Oseni Rukayat1, Ekpoanwan Esienumoh2, Fakeye Grace 3, Emmanson Emmanson 3*
- Sacred Heart College of Nursing Sciences – Lantoro Abeokuta, Ogun State, Nigeria
- Department of Nursing Sciences, University of Uyo, Akwa Ibom State, Nigeria
- Department of Human Anatomy, University of Cross River State, Nigeria
* Corresponding Author: Emmanson Emmanson, Department of Human Anatomy, University of Cross River University State, Nigeria. E-mail: emmansonemmanson35@gmail.com
Cite this article
ABSTRACT
Introduction: Inherent in every relationship irrespective of number of people involved is the tendency for conflict to occur, either at the intrapersonal, interpersonal, intra-professional or inter-professional level with positive or negative outcome depending on effective resolution of the conflict and the time of resolving it. Conflict has been known to bring about improved relationship, increased cohesiveness, improved communication and productivity when handled and resolved timely. The aims of the study are to identify perceived causes of workplace conflict among nurses and the resolution methods they employ.
Materials and Methods: A cross-sectional research design was used for the study. The sample was 90 nurses on permanent appointment with the hospital drawn using convenient sampling technique. Instruments were validated Rahim Organizational Conflict Inventory (ROCI II) and structured questionnaire on causes of conflicts adapted from Mukeshimana and Asingzwe (2016). Data were analyzed using descriptive statistics of frequencies and percentages and chi-square inferential statistics for causes and resolution methods for conflict at 0.05 level of significance.
Results: The outcome of the study revealed that majority of the respondents are registered nurses and registered midwives only 64 (71.1%), 66 (73.3%) were NO I or NO II; only 8 (8.9%) had Masters or higher education. Injustice (95.6%), unreasonable patient and relative expectation (93.3%), and lack of respect from other health professionals and unequal workload and work schedule (91.1% each) were identified as major causes of workplace conflict. Most prominent method of conflict resolution identified was collaboration (x = 69).
Conclusion: In conclusion, institution should organize training and retraining of nurses regularly, employ more nurses to prevent burnout and job dissatisfaction that can lead to conflict.
Keywords: Collaboration, Workplace conflict, Conflict resolution, Injustice, Nurses
INTRODUCTION
Conflict according to Ronquillo et al. (2023) [11], is the disagreement or difference of opinions between or among individuals which could involve conflicting group or team goals versus individual member’s agendas, insights, or goals which could be potentially harmful to the organization, however, conflict could be positive, promote team-building skills, critical thinking, and bring up new ideas when effectively managed by a competent leader.
Organizational conflict has been known to be an actual or perceived divergent opinion by opposing members of the organization which could involve values, interests, and needs. Opposing members could be individuals on horizontal line of management, or vertical line of management; irrespective of the cause the consequence is usually the same – reduced productivity if the conflict is not resolved early and appropriately (Awan & Saeed, 2015) [3].
Conflict is a part of interpersonal relations and is unfortunately unavoidable and a part of our daily life. For most people, conflict is often threatening and stressful, however conflict can result in the individual or organization discussion of differences that lead to creative solutions, accelerates change in an organization, especially in small businesses, where it is easy to formulate and implement new policies (Ronquillo et al. 2025) [12]. Ronquillo et al. 2025, continued that conflict prompts modification of policies and operation procedures in the organization. In cases of extreme conflict, the organization may conduct a complete overhaul of its leadership, bringing in managers with fresh ideas. According to Awan & Saeed (2015) [3], any threat to the harmony of the organization resulting in conflict sometimes may ultimately impacts negatively on the organization efficiency. Furthermore, where individual and organizational interest conflicts; when people working in an organization cannot maintain a work environment of harmony especially between the manager and subordinate then organizational efficiency, organizational progress cannot be achieved.
According to Oresanjo (2015) [8], conflict is widespread in human societies, meaning that it cannot be ruled out in any human organization, be it schools and colleges, business firms or even social clubs etc. He stated further that conflict is bound to occur because every individual is dependent on other individuals in the organization and once there is interaction, therefore, conflict cannot be ruled out. He maintained that conflict is seen as both disruptive force within an organization and primary source of individual stress. However, it is not entirely destructive. The goal of an organization should be how to control conflict in order not to degenerate into crisis rather than eliminating it.
Every organization is faced with one conflict or the other at a point in the organizational cycle especially when members of the organization perceived or believed that their interest or goal may be jeopardized and not achieved as the organization is progressing. According to Smiley (2010) [13]; Adeyemi and Aigbavboa (2022) [1], managing conflict or conflict resolution is one of the paramount skills that managers must be trained on and must be maintained to ensure organizational efficiency.
Most of the time organizational conflict occur as a result of unhealthy working environment, poor management with some staff being overloaded with work and some other staff are viewed as being redundant this may be consequent to poor organization structure or restructuring; unfair treatment which may be perceived or actual; there may be no clear-cut definition of job roles or job specification. The major causes being poor communication among members of the organization; favouritism with some being promoted while others are not promoted, jealousy and struggle for power have also been identified by different researchers as causes of conflict.
Workplace violence experienced by healthcare teams especially nurse seems to be due to lack of satisfying conflict resolution or when patient and their relations feel their needs are not being met. This problem has been reported repeatedly in most hospitals in Nigeria (Ogbonnaya et al., 2023) [6] same was experienced recently in Sacred Heart Hospital, Lantoro. The need for effective conflict resolution by nurses to prevent escalation of conflict prompted the interest for this study. From literature reviewed by the researcher it was discovered that there is paucity of research work conducted on causes of conflict and the methods of conflict resolution among nurses, between the nurse and other health care professionals; nurses and patient and/or patient’s relations.
This research assessed the causes of workplace conflict among nurses in Sacred Heart Hospital, Lantoro, Abeokuta, Ogun state and methods of conflict resolutions utilized by them.
MATERIALS AND METHODS
Study Population
This was a descriptive cross-sectional study conducted among clinical nurses at Sacred Heart Hospital, Lantoro, Nigeria, between September 2021 and August 2022, with final data analysis completed by December 2022.
The study targeted registered nurses currently working in the hospital across different clinical departments and nursing cadres. Nurses were selected from inpatient and outpatient units based on their availability and consent to participate.
The study protocol matched the Declaration of Helsinki ethical guidelines for clinical studies, and it was approved by the Technical Scientific Committee of Sacred Heart Hospital, Lantoro, with approval letter dated September 15, 2021, ref: SHH/EC/EA/05/09/21. All participants were informed and signed their informed consent.
Inclusion criteria
- Registered nurses licensed by the Nursing and Midwifery Council of Nigeria
- Minimum of 2 years of clinical experience
- Willingness to give informed consent and participate voluntarily
Exclusion criteria
- Nurses on annual leave, sick leave, or study leave during the study period
- Nurses who declined to provide informed consent.
Instrument
This study utilized a common instrument—the Rahim Organizational Conflict Inventory–II (ROCI–II) created by Rahim (1983)—to assess conflict management styles among nurses. Specifically, Forms A, B, and C of the ROCI-II with 28 items each were used to assess conflict resolution styles when dealing with supervisors (Form A), subordinates (Form B), and peers (Form C). The instrument assesses five conflict management styles: Integrating (Collaborating), Obliging (Accommodating), Dominating (Competing), Avoiding, and Compromising.
All of the items on the ROCI-II are measured on a 5-point Likert scale, from 1 = Strongly Disagree to 5 = Strongly Agree. The 28 items on each of the two forms are arrayed into five subscales that correspond to the five conflict resolution styles. The item classification into each style is as follows:
1) Integrating (Collaborating) – 7 items, 2) Obliging (Accommodating) – 6 items, 3) Dominating (Competing) – 5 items, 4) Avoiding – 6 items, 5) Compromising – 4 items.
In addition, an adapted version of the Causes of Conflict Questionnaire by Mukeshimana and Asingzwe (2016) [5] was employed to assess potential causes of conflict in the workplace. The adapted instrument included structured items designed to bring out nurses’ views of interpersonal, organizational, and communication-related causes of conflict. The items also received scores on a 5-point Likert scale ranging from 1 = Strongly Disagree to 5 = Strongly Agree. To ensure content validity, the instruments were reviewed by nursing science and educational measurement and evaluation specialists. They checked the items for consistency, relevance, and clarity with the initial instruments. Minor modifications were effected to improve the appropriateness and readability of the questionnaire items to the study environment from their inputs. The final instrument retained the fundamental constructs and design of the initial instruments.
Statistical Analysis
Data obtained were analyzed based on objectives and hypotheses. Socio-demographic data was analyzed using descriptive statistics and presented on a percentage and frequency table.
The non-parametric Friedman test was used for testing the differences between three or more dependent variables. If the Friedman test was positive (P<0.05), the post hoc Wilcoxon signed-rank test was used for pairwise comparison. The chi-square test or Fisher’s exact test were performed to assess significant differences in proportions or percentages between two independent variables. Fisher’s exact test was used when the chi-square test was found to be inappropriate. Causes and Methods of conflict were analyzed using SPSS version 20 and presented with tables. All the hypotheses were tested with a significance level of 0.05.
RESULTS
Ninety-six copies of the questionnaire were distributed to sample selected for the study but only 90 copies (93.8%) of returned questionnaire were completely filled and met the criteria for analysis. Therefore, 90 copies of the questionnaire were analyzed.
| Characteristics | % (n) |
| Gender | |
| Female | 95.6% (86) |
| Male | 4.4% (4) |
| Religion | |
| Christian | 93.3% (84) |
| Islam | 6.7% (6) |
| Marital status | |
| Single | 51.1% (46) |
| Married | 42.2% (38) |
| Divorced | 4.4% (4) |
| Widow | 2.2% (2) |
| Level of education | |
| RN/RM | 71.1% (64) |
| BNSc | 20.0% (18) |
| ≥MSc | 8.9% (8) |
| Cadre | |
| NO I – NO II | 73.3% (66) |
| SNO – PNO | 11.1% (10) |
| ACNO – ADN | 15.6% (14) |
| Grade level | |
| Below 13 | 73.3% (66) |
| 13 – 15 | 22.2% (20) |
| 16 and above | 4.4% (4) |
Table 1. General characteristics of the sample.
Table 1 shows that more female nurses 86 (95.6%) than male nurses 4 (4.4%) participated in the study. A majority of the respondents are Christians 84 (93.3%). About half of the respondents are single 46 (51.1%), while widows are 2 (2.2%). A majority of the respondents are RN/RM only 64 (71.1%); only 8 (8.9%) had Master’s or higher education. For the cadre, more than half 66 (73.3%) are NO I or NO II. Similarly, 66 (73.3%) are below grade level 13, followed by those on grade level 13 – 15 with 20 (22.2%).
| Causes | Agree % (n) | Disagree % (n) |
| Distrust | 88.9% (80) | 11.1% (10) |
| Refusal to take orders from doctor | 64.4% (58) | 35.6% (32) |
| Doctors consider themselves as superior | 80.0% (72) | 20.0% (18) |
| Lack of respect from other health professionals | 91.1% (82) | 8.9% (8) |
| Different level of education | 77.8% (70) | 22.2% (20) |
| Conflict of interest and absence of procedure and strategies | 80.0% (72) | 20.0% (18) |
| Lack of respect and lack of attention to patient | 71.1% (64) | 28.9% (26) |
| Being insulted by the doctor before patient | 82.2% (74) | 17.8% (16) |
| Order from a doctor which is out of the scope of my practice | 75.6% (68) | 24.4% (22) |
| Delay of the doctor to answer my call in emergency case | 88.9% (80) | 11.1% (10) |
| Injustice from some nurse managers | 95.6% (86) | 4.4% (4) |
| Favouritism | 86.7% (78) | 13.3% (12) |
| Unequal workload and work schedule | 91.1% (82) | 8.9% (8) |
| Unreasonable patient and relative expectation | 93.3% (84) | 6.7% (6) |
| Imbalance nurse-patient ratio | 88.9% (80) | 11.1% (10) |
Table 2. Distribution of Respondent on Causes of Conflict (N = 90)
Table 2 shows that all the items identified constitute strong causes of conflict ranging between 58 (64.0%) and 86 (95.6%) out of 90, with refusal to take orders from doctors being the least count 58 (64.0%) while 86 (95.6%) of the respondents supported injustice from some nurse managers as the major cause of conflict in the hospital, followed by unreasonable patient and relative expectation (93.3%), unequal workload and lack of respect from other health professionals (91.1% each). Delay of the doctor to calls in emergency cases, imbalance nurse-patient ratio, and distrust were also significant causes of conflict with 88.9% respectively.
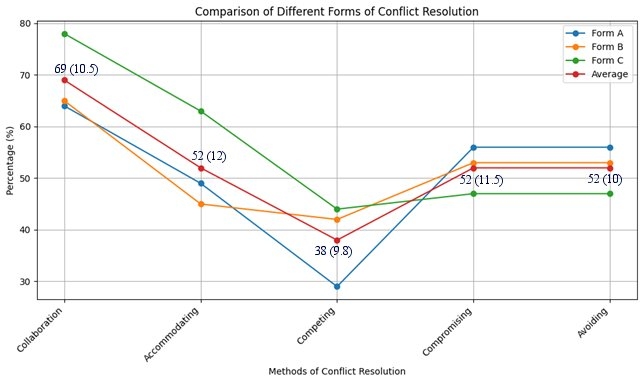
Figure 1: Percentage distribution of responses to method of conflict resolution utilized by nurses (N = 90). The figure shows the mean percentage values and the standard deviations in brackets.
The figure above shows positive response to various methods of conflict resolution in the hospital. Form A depicts conflict resolution with subordinates, Form B depicts conflict resolution among colleagues, Form C depicts method of conflict resolution among superior. Average of the responses shows the overall average performance across board or of the three forms. It can be observed that most of the respondents discouraged the use of competing resolution with an average score of 38% while they supported the use of collaboration with an average score 69%. Accommodating, compromising and avoiding have equal percentages (average 52.0% each). Therefore, it can be deduced that majority of nurses utilize collaboration in conflict resolution (69.0%) while few nurses use competing (38.0%) in resolving conflict in Sacred Heart Hospital, Lantoro, Abeokuta.
Statistical analysis using the Friedman test (χ² = 92.15, df = 4, p < 0.001) confirmed a significant difference in method preference. Post hoc Wilcoxon signed-rank tests (Holm-corrected) showed that collaboration (median: 69.0) was significantly more used than competing (median: 38.0, p < 0.001), accommodating (median: 52.0, p = 0.003), and avoiding (median: 52.0, p = 0.005). Competing was also significantly less used than accommodating (median: 52.0, p = 0.007).
Table 3 presents a cross-tabulation of the respondents’ preferred methods for conflict resolution in relation to their demographic and professional characteristics, including gender, cadre, and level of education. This descriptive overview highlights distribution patterns across the five conflict resolution styles.
| Characteristics | Accommodating | Avoiding | Collaborating | Competing | Compromising | Total |
| Gender | ||||||
| Male (n=4) | – | – | 4 (100.0%) | – | – | 100.0% |
| Female (n=86) | 6 (7.1%) | 20 (23.8%) | 37 (42.9%) | 4 (4.8%) | 18 (21.4%) | 100.0% |
| Cadre | ||||||
| NO II (n=24) | 1 (4.2%) | 4 (16.7%) | 13 (54.2%) | 1 (4.2%) | 5 (20.8%) | 100.0% |
| NO I (n=9) | 1 (11.1%) | 2 (22.2%) | 3 (33.3%) | – | 3 (33.3%) | 100.0% |
| SNO (n=2) | – | 1 (50.0%) | 1 (50.0%) | – | – | 100.0% |
| PNO (n=1) | – | – | 1 (100.0%) | – | – | 100.0% |
| ACNO (n=1) | – | – | – | 1 (100.0%) | – | 100.0% |
| CNO (n=1) | – | – | 1 (100.0%) | – | – | 100.0% |
| ADN (n=5) | – | 3 (60.0%) | 1 (20.0%) | – | 1 (20.0%) | 100.0% |
| Level of Education | ||||||
| Diploma (n=54) | 2 (3.7%) | 8 (14.8%) | 32 (59.3%) | 2 (3.7%) | 10 (18.5%) | 100.0% |
| B.Sc. (n=12) | 2 (16.7%) | 3 (25.0%) | 3 (25.0%) | 1 (8.3%) | 3 (25.0%) | 100.0% |
| M.Sc. (n=8) | – | 8 (100.0%) | – | – | – | 100.0% |
| Others (n=4) | – | 1 (25.0%) | 2 (50.0%) | – | 1 (25.0%) | 100.0% |
Table 3. Cross tabulation of association of respondent’s characteristics and their method of conflict resolution (N = 90).
Table 4 summarizes the results of statistical analyses used to examine the association between respondents’ characteristics and their chosen method for conflict resolution. Chi-square tests, likelihood ratios, and Fisher-Freeman-Halton exact tests were applied to assess significance.
The analysis showed that there is no significant association between gender and method of conflict resolution used by nurses. The Fisher’s exact test was also carried out because 60% of the expected cell frequencies were below 5, with a minimum expected count of 0.18 which violates the chi square assumption. The p-value (0.453) was greater than the significant level (0.05). Hence, there is no evidence to reject the null hypothesis.
| Gender | Value | df | Asymptotic Sig. (2-sided) | Exact Sig. (2-sided) |
| Pearson Chi-Square | 5.029a | 4 | 0.284 | 0.310 |
| Likelihood Ratio | 6.537 | 4 | 0.162 | 0.176 |
| Fisher-Freeman-Halton Exact Test | 3.402 | 0.453 | ||
| N of Valid Cases | 88 | |||
| Cadre | ||||
| Pearson Chi-Square | 62.306a | 24 | 0.0 | |
| Likelihood Ratio | 35.889 | 24 | 0.056 | 0.02* |
| Fisher-Freeman-Halton Exact Test | 31.533 | 0.049* | ||
| N of Valid Cases | 86 | |||
| Education | ||||
| Pearson Chi-Square | 19.407a | 12 | 0.079 | 0.090 |
| Likelihood Ratio | 18.398 | 12 | 0.104 | 0.097 |
| Fisher-Freeman-Halton Exact Test | 17.089 | 0.073 | ||
| N of Valid Cases | 88 | |||
| * = significant test | * = significant test | * = significant test | * = significant test | * = significant test |
Table 4. Analysis of the association between several variables and method of conflict resolution.
The analysis also showed that there is a significant association between cadre and method of conflict resolution used by nurses. The Fisher’s exact test was carried out because 88.6% of the expected cell frequencies were below 5, with a minimum expected count of 0.09 which violates the chi square assumption. The p-value (0.049) was lower than the significant level (0.05). Hence, the null hypothesis is rejected, and the conclusion is that there is an association between cadre and the conflict resolution.
The level of education was also tested with the style of conflict resolution used by nurses. The Fisher’s exact test was used instead of the chi-square test because 80% of the expected cell frequencies were below 5, with a minimum expected frequency of 0.09 which violates the chi-square assumption. The p-value (0.073) was greater than the significant level (0.05). Hence, there is no evidence to reject the null hypothesis.
DISCUSSION
The perceived factors causing conflict experienced by nurses include injustice from some nurse managers (95.6%) being the major cause of conflict, unreasonable patient and relative expectation (93.3%), unequal workload and lack of respect from other health professionals (91.1% each). Delay of the doctor to calls in emergency cases, imbalance nurse-patient ratio, and distrust (88.9% each), this was supported by Pitsillidou, et al. (2018) [9] findings among health professionals in hospitals of Cyprus to record the types of conflict management that health professionals in Cyprus hospitals encounter in their daily work and to explore the conflicts, their parameters and causes, and the role ambiguity faced by hospital employees. It was discovered that health professionals identified heavy workload, low pay, and varying instructions from different leaders as causes of conflict. In addition, the findings of a study by Olajide et al. (2015) [7] on conflict among nurses and doctors in 2 tertiary hospitals in Ekiti State indicated that odds of conflicts were significantly higher with limited opportunities for staff interaction (OR=1.8, CI=1.1-2.9); desire for power (autonomy) by doctors (OR=3.2, CI=1.9-5.2) and desire for more influence by nurses (OR=12.5, CI=4.8-41.3). Chances of expressing conflicts were significantly higher as strikes (OR=2.1; 1.3-3.5) but less with physical assaults (OR=0.1, CI=0.03-0.41). This is also, supported by Akpabio et al. (2015) [2] research finding which showed that un-resolved conflicts may be linked to poor communication resulting from refusal to cooperate, poor team collaboration and problem-solving, decreased clients’ satisfaction, distrust, split camps, gossips and disruption of work-flow, overwork and poor rewarding system each with frequency of 222 (92.0%); patients-related conflict and leadership conflicts each with frequency of 218 (90.0%); misunderstanding involving nursing colleagues with a frequency of 194 (81.0%); poor work environment 192 (80.0%); conflicts with other health professionals with 189 (78.0%) frequency and discrimination issues with 180 (61.0%) frequency.
Methods of conflict resolution include collaboration, accommodation, and compromising. The study revealed that more than half of the nurses utilized collaboration (69.0%), accommodating, compromising and avoiding (52.0% respectively) and only a few used competitions as a method of conflict resolution. A Friedman test revealed a significant difference in utilizing these conflict resolution methods (χ² = 92.15, df = 4, p < 0.001). Post hoc Wilcoxon signed-rank tests with Holm-Bonferroni correction showed that collaboration was significantly more utilized than competing (p < 0.001), meaning that nurses certainly utilize collaborative styles more than confrontational styles. This is in contrast with the results of Pitsillidou, et al. (2018) [9], that respondents utilized avoidance (73.2%) over negotiation for mutual benefit (54.2%), and compromise (40.5%) as conflict management mechanisms, as compared with the results of Adeyemi and Aigbavboa (2022) [1], that collaboration, accommodating, negotiating, compromising, and mediating were the most common conflict resolution styles utilized by Southwest Nigerian construction professionals. In addition, collaboration was employed significantly more than accommodating (p = 0.003) and avoiding (p = 0.005). These findings validate the perspective that nurses regard collaborative approaches as not only professionally appropriate but also more effective in resolving intricate interpersonal and hierarchical disputes within the clinical setting. Collaboration enhances mutual respect and problem-solving, which are essential values in nursing practice. The findings mirror Adeyemi and Aigbavboa’s (2022) [1] results, which also indicated extremely high reliance on cooperation as a conflict resolution style.
Competing was utilized significantly less than accommodating (p = 0.007), demonstrating that aggressive or assertive styles are actively avoided or rejected by nurses. This aligns with the philosophy of caregiving in nursing, which promotes empathy and de-escalation. While some degree of assertiveness may be required in critical care practice, the overall avoidance of competitive conflict resolution suggests a strong professional culture that prioritizes harmony over hierarchy.
Surprisingly, no difference was detected in the use of accommodating, compromising, and avoiding styles (p > 0.05). This can reflect the pragmatic interchangeability of these styles on a day-to-day basis, especially if nurses attempt to minimize friction but not necessarily the source. This passivity or neutrality can be a coping strategy in environments where power imbalances are prevalent, or where organizational constraints reduce formal conflict resolution mechanisms.
There is no relationship between gender and level of education, and conflict resolution style used by nurses, except cadre which influenced conflict resolution approach. This suggests that positional status in an organization plays a role in managing conflict, perhaps due to variations in authority, confidence, and experience. This finding is against Birkhoff’s (2015) [4] that gender significantly influences conflict dynamics at the individual and societal levels. In order to understand the role of gender in conflict comprehensively, it is important to examine it through individual, interpersonal, and societal levels. Gender may manifest itself in conflicts through how parties interpret and make sense of the conflict. Birkhoff also presented the findings of Gwartney-Gibbs to support his findings that gender also had an effect on dispute handling mechanisms. Conflict resolution processes for women were not as effective as those of men. For example, women would avoid more than resolving the conflict. However, the current findings show that within professional clinical environments such as Sacred Heart Hospital, formalized positions and codes of conduct can counteract the influences of gender and educational level and bring about similar conflict resolution styles across demographic groups. This highlights the importance of looking more closely at contextual and institutional determinants of conflict behaviour in healthcare organizations, particularly the influence of leadership structure and support systems on employee behaviour.
Implications for practice and future research
The findings have practical implications for policymakers and healthcare administrators. Since the most common approach to resolving conflict was collaboration, institutions should promote team-based training and workshops on collaborative communication improvement, leadership, and emotional intelligence among nurses. Resolving the main causes of conflict e.g., injustice by nurse managers, expectations of patients, and workload disparities can increase job satisfaction, collaboration, and overall patient care quality.
Future studies should seek to conduct multi-centre studies with larger populations of studies in different geopolitical settings of Nigeria for maximum generalizability. Longitudinal studies may also be helpful in identifying changes in conflict resolution patterns over time. Qualitative studies exploring nurses’ lived experiences of workplace conflict can also help in understanding factors involved and aid in devising context-specific interventions.
CONCLUSION
The study concludes that the major factors causing conflict among nurses are injustice from some nurse managers, unreasonable patient and relative expectation, unequal workload and lack of respect from other health professionals, delay of the doctor to calls in emergency cases, imbalance nurse-patient ratio, and distrust. Collaboration was discovered to be the main method of conflict resolution utilized by nurses in Sacred Heart Hospital, Lantoro, irrespective of their socio-demographic status of gender and level of education. However, cadre of the nurses influenced method of conflict resolution used.
Limitations
This study was limited to a single hospital, which may affect the generalizability of the findings. The sample size was relatively small, and data collection relied on self-reported responses, which may introduce bias. Future studies should include larger, multi-centre samples for broader applicability.
Funding statement
This research did not receive any specific grant from funding agencies in the public, commercial, or not for profit sectors.
Conflict of interest
The authors report no conflict of interest.
Authors’ contribution
- Oseni Rukayat: Conceptualized idea and conducted full research.
- Ekpoanwan Esienumoh: assisted with the design of questionnaire and conducting interviews with the selected nurses.
- Fakeye Grace: Was responsible for literature reviews
- Emmanson Emmanson: performed data analysis and edited the manuscript for publication.
Acknowledgements
We sincerely appreciate the management and nursing staff of Sacred Heart Hospital, Lantoro, for their support. Special thanks to our academic institutions, mentors, and colleagues for their guidance. We also acknowledge our families and friends for their unwavering encouragement throughout this research. Thank youall.
REFERENCES
- Adeyemi, B. S. and Aigbavboa, C. O. (2022). An Exploratory Factor Analysis for Conflict Resolution Methods among Construction Professionals. MDPI. Vol. 12(6). .
- Akpabio I. I., John M. E., Akpan M. I., Akpabio F. A. and Uyanah D. A. (2015). Work-related Conflict and Nurses’ role performance in a tertiary hospital in South-south Nigeria. Journal of Nursing Education and Practice, 6(2). . Accessed 27/10/2022.
- Awan, A. R. and Saeed S. (2015). Conflict Management and Organizational Performance: A case Study of Askari Bank Ltd. Research Journal of Finance and Accounting, 6(11), . Accessed 24/04/2022.
- Birkhoff J. (2015). Gender, Conflict and Conflict Resolution. . Accessed 17/10/2022
- Mukeshimana M. and Asingzwe D. (2016). Nurse-Doctor Relationship in Rwanda: A Questionnaire Survey. IOSR Journal of Nursing and Health Science.. Accessed 12/09/2022.
- Ogbonnaya, G. U., Ukaegbu, A. U., Aguwa, E., and Emma-Ukaegbu, U. A study on workplace violence against health workers in a Nigerian tertiary hospital. . Accessed 22/01/2023.
- Olajide, A. T., Asuzu M.C, and Obembe T.A. (2015). Doctor-Nurse Conflict in Njgerian Hospitals: Causes and Modes of expression. Journal of Advances in Medicine and Medical Research. VOL. 9(10). . Accessed 04/06/2021.
- Oresanjo, N. O. (2015). Conflict Management in School Organization in Nigeria. International Journal of Development and Management Review. V10(1). https://www.ajol.info>ijdmr>article>view.pdf. Accessed 17/10/2021.
- Pitsillidou, M. , Farmakas, A., Noula, M., and Roupa, Z. (2018). Conflict Management among health Professionals in hospitals in Cyprus. Journal of Nursing Management, 26(3-4). . Accessed on 24/04/2022.
- Rahim, M. A. (1983). Measurement of Organizational Conflict. The Journal of General Psychology, 109(2), 189-199.
- Ronquillo, Y. , Ellis, V. L, &Toney-Butler, T. J. (2023). Conflict Management. National Library of Medicine. ncbi.nlm.nih.gov/books/NBK4704321/
- Ronquillo, Y. , Ellis, V. L., &Toney-Butler, T. J. (2025). Conflict Management. In StatPearls. StatPearls Publishing. Retrieved from https://www.ncbi.nlm.nih.gov/books/NBK470432/
- Smiley, F. (2010). Leadership Guide to Conflict and Conflict Management. . Accessed 24/04/2022.
![]() This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.