Vitale Elsa1*, Donvito Simona2, Altieri Vito3
- Centre of Mental Health, Modugno, ASL BARI. Contract professor for the University of Bari.
- Nursing student at the University of Foggia.
- Nursing coordinator ASM, Matera. Professor of Nursing Degree at the University of Foggia.
* Corresponding author: Vitale Elsa, Centre of Mental Health, Modugno, ASL Bari, e-mail: vitaleelsa@libero.it
DOI: 10.32549/OPI-NSC-37
Cita questo articolo
ABSTRACT
Introduction: The Health Care Quality System began in 1992 and continues in the complex phenomenon of innovation which is necessary to improve the Health Care System.
This study aims to investigate how patients perceive the quality of care provided in the interventional cardiology service and therefore whether they are satisfied with the care received.
Materials and Methods: A questionnaire of 19 total items was elaborated and administered on 81 patients with the objective of assessing the importance of the interaction modality of the nursing staff with the patients who undergo the interventional cardiology procedure in the intra and peri- procedural moments.
Keywords: Interventional Cardiology Service; Nursing Performances; Perceived Quality; Patient Quality.
“Valutazione della percezione della qualità dei pazienti in relazione alle cure ricevute dal personale infermieristico nel Laboratorio di Emodinamica ed Elettrostimolazione:: uno studio di coorte.
ABSTRACT
Introduzione: Il sistema di qualità in sanità è iniziato dal 1992 e continua in un complesso fenomeno di innovazione, necessario per migliorare il sistema sanitario. Questo studio ha lo scopo di valutare come i pazienti percepiscono la qualità delle cure fornite dal servizio di cardiologia interventistica e, se sono soddisfatti delle cure ricevute.
Materiali e Metodi: Un questionario di 19 domande totali è stato elaborato e somministrato a 81 pazienti con l’obiettivo di valutare l’importanza della modalità di interazione del personale infermieristico con i pazienti sottoposti alla procedura di cardiologia interventistica nei momenti intra e procedurali.
Risultati: Il campione raccolto era significativamente eterogeneo perché la componente maschile era più frequente (p<0.001), i pazienti con più di 61 anni erano significativamente meno frequenti (p=0.0161) e i pazienti con diploma di scuola elementare o inferiore (p<0.001) erano significativamente più frequenti. I pazienti hanno espresso un alto livello di soddisfazione per quanto riguarda la valutazione del personale infermieristico, la gentilezza e la cortesia mostrate loro e l’attenzione prestata ai loro problemi, il tempo a loro dedicato, il livello di informazioni ricevute sulla procedura e il post-procedura, l’aiuto per risolvere eventuali inconvenienti verificatisi al momento della procedura stessa. I pazienti sono stati moderatamente soddisfatti per gli infermieri che li hanno assistiti direttamente nella procedura e di come hanno compreso e risposto a tutte le loro domande. Anche per la valutazione di: privacy, informazioni ricevute per il post- procedura, valutazione degli ambienti, pulizia, silenzio e temperatura, i pazienti hanno più frequentemente espresso un moderato livello di soddisfazione.
Discussione: Il presente studio ha mostrato un buon livello di soddisfazione per la percezione della qualità nei pazienti sottoposti a procedura cardiologica interventistica. Ulteriori sviluppi sono auspicabili al fine di generare un questionario validato che potrebbe essere adattato alle nostre realtà sanitarie e al campionamento più numeroso di pazienti.
Parole Chiave: Prestazioni infermieristiche; Qualità percepita; Qualità per il paziente; Servizio di Cardiologia Interventistica.
INTRODUCTION
The definition of Quality in Healthcare originated immediately after the end of the Second World War. Deming W. Edward [1] had developed a critical view on production methods in the U.S.A. during the war, particularly on methods of quality control, since management and engineers controlled the process and line workers played a small role. In his lectures he promoted the new statistical tools in order to quantify quality in industrial world. In the early 1950s he traveled to Japan and began to spread and compare the Quality Management in Quality Control, extending to all business sectors the goal of quality. Ten years later, Deming received a high recognition from the Emperor of Japan and, its idea known as “Total Quality Management” (TQM) became widely involved in Japanese business organizations and entrepreneurial culture. It will take another twenty years for knowledge of TQM concepts and techniques to spread to the industrialized world of the West. Since then, a rich series of theoretical approaches have followed.
Borrowing from Ceosby’s quality concept from industry, Avedis Donabedian implemented the concept of quality in the healthcare setting as: “the degree with care complies current criteria of good medicine”, by also including the concept of evaluation in its definition. Moreover, a specific definition of Quality in healthcare setting could be: “do only what is useful (theoretical efficacy), in the best way (practical efficacy) with the lowest cost (efficiency), to whom (accessibility), and only to those who really need it (appropriateness), having the care done by those who are competent to do it (competence), obtaining the results deemed best (satisfaction)”.
Always borrowing the concept of quality from industry, the ISO9000 standards – which are now a consolidated reference for this sector – are also applicable to the healthcare sector.
Moreover, thanks to the D.L. 502/92 and the D.L. 517/93 and the subsequent D.P.R. 801/97 (which introduces the concept of accreditation of healthcare structures and the systems for evaluating and improving activities) and D.L. 229/99 (which reaffirms the need to guarantee the quality of assistance and proposes the method of verification and revision, by providing agreements between the Region and Healthcare Organizations) the regulatory framework on quality in healthcare defined better the fields of action. It is on the basis of these legislative guidelines that Healthcare Companies have started to encourage the discussion on organizational quality and on the quality perceived by the user / patient [2-4].
As part of a project to improve clinical care pathways in the Interventional Cardiology Service of the “Madonna delle Grazie” Hospital sited in Matera, a questionnaire was developed and administered that aims to assess the importance of the way the nursing staff interacts with the patient who undergoes the interventional cardiology procedure in the intra and peri- procedural. The purpose of our study is to investigate how patients perceive the quality of care provided in the interventional cardiology service, and therefore, whether they are satisfied with the care received.
MATERIALS AND METHODS
Study Population
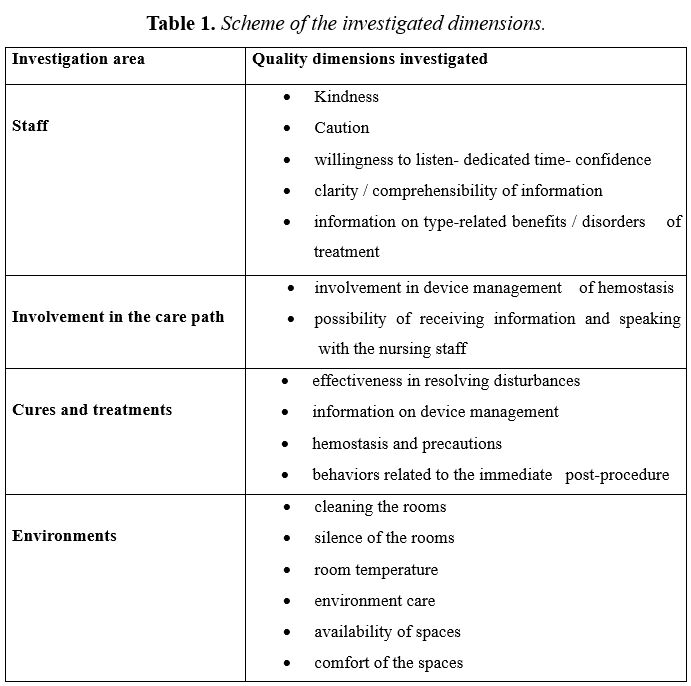
By considering the Dossier of the Regional Health Agency of Emilia Romagna, entitled: “The perceived quality in Emilia Romagna” (2006) [5], a questionnaire of 19 items (Appendix I) was elaborated and subsequently administered to 81 consecutive patients belonging to the Interventional Cardiology service of the “Madonna delle Grazie” hospital who underwent interventional cardiology procedures. The study was conducted from April 2017 to April 2018.The patient’s consent was requested and, only after his authorization was it administered anonymously and no economic incentives were offered or provided for participation in this study. Informed consent was obtained by all patients included in this study. For all patients anonymity was guaranteed. No economic incentives were offered or provided for participation in this study. This study was performed in accordance with the ethical considerations of the Helsinki Declarations. A formal authorization was requested from the hospital for data collection and Local Ethical Committee ruled that no formal ethics approval was required in this case. The questionnaire administered investigated four salient areas of perceived quality, listed in Table 1. The initial section of the questionnaire collected the socio-personal data of participants, as: sex, age, educational level, professional condition, nationality, marital status and condition of coexistence. In addition, the duration of treatment and the cardiac invasive interventions (as: coronary angiography and PTCA or implantation or replacement of PM or electrical cardioversion) were requested. In the most consistent part of the questionnaire, relating to the quality of care and treatment, in order to investigate the particularity of the patient’s condition, a section was included listing some of the typical ailments that patients could experience during the procedure and asked to indicate for each of these the possible onset, the level of tolerability and, if some intervention had been carried out and, finally, the evaluation of the latter.
Instruments
A first part of the questionnaire concerned the collection of the demographics of the participants, as the gender, the age group to which the respondents belong, if up to 40 years old, from 41 to 60 years old or above 61 years old; the qualification, also grouping this variable in 3 possible answers: if he had either an elementary or lower secondary school diploma, or if he had a diploma or a degree. The questionnaire elaborated “ad hoc” and used for the first time in this research, contained also 19 questions investigating four dimensions of healthcare quality, such as: the nursing staff evaluation, the privacy assessment, the evaluation of information received on the post procedure, the evaluation of environments (Table 1).
Each item of the questionnaire is scored with a 5-point Likert scale (1=very dissatisfied, 2=dissatisfied, 3=moderate, 4=satisfied, 5=very satisfied). For each question, participants had to indicate a single answer between proposals. The study was conducted from April 2017 to April 2018.
Statistical analysis
Statistical analyses were performed using IBM SPSS 20 software.
Data are presented as numbers and percentages for categorical variables, and continuous data expressed as the mean±standard deviation (SD) unless otherwise specified. A binomial test was performed to compare two mutually exclusive proportions. A multiple comparison chi-square test was used to define significant differences among percentages for unpaired data. In this case, if the chi-square test was significant (p<0.05), a post hoc Z-test was performed to individualize the significant most or less frequent modality. All tests with p<0.05 were considered significant.
RESULTS
In the period between April 2017 and April 2018, 81 patients agreed to participate in this interview. Of these, 24 (29.63%) were female patients and 57 (70.37%) were male patients. Among the patients interviewed 30 (37.04%) were aged up to 40 years, 36 (44.44%) were aged between 41 and 60 years and only 15 (18.52%) were aged between over 61 years old. Furthermore, as many as 50 (61.73%) interviewees had a primary or lower secondary school diploma, 24 (29.63%) a diploma and only 7 (8.64%) a degree. Therefore, overall, our sample is significantly heterogeneous as there is a strong male component (p<0.001) and the age groups were not equal in their sample size, in fact, significant less frequent were patients older than 61 years (p=0.0161). Also as regards the education level, the group of participants is not homogeneous, in fact, patients with an elementary or lower secondary school diploma, were more frequent (p<0.001).
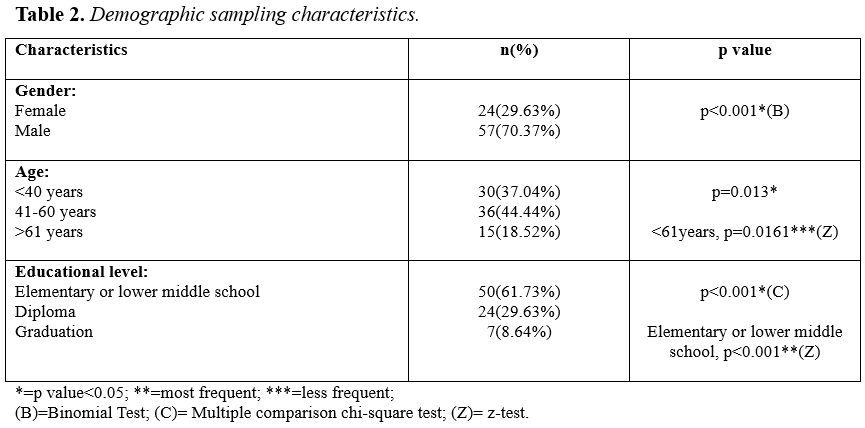
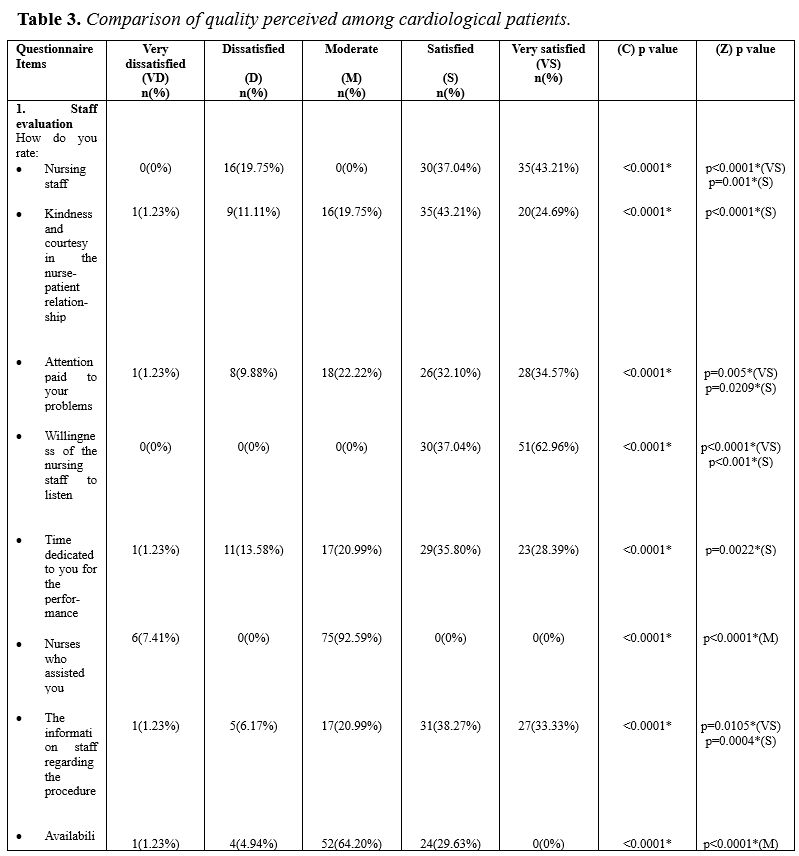
Table 3 shows the number of responses and the relative percentages for the answers given regarding the perception of the quality of the interventional cardiology service.
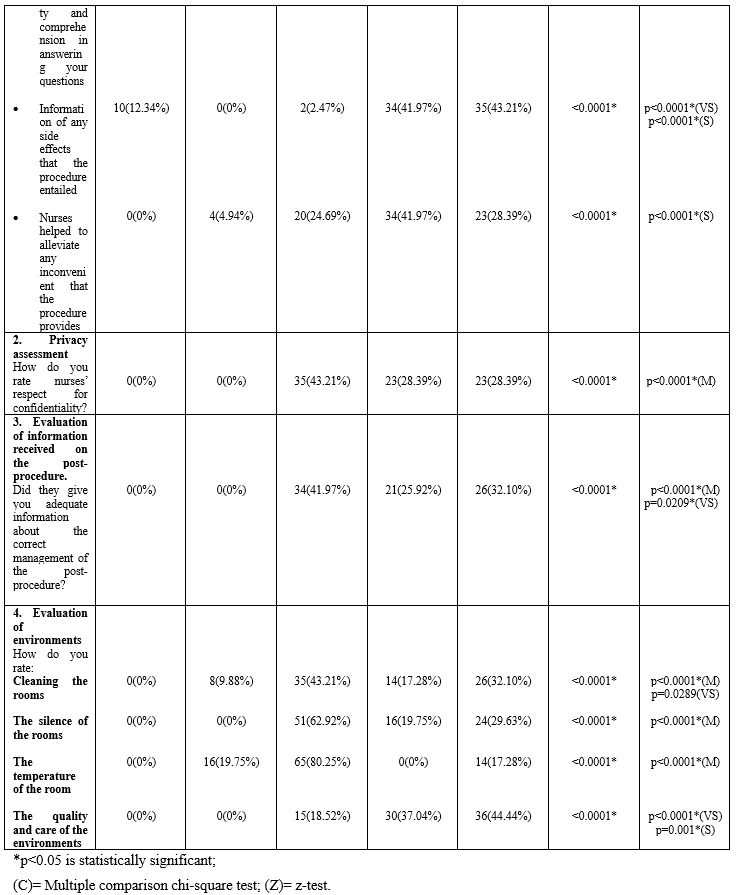
For questions related to the evaluation of nursing staff, significant more frequent answered were “satisfied” or “very satisfied”. Particularly, for the first question concerning the general evaluation of the nursing staff, about the nursing staff available to them, patients “satisfied” (p=0.001) and “very satisfied” (p<0.001) were significant more frequent. As for the level of perception of kindness and courtesy in the nurse-patient relationship, the more frequent response was “satisfied” (p<0.001), obtained by 35 (43.21%) patients. About the level of attention paid by the service nurses to the problems of the patients interviewed, satisfactory (p=0.0209) and very satisfactory (p=0.005) answers were the more frequent. A good level of willingness to listen was attributed by patients who significant most frequent responded that they were satisfied (p<0.001) and very satisfied (p<0.0001) for this aspect. About time dedicated to patients, they were significant more frequent satisfied (p=0.0022), while they were significant more frequent moderately satisfied (p<0.0001) for the nurses dedicated to them for assistance with the procedure. For the level of information received by the nursing staff about the progress, patients were significant more frequent satisfied (p=0.0004) and very satisfied (p=0.0105). On the other hand, for availability and understanding in answering their questions, patients (n=52) were significant most frequent moderately satisfied (p<0.0001). For every information of any side effects that the procedure entailed 34 (41.97%) patients were significant most frequent satisfied (p<0.0001) and 35 (43.21%) were considered significant most frequent very satisfied (p<0.0001). Moreover, as many as 34 (41.97%) patients were significant most frequent satisfied (p<0.0001) for the nursing care received in order to alleviate any inconvenience related to the procedure. For the level of evaluation of respect for privacy, 35 (43.21%) patients were significant most frequent moderately satisfied (p<0.001). As regards the evaluation of the information received for the post procedure 34 (41.97%) patients were also significant most frequent satisfied (p<0.0001) and 26 (32.10%) were significant most frequent very satisfied (p=0.0209). Finally, as regards the assessment of the rooms, in particular for the cleaning of the rooms, 35 (43.21%) patients were significant most frequent satisfied (p<0.0001) and 26 (32.01%) very satisfied (p=0.0289). For the quietness of the environments, 51 (62.92%) patients were most frequent moderately satisfied (p<0.0001) and, for the environmental temperature 65 (80.25%) patients expressed most frequent moderate level of satisfaction (p<0.0001); while for the quality of care and the environment in general 30 (37.04%) patients were significant most frequent satisfied (p=0.001) and 36 (44.44%) patients were significant most frequent very satisfied (p<0.0001).
DISCUSSION
Our data collection was completely random, mainly linked to the availability of time to devote to the administration of the questionnaire and this meant that apart from the pre-established period of time, the entire sample collected is not homogeneous in its composition. In fact there was significant most frequent male component (n=57) compared to 24 female patients (p<0.001). Furthermore, the group of patients over the age of 61 was also significantly less frequent (p=0.0161) than the other groups and there was a significant most frequent component of patients with an elementary or lower secondary school leaving qualification (p<0.001). In general, patients showed a high level of satisfaction with the interventional cardiology service. As regards the part concerning the evaluation of the nursing staff, patients were significant most frequent satisfied and very satisfied both for the evaluation of the nursing staff in general and for the kindness and courtesy shown to them, and for the attention paid their problems, the time dedicated to them, the level of information received about the procedure and the post-procedure, the help to resolve any inconvenience that occurred at the time of the procedure itself. Only for the aspects related to the nurses who directly assisted them in the procedure and in the willingness and understanding to answer all their questions, patients were significant most frequent moderately satisfied. So also for the evaluation of privacy, patients were significant most frequent as moderately satisfied. Instead, for the evaluation of the information received for the post procedure, the nurses were considered significant most frequent moderately satisfied and also satisfied. For the assessment of the rooms, in particular for the cleaning, the silence and the temperature of the rooms, patients showed a moderate level of satisfaction. While they expressed a high level of satisfaction in the general assistance received and the quality of environments, in general. Reflecting on the data collected and on their level of statistical significance, it is clear that overall patients are satisfied and very satisfied on the quality of the overall nursing care received. Only in the aspects related to the assistance received “at the moment” procedure and to the availability to answer to questions related to the moment of the procedure patients gave a more moderate answers, maybe they could show more anxiety for the procedure which could reduce patient satisfaction level. This aspect is widely discussed in the literature, in which the reduction of the quality perceived by the patient is reduced by the anxiety that a particular invasive procedure entails [6-8]. This discourse could also be the basis for the perception of quality linked to cleanliness of rooms, silence and temperature. Maybe the perception of these aspects is influenced by the anxiety of undergoing the invasive procedure, as reported in the literature.
In the current literature, there are few studies available in the literature that deal with quality assessment in interventional cardiology. Furthermore, some studies explore this aspect using the style of qualitative research. One example is the study of Nakano et al. [9] which aimed to investigate what preoccupied patients admitted to cardiac care unit with acute coronary syndrome in connection with the first hours of their admission and secondly to discuss these perceptions in relation to the nurses’ perception. In this case a qualitative descriptive analysis of 30 semi-structured interviews was carried out. It was highlighted that the patients thought that the care providers’ competencies were most important and they knew their job. The latter aspect is not in agreement with our results since the patients responded with a high statistical significance (p<0.0001) on the excellent satisfaction perceived towards the nurses always ready to relieve their pain.
Unfortunately, the perceived quality has not always been interpreted as an opportunity, an opportunity for listening and an indication for improvement: in fact, the problem of detecting the quality perceived within Healthcare Companies has often presented inconsistencies in the definition objectives and in the use and interpretation of results [10]. The absence of specific skills within the Companies, the onerousness of the methodological apparatus (sometimes, moreover, circumvented) linked to these surveys, the incomprehension on how to interpret and even more to use the data (often intended as confirmation and as mere communication tool rather than as an operating lever for improvement), have contributed to creating a context that is still very wary of perceived quality conceived as a system [11]. From these preliminary considerations, it is evident how to integrate / decline / use within the company strategies the package or system consisting of scientific instrumentation for the detection of perceived quality, which is poor in clear and clear reference points. It is therefore necessary to dwell on some definitions that will serve to trace the boundaries of the space in which one is moving: the peculiarity of the context of the Healthcare companies; the definition of quality and perceived quality, distinguishing the patient / user from the operator side; the improvement. As for the meaning of quality, in the sense referred to in this volume, the starting point is the traditional distinction proposed by Donabedian (1988) [12] which identifies three specific areas of intervention on quality:
- organizational quality linked to the available resources and the ways in which they are organized;
- professional or process quality, which refers to the product, the performances, the technical correctness of execution of the same also in terms of appropriateness and timeliness, and in a broad sense to the behavior of the operators;
- perceived quality, which instead concerns the outcome (including the patient’s point of view) or the changes in health conditions due to health interventions in terms of prolonging life and reducing pain and disabilities, or on the contrary the occurrence of iatrogenic complications or effects. From a different point of view, each dimension of the concept of quality identified in the Donabedian tripartition [12] can be interpreted as explaining the requests (even conflicting) of the major interest groups (stakeholders), which must be integrated and mediated to specify the quality of a service;
- organizational quality, that is, the most effective and productive use of resources by management within the limits set by regulatory requirements and objectives set by regional authorities or bodies that purchase services;
- professional quality, which identifies the role and point of view of the professionals and operators who provide care and assistance;
- perceived quality, which gathers the expectations of customers (external or internal) as individuals or as groups.
It must therefore be clear in the Company’s strategy that no quality is given for a single actor or for a single category of actors involved in the health process and that the evaluation of the quality of services and services is not the result of an aseptic standardization of the activities, nor the neutral application of a method; it is within a conception of evaluation as a negotiation and communication of different perspectives by multiple actors, it is multi-criteria evaluations that operate through both qualitative and quantitative investigation techniques [13].
Conclusion
The present study showed a good level of satisfaction in the quality perception in patients who underwent an invasive cardiology procedure. Further future developments are desirable both in performing a validated questionnaire, adaptable in our healthcare realities, and in the larger number of samples in order to be able to generalize the data obtained. In any case, our study represents a strong point of the nursing quality delivered to these patients at least in our working reality.
Limitations
This study discusses a very important topic, such as the perception of quality in the interventional cardiology unit. However, the survey method is characterized by a questionnaire constructed “ad hoc” for the occasion and which refers to the usual behavior of the nursing staff without considering a comparison term with an optimal or standardized nursing behavior. In any case, our questionnaire is inspired by the World Health Organization document entitled “Quality of care: a process for making strategic choices in health systems” [14] which highlights the six generic domains to improvement quality in many health systems, such as: leadership, information, patient and population engagement, regulation and standards, organizational capacity and models of care.
Funding statement
This research did not receive any specific grant from funding agencies in the public, commercial, or not for profit sectors.
Competing interests statement
There are no competing interests for this study.
REFERENCES
- Petersen PB. Total quality management and the Deming approach to quality management. Journal of Management History (Archive) 1991; 5(8):468-488. doi:10.1108/13552529910290520
- Aiken LH, Sean PC, Douglas MS. Hospital staffing, organization, and quality care: cross-national findings. Int J Qual Health Care 2002; 14:5-13
- Blumenthal D. Quality of care: what is it? N Engl J Med 1996; 335:891-894.
- Bolton LB, Aydin CE, Donaldson N, Brown DS, Nelson MS, Harms D. Nurse staffing and patient perceptions of nursing care. J Nurs Adm 2003; 33:607-14.
- Agenzia sanitaria regionale Regione Emilia – Romagna/ Dossier. La qualità percepita in Emilia – Romagna; Strategie, metodi e strumenti per la valutazione dei servizi
- Mammadov A, Gasanov R. Research on a relationship between patient satisfaction and medical services in state health organizations. Am J Ind Bus Manage 2017;07(11):1255-1266. doi:10.4236/ajibm.2017.711089.
- Liu L, Fang J. Study on potential factors of patient satisfaction: based on exploratory factor analysis. Patient Preference and Adherence 2019; 13:1983-1994. doi: 10.2147/PPA.S228073.
- Farzianpour F, Byravan R, Amirian S. Evaluation of patient satisfaction and factors affecting it: a review of the literature. Health 2015; 07(11):1460-1465. doi:10.4236/health.2015.711160
- Nakano A, Mainz J, Lomborg, K. Patient Perception and Assessment of Admission to Acute Cardiac Care Unit. European Journal of Cardiovascular Nursing 2008; 7(1):10-15. doi:10.1016/j.ejnurse.2007.05.002
- Agosta L J. Patient satisfaction with nurse practitioner-delivered primary healthcare services. Journal of the American Academy of Nurse Practitioners 2009; 21(11): 610-617.
- Aiken LH, Sermeus W, Van den Heede K, Sloane D M, Busse R, McKee M, Tishelman C. Patient safety, satisfaction, and quality of hospital care: cross sectional surveys of nurses and patients in 12 countries in Europe and the United States. British Medical Journal 2012; 344: e1717.
- Donabedian A. The quality of care. How can it be assessed? The Journal of the American Medical Association 1988; 260: 1743-1748.
- Suhonen R, Papastavrou E, Efstathiou G, Tsangari H, Jarosova D, Leino-Kilpi H, et al. Patient satisfaction as an outcome of individualised nursing care. Scandinavian Journal of Caring Sciences 2012; 26: 372-380.
- World Health Organization. (2006). Quality of care : a process for making strategic choices in health systems. World Health Organization. https://apps.who.int/iris/handle/10665/43470
Appendix I. The questionnaire administered
Sex: [ ] Female [ ] Male
Age: [ ] <40 years [ ] 41-60 years [ ] >61 years
Education level:
[ ] Elementary or lower middle school
[ ] Diploma
[ ] Graduation
1.Staff evaluation:
How do you rate:
- Nursing staff:
[ ] Very Dissatisfied; [ ] Dissatisfied; [ ] Moderate; [ ] Satisfied; [ ] Very Satisfied.
- Kindness and courtesy in the nurse-patient relationship:
[ ] Very Dissatisfied; [ ] Dissatisfied; [ ] Moderate; [ ] Satisfied; [ ] Very Satisfied.
- Attention paid to your problems:
[ ] Very Dissatisfied; [ ] Dissatisfied; [ ] Moderate; [ ] Satisfied; [ ] Very Satisfied.
- Willingness of the nursing staff to listen:
[ ] Very Dissatisfied; [ ] Dissatisfied; [ ] Moderate; [ ] Satisfied; [ ] Very Satisfied.
- Time dedicated to you for the performance:
[ ] Very Dissatisfied; [ ] Dissatisfied; [ ] Moderate; [ ] Satisfied; [ ] Very Satisfied.
- Nurses who assisted you:
[ ] Very Dissatisfied; [ ] Dissatisfied; [ ] Moderate; [ ] Satisfied; [ ] Very Satisfied.
- The information staff regarding the procedure:
[ ] Very Dissatisfied; [ ] Dissatisfied; [ ] Moderate; [ ] Satisfied; [ ] Very Satisfied.
- Availability and comprehension in answering your questions:
[ ] Very Dissatisfied; [ ] Dissatisfied; [ ] Moderate; [ ] Satisfied; [ ] Very Satisfied.
- Information of any side effects that the procedure entailed:
[ ] Very Dissatisfied; [ ] Dissatisfied; [ ] Moderate; [ ] Satisfied; [ ] Very Satisfied.
- Nurses helped to alleviate any inconvenient that the procedure provides:
[ ] Very Dissatisfied; [ ] Dissatisfied; [ ] Moderate; [ ] Satisfied; [ ] Very Satisfied.
- Privacy assessment
How do you rate nurses’ respect for confidentiality?
[ ] Very Dissatisfied; [ ] Dissatisfied; [ ] Moderate; [ ] Satisfied; [ ] Very Satisfied.
- Evaluation of information received on the post-procedure
Did they give you adequate information about the correct management of the post-procedure?
[ ] Very Dissatisfied; [ ] Dissatisfied; [ ] Moderate; [ ] Satisfied; [ ] Very Satisfied.
- Evaluation of environments
How do you rate:
Cleaning the rooms:
[ ] Very Dissatisfied; [ ] Dissatisfied; [ ] Moderate; [ ] Satisfied; [ ] Very Satisfied.
The silence of the rooms:
[ ] Very Dissatisfied; [ ] Dissatisfied; [ ] Moderate; [ ] Satisfied; [ ] Very Satisfied.
The temperature of the room:
[ ] Very Dissatisfied; [ ] Dissatisfied; [ ] Moderate; [ ] Satisfied; [ ] Very Satisfied.
The quality and care of the environments:
[ ] Very Dissatisfied; [ ] Dissatisfied; [ ] Moderate; [ ] Satisfied; [ ] Very Satisfied.
![]() This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.