Muhammad Sohrab khan 1, Jihad Hussain 2, Muhammad Ishaq 2, Shams Ul Haq 2,
Hamza Khan 2, Muhammad Shayan 2, Zohaib Hussain 3, Mah Noor Mumtaz 4,
Wajid Hussain 4, Abdur Rahman 2*, Mahnoor Ali 5
- Medical B Ward, Bacha Khan Medical College / MTI Mardan Medical Complex, Mardan, Peshawar, Pakistan.
- Department of Nursing, Elizabeth Rani College of Nursing Mardan, Peshawar, Pakistan.
- Department of Nursing, Institute of Health Sciences, Mardan, Peshawar, Pakistan.
- Department of Biochemistry, Abdul Wali Khan University, Mardan, Peshawar, Pakistan.
- Department IPMH & BS, Khyber Medical University, Khyber Pakhtunkhwa, Pakistan.
* Corresponding author: Abdur Rahman, Department of Nursing, Elizabeth Rani College of Nursing Mardan, Peshawar, Pakistan. E-mail: abdurrahman888889998@gmail.com
Cite this article
ABSTRACT
Introduction: Acid-base balance is one of the most essential physiological terms, which play a crucial role in the examination of the patient and clinical observation. To control the patients well and detect changes when they start to deteriorate, nurses should have a good grasp of acid-base physiology.
Objective: The paper examined the impact of the level of knowledge of acid-base balance on clinical surveillance practices of nurses in Northeastern Pakistan.
Material & Methods: A cross-sectional, correlational, descriptive study was conducted on 403 registered nurses in different clinical settings in Northeastern Pakistan. The questionnaire was structured and validated, and it was completed by over four weeks by five sections: demographics; acid-base knowledge (10 items); clinical monitoring skills (12 items); knowledge to practice application (5 items); and barriers to effective monitoring. The statistical tests included descriptive statistics, Pearson correlation, independent t tests, one way ANOVA and linear regression.
Results: Nurses had high scores on acid-base knowledge (mean of 9.78/10, SD of 0.58) and clinical monitoring skills (mean of 53.8/60, SD of 6.2). There was a great deal of correlation between knowledge and skills (r = 0.82, p = 0.001). Greater qualification, experience, and formal training in ABG was an indicator of superior skills. Heavy workload was the most prevalent (54.1%) and lack of time (36.0%). Knowledge explained 52% of the variance in monitoring skills (R² = 0.52).
Conclusion: The clear understanding of acid-base balance is a key to the formation of clinical monitoring skills of nurses. The enhancement of patient monitoring practices will be achieved by the strengthening of acid-base education and barriers of workload.
Keywords: Clinical monitoring skills, acid -base balance, nurses, Pakistan, nursing education.
INTRODUCTION
One of the fundamental physiologic principles required during the evaluation and observation of patients is acid-base balance. As the first-line caregivers, nurses are very important in the early detection of acid-base disorders. One of their direct impacts on patient outcomes is their ability to detect subtle differences in respiratory patterns, state of consciousness, and vital signs [1]. Systematic observation, assessment, and interpretation of patient data is called clinical monitoring and is one of the core competences that distinguish expert nurses and novices and ensure patient safety [2,3]. Although the nursing curricula addresses the physiology of acid-base, there is most of the time a gap that exists between theory and practice. This gap between theory and practice is an important topic in nursing education with the potential threat to patient safety [4-6]. It has been reported that nursing students performed poorly on written exams, but they failed to apply their learning in the bedside [4,5]. Acid-base disturbances are common in the critically ill patients and are associated with a high mortality. Deviations in the parameters of arterial blood gases are also the foretellers of bad results among patients who are under intensive care [7], low blood pH is also a strong indicator of adverse final results [8]. Septic patients in Pakistan would have metabolic acidosis, and it was associated with fatal outcomes [9]. Physical examination (respiratory rate, depth, pattern, level of consciousness, vital signs) and analysis of diagnostic data, especially arterial blood gas (ABG) are part of clinical monitoring regarding acid-base balance [2,3,10]. The proper understanding of ABG requires a good theoretical foundation [10-12]. Nurses who understand the pathophysiology of acid-base have a greater advantage to diagnose the beginning of deterioration, care formulation, effective communication with the healthcare team, and predict complications [1,2,4,7-9,10-14]. There are a number of factors that determine the capability of nurses to use acid-base knowledge in clinical practice. Increased level of education, deep clinical experience, and formal training in ABG have been associated with better monitoring skills [1,3]. On the other hand, workload, time, lack of confidence, and inadequate continuing education are the obstacles [3,9,15]. Nursing education in Pakistan has evolved in the last thirty years. Pakistan Nursing Council regulates nursing education and licensure and the Generic Bachelor of Science in Nursing program includes pathophysiology and clinical rotations [3,9]. However, the evidence on the association between theoretical knowledge of acid-base and clinical monitoring skills in the Pakistani context among nurses is lacking [3,9]. Therefore, this study was aimed at exploring the role that the classification of acid-base can play in the building of clinical monitoring proficiency in nurses in Northeastern Pakistan.
Aim
This research will focus on the importance of acid-base knowledge in developing clinical monitoring competencies in nurses in Northeastern Pakistan.
Objective: The research questions of this research are as follows:
- To determine the degree of acid-base knowledge in nurses in Northeastern Pakistan.
- To determine the self-reported degree of clinical monitoring skills in nurses working in Northeastern Pakistan.
- To establish the relationship between the knowledge of acid-base and clinical monitoring skills of the nurses.
- To compare clinical monitoring skills among various demographic and professional groups such as gender, qualification, years of experience and the trainee status of ABG training.
- To determine the obstacles that do not allow the nurses to monitor patients effectively to detect acid-base imbalances.
- To produce evidence to guide nursing education and practice on the management of acid-base balances.
MATERIALS AND METHODS
Study Design and Setting
The study was a descriptive, cross-sectional, correlational study, which was carried out across four weeks among the Registered Nurses (RNs) in various clinical environments in Northeastern Pakistan. The purpose was to test the effect of the knowledge of acid-base concepts on the clinical monitoring ability of nurses.
Sampling and Eligibility
Study Period
The research was conducted for four weeks, between 1 December 2025 and 29 December 2025.
Type of Study
The relationship between acid-base knowledge and clinical monitoring competence in nurses was examined in a descriptive cross-sectional correlational design.
Study Population
The sample included RNs who were employed in a tertiary hospital, district hospital, private clinic, and community health center in Northeastern Pakistan. The student nurses, post RN nurses and diploma-nurse graduates were not included to give similar clinical experience and training.
Inclusion Criteria
- Registered Nurse and valid license.
- In use in a clinical environment.
- Willing to participate
- Capable of comprehending and filling the questionnaire.
Exclusion Criteria
- Unregistered (yet) student nurses.
- Nurses out on long leave or out during data collection.
- Informed consent was not given by nurses.
Sample Size Calculation
The OpenEpi v3.0 was used to calculate the sample size based on Cochran formula:
Where: Z = 1.96 (95% confidence level). p = 0.50 (proportion expected; this maximizes the sample size since there was no previous research in this population) and d = 0.05 (margin of error).
Since we did not know the RN total population, we did not make any correction in terms of a finite population. In this way, the minimum number of nurses was 385. All available and qualifying RNs were invited to minimize the non-response bias. There was adequate statistical power and 403 nurses were responding.
Sampling Technique
Non-probability convenience sampling technique was selected due to the practicality: access to the participants, time and the research exploratory nature. There was no possibility to use random or probability-based sampling since a full sampling frame of all registered nurses in all clinical settings in Northeastern Pakistan was not available. Moreover, the nurses were not always available on their units since they were on shifts, leaves, and caring of patients, which made the use of probability-based sampling impossible. We recognize that convenience sampling can be a source of selection bias because nurses who were available and willing to take part might differ with those who were not. This restricts the generalization of the findings.
Participants were recruited through personal contacts
Several clinical sites that were chosen offered administrative assistance to the nurses. Recruitment was done using nursing supervisors, head nurses and clinical coordinators who used the official communication channels to pass the information about the study.
Context of Participation
The paper questionnaires were issued within the clinical setting. They could be done by nurses during breaks or after shifts. The study details were provided in a concise manner and nurses were not pressured to join in the study.
Voluntary Participation
The participation was on a voluntary basis. Nurses were given a clear information regarding the objectives of the study, procedures and possible benefits and their informed consent form was signed. They were also promised that their participation would not have any impact on their jobs or professional status.
Bias Mitigation
Although convenience sampling may introduce self-selection bias, several measures were implemented to minimize this risk. All qualified nurses were invited irrespective of previous interest and knowledge. There were several reminders which increased representativeness. The fact that the study was represented by various clinical settings in the Northeastern part of Pakistan also minimized bias.
Ethical Considerations
The research received the consent of the Institutional Review Board (IRB) of Abdul Wali Khan University, Mardan.
- IRB Title: the institutional review board, Abdul Wali Khan University Mardan.
- IRB Number: IRB/2025/Acid-Base/Biochem/Nursing/0011
- Approval Date: 21-Nov-2025
The subjects were assured confidentiality, anonymity and the freedom to withdraw whenever they wished without consequences. No personal identifiable data was gathered, all the data were coded by number and safely kept by the research team.
Informed Consent
All the participants signed written consent before data collection. The consent form described the purpose of the study, which was voluntary, the right to leave, and to confidentiality.
Incentives
No economic or non-economic rewards were provided to take part.
Instruments
Data Collection Tool
Data were collected using an organized and tested questionnaire that was based on previous and confirmed research about the knowledge of acids and bases and clinical monitoring proficiencies. The questionnaire was created based on regular nursing teaching material and subject-matter experts revised the content of the questionnaires to ensure the content validity.
The questionnaire has been categorized into five parts as reported in Table 1.
Section Content Number of Items A Demographic Characteristics 6 items B Acid-Base Understanding (Knowledge Test) 10 items C Clinical Monitoring Skills (Self-Assessed Competency) 12 items D Knowledge-to-Practice Application 5 items E Barriers to Effective Monitoring 1 item (multiple response) Table 1. Section Number of Items Content.
Section A
Demographic Characteristics such as age, gender, qualification, years of experience, work area and ABG training status were included.
Section B
Acid-Base Understanding – involved ten multiple-choice question-based tests that evaluate pH, PaCO 2, -HCO 3, nature of disorders, compensatory responses, and typical clinical situations. One point was given a correct answer, making the possible score between 0 and 10.
Section C
Clinical Monitoring Skills- included twelve questions assessing self-reported abilities in respiratory assessment, ABG and risk identification, prioritisation and communication. The scale was based on a 5-point Likert scale:
- 1 Never/Not Confident,
- 2 Rarely/Slightly Confident,
- 3 Sometimes/Moderately Confident,
- 4 Often/Very Confident,
- 5 Always/Extremely Confident.
Total scores ranged from 12 to 60.
Section D
Knowledge-to-Practice Application – consisted of five questions which tested how knowledge is implemented in clinical practice.
Section E
Barriers to Effective Monitoring – had one item which provided the respondent with multi-choice possibility of selecting more than one perceived barrier.
Validity and Reliability
Two experts a nursing educator and a clinical instructor validated content validity. Face validity was developed through pilot testing ten registered nurses. Cronbach alpha (0.85) was used to measure Section C internal consistency, which was good.
Content validity was established by two experts (a nursing educator and a clinical instructor). Pilot testing was carried out to develop face validity using ten registered nurses.
The alpha of Cronbach was determined to determine the internal consistency of every section of the questionnaire:
- Section B (10 items): α = 0.81.
- Section C (12 items): α = 0.85.
- Section D (5 items): α = 0.79.
The values are all above the acceptable level of 0.70, which means good internal consistency.
Data Collection Procedure
The questionnaire was written and sent out to the clinical situations of participants. The researcher visited the selected health-care facilities at convenient times, approached the potential participants, informed them about the study, and invited them to participate in the study. Informed consent was received by means of written informed consent. The questionnaires were given out and collected on the same day to optimise the response rates. The collection of data went on till the required sample size was achieved.
Statistical Analysis
The data were read with the help of SPSS version 26. All the variables were computed using descriptive statistics. Means, standard deviations (SD), median, interquartile range (IQR), minimum, and maximum were presented as the variables were continuous (age, knowledge scores, skills scores, and so on). Categorical variables (gender, qualification, years of experience, work area, ABG training status) were described in the form of frequencies and percentages.
Shapiro-Wilk test was used to test the normality of knowledge and skills scores; p-values were found to be greater than 0.05, which proves that knowledge and skills scores were distributed normally and, accordingly, matches the use of parametric tests.
Pearson correlation coefficients were used to test a correlation between skills scores and total knowledge scores, and the assumption of linearity and normality was checked and fulfilled.
Independent-samples t-tests were applied to test the difference in mean scores of knowledge and skills between male and female nurses.
ANOVA was used to determine the difference between the mean scores of knowledges and skills by comparing groups of years of experience, the level of qualification and the area of work. The reason why the test was selected was that the independent variables had more than two levels. Premeditative homogeneity of variance and normality were investigated: the Shapiro–Wilk test demonstrated non-significant p-values (p > 0.05) in all groups, and Levene test showed that variance was equal (p > 0.05). Type I error was controlled when ANOVA showed significant differences by Tukey, Honestly Significant Difference (HSD) post-hoc tests.
The skills scores were predicted using knowledge score as the only predictor through simple linear regression. Multiple linear regression was used to determine the independent predictors of the skills scores, such as knowledge score, years of experience, qualification, and status of ABG training. All predictors were included using the enter method. Linearity, independence of residuals, homoscedasticity, and normality of residual assumptions were met. The 95% confidence interval for correlation and regression coefficients was reported to show precision.
Regression assumptions verification: The individual predictive effect of academic knowledge score of acid–base balance on clinical monitoring skills was assessed using simple linear regression. Multiple linear regression was used to determine the independent predictors of clinical monitoring skills after controlling for possible confounders, including qualification, years of experience, and ABG training status.
The linear regression assumptions were checked before analysis. Linearity was assessed by visual inspection of scatterplots of residuals against predicted values, which did not reveal any discernible pattern. Normal distribution of residuals was verified using the Shapiro–Wilk test (p > 0.05) and Q–Q plots. Homoscedasticity was assessed using the Breusch–Pagan test (p > 0.05), confirming constant variance of residuals. Multicollinearity, where multiple regression was used, was evaluated using variance inflation factor (VIF) values, which ranged from 1.12 to 1.89, indicating no significant multicollinearity. Independence of residuals was tested using the Durbin–Watson test (value = 1.98), indicating no autocorrelation.
The statistical significance level was established at p<0.05 and all the tests were two-tailed.
RESULTS
Demographic characteristics
There were 403 registered nurses who took part in the study. The average age of the sample was 34.8 (SD 7.2) and was between 22 and 52 years. The demographic characteristics are provided in Table 1, and the rest of the relevant findings are shown in Figures 1,2,3,4.
Variable Category Frequency (n) Percentage (%) Gender Male 207 51.4 Female 196 48.6 Qualification Diploma 253 62.8 BSN 117 29 MSN 33 8.2 Experience < 1 year 33 8.2 1-5 years 132 32.8 6-10 years 123 30.5 > 10 years 115 28.5 ABG Training Yes 310 76.9 No 93 23.1 Training Recency < 6 months 48 15.5 6-12 months 54 17.4 > 1 year 208 67.1 Table 1. Demographic Traits of Participants
Figure 1 indicates the gender distribution of the 403 registered nurses. The percentage distribution of males and females is 51.4 (207 nurses) and 48.6 (196 nurses), respectively, which is rather equal.
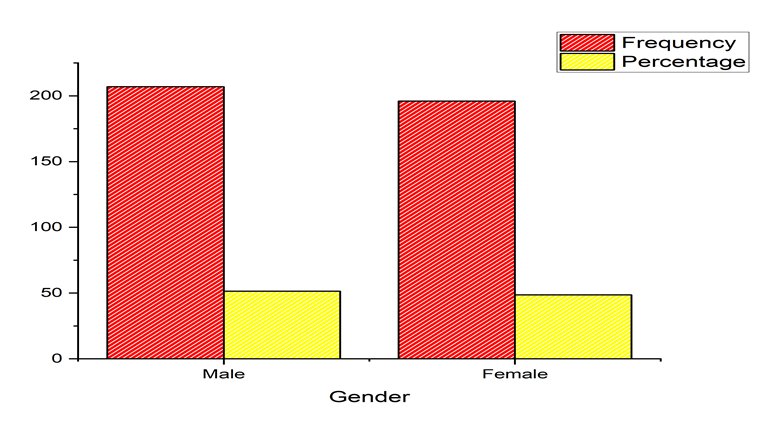
Figure 1. Gender of Participants.
Figure 2 shows the level of education of the nurses. The majority of them had a Diploma in Nursing (62.8% of 253 nurses), then a Bachelor of Science in Nursing (BSN) with 29.0% (117 nurses), and finally a Master of Science in Nursing (MSN) with 8.2% (33 nurses).
Figure 2. Qualification of the participants
Figure 3 provides the clinical experience of the nurses. The highest number was 1-5 years experience (32.8, 132 nurses), then 6-10 years (30.5, 123 nurses), over 10 years (28.5, 115 nurses) and less than one year (8.2, 33 nurses). The majority of nurses (76.9%, n=310) had received formal training in ABG, while 23.1% (n=93) had not.
Figure 4 shows the latest date in which the 310 trained nurses received the ABG training.
The majority (67.1%, 208 nurses) of them were trained more than one year ago, 17.4 percent (54 nurses) trained 6-12 months ago, and 15.5 percent (48 nurses) had been trained within the past six months.
Figure 3. Experience of the participants
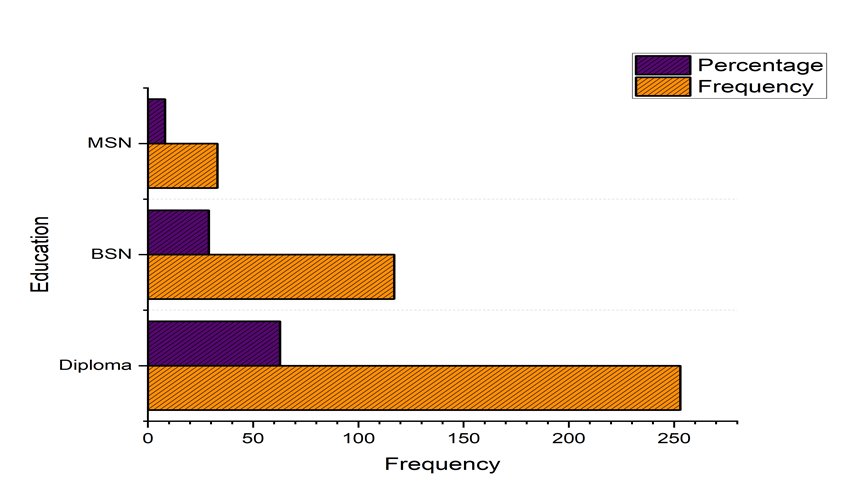
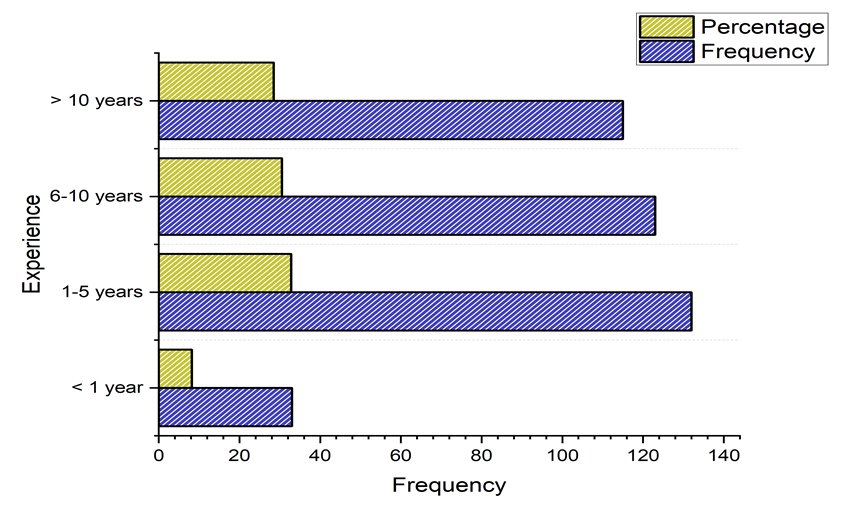
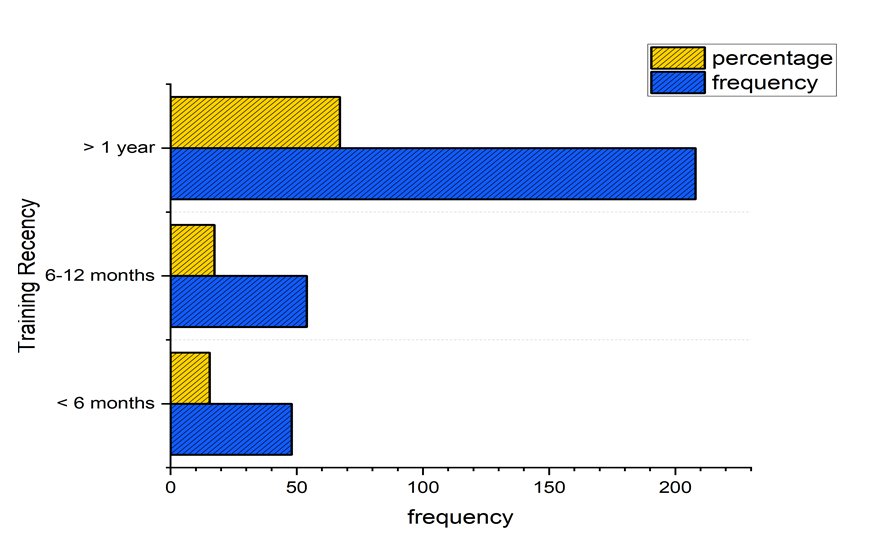
Figure 4. Training Recency of the participants
To Test the Acid-Base Knowledge Level of Nurses
Section 10 items assessed the knowledge that nurses had on the acid-base balance. Descriptive Statistics of Knowledge and Skills Scores were shown in Table 2.
Variable Mean SD Median Min Max Knowledge Score (out of 10) 9.78 0.58 10 8 10 Skills Score (out of 60) 53.8 6.2 56 38 60 Knowledge Score Distribution (Score) Frequency (n)
Percentage (%)
8 16 4 9 26 6.5 10 361 89.5 Skills Score Distribution (Score Range)
Frequency (n)
Percentage (%) 35–40 12 3 41–45 42 10.4 46–50 84 20.8 51–55 70 17.4 Table 2. Descriptive Statistics and Distribution of Knowledge and Skills Scores (N=403).
The mean score was 9.78 of 10 (SD=0.58), which means that there is high knowledge.
Very high percentage (89.5%) (n=361) scored 10, which depicts a very good understanding of acid-base concepts.
To Evaluate Self-Reported Clinical Monitoring Skills with the Nurses
Clinical monitoring skills were measured using section C (12 items) on a 5-point Likert scale. The average was 53.8 of 60 (SD = 6.2), which was high self-report competence. The highest range (56-60) had almost half (48.4) of the total scores, which reflects good monitoring skills.
To Establish the Relationship between the Acid-Base Knowledge and Clinical Monitoring Skills
Pearson’s correlation analysis was conducted to examine the relationship between knowledge scores (Section B) and skills scores (Section C). As shown in Table 2, a statistically significant, positive, and strong correlation was observed. Nurses with higher knowledge scores also demonstrated higher clinical monitoring skills scores.
Variable Pair Correlation Coefficient (r) 95% CI p-value Knowledge Score & Skills Score 0.82 [0.78, 0.86] < 0.001 Note: Pearson correlation assumptions were checked before analysis. The Shapiro-Wilk test was used to test normality (p > 0.05). Scatterplots were used to determine the linearity and the relationship was linear. No extreme outliers were observed (no values more than ±3 standard deviations of the mean) Table 3. Pearson coefficient of Knowledge and Skills Scores.
To Compare Clinical Monitoring Skills in the various demographic and professional groups
Comparison by Gender
The difference between the scores of the skills of male and female nurses did not show significant differences (p=0.156).
Comparison of Qualification
Higher level qualifications related with better clinical monitoring skills.
Comparison by Experience
As one becomes more skilled the skills increase. The distance between all the experience groups is significant (p < 0.01).
Comparison of ABG Training status
Table 3 summarizes differences in clinical monitoring skills scores according to demographic and professional variables, as assessed through t‑tests and one‑way ANOVA.
ABG trained nurses scored significantly higher (p < 0.001). Central Finding: The greater the level of qualifying is, the greater the monitoring skills. Post-hoc tests indicate that the MSN nurses had scores that were high as compared to the diploma nurses (p = 0.006).
Variable Categories N Mean Skills Score SD Statistic p-value Gender Male 207 54.2 6 t = 1.42 0.156 Female 196 53.4 6.4 Qualification Diploma 253 53.2 6.4 F = 4.89 0.008 BSN 117 54.6 5.8 MSN 33 56.1 5.2 Experience < 1 year 33 44.8 4.2 F = 48.2 < 0.001 1-5 years 132 51.2 5.1 6-10 years 123 55.4 5.3 > 10 years 115 57.8 4.6 ABG Training Yes 310 55.9 5.1 t = 12.4 < 0.001 No 93 46.8 5.5 Table.4 Comparison of Clinical Monitoring Skills by Demographic and Professional Groups
Knowledge-to-Practice Application
To assess the application of knowledge into clinical practice, Section D comprised five statements rated on a 5‑point Likert scale. Table 5 summarizes nurses’ responses in terms of mean scores and standard deviations.
Statement Mean SD D1: Theoretical knowledge helps recognize problems earlier 4.65 0.48 D2: Consciously apply acid-base concepts when assessing patients 4.42 0.69 D3: There is a gap between class learning and clinical practice 2.82 0.87 D4: Confident connecting lab results to physical assessment 4.38 0.71 D5: Continuing education would improve monitoring skills 4.92 0.27 Table 5. Knowledge-to-Practice Application Statements.
Key Findings:
- 8 percent said they agreed or strongly agreed that theoretical knowledge helps in early problem recognition.
- 1% said that they are aware of using acid-base concepts.
- Perceived gap between learning and practice in classrooms was seen in only 18.6% of the people.
- 5 percent strongly agreed that the continuation of the education would advance monitoring skills.
To Determine Bars to Counterproductive Nursing Care in the Surveillance of Acid-Base Imbalances in the Patient
Participants were asked to identify perceived barriers to effective acid–base monitoring. Table 6 summarizes the frequency and percentage distribution of the reported barriers, with heavy workload identified as the most common impediment.
Barrier Frequency (n) Percentage (%) Heavy workload / too many patients 218 54.1 Lack of time 145 36 Lack of confidence in interpreting results 32 7.9 Insufficient training 28 6.9 Limited access to ABG results 12 3 Lack of experienced staff to consult 8 2 None 18 4.5 Table 6. Hurdles to Successful Surveillance.
The most frequently reported barriers to effective acid–base monitoring were heavy workload and lack of time.
Regression Analysis
Simple Linear Regression
Simple linear regression was used to determine the prediction of clinical monitoring skills using acid-base knowledge scores.
Clinical monitoring skills were explained by knowledge score 0.52. The skills score increased by 8.82 points with each one-point increment in the knowledge score.
Model summary R2 F-statistic df numerator df denominator p-value 0.52 441.0 1 401 <0.001 Predictor Β SE t-statistic p-value 95% CI Knowledge Score 8.82 0.42 21 < 0.001 [7.99, 9.65] Table 7. Simple Linear Regression Analysis.
Multiple Linear Regression
To identify clinical monitoring skills as related to the knowledge score, qualification, experience, and status of the ABG training, the multiple linear regression was performed.
Model summary R2 F-statistic df numerator df denominator p-value 0.81 425.6 4 398 <0.001 Predictor β SE t-statistic p-value 95% CI Knowledge Score 7.45 0.38 19.6 < 0.001 [6.70, 8.20] Qualification 1.12 0.28 4 < 0.001 [0.57, 1.67] Experience 1.89 0.22 8.6 < 0.001 [1.46, 2.32] ABG Training (Yes) 4.32 0.48 9 < 0.001 [3.38, 5.26] Table 8. Multiple Linear Regression Analysis.
The entire model explained 81 percent of the variance in clinical monitoring skills. Knowledge score was the most significant one with experience coming in next, followed by ABG training status and qualification.
Critical Discussion of the Results
The researchers concluded that the majority of the nurses had a high level of knowledge and a good clinical monitoring ability associated with acid-base balance. However, on closer examination of the individual survey questions and subgroup analyses, there is a more detailed image. The nurses were not equally effective in exhibiting flawless competency in all the clinical monitoring activities. The level of knowledge was very high and K=89.5 and 10 is the highest possible mark, which means that the theoretical basis is strong. Contrastingly, the variation in terms of skills scores was less: 48.4 percent were in the upper tack (56-60), 20.8 percent were in the mid-range (46-50). This implies that academic knowledge may not necessarily become an ideal clinical practice. Self-reported skills differed even in the case of nurses who scored perfectly in terms of knowledge, which suggests that other variables have an impact on performance. Demographic analysis of skills scores was important in identifying some trends. Nurses who are less than one year experienced the lowest average skills score (44.8/60), and those who are over ten years experienced the highest (57.8/60). The gradual change highlights the importance of experiential learning but also brings up the issue of the willingness of novice nurses to be able to monitor the patients in isolation. The significant difference in means of 13 between novice and experienced nurses indicates that the development of skills with the help of structured mentorship might be faster. Formal ABG training was associated with much higher scores in skills (55.9 vs. 46.8, p 0.001). Nevertheless, 23.1 percent of nurses were not sufficiently trained on the use of ABG, which stands as a serious gap in the workforce susceptibility. On the Knowledge-to-Practice Application section, 95.8 percent of the nurses concurred that theoretical knowledge aids in diagnosing the problems at an earlier stage, but only 90.1 percent agreed to be conscious in applying the concepts of acid-base when evaluating patients. The 5.7 percent disparity is the indication of a small yet significant gap between the recognition and the regular use. Moreover, 18.6 per cent of nurses indicated that they felt disconnected between their classroom and clinical practice indicating that theory-practice gap was still present in some. The barriers analysis indicated that the most frequent barriers are heavy work load (54.1) and time (36.0). Such systemic conditions can hamper the implementation of competencies despite nurses being informed. The quality of monitoring is also a problem due to the high incidence of heavy workload which was the main area of concern regarding patient to nurse ratio. The regression models (R2 = 0.52; 0.81) and the correlation analysis (r = 0.82) indicate that there is a medium-high correlation between knowledge and skills. But the complete model predicts 81 per cent of the variance leaving 19 per cent unaccounted. The remaining variance can be due to factors that cannot be measured including personal motivation, cognitive burden, work culture, or access to mentors. When most nurses were found not lacking in confidence in their skills, quite a significant number showed concerns. Obstacles connected to the absence of confidence (7.9%), as well as the lack of training (6.9%), indicate that the knowledge does not necessarily ensure the lack of confidence or the positive attitude. These results highlight the importance of developing confidence-building techniques and workload management of nursing education and practice. In general, the findings suggest that even though the nurses are well-equipped in terms of acid-base knowledge, the usage of that knowledge in clinical monitoring is experience-dependent, training-dependent, as well as systemic. The educational interventions must be oriented not just on acquiring the knowledge, but also confidence development, exposure to practical experience in simulation and training exercises, and institutional concerns (workload, time limitations) to facilitate bedside implementation.
DISCUSSION
This paper discussed the relationship between acid-base knowledge and clinical monitoring competencies among nurses in Northeastern Pakistan. The results showed that the level of acid-base knowledge (mean = 9.78/10, SD = 0.58) and self-reported clinical monitoring skills (mean = 53.8/60, SD = 6.2) was high and there was a positive correlation between the two variables (r = 0.82, p < 0.001). Such results imply that an excellent theoretical basis in acid-base physiology is inextricably linked with improved clinical monitoring among nurses. The level of knowledge in this study (89.5% stating 10/10) is in line with Dakic et al. [1] in which interactions teaching method enhanced the students’ knowledge of acid-base physiology. On the same note, Brown et al. [2] observed that nursing students excel on written exams, but it is difficult to exercise the knowledge in clinical practice, and this correlates with the current research in which some respondents show a theory-practice gap. The correlation between knowledge and skills (r = 0.82) is strong, which is similar to those of international studies. In their study, Nassar and Schmidt [15] and Prasad et al. [18] noted that proper interpretation of ABG needs a sound theoretical foundation, which explains why we have found that knowledgeable nurses report higher monitoring skills. Moreover, Endacott et al. [5] discovered that successful monitoring involves the combination of technical skills and clinical reasoning, which is also consistent with the high level of skills given by our participants.
No differences in clinical monitoring skills were significant between the genders (p = 0.156), which concurs with Zhang et al. [10], who had no gender differences in metabolic abnormalities in nurses. But, higher qualified nurses showed much better monitoring skills (F = 4.89, p = 0.008), with the MSN-prepared nurses scoring higher than the diploma nurses (p = 0.006). This correlates with the study of Baiee and Ali [19] who observed that increased education is related to enhanced knowledge and skills. Clinical monitoring skills had a strong association with experience (F = 48.2, p < 0.001), which is consistent with Endacott et al. [5], who have found that advanced nursing competencies are acquired with time through clinical exposure. In the same vein, formal ABG training was also connected with much higher skills scores (t = 12.4, p < 0.001), which confirms the results of Fujimoto et al. [16], Zeserson et al. [17], and Prasad et al. [18] about the importance of structured training. Most of the nurses (95.8% said that theoretical knowledge would help them identify problems early and 96.5% said strongly that further education would enhance their monitoring abilities. These results indicate that continuous professional growth is necessary, as it is also stressed by Baiee and Ali [19]. The most common obstacles to effective monitoring were heavy workload (54.1) and lack of time (36.0). These findings are in line with those of Zhang et al. [10] who found that workload and shift-related stress are significant determinants of nurse behavior. These obstacles are especially applicable to the Pakistani environment, where the nurse-to-patient ratios are difficult [20]. The regression analysis showed that the knowledge score alone was sufficient to explain 52 percent of the variance in clinical monitoring skills (R2 = 0.52), whereas the complete model that contains knowledge, qualification, experience, and ABG training was sufficient to explain 81 percent (R2 = 0.81). Knowledge score was the strongest predictor (β = 7.45, p < 0.001), followed by experience (β = 1.89, p < 0.001), ABG training (β = 4.32, p < 0.001), and qualification (β = 1.12, p < 0.001).
CONCLUSION
This paper has shown that there is a close relationship between acid-base education and clinical monitoring competency among nurses in Northeastern Pakistan. These findings revealed that nurses had good acid-base knowledge (mean = 9.78/10) and clinical monitoring skills (mean = 53.8/60), and the two variables had a strong positive correlation (r = 0.82, p < 0.001). Increased qualification, experience, and formal training on ABG were linked to better monitoring skills. The barriers to effective monitoring were most often reported, 54.1%, and lack of time (36.0%).
Regression analysis found the best predictor of clinical monitoring skills is the acid-base knowledge, which explains 52% of variance. The entire model comprising experience, qualification, and training in ABG explained 81 percent of the variance. These results suggest that theoretical understanding of acid-base balance is one of the factors correlated with clinical monitoring competency in nurses.
Recommendation
For Nursing Education
The teaching of acid-base contents should be supported by interactive and case-based methods through nursing education programs to increase knowledge and memory [1,2]. The use of simulation-based training in the curricula is necessary to provide the students with a hands-on experience of ABG interpretation and clinical monitoring practice [5,7].
For Clinical Practice
A formal training process of practicing nurses should be developed by healthcare institutions since formal training was significantly associated with a higher level of monitoring skills [15,17,18]. Continuous education programs must be carried out on a regular basis to sustain and improve clinical competencies, particularly in acid -base management [19].
In the case of Healthcare Institutions
Workload and time issues should be handled with institutional leadership by maximizing the number of nurses per patient, since the issue of workload per patient is the most prevalent one that is reported as an obstacle to effective monitoring [10,20]. ABG results should be made available in a timely manner to assist in clinical decision-making and to enable some timely interventions [12,16].
For Future Research
Objective data in clinical monitoring skills including direct observation or simulation-based measures should be used in future studies to improve self-reported data [7]. Multi-centered research in the various areas of Pakistan is required to enhance the overall external validity of the results [20].
Limitations
This study has several limitations. To begin with, convenience sampling will restrict the generalizability of the findings to the whole population of nurses in Pakistan. Second, the skills reported by the self might not be the ones that are objective in clinical performance, because perceptions are not necessarily associated with competency. Third, the study design is cross-sectional and therefore no causal inferences can be made; despite a strong association, it is not possible to imply causality. Fourth, the research was only done in a single region (Northeastern Pakistan) and this could not be generalized to other geographical regions. Fifth, causal relationships cannot be drawn because of the cross-sectional design. The interrelationships mentioned in this research are not causal but correlational. These limitations could be overcome by future studies based on probability sampling, objective competency tests, and multi-center studies.
Funding statement
This research did not receive any specific grant from funding agencies in the public, commercial, or not for profit sectors.
Local ethics Committee Approval
The study was conducted in accordance with international ethical guidelines of conducting research with human participants. This was done to safeguard the rights, safety and well-being of participants by ensuring we had ethical approval prior to data collection. The study plan was discussed and reviewed by the Institutional Review Board (IRB) of Abdul Wali Khan University, Mardan.
- IRB Title: The Institutional Review Board, Abdul Wali Khan University Mardan
- IRB Number: IRB/2025/Acid-Base/Biochem/Nursing/0011.
- Date of Approval: November 21, 2025
The involvement was completely voluntary. The purpose, methodology, possible benefits and the right of the registered nurses to discontinue the study were explained to them without any penalty to their job or personal status. All the participants signed consent papers prior to data collection.
No personal identifiers were obtained, which guaranteed confidentiality and anonymity. Questionnaires were coded in numbers, and all the data were stored safely, in a place where only the research team can access. The data was only utilized in terms of academic and research purposes. The research did not produce any physical, mental, or professional damage. It was not a sensitive topic, and the participants were not required to answer any question that would not be comfortable to them, which was connected to the topic (acid-base understanding and clinical monitoring skills).
Conflict of interest
The authors do not claim any conflicts of interest.
Authors’ contribution
The conceptualization was done by Abdur Rahman and Jihad Hussain and the study design. The methodology and the instruments were developed by Shams Ul Haq, Zohaib Hussain, and Muhammad Shayan. Shams Ul Haq, Mah Noor Mumtaz and Wajid Hussain organized data collection and fieldwork. Zohaib Hussain, Mahnoor Ali and Abdur Rahman took part in the data analysis and interpretation. Muhammad Sohrab Khan, Muhammad Ishaq and Hamza Khan helped in the literature review, drafting of the manuscript and initial validation of data. Muhammad Shayan helped in logistics of the fieldwork and data entry. Abdur Rahman led the research, optimized the methodology, and supervised the writing, revision, and final approval of the manuscript.
The final version of the manuscript was approved by all the authors.
Additional Author Information
The email addresses and ORCID identifiers of the authors are reported below.
Muhammad Sohrab Khan: email: sohrab_dr2002@hotmail.com; ORCID: Not available
Jihad Hussain: email: legendenterprise094@gmail.com; ORCID: 0009-0009-4914-9045
Muhammad Ishaq: email: mishaqlkr0349@gmail.com; ORCID: 0009-0006-5906-1854
Shams Ul Haq: email: qaris729@gmail.com; ORCID: 0009-0004-6055-466X
Hamza Khan: email: khankhan983933@gmail.com; ORCID: 0009-0003-7618-7967
Muhammad Shayan: email: shayanmuhammad847@gmail.com; ORCID: 0009-0007-3498-828X
Zohaib Hussain: email: zk4542471@gmail.com; ORCID: Not available
Mah Noor Mumtaz: email: mahnoor@awkum.edu.pk; ORCID: 0009-0004-3699-7559
Wajid Hussain: email: wajid.awkum@gmail.com; ORCID: 0009-0007-4307-4287
Abdur Rahman: email: abdurrahman888889998@gmail.com; ORCID: 0009-0008-2170-146X
Mahnoor Ali: email: mahnorralimdcat2022@gmail.com; ORCID: 0009-0003-6475-2607
Acknowledgements
The authors are grateful to all registered nurses who took part in this study and also recognize the assistance of nursing supervisors, head nurses, and clinical coordinators that were used during recruitment.
Application of Artificial Intelligence Tools
No artificial intelligence software was applied other than a regular grammar and spell.
REFERENCES
- Dakic T, Cvetic Antic T, Jevdjovic T, Lakic I, Ruzicic A, Vujovic P. Balancing act: enhancing student comprehension of acid-base physiology through interactive, system-based teaching. Advances in Physiology Education. 2025;49(4):855-61. doi: 10.1152/advan.00133.2025.
- Brown CE, Henry ML, Hyslop RM. Identifying relevant acid–base topics in the context of a prenursing chemistry course to better align health-related instruction and assessment. Journal of Chemical Education. 2018;95(6):920-7. doi: 10.1021/acs.jchemed.7b00830.
- Jennings KM. The Roy adaptation model: a theoretical framework for nurses providing care to individuals with anorexia nervosa. Advances in Nursing Science. 2017;40(4):370-83. doi: 10.1097/ANS.0000000000000175.
- Bezuidenhout MC, Wiese OJ, Moodley D, Maasdorp E, Davids MR, Koegelenberg CF, et al. Correlating arterial blood gas, acid–base and blood pressure abnormalities with outcomes in COVID-19 intensive care patients. Annals of Clinical Biochemistry. 2021;58(2):95-101. doi: 10.1177/0004563220972539.
- Endacott R, Scholes J, Jones C, Boulanger C, Egerod I, Blot S, et al. Development of competencies for advanced nursing practice in intensive care units across Europe: A modified e-Delphi study. Intensive and Critical Care Nursing. 2022;71:103239. doi: 10.1016/j.iccn.2022.103239.
- Das R, Sobi RA, Sultana AA, Nahar B, Bardhan PK, Luke L, et al. A double-blind clinical trial to compare the efficacy and safety of a multiple amino acid-based ORS with the standard WHO-ORS in the management of non-cholera acute watery diarrhea in infants and young children: “VS002A” trial protocol. 2022;23(1):706. doi: 10.1186/s13063-022-06601-5.
- de Menezes HF, Camacho AC, de Sousa PA, Primo CC, Ferreira LB, da Silva RA. Validation of Nursing Diagnoses for people with chronic kidney conditions on conservative treatment. Revista da Escola de Enfermagem da USP. 2021;55:e20200396. doi: 10.1590/1980-220X-REEUSP-2020-0396.
- Zemlin AE, Sigwadhi LN, Wiese OJ, Jalavu TP, Chapanduka ZC, Allwood BW, et al. The association between acid–base status and clinical outcome in critically ill COVID-19 patients admitted to intensive care unit with an emphasis on high anion gap metabolic acidosis. Annals of Clinical Biochemistry. 2023;60(2):86-91. doi: 10.1177/00045632221134687.
- Chatchatee P, Nowak-Wegrzyn A, Lange L, Benjaponpitak S, Chong KW, Sangsupawanich P, et al. Tolerance development in cow’s milk–allergic infants receiving amino acid–based formula: A randomized controlled trial. Journal of Allergy and Clinical Immunology. 2022;149(2):650-8. doi: 10.1016/j.jaci.2021.06.025.
- Zhang H, Wang J, Zhang S, Tong S, Hu J, Che Y, et al.Relationship between night shift and sleep problems, risk of metabolic abnormalities of nurses: a 2 years follow-up retrospective analysis in the National Nurse Health Study (NNHS). International Archives of Occupational and Environmental Health. 2023;96(10):1361-71. doi: 10.1007/s00420-023-02014-2.
- Pépin M, Klimkowicz‐Mrowiec A, Godefroy O, Delgado P, Carriazo S, Ferreira AC, et al. Cognitive disorders in patients with chronic kidney disease: approaches to prevention and treatment. European Journal of Neurology. 2023;30(9):2899-911. doi: 10.1111/ene.15928.
- Sanghani H, Bansal S, Parmar V, Shah R, Sanghani DH, Parmar Sr V. Study of arterial blood gas analysis in moderate-to-severe COVID-19 patients. Cureus. 2022;14(7):e26715. doi: 10.7759/cureus.26715.
- Kieninger M, Sinning A, Vadász T, Gruber M, Gronwald W, Zeman F, et al. Lower blood pH as a strong prognostic factor for fatal outcomes in critically ill COVID-19 patients at an intensive care unit: A multivariable analysis. PLoS One. 2021;16(9):e0258018. doi: 10.1371/journal.pone.0258018.
- Moreno-Perez O, Leon-Ramirez JM, Fuertes-Kenneally L, Perdiguero M, Andres M, Garcia-Navarro M, et al. Hypokalemia as a sensitive biomarker of disease severity and the requirement for invasive mechanical ventilation requirement in COVID-19 pneumonia: a case series of 306 Mediterranean patients. International Journal of Infectious Diseases. 2020;100:449-54. doi: 10.1016/j.ijid.2020.09.033.
- Nassar BS, Schmidt GA. Estimating arterial partial pressure of carbon dioxide in ventilated patients: how valid are surrogate measures?. Annals of the American Thoracic Society. 2017;14(6):1005-14. doi: 10.1513/AnnalsATS.201701-034FR.
- Fujimoto S, Suzuki M, Sakamoto K, Ibusuki R, Tamura K, Shiozawa A, et al. Comparison of end-tidal, arterial, venous, and transcutaneous PCO2. Respiratory Care. 2019;64(10):1208-14. doi: 10.4187/respcare.06094.
- Zeserson E, Goodgame B, Hess JD, Schultz K, Hoon C, Lamb K, et al. Correlation of venous blood gas and pulse oximetry with arterial blood gas in the undifferentiated critically ill patient. Journal of Intensive Care Medicine. 2018;33(3):176-81. doi: 10.1177/0885066616652597.
- Prasad H, Vempalli N, Agrawal N, Ajun UN, Salam A, Subhra Datta S, et al. Correlation and agreement between arterial and venous blood gas analysis in patients with hypotension—an emergency department-based cross-sectional study. International Journal of Emergency Medicine. 2023;16(1):18. doi: 10.1186/s12245-023-00486-0.
- Baiee NR, Ali SA. Critical Care Nurse’s Knowledge Regarding to Fluid and Electrolytes Administration in Al-Hilla, Iraq. Medical Journal of Babylon. 2025;22(3):717-22. doi: 10.4103/MJBL.MJBL_737_23.
- Kausar S, Advani R, Ali Z, Batool W. Prevalence of acid-base disorders and impact on outcome in sepsis in critically ill patients: A retrospective cohort study. Anaesthesia, Pain & Intensive Care. 2025;29(7):764-9. doi: 10.35975/apic.v29i7.2952.
- Ciabattoni A, Chiumello D, Mancusi S, Pozzi T, Monte A, Rocco C, et al. Acid–Base Status in Critically Ill Patients: Physicochemical vs. Traditional Approach. Journal of Clinical Medicine. 2025;14(9):3227. doi: 10.3390/jcm14093227.
This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.