinent to biocontainment transfer. Furthermore, the domains 12 (Comfort) and 13 (Growth/Development) were excluded because they are not central in urgent care situations.
Domain 11 (Safety/Protection), although potentially relevant from a clinical standpoint, was excluded because it primarily focuses on physical risks such as infections or trauma. The typical patient considered is already in a similar condition; however, the main goal of the proposed model is instead to enhance the communicative, relational, and emotional dimensions of care through structured nursing interventions. Given these factors, the analysis focused on two specific domains the domain 5, (Perception/Cognition) with particular attention to cognitive understanding and communication and domain 9 (Coping/Stress Tolerance), which addresses psychological and emotional reactions. Within domain 5, only class 5 (Communication) was retained, as it includes diagnoses that are directly applicable to the needs of conscious patients experiencing communication difficulties due to the constraints of the biocontainment context, including the use of PPE. The other classes within this domain class 1 (Attention), 2 (Orientation) and 3 (Sensation/Perception), were excluded as they currently contain no NDs. Class 4 (Cognition) was also excluded, as it refers to cognitive deficits that require specific clinical and pharmacological management. In the case of a disoriented patient placed in a biocontainment isolator, such a condition would likely be exacerbated by the restrictive environment, making sedation the most appropriate and safe option for transport. Regarding domain 9, only class 2 (Emotional Responses) was included, as it encompasses diagnoses such as anxiety, ineffective coping, and stress responses, which are frequently observed in patients subjected to restrictive isolation. The remaining classes, 1 (Post-Trauma Responses) and 3 (Impulse Control), were excluded. In particular, class 1 was deliberately not considered, as the aim of the proposed model is to prevent the onset of post-traumatic stress symptoms related to the biocontainment transfer, by supporting the patient through structured interventions that reduce emotional overload and promote coping during the procedure. Based on this taxonomic analysis, the nursing care model was structured into three distinct phases, pre-transport, transport, and post-transport, each associated with specific nursing diagnoses, related interventions, and expected outcomes.
Pre-transport phase
The lack of knowledge about the biocontainment stretcher and the procedures to be carried out during the transfer generates, at this stage, significant emotional distress and anticipatory anxiety. The nursing diagnosis excessive anxiety (00400), classified under domain 9, class 2, was selected based on observations conducted in clinical practice, where behavioral and physiological signs such as agitation, increased heart rate, and verbal expressions of concern are commonly noted.
Other diagnoses within the same class, such as fear (00390) or impaired resilience (00210), were excluded because they involve long-term patterns or cannot be adequately documented within the limited timeframe of the transfer.
To address this diagnosis, the NIC interventions anxiety reduction (5820) and emotional support (5270) were selected, with the expected NOC outcome being anxiety Self-Control (1402). [14]
Since the goal of this care model is to promote coping, we preferred to use the NOC Anxiety Self-Control (1402), as it reflects the objective of enhancing the patient’s conscious management of anxiety.
The NOC Anxiety Level (1211) may be useful for an initial clinical assessment or for pre-post comparisons, but its purpose would remain limited to quantifying the symptom.
In this phase, it may be useful to conduct an initial assessment of the patient's anxiety level, followed by a second evaluation to measure the effectiveness of interventions, using a rapid-assessment tool such as the Generalized Anxiety Disorder-7 (GAD-7) scale [15,16].
Transport phase
The use of the biocontainment stretcher and PPE generates significant communication barriers between patients and healthcare professionals. Within domain 5, class 5 of the NANDA-I taxonomy, the diagnosis Readiness for Enhanced Communication (00185) was excluded, as it is focused on strengthening a communicative process that is already functioning. In this context, however, it is necessary to implement an alternative communication system to replace the traditional one, which is compromised by operational conditions.
Similarly, the diagnosis Risk for Impaired Verbal Communication (00434) was excluded because it refers to a susceptibility to communication impairment, whereas in the current scenario the impairment is already present.
The most consistent was found to be DN Impaired Verbal Communication (00051), which characterizes a limited or nonexistent capacity for verbal communication. [9,10]
The selected nursing interventions are Communication Enhancement: Speech Deficit (4976) chosen to facilitate effective information exchange through alternative communicative methods during the transport phase.
Communication (0902), the related NOC, enables the assessment of the efficacy of the patient-provider relationship in situations where communication is constrained.
Post-transport phase
In this phase, the patient faces the need for emotional recovery and coping support following the biocontainment transfer, the DNs Readiness for Enhanced Coping (00158), classified under domain 9, class 2, was selected, as it reflects the patient’s willingness and potential to strengthen adaptive strategies in response to an acute stress situation [14,16].
This choice is based on the authors’ clinical observations in most cases; conscious and cooperative patients exhibit transient emotional discomfort that can be interpreted as a normal physiological response to stress rather than a failure of their coping abilities. Consequently, diagnoses such as Ineffective Coping (00069) were excluded, as they would imply a dysfunction in stress management and risk labeling a temporary and reactive experience as a psychological disorder.
The care objective is not the treatment of a psychological condition, but rather the enhancement of the patient’s existing personal resources by fostering resilience and facilitating the emotional processing of the experience through structured interventions.
In line with this approach, several standardized nursing interventions (NIC) were selected to support the patient’s adaptation and increase their stress management capacity. Among them, Coping Enhancement (5230) represents the core intervention aimed at promoting an adaptive response to the experience.
These are supported by Emotional Support (5270) which is essential for normalizing emotional reactions, containing residual anxiety, and facilitating emotional rebalancing.
Relational interventions such as Active Listening (NIC 4920) and Counseling (NIC 5240) complete the care plan by allowing for deeper processing of the experience and fostering continuity in the nurse–patient relationship beyond the acute phase.
The expected outcomes identified are Coping (NOC 1302), Personal Resiliency (NOC 1309) and Anxiety control (NOC 1402) as they allow for the systematic evaluation of the patient’s adaptive process and the effectiveness of the nursing support provided during the recovery phase.
To assess coping strategies, the Brief COPE Inventory scale may be used, [17] while the Connor-Davidson Resilience Scale (CD-RISC), including the short form (CD-RISC-10), could be adopted to measure the ability to recover from adverse events, potentially establishing a proper follow-up for the patient [18].
The effectiveness of the proposed nursing interventions can be evaluated through a combination of NOC indicators (e.g., Anxiety Self-Control, Communication, Coping), behavioral observations, and, when applicable, validated psychological scales such as the State-Trait Anxiety Inventory (STAI-Y) or Hospital Anxiety and Depression Scale (HADS) [19,20].
The model was developed through a review of literature from related care contexts (e.g., intensive care units, isolation wards) and the consensus among the authors, formed during recent the COVID-19 pandemic. These choices provide a foundation for guiding future empirical validation and pilot implementation.
Statistical Analysis
As this work presents a theoretical nursing care model and does not involve the collection of quantitative data, no statistical analysis was performed. Future prospective studies, involving structured data collection and patient outcomes measurement, will be necessary to validate the proposed model using appropriate statistical methods.
DESCRIPTION OF THE PROPOSED MODEL
In biocontainment transfers, three distinct phases of nursing care can be identified: the preparatory phase before transport (pre-transport), the transfer phase using the isolator (transport), and the final phase after transport (post-transport). Each phase presents specific care and assistance needs.
Before transport, the patient may experience excessive anxiety related to the procedures and the outcome of the transfer, also due to the visual impact of the isolator. Its limited space may cause a sense of claustrophobia, further intensifying the level of distress.
The observation of specific defining characteristics, such as behavioral/emotional signs like anguish, psychomotor agitation, and verbalized fears, as well as physiological signs like increased heart rate and blood pressure, facial flushing, and a trembling voice, suggests a state of disproportionate and persistent concern in response to perceived threats. Based on these elements, the most appropriate nursing diagnosis is Excessive Anxiety (00400), as it accurately reflects the patient’s distress, expressed through both emotional and behavioral signs and physical hyperactivation.
The primary goal becomes Anxiety Self-Control (NOC 1402), assessed through a reduction in agitation and increased patient cooperation. To achieve this, targeted interventions are necessary. Anxiety Reduction (NIC 5820) and Emotional Support (NIC 5270) are essential to create a reassuring environment and foster empathetic communication.
During biocontainment transport, the use of PPE and the isolator may create concrete communication barriers, [3,5,8] resulting in frustration or misunderstanding. This scenario corresponds to the diagnosis Impaired Verbal Communication (00051), characterized by limited or absent ability to receive, process, transmit, and/or use a symbol system. The outcome to be achieved is Communication (NOC 0902).
The intervention plan includes a key nursing intervention, the Communication Enhancement: Speech Deficit (NIC 4976), which encourages the use of alternative communication channels (e.g., visual aids) and promotes the use of shared language, ensuring mutual understanding.
Concrete examples include:
Use of visual aids such as augmentative and alternative communication (AAC) boards, [9] shared with the patient during the pre-transport phase, or tablets/whiteboards to facilitate needs expression.
Active listening techniques: maintaining eye contact, nodding, asking clarifying questions, allowing time for patient responses [11].
Frequent comprehension checks: asking the patient to repeat or rephrase the information received to confirm understanding.
By implementing these strategies, nurses support patients in overcoming communication barriers related to PPE, isolators, and other devices, maintaining an effective and safe level of interaction.
In the post-transport phase, the need to strengthen coping strategies becomes particularly evident when the patient shows difficulty processing the experience or managing stress from isolation. In this context, the diagnosis Readiness for Enhanced Coping (00158) describes the possibility of reinforcing cognitive and/or behavioral efforts to deal with distressing situations.
The expected outcomes (NOC) include Coping (1302), Personal Resiliency (1309), and Anxiety Self-Control (1402). The aim is to increase the patient’s ability to manage stressful events, [21] show flexibility in new circumstances, and limit agitation or irritability.
Several key interventions (NIC) support this goal:
Coping Enhancement (5230), which encourages identification of existing strategies and discovery of additional resources (e.g., family support via video call, mindfulness techniques) [14].
Emotional Support (5270), offering empathetic listening and normalization of stress reactions [22].
Active Listening (4920) and Counseling (5240), which aid in processing the experience, reduce frustration, and foster patient cooperation [22-24].
Counseling (5240) supports the patient in processing emotional distress by fostering a trusting, empathetic relationship. It helps the patient identify sources of discomfort, express concerns, and explore adaptive coping strategies, thereby enhancing self-awareness and emotional stability after the transfer process [18,22].
PhaseDiagnosis (Code)DomainClass
| Phase | Diagnosis (Code) | Domain | Class | NIC | NOC |
| Pre-transport | Excessive Anxiety (00400) | 9 | 2 | Anxiety Reduction (NIC 5820) | Anxiety Self-Control (NOC 1402) |
| Emotional Support (NIC 5270) | |||||
| Transport | Impaired Verbal Communication (00051) | 5 | 5 | Communication Enhancement: Speech Deficit (NIC 4976) | Communication (NOC 0902) |
| Post-transport | Readiness for Enhanced Coping (00158) | 9 | 2 | Coping Enhancement (NIC 5230) | Coping (NOC 1302) Personal Resiliency (NOC 1309) Anxiety Self-Control (NOC 1402) |
| Emotional Support (NIC 5270) | |||||
| Active Listening (NIC 4920) | |||||
| Counseling (NIC 5240) |
Table 1. Association between the phases of biocontainment transport and the related elements of the nursing process.
Table 2 illustrates the functionality and operational implementation of the proposed model across the three phases of biocontainment transfer. That table presents a structured fictitious clinical case; for each phase, it describes a generic patient scenario along with the corresponding nursing interventions. This approach aims to exemplify how the theoretical model can be translated into clinical practice, promoting its reproducibility and applicability in high-complexity care settings.
| Phase | Fictitious Case Description | Practical Nursing Interventions |
| Pre-transport | A conscious and oriented adult patient is informed of an imminent transfer toward the radiology department using a biocontainment stretcher. Upon seeing the isolator, the patient becomes visibly agitated, expresses fear, and shows signs of anxiety (e.g., flushed face, tachycardia). | • Apply Anxiety Reduction (NIC 5820) • Use Emotional Support (NIC 5270) • Perform a rapid anxiety screening (GAD-7) • Introduce the AAC board |
| Transport | During transfer, communication is significantly impaired due to PPE and physical barriers. |
|
| Post-transport | After reaching the destination, the patient expresses emotional exhaustion and stress. |
|
Table 2. Fictitious clinical case illustrating nursing interventions across the phases of biocontainment transport.

Figure 1. Conceptual flowchart illustrating nursing diagnoses, interventions (NIC), outcomes (NOC), assessment tools and practical applications across the phases of biocontainment transport.
DISCUSSION
The aim of this study is to develop and propose an innovative structured nursing model designed to address both the clinical and psychological needs of conscious and communicative patients undergoing biocontainment transport. As mentioned in the introduction, most of the literature currently published focuses on the organizational, logistical and technological aspects of the transfer to biocontainment rather than offering organized and systematic nursing care models. Since it incorporates nursing diagnoses, interventions, and expected outcomes based on the NANDA-I, NIC, and NOC taxonomies, the model offered here represents an original contribution in this context. It provides a theoretical and practical approach focused on the psychological, communicative, and relational needs of conscious and communicative patients throughout the entire transfer process. This model is a novel idea that can be validated and applied in high-complexity care settings because of its attention to care detail, taxonomic clarity, and clinical application. The structured model developed highlights how each phase of biocontainment transfer presents specific and distinct care needs. The systematic approach to managing pre-transfer anxiety, maintaining effective communication during transport, and providing psychological support after transfer underscores the need for personalized and coordinated interventions.
The integration of nursing diagnoses, NOC outcomes, and NIC interventions enables the construction of a comprehensive care response that addresses not only clinical aspects but also emotional and relational dimensions.
The impact of biocontainment on patient-provider communication is particularly significant [3,5].
The use of PPE and isolating devices presents real obstacles and requires well-planned alternative strategies to prevent further emotional deterioration.
Finally, the post-transport phase is often underestimated but can be a critical moment for the patient to process the experience. Strengthening coping skills and promoting resilience not only improve clinical outcomes but also enhance the patient’s overall care experience [21].
Limitation
This theoretical nursing care model was developed through the integration of taxonomy and expert consensus, without direct patient involvement.
The implementation and effectiveness in real clinical settings have not yet been evaluated; future studies should be structured to assess the outcomes related to its application through quantitative measurements and subsequent evaluations in biocontainment transfer settings.
Such investigations will be essential to refine the model and confirm its clinical relevance and utility.
The proposed nursing care model can be practically applied in various high-complexity clinical settings, such as infectious disease units, intensive care units, and specialized medical transport services for highly infectious patients.
To validate the model’s effectiveness, the systematic collection of clinical data before and after the biocontainment transfer is recommended. Among the possible assessment tools, the GAD-7 scale may be used for anxiety, the Brief COPE Inventory for coping strategies, and the CD-RISC-10 for resilience levels. In cases of limited verbal communication, the use of structured observational checklists and AAC (Augmentative and Alternative Communication) tools can provide reliable alternative measurements.
The analysis of collected data may include descriptive statistics and inferential tests to compare pre- and post-intervention conditions. These strategies will allow for measuring the model’s impact on key care outcomes and refining its applicability for potential structured implementation in the future.
CONCLUSIONS
The management of patients in biocontainment requires a strategic combination of clinical and communication skills to address the nursing diagnoses that emerge throughout the three phases of transfer. By applying structured care models, it is possible to improve clinical outcomes, reduce biological risks, and ensure effective communication even in extreme isolation conditions. The integration of protocols and nursing interventions provides an effective solution to the demands of complex and highly specialized care. Although the efficiency of the suggested model has not yet been confirmed in practical situations, it constitutes a substantial theoretical advance to the nursing management of biocontainment transfers. In order to confirm its practical application and quantify its observable advantages on important care outcomes, pilot projects and prospective studies should be started and carried out in real care situations. The model's robustness can only be verified and its organized adoption encouraged by means of rigorous testing
Ethical Approval
For this study, no formal approval from the Local Ethics Committee was required.
Conflicts of Interest and Funding Sources
The authors declare that they have no conflicts of interest related to this work. The study received no financial support from public or private entities, including pharmaceutical or industrial companies.
Authors’ Contributions
Federico D’Urso: conceived the study, developed the care model, and coordinated the writing of the manuscript. Salvatore Trifiletti: contributed to the organization of the NANDA-I, NIC, and NOC framework. Edoardo Falcone: participated in literature review and content refinement. Mara Gracy Basile: contributed to methodological structure and theoretical validation. Ulrico Angeloni: revised and validated the entire study and ensured its clinical and theoretical consistency. All authors read and approved the final version of the manuscript.
Acknowledgments
The authors would like to thank the staff of the Italian Red Cross – Public Health Department for their continuous support and collaboration in developing the proposed model. Special thanks also to the academic community for the critical reflection that inspired the elaboration of this work.
REFERENCES
Gibbs, S. G., Herstein, J. J., Le, A. B., Beam, E. L., Cieslak, T. J., Lawler, J. V., Santarpia, J. L., Stentz, T. L., Kopocis-Herstein, K. R., Achutan, C., Carter, G. W., & Lowe, J. J. (2019). Review of Literature for Air Medical Evacuation High-Level Containment Transport. Air medical journal, 38(5), 359–365. HYPERLINK "https://doi.org/10.1016/j.amj.2019.06.006"https://doi.org/10.1016/j.amj.2019.06.006
D’Urso, F., Meroni, L., Rech, R., Musumeci, A., Bonini, A., Piotti, C., Ciriaci, A. and Menghini, S. (2024) “Possible care protocols for patients undergoing road transfer on a biocontainment stretcher model N 36 (36 m3 air ˃60 ACH)”, Emergency Care Journal, 20(3). doi: 10.4081/ecj.2024.12334.
Rehn, M., Heyerdahl, F., Osbakk, S. A., Andresen, Å. E., & Hagemo, J. (2023). Challenges and Risks in Out-of-Hospital Transport of Patients During the Coronavirus Disease 2019 Pandemic. Air medical journal, 42(3), 191–195. HYPERLINK "https://doi.org/10.1016/j.amj.2023.02.002"https://doi.org/10.1016/j.amj.2023.02.002
Garibaldi, B. T., Conger, N. G., Withers, M. R., Hatfill, S. J., Gutierrez-Nunez, J. J., & Christopher, G. W. (2019). Aeromedical Evacuation of Patients with Contagious Infections. Aeromedical Evacuation: Management of Acute and Stabilized Patients, 317–335. HYPERLINK "https://doi.org/10.1007/978-3-030-15903-0_20"https://doi.org/10.1007/978-3-030-15903-0_20
Aengst, J., Walker-Stevenson, G., Harrod, T., Ivankovic, J., Neilson, J., & Guise, J. M. (2022). Uncomfortable yet necessary: The impact of PPE on communication in emergency medicine. International journal for quality in health care: journal of the International Society for Quality in Health Care, 34(4), mzac095. HYPERLINK "https://doi.org/10.1093/intqhc/mzac095"https://doi.org/10.1093/intqhc/mzac095
Corradi, M., Cattaneo, A., Plicco, C., & Bossi, E. (2021). HTA of novel biocontainment systems for ambulance transport: public health implications. The European Journal of Public Health, 31(Suppl 3), ckab165.132. HYPERLINK "https://doi.org/10.1093/eurpub/ckab165.132"https://doi.org/10.1093/eurpub/ckab165.132
Flinn, J. B., Hynes, N. A., Sauer, L. M., Maragakis, L. L., & Garibaldi, B. T. (2021). The role of dedicated biocontainment patient care units in preparing for COVID-19 and other infectious disease outbreaks. Infection control and hospital epidemiology, 42(2), 208–211. HYPERLINK "https://doi.org/10.1017/ice.2020.451"https://doi.org/10.1017/ice.2020.451
Saunders, G. H., Jackson, I. R., & Visram, A. S. (2021). Impacts of face coverings on communication: an indirect impact of COVID-19. International journal of audiology, 60(7), 495–506. HYPERLINK "https://doi.org/10.1080/14992027.2020.1851401"https://doi.org/10.1080/14992027.2020.1851401
Costello, J.M. (2000). AAC intervention in the intensive care unit: The children's hospital Boston model. Augmentative and Alternative Communication, 16, 137 - 153.
Zaylskie, L. E., Biggs, E. E., Minchin, K. J., & Abel, Z. K. (2024). Nurse perspectives on supporting children and youth who use augmentative and alternative communication (AAC) in the pediatric intensive care unit. Augmentative and alternative communication (Baltimore, Md.: 1985), 40(4), 255–266. HYPERLINK "https://doi.org/10.1080/07434618.2023.2284269"https://doi.org/10.1080/07434618.2023.2284269
Ten Hoorn, S., Elbers, P. W., Girbes, A. R., & Tuinman, P. R. (2016). Communicating with conscious and mechanically ventilated critically ill patients: a systematic review. Critical care (London, England), 20(1), 333. HYPERLINK "https://doi.org/10.1186/s13054-016-1483-2"https://doi.org/10.1186/s13054-016-1483-2
Beam, E.L., Boulter, K.C., Freihaut, F., Schwedhelm, S. and Smith, P.W. (2010), The Nebraska Experience in Biocontainment Patient Care. Public Health Nursing, 27: 140-147. HYPERLINK "https://doi.org/10.1111/j.1525-1446.2010.00837.x"https://doi.org/10.1111/j.1525-1446.2010.00837.x
Swickard, S., Swickard, W., Reimer, A., Lindell, D., & Winkelman, C. (2014) Adaptation of the AACN Synergy Model for Patient Care to Critical Care Transport. Crit Care Nurse, 34(1),16–28. doi: 10.4037/ccn2014573.
Sánchez-Almagro, C. P., Romero-Sánchez, J. M., White-Ríos, M., González Del Pino, C. A., & Paloma-Castro, O. (2022). NANDA International nursing diagnoses in the coping/stress tolerance domain and their linkages to Nursing Outcomes Classification outcomes and Nursing Interventions Classification interventions in the pre-hospital emergency care. Journal of advanced nursing, 78(10), 3273–3289. HYPERLINK "https://doi.org/10.1111/jan.15280"https://doi.org/10.1111/jan.15280
Villarreal-Zegarra, D., Paredes-Angeles, R., Mayo-Puchoc, N. et al. Psychometric properties of the GAD-7 (General Anxiety Disorder-7): a cross-sectional study of the Peruvian general population. BMC Psychol 12, 183 (2024). https://doi.org/10.1186/s40359-024-01688-8
Ganesan S, Balasubramanian B, Krishnamurthy P, Govindan R, Mani N. Effects of Tele-Counseling on Reducing Anxiety Levels of COVID-19 Patients in Isolation Wards: An Observational Study. Indian Journal of Psychological Medicine. 2022;45(1):43-46. doi:10.1177/02537176221139598
Solberg, M. A., Gridley, M. K., & Peters, R. M. (2022). The Factor Structure of the Brief Cope: A Systematic Review. Western journal of nursing research, 44(6), 612–627. HYPERLINK "https://doi.org/10.1177/01939459211012044"https://doi.org/10.1177/01939459211012044
Kuiper, H., van Leeuwen, C. C. M., Stolwijk-Swüste, J. M., & Post, M. W. M. (2019). Measuring resilience with the Connor-Davidson Resilience Scale (CD-RISC): which version to choose?. Spinal cord, 57(5), 360–366. HYPERLINK "https://doi.org/10.1038/s41393-019-0240-1"https://doi.org/10.1038/s41393-019-0240-1
Dias, P., Clerc, D., da Rocha Rodrigues, M. G., Demartines, N., Grass, F., & Hübner, M. (2022). Impact of an Operating Room Nurse Preoperative Dialogue on Anxiety, Satisfaction and Early Postoperative Outcomes in Patients Undergoing Major Visceral Surgery-A Single Center, Open-Label, Randomized Controlled Trial. Journal of clinical medicine, 11(7), 1895. HYPERLINK "https://doi.org/10.3390/jcm11071895"https://doi.org/10.3390/jcm11071895
Haugan, G., & Drageset, J. (2014). The hospital anxiety and depression scale--dimensionality, reliability and construct validity among cognitively intact nursing home patients. Journal of affective disorders, 165, 8–15. https://doi.org/10.1016/j.jad.2014.04.042
Ocloo, J., Garfield, S., Franklin, B. D., & Dawson, S. (2021). Exploring the theory, barriers and enablers for patient and public involvement across health, social care and patient safety: a systematic review of reviews. Health research policy and systems, 19(1), 8. HYPERLINK "https://doi.org/10.1186/s12961-020-00644-3"https://doi.org/10.1186/s12961-020-00644-3
Madl, J. E. M., Sturmbauer, S. C., Janka, R., Bay, S., & Rohleder, N. (2022). Preparing patients according to their individual coping style improves patient experience of magnetic resonance imaging. Journal of behavioral medicine, 45(6), 841–854. HYPERLINK "https://doi.org/10.1007/s10865-022-00361-y"https://doi.org/10.1007/s10865-022-00361-y
Wallace L. M. (1986). Communication variables in the design of pre-surgical preparatory information. The British journal of clinical psychology, 25 (Pt 2), 111–118. HYPERLINK "https://doi.org/10.1111/j.2044-8260.1986.tb00679.x"https://doi.org/10.1111/j.2044-8260.1986.tb00679.x
Caddick, J., Jawad, S., Southern, S., & Majumder, S. (2012). The power of words: sources of anxiety in patients undergoing local anaesthetic plastic surgery. Annals of the Royal College of Surgeons of England, 94(2), 94–98. HYPERLINK "https://doi.org/10.1308/003588412X13171221501267"https://doi.org/10.1308/003588412X13171221501267
![]() This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
FINGER VERSUS FOREHEAD PULSE OXIMETRY IN LITERATURE: A NARRATIVE REVIEW
Rita Citarella 1*, Carmine Sammartino 2, Aniello Lanzuise 3, Marco Abagnale 4
1 Department of Surgery and Anesthesia, “Umberto I” Hospital of Nocera Inferiore”, 84014, Salerno, Italy.
2 Department of Kidney Transplantation, “San Giovanni di Dio e Ruggi d’Aragona” Hospital, 84131, Salerno, Italy.
3 Corporate Health Management, "Ospedale dei Colli",80131, Napoli, Italy.
4 Department of Critical Care, M. Scarlato Hospital, 84018, Scafati, Salerno, Italy.
*Corresponding author: Rita Citarella, Department of Surgery and Anesthesia at Umberto I Hospital o fNocera Inferiore, 84014 Salerno, Italy. E-mail: rita.citarella.91@gmail.com
Cite this article
ABSTRACT
Introduction: Pulse oximetry is a technology for monitoring oxygen saturation (SpO2) in various clinical settings.However, measurement of SpO2 value can have different accuracy depending on some factors such as the sensor placement (on the finger or on the head). This narrative review was conducted to synthetize the better evidence to compare finger and forehead pulse oximetry in patients requiring Sp02 monitoring, in order to identify which method was the most effective for nursing practice.
Objective: to describe the potential effectiveness of pulse oximetry saturation measurement using finger sensors versus forehead sensors, focusing exclusively on their reliability in various clinical conditions. This analysis aims to identify the most accurate method for SpO2 monitoring in nursing practice, particularly when addressing challenges related to peripheral perfusion and motion artifacts.
Materials and Methods: A narrative review was conducted through the PubMed and CINAHL databases, the selected articles had to answer the following research questions: “Which sensor placement, finger or forehead, is most effective for measuring oxygen saturation (SpO2) in patients with compromised peripheral perfusion?”; and “Between finger pulse oximetry and forehead pulse oximetry, which is considered the gold standard for accurate SpO2 measurement? “
Results: Four studies were selected. The selected studies show that forehead sensors provide more reliable and accurate measurements, especially under adverse conditions, due to their resistance to peripheral vasoconstriction and motion artifacts. Finger sensors, while widely used, exhibit limitations in physiologically stressful situations.
Conclusions: The finger pulse oximetry remains the standard in most scenarios, but forehead sensors may provide more reliable readings in critically ill patients with compromised peripheral perfusion.
Keywords: oxygen saturation, pulse oximetry, finger sensor, forehead sensor, digit sensor, narrative review.
INTRODUCTION
Pulse oximetry is often described as the fifth vital sign[1]; it represents a rapid, non-invasive method to measure peripheral capillary oxygen saturation (SpO2) in the blood by directing light of specific wavelengths through tissue, typically at the fingernail bed. The “SpO2” value provided by the pulse oximeter reflects the percentage of oxygenated hemoglobin in the blood.[2].The “S” stands for saturation, “p” indicates that it is measured peripherally (rather than from arterial blood) and “O2” represents the oxygen. Deoxygenated and oxygenated hemoglobin absorb light differently, at wavelengths of 660 nm and 940 nm, respectively. The light absorption data isanalyzedby a proprietary algorithm within the pulse oximeter to produce a saturation value [3]. This non-invasive technique, revolutionized patient monitoring by allowing continuous and immediate assessment of oxygenation status, which was previously possible only through invasive methods such as arterial blood gas analysis[4]. Fingernail and forehead are the most common application sites [5]. In this review, we focused our attention on the two most common application sites, finger and fore ahead, in order toassess which of these two methods is better in terms of sensibility (also in patients under impaired clinical conditions). The decision to focus exclusively on finger and forehead sites for oxygen saturation monitoring was driven by their proven reliability in both routine and critically adverse conditions, as supported by existing evidence. These locations were selected based on their widespread use in clinical practice and their relevance to nursing competencies, ensuring standardized and effective monitoring for patients.Existing studies highlight that both finger and forehead sensors outperform other alternative sites such as the earlobe or chest. While earlobe pulse oximetry is sometimes used, it has not consistently demonstrated superior reliability compared to the finger or forehead in diverse clinical scenarios, limiting its integration into evidence-based nursing protocols.[6] Pulse oximeter probes typically consist of two light emitters and a detector, which either receives light transmitted through the tissue or detects light reflected from a site like the forehead [7]. These probes are available in disposable adhesive or reusable clip designs, catering to different clinical needs. At sea level, normal oxygen saturation ranges from 96% to 100%, while individuals living at higher altitudes may have slightly lower saturation levels due to reduced atmospheric oxygen[8].Pulse oximeters are calibrated for saturation levels between 70% and 100%, with an accuracy of 2% to 4%[9]. It is important to note that various factors can influence pulse oximeter readings. For instance, colder temperatures may reduce accuracy; so, maintaining a temperature near 33°C (91.4°F) is recommended for reliable measurements. External factors (such as black or blue nail polish and artificial nails) can also interfere with readings. [10] If these obstructions cause inaccuracies, repositioning the sensor sideways on the finger bed has shown some success, though this placement falls outside the sensor's calibration parameters.However, measurement of SpO2 value can have different accuracy depending on some factors such as the sensor placement (on the finger or onthe head).[11]Monitoring oxygen saturation requires precision, and nursing professionals are extensively trained to apply and interpret results from sensors placed on the finger and forehead[12].These sites allow for continuous assessment while ensuring patient comfort and minimizing interference during routine care activities. The inclusion of additional sites could lead to inconsistencies in application and monitoring outcomes, complicating care delivery without providing significant advantages[13].By focusing on finger and forehead sites, the review aligns with clinical guidelines and promotes uniformity in practice, facilitating clearer communication and collaboration among healthcare teams.
PURPOSE
The purpose of this narrative review was to describe the potential effectiveness of pulse oximetry saturation measurement using finger sensors versus forehead sensors, focusing exclusively on their reliability in various clinical conditions.This analysis aims to identify the most accurate method for SpO2 monitoring in nursing practice, particularly when addressing challenges related to peripheral perfusion and motion artifacts.
MATERIALS AND METHODS
A comprehensive bibliographic search was conducted on PubMed (via MEDLINE), CINAHL (via EBSCO), in April 2024
Search strategy and keywords used
A narrative review of the literature [14] was conducted following the methodology reported in the ‘Scale for the Assessment of Narrative Review Articles’ (SANRA) [15].The following research question was formulated:
Which sensor, on the finger or forehead, is more reliable and accurate for measuring oxygen saturation (SpO2) in patients with compromised peripheral perfusion?”;
To conduct the literature search, a research question was previously outlined using the P.I.C.O. framework, which stands for population, intervention, comparison and outcomes (Table 1).
|
POPULATION |
PATIENTS REQUIRING SPO2 SATURATION MONITORING |
|
INTERVENTION |
FINGER PULSE OXIMETRY |
|
COMPARISON |
SENSORS FOREHEAD PULSE OXIMETRY |
|
OUTCOME |
ACCURACY AND RELIABILITY OF SpO2 READINGS |
Table 1. The PICO methodology assessment
The search strategy included combinations and synonyms of free text and MESH (medical subject headings) terms, usingthe Boolean operators “AND” and “OR” to interconnect the following keywords:oxygen saturation, pulse oximetry, finger sensor, forehead sensor, digit sensor, SpO2 accuracy, low peripheral perfusion conditions.To identify additional studies, we also examined the reference lists of retrieved articles.
Inclusion and Exclusion criteria
Studies that responded to the hypotheses of bibliographic research were considered. Primary studies, systematic reviews and guidelines were included. The inclusion criteria used for the selection of articles were: 1) human population including both males and females, 2) studies in English language, 3) available abstract and 4) publications of the last 10 years. Articles of national and international scientific literature whose title and content contained at least one of the keywords or a link to them are included.All those quotes for which it was not possible to find the written “full text” version were excluded.The results obtained were analyzed by C.R and A.M. independently, by title and abstract, to identify relevant articles.The selected studies were found in full text format, read critically and the relevant ones were included in the review.
RESULTS
The bibliographic search revealed 72 references, of which 22 in CINAHL Complete and 50 in PubMed.Two references were excluded at the beginning because they were double.After a selection by reading the title and abstract, 54articles were excluded,.The main reasons for exclusion included: lack of relevance to the research questions (for example studies not comparing finger vs forehead sensor), use of pediatric or animal populations, absence of full text, publication date older than 10 years, and articles not written in English.The articles initially included were 16full text articles. The results were analyzed by C.R. and A.M. independently and read critically; of the 16remaining papers4 were included, respectively: 3 articles in PubMed and 1 article in CINAHL Complete.After full-text reading, 12 articles were excluded for the following reasons:6 did not meet the inclusion criteria regarding a direct comparison between finger and forehead sensors or did not report clinically relevant data on SpO₂ accuracy or reliability;3 used outdated technologies not aligned with current clinical standards;2 lacked the quantitative data necessary for outcome analysis; and 1 was a narrative review without original research data.
Selected studies
The following table reports the included studies, describing their features: year of publication, name of authors, aim, methodology, study sample, their results and outcome measures(Table 2); 4 articles were identified, published between 2015 and 2025, with different methodology as follows: one prospective study and three observational studies.
|
YEAR |
AUTHORS |
AIM |
STUDY DESIGN |
SAMPLE |
RESULTS |
OUTCOME MEASURES |
|
2018 [ 16] |
Seifi S. et al. |
To Determine which placement of pulse oximetry sensors (finger, forehead, ear or toe) provides the most accurate measurements vs ABG to in intensive care unit patients. |
Prospective observational study |
50 pts admitted to the intensive care unit following coronary artery bypass surgery. |
FoSpo02 was the ↑. Finger and toe sensors showed > variability, especially in case of low peripheral perfusion conditions. |
Accuracy vs ABG, variability |
|
2020 [17] |
Kelly KL et al. |
To compare performance of pulse oximetry sensors on the finger and forehead during MXT in patients with heart failure. |
Observational study. |
40 pts |
FoSpo02 ↑ during intense exercise. |
Reliable, signal stability, response time |
|
2022 [18] |
Robertson L et al. |
To assess the accuracy, reliability and signal quality of pulse oximetry sensor placed on the forehead and finger during the 6-MWT, using CBG as the clinical reference. |
Observational study. |
80 pts with pulmonary vascular disease. |
FoSp02 is ↑ to the FiSp02. However, both sensors showed < accuracy in patients with significant desaturation (< 80% SpO2). |
Signal quality, reliable, accuracy vs CBG , sensor riability |
|
2024 [19] |
Lynggaard A. et al |
To evaluate the reliability of SpO2 measurements from sensors placed on the finger, forehead, and ear during the 6-MWT in patients with systemic sclerosis. |
Observational study. |
82 pts |
FoSp02 is ↑ to the FiSp02. FoSp02 showed < accuracy in patients with vascular complications |
Signal quality, accuracy, reliable |
Table Legend: pts= patients,FiSp02= finger sensor, FoSpo02= forehead sensor,ABG= arterial blood gas,> = major, < = minor,CBG= capillary blood gas,↑=more reliable,6-MWT=6- Minute Walking Test,MXT=maximal exercise testing
Table 2. Analysis of selected studies
The first study, conducted in Iran [16], compared four sensor placements using arterial blood gas as a reference. The results showed that the forehead sensor had the highest accuracy, particularly in patients with low peripheral perfusion, while finger ant toe sensors showed greater variability. The second study, conducted in the United Kingdom [17], assessed signal stability and response during maximal exercise in heart failure patients. It found that the forehead sensor provided more reliable readings, whereas the finger sensor tended to underestimate Sp02. The third study, from the Usa [18], involved patients with pulmonary vascular disease undergoing the 6- minute walk test. The study evaluated signal quality, accuracy vs capillary blood gas, and sensor reliability during desaturation episodes. The forehead sensor showed better signal consistency, although with a slight overestimation of Sp02, values below 80%. The fourth study, form Denmark [19], examined patients with systematics clerosis. It compared sensor placements in terms of error rate, signal dropouts, and inter -device agreement, showing the forehead sensor, outperformed the finger sensor, especially in patients with vascular complications.
Study description
According toSeifi’s study[16]comparing the different methods the forehead sensor was most accurate than the finger. Attention must be focused on low peripheral perfusion conditions; in effect, in these cases, finger and toe sensors showed higher variability, providing results that didn’t reflect the real life.This study[16], being prospective in design, provides a relevant contribution to the literature; probably, however, a larger sample could yield more robust results. For reason, other authors, such as Kelly Kl et al.[17], decided to assess the impact of the use of forehead sensor in some particular condition such as intense exercise; in this case, according to their results, the forehead sensor showed higher reliability. Furthermore, as shown by Robertson’s study[18], compared to finger sensor, the forehead sensor showed more reliable signal quality. The limit of this last study is its observational nature, although the sample is to be noted enrolling 80 patients. The problem arises in patients with vascular complications: in these cases, compared to foreheadsensor, the finger sensor showed poor accuracy [19].
DISCUSSION
The purpose of this narrative review was to describe the potential effectiveness of pulse oximetry saturation measurement using finger sensors versus forehead sensors, focusing exclusively on their reliability in various clinical conditions. This analysis aims to identify the most accurate method for SpO2 monitoring in nursing practice, particularly when addressing challenges related to peripheral perfusion and motion artifacts.Pulse oximetry is a critical tool in clinical practice; however, the accuracy of measurements can vary depending on some factors such as the sensor’s placement, the patient’s condition and motion of perfusion.The four studies analyzed provide a comprehensive overview of the differences between finger and forehead pulse oximeters in various clinical contexts, highlighting the strengths and limitations of each device. Below is a detailed comparison supported by the findings of these studies. The observational study by Seifi et al.[16], involving 67 post-coronary bypass patients, demonstrated that forehead sensors have superior accuracy compared to finger sensors, particularly in conditions of poor peripheral perfusion. Similarly, the validation study by Elkjær et al.[19],conducted on 82 patients with systemic sclerosis (SSc), found that forehead and earlobe sensors outperformed finger sensors. Forehead sensors, benefiting from better central perfusion, provided more reliable measurements in these settings. The clinical trial by Kelly et al.[17], involving 29 patients with heart failure and coronary artery disease, highlighted the superior reliability of forehead sensors during maximal exercise. Finger sensors underestimated SpO2 during peak exertion due to reduced peripheral perfusion. The clinical study by Robertson et al.[18], conducted on 80 patients with pulmonary vascular or interstitial lung diseases during the six-minute walk test (6MWT), also found forehead sensors more reliable, particularly during episodes of exercise-induced desaturation. However, the forehead sensor exhibited a slight bias compared to capillary blood gas (CBG) measurements, especially during deep desaturation. This reinforces the need for caution when interpreting extreme SpO2 values. All four studies highlight the limitations of finger pulse oximeters in conditions of poor peripheral perfusion, whether caused by critical illness, exercise or vascular disease. While finger sensors remain adequate for routine monitoring in stable patients, they underperform in situations requiring high accuracy. The forehead sensor consistently emerged as the most reliable alternative, particularly in:critically ill patients (Seifi et al.[16]), people undergoing physical exertion (Kelly et al.[17], Robertson et al.[18]) and patients with vascular conditions like systemic sclerosis (Elkjær et al.[19]). The studies involved different groups of patients and different clinical environments. These differences reflect the variety of clinical contexts and patient populations, providing a comprehensive perspective on the use of pulse oximeters in different conditions. However, despite these variations, the studies consistently agree that forehead sensors offer greater reliability than finger sensors in critical or dynamic conditions. Finally, the four studies address the research question as follows:
Research Question 1:Which sensor, on the finger or forehead, is more reliable and accurate for measuring oxygen saturation (SpO2) in patients with compromised peripheral perfusion?”:All four studies indicate that the forehead sensor placement is more reliability in patients with compromised peripheral perfusion. This is due to the fact that peripheral sites, such as the fingers, often show reduced perfusion in critically ill patients, leading to inaccurate or delayed readings. In contrast, the forehead maintains a more stable blood flow under such conditions, allowing for more accurate and reliable SPO2 measurements. Therefore, the studies consistently support the use of forehead sensors in scenarios involving low peripheral perfusion while finger pulse oximetry is widely used in routine clinical settings. Forehead sensors demonstrate faster response times and more consistent readings, minimizing the likelihood of underestimation or signal loss. As a result, in critical care contexts or when peripheral perfusion is impaired, forehead pulse oximetry is regarded as the more reliability method and may be considered the preferred standard for SpO2 monitoring.
Before drawing final conclusions, it is necessary to consider the methodological limitations of the included studies. It is also important to highlight that the included studies present some methodological limitations. Small sample sizes, variability in study design (mostly observational), and inconsistent use of reference standards (not all studies included comparison with arterial blood gas analysis) may affect the reliability of the findings. Moreover, the diversity of patient populations reduces the generalizability of the results across broader clinical settings
Implications for clinical practice
The review suggests that forehead pulse oximeters are more reliable than finger pulse oximeters in clinical scenarios involving poor peripheral perfusion, exercise-induced desaturation or specific chronic conditions such as heart failure and systemic sclerosis. The forehead sensors demonstrated superior performance in terms of accuracy, consistency and resistance to artifacts caused by motion or vasoconstriction. With this review we want to emphasize the crucial role of nurses in selecting the most appropriate pulse oximeter based on the patient's condition and clinical context. So, all nurses must be able to identify critically ill patients, those undergoing physical activity or individuals with vascular impairments (in order to ensure accurate SpO2 measurements using forehead pulse oximeters). Conversely, finger pulse oximeters remain suitable for stable patients with normal perfusion and routine monitoring. Nurses, as primary providers of patient care, play a pivotal role in monitoring oxygen saturation and must be aware of the limitations and advantages of each device. Proper training in device selection, positioning and interpretation of readings is essential to optimize patient outcomes and avoid diagnostic errors. By integrating this knowledge into daily practice, nurses can significantly contribute to more accurate assessments and improved clinical decision-making.
Strengths and limitations of the study
This review has some limitations:first, only two databases were consulted; moreover, the studies included in this review enrolled small sample sizes, often limited to patients with different diseases; for example, the study by Seifi enrolled only 50 patients following coronary artery bypass surgery [16], the Kelly’s study enrolled only 40 patients with stable heart failure [17] and theElkjaer’s study assessed only patients with systemic sclerosis [19]. For this reason, these studies did not use generalized data. In addition, Kelly [17] and Elkjaer’s[19] studies have not used a standard clinical reference like a blood gas analysis, but they only compared the different sensors without being able to validate the accuracy of the measurements. The Robertson’s study [18] used capillary blood gas (CBG) for validating Spo2 measurements, which is less accurate compared to Arterial Blood Gas, the gold standard for determining arterial oxygen saturation (Sa02). Finally, there are not many studies that have deal with this topic in the last ten years; for this reason, the review is limited to a small number of selected articles. As for the strengths, it can be noted that the research addresses a real-world clinical challenge frequently encountered in intensive care units, making to patient care and decision-making.Finally, although the exclusive inclusion of studies published in English may introduce a language bias, this decision was made to facilitate a more accessible and coherent review of the relevant literature, considering that a substantial proportion of high-quality evidence on the topic is published in English.By identifying the most reliable sensor placement under specific physiological conditions, the study offers guidance that could enhance monitoring accuracy and optimize clinical interventions.
This review, also, presents methodological limitations inherent to its narrative design. Specifically, the absence of a systematic methodology introduces a risk of subjective selection bias, as the inclusion of studies may be influenced by the reviewers' judgment. Furthermore, reproducibility is limited, and the review may not be exhaustive, potentially omitting relevant studies. These factors reduce the objectivity of the conclusions. Although a structured search strategy (PICO framework, selected databases, inclusion criteria) was applied, the narrative approach does not include a standardized critical appraisal of study quality, increasing the risk of bias.
CONCLUSION
This narrative review was conducted todescribe the potential effectiveness of pulse oximetry saturation measurement using finger sensors versus forehead sensors, focusing exclusively on their reliability in various clinical conditions. This analysis aims to identify the most accurate method for SpO2 monitoring in nursing practice, particularly when addressing challenges related to peripheral perfusion and motion artifacts. The evidence suggests that, while finger pulse oximetry remains the standard in most scenarios, forehead sensors may provide more reliable readings in critically ill patients with compromised peripheral perfusion. This evidence underscores the need for nurses and healthcare providers to adapt their monitoring strategies to ensure accurate and timely oxygenation assessments, ultimately improving patient outcomes. Further research is recommended to validate these findings across diverse clinical settings and patient populations.
Funding statement
This research did not receive any specific grant from funding agencies in public, commercial or not for profit sectors.
Conflict of interest
The authors report no conflict of interest.
Authors’ contribution
CR and AM were the major contributors in writing the manuscript. SC, and LA performed the data collection and interpreted the patient data.All authors read and approved the final manuscript.
REFERENCES
1. Checketts MR. AAGBI recommendations for standards of monitoring during anaesthesia and recovery 2015.Anaesthesia. 2016 Apr;71(4):470-1.doi: 10.1111/anae.13421. PMID: 26994537.
2. Merchant R, Chartrand D, Dain S, Dobson J,KurrekM, LeDez K, Morgan P, Shukla R; CanadianAnesthesiologists'Society. Guidelines to the Practice ofAnesthesiaRevised Edition 2012. Can JAnaesth.2012 Jan;59(1):63-102. English, French.doi: 10.1007/s12630-011-9609-0. PMID: 22183296.
3. Nitzan M,RomemA, Koppel R. Pulse oximetry: fundamentals and technology update. Med Devices (Auckl). 2014 Jul8;7:231-9.doi: 10.2147/MDER.S47319. PMID: 25031547; PMCID: PMC4099100.
4. TaenzerAH, Pyke JB, McGrath SP, BlikeGT. Impact of pulse oximetry surveillance on rescue events and intensive care unit transfers: a before-and-after concurrence study.Anesthesiology. 2010 Feb;112(2):282-7.doi: 10.1097/ALN.0b013e3181ca7a9b. Erratum in: Anesthesiology. 2020 Mar;132(3):602.doi: 10.1097/ALN.0000000000003091. PMID: 20098128.
5. Agashe GS, Coakley J, Mannheimer PD. Forehead pulse oximetry: Headband use helps alleviate false low readings likely related to venous pulsation artifact.Anesthesiology. 2006 Dec;105(6):1111-6.doi: 10.1097/00000542-200612000-00010. PMID: 17122573.
6. Kiruthiga, A.;Annamol, A.;Balamugesh, T.; Dinesh Prabhu, R.; Christopher, D.J.;Preejith, S.P.; Jayaraj, J.; Mohanasankar, S. Reflectance Pulse Oximetry for Blood Oxygen Saturation Measurement from Diverse Locations-A Preliminary Analysis. In Proceedings of the 2018 IEEE International Symposium on Medical Measurements and Applications (MeMeA), Rome, Italy, 11–13 June 2018; pp. 1–6.doi: 10.1109/MeMeA.2018.8438781.
7. Torp KD, Modi P, Pollard EJ, Simon LV. Pulse Oximetry. 2023 Jul 30. In:StatPearls. Treasure Island (FL):StatPearlsPublishing; 2025 Jan–.PMID: 29262014.Bookshelf ID:
8. Chan ED, Chan MM, Chan MM. Pulse oximetry: understanding its basic principles facilitatesappreciation of its limitations.Respir Med. 2013 Jun;107(6):789-99.doi: 10.1016/j.rmed.2013.02.004.Epub2013 Mar 13. PMID: 23490227.
9. Tusman G, Bohm SH, Suarez-Sipmann F. Advanced Uses of Pulse Oximetry for Monitoring Mechanically Ventilated Patients.AnesthAnalg. 2017 Jan;124(1):62-71.doi: 10.1213/ANE.0000000000001283. PMID: 27183375.
10. Ginosar Y, Weiniger CF, Meroz Y, Kurz V, Bdolah-Abram T,BabchenkoA, Nitzan M, Davidson EM.Pulse oximeter perfusion index as an early indicator of sympathectomy after epiduralanesthesia. ActaAnaesthesiolScand. 2009 Sep;53(8):1018-26.doi: 10.1111/j.1399-6576.2009.01968.x.Epub2009 Apr 24. PMID: 19397502.
11. HakverdioğluYöntG, Akin Korhan E, Dizer B. The effect of nail polish on pulse oximetry readings. Intensive Crit CareNurs. 2014 Apr;30(2):111-5.doi: 10.1016/j.iccn.2013.08.003.Epub2013 Sep 17.PMID: 24054173.
12. YekJLJ, Abdullah HR, Goh JPS, Chan YW. The effects of gel-based manicure on pulse oximetry. Singapore Med J. 2019 Aug;60(8):432-435.doi: 10.11622/smedj.2019031.Epub2019 Mar 11. PMID: 30854571; PMCID: PMC6717771.
13. Longmore SK, Lui GY, Naik G, Breen PP, Jalaludin B, Gargiulo GD. A Comparison of Reflective Photoplethysmography for Detection of Heart Rate, Blood Oxygen Saturation, and Respiration Rate at Various Anatomical Locations. Sensors (Basel). 2019 Apr 19;19(8):1874.doi: 10.3390/s19081874. PMID: 31010184; PMCID: PMC6514840
14. Grant MJ, Booth A. A typology of reviews: an analysis of 14 review types and associated methodologies. Health InfLibrJ2009;26:91–108..
15. BaethgeC, Goldbeck-Wood S, Mertens S. SANRA-a scale for the quality assessment of narrative review articles. ResIntegrPeer Rev2019;4:5..
16. Seifi S,KhatonyA, Moradi G, Abdi A, Najafi F. Accuracy of pulse oximetry in detection of oxygen saturation in patients admitted to the intensive care unit of heart surgery: comparison of finger, toe, forehead and earlobe probes.BMCNurs. 2018Apr17;17:15.doi: 10.1186/s12912-018-0283-1. PMID: 29692684; PMCID: PMC5905124.
17. Robertson L, Lowry R, Sylvester K, Parfrey H, Moseley B, Sheares K, Oates K. Comparison of forehead and finger oximetry sensors during thesix minutewalk test.ChronRespirDis. 2022 Jan-Dec;19:14799731211070844.doi: 10.1177/14799731211070844. PMID: 35045761; PMCID: PMC8796114.
18. Kelly KL, Carlson AR, Allison TG, Johnson BD. A comparison of finger and forehead pulse oximeters in heart failure patients during maximal exercise. Heart Lung. 2020 May-Jun;49(3):259-264.doi: 10.1016/j.hrtlng.2019.10.012.Epub2019 Nov 14. PMID: 31735457; PMCID: PMC7220844.
19. Elkjær AL, Næser EU, Aaen KT, Hovgaard HL, Juhl-Olsen P, Bendstrup E, Søndergaard K. Validity and reliability of measurement of peripheral oxygen saturation during the 6-Minute Walk Test in patients with systemic sclerosis.RheumatolInt. 2024 Apr;44(4):611-620.doi: 10.1007/s00296-024-05532-5.Epub2024 Feb 10. PMID: 38340159; PMCID: PMC10914912.
How Deep Are the Invisible Wounds? The Impact of Maternal Stress During Pregnancy on Adolescent Anxiety: A Cross-Sectional Study
Dessy Ekawati 1*, Nurul Azmi Arfan 2, Esti Pratiwi Yosin 2, Endang Yuswatiningsih 3
1 Department of Nursing, Faculty of Health, Institute of Science and Health Technology Insan Cendekia Medika Jombang, Indonesia.
2 Department of Midwifery, Faculty of Health, Institute of Science and Health Technology Insan Cendekia Medika Jombang, Indonesia.
3 Vocational Nursing Study Program, Ngawi District Government Nursing Academy, Indonesia.
* Corresponding Author: Dessy Ekawati, Department of Nursing, Faculty of Health, Institute of Science and Health Technology Insan Cendekia Medika Jombang, Indonesia. E-mail: dessyekawati.s1201@gmail.com, +6289624753811
Cite this article
ABSTRACT
Background: Pregnancy-related stress can affect a child’s development for a long time, increasing the likelihood of teenage anxiety. High levels of stress hormone exposure during pregnancy may interfere with the development of the nervous system and stress reactions, making a person more susceptible to anxiety disorders.
Objective: The purpose of this study is to determine the degree to which prenatal stress leads to teenage anxiety and to examine the association between maternal stress during pregnancy and teenage anxiety levels.
Methods: A cross-sectional design was used, involving 143 mothers with adolescents aged 10–19 years, selected through purposive sampling. The Prenatal Distress Questionnaire (PDQ) was used to measure prenatal stress, while the Generalized Anxiety Disorder-7 (GAD-7) was used to measure anxiety in adolescents. The link between prenatal stress and teenage anxiety was examined using Spearman's correlation, and the impact of prenatal stress on teenage anxiety was ascertained using ordinal regression.
Results: Prenatal stress and teenage anxiety were significantly positively correlated, according to Spearman's correlation test (r= 0.51; p < 0.0001). Ordinal regression analysis indicated that prenatal stress significantly influenced adolescent anxiety (Chi-Square = 27.9; p < 0.0001), explaining 45.6% of its variability (Nagelkerke R²= 0.46).
Conclusion: Maternal stress during pregnancy showed a moderate, significant positive correlation with adolescent anxiety (r= 0.51; p < 0.0001), explaining 45.6% of the variance in anxiety levels. Strengthening psychosocial support for pregnant women and implementing early prenatal stress detection programs are essential strategies to reduce the risk of anxiety disorders in their children. These findings highlight the need for psychological support programs for pregnant women to reduce the risk of anxiety disorders in their children.
Keywords: prenatal stress, adolescent anxiety, maternal anxiety, maternal mental health
INTRODUCTION
Pregnant women face various physical and emotional challenges that can affect their psychological well-being. Stress experienced during pregnancy not only impacts the mother but can also influence fetal development and the child's well-being in the future. Anxiety experienced by adolescents is one of the long-term effects of prenatal stress that is often overlooked [1]. Previous studies have demonstrated that maternal stress during pregnancy is significantly associated with an increased risk of anxiety symptoms in adolescents, suggesting that early life stress exposure may have enduring psychological consequences [2].
Adolescents with a history of mothers experiencing stress during pregnancy are more vulnerable to anxiety disorders compared to their peers. High exposure to stress hormones in the womb has the potential to disrupt the development of the nervous system and the child's stress response later in life. Specifically, elevated levels of maternal cortisol during critical periods of fetal development may alter the structure and connectivity of brain regions involved in emotional regulation, such as the amygdala, hippocampus, and prefrontal cortex [3]. Van Den Bergh et al. (2005) found that prenatal exposure to maternal anxiety alters amygdala connectivity in the fetus, potentially affecting emotional regulation into adolescence [4]. Anxiety in adolescents can significantly affect their social life, academic performance, and mental health. Anxiety's long-term consequences include poorer academic performance, trouble interacting with others, and a higher chance of developing other mental health conditions like depression [5].
Pregnancy can be a period of psychological stress, anxiety, and health concerns. Even in uncomplicated pregnancies, around 20% of women experience excessive worry about future events. Studies suggest that 10-16% of pregnant women are diagnosed with major depressive disorder, while up to 70% experience stress and anxiety. Though the overall prevalence of psychosocial stress during pregnancy remains unclear, research indicates that 22-25% of women experience high stress levels in each trimester [6]. A recent meta-analysis involving over 200,000 pregnant women across 102 studies reported that self-reported anxiety symptoms increased from 18.2% in the first trimester to 24.6% in the third trimester. Meanwhile, clinically diagnosed anxiety disorders were found in approximately 18% of women in the first trimester and 15% in the later stages of pregnancy. This discrepancy may be due to the overlap between depression symptoms and normal emotional fluctuations during pregnancy. Additionally, approximately 6.0–16.7% of pregnant women experience severe stress, while 13.6–91.86% experience mild to moderate stress [7].
Stress during pregnancy can be triggered by various factors, such as economic pressure, household conflicts, lack of social support, and maternal health conditions, including sleep disturbances and prenatal depression [8]. Furthermore, maternal age is important, especially for young moms, who frequently endure higher stress levels as a result of social pressure, mental unpreparedness, and restricted access to quality healthcare facilities. This problem is made worse by ignorance about pregnancy and parenting, which eventually affects the growth of the fetus as well as the health of the mother. Long-term stress can raise the risk of pregnancy issues such gestational hypertension, preeclampsia, and preterm birth by interfering with the control of cortisol, which is involved in the body's stress response [9]. Additionally, high exposure to stress hormones in the womb can affect fetal nervous system development, particularly in brain regions responsible for emotional and stress regulation, such as the amygdala and prefrontal cortex. Therefore, children of high-stress pregnant moms are more likely to have a lower stress threshold, be more susceptible to psychological strain, and develop anxiety problems during adolescence [10]. A systematic review by Tung et al. (2023) concluded that prenatal stress significantly correlates with increased risk of anxiety and behavioral issues in offspring [11].
Given these findings, it is crucial to better understand how maternal stress during pregnancy may contribute to adolescent mental health outcomes. Preventive efforts can be made by enhancing psychosocial support for pregnant women and providing education on stress management during pregnancy. Maternal mental health programs in healthcare facilities should be strengthened to enable early detection of prenatal stress. Family support and psychological counseling services can also help reduce maternal stress levels, thereby minimizing the risk of anxiety disorders in adolescents later in life [12].
Objective
This study aims to
1) examine the connection between teenage anxiety levels and the stress experienced by the mother during pregnancy, as well as;
2) assess the degree of association between prenatal stress and adolescent anxiety, considering possible confounding factors.
MATERIALS AND METHODS
Design
A cross-sectional study.
Sample
This study involved 143 mothers with adolescent children aged 10–19 years as respondents. Based on the Slovin formula with a 5% margin of error, the minimum required sample size for an estimated population of approximately 223 mothers was 143 participants. Participants were recruited from community health centers (Puskesmas) and Community Health Volunteer in Jombang District, East Java Province, Indonesia, through direct invitations and announcements with the assistance of community leaders. Inclusion criteria were:(1) mothers with adolescent children aged 10–19 years; (2) mothers able to recall and describe their experiences during pregnancy; and (3) willingness to participate by signing informed consent. Exclusion criteria included: (1) mothers with a history of severe psychiatric disorders that could affect memory reliability, and (2) mothers whose adolescent children had diagnosed neurodevelopmental disorders to avoid potential confounding factors. To minimize selection bias, recruitment procedures were standardized with uniform information sheets and consent forms provided to all candidates, and data collection was carried out by trained researchers. Nevertheless, the possibility of selection bias inherent to purposive sampling cannot be completely ruled out. Although convenience sampling allowed for timely data collection, it may have introduced selection bias and limited generalizability, compared to randomized sampling methods used in similar studies.
Data Collection
Data collection in this study was conducted in Jombang, a district in East Java Province, Indonesia, located in the eastern part of Java Island. The study took place from January 2025 to March 2025, focusing on maternal stress during pregnancy and its relationship with adolescent anxiety levels. A structured and systematic approach was implemented to ensure valid and reliable results.
Prior to data collection, a preliminary pilot test involving 10 participants was conducted to evaluate the clarity, comprehension, and cultural relevance of the instruments. To further improve data quality, several study team members with relevant expertise were involved in reviewing the research tools. Dessy Ekawati, holding a master’s degree in psychiatric nursing and formal training in Cognitive Behavioral Therapy (CBT) and statistical data processing, assessed the psychological aspects and clarity of emotional stress-related items. Nurul Azmi Arfan and Esti Pratiwi Yosin, both holding master's degrees in midwifery with a specialization in maternal and adolescent development, evaluated the cultural appropriateness and contextual suitability of the instruments. Their input was utilized to refine item wording, improve sensitivity to the local context, and enhance the comprehensibility of the questionnaires.
The primary data collection was conducted by Dessy Ekawati, with support from Nurul Azmi Arfan and Esti Pratiwi Yosin, to ensure consistency and minimize procedural bias. Endang Yuswatiningsih, a master's graduate in community nursing with expertise in statistical analysis, was responsible for supervising data management and quality control. Throughout the research process, participant anonymity and confidentiality were strictly maintained to promote honest and accurate responses. This study is part of a broader research initiative investigating the impact of maternal psychological stress during pregnancy on emotional outcomes during adolescence.
Measures
Maternal stress during pregnancy was measured using the Prenatal Distress Questionnaire (PDQ), while adolescent anxiety was assessed via the Generalized Anxiety Disorder-7 (GAD-7). The PDQ contains 12 items across six facets of prenatal stress, rated on a 5-point Likert scale (1 = Never to 5 = Very often): Baby’s Health & Childbirth, Physical Changes & Pregnancy Symptoms, Relationships & Social Support, Mother’s Role & Responsibilities, Financial & Career Concerns, and Mental & Emotional Health. Total scores range from 12 to 60, and were categorized as follows: low (12–27), moderate (28–43), and high (44–60). A validity test using Confirmatory Factor Analysis (CFA) showed that all items had a loading factor greater than 0.40, while the reliability test with Cronbach’s Alpha = 0.85 indicated good internal consistency. To ensure cultural relevance, the PDQ instrument used has been validated in the Indonesian context [13],
Teenagers' anxiety levels for the previous two weeks were evaluated using the GAD-7. It consists of seven items classified into None/Minimal Anxiety (0–4), Mild Anxiety (5–9), Moderate Anxiety (10–14), and Severe Anxiety (15–21). The items are assessed on a 4-point Likert scale (0 = Never to 3 = Nearly every day), with a total score ranging from 0 to 21. A validity test of GAD-7 using Exploratory Factor Analysis (EFA) showed a loading factor greater than or equal to 0.60, and the reliability test with Cronbach’s Alpha = 0.91 demonstrated excellent internal consistency. To ensure cultural relevance, the GAD - 7 instrument used has been validated in the Indonesian context [14].
The translation and cross-cultural adaptation of both instruments into Bahasa Indonesia were performed by the research team, composed of experts in psychiatric nursing, midwifery, and community nursing, all of whom are fluent in both English and Bahasa Indonesia. The translation followed a forward and backward translation process to ensure linguistic accuracy and cultural relevance. The pre-final versions were tested on 10 participants during a pilot phase to assess clarity, cultural appropriateness, and understanding, followed by minor linguistic adjustments where necessary.
To ensure the clarity and comprehensibility of the final versions, written instructions were provided to participants, and the operator was available to explain any unclear items during administration. This adaptation process ensured that the instruments remained valid and culturally appropriate for use in the Indonesian context.
Data Analysis
This study assessed adolescent anxiety levels using the Generalized Anxiety Disorder-7 (GAD-7) and maternal prenatal stress using the Prenatal Distress Questionnaire (PDQ). Data analysis, performed with SPSS (version 26), included descriptive statistics to characterize respondents and examine mean values, standard deviations, and data distribution. A normality test using Kolmogorov-Smirnov showed
p < 0.0001 (p < 0.05), indicating that the data were not normally distributed. Therefore, the relationship between maternal stress during pregnancy and adolescent anxiety was analyzed using Spearman’s correlation test, which is suitable for ordinal-scaled data that are not normally distributed. Additionally, to determine the influence of prenatal stress on adolescent anxiety levels, ordinal regression analysis was employed, considering that the dependent variable (adolescent anxiety level) was ordinal. Ordinal regression was used to assess the extent to which an increase in maternal prenatal stress levels contributed to a higher likelihood of adolescent anxiety. All analyses were conducted with a significance level of p < 0.05, indicating that the results obtained were statistically meaningful.
Ethical Considerations
This study was approved by the Institutional Review Board (Ref: 2025-014). Participants provided written informed consent, and data confidentiality was ensured. The study adhered to the ethical principles outlined in the Declaration of Helsinki (2013), and data were stored securely with password-protected files.
RESULTS
Sample Characteristics
All mothers were under 20 years old during pregnancy (100%). Most mothers had dropped out of school or did not continue their education beyond elementary or junior high school (74.1%). The majority of mothers were housewives (63.6%) and married (86%), while single mothers were those who had experienced divorce after giving birth. Most mothers were experiencing their first pregnancy (50.3%), while those with a second or subsequent pregnancy had a history of previous miscarriage. The majority of mothers experienced mild pregnancy complications (81.1%), such as mild anemia, excessive nausea and vomiting, or low blood pressure, while the remaining mothers experienced severe complications (18.9%). Most children of mothers who experienced stress during pregnancy have now reached adolescence, with the majority aged 10-13 years (51.0%) and currently attending junior high school (73.4%). The majority of the children were male (52.4%). Most respondent families belonged to the lower socioeconomic status category (51.0%), and the majority of the children lived in urban areas (51.0%).
During pregnancy, the majority of mothers (91.6%) experienced moderate levels of stress, while a small proportion experienced low (2.1%) or high (7.0%) stress levels, as measured by the Prenatal Distress Questionnaire (PDQ). Among adolescents, 2.7% reported mild anxiety, 88.1% moderate anxiety, and 9.8% severe anxiety, as measured by the GAD-7.
A majority of mothers reporting high stress levels also came from lower socioeconomic backgrounds, which may reflect the compounding effect of economic hardship on prenatal stress.
Table 1 presents the demographic data of respondents.
|
Characteristic |
Category |
n (%) |
M (SD) |
Median (IQR) |
|
Sociodemographic of Mother |
||||
|
Age at pregnancy |
13 – 19 |
15.91(2.02) |
15.91 (14.55–17.27) |
|
|
Education |
Elementary / Junior High School |
106 (74.1%) |
||
|
High School / Vocational High School |
37 (25.9%) |
|||
|
Occupation |
Housewife |
91 (63.6%) |
||
|
Fulltime |
28 (19.6%) |
|||
|
Part – time |
11 (7.7%) |
|||
|
Self – employed |
13 (9.1) |
|||
|
Marital Status |
Married |
123 (86%) |
||
|
Single Parent |
20 (14%) |
|||
|
Number of Children |
First child |
72 (50.3%) |
||
|
Second child or more |
67 (46.9%) |
|||
|
Twins |
4 (2.8) |
|||
|
History of pregnancy complication |
Mild |
116 (81.1) |
||
|
Severe |
27 (18.9) |
|||
|
Sociodemographic of Teenage |
||||
|
Adolescent age |
12 – 18 |
14.04 (1.89) |
14.04 (12.77–15.31) |
|
|
Adolescent gender |
Male |
75 (52.4%) |
||
|
Female |
68 (47.6%) |
|||
|
Education Level |
Junior High School |
105 (73.4%) |
||
|
Senior High School |
38 (26.6%) |
|||
|
Family Socioeconomic status |
Low |
73 (51%) |
||
|
Middle |
70 (49%) |
|||
|
Residence Environment |
Urban |
73 (51%) |
||
|
Rural |
70 (49%) |
|||
|
Maternal stress levels during pregnancy |
Low |
2(1.4%) |
||
|
Middle |
131(91.6%) |
|||
|
High |
10(7%) |
|||
|
Anxiety levels in adolescents |
Mild |
3 (2.1%) |
||
|
Moderate |
126 (88.1%) |
|||
|
Severe |
14 (9.8%) |
|||
Table 1. Sociodemographic, maternal stress levels during pregnancy and adolescent anxiety levels (n = 143)
Relationship Between Maternal Stress During Pregnancy and Adolescent Anxiety Levels
The Spearman test results indicate a positive and significant relationship between maternal stress during pregnancy and adolescent anxiety levels, with a correlation coefficient of 0.51 and a significance value of 0.005 (Table 2).
|
Mean (SD) |
Median (IRQ) |
Sig. (2 tailed) Spearman Correlation |
|
|
Maternal stress levels during pregnancy |
35.82 (4.51) |
35.82 (32.76–38.88) |
Correlation coefficient of 0.512 and significance value (p) of 0.005* |
|
Anxiety levels in adolescents |
12.55 (2.43) |
12.55 (10.91–14.19) |
*p < 0.05, SD = standard deviation, IRQ = interquartile range [Q1, Q3]
Table 2. Relationship Between Maternal Stress Levels During Pregnancy and Adolescent Anxiety Levels
Figure 1 presents a scatter plot showing a moderate positive correlation (r = 0.51) between prenatal stress and adolescent anxiety. This correlation suggests that higher maternal stress levels during pregnancy are associated with increased adolescent anxiety levels. The results also indicate that the relationship between these two variables is moderate to strong and remains statistically significant.
Figure 1 Scatter Plot of Adolescent Anxiety Levels by Maternal Stress Levels During Pregnancy
The crosstabulation table shows the distribution of respondents based on maternal stress levels during pregnancy and adolescent anxiety levels. The majority of adolescents with moderate anxiety levels came from mothers with moderate stress levels (Middle), totaling 118 out of 131 individuals. Among mothers with high stress levels (High), the distribution of adolescent anxiety varied more, with 8 adolescents experiencing moderate anxiety and 2 experiencing severe anxiety (Table 3).
|
Maternal stress levels during pregnancy |
Anxiety levels in adolescents |
Total |
||
|
Mild |
Moderete |
Severe |
||
|
Low |
2 |
0 |
0 |
2 |
|
Middle |
1 |
118 |
12 |
131 |
|
High |
0 |
8 |
2 |
10 |
|
Total |
3 |
126 |
14 |
143 |
Table 3. Crosstabulation of Maternal stress levels during pregnancy and Anxiety levels in adolescents
The Effect of Prenatal Stress on Adolescent Anxiety Levels
The ordinal regression analysis results indicate that the overall model is significant, with a Chi-Square value of 27.894 and p < 0.05, meaning that maternal stress during pregnancy significantly affects adolescent anxiety levels. The Nagelkerke R²value of 0.456 suggests that the model explains 45.6% of the variability in adolescent anxiety levels, indicating a moderate to strong relationship.
The model fit test shows that the Pearson value and Deviance value are both greater than 0.05, indicating a good model fit with the data. The parameter estimation results show that the threshold for category 2 (-3.876, p < 0.0001) is significant, meaning that higher maternal stress during pregnancy increases the likelihood of higher adolescent anxiety levels. Additionally, the variable of maternal stress during pregnancy (1.562, p < 0.0001) is also significant, confirming a direct and significant effect of maternal stress during pregnancy on adolescent anxiety levels.
In Table 4 we reported the results of the Ordinal Regression test.
|
Table 4a. Model Summary for Ordinal Regression |
|||||||||||
|
Model Component |
Value |
df |
Sig. (p-value) |
||||||||
|
Model Fit (Chi-Square) |
27.894 |
2 |
<0.0001 ** |
||||||||
|
Pearson Goodness-of-Fit |
χ² = 4.216 |
– |
0.081 |
||||||||
|
Deviance Goodness-of-Fit |
χ² = 5.678 |
– |
0.067 |
||||||||
|
Nagelkerke R² |
0.456 |
– |
– |
||||||||
|
Table 4b. Parameter Estimates for Predictors of Adolescent Anxiet |
|||||||||||
|
Variable / Threshold |
B |
SE |
Wald χ² |
df |
Sig. |
Exp(B) |
95% CI for Exp(B) |
||||
|
Threshold [Moderate Anxiety] |
–3.876 |
1.102 |
12.39 |
1 |
0.001 ** |
– |
– |
||||
|
Maternal Stress During Pregnancy |
1.562 |
0.496 |
9.91 |
1 |
0.002 ** |
4.77 |
1.60 – 5.05 |
||||
|
Threshold: cutoff value between anxiety categories. ** indicates significant contribution to the model. |
|||||||||||
Table 4. Results of Ordinal Regression Analysis
DISCUSSION
This study demonstrates that prenatal stress has a significant relationship with adolescent anxiety, aligning with the nature vs. nurture debate in child psychological development [15]. The nature factor influences children's predisposition to anxiety through genetic inheritance from parents, while the nurture factor shapes children's emotional development through environmental influences during pregnancy, including maternal stress [16]. According to a study by Van Den Bergh et al., (2005), stress experienced by the mother during pregnancy might change the responses of the fetal neurological system, especially in the limbic system, which is essential for controlling emotions [4]. Changes in the limbic system make children exposed to prenatal stress more susceptible to anxiety during adolescence [17]. Our findings are consistent with Rogers et al. (2020), who found a strong association between maternal perinatal mental health and long-term emotional outcomes in children [18].
The sociodemographic characteristics of mothers in this study reinforce the connection between nature and nurture in adolescent anxiety development. Young maternal age, low education levels, and economic pressure increase stress during pregnancy, which subsequently affects child development. Genetic factors may contribute to the inheritance of anxiety tendencies, which are then exacerbated by environmental stress [19]. A study by Sebők-Welker et al., (2024) found that mothers with low education levels have limited stress management skills, worsening the impact of prenatal stress on their children [20]. This further highlights the significant role of the prenatal environment in children's mental health.
Social and economic support plays a crucial role in clarifying the interaction between nature and nurture in adolescent anxiety development. Some children may have a more sensitive stress response system due to genetic factors, making them more vulnerable to anxiety. A supportive social environment can help mitigate the negative effects of genetic predisposition and prenatal stress [21]. According to a study by Nóblega et al., (2024), mothers from low socioeconomic backgrounds who endure prenatal stress likely to have a greater negative effect on the emotional development of their children [22]. The majority of children in this study lived in urban areas, which, according to Raman et al., (2021), is associated with higher exposure to environmental stressors such as academic and social pressures, further exacerbating their anxiety [23].
The findings of this study support the theory that the interaction between biological (nature) and environmental (nurture) factors significantly determines adolescent anxiety development. A study by Jensen, (2025) found that children whose mothers experienced prenatal stress were more likely to develop anxiety, particularly if they also had a family history of anxiety disorders [24]. Genetic factors provide an initial vulnerability to anxiety, but environmental experiences during pregnancy and childhood determine whether this predisposition develops into a more severe psychological disorder. The findings indicate that maternal stress during pregnancy is not just an individual issue but also contributes to children's future psychological well-being.
However, this study has several limitations. This study did not control for postnatal maternal anxiety or childhood trauma, which may also influence adolescent outcomes. Additionally, the use of convenience sampling may limit external validity. These limitations should be considered when interpreting the findings. Future research should address these limitations. Longitudinal studies are essential to establish causal links and to examine whether prenatal stress directly leads to persistent anxiety symptoms across developmental stages. Such research could offer deeper insight into the mechanisms linking prenatal conditions to long-term mental health outcomes.
Limitations
This study has several limitations. The use of purposive sampling facilitated the selection of respondents who could recall and describe their pregnancy experiences; however, it limits the generalizability of the findings, as the sample may not represent the broader population of mothers with adolescent children. This method also increases the risk of selection bias, as those who agreed to participate may have had particularly strong emotional experiences, potentially influencing the results. Future studies are recommended to use random or stratified sampling to enhance external validity. Additionally, the data relied on maternal recall of prenatal stress without objective verification such as medical records. This introduces the potential for recall bias, especially considering the time elapsed since pregnancy. Although participants were screened for major psychiatric disorders, no specific assessment of memory reliability was conducted. To address this, future research should consider prospective designs or data triangulation. The study was also limited to a specific geographic and cultural context, which may affect the applicability of the findings to populations with different sociocultural backgrounds. Lastly, the use of self-report measures introduces the possibility of social desirability bias, where participants may adjust their responses to align with perceived expectations.
CONCLUSION
According to this study, teenage anxiety levels are substantially correlated with maternal stress during pregnancy. These findings reinforce previous research suggesting that prenatal stress can influence children's emotional development through neuroendocrine responses and psychosocial factors. The sociodemographic characteristics of the respondents, such as young maternal age, low education levels, and unfavorable socioeconomic status, contribute to high stress levels during pregnancy, ultimately affecting children's anxiety in adolescence. The study's findings highlight the long-term effects of maternal psychological states during pregnancy on the emotional health of offspring. These findings suggest that early interventions aimed at reducing maternal stress during pregnancy may play a key role in preventing anxiety disorders and promoting long-term mental health in children.
Research Ethics and Conflict of Interest
This study was approved by the Institute of Science and Health Technology Insan Cendekia Medika Jombang's Research Ethics Committee (reference number 2025-014) on January 15, 2025. The authors declare no conflicts of interest.
Funding Sources
We extend our deepest gratitude to the mothers who sincerely recalled their pregnancy experiences and to the adolescents who were willing to share their stories and participate in this research. Without their openness, patience, and participation, this study would not have been possible.
Author Contributions
Concept and study design, manuscript writing and critical manuscript revision: DE, NAA, EPY, EY; data analysis and interpretation: DE, NAA. Final approval before publication: DE, NAA, EPY, EY.
REFERENCES
[1] Chauhan A, Potdar J. Maternal Mental Health During Pregnancy: A Critical Review. Cureus 2022;14. https://doi.org/10.7759/cureus.30656.
[2] Graham AM, Doyle O, Tilden EL, Sullivan EL, Gustafsson HC, Marr M, et al. Effects of maternal psychological stress during pregnancy on offspring brain development: Considering the role of inflammation and potential for preventive intervention. Biol Psychiatry Cogn Neurosci Neuroimaging 2021;7:461. https://doi.org/10.1016/J.BPSC.2021.10.012.
[3] Wu Y, De Asis-Cruz J, Limperopoulos C. Brain structural and functional outcomes in the offspring of women experiencing psychological distress during pregnancy. Mol Psychiatry 2024 297 2024;29:2223–40. https://doi.org/10.1038/s41380-024-02449-0.
[4] Van Den Bergh BRH, Mulder EJH, Mennes M, Glover V. Antenatal maternal anxiety and stress and the neurobehavioural development of the fetus and child: Links and possible mechanisms. A review. Neurosci Biobehav Rev 2005;29:237–58. https://doi.org/10.1016/j.neubiorev.2004.10.007.
[5] Jagtap A, Jagtap B, Jagtap R, Lamture Y, Gomase K. Effects of Prenatal Stress on Behavior, Cognition, and Psychopathology: A Comprehensive Review. Cureus 2023;15. https://doi.org/10.7759/cureus.47044.
[6] Pascal R, Casas I, Genero M, Nakaki A, Youssef L, Larroya M, et al. Maternal Stress, Anxiety, Well-Being, and Sleep Quality in Pregnant Women throughout Gestation. J Clin Med 2023;12:7333. https://doi.org/10.3390/jcm12237333.
[7] Zhang L, Huang R, Lei J, Liu Y, Liu D. Factors associated with stress among pregnant women with a second child in Hunan province under China’s two-child policy: a mixed-method study. BMC Psychiatry 2024;24:1–12. https://doi.org/10.1186/s12888-024-05604-7.
[8] Karnwal R, Sharmila K. Perspective View of Stress, Anxiety, and Depression among Pregnant Women: A Review. J Ecophysiol Occup Heal 2024;24:7–19. https://doi.org/10.18311/jeoh/2024/35771.
[9] Awad-Sirhan N, Simó-Teufel S, Molina-Muñoz Y, Cajiao-Nieto J, Izquierdo-Puchol MT. Factors associated with prenatal stress and anxiety in pregnant women during COVID-19 in Spain. Enferm Clin 2022;32:S5–13. https://doi.org/10.1016/j.enfcli.2021.10.006.
[10] Morales-Munoz I, Ashdown-Doel B, Beazley E, Carr C, Preece C, Marwaha S. Maternal postnatal depression and anxiety and the risk for mental health disorders in adolescent offspring: Findings from the Avon Longitudinal Study of Parents and Children cohort. Aust N Z J Psychiatry 2023;57:82–92. https://doi.org/10.1177/00048674221082519.
[11] Tung I, Hipwell AE, Grosse P, Battaglia L, Cannova E, English G, et al. Prenatal Stress and Externalizing Behaviors in Childhood and Adolescence: A Systematic Review and Meta-Analysis. Psychol Bull 2023;150:107–31. https://doi.org/10.1037/BUL0000407,.
[12] Wardoyo H, Moeloek ND, Basrowi RW, Ekowati M, Samah K, Mustopo WI, et al. Mental Health Awareness and Promotion during the First 1000 Days of Life: An Expert Consensus. Healthc 2024;12. https://doi.org/10.3390/healthcare12010044.
[13] Santoso JB. Pengembangan Skala Revised Prenatala Distress Questionnaire (NuPDQ) Versi Bahasa Indonesia. J Ilm Psikol MANASA 2018;7:62–71.
[14] Budikayanti A, Larasari A, Malik K, Syeban Z, Indrawati LA, Octaviana F. Screening of Generalized Anxiety Disorder in Patients with Epilepsy: Using a Valid and Reliable Indonesian Version of Generalized Anxiety Disorder-7 (GAD-7). Neurol Res Int 2019;2019. https://doi.org/10.1155/2019/5902610,.
[15] Shackman AJ, Gee DG. Maternal Perinatal Stress Associated With Offspring Negative Emotionality, But the Underlying Mechanisms Remain Elusive. Am J Psychiatry 2023;180:708–11. https://doi.org/10.1176/appi.ajp.20230630.
[16] Jami ES, Hammerschlag AR, Bartels M, Middeldorp CM. Parental characteristics and offspring mental health and related outcomes: a systematic review of genetically informative literature. Transl Psychiatry 2021;11. https://doi.org/10.1038/s41398-021-01300-2.
[17] Canini M, Pecco N, Caglioni M, KatušićA, Išasegi IŽ, Oprandi C, et al. Maternal anxiety-driven modulation of fetal limbic connectivity designs a backbone linking neonatal brain functional topology to socio-emotional development in early childhood. J Neurosci Res 2023;101:1484–503. https://doi.org/10.1002/jnr.25207.
[18] Rogers A, Obst S, Teague SJ, Rossen L, Spry EA, MacDonald JA, et al. Association between Maternal Perinatal Depression and Anxiety and Child and Adolescent Development: A Meta-analysis. JAMA Pediatr 2020;174:1082–92. https://doi.org/10.1001/JAMAPEDIATRICS.2020.2910,.
[19] Lopez M, Ruiz MO, Rovnaghi CR, Tam GKY, Hiscox J, Gotlib IH, et al. The social ecology of childhood and early life adversity. Pediatr Res 2021;89:353–67. https://doi.org/10.1038/s41390-020-01264-x.
[20] Sebők-Welker T, Posta E,Ágrez K, Rádosi A, Zubovics EA, Réthelyi MJ, et al. The Association Between Prenatal Maternal Stress and Adolescent Affective Outcomes is Mediated by Childhood Maltreatment and Adolescent Behavioral Inhibition System Sensitivity. Child Psychiatry Hum Dev 2024;55:1–21. https://doi.org/10.1007/s10578-023-01499-9.
[21] Hasriantirisna H, Nanda KR, Munawwarah. M S. Effects of Stress During Pregnancy on Maternal and Fetal Health: A Systematic Review. Adv Healthc Res 2024;2:103–15. https://doi.org/10.60079/ahr.v2i2.339.
[22] Nóblega M, Retiz O, Nuñez del Prado J, Bartra R. Maternal Stress Mediates Association of Infant Socioemotional Development with Perinatal Mental Health in Socioeconomically Vulnerable Peruvian Settings. Int J Environ Res Public Health 2024;21. https://doi.org/10.3390/ijerph21070844.
[23] Raman TL, Aziz NAA, Yaakob SSN. The effects of different natural environment influences on health and psychological well-being of people: A case study in selangor. Sustain 2021;13. https://doi.org/10.3390/su13158597.
[24] Jensen P. From nature to nurture–How genes and environment interact to shape behaviour. Appl Anim Behav Sci 2025;285:106582. https://doi.org/10.1016/j.applanim.2025.106582.
CHALLENGES TO CANCER PATIENT ADVOCACY IN NURSING PRACTICE: A NARRATIVE REVIEW
Vincenza Giordano 1*, Assunta Guillari 2, Aniello Lanzuise 3, Rita Nocerino 2, Michele Virgolesi 1, Martina Micera 4, Teresa Rea 1
- Department of Public Health, University of Naples Federico II (NA)
- Department of Translational Medical Sciences, University of Naples Federico II (NA)
- Health Management, Colli Hospital (NA)
- Department of Medical and Surgical Sciences, Agostino Gemelli University Hospital (RM)
* Corresponding author: Vincenza Giordano, Department of Public Health, University of Naples Federico II (NA). Email: enza-giordano@hotmail.it
Cite this article
ABSTRACT
Introduction: Advocacy by nurses caring for cancer patients is essential to ensure that their rights and wishes are respected throughout their care pathway. However, the ability of nurses to provide effective advocacy is limited by various organisational and managerial obstacles, potentially affecting the quality of care and patient well-being.
Objective: Description of the barriers to nursing advocacy in oncology, providing a critical summary of the available evidence to identify the main challenges and propose strategies for improvement.
Materials and Methods: A narrative review was conducted using databases such as PubMed, CINAHL and Cochrane Library between June and September 2024, using the Population, Intervention, Outcome (PIO) methodology.
Results: Four articles were deemed to be relevant to the study objective. The main issues that emerged from the narrative review were barriers to advocacy (lack of effective communication and work overload; fragmented continuity of care), improvement strategies (training and psychological support) and patients' experiences in the transition from distress to empowerment.
Conclusions: Various barriers hinder nursing advocacy in oncology, such as excessive workload, fragmentation of care and difficulties in addressing patients' emotional needs. This review underscores that the introduction of dedicated professionals, such as case managers, can provide organisational and coordinated support, helping to mitigate some of the barriers identified. Tackling the barriers to nursing advocacy is critical to ensuring high-quality, patient-centred cancer care. Strengthening organisational support, continuing education for nurses and the adoption of innovative care models are essential.
Keywords: Cancer patients, Neoplastic diseases, Nursing advocacy, Patient rights, Quality of life, Patient well-being, Patient healthcare.
INTRODUCTION
Nursing advocacy is defined as the active commitment of nurses to represent, protect and promote the rights, preferences and needs of patients, representing “the process through which nurses seek to protect the rights of patients, ensuring that their needs are met and that they receive safe, high-quality care” [1]. This involves a patient-centred approach, aimed at ensuring that patients receive high-quality care and that their decisions are respected within the healthcare system. Advocacy is based on communication skills, empathy and negotiation, as well as the ability to identify situations in which patients may be vulnerable or at risk of neglect [2]. In oncology, patients face complex and prolonged treatment pathways characterised by invasive treatment, debilitating side effects and significant emotional burden. Therefore, advocacy is particularly important for this type of patient, who requires a personalised approach and continuous support due to the changing nature of both the disease and its treatment [3]. Nurses are called upon to actively intervene to prevent patients from being subjected to injustice or neglect and to facilitate informed decision-making, an aspect that is essential to ensuring quality care. Nursing advocacy is not merely clinical support; it is an approach rooted in empathy, communication and the ability to negotiate solutions that respect the dignity and wishes of the patient. This includes support throughout the entire patient care process [2]. However, despite the recognised importance of this aspect, barriers to nursing advocacy remain widespread, including organisational pressure, lack of time and the weight of the doctor-nurse hierarchy. These factors limit the ability of nurses to provide continuous, personalised support [4].
Oncology is a complex field, and these challenges are even tougher because of the need to coordinate multidisciplinary care, which involves doctors, specialists, social workers, and psychologists. This complexity demands a high level of coordination and effective interprofessional communication, which isn't always achieved in the best way. The fragmentation of roles and responsibilities can create difficulties in information sharing and planning care, increasing the risk of problems that could compromise the patient's treatment pathway [4]. On top of that, the emotional strain of caring for cancer patients in the later stages of the disease, combined with the need to provide psychological support to patients and their families, makes it hard to balance defending patients' rights and managing professional stress [5].
Several studies [2,6] have explored nursing advocacy in a variety of clinical settings, demonstrating that it is essential for promoting a holistic approach that includes patient education, interprofessional communication and psychological support. While the importance of this topic is widely recognised, there are no specific systematic reviews describing the barriers to fully understanding nursing advocacy in oncology. This narrative review therefore aims to bridge this gap by providing a detailed overview of the barriers that limit nursing advocacy in oncology. The identification and description of these needs is essential for developing targeted strategies that improve the effectiveness of nursing care, with consequent benefits for the quality of care and the well-being of cancer patients.
Objective
To describe the barriers that hinder nursing advocacy in the oncology sector, providing a critical summary of the available evidence to identify the main challenges and suggest possible strategies for improvement.
MATERIALS AND METHODS
This narrative review was conducted in accordance with guidelines for the preparation of narrative reviews for peer-reviewed journals [7-9].
Study design
The research aims to answer the following question, formulated according to the Population, Intervention, Outcome (PIO) methodology: “What are the barriers that limit nursing advocacy for cancer patients, and how do they affect the quality of care and patient well-being?”
The PIO sets out the population to be analysed, the measures to be taken and the outcomes (Table 1).
|
P |
Cancer Patients |
|
I |
Barriers to nursing advocacy |
|
O |
Quality of patient care and well-being |
Table 1. Query according to the PIO method.
Research strategy
The study was conducted using various scientific databases, consulted between June 2024 and September 2024. The databases chosen for this work include PubMed, CINAHL, APA PsycArticles, and APA PsycInfo. During the research phase, specific keywords were used to narrow down the field of research and identify the most relevant studies, thus optimising the review process. The keywords used for the various searches were: "Cancer", "Barriers to advocacy", "Quality of Care", "Patient well-being". For each Medical Subject Headings term (MeSH), possible synonyms were identified. The keywords, together with their synonyms, have been combined using Boolean operators "AND" and "OR" to optimise the search and narrow down the most relevant results.
Inclusion and exclusion criteria
During the first phase of research and selection of studies, specific inclusion and exclusion criteria were defined. The following were included: (a) quantitative and qualitative primary studies; (b) studies investigating barriers that limit nursing advocacy for cancer patients and affect the quality of care and well-being of cancer patients; (c) articles in Italian and English language. The following were excluded: (a) secondary studies, reviews, meta-analyses or meta-syntheses; (b) studies investigating the barriers that limit nursing advocacy and affect the quality of care and well-being of non-cancer patients.
RESULTS
The survey produced a total of 542 articles, of which 536 came from databases (249 from PubMed, 218 from CINAHL and 69 from APA PsycArticles and APA PsycInfo) and 6 articles from free research. Finally, four articles were included in the review: one qualitative study, one RCT, and two cohort studies. The extraction and summary of the articles is shown in Table 2.
|
Author and type of study |
Population |
Study objective |
Results |
|
Horner et al., 2012 Randomised Controlled Trial |
N= 251 patients (intervention group exposed to the nursing navigator: n=133 patients with lung, breast and colorectal cancer |
Investigate the impact of an oncology nursing navigation programme on closing the care gap |
Patients who received support from the oncology nurse navigator rated the quality of care and continuity of care as better than those without a navigator, with fewer gaps in the care pathway. |
|
Reiser et al., 2021 Prospective cohort study |
n= 118 women with metastatic breast cancer |
Explore the impact of a nursing project to enhance coordination of supportive care in women with MBC, identifying barriers to advocacy. |
The programme demonstrated that targeted nursing assessment can overcome barriers, improve symptom management and reduce anxiety through nursing advocacy. |
|
Fillion et al., 2006 Observational cohort study |
n=158 patients with head and neck tumours (cohort exposed to professional navigators (n=83) and a historical cohort (n=75). |
Assess the impact of a case manager on the continuity of care and empowerment of cancer patients, identifying barriers that restrict access to support services and patient care. |
The navigator cohort reported better continuity of care, fewer cancer-related problems and improved quality of emotional life, highlighting the role of the navigator in overcoming barriers and supporting patient advocacy. |
|
Chan et al., Qualitative study |
n= 93 (47 women; 46 men) |
Exploring patients' perceptions of nurse-patient communication and barriers to psychosocial care in the oncology setting. |
The main barriers include high workloads and insufficient time, which hinder psychosocial support and continuity of care. |
Table 2. Data extraction
The studies selected were conducted in several countries, including Hong Kong, Canada, western Pennsylvania, and Washington. All in all, these studies involved 620 cancer patients. In qualitative studies, the average age of participants ranged from 58 years for women with metastatic breast cancer to 60-70 years for men with prostate cancer undergoing radical treatment. In quantitative studies, which included cancer patients hospitalised in hospital wards and patients with head and neck cancer, the average age of participants was between 55 and 63 years.
The main issues that emerged were barriers to advocacy (lack of effective communication and excessive workload; fragmentation of continuity of care), strategies for improvement (education and psychological support) and patients' experiences of moving from distress to empowerment.
Barriers to advocacy
Nursing advocacy is an essential component of cancer patient care, providing not only clinical support, but also emotional and informational guidance. However, a number of factors hinder the full exercise of this function, compromising the quality of care and the overall patient experience. Through analysis of the literature, several themes emerged: lack of effective communication and excessive workload, fragmentation of continuity of care, improvement strategies, education and psychological support, and patients' experiences as they move from distress to empowerment.
The themes were identified through a topical analysis of the studies included in the narrative review, which made it possible to identify recurring conceptual categories by comparing the responses and results of the studies. These were then grouped into main categories, representing the key areas of concern and the proposed strategies.
Lack of Effective Communication and Work Overload
Communication between nurses and patients is a key element of advocacy, but it can be compromised by organisational and management factors. The qualitative study by Chan et al. (2018) [3] highlighted how excessive workloads and fragmented care management pose significant obstacles, with direct repercussions on patient perception. The interviews conducted revealed a general reluctance to approach nurses for non-urgent issues, as they were seen as being too busy: "The nurses are just too busy... they don't have time to talk to patients". This results in limited opportunities to address psychological and emotional needs, as highlighted by another patient: "I don't talk to the nurses about my concerns... it's not their job to help me with psychological problems" [3]. This scenario points to a vicious circle in which a lack of time and resources hampers the building of a trusted relationship, which is essential to ensuring patient-centred care.
Fragmentation of Continuity of Care
A significant additional obstacle is the fragmentation of continuity of care. Horner et al. (2013) [10] noted an average delay of 42.93 days between diagnosis and the start of treatment in patients without a nursing reference point, demonstrating how the absence of a dedicated figure can negatively influence the clinical pathway. Furthermore, the absence of coordination led to a 30% increase in missed appointments, reflecting organisational difficulties that impact on patients' ability to adhere to treatment.
Improvement Strategies
Confronted with these barriers, a number of strategies have been developed to enhance nursing advocacy and improve the patient experience.
The development of Nursing Navigation Programmes is one of the first strategies. Studies such as those by Fillion et al. (2009) [11] and Horner et al. (2013) [10] have explored the role of specialised figures, such as the Professional Navigator (PNO) and the Oncology Nursing Navigator (ONN), in coordinating and managing care.
Il Professional Navigator (PNO), supports patients throughout their cancer journey, ensuring continuity of care and reducing logistical barriers. The study by Fillion et al. (2009) [11] highlighted how PNO significantly improves the organisation of care, with a 25% reduction in hospital admissions and a positive impact on quality of life: 60% of patients supported by PNO reported a reduction in anxiety, compared to 48% of the historical cohort.
At the same time, the Oncology Nursing Navigator (ONN), with a particular focus on oncology nursing care, has shown a significant impact in reducing delays in treatment (from 42.93 to 15.15 days) and improving treatment compliance (Horner et al., 2013) [10]. The presence of an ONN allowed for a reduction in missed appointments and guaranteed constant patient support, limiting the risk of interruptions in treatment.
Education and Psychological Support
As well as coordinating care, psychological support and health education are key to boosting patients' confidence in their treatment. Reiser et al. (2019) [6] have developed a nursing education programme specifically for women with metastatic breast cancer, demonstrating how targeted support can reduce feelings of isolation (42% of participants) and improve their quality of life.
Patient experiences moving from Discomfort to Empowerment
Patient experiences clearly reflect the important role of effective advocacy. Chan et al. (2018) [3] found that physical treatments are also perceived as a form of psychological comfort: "The fact that the nurse takes care of my physical pain makes me feel better mentally as well". However, the lack of structured emotional support has meant that many patients have lowered their expectations when it comes to discussing their psychological needs with nursing staff. Furthermore, studies such as those by Fillion et al. (2009) [11] and Reiser et al. (2019) [6] have demonstrated that integrating navigation programmes and nursing support can enhance patient empowerment, helping them make more informed decisions and improving compliance with treatment.
Study assessment
The quality of the narrative review was assessed using the SANRA Scale for the Assessment of Narrative Review Articles (SANRA) (Table 3), a validated method for making sure narrative reviews are methodologically sound [12].
|
First Author, year |
Justification of the article's significance for readers |
Statement of clear objectives or formulation of questions |
Description of Literature Research |
Referencing |
Scientific Reasoning |
Appropriate data presentation |
Score |
|
Hornet et al., 2012 |
1 |
2 |
1 |
2 |
2 |
2 |
10 |
|
Reiser et al., 2021 |
2 |
2 |
1 |
2 |
2 |
2 |
11 |
|
Fillion et al., 2006 |
2 |
2 |
1 |
2 |
2 |
2 |
11 |
|
Chan et al., 2018 |
1 |
1 |
1 |
2 |
1 |
2 |
8 |
|
Note: The six items that make up the scale are assessed using whole numbers from 0 (low score) to 2 (high score), with 1 as the midpoint. The maximum score for the overall sum is 12 |
|||||||
Table 3. SANRA Scale
An analysis of the selected articles highlights a moderate variability in the methodological quality of the narrative reviews. The overall scores range from a minimum of 8 to a maximum of 11 out of 12, suggesting an overall good level, but with room for improvement in some key areas.
In particular, the articles by Reiser et al. (2021) [6] and Fillion et al. (2006) [11] obtained the highest score (11/12), demonstrating good methodological consistency. Both clearly set out the importance of the topic, outline specific objectives and demonstrate sound scientific reasoning, although the description of the literature review remains limited (score 1), indicating a possible lack of transparency in the criteria for selecting sources. Horner et al. (2012) [10] display a similar profile but with a slightly lower score (10/12), penalised by a less convincing initial justification of the article's importance (score 1), suggesting that the article may not have clearly explained its added value for the reader. The article with the lowest score is that of Chan et al. (2018) (8/12) [3], which stands out negatively for its lack of well-defined objectives and weak scientific reasoning (scores of 1). Despite its good presentation of data (score 2), the article appears to suffer from poor methodological structure and limited description of the literature consulted, which are fundamental elements for the rigour of a narrative review. Assessment using the SANRA scale [12] reveals variability in the quality of the studies included, with some articles characterised by a more robust methodological structure and others by significant shortcomings. The strength of the conclusions depends on this diversity: studies with higher scores provide a more reliable basis, while those with lower scores should be interpreted with caution. Therefore, the final conclusions of the review must be interpreted taking into account the overall methodological quality, which represents a potential limit to the generalisability of the results.
DISCUSSION
The aim of the study was to describe the barriers that hinder nursing advocacy in the oncology context, providing a critical summary of the available evidence to identify the main challenges and propose possible strategies for improvement.
This narrative review has revealed that nursing advocacy in oncology is impeded by a series of barriers that overlap between individual, organisational and systemic dimensions. These include a lack of effective communication and excessive workloads, which have emerged as cross-cutting obstacles limiting nurses' ability to provide appropriate emotional support and establish empathetic relationships with patients [3-4]. These critical issues have a negative impact on the perception of patients, who see nurses as too busy to address their psychological needs, thus compromising the relationship of trust. Berben et al. [14] confirm this evidence, emphasising how complex nursing interventions focused on quality of life can improve perceived well-being and communication.
The fragmented nature of continuity of care is another significant obstacle. Horner et al. (2013) [14] highlight delays in treatment and difficulty in adhering to therapy when there is no regular nursing reference point. Tomaschewski-Barlem et al. (2017) [13] confirm this finding, suggesting that work environments that promote professional autonomy and collaboration between different professions facilitate better continuity of care.
Among strategies for improvement, the introduction of specialised professionals such as Professional Navigators (PNO) and Oncology Nurse Navigators (ONN) has proven useful in reducing fragmentation of care and providing significant emotional and psychological support [11,12,17,18], confirming the importance of holistic support offered by experienced professionals who are able to address not only clinical aspects, but also relational and social aspects. Likewise, Pautasso et al. (2018) [19] and McMullen et al. (2013) [20] document real benefits in terms of symptom management, care coordination, and psychological well-being.
Guided consultations by experienced nurses are another promising strategy. Drach-Zahavy et al. [15] and Grassi et al. [16] demonstrate that these approaches improve continuity of care, psycho-emotional management and patient satisfaction, underscoring the key role of nurses in the multidisciplinary team.
The experience of cancer patients, from discomfort to empowerment, stands out as a central theme. Chan et al. (2018) [3] observe that patients also see physical care as psychological comfort, but the lack of space for discussion about emotional issues can lead to isolation. Nursing navigation programmes [6,11] demonstrate that active patient involvement encourages empowerment and improves treatment adherence. The lack of specific training in advocacy is a well-documented cross-cutting barrier [21-24], and the integration of dedicated training in nursing curricula is a priority.
As a whole, the comparison with external studies complements and validates the findings, highlighting critical issues and suggesting practical solutions. The introduction of specialised figures, the enhancement of nurse training and the promotion of collaborative environments emerge as key interventions to make nursing advocacy more effective and focused on the needs of cancer patients.
Limitations and strong points
This review brings to light both significant aspects that offer opportunities for improvement and critical issues that limit its full implementation. One of the strengths that emerged is the clear identification of multidimensional barriers that include psychological, social, management and institutional aspects. A wide range of databases were included in the search, such as PubMed, CINAHL, APA PsycArticles and APA PsycInfo, ensuring broad coverage of relevant sources. This interdisciplinary approach has been beneficial in providing a comprehensive insight into the topic. Moreover, the combination of qualitative and quantitative studies allowed for the integration of experiential perspectives with measurable data, enriching the overall understanding of the challenges related to nursing advocacy. Another strong point is the focus on oncology, which is a complex field in which nursing advocacy plays a crucial role in improving the quality of care and the lives of patients. Furthermore, the review highlighted applicable operational solutions, such as the introduction of specialised roles (e.g. case managers) and proactive support programmes, which demonstrate the potential to address management barriers and improve overall care. Nevertheless, the review has some limitations. Although the narrative review method offers a broad and flexible overview, it can introduce bias in the selection and interpretation of studies, thereby limiting the generalisability of the results. A further limitation is the small number of studies included and the heterogeneity of the healthcare contexts, making it difficult to apply the findings uniformly to different healthcare systems, including the Italian one.
Finally, this narrative review was based mainly on articles published in peer-reviewed journals, excluding grey literature (e.g., theses, conference proceedings and technical reports). However, it is acknowledged that grey literature could offer further insights into barriers to nursing advocacy, in particular in settings that are less documented in the academic literature. Future studies may integrate these elements to provide a more comprehensive view of the phenomenon.
Implications for clinical practice
The implications drawn from the literature review point to the need to systematically address the barriers that limit the efficacy of nursing advocacy in the oncology setting. The most significant barriers identified include excessive workloads, fragmented continuity of care and a lack of psychological and educational support, all of which have a negative impact on the quality of care and patient well-being.
An initial priority is to improve organisational and working conditions for nursing personnel. Strategies that provide for a more even redistribution of the workload and the enhancement of human resources can mean that nurses are able to devote time to providing emotional and psychological support to patients, thereby overcoming the perception that their role is limited to physical care alone, as highlighted in the study by Chan et al. (2018) [3].
A second crucial aspect is the adoption of innovative, patient-centred care models, such as the introduction of dedicated professionals, such as the Professional Navigator and the Oncology Nurse Navigator, described in the studies by Fillion et al. (2009) [11] and Horner et al. (2013) [10]. In facilitating coordination between patients and multidisciplinary teams, these professionals are better able to improve continuity of care and reduce organisational gaps that often hinder advocacy. For example, the provision of a nursing navigator has been shown to reduce the time between diagnosis and the start of treatment and to improve treatment compliance, while providing greater emotional and psychological support for cancer patients.
Last but not least, investment in continuing education for nurses is a key step towards empowering them in their role as advocates. Training should be focused on advanced communication skills and managing the complex emotional needs of cancer patients, as recommended by the study by Reiser et al. (2019) [6]. These training initiatives not only improve the quality of care, but also increase patient confidence in the treatment process, helping to improve their quality of life.
CONCLUSIONS
In conclusion, this narrative review highlights the complex and multidimensional nature of the barriers that stand in the way of nursing advocacy in oncology. The evidence collected reveals how organisational, managerial and psychological elements limit the ability of nurses to fully establish themselves as defenders of patients' rights. Recognising these critical issues clears the way for targeted action, in particular through the adoption of specialised roles – such as Nurse Navigator and Professional Navigator – and specific training, enabling more effective coordination and consolidating advocacy practices. Furthermore, consideration of socio-cultural factors emerges as an essential factor in developing intervention strategies that are increasingly in line with the reality of different care contexts. Addressing these barriers systematically is, therefore, a fundamental step towards a model of care that integrates and enhances the role of nurses as advocates, helping to make cancer care more cohesive and focused on patients' needs.
Funding statement
This research received no external funding.
Conflict of interest
The authors report no conflict of interest.
Authors’ contribution
All Authors equally contributed.
REFERENCES
- Bu X, Jezewski MA. Developing a mid-range theory of patient advocacy through concept analysis. J Adv Nurs. 2007 Jan;57(1):101-10. doi: 10.1111/j.1365-2648.2006.04096.x.
- Vaartio H, Leino-Kilpi H, Salanterä S, Suominen T. Nursing advocacy: how is it defined by patients and nurses, what does it involve and how is it experienced? Scand J Caring Sci. 2006;20(3):282-292. doi: 10.1111/j.1471-6712.2006.00406.x
- Chan EA, Wong F, Cheung MY, Lam W. Patients' perceptions of their experiences with nurse-patient communication in oncology settings: A focused ethnographic study. PLoS One. 2018;13(6):e0199183. doi: 10.1371/journal.pone.0199183
- Negarandeh R, Oskouie F, Ahmadi F, Nikravesh M, Hallberg IR. Patient advocacy: barriers and facilitators. BMC Nurs. 2006;5:3. doi:10.1186/1472-6955-5-3
- Granek L, Nakash O, Ariad S, Shapira S, Ben-David M. Mental health distress: oncology nurses’ strategies and barriers in identifying distress in patients with cancer. Clin J Oncol Nurs. 2019;23(1):43–51. doi: 10.1188/19.CJON.43-51
- Reiser V, Rosenzweig M, Welsh A, Ren D, Usher B. The Support, Education, and Advocacy (SEA) Program of Care for Women With Metastatic Breast Cancer: A Nurse-Led Palliative Care Demonstration Program. Am J Hosp Palliat Care. 2019 Oct;36(10):864-870. doi: 10.1177/1049909119839696
- Silva, A.R., Padilha, M.I., Petry, S., Silva, E., Silva, V., Woo, K., Galica, J., Wilson, R., & Luctkar-Flude, M. (2022). Reviews of Literature in Nursing Research: Methodological Considerations and Defining Characteristics. Advances in Nursing Science, 45(3), 197-208. doi:10.1097/ANS.0000000000000418.
- Greenhalgh T, Thorne S, & Malterud K. (2018). Time to challenge the spurious hierarchy of systematic over narrative reviews? European Journal of Clinical Investigation, 48, e12931. doi:10.1111/eci.12931.
- Aveyard H, & Bradbury-Jones C. (2019). An analysis of current practices in undertaking literature reviews in nursing: Findings from a focused mapping review and synthesis. BMC Medical Research Methodology, 19(1), 105. doi:10.1186/s12874-019-0751-7.
- Horner K, Ludman EJ, McCorkle R, Canfield E, Flaherty L, Min J, et al. An oncology nurse navigator program designed to eliminate gaps in early cancer care. Clin J Oncol Nurs. 2013 Feb;17(1):43-48. doi: 10.1188/13.CJON.43-48. PMID: 23372095
- Fillion L, de Serres M, Cook S, Goupil RL, Bairati I, Doll R. Professional patient navigation in head and neck cancer. Semin Oncol Nurs. 2009;25(3):212-221. doi: 10.1016/j.soncn.2009.05.001.
- Baethge C, Goldbeck-Wood S, Mertens S. The SANRA—a scale for the quality assessment of narrative review articles. Res Integr Peer Rev. 2019;4:5. doi: 10.1186/s41073-019-0064-8
- Tomaschewski-Barlem JG, Lunardi VL, Barlem ELD, Silveira RSD, Ramos AM, Piexak DR. Patient advocacy in nursing: barriers, facilitators and potential implications. Texto Contexto Enferm. 2017;26:e0100014. doi: 10.1590/0104-07072017000100014
- Berben L, Geerits D, Deliens L, Beeckman D, Van Hecke A, Verhaeghe S, et al. Providing a nurse-led complex nursing intervention focused on quality of life assessment on advanced cancer patients: The INFO-QoL pilot trial. Eur J Oncol Nurs. 2021 Aug;53:101982. doi:10.1016/j.ejon.2021.101982. PMID: 33984605.
- Drach-Zahavy A, Goldblatt H, Maissel O, Tal-Or D, Admi H. Experiences and perspectives of patients and clinicians in nurse-led consultations in oncology: A multi-methods study. Eur J Oncol Nurs. 2022 Dec;61:102205. doi:10.1016/j.ejon.2022.102205. PMID: 36240680.
- Grassi L, Caruso R, Galli F, Nanni MG, Riva S, Sabato S, et al. The effect of consultations performed by specialised nurses or physicians on patient outcomes: A systematic review. J Adv Nurs. 2024 Feb;80(2):215–229. doi:10.1111/jan.15931.PMID: 38945063.
- Bettencourt E., et al. The Role of Case Management in Enhancing Cancer Patient Outcomes: A Comprehensive Review. Journal of Oncology Nursing. 2020; 15(4): 345–354. DOI: 10.1016/j.jon.2020.04.005.
- Katerenchuk J, Salas AS. An integrative review on the oncology nurse navigator role in the Canadian context. Can Oncol Nurs J. 2023;33(4):385-99. doi: 10.5737/23688076334385.
- Pautasso FF, Zelmanowicz ADM, Flores CD, Caregnato RCA. Role of the nurse navigator: integrative review. Rev Gaucha Enferm. 2018;39:e2017-010. doi: 10.1590/1983-1447.2018.2017-0104
- McMullen L. (2013). Oncology nurse navigators and the continuum of cancer care. Seminars in oncology nursing, 29(2), 105–117. https://doi.org/10.1016/j.soncn.2013.02.005
- Laari, L., & Duma, S. E. (2023). Barriers to nurses health advocacy role. Nursing ethics, 30(6), 844-856. https://doi.org/10.1177/09697330221146241
- Laari, L., & Duma, S. E. (2023). Health advocacy role performance of nurses in underserved populations: A grounded theory study. Nursing open, 10(9), 6527–6537. https://doi.org/10.1002/nop2.1907
- Benjamin, L. S., Shanmugam, S. R., Karavasileiadou, S., Hamdi, Y. S. A., Moussa, S. F., & Gouda, A. D. K. (2024). Facilitators and Barriers for Advocacy among Nurses-A Cross-Sectional Study. The Malaysian Journal of Nursing (MJN), 16(1), 178-188. https://doi.org/10.31674/mjn.2024.v16i01.018
- Oliveira, C., & Tariman, J. D. (2017). Barriers to the patient advocacy role: An integrative review of the literature. Journal of Nursing Practice Applications & Reviews of Research, 7(2), 7-12. https://doi.org/10.13178/jnparr.2017.0702.0704
![]()
This work is licensed under a Creative Commons
Attribution-NonCommercial-NoDerivatives 4.0 International License.
SUBSET OF NANDA-I NURSING DIAGNOSES FOR INTENSIVE CARE: DELPHI TECHNIQUE AND FOCUS GROUP
Mirko Masciullo 1, Flavio Marti 1,2*, Antonello Cocchieri 3, Lucia Mitello1, Andrea Fidanza 1, Anna Rita Marucci 1
- Department of Health Profession, San Camillo Forlanini Hospital, 00152 Rome, Italy
- School of Nursing and Midwifery, Faculty of Medicine and Psychology, Sapienza University of Rome, 00189 Rome, Italy
- Section of Hygiene, Woman and Child Health and Public Health, Gemelli IRCCS University Hospital Foundation, Catholic University of the Sacred Heart, 00168 Rome, Italy
* Corresponding author: Flavio Marti, School of Nursing and Midwifery, Faculty of Medicine and Psychology, Sapienza University of Rome, San Camillo Forlanini Hospital, 00152 Rome, Italy – ORCID: https://orcid.org/0000-0001-9569-3329 - Email: flavio.marti@uniroma1.it
Cite this article
ABSTRACT
Introduction: The NANDA-I taxonomy classifies nursing diagnoses to standardise communication and illustrate the impact of nursing on health outcomes. To improve usability in clinical practice, subsets of diagnoses, interventions, and outcomes have been developed for specific healthcare settings. These subsets facilitate documentation and decision making while supporting, rather than replacing, the clinical judgment of the nurse.
Objective: The study aims to develop a Subset of NANDA-I Nursing Diagnoses that nurses consider relevant in an intensive care setting.
Materials and Methods: A two-round Delphi study was carried out at the A.O. San Camillo Forlanini of Rome to identify the most appropriate diagnoses to constitute the Subset. Using the Delphi technique, two anonymous online questionnaires were submitted to a group of 10 experts. The nurses involved expressed their level of consensus on each of the most used NANDA-I diagnoses in intensive care.
Results: Nurses evaluated a total of 51 NANDA-I nursing diagnoses using 5-level Likert scales, including 47 diagnoses in the Subset. The most representative ones were: "(00004) Risk of infection", "(00047) Risk of compromised skin integrity", "(00030) Compromised gas exchange", "(00091) Compromised mobility in bed", "(00198) Model of disturbed sleep", "(00249) Risk of pressure injury in adults".
Conclusion: Among the included diagnoses, "Risk of infection" received unanimous agreement, confirming its essential role in intensive care. Other highly rated diagnoses, such as "Risk of compromised skin integrity," "Impaired gas exchange," and "Deficit in Self-Care: Bathroom," aligns with findings from previous studies. Some diagnoses, including "Compromised mobility in bed" and "Disturbed sleep pattern," were less commonly used in other ICUs, but were considered highly relevant by Delphi participants. The results highlight the focus of nurses on infection prevention, hygiene, gas exchange, pain management, mobilisation, and prevention of pressure injury. In particular, diagnoses related to stress, family conditions, and emotional needs received a lower consensus, suggesting the need for future research on holistic nursing care.
Keywords: nursing diagnoses, standardised nursing terminology, intensive care units, NANDA-International.
INTRODUCTION
The NANDA-I taxonomy was developed to classify nursing diagnoses related to interventions and outcomes that define the nursing process, allowing the integration of a common language within the nursing profession to improve communication, standardise care and improve patient outcomes. [1]. Standardised nursing terminology arises from the need to accurately and uniformly describe patient care. These terminologies facilitate communication by accurately describing the nursing process and illustrating the impact of nursing on health outcomes [2]. The use of standardised and validated language in clinical practice remains less widespread than expected, in part due to the challenges of integrating a common language into routine nursing documentation [1]. To simplify the use of standardised nursing languages, subsets of diagnoses, interventions, and outcomes have been developed to describe nursing actions in specific healthcare settings [3]. Subsets include specific nursing diagnoses for a specific healthcare context or condition. They are very useful tools for directing appropriate interventions and outcomes based on the clinical judgment of the nurse, who can thus focus on each individual care need of the patient [4]. The concept of Subset was introduced to respond to the need of professionals to have standardised terminology available but at the same time less confusing and easy to use. It is important, however, to specify that a Subset does not replace the nurse's judgment in any way, but rather facilitates the documentation phase of care [5].
Objective: The study aims to develop a Subset of NANDA-I Nursing Diagnoses that nurses consider relevant in an intensive care setting. The most commonly used NANDA-I diagnoses in Intensive Care, identified in a recent scoping review [6], were evaluated by a group of Intensive Care nurses.
MATERIALS AND METHODS
A two-round Delphi study was carried out to identify relevant nursing diagnoses following Skulmoski's methodology [7]. The main purpose of the Delphi technique is to generate consensus among a group of experts through a process of questionnaires interspersed with controlled [8]. It involves a structured group interaction, where members interact anonymously using questionnaires, thus preserving open discussions from influencing results [9]. Multistage interactions are envisaged to reduce the range of responses as much as possible and obtain consensus from the majority of experts [10].
Inclusion criteria
Inclusion criteria required having at least 24 months of experience in an intensive care unit of the A.O. San Camillo Forlanini in Rome.
Sample size
A group of 10 nurses were recruited, with two representatives for each of the five Intensive Care Units (ICU) of the A.O. San Camillo Forlanini of Rome (Shock and Trauma ICU, Cardiovascular ICU, Thoracic ICU, Post-surgical ICU and Neurosurgical ICU). Studies suggest an optimal Delphi group size of 10 and 15 participants [10].
Focus Group
In September 2023, the 10 study participants joined an online focus group via Google Meet. The group received a briefing on the Delphi technique and study procedures. During this session (Round 1), the first anonymous questionnaire was administered through Google Forms. The questionnaire asked to evaluate nursing diagnoses according to the NANDA-I 2020-2023 taxonomy most used in intensive care settings. After completing the questionnaire, an open discussion between participants was held to indicate further NANDA-I nursing diagnoses that should be included in the second questionnaire
At this stage, the experts' clinical judgments were recorded in free terms and converted into NANDA-I 2020-2023 nursing diagnoses by the authors (Table 2). One author acted as moderator, while the other was responsible for recording the clinical judgments expressed by the experts.
Survey tool
The questionnaire evaluated nursing diagnoses based on the NANDA-I 2020-2023 taxonomy, specifically those most commonly used in Intensive Care, emerged from the Scoping Review underlying this study [6]. The questionnaire asked to evaluate nursing diagnoses according to the NANDA-I 2020-2023 taxonomy most used in intensive care settings. Subsequently, the results of the first questionnaire were processed and sent to each of the participants. At the end of September 2023, the second questionnaire was sent by email, consisting of diagnoses that needed re-evaluation according to the predefined criteria and diagnoses added by the nurses in the Focus Group.
Data collection and analysisThe first questionnaire asked to evaluate each of the proposed NANDA-I diagnoses on a Likert scale with a score of 1 to 5, quantifying the degree of appropriateness of the single nursing diagnosis in an Intensive Care Unit context. The interpretation of the results based on the average scores obtained for the first questionnaire was as follows: diagnoses with a low degree of consensus (range 1-2.33) were excluded from the Subset; diagnoses with an uncertain degree of consensus (2.34-3.66) or with at least an evaluation of score 3, were re-evaluated in the second questionnaire; diagnoses with a high degree of consensus (3.67-5) were included in the Subset. A summary table of the results including group ratings and diagnoses added during the focus group was prepared. This table was used to provide controlled feedback and statistical group response to participants, two important characteristics of the Delphi technique [11].
The second questionnaire, in addition to diagnoses with uncertain results, also served to evaluate the NANDA-I diagnoses added directly by nurses during the Focus Group. In this phase, the interpretation of the results included the following criteria: diagnoses with a low or medium degree of consensus (1-3.66) were excluded from the Subset; diagnoses with a high degree of consensus (3.67-5) were included in the Subset. Since this was the last planned questionnaire, all diagnoses that did not reach a high degree of consensus were excluded.
Ethical considerationsThe study protocol matched the ethical guidelines of the Declaration of Helsinki for clinical studies and was submitted to the Ethics Committee of Lazio 1 that notified the acknowledgement with protocol number 1295 on 13 December 2022. Eligible participants were informed about the study’s purpose and their right to withdraw at any time without any consequences. Informed consent was obtained from all participants prior to their inclusion in the study, ensuring voluntary participation.
RESULTS
Sample description
The panel included 7 female and 3 male nurses, with an average age of 36.9 years (SD=8.5; range=26-49) and an average of years of service in the ICU of 9.1 years (SD=6.74; range=2-22). Seven nurses have a bachelor's degree in Nursing and three have a master's degree in Nursing and Midwifery.
First Delphi RoundThe first questionnaire evaluated 44 NANDA-I nursing diagnoses commonly used in ICU settings. Of these, 34 diagnoses were directly included in the Subset; 9 diagnoses obtained uncertain results or at least an uncertainty rating and were re-evaluated in the second questionnaire; a diagnosis was excluded directly from the Subset, without the need for re-evaluation. The results are summarised in Table 1 and are provided as mean scores and standard deviation for each NANDA-I Nursing Diagnosis 2020-2023.
(Code) Nursing Diagnosis NANDA-I Average Score SD (00002) Unbalanced nutrition: less than metabolic needs 4.1 0.83 (00004) Infection risk 5 0 (00011) Constipation 4.6 0.49 (00013) Diarrhea 4.4 0.49 (00022) Risk of urgent urinary incontinence 1.7 1.19 (00025) Risk of unbalanced fluid volume 4.4 0.92 (00027) Insufficient fluid volume 4 1.09 (00029) Reduced cardiac output 3.7 1.19 (00030) Compromised gas exchange 4.8 0.4 (00031) Ineffective airway clearance 4.2 1.17 (00032) Ineffective breathing pattern 4.6 0.49 (00033) Impaired spontaneous ventilation* 4.2* 0.6 (00039) Risk of aspiration 4 1.09 (00040) Risk of immobilization syndrome 4.2 0.87 (00044) Compromised tissue integrity 4.2 0.87 (00045) Compromised oral mucosa 4.4 0.49 (00046) Compromised skin integrity 4.6 0.49 (00047) Risk of compromised skin integrity 4.9 0.3 (00052) Impaired social interactions* 4.2* 0.98 (00060) Interrupted family processes 4.1 1.14 (00085) Compromised mobility 4.6 0.49 (00087) Risk of injury from perioperative positioning 3.9 1.04 (00091) Impaired mobility in bed 4.8 0.4 (00092) Reduced activity tolerance* 4.4* 0.66 (00102) Self-care deficit: nutrition 4.3 0.9 (00108) Self-care deficit: bathroom 4.7 0.9 (00110) Self-care deficit: toilet* 4* 1.34 (00114) Transfer stress syndrome* 3.3* 1.42 (00126) Insufficient knowledge 4.2 0.87 (00128) Acute mental confusion 4.5 0.92 (00155) Risk of falls in adults** 3.3** 1.34 (00177) Psychophysical overload from stress* 2.9* 1.37 (00179) Risk of unstable blood sugar 4.2 0.4 (00195) Risk of electrolyte imbalance 4.3 0.9 (00198) Disturbed sleep pattern 4.8 0.4 (00200) Risk of reduced cardiac tissue perfusion* 3.1* 1.51 (00201) Risk of Ineffective Cerebral Tissue Perfusion* 3.9* 1.14 (00204) Ineffective peripheral tissue perfusion 4.2 0.87 (00206) Risk of bleeding 4.4 0.49 (00213) Risk of Vascular Trauma 4.2 1.17 (00219) Risk of dry eyes 4 1.09 (00228) Risk of ineffective peripheral tissue perfusion 4.3 0.9 (00247) Risk of compromised oral mucosal integrity 4.6 0.49 (00249) Risk of pressure injury in adults 4.8 0.4 * Diagnosis with at least a grade 3 (uncertain) rating: to be re-evaluated in round 2.
** Diagnosis with an average score between 2.34 and 3.66: to be re-evaluated in round 2Table 1: Results of the first questionnaire (in ascending order by code NANDA-I 2020-2023
Focus group
The open discussion among the Intensive Care nurses in the Delphi group led to the inclusion of seven additional NANDA-I nursing diagnoses in the study. Participants freely expressed their clinical judgments, which were recorded and later coded by the researchers according to the NANDA-I 2020–2023 taxonomy. Expert evaluations helped identify the care needs of Intensive Care patients that best represented their clinical context but had not previously emerged from the scientific literature. This phase was essential to refine the Subset to better align with specific care settings. The results of the focus group are summarised in Table 2.
Clinical judgment (Code) NANDA-I Nursing Diagnosis “Communication alterations due to tracheostomy or language barrier” (00051) Impaired verbal communication “Dysphagia” (00103) Impaired swallowing “Postoperative or other pain (after trauma, pressure ulcer, positioning)” (00132) Acute pain “Thermoregulation problems (post-surgery, post-traumatic, or fever)” (00006) Hypothermia “Thermoregulation problems (post-surgery, post-traumatic, or fever)” (00007) Hyperthermia “Problems in the phase of weaning from the mechanical ventilator” (00034) Response to weaning from the dysfunctional ventilator “Alteration of body image in tracheostomized or mutilated patients” (00118) Body image disorder Table 2: Clinical judgments expressed by nurses in the Focus Group and coded according to the NANDA-I taxonomy
Second Delphi Round
In the second questionnaire, a total of 16 diagnoses were evaluated, nine diagnoses were re-assessed based on predefined criteria, while 7 were newly added by participants during the focus group. After completion of this questionnaire, 3 additional diagnoses were excluded from the Subset, leaving a final total of 13. The results of this phase of the Delphi study are presented in Table 3.
(Code) NANDA-I Nursing Diagnosis Average Score SD (00006) Hypothermia * 4.4 0.92 (00007) Hyperthermia * 4.4 0.92 (00033) Impaired spontaneous ventilation 4.5 0.5 (00034) Response to weaning from the dysfunctional ventilator * 4.4 0.49 (00051) Impaired verbal communication * 4.4 0.49 (00052) Impaired social interactions 4.5 0.5 (00092) Reduced activity tolerance 4.6 0.49 (00103) Impaired swallowing * 4.6 0.49 (00110) Self-care deficit: toilet 4.1 1.3 (00114) Transfer stress syndrome 3.7 1.42 (00118) Body image disorder * 3.4 1.43 (00132) Acute pain* 4.5 0.5 (00155) Risk of falls in adults 3.3 1.35 (00177) Psychophysical overload due to stress 3.4 1.43 (00200) Risk of reduced cardiac tissue perfusion 4.1 1.4 (00201) Risk of ineffective cerebral tissue perfusion 4.6 0.49 * Diagnoses added during the Focus Group Table 3: Results of the round 2 questionnaire
Subset of NANDA-I nursing diagnoses
In the first questionnaire of Round 1 (Table 1), the expert panel evaluated the NANDA-I nursing diagnoses identified through the Scoping Review by Masciullo [6]. Subsequent focus group, through open discussion among participants, helped identify additional nursing diagnoses (Table 2) considered relevant in Adult Intensive Care Unit (ICU) context. In the second questionnaire (Table 3), nurses re-evaluated diagnoses that had not achieved a sufficient score for inclusion in the Subset or had raised uncertainty for at least one participant. During this phase, the panel also evaluated the diagnoses added during the focus group. The results of the Delphi study led to the development of a validated Subset comprising 47 nursing diagnoses, approved by a panel of adult intensive care nurses. The final NANDA-I Nursing Diagnosis Subset for the ICU is presented in Table 4, ranked in descending order of Delphi consensus.
(code) Nursing diagnosis NANDA-I Average score SD (00004) Risk of infection 5.0 0.0 (00047) Risk of compromised skin integrity 4.9 0.3 (00030) Compromised gas exchange 4.8 0.4 (00091) Impaired mobility in bed 4.8 0.4 (00198) Disturbed sleep pattern 4.8 0.4 (00249) Risk of pressure injury in adults 4.8 0.4 (00108) Self-care deficit: bathroom 4.7 0.9 (00011) Constipation 4.6 0.49 (00032) Ineffective breathing pattern 4.6 0.49 (00046) Compromised skin integrity 4.6 0.49 (00085) Compromised mobility 4.6 0.49 (00092) Reduced activity tolerance 4.6 0.49 (00103) Impaired swallowing 4.6 0.49 (00201) Risk of ineffective cerebral tissue perfusion 4.6 0.49 (00247) Risk of compromised oral mucosal integrity 4.6 0.49 (00033) Impaired spontaneous ventilation 4.5 0.5 (00052) Impaired social interactions 4.5 0.5 (00132) Acute pain 4.5 0.5 (00128) Acute mental confusion 4.5 0.92 (00013) Diarrhea 4.4 0.49 (00034) Response to weaning from the dysfunctional ventilator 4.4 0.49 (00045) Compromised oral mucosa 4.4 0.49 (00051) Impaired verbal communication 4.4 0.49 (00206) Risk of bleeding 4.4 0.49 (00006) Hypothermia 4.4 0.92 (00007) Hyperthermia 4.4 0.92 (00025) Risk of unbalanced fluid volume 4.4 0.92 (00102) Self-care deficit: nutrition 4.3 0.9 (00195) Risk of electrolyte imbalance 4.3 0.9 (00228) Risk of ineffective peripheral tissue perfusion 4.3 0.9 (00179) Risk of unstable blood sugar 4.2 0.4 (00040) Risk of immobilization syndrome 4.2 0.87 (00044) Compromised tissue integrity 4.2 0.87 (00126) Insufficient knowledge 4.2 0.87 (00204) Ineffective peripheral tissue perfusion 4.2 0.87 (00031) Ineffective airway clearance 4.2 1.17 (00213) Risk of Vascular Trauma 4.2 1.17 (00002) Unbalanced nutrition: less than metabolic needs 4.1 0.83 (00060) Interrupted family processes 4.1 1.14 (00110) Self-care deficit: toilet 4.1 1.3 (00200) Risk of reduced cardiac tissue perfusion 4.1 1.4 (00027) Insufficient fluid volume 4 1.09 (00039) Risk of aspiration 4 1.09 (00219) Risk of dry eyes 4 1.09 (00087) Risk of injury from perioperative positioning 3.9 1.04 (00029) Reduced cardiac output 3.7 1.19 (00114) Transfer stress syndrome 3.7 1.42 Table 4: Subset of Nursing Diagnoses according to NANDA-International taxonomy 2020-2023
DISCUSSION
The specific Subset for the adult Intensive Care context, identified through this study, includes 47 NANDA-International Nursing Diagnoses. The expert panel excluded only one diagnosis in Round 1 and three diagnoses in Round 2. The excluded diagnoses were: (00022) Risk of urge urinary incontinence, which received a very low average score (1.7) and was unanimously considered inappropriate for the Intensive Care setting. Diagnoses (00155) Risk of falls in adults and (00177) Stress overload, initially assessed with uncertainty in Round 1 and reevaluated in Round 2, failed to achieve sufficient consensus. Finally, (00118) Disturbed body image was also excluded due to a high standard deviation (1.43), indicating inconsistent evaluations among nurses and highlighting a topic that warrants further investigation.
Among the included diagnoses, (00004) Risk of infection stood out, achieving the highest score and being unanimously recognised as essential in an ICU setting. This finding aligns with the existing literature, since the same diagnosis has been reported to be the most frequently used in similar care settings [12–16].
Other diagnoses received a high degree of consensus, being among the most representative according to experts. These diagnoses also appear frequently in similar contexts described in previous studies, including (00047) Risk of impaired skin integrity [13,14], (00030) Impaired gas exchange [17,18], and (00108) Self-care deficit: bathing [12,13,19]. These findings suggest that, for the most part, the results obtained using the Delphi technique are consistent with those of other studies. However, some diagnoses that achieved a high level of consensus differed from those commonly used in other ICUs, including (00091) Impaired bed mobility, (00198) Disturbed sleep pattern, and (00249) Risk of pressure injury in adults. Despite their lower prevalence in other Intensive Care settings, the Delphi study participants considered them highly representative of their respective operational units. The NANDA diagnosis subset is intended to support nurses in choosing the most appropriate nursing diagnoses that reflect the specific care needs of patients admitted to the ICU. However, it is not a substitute for professional judgment and therefore, it is the nurse's responsibility to formulate additional diagnoses to ensure individualization of care.
CONCLUSION
The creation of a subset of nursing diagnoses has allowed the identification of the main areas of care in which ICU nurses have focused their attention. The key themes that emerged include infection prevention, hygiene, gas exchange, pain management, patient mobilisation, and prevention of pressure injuries. Diagnoses that received a high level of consensus reflect the essential responsibilities of nurses in high-complexity care settings. These diagnoses addressed not only the patient’s actual needs but also potential problems, whose identification through risk diagnoses proved crucial for the implementation of effective preventive measures.
Furthermore, the analysis of the diagnoses included in the subset revealed a tendency to exclude or assign minimal relevance to diagnoses related to stress, family conditions, knowledge, and situational acceptance. This finding highlighted a widespread difficulty among nurses in identifying needs related to the patient’s emotional and spiritual well-being, instead of prioritising physiological problems. Therefore, it will be essential to further explore this aspect of nursing care through future studies that integrate not only NANDA-I Nursing Diagnoses but also the NIC and NOC classifications.
LimitationsTo ensure greater methodological consistency, it would be advisable to conduct a literature review that aims not only to identify nursing diagnoses but also to define specific outcomes and interventions for adult ICU. An additional limitation of this study concerns the level of knowledge of the participants regarding the use of NANDA-International nursing diagnoses. Although they were experienced ICU nurses, their familiarity with NANDA-I diagnoses was not optimal. This issue reflects a broader challenge within the Italian nursing context, where the use of standardised nursing languages is not yet fully widespread. Due to the difficulty in recruiting nurses who were experts in intensive clinical practice and experienced in the use of NANDA-I diagnoses, the primary inclusion criterion was experience in ICU patient care. Finally, it would be necessary to replicate a multicentred Delphi study to generalise the findings to other adult ICU care settings.
Funding statementThis research did not receive specific grants from funding agencies in the public, commercial, or non-profit sectors.
Conflict of interestThe authors report no conflict of interest.
Authors’ contributionM.M: Investigation, Writing - original draft. F.M.: Conceptualization, Writing - original draft, Writing - review & editing. A.C.: Writing - review & editing, Supervision. L.M.: Writing - review & editing, Supervision. A.F.: Conceptualization, Writing - review & editing. A.R.M.: Conceptualization, Supervision. All authors have read and agreed to the published version of the manuscript.
AcknowledgementsThe authors wish to thank the nurses who participated in this study. A heartfelt thanks to Federica Mauri Kurera for English editing support.
References
- D’Agostino F, Zeffiro V, Vellone E, Ausili D, Belsito R, Leto A, et al. Cross-Mapping of Nursing Care Terms Recorded in Italian Hospitals into the Standardized NNN Terminology. Int J Nurs Knowl 2020;31:4–13. https://doi.org/10.1111/2047-3095.12200.
- Rabelo-Silva ER, Dantas Cavalcanti AC, Ramos Goulart Caldas MC, Lucena A de F, Almeida M de A, Linch GF da C, et al. Advanced Nursing Process quality: Comparing the International Classification for Nursing Practice (ICNP) with the NANDA-International (NANDA-I) and Nursing Interventions Classification (NIC). J Clin Nurs 2017;26:379–87. https://doi.org/10.1111/jocn.13387.
- Bezze S, Ausili D, Erba I, Redini S, Re S, Di Mauro S. Development of a subset of ICNP Nursing Diagnoses for the promotion of self-care in people with diabetes mellitus: a multi-center observational study. Ann Ig Med Prev E Comunita 2020;32:38–49. https://doi.org/10.7416/ai.2020.2328.
- Nascimento MNR, Gomes EB, Félix ND de C, Rebouças CB de A, Nóbrega MML da, Oliveira CJ de. ICNP® terminology subset for the care of people with heart failure. Rev Bras Enferm 2021;75:e20210196. https://doi.org/10.1590/0034-7167-2021-0196.
- Marucci AR, De Caro W, Petrucci C, Lancia L, Sansoni J. ICNP- International Classification of Nursing Practice: origin, structure and development. Prof Inferm 2015;68:131–40. https://doi.org/10.7429/pi.2015.6822131.
- Masciullo M, Pucci A, Marti F, Latina R, Torretta C, Mitello L, et al. Identificazione di diagnosi infermieristiche NANDA-I e ICNP specifiche per la terapia intensiva: una scoping review. Scenario® - Il Nurs Nella Sopravvivenza 2023;40. https://doi.org/10.4081/scenario.2023.560.
- Skulmoski G, T. Hartman F, Krahn J. The Delphi Method for Graduate Research. J Inf Technol Educ Res 2007;6:001–21. https://doi.org/10.28945/199.
- Nasa P, Jain R, Juneja D. Delphi methodology in healthcare research: How to decide its appropriateness. World J Methodol 2021;11:116–29. https://doi.org/10.5662/wjm.v11.i4.116.
- McMillan SS, King M, Tully MP. How to use the nominal group and Delphi techniques. Int J Clin Pharm 2016;38:655–62. https://doi.org/10.1007/s11096-016-0257-x.
- Taylor E. We Agree, Don’t We? The Delphi Method for Health Environments Research. HERD 2020;13:11–23. https://doi.org/10.1177/1937586719887709.
- Hong QN, Pluye P, Fàbregues S, Bartlett G, Boardman F, Cargo M, et al. Improving the content validity of the mixed methods appraisal tool: a modified e-Delphi study. J Clin Epidemiol 2019;111:49-59.e1. https://doi.org/10.1016/j.jclinepi.2019.03.008.
- Buyukyilmaz, F.,PhD.B.S.N., Kus, Betul,PhD., B.S.N., & Caglar, Seda,PhD., B.S.N. (2020). Nursing diagnoses used in neonatal and adult intensive care unıts: An evaluation of theır suitability according to the nanda-I list. International Journal of Caring Sciences, 13(2), 1148-1154. Retrieved from https://www.proquest.com/scholarly-journals/nursing-diagnoses-used-neonatal-adult-intensive/docview/2462488138/se-2.
- Chianca TCM, Lima APS, Salgado P de O. Nursing diagnoses identified in inpatients of an adult intensive care unit. Rev Esc Enferm U P 2012;46:1102–8. https://doi.org/10.1590/s0080-62342012000500010.
- de Araújo DS, França AFD, Mendonça JKDS, Bettencourt ARDC, Amaral TLM, Prado PRD. Construction and validation of a systematization instrument for nursing in intensive care. Rev Rede Enferm Nordeste 2015;16:461. https://doi.org/10.15253/2175-6783.2015000400002.
- Dutra C, Silveira L, Santos A, Pereira R, Stabile A. Prevalent nursing diagnosis in patients hospitalized with sepsis at the intensive care unit. Cogitare Enferm 2014;19 (4):688–694. https://saude.ufpr.br/revistacogitare/wp-content/uploads/sites/28/2016/10/36801-145118-1-PB.pdf
- Ribeiro CP, Silveira CDO, Benetti ERR, Gomes JS, Stumm EMF. Nursing diagnoses for patients in the postoperative period of cardiac surgery. Rev Rede Enferm Nordeste 2015;16. https://doi.org/10.15253/2175-6783.2015000200004.
- da Silva AM, Bertoncello KCG, Silva TGD, Amante LN, De Jesus SC. Diagnósticos de Enfermagem na Unidade de Terapia Intensiva: Foco no problema e nos riscos. Enferm Em Foco 2021;12. https://doi.org/10.21675/2357-707X.2021.v12.n1.3506.
- Ferreira AM, Rocha EN, Lopes CT, Bachion MM, Lopes JL, Barros ALBM. Diagnósticos de enfermagem em terapia intensiva: mapeamento cruzado e Taxonomia da NANDA-I. Rev Bras Enferm 2016;69:307–15. https://doi.org/10.1590/0034-7167.2016690214i.
- Castellan C, Sluga S, Spina E, Sanson G. Nursing diagnoses, outcomes and interventions as measures of patient complexity and nursing care requirement in Intensive Care Unit. J Adv Nurs 2016;72:1273–86. https://doi.org/10.1111/jan.12913.
![]() This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.