Ika Murtiyarini, Imelda*, Yuli Suryanti, Rosmaria
Department of Midwifery, Health Polytechnic of Jambi, Indonesia
* Corresponding author: Imelda, Department of Midwifery, Health Polytechnic of Jambi, Indonesia, Email: imelda.poltekkesjambi@gmail.com
Cita questo articolo
ABSTRACT
Introduction: Prenatal stress is often encountered but is rarely recognized and is considered not to affect pregnancy. Pregnancy has the potential to cause morbidity during pregnancy. In a study in Indonesia, 64.4% of pregnant women experienced severe stress and were at risk of causing preterm labour. One of the preventive measures during pregnancy to improve the health condition of the mother and baby is yoga. Prenatal yoga can prepare pregnant women physically, mentally, and spiritually to play a role in the delivery process.
Materials and Methods: The current study is a quantitative study with a pre-experimental design with one group pretest-posttest without control to determine the effect of prenatal yoga on stress levels of pregnant women in the private midwives of Jambi City in 2020. The study population was 86 pregnant women; by purposive sampling, 30 pregnant women were taken. The time of the study was from March to November 2020. The data analysis used was univariate analysis and bivariate analysis with the Wilcoxon test.
Results: In the initial assessment, most pregnant women experienced moderate stress levels; after prenatal yoga, most pregnant women experienced mild and average stress levels. Wilcoxon test results show that prenatal yoga has an effect on stress levels of pregnant women with a p-value of 0.0001 (<0.05).
Conclusion: Prenatal yoga is effective for reducing stress in third-trimester pregnant women.
Keywords: Stress, pregnant women, Prenatal yoga, Depression Anxiety and Stress Scale (DASS)
INTRODUCTION
Pregnancy is a process that starts from the meeting of sperm and ovum in a woman’s uterus or by another name, namely fertilization or conception, to form a zygote which then implants into the uterus and develops into a baby [1–3]. Sometimes, pregnancy has a stressful impact on pregnant women. Prenatal stress is almost expected in all pregnant women, especially in primigravida [4]. This stress can be caused by external factors (external stressors) or from within (internal stressors) pregnant women. Stress is an uncomfortable condition (dysphoric) defined as an imbalance of pregnant women to feel able or resist various changes in the adaptation process of their pregnancy [5,6].
Psychosocial studies of stress during pregnancy conducted on Asian, African, and white races found that 6% of pregnant women experienced mild stress, 78% experienced severe stress, and 16% did not experience stress at all [7]. Pregnancy stress is significantly caused by economic hardship, household problems, physical violence, medical problems, busyness, work, and a pregnancy history with complications [8].
Prenatal stress is often but is rarely recognized and is thought not to affect pregnancy [9]. A Canadian study showed that pregnant women experienced low levels of psychosocial stress and 6% of high levels of stress. Pregnant women in Spain, 30% have a lower chance of experiencing stress, while in Indonesia, 64.4% of pregnant women experience severe stress and can give birth prematurely [10].
Stress in pregnancy has the potential to cause morbidity during pregnancy [11]. Complications arise from prenatal stress, such as preterm delivery caused by the placenta, increased corticotrophin-releasing hormone (CRH), and progesterone in stressful conditions [12]. In addition, in early pregnancy, stress and a decrease in progesterone can cause abortion, progesterone which is calming and slows gastric motility as a trigger for hyper emesis gravidarum to Low Birth Weight (LBW). This impact proves that the mother’s mental state can affect the mother’s health during pregnancy and the baby’s growth and development in the next period of life [13,14].
DASS-42 is an assessment of stress scale that can be used in the stress assessment of pregnant women [15]. DASS-42 has been used to identify stress in Hispanic, American, British, Australian and Indonesian populations. Assessment items in DASS-42 include emotional states, communication barriers and physical disturbances felt by pregnant women. Measurement of stress levels using the DASS-42 score can reflect the state of prenatal stress as a predisposing factor for pregnancy complications [16,17].
Maintaining the health of the mother and fetus during pregnancy can be done by exercising in the morning, static cycling, aerobics, water exercise, dancing, and yoga. Some pregnancy exercise methods that can be an option include yoga, pilates, Kegels, hypnotherapy [18]. Prenatal yoga is effective for pregnant women to achieve comfort during pregnancy even until the delivery process. Prenatal yoga is a skill to cultivate the mind in a comprehensive personality development technique that includes physical, psychological and spiritual. This prenatal yoga includes various relaxations, adjusting breathing postures and meditation done by pregnant women every day [19].
Several studies have shown that yoga positively affects pregnant women, significantly reducing stress levels and back pain [20,21]. Another study conducted by Rahma [22] showed an increase in sleep quality in pregnant women after prenatal yoga. Another study conducted by Mediarti et al. [23] showed differences in the complaints of pregnant women before and after prenatal yoga, including back pain, insomnia, leg cramps and anxiety.
Based on the results of several studies that have been carried out showing the benefits of implementing prenatal yoga in reducing stress during pregnancy, but no research focuses on primigravida pregnant women; therefore, we tried to conduct this research on third-trimester pregnant women in the independent practice of midwives in Jambi City, Indonesia.
MATERIALS AND METHODS
This pre-experimental study consisted of a pre-test and post-test without a control group design involving 30 third trimester primiparous pregnant women in independent practice of midwives (PMB) Jambi City, Indonesia, which was carried out from March to November 2020. The implementation of intervention was carried out in PMB Jambi City, carried out by researchers assisted by midwives et PMB and enumerators, after asking participants’ consent and participants agreed by signing a certificate. The criteria for participants who were included in the study were primiparous mothers and third trimester, while mothers who were not healthy at the time of the study were not included in the study. The sample has been selected using purposive sampling, namely the technique of selecting samples based on the researcher’s considerations.
The prenatal yoga intervention was given by a certified midwife as a prenatal yoga instructor, with the first procedure (1) the mother doing warm-up movements, (2) doing the Uttkatasana movement, (3) doing the Vrkasasana movement, (4) doing the Adhatasana movement, (5) perform the Virabadhanasana movement, (6) perform the Utitatrikonasana movement, (7) perform the Anjeneyasana movement, (8) perform the Utkatakonasana movement, (9) perform the Malasana movement, (10) perform the Supta Baddha Konasana movement, (11) perform the Savasana movement, and Finally, take a deep breath from the nose 5-8 times.
Treatment is carried out once a week for two weeks with duration of 1-2 hours per session. The implementation of treatment complies with health protocols during the covid-19 pandemic, including washing hands, disinfecting mats, and not doing yoga in groups. The assessment of stress levels both pre and post prenatal yoga was carried out at PMB Jambi City, Indonesia by researchers assisted by enumerators.
This stress level was measured using the Depression Anxiety Stress Scale 42 (DASS 42) (Lovibond, 1995) both before and after the implementation of prenatal yoga. Psychometric anxiety stress scale of the Depression Anxiety stress scale 42 (DASS 42) consists of 42 question items, which include 3 subvariables including 1) physical 2) emotional/psychological 3) behavior. According to Lovibond (1995) cited by Crawford & Henry (2003) in their journal entitled “DASS: Normative data & latent structure in large non-clinical sample”. DASS has a discrimant validity level and has a reliability of 0.91 which is processed based on Cronbach’s Alpha assessment, so that the stress questionnaire is not tested for reliability because the questionnaire has been applied internationally. The stress level on the DASS 42 instrument (lovibond, 1995) is classified into five levels, namely Normal, score: 0 – 7; Mild, score: 8-9; Medium, 10-14; Severe, score: 15-19; Very severe, score: ≥ 20.
No economic incentives were offered or provided for participation in this study. The study was performed in accordance with the ethical considerations of the Helsinki Declaration. Ethical eligibility was obtained from the Health Research Ethics Commission of the Ministry of Health, Jambi, No. LB.02.06/2/140/2020.
Statistical Analysis
Data were analyzed using univariate analysis to obtain a frequency distribution based on each variable studied and bivariate analysis to determine the effect of prenatal yoga on stress levels of pregnant women. Data are presented as numbers and percentages for categorical variables. Continuous data are expressed as the mean ± standard deviation (SD), or median with Interquartile Range (IQR). Wilcoxon’s test was used to evaluating repeated measurements of the same objects using them as their own control. The test was carried out on 2 groups of related samples, the measurement scale was ordinal data. All tests with p-value (p)<0.05 were considered significant. Statistical analysis performed using the SPSS app version 16.0.
RESULTS
The results of the univariate analysis, which aims to determine the frequency of each variable studied, can be seen in the following table:
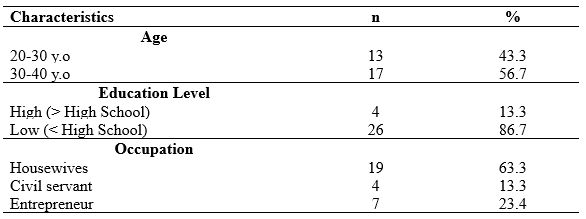
Table 1. Frequency Distribution of Respondents’ Characteristics
Table 1 shows that most respondents in group aged 20-30 years amounted to 13 people (43.3%), and respondents aged 30-40 years amounted to 17 (56.7%) people. Majority of respondents’ education level is low education as much as 86.7%, and the dominant occupation of respondents is housewives as much as 63.3%.
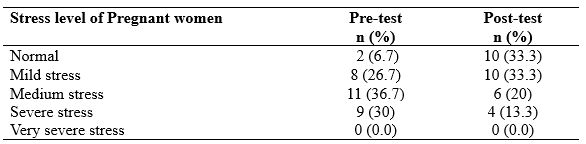
Table 2. Distribution of stress levels of pregnant women before and after prenatal yoga
Table 2 show that 11 (36.7%) respondents experienced medium stress during pregnancy, 10 (33.3%) respondents experienced mild stress levels and did not experience stress after prenatal yoga.
This analysis aims to determine the effect on variables using the Wilcoxon test, which can be seen in Table 3 below:
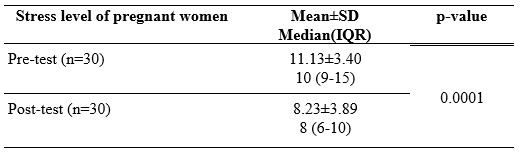
Table 3. The effect of prenatal yoga on the stress level of pregnant women in private midwives in Jambi City.
The analysis of the influence of prenatal yoga on the stress level of pregnant women in private midwives obtained a p-value = 0.0001 (p <0.05). These test results show that prenatal yoga affects the stress level of pregnant women in private midwives in Jambi City.
DISCUSSION
Anxiety in maternity mothers is related to the length of labour which results in complications in childbirth. One of the causes of prolonged labour is the stress response, and this ranks at the top among other causes [24].
Based on the study results, it is known that there are three categories of stress levels experienced by pregnant women during pregnancy. Stress is the body’s reaction to situations that cause pressure, change, emotional tension, and others. Stress is universal; that is, all people can feel it, but the way it is expressed is different. According to individual characteristics, the response is different for each person. Stress in pregnant women harms themselves and their babies. Moreover, if the stress is ongoing and chronic, it can have implications for recurring anxiety, frustration, or fear that has been suffered for a long time and can have adverse health effects.
Before prenatal yoga, most pregnant women experienced moderate stress. Many things can affect this incident, for example, worrying about the baby, not deciding where to give birth, doubting the family’s economic capacity. Prenatal stress often occurs only rarely recognized and considered not very important during pregnancy. Based on the study results, it is known that 64.4% of pregnant women in Indonesia experience severe stress.
Prenatal yoga is one way that can be done to relax pregnant women so that it can reduce stress levels in pregnant women. Based on the study results, it is known that there is a decrease in stress levels after prenatal yoga. Most of the stress levels of pregnant women drop to mild stress and even become routine.
Yoga affects the hypothalamus to suppress the secretion of CRH, which will affect the anterior lobe of the pituitary gland to suppress the release of the hormone ACTH so that the production of adrenal hormones and cortisol decreases and orders the anterior lobe of the pituitary gland to secrete endorphins. Yoga will inhibit the increase in sympathetic nerves so that the number of hormones that cause body deregulation can be reduced. The parasympathetic nervous system signals to influence catecholamine release. As a result, there is a decrease in heart rate, breathing rhythm, blood pressure, muscle tension, metabolic rate, and the production of hormones that cause anxiety or stress [25].
Based on the respondents’ stress levels before and after prenatal yoga, there was a significant decrease with the median pre-test stress value decreasing from 10 to 8 after the post-test, p=0.0001. The results of this test indicate the influence of prenatal yoga on the stress levels of pregnant women. Several previous studies showed that yoga had a positive effect on pregnant women, namely reducing stress levels and back pain [20]. Another study conducted by Rahma [22] showed an increase in sleep quality in pregnant women after prenatal yoga.
The application of prenatal yoga, which is one way to ensure the condition of the mother and fetus in a healthy and comfortable condition during pregnancy, is appropriate [26,27]. Yoga is a combination of stretching, breathing, postures, and meditation that promotes health and spiritual growth in the practitioner. This prenatal yoga includes various relaxations, adjusting breathing postures and meditation done by pregnant women every day [28].
One experimental study at a prenatal clinic in Taipei found that prenatal yoga significantly reduced pregnant women’s stress and improved their immune function. Attractive value from this study is the finding of higher immunoglobulin A (p < 0.001) in the intervention group than in the control group [29].
CONCLUSIONS
Prenatal yoga is effective for reducing stress in pregnant women in the third trimester. The variable for reducing stress levels is strongly influenced by the ability of pregnant women to control their thoughts so that the decrease in stress as a result of prenatal yoga varies in pregnant women
Study Limitations
The lack of control in this study is a limitation, so it cannot compare the intervention group who was given yoga practice and not yoga. In addition, other limitations of this study are No multicenter study, limited geographical area, small sample size.
Funding statement
This research did not receive any specific grant from funding agencies in the public, commercial, or not for profit sectors.
Competing interests statement
There are no competing interests for this study.
REFERENCES
- Nugroho T, Warnaliza D. Buku Ajar Askeb 1 Kehamilan. Nuha Medika; 2014.
- Van den Bergh BRH, van den Heuvel MI, Lahti M, Braeken M, de Rooij SR, Entringer S, et al. Prenatal developmental origins of behavior and mental health: The influence of maternal stress in pregnancy. Neuroscience & Biobehavioral Reviews. 2020;117:26–64.
- Boekhorst MGBM, Muskens L, Hulsbosch LP, Van Deun K, Bergink V, Pop VJM, et al. The COVID-19 outbreak increases maternal stress during pregnancy, but not the risk for postpartum depression. Archives of Women’s Mental Health. 2021;1–7.
- Sun S, Yang M, Zhang J, Zhou X, Jia G, Yu X. Family support for pregnant women with foetal abnormality requiring pregnancy termination in China. Health & social care in the community. 2020;28(3):1020–9.
- Woods SM, Melville JL, Guo Y, Fan M-Y, Gavin A. Psychosocial stress during pregnancy. American journal of obstetrics and gynecology. 2010;202(1):61-e1.
- Sarmita S, Nurdin S, Fattah AH. Gambaran Kecemasan Ibu Hamil Di Wilayah Kerja Puskesmas Cabenge Kabupaten Soppeng. Jurnal Pendidikan Keperawatan dan Kebidanan. 2021;1(1):20–6.
- Diane M. Korelasi Kadar Progesteron dan Kortisol Dengan Skor DASS-42 Pada Ibu Hamil Trimester 1. Universitas Andalas; 2017.
- Redshaw M, Henderson J. Fathers’ engagement in pregnancy and childbirth: evidence from a national survey. BMC pregnancy and childbirth. 2013 Mar;13:70.
- Cottrell EC, Seckl J. Prenatal stress, glucocorticoids and the programming of adult disease. Frontiers in behavioral neuroscience. 2009;3:19.
- Palmeira P, Quinello C, Silveira-Lessa AL, Zago CA, Carneiro-Sampaio M. IgG placental transfer in healthy and pathological pregnancies. Clinical and Developmental Immunology. 2012;2012.
- Sicherer SH, Wood RA, Stablein D, Lindblad R, Burks AW, Liu AH, et al. Maternal consumption of peanut during pregnancy is associated with peanut sensitization in atopic infants. Journal of Allergy and Clinical Immunology. 2010;126(6):1191–7.
- Woods‐Giscombé CL, Lobel M, Crandell JL. The impact of miscarriage and parity on patterns of maternal distress in pregnancy. Research in nursing & health. 2010;33(4):316–28.
- Johnson M, Campbell F, Messina J, Preston L, Woods HB, Goyder E. Weight management during pregnancy: a systematic review of qualitative evidence. Midwifery. 2013;29(12):1287–96.
- Brummelte S, Galea LAM. Depression during pregnancy and postpartum: contribution of stress and ovarian hormones. Progress in Neuro-Psychopharmacology and Biological Psychiatry. 2010;34(5):766–76.
- Lovibond PF, Lovibond SH. The structure of negative emotional states: Comparison of the Depression Anxiety Stress Scales (DASS) with the Beck Depression and Anxiety Inventories. Behaviour research and therapy. 1995;33(3):335–43.
- Crawford DM, Trotter EC, Hartshorn KJS, Whitbeck LB. Pregnancy and mental health of young homeless women. American Journal of Orthopsychiatry. 2011;81(2):173.
- Dong X, Qu Z, Liu F, Jiang X, Wang Y, Chui CHK, et al. Depression and its risk factors among pregnant women in 2008 Sichuan earthquake area and non-earthquake struck area in China. Journal of affective disorders. 2013;151(2):566–72.
- Krisnadi SR. Sinopsis yoga untuk kehamilan: sehat, bahagia dan penuh makna. Larasati, P, & Wibowo, A(2012) Pengaruh Keikutsertaan Senam Hamil Terhadap Kecemasan Primigravida Trimester Ketiga dalam Menghadapi Persalinan Skripsi, Universitas Airlangga, Fakultas Kesehatan Masyarakat, Surabaya. 2010;
- Amalia R, Syamsuddin S, Idris I, Limoa E, Pelupessy N, Syam A. The Effectiveness of Prenatal Gentle Yoga on the Recovery of Anxiety Level and Norepinephrine Level in Pregnant Women Aged 35 Years Old. International Journal of Health and Medical Sciences. 3(1):79–85.
- Field T, Diego M, Delgado J, Medina L. Yoga and social support reduce prenatal depression, anxiety and cortisol. Journal of bodywork and movement therapies. 2013;17(4):397–403.
- Battle CL, Uebelacker LA, Magee SR, Sutton KA, Miller IW. Potential for prenatal yoga to serve as an intervention to treat depression during pregnancy. Women’s Health Issues. 2015;25(2):134–41.
- Rahma FN. Hubungan Senam Yoga Terhadap Peningkatan Kualitas Tidur Pada Ibu Hamil Trimester III. Universitas Muhammadiyah Surakarta; 2014.
- Mediarti D, Sulaiman S, Rosnani R, Jawiah J. Pengaruh yoga antenatal terhadap pengurangan keluhan ibu hamil trimester III. Jurnal kedokteran dan kesehatan. 2014;1(1):181691.
- Hayati F, Herman RB, Agus M. Perbedaan tingkat kecemasan ibu bersalin di puskesmas dengan di bidan praktik mandiri dan hubungannya dengan lama persalinan. Jurnal Kesehatan Andalas. 2018;6(3):564–71.
- Vijayalakshmi P, Madanmohan BAB, Patil A, Babu K. Modulation of stress induced by isometric handgrip test in hypertensive patients following yogic relaxation training. Indian J Physiol Pharmacol. 2004;48(1):59–64.
- Chuntharapat S, Petpichetchian W, Hatthakit U. Yoga during pregnancy: effects on maternal comfort, labor pain and birth outcomes. Complementary therapies in clinical practice. 2008;14(2):105–15.
- Sun Y-C, Hung Y-C, Chang Y, Kuo S-C. Effects of a prenatal yoga programme on the discomforts of pregnancy and maternal childbirth self-efficacy in Taiwan. Midwifery. 2010;26(6):e31–6.
- Jahdi F, Sheikhan F, Haghani H, Sharifi B, Ghaseminejad A, Khodarahmian M, et al. Yoga during pregnancy: The effects on labor pain and delivery outcomes (A randomized controlled trial). Complementary therapies in clinical practice. 2017;27:1–4.
- Chen P-J, Yang L, Chou C-C, Li C-C, Chang Y-C, Liaw J-J. Effects of prenatal yoga on women’s stress and immune function across pregnancy: A randomized controlled trial. Complementary Therapies in Medicine. 2017;31:109–17.