Asnidawati1, Wa Ode Salma2*, Adius Kusnan3
- Public Health of Faculty, Haluoleo University, Kendari, Indonesia
- Nutrition department, Public Health of Faculty, Haluoleo University, Kendari, Indonesia
- Nursing department, Medical of Faculty, Haluoleo University, Kendari, Indonesia
* Corresponding Author: Wa Ode Salma, waode.salma@uho.ac.id, Nutrition department, Public Health of Faculty, Haluoleo University, Kendari, Indonesia
Cita questo articolo
ABSTRACT
Background: Breast’s milk is an excellent food for the growth and development of infants. The United Nations Children’s Funds (UNICEF) and the World Health Organization (WHO) recommend that children only be exclusively breastfed for six months and continued until two years. This study analyzes the effect of family support, health workers, and socio-culture on exclusive breastfeeding in the working area of the Rumbia Health Center, Rumbia District, Bombana Regency.
Methods: This study involved 86 mothers who had babies aged 0-6 months who were registered and domiciled in the working area of the Rumbia Health Center spread over 4 Kelurahan and 1 Village, which were selected by purposive sampling using a cross-sectional design from February to April 2021. Data analysis using odds ratio (OR) and logistic regression at significance level < 0.05.
Results: The largest age group in the range of 20-35 years, as many as 68 people (79.1%), undergraduate as many as 32 people (37.2%), and income above Rp. 2.552.014, – / month as many as 60 people (69.8%). The results showed an effect of family support on exclusive breastfeeding (p = 0.002<0.05). There is no influence of socio-cultural factors on exclusive breastfeeding (p = 0.282>0.05) and the results of multivariate analysis of the most dominant variables associated with exclusive breastfeeding in the working area of Rumbia Health Center District Rumbia Bombana Regency is supported by health workers with an OR = 9.199 (p-value = 0.039<0.05).
Conclusions: This study concludes that the support of health workers plays a very important role in exclusive breastfeeding to infants aged six months, which can impact improving the health of toddlers.
Keywords: Determinant, breastfeeding exclusive, toddler, mother
INTRODUCTION
Breast milk is an ideal food for infant growth and development [1,2]. The United Nations Children’s Funds (UNICEF) and the World Health Organization (WHO) recommend that children be breastfed exclusively for six months and continued until two years. Global research reports in 2018 showed that the rate of exclusive breastfeeding was quite low, only 41 percent [3]. Meanwhile, in Indonesia, data from the Basic Health Research (RISKESDAS) in 2018 showed that the rate of exclusive breastfeeding was only 37 percent [4]. It is known that the rate of exclusive breastfeeding is still low globally, and it is possible that in Indonesia, the coverage rate of exclusive breastfeeding is below 37% due to the consequences of the Covid-19 pandemic [5].
The study results in 19 developing countries show that socio-cultural factors such as maternal beliefs and other people are significantly strong barriers to exclusive breastfeeding [6–8]. Another study reported that in general, mothers know about breastfeeding, and the majority of respondents (97.3%) had breastfed their babies, 56.5% of them started within one hour after delivery, and 74.1% only gave exclusive breastfeeding until a mean age of 4 months and 30.7% had bottle-fed [9].
The importance of appropriate breastfeeding practices for the healthy growth and development of infants and children has been presented in various policy documents, and guidelines have been set on how to practice exclusive breastfeeding [10]. Social support is widely recognized as influencing the practice of breastfeeding exclusively for six months and continuing to breastfeed for at least two years [11,12]. In addition, health care worker supporting interventions have been shown to increase the rate of exclusive breastfeeding in many developing countries [13,14].
The coverage of achieving exclusive breastfeeding in 2017 in Southeast Sulawesi province for infants 0-6 months was 55.56%, and the coverage of achieving exclusive breastfeeding in 2018 increased by 72%. Although it increased from the previous year, it was not significant and still far from the national target (80%) and the target for Southeast Sulawesi Province (85%). Fluctuating achievements indicate that the exclusive breastfeeding improvement program is not standardized by related technical programs [15]. The working area of the Rumbia Health Center is 40.74%. It is still far from the target set, 50% [16].
The coverage of exclusive breastfeeding in the working area of the Rumbia Health Center has continued to decline over the last three years. It is known that the results of data observations at the Rumbia Health Center showed that data related to mothers who brought their babies to come to the Posyandu in March 2020 recorded only 63 babies and 14 babies who received exclusive breastfeeding while 49 babies were not exclusive. Still far from the expected target of 108 infants (aged 0-6 months). It means that only about 22% of babies get exclusive breastfeeding, and 78% of babies do not get exclusive breastfeeding.
The outbreak of the covid-19 virus has greatly impacted health services, especially Posyandu services in the working area of the Bombana district office, since it was announced that there were residents in Bombana Regency who were confirmed on Covid-19. Overall, Posyandu services at the Rumbia Health Center and other health centers in Bombana Regency are no longer organize the Integrated health service from April to May 2020; therefore, services, data collection, and counseling related to exclusive breastfeeding are not well controlled.
Based on the available scientific data and evidence, this research was conducted to find out how to the influence of family support, health workers, and socio-culture on exclusive breastfeeding in the working area of the Bombana District Health Office, especially at the Rumbia Health Center.
METHODS
Study design
This type of research is analytic observational using a cross sectional design with a purposive sampling technique, so that each participant in this study was selected based on the researcher’s considerations.
Participants Sampling
This study involved 86 mothers who had babies aged 0-6 months who were registered and domiciled in the working area of the Rumbia Health Center spread over 4 Kelurahan and 1 Village
Procedure Inclusion and exclusion criteria
To control the quality of research data, the researchers conducted an initial screening by setting sample criteria. The sample inclusion criteria were mothers who had babies aged 0-6 months, mothers who did not experience psychosomatic disorders, while babies who were sick during the study and were born with low birth weight were excluded from the study.
Instruments
In this study involved 3 variables, namely family support, Healthcare worker support and Social-Culture. All variables in this study were measured using a questionnaire which was prepared by the researcher himself by taking into account relevant reference sources [17–19] and had been tested and declared valid and reliable.
Statistical Analysis
Data are presented as numbers and percentages for categorical variables. Continuous data are expressed as the mean ± standard deviation (SD), or median with Interquartile Range (IQR). Data analysis in this study used the Odds Ratio (OR) test to determine the factors associated with breastfeeding exclusivity and multivariate analysis used logistic regression to determine the determinants of breastfeeding exclusivity. The results of the p-value will be the basis for the independent variables to be included in the logistic regression test if p < 0.30, while the dependent variable in the study was the provision of Breastfeeding Exclusive, which was measured using a questionnaire. All tests with p-value (p) < 0.05 were considered significant. Statistical analysis was performed using SPSS app version 16.0.
Ethical consideration
All participants in this study have signed a letter of willingness to participate in the study. No economic incentives were offered or provided for participation in this study. The study was performed in accordance with the ethical considerations of the Helsinki Declaration. This research has been approved by the Haluoleo University Health Research Ethics Commission numbered: 21/KEPK-IAKMI/III/2021.
RESULTS
In the results of this study, the characteristics of the mother, distribution of research variables, results of bivariate and multivariate analysis are presented. The distribution of respondents’ characteristics can be seen in the following Table 1:
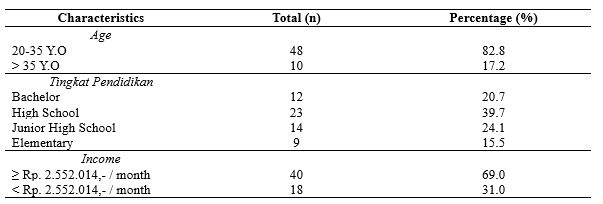
Table 1. Distribution of Respondents’ characteristics
Table 1 informs the largest age group in the range of 20-35 years, as many as 48 people (82.8%), high school as many as 23 people (39.7%), and income above Rp. 2.552.014, – / month as many as 40 people (69.0%).
Table 2 shows the distribution of the dominant study variables consisting of 50 people (58.1%) receiving family support, 67 mothers who received support from health workers (77.9%), and 79 mothers with good socio-culture. (91.9%). There is an effect of family support (p=0.002) and Healthcare worker support (p=0.004) on exclusive breast-feed. There is no influence of socio-cultural factors on the exclusive breastfeeding (p = 0.282).
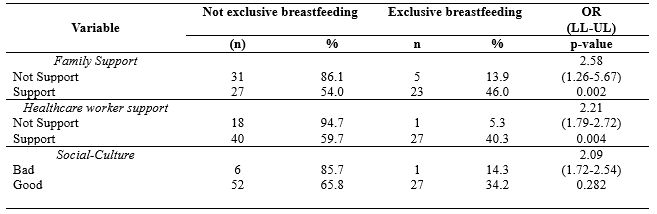
Table 2. Distribution of Study variable
Table 3 shows that after all independent variables were analyzed multivariate with logistic regression, the results obtained that the support of health workers had the greatest OR, namely 4.350 at 95% Cl with a lower limit value of 1.114 and an upper limit value of 75.974 because the confidence interval range was not. Including a value of 1 means that health workers support exclusive breastfeeding in the Work Area of the Rumbia Health Center, Rumbia District, Bombana Regency.
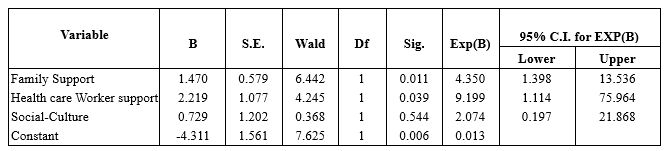
Table 3. Multivariate Analysis
DISCUSSION
- The Effect of Family Support on Exclusive Breastfeeding
The study results found that there was an effect of family support on exclusive breastfeeding in the working area of the Rumbia Health Center, Rumbia District, Bombana Regency. The results of this study are supported by several previous studies that state that exclusive breastfeeding success is closely related to family support, especially husbands and grandmothers of toddlers [20–22].
A mother needs support from the family in providing exclusive breastfeeding; support from the family will affect the mother’s decision to give exclusive breastfeeding [23]. The success in providing exclusive breastfeeding by mothers is very dependent on the environment, one of which is the husband or family. If mothers get support from the surrounding environment, mothers can comfortably provide exclusive breastfeeding and take care of their children while working at home. Support or support from other people or closest people, both family support and support from health workers, is very important in the success or failure of breastfeeding [24]. The greater support to continue breastfeeding, it makes the greater the ability to continue breastfeeding. Husband and family support is very influential; a mother who lacks her husband, mother, sister, or even being scared, is influenced to switch to formula milk [25].
The success factor of exclusive breastfeeding, in addition to knowledge, to be cleared, is accompanied by the mother’s own will. The role of health workers is very influential on the mother in the process of exclusive breastfeeding. The success of exclusive breastfeeding cannot be separated from family support because the family is the closest person who can encourage mothers to continue giving exclusive breastfeeding and the surrounding culture that encourages exclusive breastfeeding [26].
Family, apart from being a supporting factor, is also as retarder factor. The mother’s desire to give exclusive breastfeeding should have been discussed with the family, especially people who will live with the mother when the baby is born, for example, husband, mother, mother-in-law long before the baby is born or at least during the pregnancy phase [27]. In still to families regarding the importance of breastfeeding, how to give exclusive breastfeeding and what support they can provide. It is important, because in some cases, a mother’s failure to provide exclusive breastfeeding is precisely because of a misunderstanding from the family, for example, being given water, so the baby does not turn yellow, or adding a baby with formula milk because the baby cries and thinks the baby is still hungry and hungry. At that time, the baby’s mother had difficulty refusing or resisting because the one who gave it was the mother-in-law and her biological mother. This event will be minimized when the mother and family have good breastfeeding knowledge and a strong agreement and commitment to supporting mothers in exclusive breastfeeding.
- The Effect of Health Worker Support on Exclusive Breastfeeding
The study results found that there was an effect of the support of health workers on exclusive breastfeeding in the working area of the Rumbia Health Center, Rumbia District, Bombana Regency. Furthermore, the results of the multivariate analysis of this study found that the most dominant variable influencing exclusive breastfeeding in the working area of the Rumbia Health Center, Rumbia District, Bombana Regency, was the support of health workers with an OR value of 9.633.
According to the theory, the support of officers is very helpful, where the support of officers has a big influence on exclusive breastfeeding [22]. A health worker is responsible for health workers who provide health services to individuals, families, and communities. If health workers actively socialize with the community, they can change traditions or habits that can slowly harm health, such as providing complementary foods to infants before six months [28]. Thus, the public will know and understand more about traditional practices that can be detrimental to health so that they will change their behavior and mindset towards what they know from the health worker [29]. The encouragement of health workers can influence respondents to have a high intention of giving exclusive breastfeeding to their babies. The success of breastfeeding mothers requires health workers, especially perinatal service workers such as midwives who are trained and understand the ins and outs of the breastfeeding process. They are the first to help mothers give birth to give breast milk to babies. The role of health workers is the beginning of the mother’s success or failure in exclusive breastfeeding. Knowledge, attitudes, and actions of health workers such as midwives are the determinants of the readiness of officers in managing breastfeeding mothers with lactation management (lactation management) so that the implementation of exclusive breastfeeding increases.
This study is in line with previous studies concluding that there is a relationship between the support of health workers and exclusive breastfeeding (p-value = 0.0001) with a PR of 2.48, meaning that mothers who receive support from midwives have a 2.48 times greater chance of breastfeeding independently—exclusively compared to mothers who received less support from the midwife [28]. Furthermore, in line with other research in South Tomohon, it shows a relationship between the support of health workers in exclusive breastfeeding for six months in the Pangolombian Community Health Center, South Tomohon District, p-value = 0.008 [30].
- The Influence of Socio-Cultural Factors on Exclusive Breastfeeding
The results showed no influence of socio-cultural factors on exclusive breastfeeding in the working area of the Rumbia Health Center, Rumbia District, Bombana Regency. Breastfeeding cannot be separated from the cultural order. Every breastfeeding from mother to child will be related to the social culture that exists in the community. Behavior is formed by habits that are colored by social culture. Everyone is always exposed and touched by environmental habits and is influenced by the community, either directly or indirectly. Behavior that habits and beliefs have shaped about exclusive breastfeeding will impact the mother’s desire to give exclusive breastfeeding to children. This socio-cultural will affect the success of exclusive breastfeeding; respondents who have good socio-cultural categories will show success in exclusive breastfeeding. The good social culture indicates it in providing exclusive breastfeeding, as many as 27 people (34.2%) and those who do not give exclusive breastfeeding, as many as 52 people (65.8%) while out of 7 respondents with poor socio-culture giving exclusive breastfeeding, one person (14.3%) and who did not give exclusive breastfeeding were six people (85.7%). The beliefs and traditions that exist in the community lead to the community’s mindset on the actions taken to respond to something. Beliefs that exist in society are very important in shaping a person’s behavior.
A study conducted [31] in Athens, Greece, found that the breastfeeding process is often not determined by biological factors but is mainly based on habits, traditions, and behaviors in society. Tradition is a social behavior where the behavior is passed down from generation to generation by going through socialization. A tradition determines the values and morals of society because tradition contains rules according to the community about what should be done.
Habits are carried out from generation to generation and carried out by the community, the judge, and assumes that it is the most correct and good thing [32]. The mother’s beliefs and desires to imitate the mother’s intention to breastfeed her baby. The respondent’s intention to do exclusive breastfeeding is influenced by the mother’s own beliefs and beliefs [33]. Logically, the existence of a tradition in Rumbia District regarding breastfeeding is closely related to the mother’s intentions and expectations regarding exclusive breastfeeding success. Traditions and beliefs develop a pattern to lead people’s behavior to do things under the traditions and beliefs that exist in their environment, such as colostrum contained in breast milk are not good and dangerous for babies, special teas or liquids are needed by babies before breastfeeding, and babies will experience a lack of nutrients for growth if only given breast milk [34].
Unfulfilled breast milk needs will cause malnutrition in children—some dietary restrictions at certain times and certain types of food that should not be eaten while breastfeeding. The lack of knowledge of mothers about nutrition and their beliefs causes nutritional problems for their children and impacts the body’s defense against infection and delays in growth and development [35]. Interventions promoting behavior change should focus on dispelling less than optimal beliefs and practices into beliefs to build positive breastfeeding practices, involving family support (partners and other family members) as they are an important source of information about breastfeeding [36,37]. Changing people’s habits and beliefs is not an easy task, so the role of health workers is very much needed to carry out activities to increase exclusive breastfeeding programs. Guidelines for increasing exclusive breastfeeding programs cannot be separated from the reproductive process of mothers after giving birth, which is expected to change the behavior of people who initially do not believe in the benefits and benefits of breastfeeding to believe and slowly leave the culture and tradition of giving additional food to infants aged 0-6 months. which can interfere with health [38].
The development of community and religious leaders is an important strategy for the health workforce because people tend to obey the directions of trusted people around their environment than people outside their environment. Community empowerment about the importance of exclusive breastfeeding for babies is known by all levels of society, which is expected to provide support and motivation for breastfeeding mothers and can automatically improve reproductive health.
CONCLUSIONS
The success of the Breastfeeding exclusive program is strongly influenced by various factors such as family support such as husbands and grandmothers of toddlers, as well as support from health workers through promotional programs when mothers of toddlers visit health care facilities, as well as socio-cultural factors that are believed by the family such as the existence of dietary restrictions for babies of a certain age, babies born must be given sweet food immediately, at a certain age babies must be given food in traditional events.
This study suggests the importance of the role of health workers in providing a good understanding to families about the benefits of exclusive breastfeeding until the baby is 6 months old.
Limitations study’s
In this study, there are limitations such as the presence of some areas that cannot be reached by the research team so they cannot participate in the study. Then in this study using a cross-sectional design so that the information obtained by researchers is only limited to data when the research is conducted.
Clinical implications of research
The results of this study can be the basis for health workers in maximizing the role of the family in supporting mothers to provide exclusive breastfeeding to infants and paying attention to the socio-cultural background of the family, especially mothers in providing interventions in the field, especially regarding exclusive breastfeeding.
ACKNOWLEDGEMENT
We would like to express our gratitude to several parties who have provided support for our research. To the chief of the Poltekkes Jambi in her support in providing suggestions and input for the development of this research, and to mothers who have actively participated as respondents in this research.
FUNDING STATEMENT
This research did not receive any specific grant from funding agencies in the public, commercial, or not for profit sectors.
CONFLICT OF INTEREST
The author(s) declares no conflict of interest.
REFERENCES
- Meier PP, Patel AL, Bigger HR, Rossman B, Engstrom JL. Supporting breastfeeding in the neonatal intensive care unit: Rush Mother’s Milk Club as a case study of evidence-based care. Pediatric Clinics. 2013;60(1):209–26.
- Piemontese P, Liotto N, Mallardi D, Roggero P, Puricelli V, Giannì ML, et al. The effect of human milk on modulating the quality of growth in preterm infants. Frontiers in pediatrics. 2018;6:291.
- Osibogun OO, Olufunlayo TF, Oyibo SO. Knowledge, attitude and support for exclusive breastfeeding among bankers in Mainland Local Government in Lagos State, Nigeria. International breastfeeding journal. 2018;13(1):1–7.
- Kementerian Kesehatan. Profil Kesehatan Indonesia. Jakarta: Depkes RI; 2018.
- Unicef. Breastfeeding: a mother’s gift, for every child. Unicef; 2018.
- Balogun OO, Dagvadorj A, Anigo KM, Ota E, Sasaki S. Factors influencing breastfeeding exclusivity during the first 6 months of life in developing countries: a quantitative and qualitative systematic review. Maternal & child nutrition. 2015;11(4):433–51.
- Nsiah-Asamoah C, Doku DT, Agblorti S. Mothers’ and Grandmothers’ misconceptions and socio-cultural factors as barriers to exclusive breastfeeding: A qualitative study involving Health Workers in two rural districts of Ghana. PloS one. 2020;15(9):e0239278.
- Henry BA, Nicolau AIO, Américo CF, Ximenes LB, Bernheim RG, Oriá MOB. Socio-Cultural factors influencing breastfeeding practices among low-income women in Fortaleza-Ceará-Brazil: a Leininger’s Sunrise Model Perspective. Enfermería Global. 2010;19:1–13.
- Akinyinka MR, Olatona FA, Oluwole EO. Breastfeeding knowledge and practices among mothers of children under 2 years of age living in a military barrack in Southwest Nigeria. International Journal of MCH and AIDS. 2016;5(1):1.
- Tampah-Naah AM, Kumi-Kyereme A, Amo-Adjei J. Maternal challenges of exclusive breastfeeding and complementary feeding in Ghana. PloS one. 2019;14(5):e0215285.
- Laugen CM, Islam N, Janssen PA. Social support and exclusive breast feeding among Canadian women. Paediatric and perinatal epidemiology. 2016;30(5):430–8.
- Casal CS, Lei A, Young SL, Tuthill EL. A critical review of instruments measuring breastfeeding attitudes, knowledge, and social support. Journal of Human Lactation. 2017;33(1):21–47.
- Boateng M. Knowledge, attitude and practice of exclusive breastfeeding among mothers in Techiman, Ghana. Itä-Suomen yliopisto; 2018.
- Imdad A, Yakoob MY, Bhutta ZA. Effect of breastfeeding promotion interventions on breastfeeding rates, with special focus on developing countries. BMC public health. 2011;11(3):1–8.
- Dinkes Propinsi Sultra. Profil Kesehatan Propinsi Sulawesi Tenggara 2019. Kendari: Bidang Data dan Informasi; 2019.
- Dinkes Kabupaten Bombana. Profil Kesehatan. Rumbia: Bidang Data dan Informasi Kab/Bombana; 2019.
- Ramadani M. Dukungan keluarga sebagai faktor dominan keberhasilan menyusui eksklusif. Media Kesehatan Masyarakat Indonesia. 2017;13(1):34–41.
- Sitohang FD, Kahar IA, Sirait A. Faktor yang Berhubungan dengan Pemberian Asi Eksklusif pada Bayi Usia 6-12 Bulan di Wilayah Kerja Puskesmas Sigalingging Kabupaten Dairi Tahun 2017. Jurnal Ilmiah Keperawatan Imelda. 2019;5(1):568–78.
- Fajar NA, Purnama DH, Destriatania S, Ningsih N. Hubungan Pemberian ASI Eksklusif dalam Prespektif Sosial Budaya di Kota Palembang. JOURNAL-JIKM: JURNAL ILMU KESEHATAN MASYARAKAT. 2018;9(3):226–34.
- Nuzulia F. Hubungan antara dukungan keluarga dengan pemberian ASI eksklusif pada bayi di Desa Bebengan Kecamatan Boja Kabupaten Kendal. Jurnal Keperawatan Maternitas. 2013;1(1).
- Ratnasari D, Paramashanti BA, Hadi H, Yugistyowati A, Astiti D, Nurhayati E. Family support and exclusive breastfeeding among Yogyakarta mothers in employment. Asia Pacific journal of clinical nutrition. 2017;26(Supplement):S31.
- Kusumayanti N, Nindya TS. Hubungan dukungan suami dengan pemberian asi eksklusif di daerah perdesaan. Media Gizi Indonesia. 2017;12(2):98–106.
- Ku C, Chow SKY. Factors influencing the practice of exclusive breastfeeding among Hong Kong Chinese women: a questionnaire survey. Journal of clinical nursing. 2010;19(17‐18):2434–45.
- La Aga, Erwin AL. Cakupan dan Determinan Pemberian ASI Eksklusif di Pemukiman Kumuh Dalam Perkotaan di Kecamatan Tallo Kota Makassar. Majalah Kesehatan FKUB. 2019;6(1):44–55.
- Novena K. Hubungan Dukungan Keluarga terhadap Keberhasilan ASI Eksklusif pada Bayi Usia 0-6 Bulan di BPM Nihayatur Rokhmah Kuningan Kabupaten Blitar. STIKes Patria Husada Blitar; 2019.
- Hety DS, Susanti IY, Adiesti F, Muhith A. Maternal Knowledge, Husband’s Support, Cultural Support and Role of Health Workers in the Exclusive Breastfeeding Program at Mojosari Health Center. In: Proceedings of the Third International Seminar on Recent Language, Literature, and Local Culture Studies. Proceedings Series Journals Search EAI; 2020.
- Deslima N, Misnaniarti M, Zulkarnain HM. Analisis Hubungan Inisisi Menyusu Dini (IMD) Terhadap Pemberian ASI Eksklusif di Wilayah Kerja Puskesmas Makrayu Kota Palembang. JUMANTIK (Jurnal Ilmiah Penelitian Kesehatan). 2019;4(1):1–14.
- Zuhrotunida. Hubungan Dukungan Tenaga Kesehatan Dengan Keberhasilan ASI Eksklusif di Puskesmas Kutabumi. IMJ (Indonesian Midwifery Journal). 2018;1(2).
- Mi’rad KA, Agushybana F, Margawati A. Study of Madurese Perception and Behavior towards Maternal Health in Jember Regency. International Journal of Multicultural and Multireligious Understanding. 2020;7(3):273–82.
- Anita, Wantania J, Korompis M. Hubungan Antara Pengetahuan Ibu, Fasilitas Pelayanan Kesehatan, Dukungan Keluarga Dan Dukungan Petugas Dengan Pemberian Asi Ekslusif 6 Bulan Di Wilayah Kerja Puskesmas Pangolombian Kecamatan Tomohon Selatan. Paradigma. 2016;4(2).
- Daglas M, Antoniou E. Cultural Views and Practices Related to Breastfeeding. Health science journal. 2012;6(2):353.
- Kusnan A, Binekada IMC, Usman AN. The proxy determinant of complementary feeding of the breastfed child delivery in less than 6 months old infant in the fishing community of Buton tribe. Enfermeria clinica. 2020;30:544–7.
- Yusrina A, Devy SR. Faktor Yang Mempengaruhi Niat Ibu Memberikan ASI Eksklusif di Kelurahan Magersari, Sidoarjo. Jurnal Promkes: The Indonesian Journal of Health Promotion and Health Education. 2016;4(1):11–21.
- Hatta GR. Pedoman Manajemen Informasi Kesehatan di sarana pelayanan kesehatan. Jakarta: Universitas Indonesia. 2008.
- Salma WO, Suhadi LOMS, Irma A, Karo M. Rendahnya Pemberian ASI Eksklusif Pada Anak Etnik Pesisir Berhubungan dengan Kejadian Penyakit Tropis. Penguatan dan Inovasi Pelayanan Kesehatan. 2019;87.
- Wanjohi M, Griffiths P, Wekesah F, Muriuki P, Muhia N, Musoke RN, et al. Sociocultural factors influencing breastfeeding practices in two slums in Nairobi, Kenya. International breastfeeding journal. 2016;12(1):1–8.
- Joseph FI, Earland J. A qualitative exploration of the sociocultural determinants of exclusive breastfeeding practices among rural mothers, North West Nigeria. International breastfeeding journal. 2019;14(1):1–11.
- Batubara NS. Pengaruh Sosial Budaya Terhadap Pemberian ASI Eksklusif di Wilayah Kerja Puskesmas Batunadua Kota Padangsidimpuan Tahun 2015. Jurnal Kesehatan Ilmiah Indonesia (Indonesian Health Scientific Journal). 2016;1(1):59–66.